Embed Size (px)
Citation preview

LET’S BEAT DIABETES
A Five Year Plan to Prevent and Manage Type 2 Diabetes
in Counties Manukau
FINAL PLANEndorsed by the Board of Counties Manukau District Health Board
02 February 2005

Table of Contents
Part I Introduction & Overview ________________________________________ 1
Executive Summary______________________________________________________ 2
This Document __________________________________________________________ 3
A Letter From 2020 ______________________________________________________ 4
The Planning Process_____________________________________________________ 6
Diabetes in Counties Manukau____________________________________________ 10
Whole Society, Whole Life Course, Whole Family Approach___________________ 13
Part II Let’s Beat Diabetes ___________________________________________ 15
Let’s Beat Diabetes _____________________________________________________ 16
1. Supporting Community Leadership and Action ___________________________ 21
2. Promoting Behaviour Change Through Social Marketing ___________________ 30
3. Changing Urban Design to Support Healthy, Active Lifestyles _______________ 33
4. Supporting a Healthy Environment Through a Food Industry Accord ________ 37
5. Strengthening Health Promotion Co-ordination and Activity ________________ 40
6. Enhancing Well Child Services to Reduce Childhood Obesity________________ 45
7. Developing a Schools Accord to Ensure Children Are ‘Fit, Healthy and Ready to Learn’ ________________________________________________________________ 49
8. Supporting Primary Care-Based Prevention and Early Intervention __________ 55
9. Enabling Vulnerable Families to Make Healthy Choices ____________________ 59
10. Improving Service Integration and Care for Advanced Disease _____________ 64
Enablers ______________________________________________________________ 70
Part III Implementation ______________________________________________ 75
Executive Summary_____________________________________________________ 76
Scoping the task ________________________________________________________ 77
Implementation structure and process _____________________________________ 80
References_____________________________________________________________ 91
Please note: the diabetes referred to in this document is Type 2 Diabetes.

Part I
Introduction & Overview
1 FINAL PLAN 02 February 2005

Executive Summary
Counties Manukau is experiencing a growing epidemic of Type 2 Diabetes (“diabetes”).Currently there are more than 12,000 people in Counties Manukau diagnosed withdiabetes. Almost double this number remains undiagnosed. It is estimated that thenumber of people with diabetes will more than double over the next 20 years, given population growth, the ethnic, youthful and generally low socio-economic make up ofour population.
A major change to the health sector and our broader society is required to stop thediabetes epidemic.
Let’s Beat Diabetes, commissioned by Counties Manukau District Health Board(CMDHB), is a five year plan aimed at long-term structural changes to prevent and/ordelay the onset of diabetes, slow disease progression, and increase the quality of lifefor people with diabetes. It recognises the significant activity that already exists toprevent and mange diabetes, and creates a long-term vision to align existing activity and a context for new investment, based on evidence and best practice.
Let’s Beat Diabetes is a district-owned plan developed by Counties Manukau for Counties Manukau.
After extensive consultation, Ten Action Areas have been defined:
1. Supporting Community Leadership and Action
2. Promoting Behaviour Change Through Social Marketing
3. Changing Urban Design to Support Healthy, Active Lifestyles
4. Supporting a Healthy Environment Through a Food Industry Accord
5. Strengthening Health Promotion Co-ordination and Activity
6. Enhancing Well Child Services to Reduce Childhood Obesity
7. Developing a Schools Accord to Ensure Children are ‘Fit, Healthy and Ready toLearn’
8. Supporting Primary Care-based Prevention and Early Intervention
9. Enabling Vulnerable Families to Make Healthy Choices
10. Improving Service Integration and Care for Advanced Disease
The plan aligns with Government policy directions and international best practice. Strategies that focus on improved Maori and Pacific outcomes are woven through allTen Action Areas.
The plan will be supported with committed funds and a governance structure that reflects the broad societal support required for successful implementation.
The plan will be presented to the Board of CMDHB and other key stakeholder representative groups in early 2005 for endorsement and sustained funding. Developmental work and preparations will continue early 2005, with full implementationfrom 01 July 2005.
2 FINAL PLAN 02 February 2005

This Document
This document provides a context for a whole society response to diabetes, aframework for action and an implementation plan.
The intention is to provide a vision and shape for community partnerships over the nextfive years.
The planning process during 2005 will involve detailed programme development bycommunity partners in each of the Ten Action Areas. One of the outcomes of this more detailed work will be to refine the goals, targets and key performance indicators foreach of the Action Areas, as well as setting overall goals for the plan. The plan willcontinue to be updated as developmental work progresses.
Currently this plan does not include inpatient secondary and tertiary services or morbidobesity.
This document does not provide a detailed analysis of diabetes in Counties Manukau - this was covered in an earlier document: Diabetes in Counties Manukau – A Call toAction. This document is also not a business case and does not discuss fundingissues. This is addressed in a separate document.
The intended audience for the plan is the Counties Manukau community and district organisations and individuals who will take up leadership roles in the campaign to beatdiabetes.
3 FINAL PLAN 02 February 2005
A Letter From 2020
It is the year 2020. Type 2 Diabetes is still a major health problem in Counties Manukau - thenumber of people diagnosed with diabetes is greater than it was in 2010 - but positive trendsare emerging that show diabetes rates and numbers will decrease over the next decade. Weare beating diabetes!
The turning point in the battle against diabetes came in 2010, when the growth in populationobesity stabilised, and from 2012 when average weights began to decrease. Many expertshave commented on the rapid reduction in the number of obese children since 2015, with a new wave of well nourished, fit children now flowing through the primary schools.
How did we get to this point, when back in the early years of the century it seemed nothingcould stop the growth in diabetes? The simple answer is that it has been the collective efforts ofmany strategies applied over decades and a commitment from all parts of society to a sharedvision and goal – much like the smoking epidemic of 50 years earlier.
While the big gains in health have been made in the past five year (2015 – 2020), the realchanges came in the 2005 - 2010 period. Those years are remembered as the ‘hard yards’,when there was a lot of effort for little change in outcome. But they put in place many of the strategies that continue to guide us today, and most importantly, galvanised commitment and action across society.
It was during those years that the renaissance in Maori and Pacific health began, withcommunity leadership, through marae and Pacific churches, taking up the challenge of improving the health of their people, especially the young ones. The change in communityattitude and behaviour towards nutrition and physical activity seemed to reach a tipping point in2009 - adult and child obesity levels in Maori and Pacific populations began to decreasesignificantly faster than those of the general population.
The general change in community attitude had its roots in community leadership but was furthersupported by a comprehensive social marketing programme that began in 2005 and is now partof our cultural landscape. In fact, the partnerships between health sector, local government,and the food and physical activity industries, which characterises the national social marketingprogramme of today, was forged in Counties Manukau 15 years ago.
The fast food industry is now competing on product ‘health/goodness’. And while the trendstowards eating out and consuming pre-prepared food have continued, the population diet hassignificantly improved. Children cringe when they are shown some of the meals their parentsused to eat.
For more than a decade, schools have taken explicit accountability for the physical health of children while they’re at school. This has meant ensuring students get at least 30 minutes of physical activity every day. All schools in Counties Manukau actively support good nutrition.The number of children walking or cycling to school has doubled since 2010, thanks to efforts by schools, working with communities, local government, and activity organisations. Many educationalists have noted that the improved health of students has also contributed toimproved academic performance in Counties Manukau.
The Flat Bush development, which was identified as the pilot for the ‘healthy by design’ planninginitiative, is now seen across New Zealand as a watershed in urban design, with its focus onhealthy, active and socially cohesive communities. The lessons from Flat Bush have alreadybeen applied to urban developments and redevelopments across the country.
Child health has been a substantial success story, attributed to improved services and changesin attitudes towards health in the first years of life. Well Child Services are now broad in scopeand include a focus on good nutrition and chronic disease prevention, through pregnancy andfrom birth. There is a significant investment in parental education and sophisticated techniques
4 FINAL PLAN 02 February 2005

for identifying vulnerable families and children. Multi-sectoral support is available for vulnerablefamilies, with information systems helping co-ordinated service delivery across agencies. The Well Teen pilot for a structured health assessment of 13 year olds has now become a nationalprogramme.
Primary care has evolved (despite continual government restructuring … some things don’tchange) to have a far greater focus on disease prevention.
Primary Health Organisations (PHOs) have become sophisticated organisations, with a strongcommunity and civic presence. GP surgeries have in general been consolidated into fewerlarger centres, with the development of nurse-led healthy living and disease management teams
The primary-care based in-clinic and outreach teams have become expert at processes of family and group-based behaviour modification, which, coupled with early diagnosis, has led to a measurable slowing in disease progression and a reduction in expensive hospital-based care.Supporting the re-orientation of primary care is the continuous development of a world-leadingIT system that provides best practice advice to GP teams and to the health consumer.
Health promotion is often described as the glue in the system. A set of strong organisationseffectively link the community development, social marketing and primary care strategies at an operational level, and provide a source of community-based innovations to service design. One of the most remarkable and enduring changes during the 2005 - 2010 period was thedevelopment of the health alliances –self-organising groupings of community, health and socialservice providers - which developed long term place-based strategies to identify and support themost vulnerable families.
One of the key features of Counties Manukau’s efforts to beat diabetes has been an extremelystable governance and leadership structure. Representatives from many organisations andcommunities still form the core governance structure to beat diabetes, and the group hasbecome something of a Counties Manukau institution. This stability has been at the heart of the persistent year-on-year progress.
Another key feature that has been emphasised in academic reviews is the ‘success model’ of learning and service development that has been adopted across many health providers. Somehave likened it to ‘action research on a massive scale’ or a continuous quality improvementstrategy. But the result has been the rapid uptake of innovations in practice across providers.The ability to learn from each other is one of the defining features of the ‘Counties Manukauway’.
The final success factor was the decision by the District Health Board to invest ‘upstream’ andcommit effort and money to support strategies that reduced risk and identified vulnerable peopleat an early stage in their disease. It is these strategies that are providing payback now in termsof health sector costs and community vitality.
5 FINAL PLAN 02 February 2005

The Planning Process
The required outcomes of the planning process have been to develop a plan for theCounties Manukau district as a whole (not just the health sector) and to buildcommunity momentum in support of the plan. Achieving these outcomes has requiredtaking a highly participative approach, creating the foundations for long-termrelationships, collaborative partnerships and networks.
A steering group made up of community, professional and cross-sector representativeshas guided the development of the plan. The planning process has been open andtransparent at every stage. All key planning documents developed during the year andthe minutes of all the working shops and group activities have been posted on the Let’sBeat Diabetes website (www.cmdhb.org.nz) to provide a fully public view of the ideasand participants guiding the planning process. Graphic 1 below shows an outline of the planning process.
Taking a comprehensivelong termapproach
Creating an environment forcollaborativeaction
Buildingcapacity todeliver
Fosteringopendevelopment
A plan forCountiesManukau tobeatdiabetes
Key Planning Concepts
Six concepts have influenced the planning approach:
1. Guiding principles of the World Health Organisation’s (WHO) Global Strategyon Diet, Physical Activity and Health (2004)
Whilst the global strategy is aimed at the international community and national-level strategies, it contains a discussion of principles to guide action and recommendedareas of activity. The strategy provides an excellent starting point for developing along-term change programme. Key principles taken from the global strategy include:
Evidence-based strategies
Multi-sectoral action
Long-term approach
Life course approach
Broad, comprehensive efforts
Priority on most vulnerable groups
All parties accountable for policies and programmes
6 FINAL PLAN 02 February 2005
Culturally-appropriate, and challenge cultural influences
2. Evidence of need and effective action
The plan development has been based on needs analysis, and evidence of effectiveinterventions, whether it be international or local evidence. There are, however, someareas where there is a clear need for action but a lack of strong evidence for effective programmes. In these situations, it is critical that thorough evaluation is undertaken todevelop new evidence – a good example of this issue is in the schools programme.The plan structure and approach taken by Let’s Beat Diabetes closely aligns withinternational best practice and is reflected in many recent national and state strategies;examples include: The New South Wales Chronic Disease Prevention Strategy 2003-2007, the Australian National Public Health Partnership Prevention Chronic Disease aStrategic Framework (2001) and the US Centres for Disease Control PromisingPractices in Chronic Disease Prevention and Control (2003).
3. Sector capacity and community motivation
The plan has identified where need, evidence and good ideas intersect with the localcapacity and motivation for action. There is little point in proposing strategies wherethe community and organisations are not ready and/or willing to take up the call.Examples of finding fertile ground for action include the food industry being strongly motivated to develop tangible outcomes following the signing of the National FoodIndustry Accord; the new Family and Community Services division of the Ministry ofSocial Development wanting to work with the health sector in the area of vulnerablefamilies; and Pacific church leaders wanting to be more involved in supporting thephysical health of their communities.
4. Long term approach
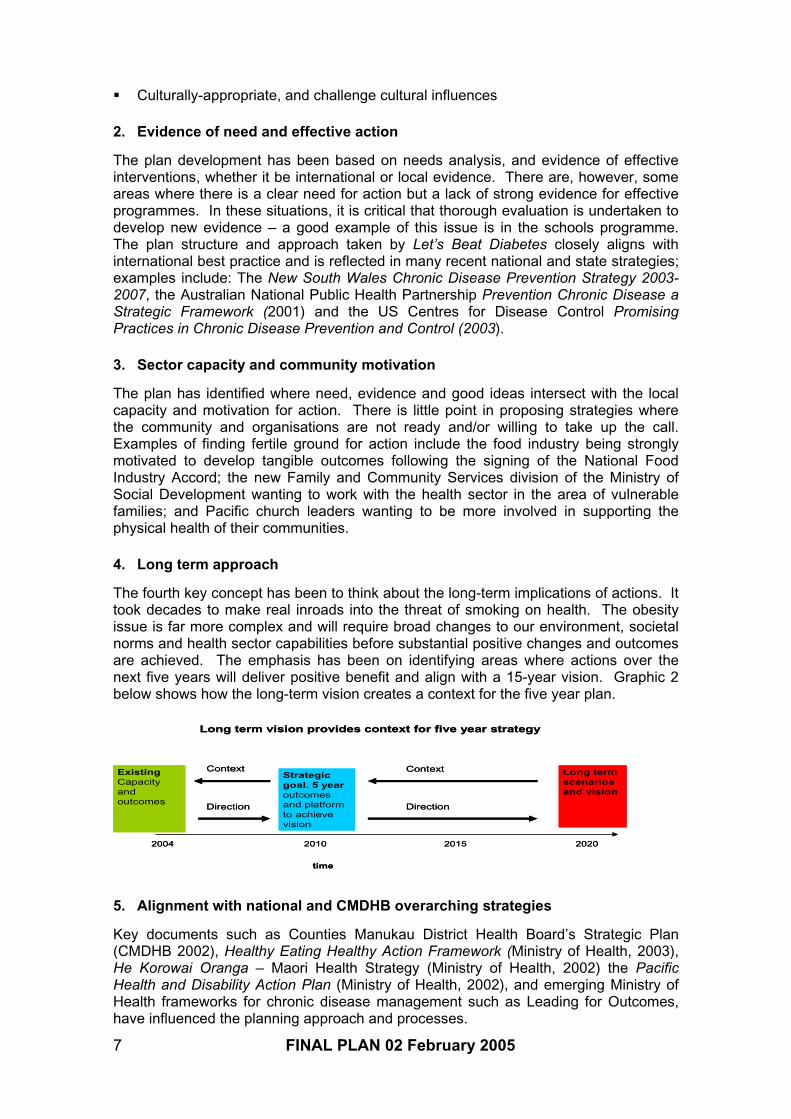
The fourth key concept has been to think about the long-term implications of actions. Ittook decades to make real inroads into the threat of smoking on health. The obesityissue is far more complex and will require broad changes to our environment, societal norms and health sector capabilities before substantial positive changes and outcomes are achieved. The emphasis has been on identifying areas where actions over thenext five years will deliver positive benefit and align with a 15-year vision. Graphic 2below shows how the long-term vision creates a context for the five year plan.
time
2004 2010 2015 2020
Long termscenariosand vision
ExistingCapacityandoutcomes
Strategicgoal. 5 yearoutcomesand platformto achievevision
Context
Direction Direction
Context
Long term vision provides context for five year strategy
time
2004 2010 2015 2020
Long termscenariosand vision
ExistingCapacityandoutcomes
Strategicgoal. 5 yearoutcomesand platformto achievevision
Context
Direction Direction
Context
Long term vision provides context for five year strategy
5. Alignment with national and CMDHB overarching strategies
Key documents such as Counties Manukau District Health Board’s Strategic Plan(CMDHB 2002), Healthy Eating Healthy Action Framework (Ministry of Health, 2003), He Korowai Oranga – Maori Health Strategy (Ministry of Health, 2002) the PacificHealth and Disability Action Plan (Ministry of Health, 2002), and emerging Ministry ofHealth frameworks for chronic disease management such as Leading for Outcomes,have influenced the planning approach and processes.
7 FINAL PLAN 02 February 2005

6. Building on lessons from past strategies and services
Counties Manukau has a long history of strategic planning and service innovations relating to diabetes, including the work undertaken by Dr David Simmons during the1990s and the South Auckland Diabetes Report prepared in 2000. In many areas, Counties Manukau service providers have developed innovative services, some ofwhich have been sustained. One of the challenges for Let’s Beat Diabetes has been tolearn from this rich background and to create the systematic conditions that supportsustainable programmes.
7. Building on existing strengths
Let’s Beat Diabetes starts from a strong base. CMDHB has for the past five yearsinvested in improved chronic care management in the primary care sector. TheChronic Care Management (CCM) programme is well advanced and involves primary care being supported by training, information technology (IT) and decision support tools to provide structured care in the community for people with advanced diabetes. CCMis supported by Whitiora, the Middlemore Hospital Diabetes Service. Whitiora provides training for practice teams and outreach education for patients as well as clinicalservices.
Primary Health Organisations (PHOs) are increasingly developing new healthpromotion and disease prevention services. Maori and Pacific providers deliverspecific services and programmes to their respective communities. Niche providerssuch as the Diabetes Projects Trust also provide community-based health promotionand education activities. Counties Manukau has a history of health leadership fromManukau City Council with the Te Ora O Manukau/Manukau the Health City and morerecently the Tomorrow’s Manukau Health and Wellbeing Outcome Group. TheAuckland Regional Public Health Service (ARPHS), which has an office in ManukauCity, provides services aimed at improving lifestyle and environmental risk factors.
8 FINAL PLAN 02 February 2005

Obesity & Diabetes - Global Epidemics
The world is currently experiencing an unprecedented growth in obesity. Obesity is amajor risk factor for Type 2 Diabetes.
In 1995, there were an estimated 200 million obese adults world-wide. By 2000, thenumber of obese adults had increased to over 300 million.
The situation in New Zealand is no different. Approximately 59.5 percent of all NewZealand adult males and 48.6 percent of all New Zealand adult females areoverweight. These figures are more marked for Maori and Pacific adult populations,where 68.5 percent of Maori males, 59.2 percent of Maori females, 80.9 percent ofPacific males and 82 percent of Pacific females are overweight (Ministry of Health,2003).
The figures for children are of particular concern with 31 percent of all childrenoverweight, 62 percent of Pacific children overweight, and 41 percent of Maori children overweight.
The prevalence of obesity is increasing. Between 1989 and 1997 adult obesityincreased by 55 percent. From 1997 to 2011 obesity is expected to increase by afurther 70 percent. It has also been estimated that by 2011 approximately 29 percentof the adult population may be obese (Ministry of Health, 2002).
Diabetes – A Disease of Inequalities
Diabetes is a serious chronic disease that leads to serious complications such as heart disease, kidney failure, stroke, and blindness. People with diabetes have a reducedlife expectancy. Currently, one in 12 adults over 45 years in New Zealand have beendiagnosed with diabetes.
Diabetes is a disease of inequalities, with Maori and Pacific peoples at greater risk ofdiabetes than other New Zealanders:
21 percent of Maori males over 45 years have diabetes compared to 8.5 percent of non-Maori
20 percent of all Maori and 17 percent of all Pacific deaths are due to diabetes – compared to 4 percent of deaths amongst European New Zealanders
The lifetime risk of being diagnosed for diabetes is one-in-four for Pacific peoplesand one-in-three for Maori – compared to one-in-ten for European New Zealanders
Approximately 8 percent of Maori and Pacific adults have diabetes compared to 3to 4 percent for European New Zealanders
Estimates are that from 1996 to 2011 the total number of adults with diabetes in New Zealand will increase by 78 percent, but the relative increase for Maori andPacific peoples will be 130 to 150 percent (Ministry of Health, 2002).
9 FINAL PLAN 02 February 2005

Diabetes in Counties Manukau
Counties Manukau is experiencing a growing epidemic of Type 2 Diabetes. Currently there are more than 12,000 people in Counties Manukau diagnosed with diabetes.Almost double this number remains undiagnosed. It is estimated that the number ofpeople with diabetes could more than double over the next 20 years, given population growth, the ethnic, youthful and generally low socio-economic make up of ourpopulation. In the graphic below the top dotted line shows the expected growth in diabetes if the prevalence of obesity goes on increasing – which is exactly what it is doing.
0
2 0 0 0
4 0 0 0
6 0 0 0
8 0 0 0
1 0 0 0 0
1 2 0 0 0
1 4 0 0 0
1 6 0 0 0
1 8 0 0 0
2 0 0 0 0
2001
2003
2005
2007
2009
2011
2013
2015
2017
2019
2021
Num
ber
of c
ases
M a o r i P a c i f i c
O t h e r T o t a l
M a o r i a d j u s t e d P a c i f i c a d j u s t e d
O t h e r a d j u s t e d T o t a l a d j u s t e d(Lindsay A, 2003)
A disturbing feature of this epidemic is that it is no longer ‘contained’ to people agedbetween 40 and 64 years of age. The number of young people being diagnosed withType 2 diabetes, while still small, is increasing. Children as young as 6 years old arenow being diagnosed with Type 2 Diabetes.
Mothers with gestational diabetes or pre-diabetic conditions may be passing on anincreased risk of diabetes to the unborn child. With more women in the childbearingage group at risk of diabetes, the risk to future generations is increasing.
People living in low decile areas of Counties Manukau are more likely to suffer fromdiabetes. The map below shows where these areas are – which are also where thereare high rates of diabetes (dark shading).
10 FINAL PLAN 02 February 2005

NORTH
SOUTH
TUREWAREWA
DENE SOUTHSTON CENTRAL
URILANDS
RANGI SOUTH
NTON
M
FREEMANS BAYNEWTON
GLENAVONAVONDALE SOUTH
WATERVIEW
ST LUKES NORTH
EPSOM CENTRAL
EPSOM SOUTH
MT HOBSON
REMUERA WEST
ORAKEI NORTH ST HELIERS
GLEN INNES NORTHGLEN INNES WEST
POINT ENGLAND
ROYAL OAK
HILLSBOROUGH EAST
WESLEY
LYNFIELD SOUTH
PENROSE
MT WELLINGTON NORTH
MT WELLINGTON SOUTH
PANMURE BASIN
PAERATA-CAPE HILL
EDEN ROAD-HILL TOP
BUCKLAND
KINGSEAT
POKENO
GLENBROOKBOMBAY
HINGAIA
WHANGAPOURI CREEK
BREMNER
DRURY
RUNCIMAN
MELLONS BAY
COCKLE BAY
OTAHUHU EAST
MIDDLEMORE
PAPATOETOE WEST
PAPATOETOE NORTH
BLEAKHOUSE
ELSMORE PARK
GOLFLAND
DANNEMORA
POINT VIEW
SHELLY PARK
TURANGA
ORMISTON
ARDMORE
TOTARA HEIGHTS
WAIRERE
RANDWICK PARKHYPERION
TAKANINI SOUTH
AMBURY
ARAHANGAVISCOUNT
MANGERE SOUTH
MANUKAU CENTRAL
BURBANK
WEYMOUTH
CLENDON
PAPAKURA CENTRAL
PAPAKURA NORTH
PUKEKOHE NORTH
BLEDISLOE PARK
WAIUKU
SOUTH WAIUKU TUAKAU
INLET-MANUKAU HARBOUR
INLET-WAIUKU RIVER
Rate per 100,000
2,400 to 6,550 (13)2,000 to 2,400 (8)1,600 to 2,000 (12)1,200 to 1,600 (13)
800 to 1,200 (21)400 to 800 (33)
1 to 400 (25)
Produced by AP Lindsay, Public Health Team, CMDHB
Based on hospital admission data only, for individual CM residents hospitalised anywhere in New Zealand
(Lindsay A 2003)
The Cost of Diabetes
Diabetes is a major driver of health sector costs within both primary and secondarycare, with increased cardiovascular disease, kidney disease, stroke, lower limb ulcersand retinal damage. Diabetes has explicit social costs through loss of work andsupport payments and implicit costs through the impact of chronic disease on family and community life.
11 FINAL PLAN 02 February 2005
Growth in diabetes leads to a huge increase in hospital costs, social support costs andloss of economic contributions. It is estimated that a person with diabetes generateshospital costs on average 2.5 times as much as someone without diabetes – and thatthe indirect costs are as much again (PriceWaterhouseCoopers, 2001). It is alsoestimated that as the number of patients with kidney failure grows (primarily due to theincreasing number of diabetics and an ageing population), the need for new dialysisstations will grow at a level that within five years, a new satellite clinic with 20 dialysisstations would be required every year to keep up with demand (Ratanjee, 2004).
The cost of diabetes to the family and community is significant and immeasurable.Diabetes robs us of our elders and the cultural richness and wisdom they bring to oursociety. With the increasing prevalence of diabetes moving down the age-spectrum, it is beginning to rob us of our future.
12 FINAL PLAN 02 February 2005

Whole Society, Whole Life Course, Whole
Family Approach
International research and evidence emphatically support a ‘whole society, whole life course, whole family’ approach to beat diabetes. The graphic below, adapted from adiabetes model developed by the US Centre for Disease Control, shows the challengefor a whole-system strategy.
Society’s healthresponse
Vulnerabilitycessation
Vulnerabilityonset
Death fromcomplications
Afflictionprogression
Afflictiononset
Tertiaryprevention
Secondaryprevention
Primaryprevention
Targetedprotection
Protectedpopulation
Vulnerablepopulation
Afflictedwithout
complications
Afflicted withcomplications
Societal responsibility Health sector responsibility
Generalprotection
Adverseliving
conditions
Investment Mix?
Adapted from (Homer J 2004)
A life course approach works across all areas from universal protection of the whole population to tertiary prevention for people already with diabetes.
The ‘afflicted with complications’ area is where most of health expenditure on diabetesoccurs at present. A life course approach supports analysis of the whole system,including public health, primary care and hospital services, and encourages explicit thinking about where to invest in the progression of risk and disease.
Investment decisions need to be based on evidence of effectiveness and also on anunderstanding on how programmes impact on disease progression and health sector costs. For example, reducing complications of someone with advanced diabetes mayhave an immediate payback in reduced hospital costs, while an investment in targetedprotection, like improving the schools environment, might not provide benefits to healthsystem costs for many years, in fact decades but may have a big impact on improvedlifelong health for many people.
Let’s Beat Diabetes
The approach taken in this plan is that well constructed strategies across the lifecourse should work in synergy. For example, a person with diabetes may be better atself management with a supportive church environment, encouraging social marketing,
13 FINAL PLAN 02 February 2005

a family that understands their problem, healthier food options and a practice team thatis proactive and motivational. Schools are more likely to take up a fit and healthy policy if the food industry is supportive, community leaders are backing them, vulnerablefamilies are identified and helped with food choices and support services make it easy for schools to schedule regular physical activity sessions.
14 FINAL PLAN 02 February 2005

Part II
Let’s Beat Diabetes
A Five Year Plan to Prevent and Manage Type 2 Diabetes in Counties Manukau
15 FINAL PLAN 02 February 2005

Let’s Beat Diabetes
Aim
The aim of the Let’s Beat Diabetes plan is to stop people getting diabetes, slow the disease progression, and increase the quality of life for people with diabetes.
Strategic Approach
A range of strategies are proposed, guided by the basic concept that a ‘whole society,whole life course, whole family/whanau’ approach is required to beat diabetes, and thatfocused effort will need to be sustained over decades.
Whole society – Acknowledgment that we cannot beat diabetes without themotivation and support of the communities, institutions and businesses that make up the social fabric of Counties Manukau.
Whole life course – A focus on supporting health and preventing and managingdiabetes at all stages of disease progression.
Whole family/whanau – Acknowledgment that an individual is part of a family/whanau (or household) which has a direct influence on environmental risks,choices and decisions. Wherever possible, working with families is central to the plan.
Guiding Principles
The principles of Partnership, Participation and Protection form the constitutionalfoundations of New Zealand through the Treaty of Waitangi. These principles are alsofundamental to the practice of modern public health.
Partnership – Institutions, organisations, communities, families and individuals must work together to beat diabetes. The scale of social response required for diabetesmeans that formal partnerships based on aligned goals and civic responsibilities will need to be developed and actively sustained.
Participation – The prevention and control of chronic disease is enabled through self management and via the ongoing participation of family, community and healthprofessionals in the lives of people with diabetes. Also, for strategies to be successful, families and communities must be able to participate in service design, development and governance.
Protection – The current diabetes epidemic has been created by a newenvironment of obesity. The ‘obesogenic environment’ is a threat to the health and wellbeing of our children and families. There is an obligation on behalf ofgovernment, business and community leadership to protect citizens from thisenvironmental hazard.
Ten Action Areas
The Let’s Beat Diabetes plan is complex and wide ranging. In order for it to beunderstood by, and motivational to our diverse communities, activity has been set out under ten key action areas. They are as follows:
16 FINAL PLAN 02 February 2005

1. Supporting Community Leadership and Action
2. Promoting Behaviour Change Through Social Marketing
3. Changing Urban Design to Support Healthy, Active Lifestyles
4. Supporting a Healthy Environment Through a Food Industry Accord
5. Strengthening Health Promotion Co-ordination and Activity
6. Enhancing Well Child Services to Reduce Childhood Obesity
7. Developing a Schools Accord to Ensure Children Are ‘Fit, Healthy and Ready toLearn’
8. Supporting Primary Care-based Prevention and Early Intervention
9. Enabling Vulnerable Families to Make Healthy Choices
10. Improving Service Integration and Care for Advanced Disease
The Ten Action Areas reflect a range of intervention strategies, including general andtargeted protection, and primary, secondary and tertiary prevention. They are designed to fit together to form an overall strategy that reduces risk factors for diabetes and slows disease progression, while building capacity in the health sector and a sustainable whole society approach. Graphic 3 below shows the zones each actionarea is designed to influence.
Vulnerabilitycessation
Vulnerabilityonset
Death fromcomplications
Afflictionprogression
Afflictiononset
Tertiaryprevention
Secondaryprevention
Primaryprevention
Targetedprotection
Protectedpopulation
Vulnerablepopulation
Afflictedwithout
complications
Afflicted withcomplications
•Food Industry Accord
•Primary care-base prevention
•Community leadership
•Urban design
•Social marketing
•Strengthening health promotion
•Schools Accord
•Enhanced Well Child
•Integrated care
•Vulnerable families
Generalprotection
Another way of looking at the Ten Action Areas is from the perspective of the family.As shown below in Graphic 4, the family is in the centre surrounded by rings of support.The outer ring is that of the social and environmental determinants of health, whichaffect everyone. The social determinants are the responsibility of society. The innerring is that of the more direct health environment and services environment. The services environment is mostly about the relationship between individuals (andfamilies) and government funded services. These are the services that the health
17 FINAL PLAN 02 February 2005

sector has more control over. Strength in both circles and strength within the family is required to reduce diabetes risk factors and control disease.
Knowledge
Culture
Food
Urban environment
Socio-econom
ic
Well ChildSchool health
Health
Prom
otion
Earlyintervention
Dis
ease
man
agem
ent
Enablers
The Ten Action Areas describe the content of activities needed to beat diabetes, butthere is also a set of support activities that must be managed in order to implement the plan in a sustainable manner. These support areas or ‘enablers’ are outlined below:
1. Consumer involvement
An effective consumer forum needs to be developed, or an existing forum enhancedand actively involved in the development of new programmes and evaluation design.
2. Maori
A Maori advisory forum will be developed, or an existing forum enhanced, to ensure allnew programmes and evaluation design are culturally responsive to Maori.
3. Pacific peoples
A Pacific advisory forum will be developed, or an existing forum enhanced, to ensureall new programmes and evaluation design are culturally responsive to Pacific peoples.
4. Funding environment
The funding environment is modified and aligned to support the Ten Action Areas.
5. Learning environment
Evaluation and learning systems are explicitly supported as part of the overall investment.
6. Sustainable governance
18 FINAL PLAN 02 February 2005

Governance and leadership for the whole plan and for each of the Ten Action Areas is developed and supported.
7. Organisational development
Investment in workforce, particularly in primary care, will be required as will thedevelopment of an ongoing centre of excellence for whole system diabetes preventionand management in Counties Manukau.
8. Information systems
The many disconnected systems and programmes used for supporting diabetesmanagement need to be brought together over time to align with the whole systemapproach outlined in the Let’s Beat Diabetes plan.
19 FINAL PLAN 02 February 2005

Let’s Beat Diabetes
Action Areas & Enablers
20 FINAL PLAN 02 February 2005

1. Supporting Community Leadership and Action
Context
The Let’s Beat Diabetes plan seeks to lay down the foundations for the long term reduction of Type 2 Diabetes in our community. These foundations are built on the understanding that real, sustainable change will require support from our whole society– from individuals, families, organisations, cultures, systems, policies and the myriaddimensions that make up our communities. Creating societal support for changerequires a proactive process of developing community leadership. Without community leadership, the Let’s Beat Diabetes plan will fail. It is individuals, within families, withincommunities, who make the decisions about their lives. Empowered communitieschange their environments through action, advocacy, local democracy and consumer choice. Our plan must work with communities in order to succeed.
The call for the community to lead and champion the fight against diabetes has beenvoiced by Maori and Pacific communities, who are most at risk from the diabetesepidemic. From our workshops, hui and fono on how to this support community leadership and change, a number of core concepts have emerged:
For Maori, it has been the need to work with the roots of culture and cultural normsin order to change behaviours that are causing diabetes. As one participant put it‘we need to change the lore’ as it applies to culture. This means working throughtraditional cultural institutions such as marae and contemporary institutions like kurakaupapa so tamariki learn and grow up in an environment where healthy eating and active living is the ‘lore’.
For Pacific peoples, it is about rediscovering, strengthening and practising thepositive aspects of their cultures and cultural practices around food and physicalactivity, and exploring opportunities for Pacific churches to be vehicles for physicalhealth promotion.
The Asian and new settlor community is diverse in its community structures and leadership. Ethnic-specific strategies will be required.
For the general population, the workplace has emerged as a place where institutions can have a tremendous positive influence on health and where there is great opportunity for improvement.
The community empowerment model, which seeks to build community connections,strength and self determination, and seeks community-based solutions to problems,has also emerged.
Programme Design
The programme design to support this Action Area is consistent with the communityempowerment model:
The strategies were developed through workshops, hui and fono, and ‘by Maori for Maori’ and ‘by Pacific for Pacific’ (please note: priority has been placed onsupporting activities for the Maori and Pacific communities, given the heightened risk these communities face from diabetes).
Let’s Beat Diabetes will support a broad range of ideas that encourage community empowerment, and utilise the strength of culture and cultural institutions to bring
21 FINAL PLAN 02 February 2005

22 FINAL PLAN 02 February 2005
about change to lifestyles and/or environments which reduce obesity or slow the progression of diabetes.
To facilitate this, Counties Manukau District Health Board (CMDHB) is proposing to set up a Community Action Fund (CAF) to support and assist initiatives that are aligned with the action plan. This funding will be available to a range of community organisations, ccessed via funding proposals.
The programme design also looks to the membership of Tomorrow’s Manukau Te Ora O Manukau/Manukau the Healthy City Outcome Group to role model healthy workplace policies. This group is comprised of key central and local government agencies and organisations in the district.

Act
ion
Pla
ns
Mao
ri
Wh
akak
ore
ng
ia t
e m
ate
hu
ka i
wae
ng
anu
i wh
anau
na
te m
oh
io m
e te
mar
ama.
To
pre
ven
t D
iab
etes
th
rou
gh
kn
ow
led
ge
and
un
der
stan
din
g.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
ers
Go
al:
T
ikan
ga
are
dev
elo
ped
an
dim
ple
men
ted
to
re
du
ce
at
risk
d
iab
etes
beh
avio
ur.
Tar
get
: ‘
Hea
lth
yea
tin
g a
ctiv
e liv
ing
’ ar
eva
lues
ado
pte
d
asan
ac
cep
ted
p
art
of
cust
om
an
d p
ract
ice.
Wha
nau,
hap
u, i
wi a
nd M
aori
com
mun
ities
of
inte
rest
dev
elop
‘hea
lthy
eatin
gac
tive
livin
g’ g
uide
lines
in c
onju
nctio
nw
ith h
ealth
org
anis
atio
ns.
Res
ourc
esw
hich
con
vert
‘hea
lthy
eatin
gac
tive
livin
g’ r
ules
/ gu
idel
ines
into
prac
tical
app
licat
ors
are
deve
lope
d (e
.g.
Bill
yT
han
dboo
ks).
R
esou
rces
nee
dto
be
targ
eted
at M
aori
envi
ronm
ent i
n bo
th la
ngua
ges.
‘Hea
lthy
eatin
g’ T
ikan
ga a
re d
evel
oped
byM
arae
, K
ohan
ga R
eo a
nd M
aori
orga
nisa
tions
in a
ll se
ctor
s.
‘Hea
lthea
ting
activ
e liv
ing’
aw
ards
are
awar
ded
annu
ally
at a
n ev
ent
toce
lebr
ate
‘wha
nau
ora’
life
styl
es.
Wha
nau,
ha
pu,
Iwi,
Mao
rico
mm
uniti
es
of
inte
rest
(e
.g.
educ
atio
n pr
ovid
ers,
spo
rt te
ams)
AR
PH
S,
Mao
ri he
alth
pr
ovid
ers,
heal
th p
rom
otio
n se
ctor
Mao
ri or
gani
satio
ns,
Mao
ri he
alth
prov
ider
s, M
aori
Hea
lth, C
MD
HB
Go
al:
T
o
iden
tify
o
pp
ort
un
itie
s (p
eop
lean
d
even
ts)
wit
hin
th
e co
mm
un
ity
toch
amp
ion
Mao
ri a
pp
roac
hes
to
red
uci
ng
Dia
bet
es.
Tar
get
:A
ca
len
dar
o
f ‘P
atu
a i
te
mat
eh
uka
’ ev
ents
is
ad
op
ted
ea
ch
year
.C
alen
dar
to
b
e d
evel
op
edw
ith
th
eco
mm
un
ity.
Wan
anga
M
ate
Huk
a ar
eho
sted
to
di
scus
s M
aori
appr
oach
es
to
beat
diab
etes
, an
dth
e ka
iwha
kaha
ere
(cha
mpi
on)
role
s to
be
play
edby
wha
nau
hapu
an
d iw
i.T
he
Wan
anga
in
clud
e M
anaw
henu
a,
kuia
/ ka
umat
ua,
cons
umer
s, r
anga
tahi
, tak
ataa
puia
nd o
ther
‘at r
isk’
Mao
ri gr
oups
.
For
mal
de
velo
pmen
t of
ka
iwha
kaha
ere
role
san
d re
spon
sibi
litie
s to
dr
ive
‘Pat
ua i
te m
ate
huka
’ are
und
erta
ken.
Rel
atio
nshi
psw
ith c
urre
nt M
aori
lead
ers
to p
rom
ote
posi
tive
Mao
ri di
abet
esm
essa
ges
are
esta
blis
hed.
T
hese
lea
ders
cou
ld i
nclu
deT
e A
taira
ngi
Kah
u,M
HA
C m
embe
rs, S
tace
y Jo
nes
and
Vee
shan
e A
rmst
rong
.
CM
DH
B,
Mao
ri he
alth
pr
ovid
ers,
Mao
ri,
Mao
riH
ealth
, M
anaw
henu
a,C
ount
ies
Man
ukau
Spo
rt
Go
al:
E
nsu
re
all
Mao
ri
un
der
stan
dd
iab
etes
an
d
the
risk
b
ehav
iou
rsw
hic
hin
crea
se t
he
chan
ces
for
get
tin
g d
iab
etes
.
Tar
get
: O
pp
ort
un
itie
s ar
e m
ade
avai
lab
lefo
r M
aori
to
ac
cess
h
ealt
hp
rom
oti
on
reso
urc
es a
nd
info
rmat
ion
on
dia
bet
es.
On-
goin
g de
velo
pmen
tof
hea
lth p
rom
otio
n re
sour
ces
are
clea
rly t
arge
ted
atM
aori,
acr
oss
the
age
spec
trum
.
Rec
ogni
sed
trai
ning
an
d ed
ucat
ion
pack
ages
fo
r de
liver
y to
M
aori
in
the
com
mun
ityar
e de
velo
ped.
The
se t
rain
ing
pack
ages
are
aim
edat
spe
cific
grou
ps, a
cros
s th
e ag
e sp
ectr
um.
A r
egul
ar t
imet
able
of
Wan
anga
Wha
nau
Ora
for
Mao
ri to
dis
cuss
dia
bete
s is
AR
PH
S,
Mao
ri pu
blic
heal
th,
heal
thpr
omot
ion
sect
or
AR
PH
S,
Mao
ri pu
blic
heal
th,
heal
thpr
omot
ion
sect
or
AR
PH
S,
Mao
ri pu
blic
heal
th,
heal
th
23F
INA
L P
LA
N 0
2 F
ebru
ary
2005

put
toge
ther
. W
here
pos
sibl
e th
ese
hui
will
lin
k in
with
exi
stin
g hu
i (e
.g.
Pou
kai,
Kap
a H
aka
com
petit
ions
et
c).
Util
ise
Mao
riev
ents
ca
lend
ar
to
prom
ote
key
‘hea
lth e
atin
g ac
tive
livin
g’ m
essa
ges.
prom
otio
n se
ctor
Go
al:
Mak
e p
hys
ical
act
ivit
ya
fun
, n
atu
ral
par
t o
f a
per
son
’s d
ay.
Tar
get
:
Mao
ri
of
all
ages
en
gag
e in
ph
ysic
al a
ctiv
ity
as a
par
to
f th
eir
no
rmal
day
.
A s
urve
y to
iden
tify
the
rang
eof
phy
sica
l act
ivity
activ
ities
cur
rent
lyca
rrie
d ou
tin
the
Cou
ntie
s M
anuk
au a
rea
by M
aori
is u
nder
take
n. I
nclu
deal
l fo
rms
ofac
tivity
incl
udin
g da
nce,
eld
erly
wal
king
cla
sses
etc
.
Wor
kw
ith r
egio
nal
and
natio
nal
bodi
es t
o id
entif
y ph
ysic
al a
ctiv
ity i
nitia
tives
curr
ently
unde
r de
velo
pmen
t, fo
r pi
lotin
g/la
unch
ing
with
in t
he l
ocal
are
a.E
nsur
e th
ere
is lo
cal i
nput
to m
ake
the
initi
ativ
e M
anuk
au–c
entr
ic.
Wor
kw
ith th
e co
mm
unity
to id
entif
y na
tura
lfit
of a
ctiv
ities
cur
rent
ly o
ffere
d an
dco
mm
unity
lead
er(s
) fo
r th
is a
ctiv
ity (
deve
lopm
ent p
roce
ss).
Pro
mot
e th
e de
velo
pmen
t of f
un, c
omm
unity
-orie
nted
act
ive
livin
g in
itiat
ives
, to
be le
ad b
y co
mm
unity
(e.
g.T
ake
Nan
/ Pop
for
a w
alk)
.
CM
DH
B,
SP
AR
C,
Cou
ntie
sM
anuk
auS
port
CM
DH
B,
SP
AR
C,
Cou
ntie
sM
anuk
ausp
ort
CM
DH
B, C
ount
ies
Man
ukau
Spo
rt
Com
mun
ity
lead
ers,
C
MD
HB
,C
ount
ies
Man
ukau
Spo
rt
Go
al:
Mak
e h
ealt
h e
atin
g a
fu
n,
nat
ura
lp
art
of
a p
erso
n’s
day
.
Tar
get
:
Mao
ri
of
all
ages
en
gag
e in
ph
ysic
al a
ctiv
ity
as a
par
to
f th
eir
no
rmal
day
.
A s
urve
y to
ide
ntify
the
ran
ge o
f he
alth
y ea
ting
initi
ativ
es a
nd r
esou
rces
avai
labl
e in
the
Cou
ntie
s M
anuk
au a
rea
is u
nder
take
n. I
nclu
de a
reas
whe
reM
aori
com
mun
ities
act
en
mas
s (e
.g.
Sec
onda
ry s
choo
ls f
estiv
al,
mar
kets
,sp
orts
occ
asio
ns,
etc.
) T
his
shou
ld in
clud
ew
hat
is h
ealth
y fo
od,
and
how
do
you
cook
hea
lthy
food
in a
hea
lthy
way
.
A ‘
heal
thy
eatin
g’ t
oolk
it (r
ouro
u) i
s de
velo
ped
to b
eus
ed a
s th
eba
sis
for
educ
atio
n/
heal
th
prom
otio
n se
ssio
nsfo
r de
liver
y in
al
l M
arae
/ M
aori
orga
nisa
tions
in th
e di
stric
t.
‘Hea
lth e
atin
gac
tive
livin
g’ m
arae
aw
ards
whi
ch a
ckno
wle
dge
the
wor
k ca
rrie
dou
t in
M
arae
to
ch
ange
th
e di
etar
yha
bits
of
ta
ngat
a w
henu
aan
d th
eir
man
uhiri
are
dev
elop
ed.
CM
DH
B, M
aori
Pub
lic H
ealth
CM
DH
B, A
RP
HS
, Mao
ri P
ublic
Hea
lthP
rovi
der
CM
DH
B, M
aori
Go
al:
R
ang
atah
i d
evel
op
a
Tik
ang
a/cu
ltu
rew
her
e th
ey
are
able
to
mak
e in
form
ed
nu
trit
ion
an
d
ph
ysic
alac
tivi
ty c
ho
ices
.
Tar
get
: R
ang
atah
i ar
eab
le t
o d
efin
ew
hat
hea
lth
yea
tin
g a
nd
act
ive
livin
g m
ean
s fo
rth
em a
s ex
amp
les
to e
very
on
e.
A r
anga
tahi
cou
ncil
to d
iscu
ss d
iabe
tes
is c
onve
ned.
M
ain
aim
of t
he fo
rum
isto
eng
age
Ran
gata
hi in
to H
ealth
foru
ms,
with
a p
urpo
se.
Wor
kw
ithyo
uth
to
iden
tify
barr
iers
to
heal
thy
livin
g an
dac
tive
lifes
tyle
sin
clud
ing:
Who
are
thei
r ro
le m
odel
s? T
he p
eopl
eyo
u lo
ok u
p to
?W
ho a
re th
eym
ore
likel
y to
take
info
rmat
ion
on b
oard
from
?W
ho w
illm
ake
a di
ffere
nce?
Wha
t thi
ngs
mak
e it
diffi
cult
to li
ve h
ealth
y,ac
tive
lifes
tyle
s?
CM
DH
B, M
aori
Hea
lth
CM
DH
B, M
aori
Hea
lth
24F
INA
L P
LA
N 0
2 F
ebru
ary
2005

Ran
gata
hi-f
ocus
ed ‘
heal
thy
eatin
gac
tive
livin
g’re
sour
ces
are
deve
lope
d an
ddi
strib
uted
thro
ugho
ut th
e co
mm
unity
.M
aori
publ
ic h
ealth
, he
alth
prom
otio
nse
ctor
Pac
ific
peo
ple
s
Su
amal
ie i
le g
utu
a’e
oo
na
i le
man
ava
– fa
’ala
lo le
ma'
i su
ka.
A T
on
gan
-led
dia
bet
es w
ork
forc
e, r
eso
urc
edto
wo
rk t
og
eth
er w
ith
th
e C
ou
nti
es M
anu
kau
co
mm
un
ity
to s
erve
ou
r fa
mili
es.
Ou
r ai
ms:
(1)
Ke
hao
faki
’i h
ota
u n
gaa
hi f
amili
mei
he
suka
an
d (
2) K
e le
va’i
lele
i e s
uka
‘i h
e fa
mili
.
Tam
ate
i te
toto
ven
e.
Om
ai k
e ka
u f
akal
atah
a ke
tu
ku h
ifo
e g
agao
su
ka k
i lal
o.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
ers
Go
al:
Lea
der
ship
Pac
ific
p
eop
les
lead
ersh
ip
gro
up
sw
ork
wit
h
the
hea
lth
se
cto
r to
le
ad
Pac
ific
co
mm
un
itie
s’ f
igh
t ag
ain
std
iab
etes
.
Tar
get
: G
rou
ps
esta
blis
hed
by
Ap
ril 2
005.
Eth
nic-
spec
ific
lead
ersh
ip g
roup
s es
tabl
ishe
d to
lead
the
Pac
ific
com
pone
nt o
f th
e ‘C
omm
unity
Le
ader
ship
an
d A
ctio
n’
activ
ity
area
of
the
Let’s
B
eat
Dia
bete
s pl
an.
Pac
ific
chur
ches
as
part
ners
and
cha
mpi
ons
for
heal
th p
rom
otio
nw
ill b
e su
ppor
ted
to p
rovi
de c
omm
unity
set
tings
for
serv
ice
prov
isio
n.
Rep
rese
ntat
ives
fro
m t
he e
thni
c-sp
ecifi
c gr
oups
app
oint
edto
the
Let’s
Bea
t D
iabe
tes
Gov
erna
nce
Gro
up.
The
eth
nic-
spec
ific
lead
ersh
ip g
roup
s, s
uppo
rted
by
the
heal
th p
rom
otio
nse
ctor
, cha
mpi
on, p
rom
ote
and
enco
urag
e he
alth
y ea
ting
and
phys
ical
act
ivity
to th
eir
vario
us c
omm
unity
grou
ps a
nd o
rgan
isat
ions
. K
eygr
oups
incl
ude:
Chu
rche
s an
dch
urch
gro
ups
H
omes
E
arly
chi
ldho
od c
entr
es a
ndpr
e-sc
hool
s
Wor
kpla
ces
V
illag
em
eetin
gs
Ex-
Stu
dent
sA
ssoc
iatio
ns
Pac
ific
com
mun
ities
, C
MD
HB
, et
hnic
-sp
ecifi
c le
ader
ship
gr
oups
,he
alth
prom
otio
n se
ctor
25F
INA
L P
LA
N 0
2 F
ebru
ary
2005

Go
al:
Par
tner
ship
s &
Co
llab
ora
tio
n
Pac
ific
co
mm
un
itie
s, t
he
hea
lth
sec
tor
and
oth
er
key
agen
cies
wo
rk
effe
ctiv
ely
tog
eth
erto
p
rom
ote
and
su
pp
ort
h
ealt
han
dw
ellb
ein
g t
o P
acif
ic c
om
mu
nit
ies.
Tar
get
:L
et’s
Bea
t D
iab
etes
pla
n a
lign
sw
ith
th
e H
ealt
hy
Cit
y C
har
ter
Spe
cific
dia
bete
spr
even
tion
obje
ctiv
es i
nclu
ded
as p
art
of t
he T
omor
row
’sM
anuk
au T
e O
ra O
Man
ukau
/Man
ukau
the
Hea
lthy
City
Out
com
e G
roup
revi
ewof
the
Hea
lthy
Citi
es C
hart
er.
Ann
ual a
ctio
npl
ans
deve
lope
dw
hich
foc
us o
n di
abet
es a
nd h
ow e
very
heal
thpr
ovid
erw
ill e
ndor
se a
nd im
plem
ent t
he id
entif
ied
actio
ns.
Dat
abas
e of
all
prov
ider
s an
d gr
oups
wor
king
in t
he d
iabe
tes
field
acc
essi
ble
to c
omm
unity
gro
ups
as a
mea
nsof
net
wor
king
and
deve
lopi
ngw
orki
ngpa
rtne
rshi
ps.
Pac
ific
prov
ider
s an
d pa
rtne
rs i
nclu
ded
in w
eb-b
ased
inf
orm
atio
n lin
ked
to
Let’s
Bea
t Dia
bete
s w
ebsi
te.
Pro
toco
l fo
r in
form
atio
n sh
arin
g de
velo
ped
to e
nsur
e th
at b
oth
prim
ary
and
seco
ndar
y ca
re p
rovi
ders
hav
eac
cess
to r
elev
ant i
nfor
mat
ion.
Pac
ific
chur
ches
and
hea
lthpr
omot
ion
expl
ore
oppo
rtun
ities
to
wor
k to
geth
erto
pr
omot
e an
d de
liver
he
alth
an
d ph
ysic
al
activ
ity
prog
ram
mes
to
th
eco
mm
uniti
es, w
ith th
e vi
ew to
bec
omin
ga
key
setti
ng fo
r se
rvic
e pr
ovis
ion.
Tom
orro
w’s
Man
ukau
T
e O
ra
O
Man
ukau
/Man
ukau
th
e H
ealth
y C
ityO
utco
me
Gro
up, C
MD
HB
, pro
vide
rs
Go
al:
Ed
uca
tio
n &
Em
pow
erm
ent
Pac
ific
co
mm
un
itie
s ar
e kn
ow
led
gea
ble
and
in
form
ed
abo
ut
dia
bet
es,
its
risk
fact
ors
, h
ow
to
p
reve
nt
it,
and
h
ow
tom
anag
e it
.
Tar
get
: B
y20
08 a
mea
sura
ble
incr
ease
inp
reve
nti
on
kn
ow
led
ge
in c
hild
ren
, ad
ult
san
d o
lder
ad
ult
s.
Com
mun
ity-w
ide,
cul
tura
llyap
prop
riate
dia
bete
saw
aren
ess
and
educ
atio
npr
ogra
mm
es fa
cilit
ated
com
mun
ityw
ide.
Chu
rche
s an
dch
urch
gro
ups
H
omes
P
re-s
choo
ls a
nd e
arly
chi
ldho
od c
entr
es
W
orkp
lace
s
Vill
age
mee
tings
E
x-S
tude
nts
Ass
ocia
tions
Eth
nic-
spec
ific
spok
espe
rson
sw
ork
with
th
e he
alth
pr
omot
ion
sect
or
and
Auc
klan
d P
ublic
Hea
lth R
esou
rce
Ser
vice
(A
RP
HS
) to
edu
cate
and
inf
orm
Hea
lth
prom
otio
n se
ctor
, et
hnic
-sp
ecifi
c sp
okes
pers
ons,
he
alth
prom
otio
n se
ctor
, A
RP
HS
, M
inis
try
ofP
acifi
c Is
land
s A
ffairs
(M
PIA
), M
inis
try
of H
ealth
(M
oH),
Chu
rche
s, C
MD
HB
,he
alth
pro
vide
rs
26F
INA
L P
LA
N 0
2 F
ebru
ary
2005
Pac
ific
com
mun
ities
on
diab
etes
and
on
a re
gula
r ba
sis
via
Pac
ific
radi
o an
d ne
wsp
aper
s.
Pos
itive
diab
etes
rol
e m
odel
s an
d st
orie
s ar
e co
llate
d an
ddi
strib
uted
aspa
rtof
edu
catio
n an
d em
pow
erm
ent.
Dia
bete
san
d di
abet
es-r
elat
edin
form
atio
n re
view
ed a
nd t
rans
late
din
toth
edi
ffere
nt P
acifi
c la
ngua
ges,
and
dis
trib
uted
thro
ugh
Pac
ific
netw
orks
Eth
nic-
spec
ific
guid
elin
es
for
man
agin
g di
abet
es
for
Pac
ific
peop
les
deve
lope
d. T
hey
incl
ude:
A d
iabe
tes
focu
sed
clin
ic
Hea
lthpr
omot
ion
T
rain
ing
man
uals
Rec
ogni
sed
trai
ning
pro
vide
rs
Pac
ific
chur
ches
and
hea
lthpr
omot
ion
expl
ore
oppo
rtun
ities
to
wor
k to
geth
erto
pr
omot
e an
d de
liver
he
alth
an
d ph
ysic
al
activ
ity
prog
ram
mes
to
th
eco
mm
uniti
es, w
ith th
e vi
ew to
bec
omin
ga
key
setti
ng fo
r se
rvic
e pr
ovis
ion.
Go
al:
Hea
lth
y,A
ctiv
eC
om
mu
nit
ies
Pac
ific
co
mm
un
itie
s ar
e h
ealt
hy,
ac
tive
and
vib
ran
tco
mm
un
itie
s.
Tar
get
: B
y 20
08 a
mea
sura
ble
in
crea
sein
hea
lth
yea
tin
g
and
ac
tive
lif
esty
les
by
Pac
ific
peo
ple
s in
Co
un
ties
Man
uka
u.
Pac
ific
com
mun
ityor
gani
satio
ns a
nd g
roup
sw
ork
with
AR
PH
S to
dev
elop
and
impl
emen
t cu
ltura
llyap
prop
riate
nut
ritio
ngu
idel
ines
tha
t pr
omot
e an
d su
ppor
the
alth
yea
ting.
The
se o
rgan
isat
ions
and
gro
ups
incl
ude:
Chu
rche
s an
dch
urch
gro
ups
H
omes
P
re-s
choo
l and
ear
ly c
hild
hood
edu
catio
n ce
ntre
s
Wor
kpla
ces
V
illag
em
eetin
gs
Ex-
Stu
dent
sA
ssoc
iatio
ns
Com
mun
ity o
rgan
isat
ions
and
grou
ps s
uppo
rted
by
heal
thpr
omot
ion
sect
or t
ode
velo
p an
dim
plem
ent
phys
ical
activ
itypr
ogra
mm
es
that
ar
e cu
ltura
llyap
prop
riate
and
age
-spe
cific
.
AR
PH
S,
Pac
ific
com
mun
ities
, he
alth
prom
otio
n se
ctor
Go
al:
Wo
rkfo
rce
Dev
elo
pm
ent
‘By
Pac
ific
fo
r P
acif
ic’
wo
rkfo
rce
dev
elo
pm
ent.
Pac
ific
co
mm
un
itie
s an
dC
MD
HB
sup
port
s an
d re
sour
ces
the
deve
lopm
ent
and
ongo
ing
deve
lopm
ent
of q
ualif
ied
Pac
ific
wor
kers
in
the
diab
etes
fie
ld,
incl
udin
g nu
rses
, do
ctor
s,C
MD
HB
, pro
vide
rs, M
anuk
au In
stitu
te
of T
echn
olog
y(M
IT)
27F
INA
L P
LA
N 0
2 F
ebru
ary
2005
CM
DH
Bw
ork
to
in
crea
se t
he
nu
mb
er o
f q
ual
ifie
dw
ork
ers
in t
he
dia
bet
es f
ield
tod
eliv
er t
o P
acif
ic c
om
mu
nit
ies.
Tar
get
:
Th
e n
um
ber
o
f P
acif
ic
nu
rses
,d
oct
ors
and
com
mu
nit
y w
ork
ers
wo
rkin
gin
Co
un
ties
Man
uka
u d
ou
ble
s b
y 20
10.
diet
icia
ns, c
omm
unity
wor
kers
and
oth
er n
eces
sary
prof
essi
ons.
Go
al:
Eva
luat
ion
Eva
luat
ion
id
enti
fies
su
cces
sfu
l st
rate
gie
san
d
sup
po
rts
a le
arn
ing
fr
amew
ork
th
atsu
pp
ort
s fu
nct
ion
alan
d
effe
ctiv
ep
artn
ersh
ips
and
act
ivit
ies.
Tar
get
: E
valu
atio
n f
ram
ewo
rk s
et u
pb
yJu
ly 2
005
Pac
ific
com
mun
ities
, M
anuk
au C
ity C
ounc
il(M
CC
) an
d C
MD
HB
wor
kw
ith t
heS
choo
l of
Pop
ulat
ion
Hea
lth(U
oA–S
oPH
) to
dev
elop
a fr
amew
ork
for
proc
ess
and
outc
omes
eva
luat
ion
of t
he a
gree
dac
tion
plan
s,w
ith t
he k
ey o
bjec
tive
bein
g to
sup
port
a le
arni
ng fr
amew
ork
and
effe
ctiv
e su
stai
nabl
e pa
rtne
rshi
ps.
Pac
ific
com
mun
ities
, M
CC
, C
MD
HB
,U
oA-S
oPH
Th
e W
ork
pla
ce
Hea
lth
y, A
ctiv
e W
ork
pla
ces.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
ers
Go
al:
Par
tner
ship
s
To
mo
rro
w’s
M
anu
kau
/Te
Ora
OM
anu
kau
/Man
uka
u
the
Hea
lth
yC
ity
Ou
tco
me
Gro
up
, w
ith
sup
po
rt
fro
mC
MD
HB
an
d
AR
PH
Sw
ork
effe
ctiv
ely
tog
eth
er t
o a
dvo
cate
for
init
iati
ves
wit
hin
thei
r o
wn
wo
rkp
lace
s th
at
pro
mo
te
and
sup
po
rt h
ealt
hy,
act
ive
lifes
tyle
s.
Tar
get
: B
yD
ecem
ber
2004
su
pp
ort
in
pri
nci
ple
fr
om
T
om
orr
ow
’s
Man
uka
u/T
eO
ra O
Man
uka
u/M
anu
kau
th
e H
ealt
hy
Cit
yO
utc
om
e G
rou
p.
Tom
orro
w’s
Man
ukau
T
e O
ra
O
Man
ukau
/Man
ukau
th
e H
ealth
y C
ityO
utco
me
Gro
up a
nd A
RP
HS
form
ally
agr
eeto
wor
k to
geth
er t
o ad
voca
tefo
rin
itiat
ives
with
in th
eir
own
wor
kpla
ce th
at p
rom
ote
and
supp
ort h
ealth
y, a
ctiv
elif
esty
les.
Tom
orro
w’s
Man
ukau
/Te
Ora
O
M
anuk
au/M
anuk
au
the
Hea
lthy
City
Out
com
e G
roup
, CM
DH
B, A
RP
HS
28F
INA
L P
LA
N 0
2 F
ebru
ary
2005

29F
INA
L P
LA
N 0
2 F
ebru
ary
2005
Go
al:
Hea
lth
y, A
ctiv
e W
ork
pla
ces
To
mo
rro
w’s
M
anu
kau
/Te
Ora
O
M
anu
kau
/Man
uka
u
the
Hea
lth
y C
ity
Ou
tco
me
Gro
up
m
emb
ers
imp
lem
ent
init
iati
ves
wit
hin
th
e w
ork
pla
ce
that
p
rom
ote
an
d
sup
po
rt
hea
lth
y,
acti
ve
lifes
tyle
s.
Tar
get
: B
y Ju
ly 2
005
form
al a
gre
emen
t b
y in
div
idu
al
mem
ber
s o
f T
om
orr
ow
’s
Man
uka
u/T
e O
ra O
Man
uka
u/M
anu
kau
th
e H
ealt
hy
Cit
y to
in
tro
du
ce
hea
lth
y w
ork
pla
ce
po
licie
s,
wh
ere
they
d
o
no
t al
read
y ex
ist.
Tom
orro
w’s
M
anuk
au/T
e O
ra
O
Man
ukau
/Man
ukau
th
e H
ealth
y C
ity
Out
com
e G
roup
, with
sup
port
from
CM
DH
B a
nd A
RP
HS
wor
k to
geth
er to
in
trod
uce
initi
ativ
es w
ithin
thei
r ow
n w
orkp
lace
s th
at p
rom
ote
and
supp
ort
heal
thy,
act
ive
lifes
tyle
s.
Thi
s in
itiat
ive
is r
olle
d ou
t to
sim
ilar
inte
rsec
tora
l w
orki
ng g
roup
s in
the
P
apak
ura
and
Fra
nklin
Dis
tric
ts,
and
all
cent
ral
and
loca
l go
vern
men
t ag
enci
es in
Cou
ntie
s M
anuk
au.
In c
olla
bora
tion
with
the
Foo
d in
dust
ry A
ccor
d A
ctio
n A
rea,
the
foo
d in
dust
ry i
s en
cour
aged
and
sup
port
ed t
o in
trod
uce
heal
thy
eatin
g ac
tive
livin
g po
licie
s in
to it
s w
orkp
lace
s.
Tom
orro
w’s
M
anuk
au
Te
Ora
O
M
anuk
au/M
anuk
au
the
Hea
lthy
City
O
utco
me
Gro
up, A
RP
HS
Go
al:
Eva
luat
ion
Eva
luat
ion
o
f th
e ac
tivi
ty
will
b
e u
nd
erta
ken
w
ith
th
e o
bje
ctiv
e o
f id
enti
fyin
g
succ
essf
ul
hea
lth
y w
ork
pla
ce
pra
ctic
es a
nd
su
pp
ort
ing
lea
rnin
g a
cro
ss
org
anis
atio
ns.
Tar
get
:
By
July
20
05
an
eval
uat
ion
fr
amew
ork
is
in p
lace
wh
ich
will
su
pp
ort
p
roce
ss a
nd
ou
tco
me
eval
uat
ion
.
Tom
orro
w’s
M
anuk
au/T
e O
ra
O
Man
ukau
/Man
ukau
th
e H
ealth
y C
ity
Out
com
e G
roup
, C
MD
HB
an
d A
PH
RS
, w
orks
w
ith
the
Uni
vers
ity
of
Auc
klan
d S
choo
l of
P
opul
atio
n H
ealth
(U
oA
– S
oPH
) to
de
velo
p a
fram
ewor
k fo
r pr
oces
s an
d ou
tcom
es e
valu
atio
n of
the
agr
eed
actio
n pl
ans,
with
the
obje
ctiv
e of
sup
port
a le
arni
ng fr
amew
ork
and
an e
ffect
ive
sust
aina
ble
part
ners
hip.
Tom
orro
w’s
M
anuk
au/T
e O
ra
O
Man
ukau
/Man
ukau
th
e H
ealth
y C
ity
Out
com
e G
roup
, C
MD
HB
, A
RP
HS
, U
oA-
SoP
H
2. Promoting Behaviour Change Through Social
Marketing
Context
Beating obesity and diabetes will require a change in norms – of government, industry,community, family and individuals. Changing norms means changing environmentsand behaviour. The scale of change required will not occur without a substantialinvestment in the information and knowledge environment for all people in Counties Manukau.
Effective social marketing involves consistent messages reinforced in different waysand received from multiple trusted sources. In Counties Manukau that could meanmessages from sources such as kaumatua, church leaders, doctors, health workers, the local council and the media. The changes being promoted must also be relevant,practical, and achievable and deliver value when accomplished.
New Zealand experience shows that well constructed social marketing programmes are an effective and critical part of broad public health programmes. Examples includethe stop smoking campaigns, seatbelts, drink driving, and mental healthdestigmatisation. However, the obesity and diabetes message is far more complexthan these examples, and the difficulties are amplified by those most at risk being hard to reach through traditional social marketing avenues. The social marketing strategyfor Let’s Beat Diabetes will need to recognise these complexities and need to have suitable messages for different audiences and communities of interest. Ongoingevaluation of social marketing is required to assess whether it is being effective in changing knowledge, attitudes and behaviour.
A number of organisations have indicated their interest in supporting a broader social marketing strategy, including Manukau City Council (MCC) and the Food Group. Thereare also existing social marketing programmes by Sport and Recreation New Zealand(SPARC), the Heart Foundation and the Auckland Regional Public Health Service (ARPHS) which support healthy eating and/or active living. A marketing strategy tosupport the national Healthy Eating Healthy Action Framework is also being developed.It is prudent that Counties Manukau’s Let’s Beat Diabetes plan’s social marketingprogramme aligns with existing programmes.
Marketing is not just about selling an idea or service, effective marketing is based ondeveloping an intimate understanding of and relationship with, the customer so that thedesign of products and services meet customer needs and wants – and deliver value.
Programme Design
The social marketing programme design has a number of components to it:
1. The branding: The publicising and positioning the Let’s Beat Diabetes plan itself.The plan must develop a profile and be understood by community and health sectorleaders. We can not expect a broader audience to understand the detail of theplan, but the core concepts and key action strands should be known. The plan also needs to develop an emotional response and to represent hope and the ‘can-do’ Counties Manukau attitude. In response to these needs, it is proposed to develop an identity and profile for the plan that resonates with the Counties Manukaucommunity.
30 FINAL PLAN 02 February 2005

31 FINAL PLAN 02 February 2005
2. The social marketing programme: A comprehensive and integrated programme that runs for five years with the objective of changing knowledge, attitudes and behaviour towards nutrition and physical activity.
The plan will require support from market research to better understand the profile and issues for the Counties Manukau population. A professionally designed and executed marketing/information strategy will developed with alignment to activity by Health Promotion, Primary Care-based Prevention, Schools, Well Child and support from other sectors such as industry and local government.
A programme of evaluation is required to identify the impact of the strategy and provide direction for future developments.
The social marketing strategy must also fulfil the function of understanding the needs and wants of the people of Counties Manukau so that substantive issues such as health service design and access can be based on what the people want. This feedback process will guide service developments across all action areas of the Let’s Beat Diabetes plan.

FIN
AL
PL
AN
02
Feb
ruar
y 20
05
Act
ion
Pla
n
A w
ho
le s
yste
m c
om
mu
nic
atio
ns
pro
gra
mm
e ch
ang
es p
eop
le’s
beh
avio
ur.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
er
Go
al:
Th
eL
et’s
B
eat
Dia
bet
es
pla
nb
eco
mes
a m
oti
vati
on
al c
all
to a
ctio
n f
or
com
mu
nit
ies
and
o
rgan
isat
ion
sin
Co
un
ties
Man
uka
u.
Tar
get
: F
ebru
ary
– Ju
ly20
05 t
he
pla
n i
s m
arke
ted
acr
oss
ou
r co
mm
un
itie
s.
An
iden
tity
and
mar
ketin
g pl
an
for
the
Let’s
Bea
t D
iabe
tes
plan
its
elf
is
deve
lope
d an
d im
plem
ente
d.
Sum
mar
y ve
rsio
nsof
the
pla
n ar
ede
velo
ped
and
dist
ribut
ed,
alon
g w
ithpr
esen
tatio
nsan
d su
ppor
tive
med
ia
to
deve
lop
good
unde
rsta
ndin
g an
dsu
ppor
t fo
r th
e pl
an f
rom
lea
ders
ins
ide
Cou
ntie
s M
anuk
au a
nd a
t a
natio
nal
leve
l.
The
pla
n id
entit
y an
dpr
esen
tatio
n m
ust
be r
elev
ant
to a
nd m
otiv
atio
nal
for
Mao
ri an
d P
acifi
c pe
ople
s.
Cou
ntie
s M
anuk
au
Dis
tric
t H
ealth
Boa
rd (
CM
DH
B)
Go
al:
Aw
ell
dev
elo
ped
so
cial
mar
keti
ng
stra
teg
y is
su
stai
ned
ove
r fi
veye
ars
and
inte
gra
ted
wit
h w
ider
pla
no
bje
ctiv
es.
Kn
ow
led
ge,
at
titu
des
and
b
ehav
iou
rch
ang
es
as
a re
sult
o
f a
five
-yea
rco
mp
reh
ensi
ve
soci
al
mar
keti
ng
pro
gra
mm
e.
The
go
vern
ance
gr
oup
deve
lops
a
com
mer
cial
re
latio
nshi
pw
ithsu
rvey
/eva
luat
ion
and
com
mun
icat
ion
prof
essi
onal
s to
de
vise
,de
velo
p,im
plem
ent a
nd e
valu
ate
a co
mpr
ehen
sive
five
-yea
r so
cial
mar
ketin
g st
rate
gy.
Tar
get
s:
S
eco
nd
h
alf
2005
th
e m
edia
asp
ect
of
the
soci
al m
arke
tin
g p
rog
ram
me
beg
ins.
Mea
sura
ble
ch
ang
e in
kn
ow
led
ge
atti
tud
es a
nd
beh
avio
ur
(act
ual
mea
sure
sye
t to
be
dev
elo
ped
).
A g
over
nanc
egr
oup
is s
et u
p to
gui
de t
he d
evel
opm
ent
of a
soc
ial m
arke
ting
prog
ram
me
that
is
lin
ked
with
th
e br
oade
r st
rate
gies
of
th
e Le
t’s
Bea
tD
iabe
tes
plan
,is
res
pons
ive
to n
eeds
of
Mao
ri an
d P
acifi
c pe
ople
san
d al
igns
with
the
natio
nalH
ealth
y E
atin
g H
ealth
y A
ctio
n st
rate
gies
.
The
str
ateg
y in
clud
es th
e fo
llow
ing
com
pone
nts:
Sur
veys
to
crea
te a
bas
elin
e an
d to
inf
orm
the
dev
elop
men
t of
a f
ive
year
soc
ial m
arke
ting
stra
tegy
.
Str
ateg
y im
plem
ente
dw
ithsu
ppor
t fr
om
mul
tiple
or
gani
satio
ns
and
whi
ch is
inte
grat
edw
ith o
ther
com
pone
nts
of th
e br
oade
r pl
an.
Ong
oing
eval
uatio
n un
dert
aken
to
in
form
an
d im
prov
e pr
ogra
mm
ede
sign
.
CM
DH
B,
MC
C,
Min
istr
yof
H
ealth
(MoH
),
SP
AR
C,
PH
AR
MA
C,
Foo
d gr
oup,
P
rimar
y H
ealth
O
rgan
isat
ions
(PH
Os)
, N
on-G
over
nmen
tO
rgan
isat
ions
(N
GO
s)
Go
al:
H
ealt
h
serv
ices
im
pro
ve
thei
rp
erfo
rman
ce
thro
ug
h
hav
ing
b
ette
rkn
ow
led
ge
of
pat
ien
t n
eed
s an
d is
sues
.
Tar
get
:
By
Oct
ob
er20
06
init
ial
surv
eyco
mp
lete
d.
Sur
vey
on s
ocia
l mar
ketin
g is
sues
als
o se
ek a
n un
ders
tand
ing
of w
ider
heal
thse
rvic
e is
sues
and
are
used
to
info
rm d
ecis
ions
on
serv
ice
desi
gnac
ross
the
Ten
Act
ion
area
s of
the
Let’s
Bea
t Dia
bete
s pl
an.
Soc
ial m
arke
ting
prov
ider
, CM
DH
B
32

3. Changing Urban Design to Support Healthy, Active
Lifestyles
Context
Urban design influences the physical environment (such as road and parks), the service environment (such as shops and public transport) and the social environment (such as social cohesion and community safety) (Kawachi I, 2003). Urban environments also impact on ourlifestyle choices and decisions, and subsequently our health and risk of disease. A key issue for the health sector is to ensure urban design in Counties Manukau encourages and supports physical activity, and provides access to medical facilities.
In recent decades, the predominant urban residential design globally, as well as in Counties Manukau has been towards suburban, car-based living. This suburban lifestyle brought largersections and low density living which has been considered desirable. There have also beendownsides with traffic jams, social isolation, poor public transport, community safety concerns,poor access to many service amenities (except by car) and less opportunity for daily physical activity.
There is good evidence to show that good urban design can increase physical activity.Germany and the Netherlands have implemented a wide range of policies over the past two decades that have simultaneously encouraged walking and cycling while dramatically loweringpedestrian and bicyclist fatalities and injuries and keeping auto use at only half the Americanlevel (Pucher J, 2003). Urban environments also impact on community life, which influencesperceptions of safety, leading to concerns over children walking to school or walking andjogging for exercise.
Changing urban design is difficult because of the expensive and permanent nature of basic infrastructure. It is also very slow.
A number of initiatives are already under way. Manukau City Council (MCC) and otherstakeholders are supportive of the priorities identified in the Auckland Regional Growth Strategy and the Urban Design Protocols which will address active transport provision, injury preventionmeasures and availability of public transport in city and urban design. Healthy urban designconcepts also encourage ‘liveable cities that support social wellbeing, quality of life and culturalidentities’, which is one of the key government outcomes in the sustainable cities component of the national Sustainable Development Programme of Action. Manukau City along withInfrastructure Auckland has invested in the development of cycle-ways across the district aspart of the cycling/walking strategy.
Programme Design
MCC is demonstrating healthy urban design concepts in the Flat Bush development. Flat Bush will be a new town of more than 40,000 people. The development will not be another sprawling suburb, but is being designed to be a ‘town’, with a town centre, extensive parkland, cycleways, local shopping centres and green fingers of protected stream-ways running through theresidential areas. MCC also intends to introduce urban design concepts that support moreactive, connected and healthy communities as it redevelops the various urban hubs and town centres in the district. Introducing these new concepts in the urban hubs represents new
33 FINAL PLAN 02 February 2005

34 FINAL PLAN 02 February 2005
design priorities for MCC and reflects their commitments to healthy city and sustainable city ideals.
CMDHB and Auckland Regional Public Health Service (ARPHS) will work in partnership with MCC, providing health advice and expertise, where required for urban design planning.

Act
ion
Pla
n
Th
e u
rban
en
viro
nm
ent
in C
ou
nti
esM
anu
kau
su
pp
ort
s in
crea
sed
ph
ysic
al a
ctiv
ity
leve
lsan
d im
pro
ved
so
cial
co
hes
ion
.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
er
Go
al:
S
ust
ain
able
ap
pro
ach
es
to
sup
po
rtin
gh
ealt
hy
urb
an
des
ign
ar
e d
evel
op
ed
and
imp
lem
ente
d
in
par
tner
ship
wit
h
Man
uka
u
Cit
yC
ou
nci
l (M
CC
), P
apak
ura
Dis
tric
t C
ou
nci
l (P
DC
) an
d F
ran
klin
Dis
trci
t C
ou
nci
l (F
DC
).
Tar
get
:
By
2005
C
MD
HB
an
d
MC
C
sig
n
the
Min
istr
y fo
r th
e E
nvi
ron
men
t sp
on
sore
d
Urb
anD
esig
n p
roto
col,
wh
ich
is
a co
mp
on
ent
of
the
Su
stai
nab
le C
itie
s n
atio
nal
stra
teg
ic in
itia
tive
.
MC
C a
ndC
MD
HB
sig
n th
eM
inis
try
for
the
Env
ironm
ent
spon
sore
dur
ban
desi
gn p
roto
col,
whi
ch i
s co
mpo
nent
of
the
Sus
tain
able
Citi
esin
itiat
ive.
CM
DH
B s
uppo
rts
MC
C,
FD
C a
ndP
DC
in
anal
ysis
and
plan
ning
proc
esse
s to
im
plem
ent
urba
n de
sign
whi
ch
prom
otes
he
alth
ylif
esty
les
and
acce
ssib
le h
ealth
ser
vice
s.
MC
C, C
MD
HB
, AR
PH
S, P
DC
, FD
C
Go
al:
F
lat
Bu
sh
dev
elo
pm
ent
wit
h
imp
rove
dh
ealt
hy
des
ign
co
nce
pts
co
ntr
ibu
tes
to i
ncr
ease
dp
hys
ical
act
ivit
y o
f re
sid
ents
.
Tar
get
E
nh
ance
d
safe
wal
kin
g
and
cy
clin
go
pp
ort
un
itie
s ar
e in
tro
du
ced
in
to
Fla
t B
ush
dev
elo
pm
ent.
MC
C d
evel
ops
over
all d
esig
nco
ncep
ts a
nd p
rovi
des
publ
icam
eniti
esw
hich
sup
port
hea
lthy
urba
nde
sign
in F
latB
ush.
MC
C d
evel
ops
spec
ifica
tions
for
priv
ate
deve
lope
rsw
hich
ensu
reth
at t
he h
ealth
y ur
ban
desi
gn c
once
pts
are
take
n up
in
com
mer
cial
deve
lopm
ents
thro
ugho
ut th
e F
lat B
ush
area
.
CM
DH
B
prov
ides
M
CC
, P
DC
an
d F
DC
with
a re
view
of
the
inte
rnat
iona
l lite
ratu
re a
s it
rela
tes
to h
ealth
yur
ban
envi
ronm
ents
.
CM
DH
Bw
orks
with
MC
C t
o de
velo
pa
plan
for
the
hea
lth f
acili
tyan
dse
rvic
e in
fras
truc
ture
for
the
Fla
t Bus
h de
velo
pmen
t.
MC
C, A
RP
HS
, CM
DH
B, P
DC
, FD
C
Go
al:
In
crea
sed
p
hys
ical
ac
tivi
ty
leve
ls
and
soci
al
coh
esio
n
are
sup
po
rted
by
the
red
evel
op
men
t o
f ex
isti
ng
urb
an h
ub
s an
d t
ow
nce
ntr
es.
Tar
get
: D
etai
led
rev
iew
an
d r
edev
elo
pm
ent
pla
ns
for
at
leas
to
ne
urb
an
hu
b
in
a lo
w
soci
o-
As
Cou
ncils
unde
rtak
e re
deve
lopm
ent
activ
ities
for
exi
stin
g ur
ban
infr
astr
uctu
re,
the
appr
oach
will
be g
uide
d by
new
prio
ritie
sfo
r ur
ban
desi
gns
whi
ch in
crea
se p
hysi
cal a
ctiv
ityan
d so
cial
coh
esio
n.
CM
DH
Bw
ill a
dvoc
ate
to M
CC
, P
DC
and
FD
C o
n a
case
by
case
basi
s to
pro
vide
evi
denc
e an
d an
alys
is th
at w
ill s
uppo
rthe
alth
yur
ban
desi
gn,
whi
chin
clud
es a
dequ
ate
and
acce
ssib
le c
omm
unity
hea
lth
MC
C, F
DC
, PD
C, C
MD
HB
, AR
PH
S
35F
INA
L P
LA
N 0
2 F
ebru
ary
2005

36F
INA
L P
LA
N 0
2 F
ebru
ary
2005
eco
no
mic
are
a.
faci
litie
s,
publ
ic
open
sp
ace
and
com
mun
ity
faci
litie
s,
safe
ty
and
incr
ease
d op
port
uniti
es fo
r ph
ysic
al a
ctiv
ity.
Go
al:
MC
C a
nd
CM
DH
B s
up
po
rt h
ealt
hy
urb
an
des
ign
th
rou
gh
p
lan
nin
g,
imp
lem
enta
tio
n
and
ev
alu
atio
n
par
tner
ship
s in
F
lat
Bu
sh
dev
elo
pm
ent.
Tar
get
:
By
July
20
05
ther
e is
ag
reem
ent
for
eval
uat
ion
fo
r th
e F
lat
Bu
sh d
evel
op
men
t w
ith
th
e U
niv
ersi
ty
of
Au
ckla
nd
S
cho
ol
of
Po
pu
lati
on
H
ealt
h (
Uo
A-S
oP
H)
CM
DH
B,
MC
C a
nd t
he U
nive
rsity
of
Auc
klan
d S
choo
l of
Pop
ulat
ion
Hea
lth (
UoA
–SoP
H)
wor
k to
dev
elop
an
eval
uatio
n fr
amew
ork
for
the
Fla
t Bus
h de
velo
pmen
t and
ong
oing
urb
an r
edes
ign
initi
ativ
es.
MC
C,
FD
C,
PD
C,
CM
DH
B,
AR
PH
S,
UoA
S
oPH

4. Supporting a Healthy Environment Through a Food
Industry Accord
Context
Changes to the food environment have been a major contributor to the current obesity epidemic (Critser G, 2003) The food environment during pregnancy, childhood, adolescence and adult life all contributes to health and can cause disease. The food environment also amplifies the issues of disparity in diabetes rates in our society. Generally, people who have high incomes eat food that is higher in nutrients and lower in fats and carbohydrates. People who have low incomes tend to eat low-cost high-fat/high-sugar/high-salt take-away foods more often than is considered ‘healthy’. Children from families with lower incomes are also less likely to eat a proper breakfast at home and a nutritious lunch at school (FAO/WHO Expert Consultation,2003; Barnfather D, 2004; Ministry of Health, 2003).
The current ‘obesogenic’ food environment is a global issue, with governments from manycountries and international agencies like the World Health Organisation looking at how to makechanges to protect populations from poor diets. Strategies being investigated includeregulation of aspects of food industry behaviour and more collaborative approaches with industry seeking voluntary changes to commercial behaviour.
Industry itself has identified that its customers are seeking healthier food and that there is an obligation for responsible corporates to work with health agencies to develop an overall healthier food environment to reduce population obesity and subsequent disease.
Representatives of major food producers and retailers in New Zealand signed the Food Industry Accord in September 2004, which commits the signatories to supporting the Ministry ofHealth’s Healthy Eating Healthy Action Framework, and recommends that a pilot of theAccord’s activities is instigated in the Auckland Region (New Zealand Food Industry Accord2004). Counties Manukau Distrcit Health Board (CMDHB) and representatives of the foodindustry have agreed to collaborate to undertake a ‘demonstration pilot’ of the Food Industry Accord in Counties Manukau.
Programme Design
The Counties Manukau food industry ‘demonstration pilot’ represents a number of major foodorganisations working together with the health sector for a common health objective.
The initial component of programme design is to develop a set of trusting and functionalrelationships, which acknowledge the unique nature of the collaboration and identify ways to deliver real improvements to the food environment.
A collaborative working group will be set up which includes representatives from industry,CMDHB, the Auckland Regional Public Health Service (ARPHS) and Manukau City Council (MCC) in the first instance. Others groups may join at a later date.
The food industry has identified a number of Action Areas it is interested in supporting, namely: Community Leadership and Action; Social Marketing; Food Accord; Schools; and VulnerableFamilies
37 FINAL PLAN 02 February 2005
38 FINAL PLAN 02 February 2005
Specific practical activities will be developed in each of these areas. As the relationships and programmes mature, it would be expected that a wider range of food industry partners would join the collaborative group.
It is proposed that the food industry group be represented on the wider governance group for the Let’s Beat Diabetes plan.
Evaluation of the strategies will need to be undertaken for process and outcomes to ensure that all parties are informed of performance and value issues associated with the collaboration. The objective is to develop a learning environment which supports continuous quality improvement methodology and measures the effectiveness of this new partnership.

FIN
AL
PL
AN
02
Feb
ruar
y 20
05
Act
ion
Pla
n
Th
e fo
od
en
viro
nm
ent
in C
ou
nti
es M
anu
kau
ch
ang
es t
o in
crea
se h
ealt
hy
foo
d a
vaila
bili
ty a
nd
co
nsu
mp
tio
np
arti
cula
rly
for
fam
ilies
wit
h lo
w in
com
es a
nd
hig
h r
isk
of
dia
bet
es.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
er
Go
al:
Th
e fo
od
in
du
stry
an
d c
om
mu
nit
ies
of
inte
rest
wo
rk e
ffec
tive
ly t
og
eth
er t
o d
esig
n a
nd
del
iver
ob
esit
y-re
du
cin
g s
trat
egie
s.
Tar
get
: B
y 20
07 t
he
Fo
od
Gro
up
will
hav
e sh
ow
nth
at e
ffec
tive
co
llab
ora
tive
act
ivit
ies
can
occ
ur
and
oth
er D
istr
ict
Hea
lth
Bo
ard
sw
ill s
eek
to j
oin
the
Fo
od
Ind
ust
ryA
cco
rd in
itia
tive
s.
CM
DH
B,
AR
PH
S,
MC
C a
ndth
e F
ood
Gro
up f
orm
aw
orki
nggr
oup
that
will
lea
dth
e ‘F
ood
Indu
stry
’ act
ivity
are
a of
the
Let’s
Bea
t Dia
bete
spl
an.
Foo
d in
dust
ryre
pres
enta
tion
is i
nclu
ded
on t
heLe
t’s B
eat
Dia
bete
s G
over
nanc
eG
roup
.
CM
DH
B, F
ood
Gro
up, A
RP
HS
, MC
C
Go
al:
Th
e av
erag
e p
er c
apit
a en
erg
y in
take
of
the
Co
un
ties
Man
uka
u p
op
ula
tio
nd
ecre
ases
as
a re
sult
of
the
Fo
od
Ind
ust
ryA
cco
rd in
itia
tive
s.
Tar
get
: B
yJu
ly 2
005
spec
ific
str
ateg
ies
to b
ed
evel
op
ed i
n e
ach
of
the
five
id
enti
fied
act
ion
area
s (t
arg
et t
o b
e u
pd
ated
at t
hat
sta
ge)
.
The
food
wor
king
gro
up im
plem
ents
pra
ctic
al s
trat
egie
s in
the
area
s of
:
C
omm
unity
Lead
ersh
ip
Soc
ialM
arke
ting
F
ood
Acc
ord
S
choo
ls
Vul
nera
ble
Fam
ilies
The
se s
trat
egie
s ar
e to
be
deve
lope
d an
dim
plem
ente
din
a c
olla
bora
tive
man
ner.
At
the
time
of w
ritin
g th
e de
velo
pmen
t of
the
spe
cific
str
ateg
ies
is a
t a
very
early
stag
e an
dw
ill b
e co
mpl
eted
dur
ing
the
first
six
mon
ths
of 2
005.
Foo
d G
roup
, MC
C, C
MD
HB
, AR
PH
S,
Go
al:
E
valu
atio
n
of
the
foo
d
ind
ust
ryre
lati
on
ship
an
d
acti
vity
d
evel
op
s an
den
viro
nm
ent
of
tru
st
and
o
ng
oin
g
evid
ence
-b
ased
ac
tivi
ties
to
im
pro
ve
the
foo
den
viro
nm
ent.
Tar
get
: B
y Ju
ly 2
005
an e
valu
atio
n f
ram
ewo
rk is
in
pla
cew
hic
hw
ill s
up
po
rt p
roce
ssan
d o
utc
om
eev
alu
atio
n.
The
food
wor
king
grou
pw
orks
with
the
Uni
vers
ity o
f Auc
klan
d S
choo
lof P
opul
atio
nH
ealth
(U
oA –
SoP
H)
to d
evel
op a
fra
mew
ork
for
proc
ess
and
outc
ome
eval
uatio
nof
the
agr
eed
actio
n pl
ans
with
the
obj
ectiv
e of
sup
port
ing
a le
arni
ng f
ram
ewor
kan
d an
effe
ctiv
e su
stai
nabl
e re
latio
nshi
p.
CM
DH
B, F
ood
Gro
up, U
oA -
SoP
H
39

5. Strengthening Health Promotion Co-ordination and
Activity
Context
Health promotion in Counties Manukau is a small sector with many providers and multiplefunders. The diversity of providers is a strength, with organisations establishing strong relationships with their local communities to deliver well targeted programmes. Many providers deliver population based services as well as personal health services such as health education.
The health promotion environment is also somewhat fragmented, with low levels ofcommunication between funders leading to poor alignment of funding streams and strategic objectives. Health promotion funders include Ministry of Health (MoH), Counties ManukauDistrict Health Board (CMDHB), Manukau City Council (MCC) and Primary HealthOrganisations (PHOs). Providers operate in an environment where there is often limitedknowledge of each other’s activities and there is not a long term view about capacity development across the sector.
There is a history of broad collaboration associated with Te Ora O Manukau/Manukau theHealth City and more recently the Tomorrow’s Manukau Health and Wellbeing Outcome Group,which provides an umbrella forum for health and social service organisations. At a morespecific level, CODA (Community Organisations working together) has acted as a network forhealth promotion organisations with an interest in diabetes.
Recently PHOs have begun to receive funding for health promotion and the Counties Manukau PHOs have agreed to a charter that will see coordination of health promotion activity acrossPHOs.
Maori and Pacific communities would like to see the strengthening of health promotionproviders and programmes that work within a cultural framework of ‘by Maori for Maori’ and ‘byPacific for Pacific’. The Pacific communities also support ethnic-specific programmes within the broader Pacific community, especially church-based programmes.
The development of effective health promotion programmes for Asian and new settler communities is a challenge given the range of languages, cultures and community structureshealth promoters must work within.
The overall health sector expenditure in health promotion is low despite good evidence from multiple sources that investment in effective health promotion delivers good returns compared to other parts of the health sector.
Programme Design
The programme design is a direct response to the issues raised by health promotion providersand community leaders at a series of workshops, hui and fono held in Counties Manukau. They include:
Funder Alignment: the need to ensure there is communication and strategic alignment between funders as it applies to programme priorities and design, and also to long-termviews about building the capacity of the health promotion sector.
40 FINAL PLAN 02 February 2005

41 FINAL PLAN 02 February 2005
Workforce Capacity: the need to identify the workforce development requirements for health promotion providers, and put in place a sustainable system to develop a new heath promotion workforce and grow the skills in the existing workforce.
Communications & Resources: the need to review the quality, accessibility and suitability of resources being used by health promotion providers as they relate to diabetes prevention and management; and to develop new resources as required, and ensure all providers are aware of existing resources.
Networking & Aligned Activity: the need to develop an effective process for networking health promotion providers so there is a forum for raising and resolving common issues, aligning programmes and communicating with one voice to funders. It is important to maintain communication between the PHO services and other health promotion providers.
Health promotion needs to fulfill a role of being the glue that holds many parts of the plan together, which can only be achieved through improved provider capacity and whole system coordination. Let’s Beat Diabetes will strengthen health promotion providers, support existing partnerships and create new ones to encourage more effective cross sector activity.
The sector acknowledges that all actions must be culturally responsive to the needs and aspirations of Maori, Pacific peoples, Asians and other ethnic groups. To this end ethnic groups and communities of interest will be involved in all aspects of design, development, implementation and evaluation, including strengthening of programmes that work within a cultural framework of ‘by Maori for Maori’ and ‘by Pacific for Pacific’.
Act
ion
Pla
n A v
ibra
nt,
ski
lled
an
d c
o-o
per
ativ
e h
ealt
h p
rom
oti
on
sec
tor
that
wo
rks
effe
ctiv
ely
wit
h a
ll g
rou
ps
and
in a
ll se
ttin
gs
to r
edu
ce t
he
inci
den
ce a
nd
imp
act
of
dia
bet
es a
nd
hea
lth
ineq
ual
itie
s.A
ll ac
tions
mus
t be
cultu
rally
res
pons
ive
to th
e ne
eds
and
aspi
ratio
ns o
f Mao
ri, P
acifi
c pe
ople
s, A
sian
s an
d ot
her
ethn
ic g
roup
s. T
o th
is e
nd, M
aori,
P
acifi
c pe
ople
s, A
sian
s an
d ot
her
ethn
ics
grou
ps w
ill b
e in
volv
ed in
all
face
ts o
f des
ign,
dev
elop
men
t and
impl
emen
tatio
n.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
ers
Go
al:
Fu
nd
er A
lign
men
t
A
mo
rep
rod
uct
ive
and
su
stai
nab
leen
viro
nm
ent
for
effe
ctiv
eh
ealt
h p
rom
oti
on
is
crea
ted
th
rou
gh
b
ette
r co
llab
ora
tio
nb
etw
een
fu
nd
ing
ag
enci
es.
Tar
get
:
Fu
nd
er
agre
emen
t o
n
Let
’s
Bea
td
iab
etes
fu
nd
ing
in
itia
tive
s fo
r h
ealt
hp
rom
oti
on
by
May
200
5.
Hea
lth P
rom
otio
n fu
nder
san
d ot
her
rele
vant
org
anis
atio
ns m
eet
at l
east
tw
ice
aye
ar a
s a
grou
p to
dis
cuss
issu
es, p
erfo
rman
ce,s
trat
egie
s, p
rogr
amm
e de
sign
and
fund
ing
allo
catio
ns in
ord
er t
o de
velo
p an
alig
ned
and
effic
ient
fun
ding
fra
mew
ork
for
all h
ealth
pro
mot
ion
prov
ider
s in
Cou
ntie
s M
anuk
au.
CM
DH
B d
evel
ops
its f
undi
ng s
trat
egie
s fo
rLe
t’s B
eat
Dia
bete
s in
col
labo
ratio
nw
ith o
ther
fun
ders
to
iden
tify
syne
rgie
s,re
duce
ove
rlap
and
ensu
re f
unds
are
use
def
ficie
ntly
.
A c
ross
fund
erpl
an is
dev
elop
ed fo
r Le
t’s B
eat D
iabe
tes
that
incl
udes
budg
ets
and
serv
ice
obje
ctiv
es.
CM
DH
B, M
oH, S
PA
RC
, MC
C, P
HO
s
Go
al:
Par
tner
ship
s
CO
DA
and
th
e P
HO
H
ealt
h
Pro
mo
tio
nW
ork
ing
Gro
up
wo
rk e
ffec
tive
ly t
og
eth
er t
o
ove
rsee
to
im
ple
men
tati
on
of
this
pla
n o
fac
tio
n
in
colla
bo
rati
on
wit
h
MC
C
and
To
mo
rro
w’s
M
anu
kau
/Te
Ora
O
M
anu
kau
/Man
uka
u t
he
Hea
lth
y C
ity
Ou
tco
me
Gro
up
.
Tar
get
: C
on
trac
t to
su
pp
ort
h
ealt
hp
rom
oti
on
cap
acit
y in
pla
ce b
y Ju
ne
2005
.
The
CO
DA
hea
lthpr
omot
ion
foru
m a
nd P
HO
HP
WG
wor
k to
geth
er t
o ov
erse
e th
esu
cces
sful
im
plem
enta
tion
of t
his
plan
of
actio
n, i
n co
llabo
ratio
nw
ith T
omor
row
’sM
anuk
au/T
e O
ra O
Man
ukau
/Man
ukau
the
Hea
lthy
City
Out
com
e G
roup
,
CM
DH
B e
xplo
res
oppo
rtun
ities
for
a h
ealth
pro
mot
ion
prov
ider
to
take
a m
ore
activ
e ro
le
to
supp
ort
the
netw
orki
ngan
dad
min
istr
atio
n re
quire
d fo
r th
e pa
rtne
rshi
pap
proa
ch a
nd th
e ca
paci
ty b
uild
ing
aspe
cts
of th
e pl
an.
A r
epre
sent
ativ
e fr
om th
e he
alth
pro
mot
ion
part
ners
hip
grou
p si
ts o
n th
e Le
t’s B
eat
Dia
bete
sG
over
nanc
e G
roup
.
Dia
bete
s P
roje
cts
Tru
st,
CO
DA
, P
HO
H
PW
G,T
omor
row
’s M
anuk
au/T
e O
ra O
Man
ukau
/Man
ukau
th
e H
ealth
yC
ityO
utco
me
Gro
up, A
RP
HS
CM
DH
B
Go
al:
Wo
rkfo
rce
Cap
acit
y
Hea
lth
Pro
mo
tio
nw
ork
forc
e is
div
erse
an
dh
igh
ly
skill
ed,
and
p
rovi
des
ef
fect
ive,
Con
sulta
tion
and
need
s as
sess
men
t –
iden
tify
a nu
mbe
r of
rol
es t
hat
peop
lepe
rfor
m in
heal
th p
rom
otio
n an
des
tabl
ish
wha
t ty
pe o
f sk
ills
thes
e ro
les
need
and
Dia
bete
s P
roje
cts
Tru
st,
CO
DA
, P
HO
H
PW
G,T
omor
row
’s M
anuk
au/T
e O
ra O
42F
INA
L P
LA
N 0
2 F
ebru
ary
2005

cult
ura
lly
resp
on
sive
h
ealt
h
pro
mo
tio
n
top
eop
le f
rom
all
eth
nic
gro
up
s.
Tar
get
: C
on
trac
t to
su
pp
ort
h
ealt
hp
rom
oti
on
cap
acit
y in
pla
ce b
y Ju
ne
2005
.
whe
ther
peo
ple
have
or
can
easi
lyga
in th
ese
skill
s.
Cur
ricul
um –
iden
tify
or d
evel
op a
cur
ricul
umfo
r ea
ch o
f the
se r
oles
.
Tra
inin
g –
sour
ce t
rain
ing
for
each
of
thes
e ro
les
incl
udin
g tr
aini
ng t
hat
allo
ws
peop
le to
mov
e be
twee
n ro
les
of d
iffer
ent s
kill
leve
ls a
nd tr
aini
ng to
mai
ntai
n sk
ills.
Adv
ocat
e to
ens
ure
that
fun
ding
is a
vaila
ble
for
peop
le t
o at
tend
tra
inin
g.D
evel
opex
istin
g he
alth
pr
omot
ion
educ
atio
n pr
ogra
mm
es
to
acco
mm
odat
eLe
t’s
Bea
tD
iabe
tes
wor
kfor
ceco
mpe
tenc
ies.
Rec
ogni
tion
– en
sure
that
peo
ple
who
und
erta
ketr
aini
ngre
ceiv
ere
cogn
ition
of t
his
trai
ning
from
em
ploy
ers
such
as D
HB
s, P
HO
s an
d N
GO
s
Spe
cial
ist
skill
s –
reco
gnis
e th
at m
ost
orga
nisa
tions
will
not
be
able
to
empl
oype
ople
with
all
spec
ialis
t sk
ills.
E
nsur
e pe
ople
with
spe
cial
ski
lls a
re k
now
n ab
out
and
avai
labl
eto
pro
vide
adv
ice.
Spe
cial
ist
skill
s m
ayin
clud
e cu
ltura
l sk
ills
for
wor
king
with
Mao
ri, P
acifi
c pe
ople
san
dot
her
ethn
ic g
roup
s, e
valu
atio
n, I
T,
and
med
ia s
kills
etc
.
Man
ukau
/Man
ukau
th
e H
ealth
yC
ityO
utco
me
Gro
up, A
RP
HS
, CM
DH
B
Go
al:
Net
wo
rkin
g &
Alig
nm
ent
Hea
lth
Pro
mo
tio
n e
nvi
ron
men
t an
d a
ctiv
ity
is
co-o
rdin
ated
an
d
focu
sed
,w
ork
ing
tow
ard
s a
shar
edvi
sio
n.
Tar
get
:
Co
ntr
act
to
sup
po
rth
ealt
hp
rom
oti
on
cap
acit
y in
pla
ce b
y Ju
ne
2005
.
Web
site
– d
evel
op a
nd m
aint
ain
aw
ebsi
tew
here
gro
ups
can
shar
e in
form
atio
non
activ
ities
an
d ev
ents
, tr
aini
ng
oppo
rtun
ities
, hu
man
an
dph
ysic
al
reso
urce
s,re
sear
ch i
nfor
mat
ion
etc.
Li
nk t
o T
omor
row
’s M
anuk
auan
dot
her
agen
cies
web
site
s w
here
appr
opria
te.
Mee
tings
–
esta
blis
h a
min
imum
nu
mbe
rof
fo
rum
s th
at
mee
t th
e ne
eds
ofor
gani
satio
ns (
qual
ity f
orum
s, in
form
atio
n sh
arin
g)w
orki
ngin
the
fie
ld a
nd e
nsur
eth
at t
hey
are
run
effe
ctiv
ely
and
thei
r de
cisi
ons
are
diss
emin
ated
to
all
inte
rest
edpa
rtie
s.B
uild
ing
trus
t be
twee
n or
gani
satio
ns –
fos
ter
co-o
pera
tion
betw
een
orga
nisa
tions
byen
surin
g in
divi
dual
s ca
nm
eet
and
wor
k to
geth
er a
nd d
evel
opin
ga
set
ofm
utua
llyag
reed
gro
und
rule
s.
Key
coo
rdin
ator
s –
iden
tify
a nu
mbe
r of
indi
vidu
als
who
can
act
as
key
peop
le f
orho
ldin
g an
d sh
arin
g in
form
atio
n in
spe
cific
top
ic a
reas
(e.
g. s
choo
ls/y
outh
, M
arae
, ph
ysic
al a
ctiv
ity, G
P, e
tc).
Dia
bete
s P
roje
cts
Tru
st,
CO
DA
, P
HO
H
PW
G,T
omor
row
’s M
anuk
au/T
e O
ra O
Man
ukau
/Man
ukau
th
e H
ealth
yC
ityO
utco
me
Gro
up,
AR
PH
S,
Hea
lthpr
ovid
ers,
CM
DH
B
43F
INA
L P
LA
N 0
2 F
ebru
ary
2005

44F
INA
L P
LA
N 0
2 F
ebru
ary
2005
Go
al:
Co
mm
un
icat
ion
& R
eso
urc
es
Key
mes
sag
es a
rou
nd
dia
bet
es p
reve
nti
on
to
b
e ev
iden
ce
bas
ed
and
ef
fect
ivel
y an
d
con
sist
entl
y d
isse
min
ated
.
Tar
get
:Co
ntr
act
to s
up
po
rt h
ealt
h p
rom
oti
on
ca
pac
ity
in p
lace
by
Jun
e 20
05.
Key
mes
sage
s–
deve
lop
a gr
oup
that
can
ide
ntify
and
upd
ate
key
mes
sage
s fo
r di
abet
es r
elat
ed h
ealth
pro
mot
ion
for
the
regi
on.
Ens
ure
that
the
se m
essa
ges
are
diss
emin
ated
to th
ose
who
will
use
them
.
Res
ourc
es –
iden
tify
or f
und
and
deve
lop
a ra
nge
of a
ppro
pria
te (
pref
erab
ly lo
cally
de
velo
ped
or e
valu
ated
) re
sour
ces
that
inc
lude
the
key
mes
sage
s.
Ens
ure
thes
e re
sour
ces
are
used
by
effe
ctiv
e di
ssem
inat
ion
and
havi
ng a
reg
iste
r of
res
ourc
es.
Oth
er s
ecto
rs –
ens
ure
that
the
str
ateg
ies
and
activ
ity o
f th
e he
alth
pro
mot
ion
sect
or is
com
mun
icat
ed to
oth
er a
reas
of t
he h
ealth
sec
tor
(prim
ary
and
seco
ndar
y ca
re)
and
othe
r re
leva
nt s
ecto
rs th
roug
h ke
y id
entif
ied
cont
acts
.
CM
DH
B,
Spe
cial
ists
, P
HO
s,
Non
-G
over
nmen
t O
rgan
isat
ions
(N
GO
s),
MoH
, C
OD
A,
AR
PH
S,
Dia
bete
s A
uckl
and

6. Enhancing Well Child Services to Reduce Childhood
Obesity
Context
‘A life-course perspective is essential for the prevention and control of non-communicablediseases. This approach starts with maternal health and prenatal nutrition, pregnancyoutcomes, exclusive breastfeeding for six months, and child and adolescent health; reacheschildren at schools, adults at worksites and other settings, and the elderly; and encourages a healthy diet and regular physical activity from youth into old age’ (WHO, 2004).
The World Health Organisation’s (WHO) Global Strategy on Diet, Physical Activity andHealth acknowledges the importance of a life course approach in beating chronicdiseases like diabetes. A life course approach starts with maternal health and thecritical early years of life. An increasing body of evidence now supports the impactmaternal nutrition and child nutrition and physical activity have on a person’s healththroughout life (Barnfather D, 2004).
The importance of the health of our young children has been echoed in hui and fonoundertaken as part of the Let’s Beat Diabetes planning process. Maori and Pacific peoples have given clear guidance that the strategy must focus strongly on the newgeneration and place more effort on protecting children from obesity and subsequentdisease. Recent statistics show that 31 percent of New Zealand children areoverweight or obese; 62 percent of Pacific children overweight or obese; and 41percent of Maori children overweight or obese. Childhood obesity can lead to earlyonset of diabetes and is a strong predictor of adult obesity.
While international and local communities call for health services to address chronicdisease throughout the life course, there is little national policy or service provision targeting good nutrition and physical activity in the early years - breastfeeding being theexception. There is also a need to improve identification and management ofgestational diabetes.
The Let’s Beat Diabetes consultation process has also identified community concernsabout how best to support ‘at-risk’ families. Many of these families have multipleproblems, and providing appropriate nutrition for their children is beyond their reach.Health services on their own are limited in what they can do to support children insituations where the family is dysfunctional or has very limited resources.
Programme Design
The objective of this action area is to develop an environment in which parents havethe knowledge and opportunity to provide appropriate nutrition and physical activity for their young children. There is an opportunity to enhance the current maternity and WellChild frameworks to support a life course approach to diabetes prevention. There is also an opportunity to forge new partnerships with the Ministry of Social Developmentto better identify and support vulnerable families.
To achieve the desired changes in service provision, it is proposed that a district-widenational pilot programme is developed which, due to its broad and cross-sectoralimplications, includes the Ministry of Health (MoH), Ministry of Social Development(MSD), Counties Manukau District Health Board (CMDHB) and service providers in the
45 FINAL PLAN 02 February 2005

46 FINAL PLAN 02 February 2005
planning and development phases. The pilot would seek to achieve four key outcomes:
Enhancement of Maternity and Well Child frameworks to facilitate greater family uptake of appropriate nutrition and physical activity in the early years, and throughout childhood.
Improved capabilities of Well Child services to assess children with developing obesity risks, and provide more intensive support or referral were required.
Develop a cross-sectoral approach to identification of, and support for, vulnerable families. Increase the ability of maternity and Well Child providers to identify vulnerable families and refer for support services.
Develop a broader strategic framework for reducing childhood obesity, which may include an extension of Well Child support systems into the school environment.
Implementation of the proposed service enhancements would not take place until the roll out of the current update to the Well Child service framework is completed, which is expected in late 2005. Implementation of the enhanced Well Child framework may require greater CMDHB control over the Well Child funding stream than is currently the case.

47F
INA
L P
LA
N 0
2 F
ebru
ary
2005
Act
ion
Pla
n
Ch
ildre
n b
egin
th
eir
lives
in a
n e
nvi
ron
men
t th
at s
up
po
rts
life
lon
g h
ealt
h.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
s A
ctio
n L
ead
er
Go
al:
Su
stai
nab
le s
tru
ctu
res
are
set
up
to
su
pp
ort
new
ear
ly y
ear’
s se
rvic
es.
Tar
get
: B
y 20
05 a
gre
emen
t fo
r d
etai
led
p
ilot
stru
ctu
re a
nd
ou
tco
mes
.
Dev
elop
an
agre
emen
t be
twee
n C
MD
HB
, M
oH,
and
MS
D t
o tr
ial
enha
nced
M
ater
nity
and
Wel
l C
hild
fra
mew
orks
in
Cou
ntie
s M
anuk
au i
n a
dist
rict-
leve
l pi
lot.
Dev
elop
a g
over
nanc
e st
ruct
ure
for
the
pilo
t pro
gram
me.
CM
DH
B, M
oH, M
SD
Go
al:
Ob
esit
y in
yo
un
g c
hild
ren
red
uce
s d
ue
to
imp
rove
d
nu
trit
ion
an
d
ph
ysic
al
acti
vity
.
Tar
get
:
By
2006
en
han
ced
ed
uca
tio
n
op
erat
ion
al.
By
2010
th
e ri
se i
n c
hild
ob
esit
y w
ill h
ave
sto
pp
ed.
Dev
elop
a s
et o
f le
arni
ng o
bjec
tives
and
a c
urric
ulum
to
cove
r bo
th a
nten
atal
an
d ea
rly y
ears
act
iviti
es t
hat
goes
bey
ond
the
curr
ent
supp
ort
for
brea
st
feed
ing.
C
urric
ulum
cov
ers
know
ledg
e an
d be
havi
our
chan
ge t
echn
ique
s to
su
ppor
t cha
nged
atti
tude
s to
chi
ldho
od o
besi
ty.
Intr
oduc
e th
e le
arni
ng o
bjec
tives
and
cur
ricul
um in
to th
e se
rvic
e sp
ecifi
catio
ns
of m
ater
nity
and
Wel
l Chi
ld p
rovi
ders
. D
evel
op s
uppo
rtin
g re
sour
ces.
Tra
in s
ervi
ce p
rovi
ders
in th
e ne
w c
urric
ulum
and
del
iver
enh
ance
d se
rvic
es.
CM
DH
B,
Wel
l C
hild
pro
vide
rs,
Man
ukau
In
stitu
te o
f Tec
hnol
ogy
(MIT
), M
oH
Go
al:
Vu
lner
able
fam
ilies
will
be
able
to
b
rin
g u
p h
ealt
hy
child
ren
.
Tar
get
: B
y 20
06 n
ew r
efer
ral m
ech
anis
ms
in p
lace
.
Sup
port
tra
inin
g an
d de
velo
pmen
t pr
oces
ses
to e
nabl
e m
ater
nity
and
Wel
l C
hild
pr
ovid
ers
to
accu
rate
ly
asse
ss
and
iden
tify
fam
ilies
in
vu
lner
able
si
tuat
ions
, w
ho a
re u
nabl
e to
pro
vide
an
appr
opria
te n
utrit
ion
envi
ronm
ent
for
thei
r ch
ildre
n.
Dev
elop
exp
licit
proc
esse
s fo
r m
ater
nity
and
Wel
l C
hild
pro
vide
rs t
o re
fer
vuln
erab
le fa
mili
es to
MS
D-li
nked
ser
vice
s fo
r su
ppor
t and
rec
over
y.
Mai
ntai
n co
llabo
rativ
e he
alth
/wel
fare
su
ppor
t fo
r fa
mily
re
silie
ncy
and
Chi
ld
Hea
lth
outc
omes
.
CM
DH
B, W
ell C
hild
pro
vide
rs, M
IT, M
oH
Go
al:
C
hild
o
bes
ity
is
iden
tifi
ed
and
re
spo
nd
ed
to
in
an
evid
ence
-bas
ed
man
ner
.
Tar
get
: A
ll o
bes
e ch
ildre
n p
re f
ive
are
iden
tifi
ed
and
p
aren
ts
pro
vid
ed
wit
h
advi
ce o
n a
pp
rop
riat
e re
spo
nse
.
Sup
port
trai
ning
and
dev
elop
men
t pro
cess
es to
ena
ble
Wel
l Chi
ld p
rovi
ders
to
accu
rate
ly a
sses
s an
d id
entif
y ch
ildre
n at
ris
k of
obe
sity
or
who
are
alre
ady
obes
e an
d w
hose
hea
lth m
ay b
e co
mpr
omis
ed.
Dev
elop
spe
cial
ist s
uppo
rt a
nd r
efer
ral s
ervi
ces
to e
nabl
e W
ell C
hild
pro
vide
rs
to
prov
ide
mor
e in
tens
ive
supp
ort
for
high
ris
k ch
ildre
n an
d re
ferr
al
to
spec
ialis
t ser
vice
s if
nece
ssar
y.
CM
DH
B, W
ell C
hild
pro
vide
rs, M
IT, M
oH
Go
al:
S
ervi
ce
con
tin
uit
y is
d
evel
op
ed
Dev
elop
a m
ore
stra
tegi
c co
ncep
tual
vie
w o
f W
ell C
hild
ser
vice
s fo
r C
ount
ies
CM
DH
B,
MoH
, M
SD
, M
inis
try
of

48F
INA
L P
LA
N 0
2 F
ebru
ary
2005
bet
wee
n W
ell
Ch
ild a
nd
‘h
ealt
hy
sch
oo
l’ se
rvic
es.
Tar
get
:
By
July
20
05
sco
pin
g
revi
ew
com
ple
te
wit
h
reco
mm
end
atio
ns
for
furt
her
act
ion
.
Man
ukau
in th
e fu
ture
, whi
ch s
ees
the
stru
ctur
ed p
roce
ss o
f Wel
l Chi
ld a
ctiv
ity
flow
thr
ough
int
o pr
imar
y sc
hool
Hea
lth P
rom
otin
g S
choo
ls f
ram
ewor
ks a
nd
on i
nto
a W
ell
Tee
n co
ncep
t th
at c
ould
em
erge
fro
m t
he c
urre
nt Y
ear
9 as
sess
men
ts a
nd ‘
Nut
ritio
n E
xerc
ise
and
Wei
ght’
prog
ram
me
with
in t
he A
im
Hi c
lust
er o
f low
dec
ile s
econ
dary
sch
ools
.
Thi
s m
ore
stra
tegi
c vi
ew o
f a
‘Wel
l C
hild
to
Wel
l T
een’
fra
mew
ork
coul
d be
de
velo
ped
as a
pilo
t in
par
tner
ship
with
the
Min
istr
y of
Edu
catio
n an
d M
SD
to
mee
t the
pol
icy
obje
ctiv
es o
f hea
lth, w
elfa
re a
nd e
duca
tion.
Edu
catio
n
Go
al:
A c
on
tin
uo
us
lear
nin
g a
nd
qu
alit
y im
pro
vem
ent
envi
ron
men
t en
cou
rag
e im
pro
ved
pro
vid
er e
ffec
tive
nes
s.
Tar
get
: E
valu
atio
n f
ram
ewo
rk d
evel
op
ed
by
July
200
5.
Wor
k w
ith th
e U
nive
rsity
of A
uckl
and
Sch
ool o
f Pop
ulat
ion
Hea
lth (
UoA
-SoP
H)
to d
evel
op a
fram
ewor
k fo
r ev
alua
tion
of th
e W
ell C
hild
initi
ativ
e.
Ong
oing
pr
oces
s an
d ou
tcom
e ev
alua
tion
unde
rtak
en,
desi
gned
to
fo
ster
qu
ality
impr
ovem
ent c
ycle
s.
UoA
-SO
PH
, C
MD
HB
, W
ell
Chi
ld
prov
ider
s, M
IT, M
oH

7. Developing a Schools Accord to Ensure Children
Are ‘Fit, Healthy and Ready to Learn’
Context
The school environment is important for the health of our growing children. Childrenspend up to thirteen years in school. What they learn during these formative years will influence their choices and decisions in later life. Also, the nutrition and physical activity environment at school directly affects children’s health and predisposition for chronic diseases, like diabetes, later in life. Children’s levels of physical activity during school years are dropping and children are eating more energy dense foods, leading toobesity (Barnfather D, 2004). In 2002, 30 percent of all New Zealand children were overweight or obese. A recent survey of Year 9 pupils in AIMHI secondary schools inCounties Manukau showed that in excess of 30 percent are already obese.
Many schools within Counties Manukau have challenging educational environmentsand relatively low levels of financial support from their communities. Schools are underpressure to meet academic outcomes. A number of observers have noted that schoolsplace less emphasis on physical activity now than they have in the past in order todevote more time to academic learning.
The benefits of improving the health environment in schools are not only health-related.There is an emerging body of evidence linking physical activity and good nutrition witheducational attainment, the most recent being The Learning Connection: The Value ofImproving Nutrition and Physical Activity in Our Schools report. The report documentsthat the rise in poor nutrition and inactivity is adversely affecting academic achievementand increasing financial pressures on schools. It is in the school’s interest to support ahealth promoting environment.
The importance of health in schools has recently been noted by a new Governmentpolicy that primary schools will be expected to provide students with one hour of physical activity a week.
Many schools will require increased levels of support if they are to reorient themselvesto address the obesity epidemic and actively create healthy environments, including skills, programmes, resources and community support. Many schools have said theyprefer to operate comprehensive or integrated programmes which have a whole-school approach, reflect each school’s unique situation and look at student health in a holisticmanner.
Currently there are a number of organisations and providers that support healthy schools but in general they work in only a small number of schools and lack sector-wide coordination or long term goals. There are a number of advice-only programmes,where-as schools have indicated they want on-the-ground practical help. The KidsFirstpublic nursing service is one of the few health-based services delivered across allprimary schools. A comprehensive approach to school health is being supported in asmall number of high needs secondary schools through the Nutrition Exercise andWeight (NEW) programme.
Despite the issues with fragmented providers, there is a platform of skills andprogrammes that can grow to provide more substantial support for schools. Primary Health Organisation (PHO)-based health promotion services have recognised that theymay have a role in the schools environment. The Food Group has indicated its interest
49 FINAL PLAN 02 February 2005

50 FINAL PLAN 02 February 2005
in activities associated with the schools environment. Schools themselves are taking a stronger interest in their health promoting role.
Consistent approaches to achieving best practice in schools are required, as well as better feedback on which programmes are achieving the desired outcomes.
Programme Design
The fundamental requirement of programme design is to create a vision and a framework that enables schools and service providers to work in a more coordinated and effective way. The programme design seeks to develop a collaborative approach that includes teachers, principals, trustees and the health and physical activity sectors. A sustainable governance structure is required that can provide a direction that all parties own.
A set of realistic goals need to be developed that contribute to reducing the obesity epidemic but are also achievable. Some proposed goals are outlined in this paper. A number of these actions can be started immediately with existing services and resources.
In order to achieve a far reaching change in school environments the existing level of support and general activity may not be enough. A more thorough review of the programmes and resources required to achieve the fit and healthy schools goals may be needed.
Existing service providers should be encouraged and supported where their programmes are well accepted and effective. It is proposed that the various services on offer are presented to trustees and principals as a consolidated menu of services, which schools can choose from to help them meet their objectives.
Early childhood education, primary schools and secondary schools have different needs and dynamics. Strategies need to look at each of these sectors separately.

Act
ion
Pla
ns
Ear
ly C
hild
ho
od
Ed
uca
tio
n
Sch
oo
ls a
re a
n e
nvi
ron
men
t th
at p
rote
cts
agai
nst
ob
esit
y.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
er
Go
al:
By
2010
Co
un
ties
Man
uka
u e
arly
child
ho
od
edu
cati
on
lead
s th
e co
un
try
in t
hei
r co
mm
itm
ent
to
sup
po
rtin
gh
ealt
hy
eati
ng
an
d a
ctiv
e liv
ing
.
Tar
get
:
By
2010
10
0%
of
earl
y le
arn
ing
envi
ron
men
ts h
ave
aud
ited
eff
ecti
ve h
ealt
hy
eati
ng
acti
ve li
vin
g p
olic
ies.
Adi
stric
t go
vern
ance
gro
up i
s es
tabl
ishe
d th
at i
nclu
des
early
chi
ldho
oded
ucat
ion
staf
f, pa
rent
s an
d he
alth
sec
tor
togu
ide
wor
kas
sess
ing
need
s fo
rea
rly c
hild
hood
, fiv
e ye
ar g
oals
and
rec
omm
ende
d pr
ogra
mm
es.
A r
epre
sent
ativ
e fr
om th
e gr
oup
sits
on
the
Let’s
Bea
t Dia
bete
sG
over
nanc
eG
roup
.
Cou
ntie
sM
anuk
au
Dis
tric
t H
ealth
Boa
rd(C
MD
HB
),
Min
istr
yof
E
duca
tion
(MoE
),
Man
ukau
C
ity
Cou
ncil
(MC
C),
Ear
lyC
hild
hood
Cen
tres
(E
CE
), K
ohan
ga R
eo
Go
al:
Ph
ysic
al a
ctiv
ity
By
2010
ob
esit
y g
row
th i
n c
hild
ren
has
sto
pp
edan
d is
red
uci
ng
.
Tar
get
:
By
2010
10
0%
of
earl
y le
arn
ing
envi
ron
men
ts h
ave
aud
ited
eff
ecti
ve h
ealt
hy
eati
ng
acti
ve li
vin
g p
olic
ies.
Spo
rt a
nd R
ecre
atio
n N
ew Z
eala
nd (
SP
AR
C),
sup
port
edby
the
edu
catio
nan
d he
alth
sec
tors
, im
plem
ents
its
Kiw
iba
by,
Kiw
i to
ddle
r an
d K
iwi
pre-
scho
ol p
rogr
amm
es in
EC
Es
in C
ount
ies
Man
ukau
. T
his
incl
udes
Koh
anga
Reo
and
Pac
ific
EC
Es.
Str
ateg
ies
are
inve
stig
ated
tha
t le
vera
ge c
ultu
ral k
now
ledg
e an
d pr
actic
ein
Koh
anga
Reo
and
Pac
ific
EC
Es
to s
uppo
rt h
ealth
yap
proa
ches
to
phys
ical
activ
ity.
SP
AR
C,
heal
th
sect
or,
EC
Es,
N
on-
Gov
ernm
ent O
rgan
isat
ions
(N
GO
s)
Go
al:
Nu
trit
ion
By
2010
ob
esit
y g
row
th i
n c
hild
ren
has
sto
pp
edan
d is
red
uci
ng
.
Tar
get
:
By
2010
10
0%
of
earl
y le
arn
ing
envi
ron
men
ts h
ave
aud
ited
eff
ecti
ve h
ealt
hy
eati
ng
acti
ve li
vin
g p
olic
ies.
Auc
klan
d R
egio
nal
Pub
lic
Hea
lthS
ervi
ce
(AR
PH
S)
supp
orts
S
PA
RC
’sef
fort
s by
pr
ovid
ing
nutr
ition
al
info
rmat
ion
and
supp
ort
to
the
EC
Es
inC
ount
ies
Man
ukau
.T
his
incl
udes
Koh
anga
Reo
and
Pac
ific
EC
Es.
Str
ateg
ies
are
inve
stig
ated
tha
t le
vera
ge c
ultu
ral k
now
ledg
e an
d pr
actic
ein
Koh
anga
Reo
and
Pac
ific
EC
Es
to s
uppo
rt h
ealth
y ap
proa
ches
to n
utrit
ion.
AR
PH
S, N
GO
s, S
PA
RC
Go
al:
Eva
luat
ion
Eva
luat
ion
su
pp
ort
s a
lear
nin
g
fram
ewo
rk
and
sup
po
rts
esta
blis
hm
ent
of
bes
t p
ract
ice
in e
arly
lear
nin
g c
entr
es.
SP
AR
C e
valu
ates
its
prog
ram
mes
.S
PA
RC
, CM
DH
B, U
oA-S
oPH
51F
INA
L P
LA
N 0
2 F
ebru
ary
2005

Tar
get
: E
valu
atio
n f
ram
ewo
rk s
et u
p b
y Ju
ly 2
005.
SP
AR
Cw
orks
with
C
MD
HB
an
d th
e U
nive
rsity
of
A
uckl
and-
Sch
ool
ofP
opul
atio
n H
ealth
(U
oA–S
oPH
) to
dev
elop
a f
ram
ewor
k fo
r pr
oces
s an
dou
tcom
es e
valu
atio
n of
the
agre
ed a
ctio
n pl
ans.
Pri
mar
y S
cho
ols
Pri
mar
y sc
ho
ols
are
an
en
viro
nm
ent
that
pro
tect
sag
ain
st o
bes
ity.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
er
Go
al:
B
y 20
10 C
ou
nti
es M
anu
kau
sch
oo
ls l
ead
th
e co
un
try
in
thei
r co
mm
itm
ent
to
sup
po
rtin
gh
ealt
hy
eati
ng
an
d a
ctiv
e liv
ing
.
Su
gg
este
d t
arg
ets:
By
2008
:10
0%
of
pri
mar
ysc
ho
ols
p
rovi
de
1 h
ou
rex
erci
se p
er w
eek.
By
2010
:90
% o
f p
rim
ary
sch
oo
ls p
rovi
de
30 m
inu
tes
exer
cise
a d
ay.
100%
of
sch
oo
ls h
ave
aud
ited
hea
lth
y m
enu
can
teen
s.
A
repr
esen
tativ
e go
vern
ance
gr
oup
is
esta
blis
hed
(incl
udes
st
uden
ts,
teac
hers
, pr
inci
pals
, tr
uste
es
and
heal
th/
activ
ity
prov
ider
s)
to
guid
eas
sess
men
t of
nee
d in
prim
ary
scho
ols,
ide
ntify
the
fiv
eye
argo
als
and
reco
mm
end
prog
ram
mes
.
A r
epre
sent
ativ
e fr
om th
e gr
oup
sits
on
the
Let’s
Bea
t Dia
bete
sG
over
nanc
eG
roup
.
Kid
z F
irst,
CM
DH
B,
Sch
ools
, N
GO
s, M
OE
,A
RP
HS
, MC
C
Go
al:
Res
ou
rces
are
ava
ilab
le t
o a
chie
ve g
oal
s.
Tar
get
: B
yJu
ly 2
005,
rev
iew
com
ple
ted
.
A r
evie
w i
s un
dert
aken
loo
king
at
wha
t le
vels
of
inpu
t, pr
ogra
mm
e de
sign
san
d re
sour
ces
will
be
requ
ired
to a
chie
ve th
e id
entif
ied
goal
s.
The
rep
ort w
illgu
ide
the
actio
n pl
an.
Sch
ools
gov
erna
nce
grou
p, C
MD
HB
Go
als:
S
cho
ols
are
su
pp
ort
ed t
o d
evel
op
hea
lth
yen
viro
nm
ents
.
Tar
get
:A
ll sc
ho
ols
are
per
son
ally
co
nta
cted
and
serv
ices
on
off
er p
rese
nte
d d
uri
ng
200
5.
The
re is
impr
oved
co-
ordi
natio
n of
pro
gram
mes
am
ongs
tpr
ovid
ers
to m
ake
it ea
sier
for
prin
cipa
ls t
o un
ders
tand
wha
t su
ppor
t se
rvic
es a
re a
vaila
ble
to
assi
st th
em to
ach
ieve
the
iden
tifie
d go
als.
Prin
cipa
ls a
re in
form
ed a
bout
the
supp
ort s
ervi
ces
and
reso
urce
s av
aila
ble.
The
re
is
proa
ctiv
e co
mm
unic
atio
nw
ith
all
scho
ols
abou
t th
e ne
ed
to
CM
DH
B,
SP
AR
C,
PH
Os,
Min
istr
yof
Hea
lth(M
oH),
NG
Os
52F
INA
L P
LA
N 0
2 F
ebru
ary
2005
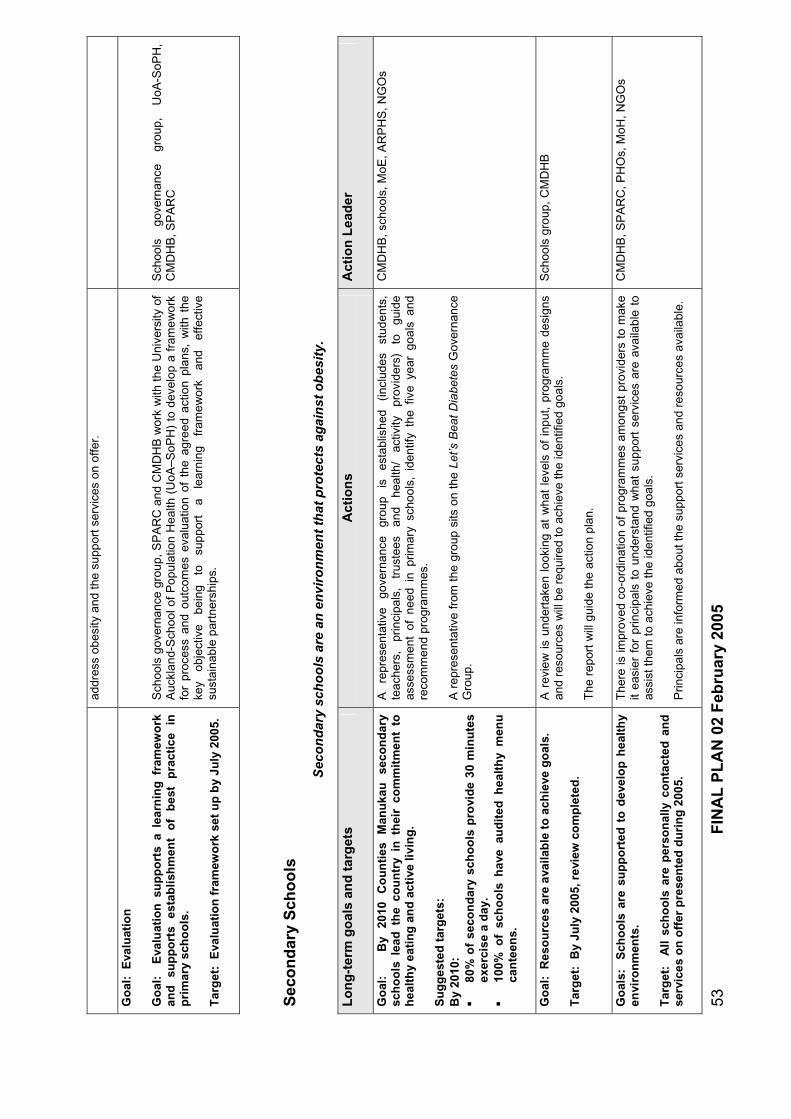
addr
ess
obes
ity a
nd th
e su
ppor
t ser
vice
s on
offe
r.
Go
al:
Eva
luat
ion
Go
al:
Eva
luat
ion
su
pp
ort
s a
lear
nin
g f
ram
ewo
rkan
d
sup
po
rts
esta
blis
hm
ent
of
bes
t p
ract
ice
in
pri
mar
y sc
ho
ols
.
Tar
get
: E
valu
atio
n f
ram
ewo
rk s
et u
p b
y Ju
ly 2
005.
Sch
ools
gov
erna
nce
grou
p, S
PA
RC
and
CM
DH
B w
ork
with
the
Uni
vers
ityof
Auc
klan
d-S
choo
l of
Pop
ulat
ion
Hea
lth (
UoA
–SoP
H)
to d
evel
op a
fra
mew
ork
for
proc
ess
and
outc
omes
eval
uatio
n of
the
agr
eed
actio
n pl
ans,
with
the
key
obje
ctiv
e be
ing
to
supp
ort
a le
arni
ng
fram
ewor
k an
d ef
fect
ive
sust
aina
ble
part
ners
hips
.
Sch
ools
go
vern
ance
gr
oup,
U
oA-S
oPH
,C
MD
HB
, SP
AR
C
Sec
on
dar
y S
cho
ols
Sec
on
dar
y sc
ho
ols
are
an
en
viro
nm
ent
that
pro
tect
s ag
ain
st o
bes
ity.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
er
Go
al:
By
2010
C
ou
nti
es
Man
uka
use
con
dar
ysc
ho
ols
lea
dth
e co
un
try
in t
hei
r co
mm
itm
ent
to
hea
lth
y ea
tin
g a
nd
act
ive
livin
g.
Su
gg
este
d t
arg
ets:
By
2010
:80
% o
f se
con
dar
y sc
ho
ols
pro
vid
e 30
min
ute
sex
erci
se a
day
.10
0% o
f sc
ho
ols
hav
eau
dit
ed h
ealt
hy
men
uca
nte
ens.
A
repr
esen
tativ
e go
vern
ance
gr
oup
is
esta
blis
hed
(incl
udes
st
uden
ts,
teac
hers
, pr
inci
pals
, tr
uste
es
and
heal
th/
activ
ity
prov
ider
s)
to
guid
eas
sess
men
t of
nee
d in
prim
ary
scho
ols,
ide
ntify
the
fiv
eye
argo
als
and
reco
mm
end
prog
ram
mes
.
A r
epre
sent
ativ
e fr
om th
e gr
oup
sits
on
the
Let’s
Bea
t Dia
bete
sG
over
nanc
eG
roup
.
CM
DH
B, s
choo
ls, M
oE, A
RP
HS
, NG
Os
Go
al:
Res
ou
rces
are
ava
ilab
le t
o a
chie
ve g
oal
s.
Tar
get
: B
yJu
ly 2
005,
rev
iew
com
ple
ted
.
A r
evie
w i
s un
dert
aken
loo
king
at
wha
t le
vels
of
inpu
t, pr
ogra
mm
e de
sign
san
d re
sour
ces
will
be
requ
ired
to a
chie
ve th
e id
entif
ied
goal
s.
The
rep
ort w
illgu
ide
the
actio
n pl
an.
Sch
ools
gro
up, C
MD
HB
Go
als:
S
cho
ols
are
su
pp
ort
ed t
o d
evel
op
hea
lth
yen
viro
nm
ents
.
Tar
get
:A
ll sc
ho
ols
are
per
son
ally
co
nta
cted
and
serv
ices
on
off
er p
rese
nte
d d
uri
ng
200
5.
The
re is
impr
oved
co-
ordi
natio
n of
pro
gram
mes
am
ongs
tpr
ovid
ers
to m
ake
it ea
sier
for
prin
cipa
ls t
o un
ders
tand
wha
t su
ppor
t se
rvic
es a
re a
vaila
ble
to
assi
st th
em to
ach
ieve
the
iden
tifie
d go
als.
Prin
cipa
ls a
re in
form
ed a
bout
the
supp
ort s
ervi
ces
and
reso
urce
s av
aila
ble.
CM
DH
B, S
PA
RC
, PH
Os,
MoH
, NG
Os
53F
INA
L P
LA
N 0
2 F
ebru
ary
2005

54F
INA
L P
LA
N 0
2 F
ebru
ary
2005
The
re
is
proa
ctiv
e co
mm
unic
atio
n w
ith
all
scho
ols
abou
t th
e ne
ed
to
addr
ess
obes
ity a
nd th
e su
ppor
t ser
vice
s on
offe
r.
Go
al:
Sch
oo
ls s
erve
on
ly d
iet
dri
nks
an
d w
ater
.
Tar
get
: B
y 20
06,
90%
die
t d
rin
ks a
nd
wat
er t
arg
et
ach
ieve
d.
Sch
ools
are
enc
oura
ged
to r
educ
e th
e av
aila
bilit
y of
hig
h ca
rboh
ydra
te
drin
ks o
n sc
hool
gro
unds
. S
choo
ls, A
RP
HS
, Foo
d G
roup
, CM
DH
B
Go
al:
Stu
den
ts t
ake
up
lea
der
ship
ro
les
wit
hin
th
eir
sch
oo
ls
to
sup
po
rt
hea
lth
y ea
tin
g
acti
ve
livin
g.
Tar
get
: S
tud
ent-
led
act
ivis
m b
egin
s d
uri
ng
200
6.
Stu
dent
-led
activ
ism
in
the
area
of
fit a
nd h
ealth
y sc
hool
s is
enc
oura
ged
and
reso
urce
s ar
e m
ade
avai
labl
e to
sup
port
app
ropr
iate
stu
dent
act
iviti
es.
Sch
ools
gov
erna
nce
grou
p
Go
al:
E
valu
atio
n
of
inte
rven
tio
ns
at
the
AIM
HI
sch
oo
ls
pro
vid
es
gu
idan
ce
for
on
go
ing
h
igh
sc
ho
ol s
trat
egie
s.
Tar
get
:
Pre
limin
ary
resu
lts
of
NE
W
eval
uat
ion
co
mp
lete
d b
y en
d o
f 20
06,
wit
h d
ecis
ion
s m
ade
abo
ut
on
go
ing
pro
gra
mm
e d
esig
n.
A f
urt
her
eva
luat
ion
of
sch
oo
ls i
nte
rven
tio
ns
will
b
e u
nd
erta
ken
by
Uo
A-S
oP
H,
wh
ich
wit
h r
esu
lts
avai
lab
le in
200
7/08
.
The
ex
istin
g N
EW
pr
ogra
mm
e,
a co
mpo
nent
of
th
e A
IMH
I H
ealth
y C
omm
unity
Sch
ools
ini
tiativ
e, d
eliv
ered
in
asso
ciat
ion
with
the
Dia
bete
s P
roje
cts
Tru
st,
is s
uppo
rted
as
a pi
lot
prog
ram
me
- w
ith i
ts o
wn
eval
uatio
n co
mpo
nent
.
The
U
nive
rsity
of
A
uckl
and
Sch
ool
of
Pop
ulat
ion
Hea
lth
(UoA
-SoP
H)
seco
ndar
y sc
hool
in
terv
entio
n an
d ev
alua
tion
is
also
su
ppor
ted
and
syne
rgie
s de
velo
ped
betw
een
the
two
prog
ram
mes
.
Bot
h se
ts o
f ev
alua
tion
resu
lts w
ould
be
used
to
guid
e on
goin
g pr
ogra
mm
e de
sign
, im
plem
enta
tion
and
inve
stm
ent
in
seco
ndar
y sc
hool
-bas
ed
prog
ram
mes
.
AIM
HI
scho
ols,
D
iabe
tes
Pro
ject
s T
rust
, U
oA-S
oPH
, CM
DH
B, M
oE

8. Supporting Primary Care-Based Prevention and
Early Intervention
Context
A large number of government policies call on primary health care to make a greatercontribution to the health of populations, to work with families, and to focus on chronic disease prevention and management (NZ Health Strategy, NZ Primary Health CareStrategy, He Korowai Oranga, The Pacific Health and Disability Action Plan). (Ministry of Health 2000; 2001; 2002).
Primary Health Organisations (PHOs) have been set up and new funding streams are now available to support chronic disease prevention and management. However, thereis also a lack of clear evidence about exactly how PHOs and General Practitioner (GP)teams can go about preventing disease in a cost effective way. Prevention anddisease management programmes challenge the primary care sector to define new relationships with patients and new roles and responsibilities within primary careteams.
Counties Manukau District Health Board (CMDHB) and the primary care sector haveinvested considerable resources over the past five years developing the Chronic CareManagement programme (CCM), which supports community-based structuredmanagement of people with advanced and complicated diabetes. The CCM projectinvolves collaborations between CMDHB and PHOs. CCM delivers training programmes for GP teams, information technology support and incentive payments toGPs. It is one of New Zealand’s most sophisticated disease management initiatives,and provides a strong platform for further collaborative activities between CMDHB and the PHOs.
Developing primary care initiatives that focus on disease prevention and managementwill need sound evidence and be achievable in the busy practice environment. TheCCM experience has identified that significant training, support and strong projectmanagement is required to bring about changes in the general practice environmentand that even small changes can take considerable time to introduce. PHOs haveshown a willingness to become more involved in disease prevention activities.
Primary care involvement in, and support for, broader social marketing programmes is essential to change population behaviour. There is an increasing body of evidenceabout the role for primary care in providing brief intervention advice on behaviour change and support for improved education to support the “expert patient” andimproved self management. General practice is the key environment for the earlyidentification of risk factors and screening to identify diabetes. New Zealand has published national guidelines for the screening for and management of diabetes. Thefact that the major health sector costs from complications of diabetes are heartdisease, especially in the early stages of disease progression, suggests that peoplewith diabetes should also be proactively managed in terms of their cardiovascular risk. PHO funding streams allow for significant flexibility for primary care based healthpromotion and disease prevention activities – especially targeting high risk groups.
Programme Design
The following four initiatives have been identified in collaboration with the primary caresector. They are based on supporting evidence that they will have a positive impact,
55 FINAL PLAN 02 February 2005

56 FINAL PLAN 02 February 2005
they are achievable, they fit together to support improved overall system capacity in primary care, and they link into the broader Let’s Beat Diabetes plan:
To provide consistent and persuasive information to ‘at risk’ people to support lifestyle change;
To improve identification of people who have diabetes at an earlier stage of their disease progression; (New Zealand Guidelines Group 2003)
To improve the level of education given to newly-diagnosed diabetics to support improved self management of diabetes and of their cardiovascular risk; and
To trial a new approach to disease management in which the primary care team works with the whole family of a person with diabetes, to support better health for the whole family/whole whanau approach (links with He Korowai Oranga).
These programmes will require collaborative leadership across CMDHB and PHOs. They will also require investment in training and development of primary care teams and in the community outreach medical and nursing specialist service at Middlemore Hospital.
Information Technology (IT) infrastructure will be required to support activities. The projects will require CMDHB project management and clinical expertise and well as PHO-led operational management. Evaluation will also be a key component of the activity, and will inform how the programmes develop, particularly the family group practice trial.

Act
ion
Pla
n
Pri
mar
y h
ealt
h c
are
pro
acti
vely
an
d p
rofi
cien
tly
wo
rks
wit
h p
atie
nts
an
d t
hei
r fa
mili
es
to r
edu
ce d
iab
etes
ris
k an
d im
pro
ve d
isea
se m
anag
emen
t.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
er
Go
al:
P
atie
nts
at
ten
din
g
GP
te
ams
pro
acti
vely
re
ceiv
e in
form
atio
n
and
cou
nse
llin
g t
o s
up
po
rt h
ealt
hy
eati
ng
an
dac
tive
livi
ng
.
Tar
get
: 7
0% o
f at
ris
k p
atie
nts
att
end
ing
GP
s re
ceiv
e a
‘do
se’
of
pra
ctic
al
hea
lth
info
rmat
ion
ab
ou
tlif
esty
lew
hic
h a
lign
sw
ith
the
soci
al m
arke
tin
g s
trat
egy.
GP
te
ams
are
trai
ned
in
evid
ence
-bas
ed
appr
oach
es
to
effe
ctiv
e br
ief
inte
rven
tion
coun
selli
ng.
GP
team
sar
e in
volv
ed in
and
info
rmed
of t
he s
ocia
l mar
ketin
gpr
ogra
mm
ean
d ar
e aw
are
of t
heir
role
in
supp
ort
of t
he d
esire
d be
havi
our
chan
geou
tcom
es.
GP
tea
ms
are
prov
ided
with
res
ourc
es a
nd t
ools
(e.
g. c
ompu
ter-
base
dad
vice
/pro
mpt
s an
d pa
tient
reso
urce
s) to
und
erta
ke b
rief i
nter
vent
ions
.
Fun
ding
sys
tem
s ar
e de
velo
ped
to s
uppo
rt G
P t
eam
abi
lity
to d
eliv
erbr
ief
inte
rven
tion
coun
selli
ng.
P
rogr
amm
es
rolle
d ou
t w
itha
best
pr
actic
efr
amew
ork.
PH
Os,
C
MD
HB
, ho
spita
l se
rvic
es,
RN
ZC
GP
Go
al:
P
eop
le
at
risk
o
f d
iab
etes
ar
esc
reen
ed i
n a
tim
ely
man
ner
in
acc
ord
ance
wit
h N
ewZ
eala
nd
gu
idel
ines
.
Tar
get
:B
y 20
10
80%
of
pra
ctic
es
are
effe
ctiv
ely
and
sys
tem
atic
ally
scr
een
ing
for
dia
bet
es a
sd
escr
ibed
in
th
e N
ewZ
eala
nd
Gu
idel
ine
for
the
Ass
essm
ent
and
Man
agem
ent
of
Car
dio
vasc
ula
r R
isk.
CM
DH
Bw
orks
with
PH
Os
to a
ssis
t up
take
of
IT b
ased
dec
isio
n su
ppor
tto
ols
and
man
agem
ent
prot
ocol
s,w
hich
wou
ld f
acili
tate
accu
rate
, ev
iden
ce-
base
d sc
reen
ing
and
follo
wup
act
iviti
es.
Rol
l out
of
scre
enin
g is
alig
ned
with
bro
ader
sys
tem
rev
iew
to
ensu
re t
here
is c
apac
ity to
pro
vide
effe
ctiv
e fo
llow
up
activ
ities
.
CM
DH
B, P
HO
s, H
ealth
Alli
ance
Go
al:
All
new
ly
dia
gn
ose
d
peo
ple
wit
hd
iab
etes
par
tici
pat
e in
qu
alit
y ed
uca
tio
n a
nd
lear
nin
g
to
sup
po
rt
effe
ctiv
e se
lfm
anag
emen
t o
f th
e co
nd
itio
n.
Tar
get
: B
y 20
10 8
0% o
f p
eop
le d
iag
no
sed
wit
h
dia
bet
es
rece
ive
an
enh
ance
ded
uca
tio
n
fro
m
a h
ealt
h
pro
fess
ion
alw
ho
has
rec
eive
dac
cred
ited
tra
inin
g.
Dev
elop
accr
edite
d tr
aini
ng p
rogr
amm
es fo
r pr
imar
y ca
re te
ams
for
diab
etes
educ
atio
n an
dsu
ppor
t fo
r se
lf m
anag
emen
t.
It is
like
ly s
uch
a pr
ogra
mm
eco
uld
be p
rovi
ded
by M
IT, r
esul
ting
in a
form
al q
ualif
icat
ion.
Sup
port
GP
tea
ms
to u
nder
take
tra
inin
g an
d de
velo
pmen
t (t
here
will
bea
need
for
con
sist
ency
acro
ssth
e tr
aini
ng b
ut d
iffer
ent
team
mem
bers
will
requ
ire d
iffer
ent t
rain
ing
mod
ules
).
Col
labo
rate
with
Wai
tem
ata
Dis
tric
t H
ealth
Boa
rd i
n th
e de
velo
pmen
t of
PH
Os,
MIT
, CM
DH
B, W
hitio
ra
Dia
bete
s S
ervi
ce, W
aite
mat
a D
istr
ict
Hea
lth B
oard
57F
INA
L P
LA
N 0
2 F
ebru
ary
2005

58F
INA
L P
LA
N 0
2 F
ebru
ary
2005
reso
urce
s an
d be
st p
ract
ice
mod
els
for
self
man
agem
ent
Intr
oduc
e ‘a
ccre
dite
d’ e
duca
tion/
self
lear
ning
pro
cess
int
o no
rmal
GP
-tea
m
activ
ity.
Rol
l out
trai
ning
pro
gram
mes
acr
oss
GP
team
s.
Go
al:
GP
tea
ms
wo
rk w
ith
wh
ole
fam
ilies
to
b
ette
r su
pp
ort
peo
ple
wit
h d
iab
etes
an
d t
o
hel
p f
amili
es s
tay
hea
lth
y.
Tar
get
:
By
2008
th
e tr
ial
of
new
‘f
amily
g
rou
p’ a
pp
roac
h c
om
ple
ted
an
d e
valu
ated
.
Dev
elop
det
aile
d ev
iden
ce a
nd p
rogr
amm
e de
sign
for
a s
econ
d P
hase
of
the
Chr
onic
C
are
Man
agem
ent
prog
ram
me,
w
hich
su
ppor
ts
GP
te
ams
wor
king
m
ore
clos
ely
with
th
e fa
mili
es
of
peop
le
with
di
abet
es.
The
pr
ogra
mm
e w
ould
inv
olve
a t
rail
with
a l
imite
d nu
mbe
r of
GP
pra
ctic
es
beco
min
g in
volv
ed in
the
new
pro
gram
me,
with
form
al e
valu
atio
n.
Whi
le p
rimar
y ca
re b
ased
, th
e tr
ial
may
hav
e lin
ks t
o th
e ‘fa
mili
es’
actio
n ar
ea o
f Le
t’s B
eat
Dia
bete
s, w
hich
aim
s to
sup
port
vul
nera
ble
fam
ilies
to
mak
e he
alth
y ch
oice
s.
The
pr
ogra
mm
e de
sign
w
ould
in
volv
e tw
o st
ages
of
ac
tivity
; fir
stly
to
de
term
ine
whe
ther
the
app
roac
h is
effe
ctiv
e, a
nd s
econ
dly
to t
est
if it
is
effe
ctiv
e in
an
aver
age
gene
ral p
ract
ice
situ
atio
n.
The
tria
l obj
ectiv
es a
re t
o im
prov
e di
seas
e m
anag
emen
t fo
r th
e pe
rson
with
di
abet
es a
nd a
lso
to id
entif
y an
d re
duce
ris
k fa
ctor
s fo
r th
e fa
mily
mem
bers
.
PH
Os,
RN
ZC
GP
, CC
RE
P, C
MD
HB

9. Enabling Vulnerable Families to Make Healthy
Choices
Context
Many families in Counties Manukau find it very difficult to live healthy lives.
Some families are able to change their behaviour to support a family member who hasdiabetes or to reduce the risk of getting diabetes, but for some families there are somany other difficulties in their lives, making healthy choices is not an option.
Counties Manukau has a high proportion of families that are in difficulty or are‘vulnerable’ and may not be far from a crisis. Vulnerable families may have low incomes through unemployment or low-wage jobs, be new immigrants, have relationship difficulties, suffer from domestic violence or crime, or simply become isolated in their community. It is these vulnerable families, for whom a healthy lifestyleis a low priority, who are most at risk of diabetes. Disease then adds to their difficulties. It is a vicious circle.
Many of the strategies in the Let’s Beat Diabetes plan make it easier for families to make healthy choices (Community Leadership, Well Child, Schools, Social Marketing, Health Promotion, Primary Care-based Prevention), but these strategies on their ownare unlikely to work for vulnerable families. Action is required to help those families most ‘at risk’. Many organisations and agencies support vulnerable families but morefocus is needed on how they work together to support healthy living and self management of disease. A new level of collaboration is required across governmentagencies at policy and funding levels and across providers at operational levels to provide well targeted support for families.
Over the past year, there has been a major government focus on improved support forvulnerable families. This has been reflected in a number of budget initiatives throughthe Ministry of Social Development (MSD), including:
Working for families package – increased number of social support entitlements for working families, such as childcare subsidies, accommodation supplements andreturn to work support.
Family Start expansion – expansion of service aimed at families with very youngchildren who have the greatest needs. It provides early help to improve outcomesfor children by providing intensive cross-government support to parents (coming into Manukau in 2005).
Pacific family violence – funding has been made available to begin implementationof education and awareness programmes as part of the Framework for PreventingFamily Violence in Pacific Communities.
Social workers in schools expansion – social workers in schools supportparticipating families to achieve improvements in their children’s educational, healthand social outcomes as well as improvements in parenting and management ofhousehold resources.
There are also many existing family focused programmes supported by MSD, including: Strengthening Families, Heartlands, Youth Interagency Project, TeenageParents Project, Enhanced case management for people on a sickness benefit andinvalids benefit and Youth Transitions.
59 FINAL PLAN 02 February 2005
MSD has also set up a new service called Family and Community Services (FACS).The FACS’s role is to support government and non government organisations inworking collaboratively to strengthen family support services and make them more effective for families. There is a strong focus on prevention and early intervention.Some of the action areas for FACS include:
The development of a detailed web-based national social services directory that enables social agencies to accurately refer to other support organisations
The Strategies for Kids/Information for Parents (SKIP) programme which aims toprovide positive patenting skills and resources for parents and caregivers ofchildren aged from one to five
A number of programmes which aim at prevention and early intervention of familyviolence
Local services mapping – a framework for determining how services provided by central government, local government and local agencies can be managed to better meet local needs
There are opportunities for the health sector to more effectively interface with the MSDsuite of services to enable families to live healthier lives and better manage disease.
Programme Design
It is proposed MSD take the lead in the development of activities to support families to make healthy choices. MSD has responsibility for Government policy and servicedelivery in many areas of social support, such as Work and Income and FACS. It alsohas links with many other organisations and a history of working closely with the healthsector and local government in Counties Manukau. As noted above, there are a number of new service initiatives and funding streams based in MSD, which candirectly support vulnerable families.
The approach will need to create a sustainable collaboration between health andwelfare at a policy and design level and also at the level of implementation, which would be accomplished through the development of an MSD-led working group. Thisworking group could emerge from one of the existing interagency groups, such as Strengthening Families.
The broad aim is to develop the health sector’s ability to identify vulnerable families and to refer those families to the most appropriate point for ongoing support, and then towork with those support organisations in a co-coordinated manner. For MSD services,there is an opportunity to be involved with families at a point of vulnerability - asopposed to crisis – where families may be more amenable to early intervention. Thereis also opportunity for MSD to better achieve its policy goals such as return-to-work,reduction in disparities and reduction in family violence if it is working with the healthsector.
A number of the programmes will emerge once the working group has beenestablished, however, some areas that have been identified where collaborativeprogrammes should be developed.
Aligning an enhanced Well Child programme (the focuses more strongly onchildhood nutrition) with Strengthening Families and the expanded Family Start
60 FINAL PLAN 02 February 2005

61 FINAL PLAN 02 February 2005
programme to provide improved assessment and referral processes for vulnerable families
Strengthening vulnerable families, within the context of their community, to make healthy choices for themselves and their children
Alignment of the primary care family group intervention trial with family group focused welfare support
Supporting accurate and appropriate referral from health services to welfare support agencies.
Ensuring the local area mapping service programme is undertaken in relation to the health welfare interface and the needs of chronic disease prevention and management.
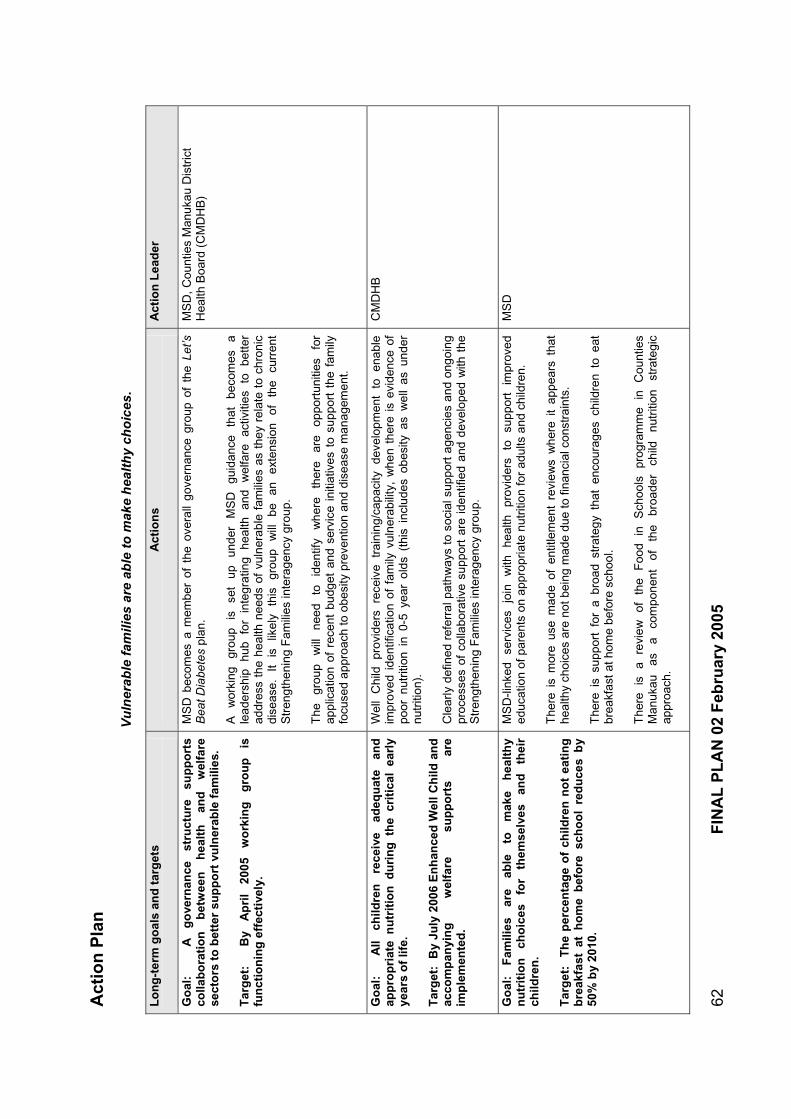
Act
ion
Pla
n
Vu
lner
able
fam
ilies
are
ab
le t
o m
ake
hea
lth
y ch
oic
es.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
er
Go
al:
A
g
ove
rnan
ce
stru
ctu
resu
pp
ort
sco
llab
ora
tio
n
bet
wee
n
hea
lth
an
dw
elfa
rese
cto
rs t
o b
ette
r su
pp
ort
vu
lner
able
fam
ilies
.
Tar
get
:
By
Ap
ril
2005
wo
rkin
gg
rou
pis
fun
ctio
nin
g e
ffec
tive
ly.
MS
D b
ecom
es a
mem
ber
of t
he o
vera
ll go
vern
ance
gro
up o
f th
e Le
t’sB
eat D
iabe
tes
plan
.
Aw
orki
ng
grou
p is
se
t up
un
der
MS
D
guid
ance
th
at
beco
mes
ale
ader
ship
hu
b fo
r in
tegr
atin
g he
alth
an
dw
elfa
re
activ
ities
to
be
tter
addr
ess
the
heal
th n
eeds
of v
ulne
rabl
e fa
mili
es a
s th
ey r
elat
e to
chr
onic
dise
ase.
It
is
likel
y th
is
grou
pw
illbe
an
ex
tens
ion
of
the
curr
ent
Str
engt
heni
ngF
amili
es in
tera
genc
y gr
oup.
The
gr
oup
will
ne
ed
to
iden
tify
whe
re
ther
e ar
eop
port
uniti
esfo
rap
plic
atio
n of
rec
ent
budg
etan
d se
rvic
e in
itiat
ives
to
supp
ort
the
fam
ilyfo
cuse
d ap
proa
ch to
obe
sity
prev
entio
nan
d di
seas
e m
anag
emen
t.
MS
D, C
ount
ies
Man
ukau
Dis
tric
tH
ealth
Boa
rd (
CM
DH
B)
Go
al:
All
child
ren
re
ceiv
ead
equ
ate
and
app
rop
riat
e n
utr
itio
n d
uri
ng
th
e cr
itic
al e
arly
year
s o
f lif
e.
Tar
get
: B
yJu
ly20
06 E
nh
ance
d W
ell C
hild
an
dac
com
pan
yin
gw
elfa
resu
pp
ort
sar
eim
ple
men
ted
.
Wel
l C
hild
pr
ovid
ers
rece
ive
trai
ning
/cap
acity
de
velo
pmen
t to
en
able
impr
oved
iden
tific
atio
n of
fam
ily v
ulne
rabi
lity,
whe
n th
ere
is e
vide
nce
ofpo
or n
utrit
ion
in 0
-5ye
ar o
lds
(thi
s in
clud
es o
besi
ty a
sw
ell
as u
nder
nutr
ition
).
Cle
arly
defin
ed r
efer
ral p
athw
ays
to s
ocia
l sup
port
age
ncie
s an
don
goin
gpr
oces
ses
of c
olla
bora
tive
supp
ort
are
iden
tifie
d an
d de
velo
ped
with
the
Str
engt
heni
ngF
amili
es in
tera
genc
y gr
oup.
CM
DH
B
Go
al:
Fam
ilies
ar
e ab
le
to
mak
e h
ealt
hy
nu
trit
ion
ch
oic
es
for
them
selv
esan
d
thei
rch
ildre
n.
Tar
get
: T
he
per
cen
tag
e o
f ch
ildre
n n
ot
eati
ng
bre
akfa
st a
t h
om
e b
efo
re s
cho
ol
red
uce
s b
y50
% b
y 20
10.
MS
D-li
nked
se
rvic
es
join
with
he
alth
prov
ider
s to
su
ppor
t im
prov
eded
ucat
ion
of p
aren
ts o
n ap
prop
riate
nut
ritio
n fo
r ad
ults
and
chi
ldre
n.
The
re i
s m
ore
use
mad
e of
ent
itlem
ent
revi
ews
whe
reit
appe
ars
that
heal
thy
choi
ces
are
not b
eing
mad
e du
e to
fina
ncia
l con
stra
ints
.
The
re i
s su
ppor
t fo
r a
broa
d st
rate
gy t
hat
enco
urag
es c
hild
ren
to e
atbr
eakf
ast a
t hom
e be
fore
sch
ool.
The
re
is
a re
view
of
th
e F
ood
in
Sch
ools
pr
ogra
mm
e in
C
ount
ies
Man
ukau
asa
com
pone
nt
of
the
broa
der
child
nu
triti
on
stra
tegi
cap
proa
ch.
MS
D
62F
INA
L P
LA
N 0
2 F
ebru
ary
2005

63F
INA
L P
LA
N 0
2 F
ebru
ary
2005
Go
al:
Im
pro
ved
wh
ole
sys
tem
ap
pro
ach
es t
o
pre
ven
tio
n
and
ea
rly
inte
rven
tio
n
are
dev
elo
ped
.
Tar
get
:
By
2008
H
ealt
h
and
w
elfa
re
fam
ily
gro
up
inte
rven
tio
n t
rial
co
mp
lete
d.
The
prim
ary
care
bas
ed t
rial
of f
amily
gro
up i
nter
vent
ions
als
o in
clud
es
expl
icit
linka
ge
with
w
hole
fa
mily
ba
sed
appr
oach
es
from
w
elfa
re
agen
cies
. T
he t
rial w
ill b
e ab
le t
o id
entif
y th
e va
lue
of t
his
cros
s ag
ency
w
hole
fam
ily a
ppro
ach
for
wor
king
with
hig
h ris
k fa
mili
es.
Wel
fare
age
ncie
s ne
ed to
be
invo
lved
in d
evel
opm
ent o
f the
tria
l des
ign.
CM
DH
B
Go
al:
In
crea
se e
ffec
tive
su
pp
ort
fo
r fa
mili
es
thro
ug
h
app
rop
riat
e re
ferr
al
bet
wee
n
hea
lth
an
d w
elfa
re a
gen
cies
.
Tar
get
:
By
July
20
05
nat
ion
al
dir
ecto
ry
is
up
dat
ed a
nd
mar
kete
d t
o h
ealt
h s
ervi
ces.
Rev
iew
the
app
licab
ility
of
the
Fam
ily a
nd C
omm
unity
Ser
vice
s w
eb
base
d na
tiona
l se
rvic
es d
irect
ory
as a
cor
e to
ol f
or u
se i
n su
ppor
ting
appr
opria
te
refe
rral
be
twee
n he
alth
an
d w
elfa
re
agen
cies
. E
nhan
cem
ents
cou
ld i
mpr
ove
the
usef
ulne
ss o
f th
e di
rect
ory
for
heal
th
prov
ider
s.
Mar
ket u
se o
f the
nat
iona
l dire
ctor
y to
hea
lth s
ervi
ces.
MS
D
Go
al:
T
her
e is
a
clea
r lo
ng
te
rm
stra
teg
y id
enti
fied
fo
r se
rvic
e st
ruct
ure
s th
at w
ill m
ost
ap
pro
pri
atel
y m
eet
the
nee
ds
of
the
Co
un
ties
M
anu
kau
po
pu
lati
on
.
Tar
get
: P
apak
ura
ser
vice
map
pin
g c
om
ple
te
by
the
end
of
2005
.
The
Loc
al S
ervi
ces
map
ping
initi
ativ
e by
FA
CS
will
exp
licitl
y fo
cus
on th
e ne
eds
of t
he h
ealth
/wel
fare
/edu
catio
n in
terf
ace
in r
elat
ion
to v
ulne
rabl
e fa
mili
es a
nd d
evel
op a
long
term
str
ateg
y fo
r se
rvic
e de
velo
pmen
t.
MS
D

10.Improving Service Integration and Care for
Advanced Disease
Context
The Let’s Beat Diabetes plan has a strong focus on stopping diabetes through whole-society strategies. It also supports primary care to have a greater capacity to preventdiabetes, identify diabetes early, and support lifestyle change to slow or stop diseaseprogression. However, many people already have advanced diabetes and will continueto get serious complications from diabetes despite better prevention.
For most people with diabetes, the disease gets steadily worse over time. The averagetime from diagnosis to death for diabetes for Europeans is approximately 22 years, Pacific peoples approximately 20 years, and Maori approximately 18 years (Ministry ofHealth, 2002). The complications from diabetes include heart disease, kidney failure,stroke, blindness and ulceration/amputation of lower limbs. The disease leads to suffering for the patient and also cost for the health sector. In 2003, diabetes-relatedcost for the top 20 diabetes patients at Counties Manukau District Health Board’s(CMDHB) inpatient and outpatient service was $77,000 to $170,000 per patient (Thomas E, 2004). The average cost of clinic-based haemodialysis is $45,000 a year.
There is very good evidence that best practice health interventions and lifestyle changecan make a significant difference to the outcomes of people who have diabetes,including people with advanced diabetes with serious complications (UKPDS, 1975 - 204).
A number of initiatives have been introduced at a national, regional and district level tosupport more effective care and treatment for people with diabetes, including:
National level
Get Checked - a national programme, where General Practitioners (GPs) are paid$40 to provide a recall and check-up for people with diabetes – and to provide datafor a national database. (There is currently a review of the electronic support for theGet Checked programme).
Care Plus - a national funding initiative that provides GP teams with $200 a year toprovide extra care for people with chronic disease. It can be applied to supportstructured care for people with diabetes.
National Diabetes Guidelines – The New Zealand Guidelines Group publishedevidence based best practice guidelines for the management of Type 2 Diabetes inDecember 2003, including a view on Maori and Pacific perspectives onmanagement.
Electronic decision support tools – the Ministry of Health has funded the publishingof the guidelines within an electronic decision support environment. The guidelineswill be embedded in the Predict decision support tool and are expected to bereleased in early 2005.
Regional level
Dialysis review – a regional review of dialysis services, access criteria and demandmanagement strategies is currently underway in collaboration between theWaitemata, Auckland and Counties Manukau District Health Boards (DHBs).
64 FINAL PLAN 02 February 2005

Chronic disease strategy review – there is currently an analysis of the approachesto chronic disease management being taken by the four northern DHBs, looking at areas of convergence and divergence in approaches and at the risks and opportunities associated with the current approaches, with a view to developing more effective regional collaboration.
Activities of other DHBs – Auckland DHB is working with Primary Health Organisations(PHOs) to provide enhanced primary-care-based services for people with advanceddiabetes, similar to services provided under the Chronic Care Management (CCM) programme. Waitemata DHB is focusing on improving PHO-based retinal screeningand intensive education post diagnosis to support improved self management.Waitemata has also introduced a practice based quality and learning cycle – based broadly on the Institute of Healthcare Improvement’s ‘Collaborative Model for AchievingBreakthrough Improvement.’ The learning programme is delivered in partnership withthe Royal New Zealand College of General Practice (RNZCGP). Across the threeAuckland DHBs, similar frameworks to diabetes management are emerging, all involving defined levels of care intensity, with associated expectation of serviceresponse.
District level
Chronic Care management - Counties Manukau has for the past five years beendeveloping and implementing the CCM programme, which aims to provide qualitymanagement of diabetes within the primary care environment. CCM involvestraining and development for practice teams, increased levels of nurse-basedsupport, structured care and an Information Technology (IT) system that supports GP decisions and provides reports on how patients are responding. CCM alsoprovides GPs with extra funding to carry out the structured care activities and itreduces the financial barriers for people to access GPs.
Retinal Screening – In 2003 the Counties Manukau Diabetes Advisory Group(CMDAG) commissioned a review was undertake to develop improved co-ordination, clinical pathways and capacity development for diabetes retinal screening services. The recommendations of that review are now beingimplemented.
Gestational diabetes – A project is currently under way to provide better integrationbetween hospital and primary care services to support women with diabetes tohave healthy babies and to provide better follow up of women with gestational diabetes.
Community pharmacy – a strategy is being developed to improve the contribution pharmacists make to the management of chronic disease through providing adviceto practice teams and through enhanced counseling services for patients on correctuse of medicines and improving adherence to medication regimes.
As the above list of existing and emerging activities show, there is no shortage of newprogrammes and review processes in the treatment and management of diabetes. Themajor issue for improving diabetes outcomes is the effective uptake of best practiceprocesses in the general practice environment and the co-ordination of services across primary and secondary care. There are few practices which are currently working atthe level of identifying and managing diabetes in a manner which meets the national guidelines.
The CCM programme has recently released information which shows that whilst the early adopter practices were making a significant change in outcomes due to taking upthe CCM structured care approach, late adopter practices are not making the same
65 FINAL PLAN 02 February 2005

66 FINAL PLAN 02 February 2005
impact, despite financial incentives and considerable IT support. This outcome illustrates the difficulties in introducing chronic disease based programmes that require culture and systems change into the general practice environment. In other words, some of the major impacts on patient outcomes for diabetes are not patient characteristics or programme design but provider characteristics and capacity.
Progress is not being held back by a lack of ideas, but the need for effective implementation.
Programme Design
The objective of the programme design is to develop robust and sustainable systems that support broad primary care uptake of best practice care and improved integration with secondary care. Achieving this improved uptake of innovations requires a multifaceted change management programme, with strong governance, management (including knowledge management) and clinical leadership, as well as investment in workforce capacity and the use of innovative funding mechanisms.
The proposals outlined below are wide ranging and will challenge existing roles and relationships, however, this type of systems approach is required if the sector is to take on the changes required to effectively manage diabetes and other chronic diseases. The programme design supports:
Developing an improved framework for delivering care and organising integration
Creating an improved governance and management framework for diabetes care
Developing improved medical and nursing clinical leadership and a centre of excellence for whole system diabetes management
Creating an explicit learning collaboration to support innovation adoption, which includes general practice and secondary care
Building a sustainable and professionalised education courses/qualifications for the educational aspects of chronic disease management
Bringing various IT developments together to create a unified system
Defining a funding structure that incentivises outcomes as well as inputs
Building process and outcome evaluation to support whole system learning.

Act
ion
Pla
n
Peo
ple
wit
h d
iab
etes
are
man
aged
acc
ord
ing
to
the
New
Zea
lan
d b
est
pra
ctic
e g
uid
elin
es.
Lo
ng
-ter
m g
oal
s an
d t
arg
ets
Act
ion
sA
ctio
n L
ead
er
Go
al:
Dia
bet
es m
anag
emen
t ac
tivi
ties
are
imp
lem
ente
d
effe
ctiv
ely
in
a co
nsi
sten
tfr
amew
ork
acr
oss
pri
mar
yan
d s
eco
nd
ary
care
.
Tar
get
:B
y 20
05
fram
ewo
rk
for
care
agre
ed.
An
orga
nisi
ng f
ram
ewor
k fo
r di
abet
es c
ross
-sec
tor
man
agem
ent
is d
evel
oped
and
endo
rsed
tha
t lin
ks t
o th
e N
Z G
uide
lines
,is
sup
port
edby
fund
ing
fram
ewor
ks a
nd i
sco
ngru
ent
with
oth
er D
HB
sin
the
Auc
klan
d re
gion
. Alig
nw
ith r
etin
al s
cree
ning
pro
ject
,di
alys
is r
evie
w, g
esta
tiona
l dia
bete
s re
view
, nat
iona
l dev
elop
men
ts.
An
outli
ne o
f co
re a
ctiv
ities
to
be u
nder
take
n is
dev
elop
ed(w
ith u
sefu
l re
fere
nce
toW
aite
mat
a D
HB
wor
k)
in
part
ners
hip
betw
een
DH
B
and
PH
Os.
Rol
es
and
resp
onsi
bilit
ies
of v
ario
us s
ecto
r pa
rtne
rs a
re c
larif
ied.
Fun
ding
and
sup
port
mec
hani
sms
are
deve
lope
d,w
ith p
rogr
amm
e of
impl
emen
tatio
n.
CM
DH
B, P
HO
s, W
hitio
ra, W
DH
B
Go
al:
Dia
bet
es
go
vern
ance
st
ruct
ure
ssu
pp
ort
a
wh
ole
sy
stem
view
an
dm
anag
emen
t.
Tar
get
:
New
go
vern
ance
st
ruct
ure
in
pla
ce b
y Ju
ly20
05.
The
cur
rent
str
uctu
re a
nd t
erm
s of
ref
eren
ce o
f th
e D
iabe
tes
Adv
isor
y G
roup
and
the
Chr
onic
Car
e M
anag
emen
t G
over
nanc
eG
roup
s ar
e re
view
edw
ith a
nob
ject
ive
of
ensu
ring
ther
e is
effe
ctiv
e cr
oss
sect
or g
over
nanc
e of
issu
es a
nd p
rogr
amm
es a
cros
sal
l lev
els
of d
iabe
tes
man
agem
ent,
incl
udin
g ou
tpat
ient
ser
vice
s.
Gov
erna
nce
and
asso
ciat
ed m
anag
emen
tro
les
and
rela
tions
hips
acr
oss
PH
Os
and
DH
B a
re d
efin
ed a
nd im
plem
ente
d.
CM
DH
B, P
HO
s
Go
al:
Asu
stai
nab
le l
earn
ing
en
viro
nm
ent
is
crea
ted
wh
ich
su
pp
ort
s u
pta
keo
fse
rvic
e in
no
vati
on
s in
p
rim
ary
and
se
con
dar
y ca
re.
Tar
get
:
Init
ial
lear
nin
g
colla
bo
rati
veb
egin
s Ju
ly 2
005,
ru
ns
for
six
mo
nth
s.
30%
of
GP
s h
ave
par
tici
pat
ed in
a le
arn
ing
colla
bo
rati
on
by
2010
.
CM
DH
B,
PH
Os
and
the
RN
ZC
GP
set
up
anap
proa
ch t
o le
arni
ng a
mon
gst
prac
tice
team
s ba
sed
on
the
lear
ning
an
d ac
tion
cycl
esde
scrib
ed
in
the
Col
labo
rativ
eA
ppro
ach
to B
reak
thro
ugh
Impr
ovem
ents
lite
ratu
re.
The
obj
ectiv
eof
the
pro
ject
is t
om
ove
aver
agel
ype
rfor
min
gm
ains
trea
m p
ract
ices
tow
ards
bes
t pr
actic
e ac
tivity
and
achi
evin
g th
e pe
rfor
man
ce s
tand
ards
set
by
exis
ting
lead
ing
prac
tices
.
Set
le
arni
ng
obje
ctiv
es,
choo
se
colla
bora
ting
part
ners
, de
sign
st
ruct
ure
ofle
arni
ng/a
ctin
g cy
cles
, pr
ovid
e fu
ndin
g to
sup
port
pr
actic
e te
am r
elea
se t
ime
for
lear
ning
cyc
les.
Impl
emen
t ini
tial B
reak
thro
ugh
Col
labo
ratio
n,w
ith c
olla
bora
tive
grou
ps e
xpan
ding
ove
rfiv
eye
ars
to in
clud
e in
crea
sing
num
ber
of p
ract
ices
.
CM
DH
B, P
HO
s, W
hitio
ra, R
NZ
CG
P
Go
al:
Th
ere
is e
ffec
tive
clin
ical
lead
ersh
ipfo
r th
e d
eliv
ery
of
inte
gra
ted
d
iab
etes
man
agem
ent
stra
teg
ies.
Rec
ogni
se a
nd e
nhan
ce t
he r
ole
of t
he W
hitio
ra M
iddl
emor
e D
iabe
tes
Ser
vice
as
the
dist
rict
cent
re o
f ex
celle
nce
for
who
le s
yste
m c
linic
al d
esig
n, p
rovi
ding
sect
orw
ide
med
ical
, nu
rsin
g an
d di
seas
e ps
ycho
logy
expe
rtis
e, p
rogr
amm
e co
nten
t le
ader
ship
and
capa
city
dev
elop
men
t for
the
wid
er s
ecto
r.
Whi
tiora
, CM
DH
B
67F
INA
L P
LA
N 0
2 F
ebru
ary
2005
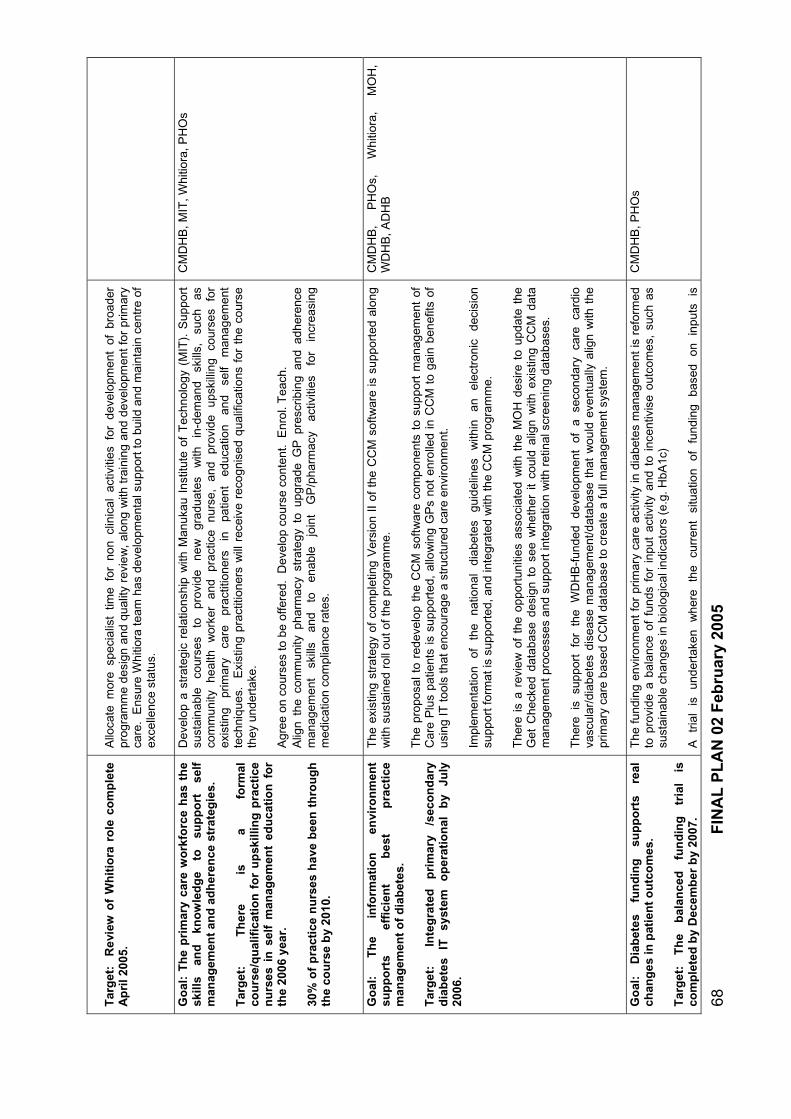
Tar
get
: R
evie
w o
f W
hit
iora
ro
le c
om
ple
te
Ap
ril 2
005.
Allo
cate
mor
e sp
ecia
list
time
for
non
clin
ical
act
iviti
es f
or d
evel
opm
ent
of b
road
erpr
ogra
mm
e de
sign
and
qual
ity r
evie
w,a
long
with
trai
ning
and
deve
lopm
ent f
or p
rimar
yca
re.
Ens
ure
Whi
tiora
team
has
deve
lopm
enta
l sup
port
to b
uild
and
mai
ntai
n ce
ntre
of
exce
llenc
e st
atus
.
Go
al:
Th
e p
rim
ary
care
wo
rkfo
rce
has
th
esk
ills
and
kn
ow
led
ge
to
sup
po
rt
self
man
agem
ent
and
ad
her
ence
str
ateg
ies.
Tar
get
: T
her
e is
a
form
alco
urs
e/q
ual
ific
atio
n f
or
up
skill
ing
pra
ctic
e n
urs
es i
n s
elf
man
agem
ent
edu
cati
on
fo
r th
e 20
06 y
ear.
Dev
elop
a s
trat
egic
rel
atio
nshi
pw
ith M
anuk
au I
nstit
ute
of T
echn
olog
y (M
IT).
Sup
port
su
stai
nabl
e co
urse
s to
pr
ovid
e ne
wgr
adua
tes
with
in
-dem
and
skill
s,
such
as
com
mun
ity
heal
thw
orke
r an
d pr
actic
e nu
rse,
an
d pr
ovid
e up
skill
ing
cour
ses
for
exis
ting
prim
ary
care
pr
actit
ione
rs
inpa
tient
ed
ucat
ion
and
self
man
agem
ent
tech
niqu
es.
Exi
stin
g pr
actit
ione
rsw
ill r
ecei
ve r
ecog
nise
d qu
alifi
catio
ns f
or t
he c
ours
eth
ey u
nder
take
.
30%
of
pra
ctic
e n
urs
es h
ave
bee
n t
hro
ug
hth
e co
urs
e b
y20
10.
Agr
ee o
n co
urse
s to
be
offe
red.
Dev
elop
cou
rse
cont
ent.
Enr
ol. T
each
.A
lign
the
com
mun
ity p
harm
acy
stra
tegy
to
upgr
ade
GP
pre
scrib
ing
and
adhe
renc
em
anag
emen
t sk
ills
and
to
enab
le
join
t G
P/p
harm
acy
activ
ities
fo
r in
crea
sing
med
icat
ion
com
plia
nce
rate
s.
CM
DH
B, M
IT, W
hitio
ra, P
HO
s
Go
al:
Th
e in
form
atio
n
envi
ron
men
tsu
pp
ort
sef
fici
ent
bes
t p
ract
ice
man
agem
ent
of
dia
bet
es.
Tar
get
:
Inte
gra
ted
p
rim
ary
/sec
on
dar
yd
iab
etes
IT
syst
em
op
erat
ion
al
by
July
2006
.
The
exi
stin
g st
rate
gy o
f co
mpl
etin
g V
ersi
on I
I of
the
CC
M s
oftw
are
is s
uppo
rted
alon
gw
ith s
usta
ined
roll
out o
f the
pro
gram
me.
The
pro
posa
l to
rede
velo
p th
e C
CM
sof
twar
e co
mpo
nent
sto
sup
port
man
agem
ent
ofC
are
Plu
s pa
tient
s is
sup
port
ed,
allo
win
gG
Ps
not
enro
lled
in C
CM
to
gain
ben
efits
of
usin
g IT
tool
s th
at e
ncou
rage
a st
ruct
ured
car
e en
viro
nmen
t.
Impl
emen
tatio
n of
th
e na
tiona
l di
abet
esgu
idel
ines
with
in
an
elec
tron
ic
deci
sion
supp
ort f
orm
at is
sup
port
ed, a
nd in
tegr
ated
with
the
CC
M p
rogr
amm
e.
The
re i
s a
revi
ewof
the
opp
ortu
nitie
s as
soci
ated
with
the
MO
H d
esire
to
upda
te t
heG
et C
heck
edda
taba
sede
sign
to
see
whe
ther
it
coul
d al
ign
with
exis
ting
CC
M d
ata
man
agem
ent p
roce
sses
and
sup
port
inte
grat
ion
with
ret
inal
scre
enin
g da
taba
ses.
The
re
is
supp
ort
for
the
WD
HB
-fun
ded
deve
lopm
ent
of
a se
cond
ary
care
ca
rdio
vasc
ular
/dia
bete
s di
seas
e m
anag
emen
t/dat
abas
e th
atw
ould
eve
ntua
llyal
ign
with
the
prim
ary
care
bas
ed C
CM
dat
abas
e to
cre
ate
a fu
ll m
anag
emen
t sys
tem
.
CM
DH
B,
PH
Os,
W
hitio
ra,
MO
H,
WD
HB
, AD
HB
Go
al:
Dia
bet
es
fun
din
g
sup
po
rts
real
chan
ges
in p
atie
nt
ou
tco
mes
.
Tar
get
: T
he
bal
ance
d
fun
din
g
tria
l is
com
ple
ted
by
Dec
emb
er b
y20
07.
The
fund
ing
envi
ronm
ent f
or p
rimar
y ca
re a
ctiv
ityin
dia
bete
s m
anag
emen
t is
refo
rmed
to p
rovi
dea
bala
nce
of f
unds
for
inp
ut a
ctiv
ityan
d to
inc
entiv
ise
outc
omes
, su
ch a
ssu
stai
nabl
e ch
ange
s in
bio
logi
cal i
ndic
ator
s (e
.g. H
bA1c
)
A
tria
l is
un
dert
aken
whe
re
the
curr
ent
situ
atio
n of
fu
ndin
g ba
sed
on
inpu
ts
is
CM
DH
B, P
HO
s
68F
INA
L P
LA
N 0
2 F
ebru
ary
2005

69F
INA
L P
LA
N 0
2 F
ebru
ary
2005
com
pare
d w
ith a
bal
ance
d fu
ndin
g st
rate
gy w
here
the
re is
a s
plit
of in
cent
ives
acr
oss
inpu
ts a
nd o
utco
mes
.
Go
al:
Eva
luat
ion
p
rovi
des
ev
iden
ce
of
effe
ctiv
enes
s o
f in
vest
men
t in
sy
stem
ca
pac
ity
The
Cen
tre
for
Clin
ical
Res
earc
h an
d E
ffect
ive
Pra
ctic
e (C
CR
EP
) de
velo
ps a
pro
cess
an
d ou
tcom
e ev
alua
tion
fram
ewor
k fo
r th
e ab
ove
stra
tegi
es
and
links
w
ith
the
RN
ZC
GP
in s
uppo
rtin
g a
plan
-do-
stud
y-ac
t qua
lity
cycl
e am
ongs
t gen
eral
pra
ctic
e.
CC
RE
P, R
NZ
CG
P, C
MD
HB
, SoP
H
Enablers
Let’s Beat Diabetes is not only about diabetes prevention and management, but aboutthe types of changes society and the health sector need to make to better prevent and manage a number of chronic diseases, most obviously heart disease.
The change required challenges how the many different parts of the health sectoroperate, particularly the role of the District Health Board. The plan is divided into theTen Action Areas. However, there are many cross cutting themes, capacity andsystems issues that require proactive management to create an environment that inconducive to change. Some of these will require DHB management; others willemerge as the plan’s development process continues.
1. Consumer involvement
There is currently no well supported consumer forum to support consumer consultationabout issues of service design and quality. There are some existing consumer groups,one of these could be supported and expanded or a new group developed. Theconsumer group should include people from various ethnicities and stages of diabetesprogression. The group should also receive training and development in effectiveadvocacy. There may be an opportunity to more effectively use existing communityvehicles and networks, such as community boards, to support consumer involvement.
2. Maori and Pacific peoples
The priority placed on Maori and Pacific diabetes outcomes means that there needs tobe a special focus through the plan to ensure that Maori and Pacific health needs arebeing met in all Ten Action Areas. There needs to be separate stand-alone plans forMaori and Pacific peoples that pull together all aspects of the broader Let’s BeatDiabetes plan into one document to provide focused communication about the plan for Maori and Pacific communities. The strategies designed to assist Maori and Pacific peoples are outlined below:
Community Action Fund: This fund will enable Maori and Pacific communityorganisations, marae and churches to apply for funding to support activities which prevent diabetes and support people with diabetes.
Focus on marae/kura: The Maori leadership strategy supports the development ofmarae and kura as health promoting environments through knowledge, cultural lore and activities.
Focus on churches: The Pacific leadership strategy supports the development ofmulti-ethnic strategy that is responsive to each of the Pacific peoples and enables Pacific churches to support the physical as well as spiritual health of their congregation.
Cultural training (professionalise in primary care): The professionalisation of upgrading skills within primary care will enable greater uptake of training in cultural issues and safety.
Health Promotion capacity: Maori and Pacific health promotion providers willreceive more support for capacity development and more opportunity forprogramme developments, plus more effective links with mainstream providers.
Family/whanau focus to work: The core family focus to the strategy aligns with the national He Korowai Oranga (Maori Health Strategy) and Pacific Health and
70 FINAL PLAN 02 February 2005

Disability Action plan. The family focus is illustrated in the Vulnerable Familiesstrategy and in the ‘family group’ trial of the Prevention Focused Primary Carestrategy.
Targeted social marketing: The social marketing programme will target Maori andPacific peoples in an encouraging environment and provide practical information onlifestyle change.
Evaluation of outcomes for Maori and Pacific peoples: The evaluation frameworkwill develop special considerations for process and outcomes issues for Maori and Pacific peoples, utilise Maori and Pacific researchers and include communities inprocess.
3. Funding Environment
One of the key functions of CMDHB in creating a supportive environment for Let’s BeatDiabetes is to provide resources for action and to realign existing resources under itscontrol and influence resources under the control of other organisations. Fundingactivities required to support the plan include:
Aligned Health Promotion Funding: CMDHB will work with other funding organisations in the health promotion area to gain greater synergy between fund allocation in terms of programme design, target group and capacity building in thesector.
Sustained upstream funding: CMDHB will provide an estimate about a level offunding that will be allocated to the Let’s Beat Diabetes strategy for a period of five years, so that there is security from the health sector and confidence from non-health partners that diabetes is a priority area and CMDHB is committed tosustained action for the five years of the plan.
Balanced primary care input/outcome incentives: The funding for activities within the primary care environment will be reviewed to see if improved outcomes can beachieved by a balanced funding strategy across inputs and outcomes – as opposedto purely funding inputs as is currently the case.
Allocation to evaluation: A proportion of the overall investment in Let’s BeatDiabetes will be set aside for evaluation.
Seeking matched funding with other agencies: Where possible CMDHB will seekmatched funding or resource input from other agencies in new areas of activitywhere there is cross agency jurisdiction and interest in order to maximise societal investment in diabetes prevention. This may include sponsorship in some areas.
Support for specific strategies and the Community Action Fund: Funds will be allocated to support specific strategies outlined in the Let’s Beat Diabetes plan andthere will also be a general fund which will allocate small grants to community organisations to support diabetes prevention programmes that work within aparadigm of cultural strength and community empowerment.
4. Learning Environment
Let’s Beat Diabetes proposes strategies that expand health sector activity and society efforts into challenging new areas of activity. The plan will not succeed unless thereare strong evaluation and learning frameworks to support continual reassessment andfine turning of activities and to know whether the plan is having the desired impact.
Overall evaluation – continuous quality improvement: It is proposed that CMDHB develop a partnership with the University of Auckland School of Population Health
71 FINAL PLAN 02 February 2005
(UoA-SoPH) and Counties Manukau communities to develop an evaluationframework that sits across the entire 10 strands of the plan and the governanceprocess. The evaluation would be designed to measure outcomes but to also support a process of learning through a continuous quality improvement cycle.
PDSA cycle – Breakthrough Collaboration: Approaches will be made to GPs,PHOs and the Royal New Zealand College of General Practice to implement a series of action learning cycles (based loosely on the IHI Breakthrough Collaborations) to support uptake of innovations by GPs and to better understandthe blockages to innovation adoption.
Workforce development – education and self management: A major issue for primary care and to some extend in secondary care is the need for there to beimproved expertise in patient education, motivational interviewing and support for self management. This requirement applies to all chronic disease, not justdiabetes. There needs to be a move to a proper professionalised course based inan education institute that can access education funding streams, provide new skills to a wider range of health professionals, deliver a recognised qualification andcreate a common language and approach to help foster a new paradigm in the management of chronic disease. There is also a need to enhance training opportunities for a broad range of community workers so they are better able tocontribute to community wellness and chronic disease management.
Mangere schools evaluation: The UoA research project into the impact of healthinterventions at secondary schools should be supported as it provides an opportunity to accurately quantify the impact and outcomes of such interventions and build an evidence base for ongoing investment in schools programmes.
5. Sustainable Governance
The development of a sustainable governance structure will require a strong andinclusive initial structure, powerful links to the action areas, the delivery of value for participating organisations and individuals and good administration support:
Overarching governance model: The overarching governance group for Let’s BeatDiabetes will guide the plan implementation. The group will have representationfrom all Ten Action Areas, plus key partnership organisations, community leaders,clinical experts and consumers.
Links to Tomorrow’s Manukau: The governance group will link with the Health andWellbeing sub committee of the Tomorrow’s Manukau group to ensure that the partnership and information flow with Manukau City Council (MCC) and other key government agencies is maintained.
Leadership Hubs for each area: Each of the Ten Action Areas will have its own leadership hub or group. The make-up of each hub will differ as each will havedifferent requirements. For example, the Food Group will differ from the Well Childgroup. Different organisations will lead each area. For example, Ministry of SocialDevelopment will lead the Vulnerable Families area, whereas Manukau City Council will lead the Urban Design area. The ‘action leader’ approach is similar tothat used in the Tomorrow’s Manukau plan.
Administration support: CMDHB will support resources and networks to provideoverall administrative co-ordination of the various work streams.
72 FINAL PLAN 02 February 2005
6. Organisational Development
The development of appropriate and trained workforce may be the single mostimportant factor for enabling primary care to meet the challenge of improved chronicdisease management. Workforce development must be a priority. Health programmes also require strong professional leadership. It is proposed that the Whitiora DiabetesService is supported to maintain a centre of excellence status with regards to wholesystem diabetes management. CMDHB will also have to look to its own capacity inorder to support Let’s Beat Diabetes. It is proposed that enabling cross-sector learningcould be a central pillar to the DHB role:
Workforce – new workforce and training in primary care: Modeling has shown that there is likely to be a substantial demand for practice nurses and community healthworkers as primary care changes to support improvements in chronic diseasemanagement. There will also be requirements for proportionally more dieticians, psychologists, nurse practitioners, nurse specialists, social workers, pharmacists as part of the primary care team but these are likely to be provided by existing marketplace mechanisms. Indications are that there will be shortages in practice nurses and community workers unless proactive activity is undertaken to develop an increased workforce.
There is also a need to professionalise the upskilling of the existing primary careteams (discussed under the ‘Learning Environment’ heading).
Workforce – constraints within secondary care: If the current increase in dialysis continues there is a high likelihood that the existing global shortage ofnephrologists will become an acute issue in terms of quality and capacity. Forwardplanning is required across the entire area of demand and service capacity for dialysis.
Whitiora centre of excellence – clinical leadership: Middlemore Whitiora DiabetesService currently provides the clinical base and centre of excellence that has drivenmuch of the capacity increase across primary care, through training, advice andsupport for nursing and medical practitioners. The Whitiora team is under considerable pressure from clinical workloads and needs to be able to retain astrong strategic role in broad guidance across clinical issues and whole system capacity and processes as they relate to best practice care for people withdiabetes.
Let’s Beat Diabetes creates greater demand for centre-of-excellence medical,nursing and health psychologist leadership. Investment in increased medicalspecialist time devoted to system-wide clinical leadership and ongoing developmentof nursing staff in their nurse specialist roles is required to implement the system improvements outlined in the plan.
DHB co-ordination and system change model: Let’s Beat Diabetes challenges therole of the DHB in system change. How much is CMDHB a hands-off policy/funding organisation and to what extent does it become involved in themanagement of programmes and change processes? CMDHB is already involvedat quite a detailed level with broad whole system processes, like the CCM programme. While there will be leadership from many organisations andcommunities with the plan implementation, there will still have to be a core administrative heart across the wider process – and this role legitimately falls to the DHB as it has the requisite administrative, management, policy and strategic skillsand the governance mandate.
It is suggested that CMDHB focus its attention strong on the whole system learningrequirements of the plan. The plan will not work with a purely top down command and
73 FINAL PLAN 02 February 2005

control structure. A network based learning environment will need to be encouragedwhich is supported with robust proven, learning processes and with regularperformance information from the evaluation process.
In this manner, CMDHB will develop a core competency in directing and encouraging learning and innovation adoption within the health environment, which will be importantto its ongoing effectiveness as a leadership organisation.
7. Information Systems
There are many powerful information systems tools to support clinical decisions,patient administration and performance measurement. At present there are a numberof unlinked systems that have the potential to become better aligned/linked/integratedto form a complete system of clinical management support for people with diabetes:
CCM Version II/CCM Care Plus/ Ministry guidelines in Predict: Complete thedevelopment of the CCM Version II plan to make the CCM tools more useful and user friendly, update the CCM tools to support the clinical and administrative tasks associated with the Care Plus disease management activities and include the new guideline-based decision support tools in the CCM suite of tools.
Screening – CV/diabetes: Provide general practice with the ability to undertakedecision-support-assisted screening for CV risk and diabetes according to the NewZealand guidelines. There may have to be a dual approach. The preferredapproach of embedding the screening tools and activity within the CCM suite of tools, and the contingency plan for those GPs who appear unlikely to take up CCM of supporting web based screening and risk assessment decision support tools.The objective is to maximise the penetration of screening and introduce general practice to the use of decision support tools to assist clinical activities.
Get Checked – annual check database: The national data system that supports theDiabetes Get Checked programme should be aligned, or at least linked, with the CCM system to allow for simplified user data entry and reporting.
WDHB secondary care module: Waitemata District Health Board is investing in thedevelopment of a secondary care based clinical support system and database for diabetes and cardiovascular disease. This system is being designed to fit with theCCM system to create a wider whole clinical system for primary and secondary care management of CV and diabetes. Counties Manukau needs to maintain close links with the development of the Waitemata system to see where the synergies liewith Counties Manukau secondary care needs and that issues of integration withthe existing CCM system are managed from the user perspective.
Advice only support for brief interventions and self management counseling andresources on line: A scoping study should be undertaken as to the practicality and value of the CCM platform being used to support brief intervention counseling and patient education via on-line evidence-based advice for practice staff and theprovision of online education resources.
74 FINAL PLAN 02 February 2005

Part III
Implementation
75 FINAL PLAN 02 February 2005

Executive Summary
Let’s Beat Diabetes presents an implementation challenge due to its breadth,complexity and cross sectoral approach. The need to reduce the risk factors fordiabetes, slow disease progression and increase the quality of life for people withdiabetes requires a response that encompasses whole-society action across the lifecourse.
The implementation process must develop a community partnership that can create an‘atmosphere of leadership’ that permeates local government, industry, the health sector and the population itself. The ‘newness’ of this project means implementation mustsupport an explicit learning framework and strong feedback loops.
A governance structure is proposed that includes a broad stakeholder governancegroup that meets as a forum twice a year to provide overall guidance for the projectand feedback from the broader society, a steering group made up of key action leadersthat meets monthly and leadership hubs for each of the Ten Action Areas.
Counties Manukau District Health Board (CMDHB) will provide support for a project management team that coordinates the overall implementation process through thegovernance and steering groups and provides links across the various health sectoractions.
The project management team will need to work closely with each of the partnerorganisations to ensure Let’s Beat Diabetes is aligned to their strategic objectives and that the plan and implementation continue to deliver value to stakeholders and thereby maintains their commitment.
The implementation process includes an establishment phase for the first six months of2005 when the governance and management structures are set up, detailedprogrammes designed in each of the Ten Action Areas, targets and key performanceindicators set, reporting and evaluation mechanisms set up, and funding committed.
Implementation will be phased with most programme activity beginning from July 2005,but with some programmes scheduled to begin a year later to enable more detaileddesign and to manage the workload and complexity of the project, and a small number of programmes beginning earlier to ensure momentum is maintained from the planning during 2004.
There are a number of significant risks with the project associated with its breadth and complexity and the need for effective community and organisational partnership processes. These risks are mitigated to some extent by the community commitmentshown to date, the strong interagency relationships in Counties Manukau, and the skills CMDHB, Manukau City Council (MCC), and other agencies have developed inimplementing community based programmes.
It is noted that the implementation plan does not include a discussion on fundingissues. These will be included in a separate ‘business case’ document.
76 FINAL PLAN 02 February 2005

Scoping the task
The Challenge
Implementing Let’s Beat Diabetes represents a huge challenge for the health sectorand for the wider Counties Manukau society. Reducing the risk factors for diabetesrequires us to change some of the core components of our modern environment andlifestyle. Treating diabetes effectively needs health sector reorientation from its historicacute care model to a chronic care model, which requires a paradigm shift in roles,relationships and skill sets.
As the WHO has noted: ‘In developed countries, the epidemiological shift in diseaseburden from acute to chronic diseases over the past 50 years has rendered acute care models of health service delivery inadequate to address the health needs of thepopulation’ (WHO, 2003)
Our immediate challenge is diabetes - but to beat diabetes we must address head-onthe current inability of society and our health sector to respond effectively to chronicdisease.
These deep structural issues must be manifest in both programme design and inimplementation.
Implementation challenges inherent in the programme design
Let’s Beat Diabetes describes a set of Ten Action Areas that, when implemented,will have a material impact on obesity, diabetes and other chronic diseases, suchas cardiovascular disease. The 10 areas are wide in scope and emphasise awhole society approach and the need for sustained commitment over time by government agencies, industry and communities.
Let’s Beat Diabetes is committed to the principles of partnership, participation andprotection permeating all aspects of design and delivery, specifically in its relationship with Maori and more generally as a guiding philosophy for meaningfulcivic leadership.
Let’s Beat Diabetes notes the importance of community ownership and the use ofculture to embed sustainable change in our society.
Let’s Beat Diabetes is a plan for the Counties Manukau district (not just a health plan) and as such has a different and far more complex dynamic in terms ofgovernance and operational management than a normal sector-specific strategicplan.
Let’s Beat Diabetes is new. It is moving into new ground for a district health board in New Zealand, forging new partnerships and designing and implementing new programmes. Some programmes are being developed in areas where there is notconclusive evidence of effectiveness, therefore a strong learning and evaluation framework is required.
In some areas Let’s Beat Diabetes programmes cannot be implemented without a fundamental change to the traditional skill sets, organisational capacity andaccountabilities of parts of the health sector.
77 FINAL PLAN 02 February 2005
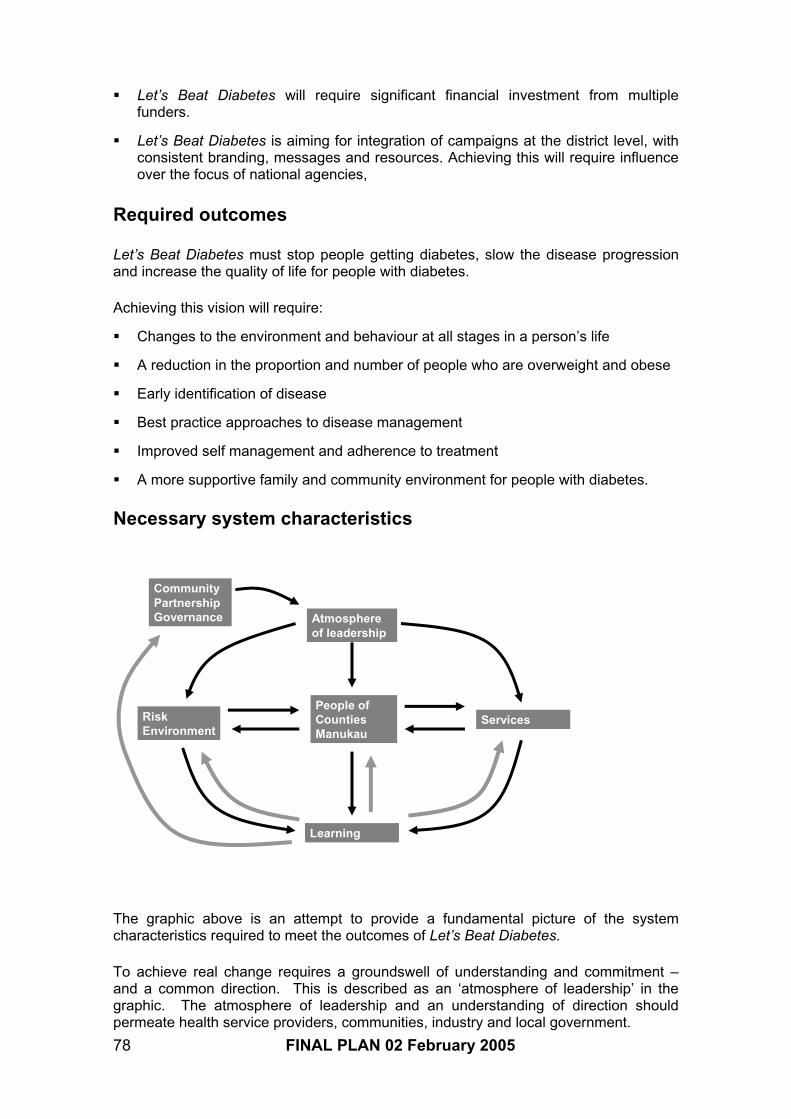
Let’s Beat Diabetes will require significant financial investment from multiplefunders.
Let’s Beat Diabetes is aiming for integration of campaigns at the district level, withconsistent branding, messages and resources. Achieving this will require influenceover the focus of national agencies,
Required outcomes
Let’s Beat Diabetes must stop people getting diabetes, slow the disease progressionand increase the quality of life for people with diabetes.
Achieving this vision will require:
Changes to the environment and behaviour at all stages in a person’s life
A reduction in the proportion and number of people who are overweight and obese
Early identification of disease
Best practice approaches to disease management
Improved self management and adherence to treatment
A more supportive family and community environment for people with diabetes.
Necessary system characteristics
Atmosphereof leadership
Services
Learning
People ofCountiesManukau
RiskEnvironment
CommunityPartnershipGovernance
The graphic above is an attempt to provide a fundamental picture of the systemcharacteristics required to meet the outcomes of Let’s Beat Diabetes.
To achieve real change requires a groundswell of understanding and commitment –and a common direction. This is described as an ‘atmosphere of leadership’ in thegraphic. The atmosphere of leadership and an understanding of direction shouldpermeate health service providers, communities, industry and local government.
78 FINAL PLAN 02 February 2005

The atmosphere of leadership will take on a life of its own, as all successful societalchanges do, but in the early stages it will require spark and fuel – and this is the role ofthe community partnership governance.
Activities to change the risk environment (both behavioural and environmental risk) and the service environment will be more effective if the population is not a passive recipient, but an active participant in shaping the sorts of changes required.
Finally, there are no ‘off-the-shelf’ models for beating diabetes. There is evidence frommultiple sources to help plan the journey, but central to success will be the ability of allparties to learn fast about what is working and what is not. This new knowledge needsto be shared at a local level and also to be fed back to the community partnershipleadership in order to shape the overall plan.
The implementation plan attempts to influence all of the necessary system characteristics.
79 FINAL PLAN 02 February 2005

Implementation structure and process
Programme shape and implementation phasing
The Gantt chart above describes the basic shape of the Let’s Beat Diabetes plan. Thefirst six months of 2005 are an establishment phase in which district governance structures are put in place and the project team set up. There is intensive detailed programme design. A small number of CMDHB-funded initiatives begin in order to maintain momentum from 2004 planning.
From 01 July 2005, sustainable funding becomes available for the programme. Thesecond half of 2005 sees a number of programmes (Phase I programmes)implemented with programme design work continuing for Phase II programmes.
The programme design and implementation is divided into two phases to manage theworkload, complexity and to align with other external programmes and activity. Thefirst wave of programmes will create a more conducive environment for those that follow later in the year.
The evaluation process will be ongoing from mid 2005, supporting a continuous qualityimprovement process and rich learning environment, however, it is proposed that thereis a major milestone report at the end of year three to review progress and support any adjustments that are required over the final two years of the project.
It is proposed that a substantive planning process is undertaken in year five to developstrategic directions for the next five years.
80 FINAL PLAN 02 February 2005

Developing community partnership governance
Community Governance Group
Overall guidance from communitypartners
PartnershipSteering Group
Urban design
Social
marketing
Schools
Integration
Primary care Community
leadership
Food
Well child
Vulnerable
families
Health
promotion
Governance
Meets 4 times ayear – districtownership (linksto Tomorrow’sManukau)
Steering Group
Monthly –leadership fromaction areas andproject team
Leadership hubs
Explicit leadershipstructures foreach of the 10 action areas
DHB roles
The DHB willprovide adminsupport to thegovernance andsteering groups.
It will also providea projectmanagementteam to providecore managementsupport for thewholeprogramme. Theprojectmanagementteam will supportthe 10 actionareas to varyingdegrees,depending on need andprogrammecharacteristics
Projectmanagement
team
The graphic above describes the overall governance and leadership structure for Let’sBeat Diabetes. There has been much discussion and debate over the most effectiveformat for community partnership governance. There is a tension between having an effective and focused leadership group to drive the project forward and the need forbroad community membership and guidance for the project.
There is also a tension between wanting community governance to retain guidance forthe plan as a ‘whole’ but also to maximise the ability of the various parts to be actionorientated, not held back by bureaucracy and to learn from each other without a hierarchical system of control. Conversely, if governance groups do not have anypower or influence, participants soon lose commitment to the process.
Underlying the governance structure is a commitment to open governance andcommunity empowerment, with documentation from meetings available on the Let’sBeat Diabetes website.
The proposed governance structure is an attempt to navigate through these issues.
The structure has three key levels.
i. Community Governance Group: This group will own the plan and provide overall high level leadership and guidance for its implementation. The group will representthe key organisational and community stakeholders. It will be quite large (e.g. 30 members) and would meet in a forum situation twice a year (or more often if required) to receive reports on progress, provide feedback from the community andpartner organizations, and provide guidance on issues.
81 FINAL PLAN 02 February 2005

ii. Partnership Steering Group: The Partnership Steering Group provides operational leadership and co-ordination for the plan implementation. The group will be madeup of leaders from the action areas, CMDHB project team members, and identifiedenthusiasts and experts. Consumer representatives may also with to participate inthe steering group on particular issues. It is anticipated the steering group will meet monthly. The steering group will also develop reports for Tomorrow’s Manukau TeOra O Manukau/Manukau the Healthy City Outcome Group to ensure that thepartnership and information flow with Manukau City Council (MCC) and other key district organisations is maintained.
iii. Leadership hubs: Leadership hubs will be established for each of the ten action areas. The hubs will vary considerably from area to area. In some cases it may bea specific new working group, in others it may be a new accountability for an existing group. Composition will differ to fit the functional needs of the programmes.Efforts will be made to develop stable individual leadership within each action area so that a consistent team develops at the steering group level. Efforts will be madeto support non-DHB leadership in many of the action areas to reflect the whole society approach. Functional networking across the action areas will beencouraged.
Supporting effective project management
The governance structure must be supported by effective project management. Thebreadth and complexity of Let’s Beat Diabetes creates new challenges andaccountabilities across the societal response and across the health sector.
It is proposed that a dedicated project support team is located in CMDHB and would befunded by CMDHB.
The role of the project support team would be to provide administrative and projectsupport for the governance, steering and action areas. It would also deliver expertise and programme design skills for the overall project and to lead and co-ordinate CMDHB’s commitment to the project. The project team would also be responsible foroverall performance reporting and would provide links back into CMDHB funder andprovider operations.
The project team will require management and clinical leadership, with support for the complex co-ordination task.
Alignment and commitment
A critical success factor in creating the ‘atmosphere of leadership’ necessary to beatdiabetes is the ongoing commitment from multiple organisations. CMDHB acknowledges that it will provide the greatest component of resource andadministrative support for the programme but other organisations must also commit or the plan will fail.
In order for organisations to commit, the plan must align with their directions anddeliver strategic and operational value. If Let’s Beat Diabetes ceases to deliverperceived value to stakeholders, they will disengage. All organisations have a differentview of what constitutes value, and sustainable partnerships will require continuallyassessing what value is being delivered for all stakeholders and modifying activity where necessary.
82 FINAL PLAN 02 February 2005

The CDHB project team must develop a set of relationships which are not ‘one size fits all’ but which encompass an in-depth understanding of the needs of key partners in terms of their requirements of partnership, their ability to participate, outcomes that are valuable and meaningful for them, and effective means of communication for theirorganisation.
A key early point for alignment and commitment will be in constituting the make-up of the partnership steering group, leadership groups for each of the Ten Action Areas,and in the detailed programme design and resource commitment.
Outlined below are the Ten Action Areas and the Enablers and some indications of potential organisations involved in each of the areas. The CMDHB project team willoffer administrative and project support for all Ten Action Areas, but the level and typeof support will vary considerably depending on need and function. A number of theaction areas may be provided administrative and project support by partner organisations.
Action Area Organisational leadership1. Community Leadership & Action Church and marae
Community organisationsTomorrow’s Manukau organisationsCMDHB, ARPHS, PHOs
2. Social Marketing CMDHB, SPARC, Pharmac, MCC, ARPHS, MOH, NGOs 3. Urban Design MCC, CMDHB, ARPHS, Housing4. Food Industry Food industry, CMDHB, ARPHS5. Health Promotion CODA group, CMDHB, Diabetes Projects Trust, NGOs,
PHOs, ARPHS, DPT6. Well-Child CMDHB, Plunket, MOH, NGOs, Kidz First, PHOs 7. Schools CMDHB, MOE, MCC, Trustees, Principals, SPARC, NGOs,
food industry, Kidz First8. Primary Care (Chronic Care
Management)CMDHB, PHOs, RNZCGP, Whitiora, NGOs
9. Vulnerable Families MSD (Work and Income, Family and Community Services),NGOs, CMDHB, Plunket,
10.Service integration CMDHB, Chronic Care Management, Whitiora, PHOsEnablersConsumer Consumers, NGOsMaori Marae, Kura, NGOs, CMDHB, PHOsPacific peoples Churches, NGOs, ethnic leadership groups, CMDHB, PHOsFunding Environment CMDHB, MOH, SPARC, MCC, PHOs, Pharmac, MOE, UoALearning Environment CMDHB, UoA, RNZCGP, CCREP, MIT, other DHBsGovernance CMDHB funder and provider, local govt (x3), reps of 10
action areas, Maori, Pacific, Asian communities,consumers, national agencies, evaluation, clinical reps
Organisational Development CMDHB, MIT, NGOs, Whitiora, PHOs, Kidz firstInformation Technology CMDHB, PHOs, MOH, other DHBs, IT providers
Design, performance and learning
Programme design work during 2005 will require detailed development of each of the Ten Action Areas, many of which require cross organisational planning.
Some of the projects are relatively straight forward. Others will require significantdetailed technical design. The CMDHB Let’s Beat Diabetes project team will need to
83 FINAL PLAN 02 February 2005

provide technical support and guidance for programme design in a number of areas,with specialist skills being seconded into support roles as required.
The development of the programmes should link closely to the learning systems andperformance measures for Let’s Beat Diabetes.
It is important that the leadership groups for each of the Ten Action Areas develop their own targets and performance measures. Top down goals and measures may work ina single organisational structure, but since Let’s Beat Diabetes works with crossorganisational collaborations, goals and measures must be owned by all parties.
The leadership groups for each of the Ten Action Areas will be expected to provide a set of goals and Key Performance Indicators by April 2005 and these will beconsolidated into a document that outlines goals and measures for the entire Let’s BeatDiabetes programme.
The evaluation process can help to develop ways of measuring whether processes areeffective and outcomes are being achieved. It is much more effective to develop theseevaluation measures at the point of design, rather than add them on later. Theevaluation plan is expected to be completed by May 2005. The evaluation approach is that of supporting Continuous Quality Improvement across the Let’s Beat DiabetesAction Areas. The evaluators will have to be familiar with each of the Ten Action Areasto determine how they can best add value and learning outcomes for each area as well as for the wider plan.
The enabler areas will be supported through the CMDHB project team and throughsome existing support structures within the CMDHB environment (e.g. workforce development, information systems, Maori and Pacific services).
Branding and developing the plan as an entity
One of the core aspects of the atmosphere of leadership is to develop the Let’s BeatDiabetes plan as part of the Counties Manukau cultural landscape. The plan itselfneeds a positioning and marketing strategy – which is a different issue to the social marketing strategy about diabetes.
One of the early tasks in the implementation process will be to develop a branding andmarketing strategy for the plan.
The plan needs to have a recognisable image and identify and to represent a set ofgoals that all parts of Counties Manukau wish to contribute to. It must be set up for longevity and to be around in a recognisable form in five years time.
The branding strategy will need to appeal to key communities, such as Maori andPacific people, as well as to industry and other government agencies. It will also needto be able to align with government strategies, such as the national Healthy Eating Healthy Action Framework.
84 FINAL PLAN 02 February 2005

Risk management
There are risks inherent in the Let’s Beat Diabetes programme design andimplementation.
The programme design is broad, complex and ambitious, and relies to a considerableextent on the motivation and goodwill of partner organisations and communities to join the health sector in fighting obesity and diabetes. The implementation of a plan of thisnature has not been tried by a DHB before. In many ways CMDHB is running ahead ofgovernment policy and MOH guidelines in the scale and scope of the Let’s BeatDiabetes plan, and hence there may not be a great deal of guidance and supportiveprocesses at a national level.
The positive balance to the inherent risk is that the response to date to the Let’s BeatDiabetes planning process has shown the depth of commitment in Counties Manukauto beat diabetes and the strong history of functional interagency relationships providesa platform to build from. The timing feels ‘right’ in terms of a conducive Counties Manukau environment.
CMDHB has excellent skills in community partnering and project management and hasindicated that it will provide sustained resources to support Let’s Beat Diabetes over afive year period. Given the trends in obesity and diabetes, it is likely that thegovernment will provide support to the programme and will highlight it as an exemplarfor other DHBs to follow.
Further details of risks and mitigating strategies are outlined below.
Risks Descriptions Mitigation
Poor external ownership Failure of organisational commitment to governance structure and action arealeadership
Significant effort has gone intoplanning phase to align organisations (commitmentthrough summit)This will be firmed up intospecific commitment duringQ1&2 of 2005
Poor internal ownership Failure of internal support, alignmentwithin DHB funder and provider arms(other priorities)
High level support from EMTand the Board, and alignmentof goals across diabetes planand broader system and clinical outcomes
Swamped by complexity Project team is unable to deliver on timedue to size and scope of project, designcomplexity and operational complexity
Maintain high skill level in coreteam, fund access to specific experts when required, phaseactivity, review regularly
Evaporation of interest Internal and external interest evaporatesat multiple levels (governance and operational)
Maintain pace of change,include strong learningframework in programmedesign and evaluation,highlight achievements (andachievers) and provide positivefeedback across the broaderchange programme (a sense of campaign)
Slow wins Lack of tangible results leads to loss ofmomentum.
Structure programmes withexplicit early wins, identify andpublicise KPIs, and celebrateprocess as well as outcome
85 FINAL PLAN 02 February 2005

achievementsCapacity and skill lack Change management, programme design
and implementation skills lacking leads to stalled programmes. Risk especially inprimary care sector given extent ofchange
Early identification ofskill/capacity lack andinvestment is skilldevelopment. Present andreinforce as top priority
Inconsistent fundingenvironment
Funding environment changes from yearto year leading to sector uncertaintyabout commitment
CMDHB Board agrees to committed and stable fundingstream. CMDHB fundssupported by resources fromother sources. Ongoingengagement of key funders
86 FINAL PLAN 02 February 2005

Establishment phase and developmental
phase activities
The set of graphics below outline the key tasks for the establishment phase (first six months of 2005) and the developmental phase (July 2005 – June 2006) of Let’s BeatDiabetes.
The set of tasks is broken up into governance and management tasks and the activityareas themselves.
Governance, project support and establishment
ID Task NameQ1 05 Q2 05 Q3 05 Q4 05 Q1 06 Q2 06
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul
12
Develop detailed programme designfor 10 action areas to inform phasingissues for project management andfunding requirements.
2
1 Governance
Identify key partners and set upStakeholder Governance Group
11
10
9
8
7
6
4
3Develop leadership structures for eachof the 10 action areas
Build operational steering group fromkey leaders form 10 areas
Project support
Appoint staff to LBD project teamwithin CMDHBClarify roles and accountabilities withexisting DHB structures
5Review existing governance structuresand align with LBD structures
Programme design andperformanceIdentify targets and KPIs with 10action areas
Ensure targets and KPIs are reflectedin partner organisation strategic andoperational plans
15
14
13 Communications and relationships
Presentation of diabetes plan to keypartner organisations
Evaluation and learning
Develop overarching evaluationframework, aligned to CQI learningprocess and identified keyperformance indicators
18
17
Implement evaluation
Maintain open process ofcommunication and learning throughLet’s Beat Diabetes web site, whichwill include core information about allprojects and evaluation
16
87 FINAL PLAN 02 February 2005

Action Area tasks
ID Task NameQ1 05 Q2 05 Q3 05 Q4 05 Q1 06 Q2 06
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul
1 Community leadership
2Set up community fund and developworkforce programmes for Tomorrow’sManukau organisations
3Community fund operational andorganisations implementing healthworkforce plans
4 Social marketing
5
Launch Let’s Beat Diabetes,communicate plan to district, developcontract relationship with professionalpartner to deliver social marketingprogramme
6 Begin social marketing programme
7 Urban design
8
CMDHB to work with Manukau City tosupport healthy urban design in FlatBush and redevelopments of existingurban hubs
9 Integrated Health Promotion
10
Revitalise district health promotion co-ordination through improved supportfor CODA group and links to HPOs.Develop plan of action.
11Implement contracts for capacitybuilding, co-ordination and resourcedevelopment for health promotion
Develop enhanced programmes to achieve targets and implement
12
88 FINAL PLAN 02 February 2005
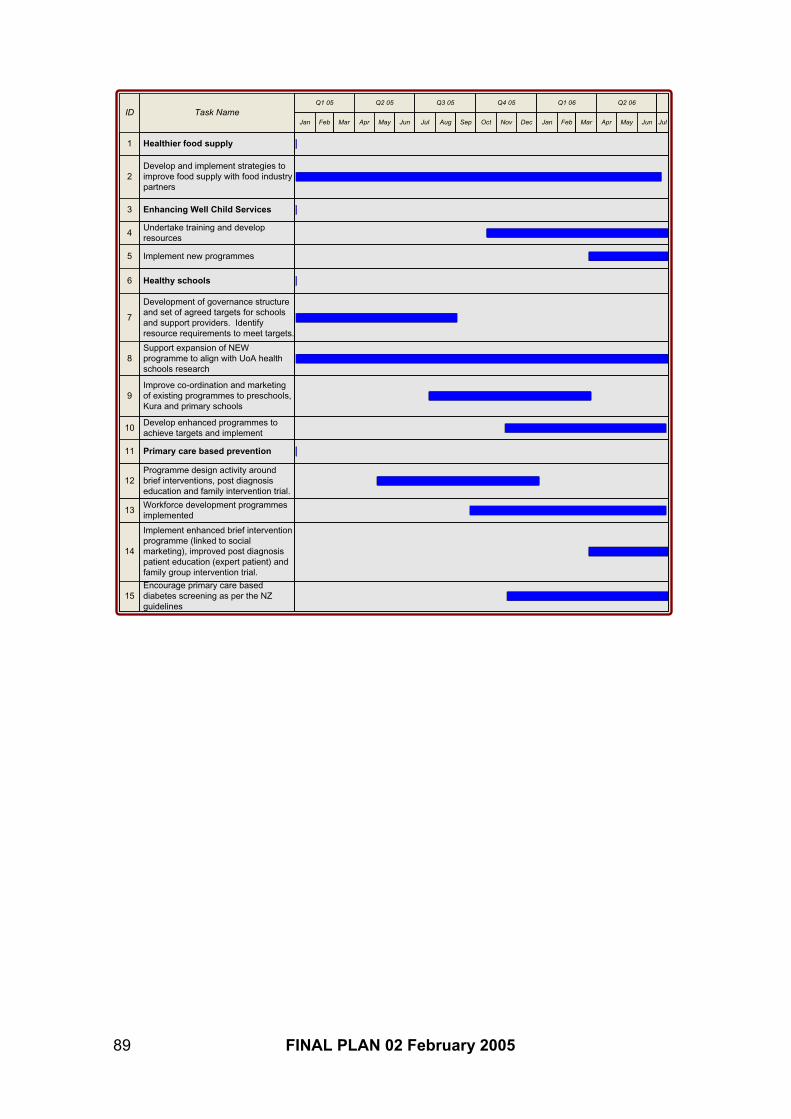
ID Task NameQ1 05 Q2 05 Q3 05 Q4 05 Q1 06 Q2 06
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul
1 Healthier food supply
2Develop and implement strategies toimprove food supply with food industrypartners
3 Enhancing Well Child Services
12
11
Undertake training and developresources
Implement new programmes5
4
Primary care based prevention
Programme design activity aroundbrief interventions, post diagnosiseducation and family intervention trial.
14
13Workforce development programmesimplemented
Implement enhanced brief interventionprogramme (linked to socialmarketing), improved post diagnosispatient education (expert patient) andfamily group intervention trial.
15Encourage primary care based diabetes screening as per the NZ guidelines
9
8
7
Development of governance structureand set of agreed targets for schoolsand support providers. Identifyresource requirements to meet targets.
Support expansion of NEWprogramme to align with UoA healthschools research
Develop enhanced programmes to achieve targets and implement
Improve co-ordination and marketingof existing programmes to preschools,Kura and primary schools
10
6 Healthy schools
89 FINAL PLAN 02 February 2005
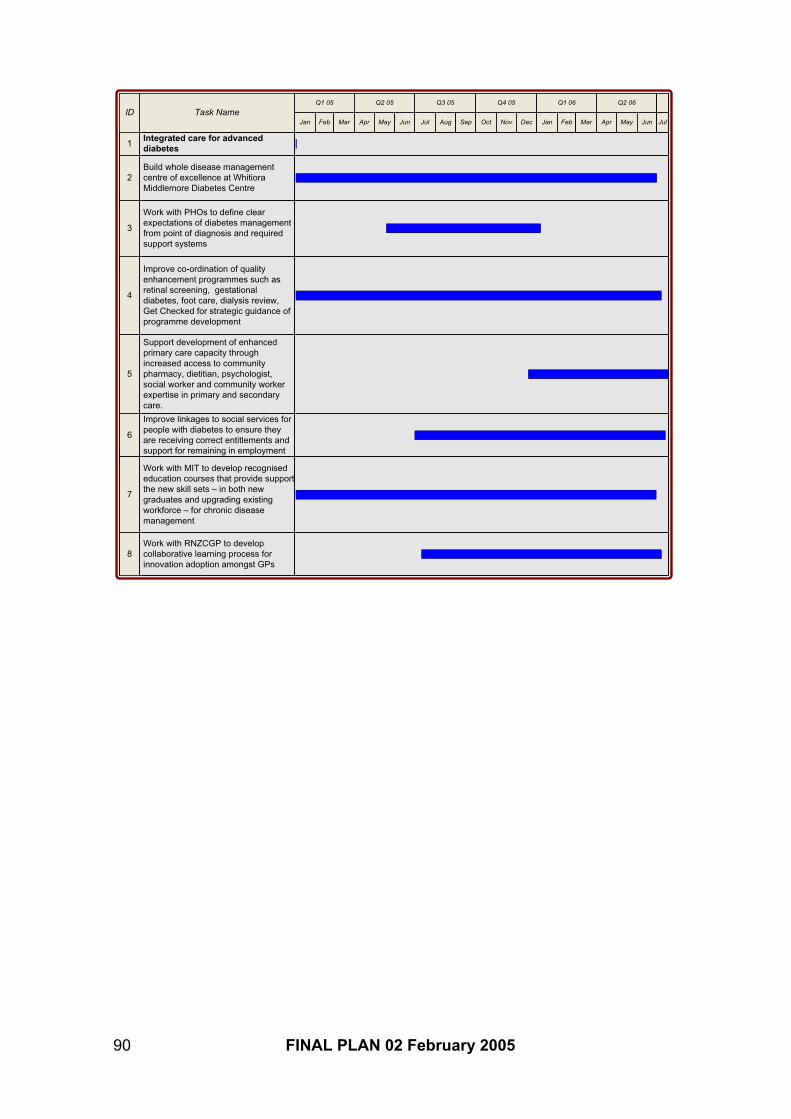
ID Task NameQ1 05 Q2 05 Q3 05 Q4 05 Q1 06 Q2 06
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul
8
3
2
1Integrated care for advanceddiabetes
Build whole disease managementcentre of excellence at WhitioraMiddlemore Diabetes Centre
Work with PHOs to define clearexpectations of diabetes management from point of diagnosis and requiredsupport systems
Work with RNZCGP to developcollaborative learning process for innovation adoption amongst GPs
Improve co-ordination of qualityenhancement programmes such asretinal screening, gestationaldiabetes, foot care, dialysis review,Get Checked for strategic guidance ofprogramme development
4
6
Improve linkages to social services for people with diabetes to ensure theyare receiving correct entitlements andsupport for remaining in employment
7
Work with MIT to develop recognisededucation courses that provide support the new skill sets – in both newgraduates and upgrading existingworkforce – for chronic disease management
5
Support development of enhanced primary care capacity throughincreased access to communitypharmacy, dietitian, psychologist,social worker and community workerexpertise in primary and secondary care.
90 FINAL PLAN 02 February 2005

References
Barnfather D (2004). "Childhood Obesity Prevention Programmes in Auckland."
Counties Manukau District Health Board (2002). "Healthy Futures: A Strategic Plan for Counties Manukau District Health Board."
Counties Manukau District Health Board (2004). "Survey of Year 9 pupils at Aim Hi Schools."
Critser G (2003). Fat Land: How Americans became the fattest people in the world, Allen LaneThe Penguin Press.
FAO/WHO Expert Consultation (2003). Diet, nutrition and the prevention of chronic diseases:Report of a joint WHO/FAO expert consultation, Geneva 28 January- 1 February 2002. Geneva,WHO.
Homer J, J. A., Seville D, et al (2004). The CDC's Diabetes Systems Modeling Project: Developing a New Tool for Chronic Disease Prevention and Control. Atlanta, Centre for DiseaseControl: 10.
Kawachi I (2003). Promoting Physical Activity and Health by Urban Design.
Lindsay A (2003). Diabetes Rates by Census Area Unit in Counties Manukau.
Ministry of Health (2000). "The New Zealand Health Strategy."
Ministry of Health (2001). "The Primary Health Care Strategy."
Ministry of Health (2002). "He Korowai Oranga - Maori Health Strategy."
Ministry of Health (2002). "Modeling Diabetes: Forecasts to 2011."
Ministry of Health (2002). Modeling Diabetes: Forecasts to 2011.
Ministry of Health (2002). "The Pacific Health and Disability Action Plan."
Ministry of Health (2003). "Healthy Eating - Healthy Action: A strategic Framework."
Ministry of Health (2003). "NZ Food, NZ Children. Findings of the 2002 National Children'sNutrition Survey."
Ministry of Health (2003). "A Snapshot of Health, Provisional Results of 202/03 New ZealandHealth Survey."
New Zealand Food Industry Accord (2004).
New Zealand Guidelines Group (2003). Management of Type 2 Diabetes, Ministry of Health.
PriceWaterhouseCoopers (2001). "Type 2 Diabetes. Managing for Better Health Outcomes."
Pucher J, D. L. (2003). "Promoting Safe Walking and Cycling to Improve Public Health: LessonsFrom the Netherlands and Germany." American Journal of Public Health 93.
Ratanjee (2004). Personal communication.
91 FINAL PLAN 02 February 2005

Thomas E (2004). The Management of Diabetes at Counties Manukau District Health Board from the Time of Diagnosis.
UKPDS (1975 - 204).
WHO (2004). Global strategy on diet, physical activity and health.
92 FINAL PLAN 02 February 2005





























