Embed Size (px)
Citation preview

Limited Radiat ion Therapy for Selected Pat i ents With Patholog ica l Stages IA and IIA Hodgkin's Disease Ellen Jones and Peter Mauch
The first definitive reports that early stage Hodgkin's disease (HD) could be cured by radiotherapy were published by Vera Peters in 1950 and by Easson and Russell in 1963. Since then, advances in understanding the natural history, refining the histopathologic classifi- cation, and development of a staging system have improved the management of HD. Several studies of early stage HD show greater than 80% actuarial 10- to 15-year freedom from relapse, and less than a 10% mortality from HD after treatment with radiation therapy
alone. Radiotherapy has become so successful in the treatment of early stage HD (with combination chemo- therapy reserved for relapse) that the risk of dying from other causes approaches the risk of dying from HD itself at 15 to 20 years following treatment. This article outlines the principles of treatment for favorable progno- sis clinical stages IA and IIA HD, with emphasis on identifying patients with favorable features who may be treated effectively with mantle irradiation only. Copyright �9 1996 by W.B. Saunders Company
S ince the first definitive reports that early stage Hodgkin's disease (HD) could be cured by radio-
therapy, advanCes in understanding the natural his- tory, changes in histopathology and staging, and development of improved radiation therapy and chemotherapy have resulted in cures in more than 80% of patients. 1-9 The treatment rationale for Hodgkin's disease (HD) is based on the natural history of the disease, with its characteristic orderly spread among contiguous lymph nodes. Gilbert l~ is credited with first describing the pattern of spread of HD and these concepts were further developed by Peters 1 and Kaplan et al II who applied prophylactic radiotherapy to adjacent nodal groups. These pat- terns of presentation were confirmed in a recent study involving 719 patients which described the sites of involvement, histological, and clinical features for laparotomy-staged HD patients. I2 These patterns indicated evidence for contiguous spread for patients with nodular sclerosis (NS) and mixed cellularity (MC) histology. For these subtypes, the HD typically began in the chest or neck, and significant associa- tions were found between the mediastinum and cervical nodes, cervical nodes and ipsilateral axilla, mediastinum and hilum, and spleen and abdominal involvement.
Clinical Versus Pathological Staging The selection of favorable patients for consideration of mantle radiation depends on accurate thoracic
From the Joint Center far Radiation Therapy, Department of Radiation Oncology, Harvard Medical School, Boston, MA.
Address reprint requests to Peter Mauch, MD, Joint Center for Radiation Therapy, 330 Brookline Ave, Boston, MA 02215.
Copyright �9 1996by W.B. Saunders Company 1053-4296/96/0603-000555.00/0
staging. The routine use of computed axial tomogra- phy (CAT) and gallium scans (67Ga) have contrib- uted to the primary workup of patients with HD by defining areas of initial involvement, including pulmo- nary parenchymal nodules, chest wall or pericardial invasion, and cardiophrenic adenopathy. 13-16 Large mediastinal adenopathy (LMA), low thoracic involve- ment (hilar, subcarinal, or cardiac nodal involve- ment), or large numbers of sites of involvement are all poor prognostic features; these patients should be treated with combined radiation therapy and chemo- " therapy (see article by Cosset et al elsewhere in this issue).
Before effective multiagent chemotherapy, stag- ing laparotomy was used extensively as occult abdomi- nal disease altered the extent of radiotherapy. Many institutions now apply prognostic factors to deter- mine treatment, and staging laparotomy is used more selectively as a means of adapting treatment when ruling out infradiaphragmatic HD would modify the radiation field. The costs of staging laparotomy include a 5- to 7-day hospitalization and potential morbidity and mortality. At large centers performing routine surgical staging, mortality is well under 1% and morbidity from wound abscess, subphrenic ab- scess, or small bowel obstruction is as low as 3~ 17 Vaccination before splenectomy has decreased the risk of bacterial sepsis. Is There is a small potential increased relative risk of leukemia (approximately twofold) following splenectomy, contrastedvTfth a 60- to 120-fold increased risk following alkylating multi- agent chemotherapy such as mechlorethamine, vin- cristine, procarbazine, and prednisone (MOPP). l~
The European Organization for the Research and Treatment of Cancer (EORTC) H6F randomized trial studied whether clinical staging and subtotal
1 6 2, Seminars in Radiation Oncology, Vol 6, No 3 (Ju~), 1996.'pp 162-171

Favorable CSI-II Hodgkin's Disease 163
lymphoid irradiation (STLI) spleen were comparable to staging laparotomy and treatment adaptation (mantle radiation alone or STLI for pathological stages [PS] I and IIA or combined modality therapy for PS III and IV) for favorable prognosis clinical stages (CS) I and II HD. Favorable patients were without large mediastinal adenopathy and had an erythrocyte sedimentation rate (ESR) less than 50 without B symptoms, or an ESR less than 30 with B symptoms. The H6 "favorable" trial revealed that 30% of the patients randomized to laparotomy had infradiaphragmatic HD. There was no statistical difference in 6-year overall smvival or freedom from progression (FFP) between the two arms suggesting that the use of staging laparotomy may result in a reduction in the amount of treatment delivered, but not an improvement in disease-free or overall sur- vival.
The typical rate of pathological upstaging for most patients with clinical stages IA and IIA HD is 20% to 30%. Thus, the treatment philosophy be- comes a choice between more staging and less treatment (ie, laparotomy and mantle radiation for PS IA and IIA patients) versus less staging and more treatment (ie, clinical staging and larger radiation fields or chemotherapy). Because HD occurs in a younger population with a high likelihood of survival, these treatment choices may have far-reaching impli- cations including pulmonary and cardiac toxicity, fertility, and risk of second tumors. The application of prognostic factors may help to determine a subset of favorable patients who may benefit from lapa- rotomy and reduction of treatment in an eflbrt to minimize potential long-term treatment sequellae. Likewise, a subset of unfavorable patients may be identified who require more aggressive upfront therapy that would not be modified on the basis of laparotomy findings.
Prognostic Factors for Clinically Staged and Pathologically Staged Patients
Clinically Staged Patients Favorable and unfavorable features have been identi- fied in CS I and II HD as prognostic factors for disease-free and overall survival. Several large series involving CS I and II patients treated with radiation, combined modality treatment, or chemotherapy alone have identified adverse factors including male sex, older age (>40 to 50 years old), elevated ESR, B symptoms, MC/lymphocyte depleted (LD) histology,
number of involved sites is three or four or more, and large mediastinal adenopathy (LMA)? 2-24 Many of these features likewise predict for an increased risk of occult abdominal involvement, In a series of 552 pathologically staged patients seen at Harvard Medi- cal School from 1969 to 1986,17 significant factors for surgical upstaging of CS I and II patients included sex (females, 18% v males, 29%), symptomatic stage (no B symptoms, 21% v B symptoms, 34%), number of sites (1 site, 17% v >2 sites, 27%). In this study, age of 40 years or older and histology were not significant independent parameters for upstaging of the CS I and II patients. Among the most favorable groups were CS IA females with mediastinum only (0 of 15 upstaged) and CS IA females with left neck only (1 of 24 upstaged). Overall CS IA females and CS IA patients with lymphocyte-predominant histology had a 6% or less risk of occult abdominal involvement. In almost all instances, upstaging resulted in change of treatment. For minimal abdominal involvement, pa- tients received total nodal irradiation instead of mantle and paraaortic/splenic pedicle, and for more extensive disease, patients received chemotherapy or combined modality therapy.
Pathologically Staged Patients Several series have identified prognostic factors in PS I and II patients with increased risk of relapse or worse survival. Two studies examined PS IA and IIA patients treated with STLI total nodal irradiation (TLI) alone, and found LMA as the major factor predicting for relapse. 5,3 Despite the increased rate of relapse, overall survival was not significantly affected for patients with LMA in either study. The Harvard Medical School study found that age 40 years or older and MC/LD histology were significant predictors for decreased survival. Another study examined PS IA and IIB patients treated with radiation or combined modality therapy, 25 and found high tumor burden, treatment with radiation alone, and male sex as prognostic factors for freedom from relapse. Only tumor burden and age of 40 years or older were significant for overall survival. Several retrospective series have also found LMA as an adverse prognostic factor for relapse in surgically staged patients. 26-32 Most relapses occur in supradiaphragmatic nodes or extranodal sites including pleura, chest wall, or pulmonary parenchyma. 26-31 A large retrospective study combining PS IB and IIB patients from Har- vard andStanford suggested that patients with night sweats as their only constitutional symptom had a more favorable prognosis similar to PS IA and, IIA

164 Jones and Mauch
patients, whereas LMA, age of 40 years or older, fevers, and weight loss all independently predicted for increased risk of relapse. 33 In summary, fewer prognostic factors (LMA, fevers, and weight loss) are consistently identified in a pathologically staged co- hort, as prognostic factors in clinically staged pa- tients may also predict for surgical upsl!aging.
Classification Systems for Favorable Patients
The EORTC initiated a series of clinical trials in 1964 aimed at individualized t reatment of HD. 34 As treat- ment strategies evolved, a classification system devel- oped to adapt t reatment based on prognostic factors. The recent H7 trial 35 and ongoing H8 trial have defined a three-tiered classification as shown in Table 1. Similarly, the group at Princess Margaret Hospital has defined a classification system based on similar observations from their retrospective experi- ence over more than 20 years. These systems share many features and differ slightly in the definitions of bulky mediastinal adenopathy and ranges of labora- tory values. In both series, the majority of patients are in the favorable prognostic subset. Because only
patients treated with radiation alone are included in the Princess Margaret Hospital series, this naturally selects for more favorable features, accounting for the very low proportion of patients in the unfavorable group. The EORTC experience includes all patients with CS I and II supradiaphragmatic HD, and the proportions of patients in each category may be more representative of the general distribution of patients presenting with early stage HD.
Standard Treatment for Early Stage Hodgkin's Disease: Results of Early Randomized Trials Evaluating Radiation Field Size
Early prospective randomized trials evaluated the effect of radiation field size for both CS and P S I and II patients. At Stanford, PS IA and IIA patients were randomized to STLI or TLI versus involved field radiation. 36 There was a significant difference in freedom from relapse (FFR), with STLI/TLI pa- tients having 83% FFR and involved field patients having 32% FFR at 15 years follow-up. Significant
Table 1. Modern Classification Systems for Clinically Staged Patients
Institution Prognostic Features Percentage of Total Patients
EORTC (n = 1,641 from H1, H2, H5, and H6 trials 34)
Princess Margaret Hospital (n = 250; retrospective experience > 20 years of patients treated with radiation alone23, 44)
Very favorable CS I female Age < 40 years No B symptoms ESR < 50 mm LP or NS histology No bulky mediastinal involvement
Unfavorable 40% Age > 50 years No B symptoms with ESR > 50, or B
symptoms with ESR > 30 Four or more involved sites Bulky mediastinal involvement, i.e.,
(M/T ratio > 0.35) Favorable 54%
All patients not in the previous two groups
Favorable (group 2) No B symptoms Age _< 50 years ESR _< 40 NS/LP histology No large mediastinal adenopathy
(> 10cm) Very favorable (group 1) 10%
Favorable features and isolated upper cervical stage IA disease
Unfavorable (group 3) 6% All patients not in the previous two
groups
6% of CS I and II supradiaphagmatic HD
84% of CS I and II supradiaphagmatic HD treated with radiation alone

Favorable CSI-II Hodgkin's Disease 165
differences were also noted for PS and CS I and II patients randomized in the Collaborative Clinical Trial favoring STLI over involved field radiation. 37 Surgically staged patients had a 66% FFR with STLI versus a 52% FFR with involved field radiation therapy, and clinically staged patients had a 59% FFR with STLI versus a 32% FFR with involved field radiation therapy. Despite differences in FFR, nei- ther of these trials evaluating radiation field size demonstrated a difference in overall survival. The British National Lymphoma Investigation also exam- ined regional versus involved field radiation in clini- cally and pathologically staged patients. 38,39 No signifi- cant differences in FFR were found between the two radiation field sizes. Patients in this study were not randomized by extent of staging, and the definitions of regional field irradiation differed significantly from STLI because the British National Lymphoma Investigation's wide field usually encompassed less than a mantle field.
Since the early 1970s, the standard treatment for PS IA and IIA HD has been STLI. As experience with STLI matures and follow-up lengthens, concerns regarding long-term treatment sequelae gain increas- ing importance. 6,4~ Therefore, the selective reduc- tion of the extent of initial therapy while maintaining a high rate of freedom from relapse may further refine the management of early stage HD.
Mant le Irradiation Alone as Treatment for Early Stage Hodgkin's Disease
Clinically Staged Patients The EORTC H1 trial studied mantle irradiation alone in CS I and II patients. Following RT, patients were randomized to either weekly vinblastine for 2 years following radiation or no additional treatment. Although the 15-year disease-free survival was greater for the mantle plus vinblastine group (60%) com- pared with the mantle only group (38%), this did not translate into a significant overall survival advantage, suggesting that salvage was more effective in pa- tients treated with radiation only. 34 In this clinically staged series which predates modern CAT and gal- lium scanning, there was a high incidence of subdia- phragmatic re!apse in patients with MC histology (40%) treated Jwith mantle irradiation alone com- pared with the lymphocyte predominant (LP) and NS subtypes (11%). 43 Based on this unacceptably high incidence of subdiaphragmatic failure, particu- larly in the MC histology cohort, the subsequent H2
trial randomized 300 patients with supradiaphrag- matic HD to staging laparotomy and splenectomy followed by mantle and paraaortic radiation, or no laparotomy and mantle, paraaortic, and splenic radia- tion (STLI-spleen). Following radiation, patients with MC or LD histology also were randomized to vinblas- tine or vinblastine plus procarbazine for 2 years. At 12 years follow-up, the disease-free survival was 68% }'or STLI-spleen and 76% for laparotomy and STLI (P = not significant). Results of these two trials suggest that mantle irradiation alone is not sufficient treatment for unselected patients with CS I and II HD.
A retrospective series from Princess Margaret Hospital reviewed their experience with CS I and II patients receiving radical radiation between 1968 and 1977. 44 The extent of radiation fields varied considerably during the 10 years covered and ranged from involved field (radiation only to areas of known nodal involvement), extended field radiation (mantle field or inverted Y for infradiaphragmatic disease), or adjuvant paraaortic radiation-classified as receiv- ing "greater than a mantle field." For mantle field irradiation, the 10-year relapse-free rates for CS IA and CS IIA were 81% (n = 37) and 54% (n = 84), respectively. Although the patterns of relapse are not described for each subgroup, these relatively high rates of relapse are not unusual given the incidence of occult infradiaphragmatic disease in clinically staged patients with varied clinical features. These data suggest that selected patients with CS IA HD may be suitable for mantle irradiation alone. The EORTC H7 trial is currently studying the use of mantle only in a very favorable subgroup of CS IA female patients with NS or LP histology and ESR less than 50 who are expected to have a risk of abdominal involvement approximately 6% or lower.
Pathologically Staged Patients The EORTC H5F trial studied the management of patients with favorable CS I and II disease on the basis of clinical features including NS or LP histology, age 40 years or younger, and ESR _< 70 mm/h. 22 Patients underwent staging laparotomy and, if the results were negative, were randomized fo mantle irradiation alone versus STLI. A total of 198 patients were randomized. At 9 years median follow-up there was no significant difference in disease-free survival (69% v 70%) or overall survival (94% v 91%) for the mantle and STLI groups, respectively. The patterns of relapse differed, with 4% of STLI patients relaps- ing below the diaphragm compared with 11% for the

166 Jones and Mauch
mantle patients. This increased risk of subdiaphrag- matic recurrence did not impact on disease-free or overall survival, but did highlight the need for consis- tent follow-up and surveillance in the mantle irradia- tion alone cohort.
A retrospective series of stage I HD patients from St. Bartholomew's hospital included 62 patients with PS IA treated with mantle only. 45 The histology included 41% of patients with nodular sclerosing, 33% of patients with lymphocyte predominant, and 26% of patients with mixed cellularity. The majority of patients presented with disease in the neck (85%); there were four axillary and two thymic presenta- tions. Complete response was achieved in all pa- tients, and the actuarial FFR was 82% at 15 years. Eight patients have relapsed; six of the eight recur- rences were below the diaphragm.
Harvard Jo int Center for Radiat ion Therapy Trial
The results of an ongoing single-arm prospective trial involving PS IA and II A patients are updated. 46 Interest in this approach was fostered by early results of the EORTC H-5 trial, as well as other retrospec- tive series.22,44,45 For patients meeting eligibility crite- ria following negative laparotomy, radiotherapy is given to a mantle field over 4 to 5 weeks. Involvement above the diaphragm is documented with chest CAT and gallium scanning. Entry criteria include patients with CS IA or IIA disease with a negative staging laparotomy (PS IA and IIA). Further criteria include patients with upper mediastinal involvement; how- ever, hilar or subcarinal adenopathy or LMA are exclusion criteria. In contrast to the EORTC H-5 trial, Patients over age 40 years were eligible. Pa- tients are not excluded on the basis of a high ESR or large number of sites of disease; however, none of the patients entered have had four or more sites of involvement. The original trial was limited to pa- tients with NS or LP histology. Patients with PS IA MC histology have recently been eligible for enroll- ment; in addition, staging laparotomy is no longer required for patients with CS IA LP HD. To date, 55 patients have been enrolled on the prospective study.
An additional retrospective series was derived from thd Harvard Joint Center for Radiation Therapy database as 'a means of evaluating longer t e rm experience with mantle radiotherapy. This group consisted of 26 patients 'who were comparably staged and treated as with the'prospective series. Seventeen of the 26' met the inclusion criteria fro: the original prospective study, and the remaining 9 patients with
MC histology met the eligibility requirements of the updated prospective trial.
Patient characteristics are listed in Table 2. The 55 patients in the prospective group have a median follow-up of 25 months (range, 1 to 79); the retrospec- tive group has a median follow-up of 126 months (range, 31 to 319). There is no significant difference in median age between the two groups, but there were significant, differences in histology and stage distribution. The majority of prospective patients had NS histology, and approximately 60% had PS IA. For the retrospective group, there were fewer NS patients and nearly all were PS IA.
Meticulous delineation of initial nodal involve- ment and careful radiotherapeutic techniques are essential for management of l iD with mantle irradia- tion alone. The patient is treated in a chin-extended, hands on head position to spare the oral cavity mucosa and draw the lower axillary nodes clear of the chest wall. Customized lung blocks are drawn using thoracic CT scans as a guide in delineating the clinical target volume, while shielding a maximum amount of normal lung tissue. Weekly portal films are taken to verify proper field alignment. Dose heterogeneity is minimized by treating at extended distance (source to skin distance > 110 cm), and using a 6-MV linear accelerator. The mantle field" receives 3,600 cGy, with a boost given to gross disease to a total dose of 4,000 to 4,200 cGy. Because of increased dose in the neck region, a posterior spinal block extending down to the level of C7 is added at 3,000 cGy. An anterior larynx block may be added at 2,000 cGy provided that the immediate adjacent cervical nodes are uninvolved. The recommended lower field border for the mantle is at the T8 or T9 vertebral body to cover the hilar and subcarinal nodes. I f there is upper mediastinal disease, then the border is extended to T10 or T11 to include the low
T a b l e 2. Patient CharacteristicsofMantle Irradiation Alone
Prospective Retrospective
No. patients 55 26 Median age (years) 27 (11-54) 24 (3-59) Median follow up (months) 25 (1-79) . 126-(31-319) Histology
LP 12 13 NS 43 4 MC 9
Stage IA 33 22 IIA 22 4

Favorable CSI-II Hodgkin's Disease 167
central cardiac nodes. A subcarinal block is added at 3,000 cGy if the lower field border is used.
The actuarial survival (all causes) and freedom from first relapse for the combined prospective and retrospective groups are shown in Figure 1. The 10-year actuarial rates of freedom from relapse and overall survival were 76% and 91%, respectively. No significant differences in survival by stage, histology, age, and mediastinal involvement were noted; how- ever, the follow-up is relatively short in the prospec- tive group.
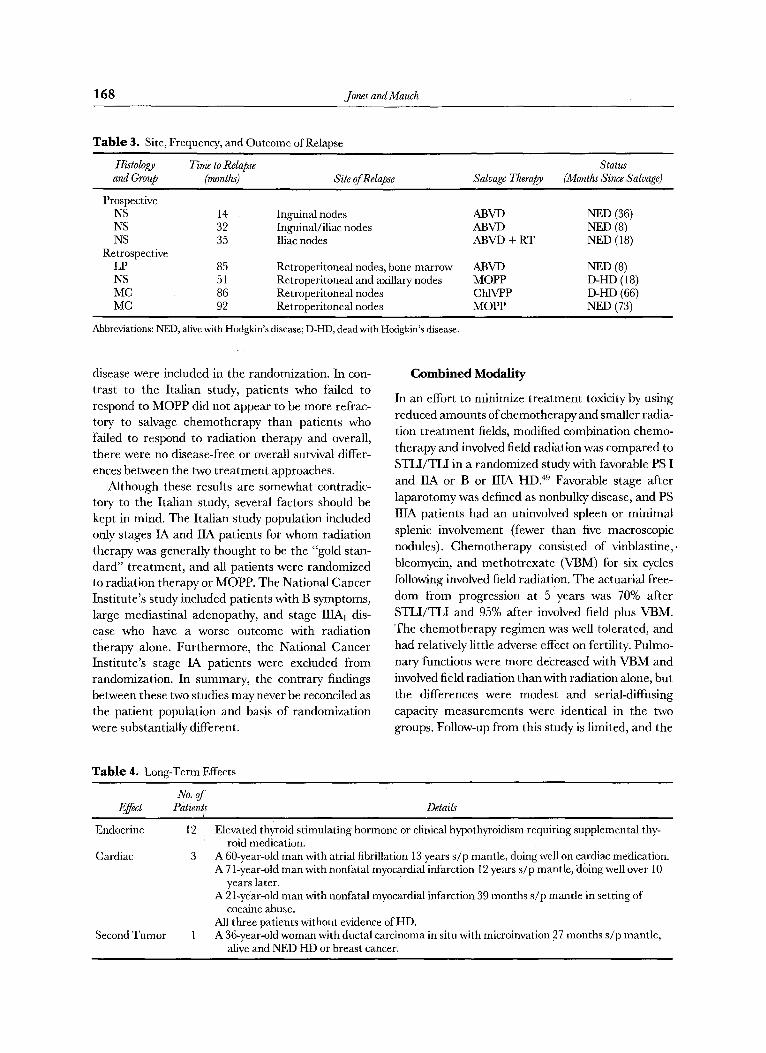
Overall, there have been seven relapses and three deaths among 81 patients. The site of relapse, histol- ogy, and outcome of salvage therapy are detailed in Table 3. Three patients with NS histology in the prospective group have relapsed at 14, 32, and 35 months in the inguinal, inguinal and iliac, and iliac nodes, respectively. All were treated with doxorubi- cin, Neomycin, vinblastine, and dacarbazine (ABVD) chemotherapy, and the patient relapsing at 35 months in the iliac nodes also received pelvic radiotherapy. All relapsed patients from the prospective group achieved a complete response to salvage therapy and are currently alive and without evidence of liD.
In the retrospective group, there have been four relapses. The patient with LP histology relapsed at 85 months in retroperitoneal nodes and bone marrow, and is without evidence of disease following salvage with ABVD chemotherapy. In the patient with NS histology, H D recurred at 51 months in the axillary and retroperitoneal nodes. This patient died of HD 18 months following MOPP salvage chemotherapy. Two patients with MC histology relapsed in retroperi-
10C
8C
.-4
60
::b c,,} 46
20
E• 91%(14) [ Survival -
76% (12) - Relapse-free []
1~0 1~5 10 25 YEARS
Figure 1. Disease-free and overall smvival of 81 patients with favorable prognosis stages I and II HD treated with mantle irradiation alone at the Harvard Joint Center for Radiation Therapy (see text for patient characteristics and treatment details).
toneal nodes, one died of HD 66 months following salvage with chlorambucel, vinblastine, procar- bozine, prednisone (ChlVPP), and the other is with- out evidence of disease 73 months following salvage with MOPP. Another patient from the retrospective series who was without evidence of HD died of subacute bacterial endocarditis 76 month s following mantle radiotherapy. Long-term effects of treatment have been infrequent, as outlined in Table 4. Again, it may be too early to appreciate the full extent of late effects in the prospective group.
A l t e r n a t i v e T r e a t m e n t s
Chemotherapy Only
Several divergent approaches to the treatment of early stage HD have been explored. Combination chemotherapy has been compared with radiotherapy in two randomized prospective trials. An Italian study examined 89 consecutive patients with PS IA and IIA HD who were randomized to STLI or six cycles of MOPP chemotherapy. 47 With 8 years of follow-up there were similar relapse rates in the two treatment arms. The patterns of failure correlated significantly with treatment modality. True relapses (occurring in areas of previous nodal involvement) were significantly higher in the MOPP versus the RT group (8 recurrences v one recurrence, respectively), whereas lymph node extension or dissemination of disease were observed in two patients after RT and in four patients after MOPP, Response to salvage treat- ment was significantly worse for the MOPP group. The actuarial survival of relapsing patients signifi- cantly differed based on initial treatment. At 80 months after HD, the survival rates were 85% and 15% for the radiation and MOPP groups, respec- tively. In summary, this study showed a significantly greater survival for PS IA and IIA patients treated with STLI versus MOPP chemotherapy.
A randomized prospective trial conducted at the National Cancer Institute compared MOPP versus radiation therapy in a group of 136 patients with stage IB, RA, IIB, and ILIA1 HD. 48 Patients with peripheral IA disease were excluded from randomiza- tion and all were treated with radiation therapy and remain in complete response at 7.5 years median follow-up. Patients with other stages were random- ized to radiation therapy or MOPP. The design of this trial differs from the Italian study in that a substantial number of patients with poor prognosis P S I and II disease and some patients with PS IIIA
16 8 Jones and Mauch
T a b l e 3. Site, Frequency, and Outcome of Relapse
Histology Time to Relapse Status and Group (months) Site of Relapse Salvage Therapy (Months Since Salvage)
Prospective NS 14 NS 32 NS 35
Retrospective LP 85 NS 51 MC 86 MC 92
Inguinal nodes ABVD NED (36) Inguinal/iliac nodes ABVD NED (8) Iliac nodes ABVD + RT NED (18)
Retroperitoneal nodes, bone marrow ABVD Retroperitoneal and axillary nodes MOPP Retroperitoneal nodes ChlVPP Retroperitoneal nodes MOPP
NED (8) D-HD (18) D-HD (66) NED (73)
Abbreviations: NED, alive with Hodgkin's disease; D-HD, dead with Hodgkin's disease.
disease were included in the randomization. In con- trast to the Italian study, patients who failed to respond to MOPP did not appear to be more refrac- tory to salvage chemotherapy than patients who failed to respond to radiation therapy and overall, there were no disease-free or overall survival differ- ences between the two treatment approaches.
Although these results are somewhat contradic- tory to the Italian study, several factors should be kept in mind. The Italian study population included only stages IA and IIA patients for whom radiation therapy was generally thought to be the "gold stan- dard" treatment, and all patients were randomized to radiation therapy or MOPP. The National Cancer Institute's study included patients with B symptoms, large mediastinal adenopathy, and stage IIIA1 dis- ease who have a worse outcome with radiation therapy alone. Furthermore, the National Cancer Institute's stage IA patients were excluded from randomization. In summary, the contrary findings between these two studies may never be reconciled as the patient population and basis of randomization were substantially different.
Combined Modality
In an effort to minimize treatment toxicxty by using reduced amounts of chemotherapy and smaller radia- tion t reatment fields, modified combination chemo- therapy and involved field radiation was compared to STLI/TLI in a randomized study with favorable P S I and IIA or B or IIIA HD. 49 Favorable stage after laparotomy was defined as nonbulky disease, and PS IIIA patients had an uninvolved spleen or minimal splenic involvement (fewer than five macroscopic nodules). Chemotherapy consisted of vinblastine,. bleomycin, and methotrexate (VBM) for six cycles following involved field radiation. The actuarial free- dom from progression at 5 years was 70% after STLI/TLI and 95% after involved field plus VBM. The chemotherapy regimen was well tolerated, and had relatively little adverse effect on fertility. Pulmo- nary functions were more decreased with VBM and involved field radiation than with radiation alone, but the differences were modest and serial-diffusing capacity measurements were identical in the two groups. Follow-up from this study is limited, and the
Tab le 1. Long-Term Effects
Effect
Endocrine
Cardiac
Second Tumor
No. of Patients
1 2
Details
Elevated thyroid stimulating hormone or clinical hypothyroidism requiring supplemental thy- roid medication.
3 A 60-year-old man with atrial fibrillation 13 years s/p mantle, doing well on cardiac me'dication. A 71-year-old man with nonfatal myocardial infarction 12 years s/p mantle, doing well over 10
years later. A 21-year-old man with nonfatal myocardial infarction 39 months s/p mantle in setting of
cocaine abuse. All three patients without evidence of liD.
1 A 36-year-old woman with ductal carcinoma in situ with microinvation 27 months s/p mantle, alive and NED HD or breast cancer.

Favorable CSI-II Hodgkin's Disease 169
potential for secondary tumors, long-term follow-up of late effects, and response rates to salvage need to be addressed.
A pilot study from the British National Lym- phoma Investigation studied the efficacy and toxicity of VBM with involved field radiation in CS IA and IIA patients. 5~ Thirty eight patients were enrolled in this prospective single-arm trial and were given two cycles of VBM followed by radiation and four addi- tional cycles of VBM. With 30 months median follow-up, 2 of 30 patients had relapsed. Pulmonary symptoms were unexpectedly severe, with 14 pa- tients developing a dry cough, dyspnea, or both. Accrual to the study was stopped early because of the unacceptable high toxicity.
Another study in early and intermediate stage HD compared four cycles of MOPP and radiation with four cycles of thiotepa, bleomycin, and vinblas- tine (TBV) and radiation. 51 For CS IA and :IIA patients, similar results were found for both treat- ment arms, with a disease-free survival of approxi- mately 90% at 5 years. This study demonstrated that reduced cycles of MOPP combined with radiation therapy could achieve comparable results to an alternative chemotherapy regimen combined with radiation therapy. The incidence of azospermia and amenorrhea was no different from previous studies with six cycles of MOPP, and sterility remained a problem. There also remained a potential risk for secondary acute leukemia; 1 patient developed leuke- mia out of 61 patients treated with four cycles of MOPP.
Table 5 lists several ongoing trials and one re- cently closed trial (EORTC H7) studying further aspects of combined modality therapy for early stage HD. The EORTC H7 trial tested chemotherapywith epirubicin, bleomycin, vinblastine, prednisone (EBVP) and involved field radiation versus STLI-spleen in favorable CS I and II patients. 35 The 3-year failure-
free survival rates were 81% and 79% for the STLI- spleen and 6 x EBVP + involved field radiation therapy groups, respectively. Of note, the standard of comparison arm for all these series studying CS patients includes STLI and splenic radiation. Inclu- sion of the spleen in clinically staged patients causes a significant increase in the volume of upper abdo- men within the radiation portal, and splenic irradia- tion is associated with the same increased risk of sepsis and leukemia reported for patients after sple- nectomy.
Conc lus ions
In summary, the rationale for treating selected patients with PS IA and IIA HD with mantle radia- tion alone is supported by retrospective series 44,45 and by a randomized prospective trial for patients with NS or LP histology with favorable prognostic fea- tures. 99 Retrospective and prospective data from the Joint Center for Radiation Therapy also support this approach, although longer follow-up is needed for the prospective series. This article has addressed several important questions regarding mantle radia- tion including the following:
1. Which patients are appropriate for treatment? Patients with favorable or very favorable features as described in the EORTC and Princess Marga- ret experiences (see Table 1) may be considered for mantle radiation. Also, PS IA patients with MC histology may be eligible for mantle treat- ment based on the favorable outcome of this subgroup with long-term follow-up. 45 The EORTC H5F trial did exclude patients who were 40 years old or older or those with ESR _> 70. However, based on analysis of prognostic factors for patho- logically staged patients, t he JCRT protocol does
Table 5. Ongoing Trials With Radiation Versus Combined Modality Therapy
No. of Patients Radiation Combined Institution Enrolled as of 9~ 95 Arm Modality Arm
SWOG/CALGB 19 CS IA-IIA STLI-spleen EORTC HSF 205 CS I-1I STLI-spleen EORTC H7F 332 CS MI STLI-spleen GHSG HD-7 CS/PS MI STLI-spleen ROME 72 CS IIA STLI-spleen Stanford G 1 78 CS IA-IIA STLI-spleen
STLI-Spleen + AV • 4 cycles IF RT + MOPP/ABV x 3 cycles IF RT + EBVP • 6 cycles STLI-Spleen + ABVD x 2 cycles STLI-Spleen + ABVD x 1 cycles Mantle + VBM X 6
NOTE. Enrollment estimates as of the September 1995 German Hodgkin's Study Group (GHSG) meeting. AV: adriamycin, vincristine; IF RT: involved field radiotherapy; ABV: adriamycin, vinblastine, bleomycin; EBVP: etoposide, bleomycin, vincristine, prednisone; ABVD: adriamycin, bleomycin, vinblastine, dacarbazine; VBM: vinblastine, bleomycin, methotrexate.

170 Jones and Mauch
not exclude patients solely on the basis of age or ESR.
2. Is there a subset of patients who do not need laparotomy? Patients meeting the EORTC criteria for very favorable features may not requil"e laparotomy. The Joint Center for Radiation Therapy trial does not mandate laparotomy for PS IA patients with LP histology. Long term follow-up of the H7-VF trial will help determine the role for staging laparotomy for female patients with CS IA dis- e a s e .
3. W h a t are the advan tages and l imita t ions o f this
approach?
Using man t l e radia t ion, pat ients wi th favorable
PS IA and IIA H D m a y benefi t f rom the selective
reduc t ion of the ex ten t o f initial therapy wi thout
compromis ing re lapse-f ree survival. The risk o f
some long- t e rm t r e a t m e n t sequel lae m a y be re-
duced by excluding the upper a b d o m e n and thus
i r rad ia t ing smal le r volumes. C h e m o t h e r a p y re-
served for salvage m a y have g rea t e r efficacy in
pat ients who init ial ly received radia t ion only. This
t r e a t m e n t s t ra tegy m a y be l imi ted by pa t ien t
compliance and requires dil igent follow-up. Surveil-
lance o f the a b d o m e n and pelvis has increased
impor tance , and abdomina l /pe lv ic C A T scans
a n d / o r ga l l ium scans a re r e c o m m e n d e d at 6- to
12-month intervals for the first 5 years.
Wi th careful pa t ien t se lect ion and met icu lous radia-
tion techniques, m a n t l e rad ia t ion is becoming the
s tandard o f care for se lec ted PS IA and IIA patients .
Min imiza t ion of init ial t r e a t m e n t while ma in ta in ing
a high disease-free and overall survival is especially
impor t an t in this young pa t i en t populat ion, as poten-
tial long- te rm t r e a t m e n t sequel lae m a y have signifi-
cant consequences.
R e f e r e n c e s
l. Peters M: A study in survivals in Hodgkin's disease treated radiologically. AmJ Roefitgeno163:299-311, 1950
2. Easson E, Russell M: The cure of Hodgkin's disease. BMJ 1:1704-1707, 1963
3. Mauch P, Tarbell N, Weinstein H, et al: Stage IA and HA supradiaphragmatic Hodgkin's Disease: Prognostic factors in surgically staged patients treated with mantle and paraaortic irradiation.J Clin Oncol 6:1576-1583, 1988
4. Farah J, Ultmann J, Griem M, et al: Extended mantle radiation therapy for pathologic stage I and II Hodgkin's disease.J Clin Oncol 6:1047-1052, 1988
5. Hoppe R, Coleman C, Cox R, et al: The management of stage I-II Hodgkin's disease with irradiation alone or combined
modality therapy: The Stanford experience. Blood 59:455465, 1982
6. Cosset J, Henry-Amar M, Meerwaldt J: Long-term toxicity of early stages of Hodgkin's disease therapy: The EORTC experience. Ann Oncol 2:77-82, 1991
7. Hancock S, Hoppe R, Homing S, et al: Intercurrent death after Hodgkin disease therapy in radiotherapy and adjuvant MOPP trials. Ann Intern Med 109:183-189, 1988
8. Henry-Amar M, Hayat M, MeerwaldtJ, et al: Causes of death after therapy for early stage Hodgkin's disease entered on EORTC protocols. IntJ Radiat Oncol Biol Phys 19:1155-1157, 1990
9. Mauch P, Kalish L, Marcus K, et al: Long-term survival in Hodgkin's disease: Relative impact of mortality; infection, second tumors, and cardiovascular disease. The Cancer Jour- nal Scientific American 1:33-42, 1995
10. Gilbert R: La roentgentherapie de la granulomatose maligne. J Radiol Electrol 9:509-514, I925~
1 I. Glatstein E, Guernsey J, Rosenberg S, et at: The value of laparotomy and splenectomy in the staging of Hodgkin's disease. Cancer 24:709-718, 1969
12. Mauch P, KalishL, Kadin M, et al:Patternsofpresentationof Hodgkin's disease. Cancer 71:2062-2071, 1993
13. Hopper K, Diehl L, Lesar M, et al: Hodgkin's disease: clinical utility of CT in initial staging and treatment. Radiology 169:17, 1988
14. Howman-Giles: Role of Ga67 in pediatric solid tumors. Aust PaediatrJ 18:120-125, 1982
i5. Rostock R, Giangreco A, Wharam M, et al: CT scan modifica- tion in the treatment of mediastinal Hodgkin's disease. Cancer 49:2267-2275, 1982
16. Jochelson M, Herman T, Stomper P, et ah Planning mantle radiation therapy in patients with Hodgkin's disease: Role of Galliun-67 scintigraphy. AJR AmJ Roentgenol 151:1229-1231, 1988
17. Mauch P, Larson D, Osteen R, et al: Prognostic factors for positive surgical staging in patients with Hodgkin's disease.J Clin Oncol 8:257-265, 1990
18. Siber G, Gorham C, Martin P, et al: Antibody response to pretreatment immunization and post-treatment boosting with Bacterial Polysaccharide Vaccines in patients with Hodgkin's disease. Ann Intern Med 104:467-475, 1986
19. Andrieu J-M, Ifrah N, Payen C, et al: Increased risk of secondary acute nonlymphocytic leukemia after extended- field radiation combined with MOPP chemotherapy for Hodgkin's disease.J Clin Oncol 8:1148-1154, 1990
20. van Leeuwen F, Somers R, Taal B, et al: Increased risk of lung cancer, non-Hodgkin's lymphoma and leukemia following Hodgkin's disease.J Clin Oncol 7:1046-1058, 1989
21. KaldorJ, DayN, Clarke A, et al: Leukemia following Hodgkin's disease. N EnglJ Med 322:7-13, 1990
22. Tubiana M, Henry-Amar M, Carde P, et al: Toward compre- hensive management tailored to prognostic factors of patients with clinical stages I and II in Hodgkin's disease" The.EORTC Lymphoma Group controlled clinical triMg: 1w Blood -73:47-56, 1989
23. Gospodarowicz M, Sutcliffe S, Clark R, et al: Analysis of supradiaphragmatic clinical stage I and II Hodgkin's disease treated with radiation alone. Int J Radiat Oncol Biol Phys 22:859-865, 1992
24. Pavlovsky S, Maschio M, Santarelli M, et al: Randomized trial of chemotherapy versus chemotherapy plus radiotherapy for

Favorable CSI-H Hodgkin's Disease 1 7 1
stage MI Hodgkin's disease.J Natl Cancer Inst 80: t466-1473, 1988
25. Specht L, Nordentoft A, Cold S, et al: Tumor burden as the most important prognostic factor in early stage Hodgkin's disease. Relations to other prognostic factors and implications for choice of treatment. Cancer 61:1719-1727, 1988
26. Mauch P, Goodman R, Hellman S: The significance of mediastinal involvement in early stage hodgkin's disease. Cancer 42: t 039-1045, 1978
27. Mauch P, Gorshein D, Cunningham J, et al: Influence of mediastinal adenopathy on site and frequency of relapse in patients with Hodgkin's disease. Cancer Treatment Reports 66:809-817, 1982
28. Prosnitz L, Curtis A, Knowlton A, et al: Supradiaphragmatic Hodgkin's Disease: Significance of large mediastinal masses. IntJ Radiat Oncol Biol Phys 6:809-813, 1980
29. Fuller L, !Madoc-Jones H, Shullenberger C, et al: Further follow-up of results of treatment in 90 laparotomy-negative stage I and II Hodgkin's disease patients: Significance of mediastinal and non-mediastinal presentations. Int J Radiat Oncol Biol Phys 6:799-808, 1980
30. Lee C, Bloomfield C, Goldman A, et al: Prognostic signifi- cance of mediastinal involvement in Hodgkin's disease treated with curative radiotherapy. Cancer 46:2403-2409, 1980
31. Schomberg P, Evans R, O'Connell M, et al: Prognostic significance of mediastinal mass in adult Hodgkin's disease. Cancer 53:324-328, 1984
32. Velentjas E, Barrett A, McEIwain T: Mediastinal involvement in early-stage Hodgkin's disease: Response to treatment and pattern of relapse. EurJ Cancer 16:1065-1068, 1980
33. Crnkovich M, Leopold K, Hoppe R, et al: Stage I to IIB Hodgkin's disease: The combined experience at Stanford University and the Joint Center for Radiation Theraw. J Clin Oncol 5:1041-1049, 1987
34. Cosset J, Henry-Amar M, Meerwaldt J, et al: The EORTC trials for limited stage Hodgkin's disease. Eur J Cancer 11:1847-1850, 1992
35. Noordijk E, Carde P, Mandard A, et al: Preliminary results of the EORTC-GPMC controlled clinical trial H7 in early stage Hodgkin's disease. Ann Oncol 5:107-112, 1994
36. Rosenberg S, Kaplan H: The evolution and summary results of the Stanford randomized clinical trials of the management of Hodgkin's disease: 1962-1984. IntJ Radiat Onc01Biol Phys 11:5-22, 1985
37. Fuller L, Hutchison G: Collaborative clinical trial for stage I and II Hodgkin's disease: Significance of mediastinal and nonmediastinal disease in laparotomy- and non-laparotomy- staged patients. Cancer Treatment Reports 66:775-787, 1982
38. HaybittleJ, Easterling M, Bennett M, et al: Review of British
National Lymphoma Investigation Studies of Hodgkin's dis- ease and Development of Prognostic Index. The Lancet 1:967-972, 1985
39. Hope-Stone H: The place ofradiatherapy in the management of localized Hodgkin's disease. Clin Radio132:519-522, t 981
40. Coia L, Hanks G: Complications from large field intermediate dose infradiaphragmatic radiation: An analysis of the patterns of care outcome studies for Hodgkin's disease and seminoma. IntJ Radiat Oncol Biol Phys 15:29-35, 1988
41. Tarbell N, Thompson L, Mauch P: Thoracic irradiation in Hodgkin's Disease: Disease control and long-term complica- tions. IntJ Radiat Oncol Biol Phys 18:275-281, 1990
42. Tucker M, Coleman C, Cox R, et al: Risk of second cancers after treatment for Hodgkin's disease. N EnglJ Med 318:76- 81, 1988
43. Tubiana M, Henri-Amar M, Hayat M, et al: The EORTC treatment of early stages of Hodgkin's disease: The role of radiotherapy. IntJ Radiat Oncol Biol Phys 10:197-210, 1984
44. Sutcliffe S, Gospodarowicz M, Bergsagel D, et al: Prognostic groups for management of localized Hodgkin's disease.J Clin Oncol 3:393-401, 1985
45. Ganesan T, Wrigley P, Murray P, et al: Radiotherapy for stage I Hodgkin's disease: 20 years of experience at St Bartho- lomew's Hospital. BrJ Cancer 62:314-318, 1990
46. ,Mauch P, Canellos G, Shulman L, et al: Mantle irradiation Mone for selected patients with laparotomy-staged IA to IIA Hodgkin's disease: Preliminary results of a prospective trial.J Clin Oncol 13:947-952, 1995
47. Biti G, Cimino G, Cartoni C, et al: Extended-field radio- therapy is superior to MOPP chemotherapy for the treatment of pathologic stage I-IIA Hodgkin's disease: Eight-year update of an Italian prospective randomized study. J Clin Oncol 10:378-382, 1992
48. Longo D, Glatstein E, Duffey P, et al: Radiation therapy versus combination chemotherapy in the treatment of early- stage Hodgkin's disease: Seven-year results of a prospective randomized trial.J Clin Oncol 9:906-917, 1991
49. Horning S, Hoppe R, Hancock S, et al: Vinblastine, bleomycin, and methotrexate: An effective adjuvant in favorable Hodgkin's disease .J Clin Oncol 6:1822-1831, 1988
50. Bates N, Williams M, Bessell E, et al: Efficacy and toxicity of vinblastine, bleomycin, and methotrexate with involved field radiotherapy in clinical stage IA and HA Hodgkin's disease: A British National Lymphoma Investigation pilot study. J Clin Onco112:288-296, i994
51. Straus D, YahalomJ, GaynorJ, et al: Four cycles of chemother- apy and regional radiation therapy for clinical early-stage and intermediate-stage Hodgkin's disease. Cancer 69:1052-1060, 1992





























