Embed Size (px)
Citation preview
Linking ARVs with Nutrition, Food Security and Livelihoods:
RENEWAL in Africa
Stuart GillespieInternational Food Policy Research Institute
International AIDS Conference, Toronto, 15 August 2006

HIV and AIDSHIV and AIDS
Food and nutrition insecurityFood and nutrition insecurity - chronic- chronic
- acute- acute
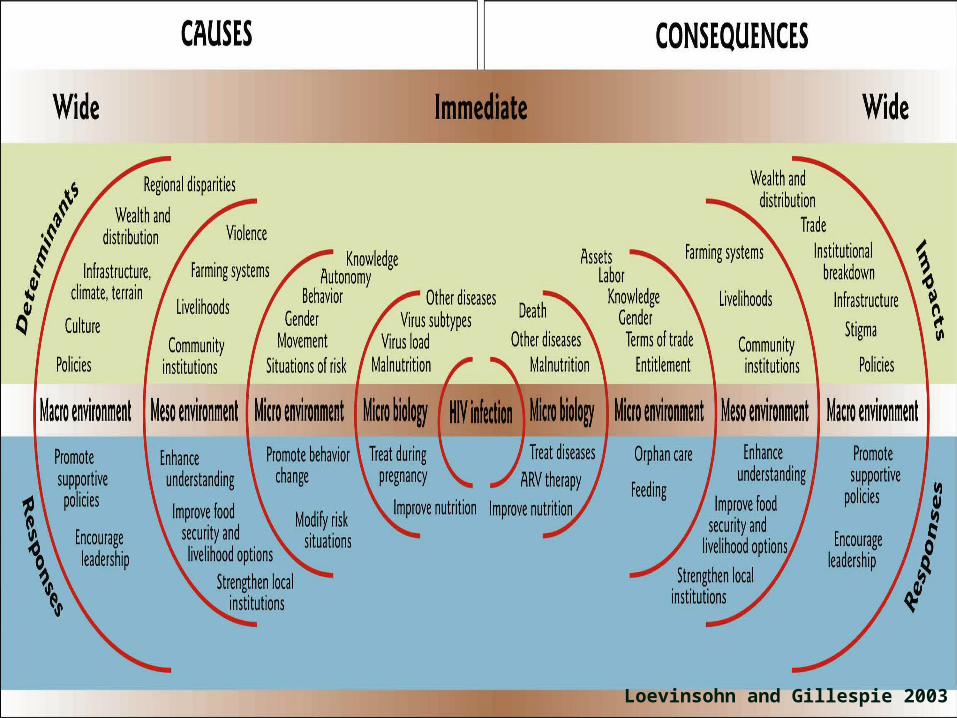
Loevinsohn and Gillespie 2003
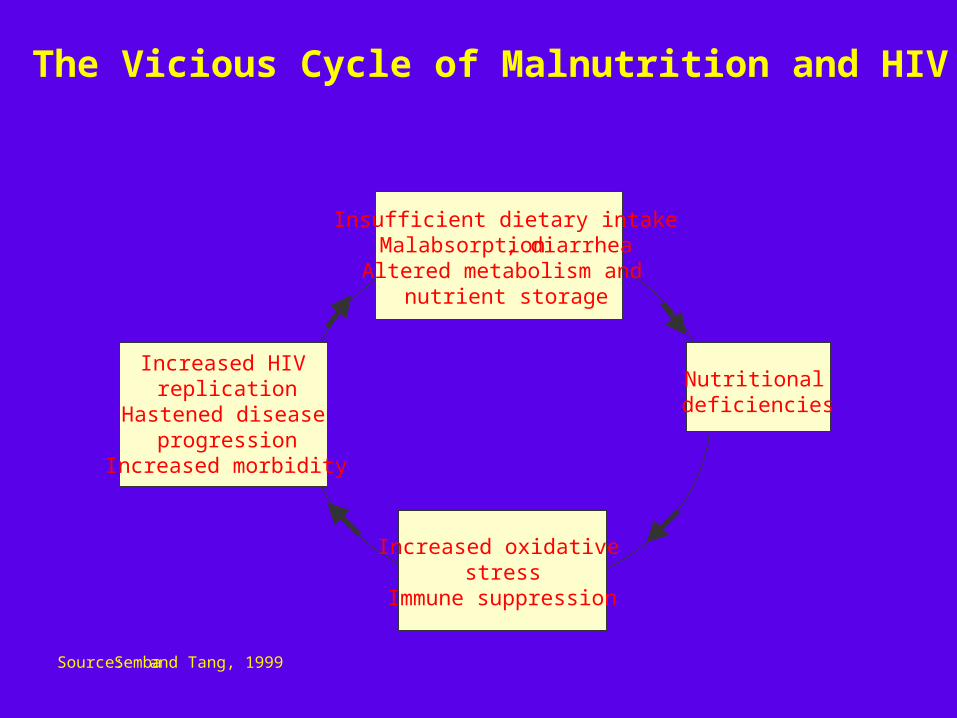
The Vicious Cycle of Malnutrition and HIV
Insufficient dietary intakeMalabsorption , diarrheaAltered metabolism and
nutrient storage
Increased HIV replication
Hastened disease progression
Increased morbidity
Increased oxidative stress
Immune suppression
Nutritional deficiencies
Source:Semba and Tang, 1999

The Regional Network on HIV/AIDS, Rural
Livelihoods, and Food Security (RENEWAL)
Facilitated by IFPRI, RENEWAL brings together national networks of researchers, policymakers, public & private
organizations, and NGOs to focus on the interactions between HIV/AIDS and food and nutrition security.

Core pillars/processes of RENEWAL
Action research
CommunicationsCapacity
Why link nutrition with treatment?
Because malnutrition and disease interactMany PLWHAs are often malnourishedBecause PLWHAs and families often demand food firstNutritional support leads to:• Better drug bioavailability and efficacy of treatment• Better tolerance/ fewer side effects leads to better
adherence, which in turn leads to delays in development of drug resistance
• May prolong period before ARVs are requiredBetter nutritional status at start of treatment increases
survival (by a factor of six)
…but nutrition security is the goal
• Targeted nutrition interventions may provide useful short-term support for people living with HIV, so long as stigma and other barriers are dealt with….
• ….but ultimate aim should be to promote sustainable livelihoods which will ensure household and community-level nutrition security
Community-driven approaches are key
• Communities are responding to HIV and AIDS• They have incentives, local information, transparency,
accountability, latent capacity -- but they lack power and resources.
• AIDS is crosscutting, multisectoral, horizontal....
..…just like people’s lives.• Experience to build on (nutrition, CDD)• Community-government partnerships
Pillars of community–driven development
Local governmentCommunities and NGOS
Sectors
Can formal nutrition interventions complement local support networks?
A case study of AMPATH’s Nutrition Supplementation Program for Individuals on ARV treatment, in western Kenya
Elizabeth Byron, Stuart Gillespie and Mabel Nangami
Methodology
• Data Collection:1. Qualitative Research (Dec. ’05 – Feb. ’06)
• Key Informant Interviews (18)• Focus Group Discussions (9)• In-depth Interviews (80)
2. Modular household survey (March-Sept. ’06)
3. Clinical data from AMPATH Medical Records System
4. Data from HAART & Harvest Initiative on food distribution
Sources of support to PLWHA
• Formal Support – narrow and focused– ARV treatment– HHI/WFP food supplements – short-term– FPI- loans, skills training, employment– Patient support groups
• Informal Support – irregular, reciprocal– Family and relatives – informal transfers– Borrow from neighbours/friends– Religious institutions– Community (Harambee, merry-go-rounds)
Factors determining support
• Stigma and attitude toward PLWHA• Disclosure (awareness of needs vs. discrimination)• Social relationships (family, in-laws)• Competing needs and availability of resources• Seasonality (demand/supply)• Marital status• Gender• Children• Health status, duration of sickness
Interactions between nutrition intervention and informal social support networks
• Positive impact– Improved health status Catalyst for greater support – Balanced diet becomes accessible– Reallocation of household resources to other needs
• No change– No prior support (formal program fills gap)– Support remains constant
• Negative impact – Stigma, initially with food collection, declining – “Weaning” preparation not integrated – Dependency and expectation of support
Lessons1. Stigma remains a barrier to accessing community support2. Formal nutrition intervention acts as temporary relief and often
replaces overstressed informal networks.3. Observable health improvements in PLWHA can serve as a
catalyst for additional sources of support from community/family.4. Seasonal patterns of food availability imply a greater need for
formal support at different times of year.5. Large variation in individual access to support and ability to
successfully transition off food support at 6 months6. AMPATH Patient Support Groups fill unmet psychosocial needs
that family/friends may be unwilling to provide.7. Need for better local and external linkages and partnerships re:
livelihood support













![[Cailein Gillespie] Food and Beverage Management M(BookFi.org)](https://img.dokumen.tips/doc/110x75/55cf99b4550346d0339ec4f1/cailein-gillespie-food-and-beverage-management-mbookfiorg.jpg)















