Embed Size (px)
Citation preview

MATERNAL SEPSIS: RISKS, ASSESSMENT, &
TREATMENT
Lisa Brening, RN, BSNOB Clinical Supervisor04/28/2015

OBJECTIVES
Recognize the prevalence of maternal sepsis in the ante/intra/post partum period.
Have a basic knowledge of the reasons that sepsis occurs in pregnancy and is often masked until severe sepsis presents.
Identify the risk factors that predispose our maternal population to sepsis.
Identify subtle changes in vital signs, lab work, and patient status that could be suggestive of impending sepsis.
Explain the importance of the sepsis tool. Identify the proper actions to take when sepsis is
suspected. Explain how to adequately document the signs/symptoms
that are presented to you with your interventions.

“The microorganisms that seem to have it in for us..turn out..to be rather more like bystanders..it is our response to their presence that makes the disease.”
~Lewis Thomas
Germs NEJM 1972;287:553-5

PREVALENCE Sepsis in general is a frequent cause of morbidity
and mortality. Although maternal sepsis is rare in today’s
developed countries, it remains a persistent and substantial problem.
Recent data has shown that, despite lower levels from decades past, maternal morbidity and mortality is on the rise globally due to severe sepsis (mortality ~ 0.60/100,000 live births; severe sepsis morbidity ~ 20.9/100,000 deliveries in the U.S.)
With the current mortality rates in the U. K. (1.13/100,000) sepsis is classified as the leading cause of direct maternal death.

WHY NOW??
“Given the recent increase in maternal deaths and an increase in morbidity in the general population caused by sepsis, an understanding of the risk factors for sepsis in pregnant and postpartum women is needed to better target potential points of clinical intervention” (Acosta, et. Al, 2011, p. 475)

DEFINING SEPSIS
“Severe sepsis is a potentially life-threatening condition that is characterized by systemic inflammatory response syndrome with infection, organ dysfunction, hypoperfusion and hypotension” (Acosta, et al, 2012, p. 474)

DEFINING SEPSISACCP/SCCM
named conditionDefining criteria
SIRS Core body temperature >38°C or <36°C, HR ≥90 bpm,Respirations ≥20/min (or PaCO2 <32 mmHg,) WBC ≥12,000/μl or ≤4000/μl or >10% immature forms
Sepsis At least two SIRS criteria caused by known or suspected infection
Severe sepsis Sepsis with acute organ dysfunction (including hypoperfusion and hypotension) caused by sepsis
Septic shock Sepsis with persistent or refractory hypotension or tissue hypoperfusion despite adequate fluid resuscitation
MODS The presence of organ dysfunction in an acutely ill patient such that homeostasis cannot be maintained without intervention.
Martin, G. S. (2012).

ORGAN DYSFUNCTION/TISSUE PERFUSION VARIABLES
Arterial hypoxemia (PaO2/FiO2 <300) Acute oliguria (<0.5 ml/kg/hr OR
45mmol/l for at least 2 h) Creatinine increase >0.5 mg/dl Coagulation abnormalities (INR > 1.5
OR aPTT >60s)

ORGAN DYSFUNCTION/TISSUE PERFUSION VARIABLES
Illeus (absent bowel sounds) Thrombocytopenia (<100,000) Hyperbilirubinemia (plasma total bili
>4mg/dl or 70 mmol/l) Hyperlactemia (>1 mmol/l) Decreased cap refill or mottling

PHYSIOLOGY OF PREGNANCY
Hyperdynamic circulation/increased cardiac output = tachycardia
Hypercoaguable status Reduced reserve to tolerate hypoxia
due to increased oxygen consumption = tachypnea
Increased WBC’s during labor/post-partum d/t stress response or tissue compromise

PATHOPHYSIOLOGY
Maternal immune system modulation during pregnancy
Physiologic changes of pregnancy that can mimic or mask biomarkers of sepsis
Increased susceptibility to infection via wounds from delivery.
Typically polymicrobial microorganisms from vaginal colonization are seen

PATHOPHYSIOLOGY
Chorioamnionitis, endometritis, and pyelonephritis being the most significant causes of septic shock in pregnancy
Pregnancy related infections, Non-pregnancy related infections, infections incidental to pregnancy and nosocomial infections are the four classes.

PATHOPHYSIOLOGY
Robinson, D. P., & Klein, S. L. (2012).

MATERNAL RISK FACTORS
Low socioeconomic status Prolonged labor Poor nutrition Multiple vag exams in
labor (>5) Overweight/obesity Home birth in unhygienic
conditions
**Van Dillen, et. Al, 2010, p. 252
Anemia Cesarean Primiparity Obstetrical
maneuvers Multiple
pregnancy Prolonged rupture

SEPSIS PREVENTION
HAND WASHING Prophylactic abx as indicated –
continued research being done to see if they should be used more routinely (ROM without labor at or near term, routinely in 2nd or 3rd trimester, etc)
Good hygiene post-delivery

CASE STUDY
M. R. 18 y.o., G2 P0 In frequently during pregnancy In 5/2 with preterm labor (~31 weeks) -
magnesium sulfate, betamethasone given.
VS during OP visit: T: 97.8-98.5 P: 93-123 RR:16-20 BP: 98-137/55-76 (M): 55-76
Urine WNL, reactive FHR, no cervical change (1/50%). Home 5/3

CASE STUDY Presented 5/6 31.6 weeks @ 0645 with
contractions Dilated 3/100/-1 with bulging bag VS’s on admit: 99.1-100-24-114/65 CBC on admit: WBC: 13.8 H&H: 9.7 &
29.6 PLT: 241; no urine obtained. Cesarean section at 0908 for non-
reassuring FHT’s (minimal variability with recurrent late, variable decels) with foul smelling amniotic fluid noted at delivery

CASE STUDY 1gm ancef and 1 liter LR infused prior to
cesarean Post partum VS’s on 5/6: T: 98.1-101.1 P:
116-136, RR 20-26 (consistently 22-24), BP: 90-133/40-78, MAP: 59-92
Received fluid bolus of 500ml NS at 1141, Mefoxin started at 1211 (specific Dr’s routine post-op order) – 1gm IV q 12H
Blood culture x2 & CBC obtained at 1300: WBC 11.6, H&H 9.5 & 28.8, PLT:160, segs: 70, bands: 22

CASE STUDY Internal Medicine consult at 1500 for
continued tachycardia. Additional 500ml NS at 1724. Dx: Probable chorioamnionitis and possible postop endometritis
VS’s 5/7: T: 97.8-99.4, P: 82-114, RR: 20, BP: 90-128/40-78, MAP: 60-95, SpO2: 90-96
VS’s 5/8: T: 97.7-98.8, P: 86-100, RR: 18-22, BP: 106-116/54-70, MAP: 71-84, SpO2: 90-95%
Placental histology: chorioamnionitis; placenta culture: negative; Blood cultures: neg
Pt dismissed 5/8 to get to her baby at tertiary care facility – no further abx given.

MATERNAL SEPSIS TOOL
The need for a sepsis tool for ante/intra/post partum patients is considerable.
Meta-analysis by Bauer, et. (2014) shows: Temp values in healthy pregnant/postpartum women
were not greater than 38 C “PaCO2 was less than 32 mm Hg for all stages of
pregnancy up to 48 hours postpartum reflecting normal maternal physiology” (p. 538)
A respiratory rate of greater than 20 in the 3rd trimester and in labor was within 1 SD of the mean
HR was 2 SD above mean at 107 and authors recommend following the position of Barton and Sibai (2014) who encourage sepsis eval at greater than 110 BPM in pregnant women.

MATERNAL SEPSIS TOOL
**Dignity Health, 2013

MATERNAL SEPSIS TOOL
**Dignity Health, 2013

SEPSIS TREATMENT – CMS CORE MEASURES TO BE COMPLETED WITHIN 3 HOURS OF TIME
OF PRESENTATION ** : Measure lactate level Obtain blood cultures prior to administration
of antibiotics Administer broad spectrum antibiotics Administer 30ml/kg crystalloid for hypotension
or lactate ≥4mmol/L
**“time of presentation” is defined as the time of triage in the Emergency Department or, if presenting from another care venue, from the earliest chart annotation consistent with all elements severe sepsis or septic shock ascertained through chart review.

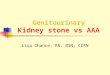
SEPTIC SHOCK: TIMING OF ANTIBIOTICS
Kumar Crit Care Med 2006
0.0
.20
.40
.60
.80
1.00 % Survival
% Total receiving antibiotics
0 - .5
.5 – 1.01 - 2 2 - 3 3-4 4 - 5 5 - 6
6 - 9 9 - 12
12 - 24
24 - 36
> 36
Fraction
Time, hrs
14 ICUs; n = 2,731
Only 50% of patients in Septic Shock
received antibiotics w/in 6 hrs.
.
**Borrowed with permission from Dr. Simpson’ s (KU Med) sepsis presentation 2015

0
50
100
150
200
250
300
SEVERE SEPSISHOW COMMON – HOW DEADLY?SEVERE SEPSISHOW COMMON – HOW DEADLY?
†National Center for Health Statistics, 2001. §American Cancer Society, 2001.
*American Heart Association. 2000. ‡Angus DC et al. Crit Care Med. 2001 (In Press).
AIDS* Colon BreastCancer§
CHF† Severe Sepsis‡
Cases/100,000
Incidence of Severe Sepsis
0
50,000
100,000
150,000
200,000
250,000
De
ath
s/Y
ea
r
Mortality of Severe Sepsis
AIDS* SevereSepsis‡
AMI†Breast Cancer§
**Borrowed with permission from Dr. Simpson’ s(KU Med) sepsis presentation 2015

SEPSIS TREATMENT – CMS CORE MEASURES TO BE COMPLETED WITHIN 6 HOURS OF
TIME OF PRESENTATION: Apply vasopressors (for hypotension that
does not respond to initial fluid resuscitation to maintain a mean arterial pressure (MAP) ≥65mmHg)
In the event of persistent hypotension after initial fluid administration (MAP < 65 mm Hg) or if initial lactate was ≥ 4 mmol/L, re-assess volume status and tissue perfusion and document findings.*
* To meet the requirements, a repeat focused exam† by a licensed independent practitioner (LIP) as detailed below or any 2 other items are required:

SEPSIS TREATMENT – CMS CORE MEASURES
TO BE COMPLETED WITHIN 6 HOURS OF TIME OF PRESENTATION:
Measure CVP Measure ScvO2 Bedside cardiovascular ultrasound Dynamic assessment of fluid responsiveness
with passive leg raise or fluid challenge Focused exam† including vital signs,
cardiopulmonary, capillary refill, pulse and skin findings.
Re-measure lactate

BARRIERS ALONG THE WAY
How will patients be managed? What physician will implement
bundles? Provider apprehension in process
implementation. Confusion/resistance to a new process

SEPSIS WORKSHEET

CASE STUDY
M. R. 18 y.o., G2 P0 In frequently during pregnancy In 5/2 with preterm labor (~31 weeks) -
magnesium sulfate, betamethasone given.
VS during OP visit: T: 97.8-98.5 P: 93-123 RR:16-20 BP: 98-137/55-76 (M): 55-76
Urine WNL, reactive FHR, no cervical change (1/50%). Home 5/3

CASE STUDY Presented 5/6 31.6 weeks @ 0645 with
contractions Dilated 3/100/-1 with bulging bag VS’s on admit: 99.1-100-24-114/65 CBC on admit: WBC: 13.8 H&H: 9.7 &
29.6 PLT: 241; no urine obtained. Cesarean section at 0908 for non-
reassuring FHT’s (minimal variability with recurrent late, variable decels) with foul smelling amniotic fluid noted at delivery

CASE STUDY 1gm ancef and 1 liter LR infused prior to
cesarean Post partum VS’s on 5/6: T: 98.1-101.1 P:
116-136, RR 20-26 (consistently 22-24), BP: 90-133/40-78, MAP: 59-92
Received fluid bolus of 500ml NS at 1141, Mefoxin started at 1211 (specific Dr’s routine post-op order) – 1gm IV q 12H
Blood culture x2 & CBC obtained at 1300: WBC 11.6, H&H 9.5 & 28.8, PLT:160, segs: 70, bands: 22

CASE STUDY Internal Medicine consult at 1500 for
continued tachycardia. Additional 500ml NS at 1724. Dx: Probable chorioamnionitis and possible postop endometritis
VS’s 5/7: T: 97.8-99.4, P: 82-114, RR: 20, BP: 90-128/40-78, MAP: 60-95, SpO2: 90-96
VS’s 5/8: T: 97.7-98.8, P: 86-100, RR: 18-22, BP: 106-116/54-70, MAP: 71-84, SpO2: 90-95%
Placental histology: chorioamnionitis; placenta culture: negative; Blood cultures: neg
Pt dismissed 5/8 to get to her baby at tertiary care facility – no further abx given.

RAPID RESPONSE TEAM COLLABORATION Add sepsis risk factors to your Rapid
Response Team notification protocol RRT members are usually more comfortable
with some of the interventions listed in the CMS Sepsis bundle than the typical OB nurse.
Train your RRT in the specifics of maternal sepsis – maternal nurse needs to work closely with RRT members during RRT notifications

PHYSICIAN NOTIFICATION
Be sure to keep your physician in the know: Call with abnormal vital signs or lab work Suggest appropriate lab/intervention
according to CMS sepsis bundles Document intervention with physician in
the medical record

DOCUMENTATION
Imperative to document accurately and timely. When phone calls were made to physicians When labwork was obtained When antibiotics were administered Vital signs in a frequency that will help
analyze effectiveness of interventions Repeat lab ordered as needed

REFERENCES
Accosta, C. D., Bhattacharya, S., Tuffnell, D. Kurinczuk, J. J., & Knight, M. (2012). Maternal sepsis: A Scottish population-based case-control study. British Journal of Obstetrics and Gynaecology, 119, 474-483.
Acosta, C. D., Knight, M., Lee, H. C., Kurinczuk, J. J., Gould, J. B., & Lyndon, A. (2013). The continuum of maternal sepsis severity: Incidence and risk factors in a population-based cohort study. PLoS ONE 8(7): e67175. doi:10.1371/journal.pone.0067175
Barton, J. R., & Sibai, B. M. (2012). Severe sepsis and septic shock in pregnancy. Obstetrics & Gynecology, 120(3), 689-706.
Bauer, M. E., Bauer, S. T., Rajala, B., MacEacher, M. P., Polley, L. S., Childers, D., & Aronoff, D. M. (2014). Maternal physiolologic parameters in relationship to systemic inflammatory response syndrome criteria. Obstetrics & Gynecology, 124(3), 535-541.
Dillen, J. V., Zwart, J., Schutte, J., & Roosmalen, J. V. (2010). Maternal sepsis: Epidemiology, etiology and outcome. Current Opinion in Infectious Diseases, 23, 249-254. doi:10.1097/QCO.0b013e328339257c

REFERENCES
Martin, G. S. (2012). Sepsis, severe sepsis and septic shock: changes in incidence, pathogens and outcomes. Expert Review of Anti-Infective Therapy, 10(6), 701–706. doi:10.1586/eri.12.50
National Quality Forum (2012). Severe Sepsis and Septic Shock: management Bundle. Accessed June, 2015: http://www.qualityforum.org/WorkArea/linkit.aspx?LinkIdentifier=id&ItemID=71548
Ouzounian, J. G., & Elkayam, U. (2012). Physiologic changes during normal pregnancy and delivery. Cardiology Clinics, 30(3), 317-329. doi:10.1016/j.ccl.2012.05.004
PrabhuDas, M., Bonney, E., Caron, K., Dey, S., Erlebacher, A.,..…..&Yoshinaga, K. (2015) Immune mechanisms at the maternal-fetal interface: Perspectives and Challenges. Nature Immunology, 16(4), 328-334.
Robinson, D. P., & Klein, S. L. (2012). Pregnancy and pregnancy-associated hormones alter immune responses and disease pathogenesis. Hormones and Behavior, 62(3), 263–271. doi:10.1016/j.yhbeh.2012.02.023

REFERENCES
Sepsis Alliance.org “Sepsis and Pregnancy & Childbirth” Accessed 4/26/15 http://www.sepsisalliance.org/sepsis_and/pregnancy_and_childbirth/
Zakour, N. L. B., Venturini, C., Beatson, S. A., & Walker, M. J. (2012) Analysis of a steptococcus pyogenes puerperal sepsis cluster by use of whole genome sequencing. Journal of Clinical Microbiology, 50(7), 2224-2228. doi:10.1128/JCM.00675-12

TEST
1) True or false, most OB patients are young and healthy and it would be nearly impossible for them to become septic. T F
2) Why is sepsis during the ante/intra/post partum period so difficult to recognize?
a) A degree of tachycardia and tachypnea is a physiologic response to the increased volume and decreased lung space d/t pregnancyb) It isn’t difficult as long as you follow SIRS criteriac) Decreased WBC count is normal during this period of pregnancyd) None of the above
3) What is one of the major sepsis prevention measures in the OB arena?a) Wash handsb) Keep vag exams to a minimumc) Labor duration of less than 18-24 hoursd) All of the above

TEST
4) What puts maternal patients at higher risk for sepsis development?a) Multiparityb) Prolonged rupture of membranesc) Using good aseptic techniques during labor and deliveryd) High socioeconomic status
5) What limitations does the current sepsis tool have?a) There are many overlapping variables of normal pregnancy physiology and SIRSb) It can’t be used in pregnancy because it was only tested on malesc) All of our patient have an invasive procedure, and therefore they will always be at risk for sepsisd) None of the above
6) Who should be notified in the event of suspected/known sepsis?a) Rapid Response Teamb) Charge Nursec) Physiciand) All of the above

TEST7) True or false, core measures only apply to confirmed sepsis?
8) Where should your interventions/notifications be documented?a) Each intervention done needs to be documented in the appropriate intervention and any other significant information placed in notes.b) RRT will handle all documentationc) As long as antibiotics are started in a timely manner, you don’t have to document anything.d) None of the above
9) A patient ‘s vital signs on admit and through labor were as follows: T: 97.4-99.5; p: 78-100; RR: 16-20; BP: 124-168/78-92, spo2 95-100%. Her admit CBC showed WBC of 17,000. On post-partum day 2, VS’s are as follows: 99.9, 118, 22, 108/58. Should your risk of suspicion for sepsis be increased in this patient and why or why not?
a) Yes, because her WBC was 17,000 and that alone give suspicion for infectionc) Physicianb) Not necessarily, Because her vs’s are not much out of range and could be considered part of normal pregnancy physiology. She bears watching.c) Yes, because her day 2 vs’s are significantly different from her admit/labor vital signsd) None of the above

TEST10) Once a patient shows signs of sepsis, how soon should antibiotics be started?
a) Within 1 hourb) Within 3 hoursc) Within 6 hoursd) None of the above