Embed Size (px)
Citation preview

Likely Amantadine-Induced Livedo Reticularisin a Child
Fernando Barrera, B.A.,* and John C. Browning, M.D.*,�
*Division of Dermatology and Cutaneous Surgery and �Pediatric Dermatology Section, Department of Pediatrics,University of Texas Health Science Center at San Antonio, San Antonio, Texas
Abstract: We present an 11-year-old boy with livedo reticularis (LR)secondary to amantadine treatment for his attention deficit hyperactivitydisorder (ADHD). We are unaware of previous reports of amantadine-inducedLR associated with treatment for ADHD in the pediatric population.
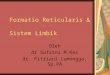
An 11-year-old boy presented to our clinic withcomplaints of an asymptomatic rash on his arms andlegs. This pattern persisted consistently and did not varywith cold or heat. The patient had a mild allergy topeanuts and had been taking dexmethylphenidate,amantadine, melatonin, trazodone, and lamotrigine forattention deficit hyperactivity disorder (ADHD) andanxiety. The patient initially noticed a mild lacyappearance on his legs shortly after starting the aman-tadine. The amantadine dose had been 100 mg twicedaily andwas then increased to 200mg twice daily. Afterthe increase, the lacy reticulated pattern became muchmore pronounced on the legs and also appeared on thearms. On examination, an erythematous net-like patternwas present on both legs and arms (Fig. 1). A diagnosisof amantadine-induced livedo reticularis (LR)wasmade.It was recommended that the patient see his neurologistto consider alternative medications for ADHD, butbecause of the asymptomatic nature of the LR, thepatient’smotherelected tocontinuewith theamantadine.
DISCUSSION
LR is a common vascular condition that manifests as amottled, net-like reddish-blue pattern on the skin. Most
cases of LR are asymptomatic and require no treatment,although some cases may lead to ulcerations (1). Table 1details the various causes of LR.
Address correspondence to John C. Browning, M.D., PediatricDermatology Section, University of Texas Health Science Center,San Antonio, 7703 Floyd Curl Drive, MSC 7808, San Antonio, TX78229, USA, or e-mail: [email protected].
DOI: 10.1111/j.1525-1470.2011.01437.x
Figure 1. Reddish-blue reticulated pattern on the legs.
� 2011 Wiley Periodicals, Inc. 329
Pediatric Dermatology Vol. 29 No. 3 329–330, 2012

The Food and Drug Administration (FDA) initiallyapproved amantadine in 1966 to prevent or treat influ-enza A virus infection but is rarely used now for thatindication since the development of the influenza vac-cine and oseltamivir. In recent years, amantadine hasbecome a common mode of treatment for Parkinson’sdisease (PD) and multiple sclerosis (1). The reportedincidence ofLR in patients treatedwith amantadine is upto 40% (1). Recent studies suggest that amantadine actsas a noncompetitive N-methyl-D-aspartate (NMDA)receptor antagonist and thereby promotes dopaminerelease, leading to reduced symptoms of PD andADHD(2,3).
The patient presented here was taking dexmethyl-phenidate and amantadine for ADHD. Dexmethyl-phenidate, a FDA-approved drug forADHDtreatment,is anecdotally reported to contribute to the developmentof LR (4). Amantadine, which is not FDA approved forADHD treatment, is a better recognized cause of LR (1).Although dexmethylphenidate, in conjunction withamantadine, may have concomitantly increased thepatient’s risk of LR, we believe this is a case of amanta-dine-induced LR because of the temporal associationbetween the increased dosage of amantadine and themanifestationofLR.LR ismost commonly foundon thelegs, followed by the trunk and arms. Amantadine isreported to cause the loss of catecholamines in peripheralnerve terminals, which may induce venodilation, leadingto the development of LR (5). To our knowledge,amantadine-induced LR has never been reported in thepediatric population, probably because of the rarity ofamantadine being prescribed in this population becausePD would be exceedingly unlikely in children. ADHD,however, is a common diagnosis in children, andamantadine may continue to be prescribed off-label asphysicians search for alternative treatment modalities inrecalcitrant situations. It is important forphysicians tobeaware of this potential drug-induced reaction.
REFERENCES
1. Gibbs MB, English JC 3rd, Zirwas MJ. Livedo reticularis:an update. J Am Acad Dermatol 2005;52:1009–1019.
2. Donfrancesco R, Calderoni D, Vitiello B. Open-labelamantadine in children with attention-deficit ⁄hyperactivitydisorder. J Child Adolesc Psychopharmacol 2007;17:657–664.
3. LugingerE,WenningGK,BoschS et al. Beneficial effects ofamantadine on L-dopa-induced dyskinesias in Parkinson’sdisease. Mov Disord 2000;15:873–878.
4. Syed RH,Moore TL.Methylphenidate and dextroamphet-amine-induced peripheral vasculopathy. J Clin Rheumatol2008;14:30–33.
5. Vollum DI, Parkes JD, Doyle D. Livedo Reticularis duringAmantadine Treatment. Br Med J 1971;2:627–628.
TABLE 1. Various reasons for the presence of livedo reticularis
Cause ⁄ association
Type oflivedoreticularis
Commonpopulation
LR induced by coldtemperature
Physiologic ⁄ cutismarmorata
Neonate,female
Local hypoxia Primary N ⁄AUnknown Idiopathic Females of
20–60 yearsCongenital CMTC* 0–5 yearsHematologic ⁄ hypercoaguable
Antiphospholipid syndrome Secondary N ⁄ASystemic lupus erythematosus Secondary N ⁄ASneddon’s syndrome Secondary N ⁄ACryoglobulinemia Secondary N ⁄ACryofibrinogenemia Secondary N ⁄ACutaneous polyarteritisnodosa
Secondary N ⁄A
Autoimmune disordersDermatomyositis Secondary N ⁄AWegener’s granulomatosis Secondary N ⁄ATakayasu’s arteritis Secondary N ⁄A
Emboli ⁄Vessel wall depositionCholesterol embolizationsyndrome
Secondary N ⁄A
Postinstrumentation septicemboli
Secondary N ⁄A
Calciphylaxis Secondary N ⁄AHyperoxaluria Secondary N ⁄A
Infectious diseaseSyphilis Secondary N ⁄ATuberculosis Secondary N ⁄ARheumatic fever Secondary N ⁄ABrucella Secondary N ⁄ATyphus fever Secondary N ⁄AEndocarditis Secondary N ⁄AHepatitis C Secondary N ⁄ARickettsia Secondary N ⁄A
Neurologic disorderReflex sympatheticdystrophy
Secondary N ⁄A
Pernicious anemia Secondary N ⁄AApoplexia Secondary N ⁄AMultiple sclerosis Secondary N ⁄AEncephalitis Secondary N ⁄AParkinson’s disease Secondary N ⁄A
Endocrine ⁄ nutritionalCushing’s disease Secondary N ⁄AHypercalcemia Secondary N ⁄AHyperthyroidism Secondary N ⁄APheochromocytoma Secondary N ⁄A
MedicationAmantadine Secondary,
drug-inducedN ⁄A
Anticoagulants Secondary,drug-induced
N ⁄A
Bismuth Secondary,drug-induced
N ⁄A
Catacholamines Secondary,drug-induced
N ⁄A
Methylphenidate Secondary,drug-induced
N ⁄A
Quinidine Secondary,drug-induced
N ⁄A
Thrombolytics Secondary,drug-induced
N ⁄A
Physiologic causes of LR: Altered ANS function, Circulatingvenodilators, Local hypoxia, Vasospasm due to cold or ANS input,Arterial thrombosis, Venous thrombosis, Increased blood viscosity.*Cutis marmorata telangiectatica congenita.
330 Pediatric Dermatology Vol. 29 No. 3 May ⁄ June 2012