Embed Size (px)
Citation preview

9/10/2018
1
Lessons from the
Oldest Old: The 90+ StudyDana Greenia, R.N., M.S.
Co-Investigator
Western Region Chapter
Aging Life Care Association
28th Annual Conference
September 21, 2018Clinic for Aging Research and Education
Institute for Memory Impairments & Neurological Disorders
University of California, Irvine
Madame Jeanne-Louise CalmentArles, France
1875 – 1997Age 122
Madame Jeanne-Louise Calment

9/10/2018
2
Supercentenarian
If increases in life expectancy continue,
more than half of all children born
today in developed countries can
expect to celebrate their 100th
birthdays
Christensen, Ageing Populations: The Challenges Ahead, Lancet , 2009
Overview
1. The 90+ Study
2. Factors that promote longevity
3. Incidence and Risk Factors for Dementia in the Oldest Old
4. Clinical Pathological Correlations for Dementia
5. Describe the Relationship between Exercise and Falls in 90+ year olds

9/10/2018
3
U.S. Projected Population GrowthAmong 90+ Year Olds
Population Projections U.S. Census Bureau 2002, Middle Series
0
2,000,000
4,000,000
6,000,000
8,000,000
10,000,000
2001 2010 2020 2030 2040 2050
Year
Mill
ion
s o
f P
eop
le
Age-Specific Incidence of Dementia in Studies with Subjects Aged 90+
The Relative Frequency of
“Dementia of Unknown Etiology” Increases with
Age and is Near 50% in Nonagenarians
• Series of 128 subjects
• Dementia of unknown etiology
– 5% of all cases dying in their 70’s
– 21% of all cases dying in their 80’s
– 48% of all cases dying in their 90’s
Crystal, et al, Arch Neurol 2000

9/10/2018
4
Unknown in 90+ Year Olds
• Risk/Protective Factors Related to Longevity
• Prevalence and Incidence of Dementia
• Risk/Protective Factors Related to Dementia
• Types of Dementia
The Leisure World Cohort StudyUSC
• Prospective Cohort Study Design• Residents of Southern California Retirement Community• 13,978 Enrolled 1981-1985
- Primarily white
- 2/3 female
- Median age at enrollment: 73 years- Well-educated
• Follow-up Surveys1983, 1985, 1992, 1998
The 90+ Study

9/10/2018
5
UCI Clinic for Aging Research and Education Laguna Woods, CA
The 90+ Study
• 2003: ~ 1,140 survivors of the Leisure World Cohort (13,978 were enrolled) aged 90 years old and older were invited
• Today we have a total of 1,882 participants enrolled • Participants evaluated every 6 months
• neuropsychological tests• physical and neurological examinations • Neuroimaging – Brain Pet scans & MRIs
• Many enrolled in The 90+ Autopsy Study
Assessments• Intake
– Demographics & Medical History
• Neuropsychological Tests
– Memory, Language, Executive function
• Neurological Examination
• Informant Questionnaires
• Genetic studies
– DNA
• Brain Donation

9/10/2018
6
Physical Performance Measures
The 90+ Study ParticipantsBaseline Results
# of Participants 1882
EducationCollege grad or more 41%
Marital StatusWidowed 77%
Married 14%
% of Women
Mean Age 96Type of Residence
Nursing or group home 40%
Assisted Living 30%
Home alone 30%
Neurological Exam Cognitive Diagnosis Women Men
Normal
Cognitively Impaired, not Demented
Demented
76%
33% 43%
26% 33%
41% 24%
• Russia-2 TV Documentary 2012 • Newport Beach Daily Pilot 2010• Bottom Line Health magazine 2010• New York Times front page 2009• Louie B. Free radio program 2009 • Los Angeles Times front page 2004• KCET Life & Times 2003• My Generation Magazine 2015
• 60 minutes Australia May 2015• CBS 60 minutes May 2014 • Good Day LA 2014 • OC Register Jan, Oct & Nov 2013• KCAL 9 TV 2013• NPR Radio 2012• Italian Public TV 2012• Laguna Woods Globe 2012

9/10/2018
7

9/10/2018
8
Research Goal
To study potentially modifiable risk factors that may contribute to the
prevention or the delay of the development of Alzheimer’s disease
and dementia
# of participants
719
16
6
4
3
2
9
1
35 States Traveled To Visit Participants
5
Frequency of Medical Histories at Baseline
7
8
11
14
13
15
18
20
21
22
27
29
29
39
43
51%
Diabetes
Rheum Arthr
MI
CAD
Stroke
CHF
Glaucoma
Depression
TIA
Atrial Fib / Arryth
Thyroid
High Chol
Macular Degen
Cancer
Osteoarthritis
HBP
12/2012
9/10/2018
9
What is Related to Longevity?
Vitamins, Beverages and Longevity
• Vitamin C (diet + supplements)• Vitamin A (diet + supplements)• Vitamin E (supplements)• Calcium (diet)• Soft drinks (cola & other)• Tea (black or green)• Body Mass Index• Activities - Exercise • Activities - Leisure• Caffeine• Alcohol (wine, beer, other)
Corrada 2006; Paganini-Hill 2007, 2011,2015
Studies of Factors Associatedwith Longevity

9/10/2018
10
BMI and All-Cause MortalityLeisure World Cohort: 1981-2004
-10
0
10
20
30
40
50
60
70
Ch
an
ge i
n R
isk (
Perc
en
t)
BMI at Baseline (Avg Age 73)
BMI at Age 21
BMI Categories
+53%
-3%
+12%
+2%
+15%
Corrada, et al. Am J Epidemiology 2006
N = 13,451
‘Active’ Activities and MortalityLeisure World Cohort: 1981-2004
N = 13,601
-35
-30
-25
-20
-15
-10
-5
0
5
None 15 min 30 min 45 min 1-1.75hrs 2-2.75 hrs 3+ hrs
Ch
an
ge i
n R
isk (
Perc
en
t)
Time Spent per day
‘Active’ Activities Swimming
Biking
Jogging
Tennis
Vigorous walking
Exercising
Dancing-11%
-18%
-24% -25%-23% -22%
‘Other’ Activities and MortalityLeisure World Cohort: 1981-2004
N = 13,601
-40
-35
-30
-25
-20
-15
-10
-5
0
5
0-45 1-1.75 hrs 2-2.75 hrs 3-3.75 hrs 4-4.75 hrs 5-5.75 hrs 6+ hrs
Ch
an
ge i
n R
isk (
Perc
en
t)
Time Spent per day
‘Other’ Activities
-17%
-21%-22%
-25%-26%
-30%
SightseeingFishingGolfGardeningReadingSewingCraftsBoard gamesTheaterConcerts

9/10/2018
11
Intake of Alcohol and Caffeine
Alcohol (wine, beer, other)
1-2 glasses of alcohol a day reduction in mortality up to 18%
Caffeine
Equivalent to ~2 cups of coffee a day reduction in mortality of 10%
Paganini-Hill, et al. Age & Ageing 2007; Preventive Medicine 2007
What is related to Dementia in the
Oldest-Old
?
What is Dementia?
• A decline in mental ability severe enough to interfere with daily life

9/10/2018
12
52
8%
2%
2%
4%
14%
17%
Causes of Dementia in the Elderly
Alzheimer’s
Disease
Vascular
Dementia
Lewy Bodies
Mixed Dementia (both AD and
minor strokes)
Fronto-temporal
Parkinson’s disease
Other
Age-Specific Incidence of Dementia in Studies with Subjects Aged 90+
Age-Specific Incidence of Dementia in Studies with Subjects Aged 90+

9/10/2018
13
AgingThe Elephant in the Room!
Age is the biggest risk factor for dementia
Oldest old have the highest rates of dementia
Cross-sectional Investigations of Risk
Factors and Dementia
• Vitamin E (supplementation)
• Vitamin C (diet and supplementation)
• BMI
• Alcohol
• Caffeine
• Activities
• Homocysteine levels
• Thyroid function
Vascular Risk Factors andPrevalent Dementia
Vascular risk factors did not distinguish demented and non-demented participants
except hypertension
46% Hypertension
12% Coronary Artery Disease
12% Myocardial Infarction
17% Congestive Heart Failure
22% Atrial Fibrillation

9/10/2018
14
Background
• Cardiovascular diseases in midlife are commonly associated with an increased risk of dementia later in life. (Kivipelto, Brit Med J 2001; Whitmer, Neurology 2001; Launer, Neurobiol
Aging 2000)
• In contrast, history of hypertension in the oldest-old is associated with a decreased risk of dementia. (Li G, JAGS
2007; Ruitenberg, Geriatr Cogn Disord 2001; MM Corrada, Alzheimers Dement. 2014)
• Whether the apparent change in risk with age is unique to hypertension, or other cardiovascular risk factors behave in a similar manner, is not known.
Prevalence of Cardiovascular Risk Factors at Baseline
6
7
10
10
12
15
15
27
36
58
0 10 20 30 40 50 60
Diabetes
Heart Valve Disease
Congestive Heart Failure
Stroke
Myocardial Infarction
Coronary Artery Disease
Transient Ischemic Attack
Arrhythmia
High Cholesterol
Hypertension
Percent
0.730.78
0.90
1.201.29 1.32
1.53
1.72 1.72
2.15
0.5
Haz
ard
Rat
io (
95
% C
I) (
log
scal
e)
Cox regression adjusting for age (time scale), gender, & education.
Association between Cardiovascular Risk Factors& Risk of Dementia in the Oldest-Old (N=559)
1.0
3.0
2.0
58% 36% 15%27%15% 12% 6%
Prevalence
10% 7% 10%
Medical Histories Analyzed Separately

9/10/2018
15
0.73
1.72 1.72
2.15
0.5Hyper-tension
HighCholest
CoronaryArtery
Disease
Arrhyth-mia
TransientIschemic
Attack
MyocardialInfarction
Diabetes Stroke HeartValve
Disease
CongestiveHeart
Failure
Hazard
Ratio (
95%
CI)
(lo
g s
cale
)
Cox regression adjusting for age (time scale), gender, & education.
Association between Cardiovascular Risk Factors& Risk of Dementia in the Oldest-Old (N=559)
58% 36% 15%27%15% 12% 6%
Prevalence
10% 7% 10%
1.0
3.0
2.0
0.74
1.681.60
2.23
0.5
Haz
ard
Rat
io (
95
% C
I) (
log
scal
e)
Association between Cardiovascular Disease& Risk of Dementia in the Oldest-Old (N=559)
Medical Histories Analyzed Together
58% 36% 15%27%15% 12% 6%
Prevalence
10% 7% 10%
1.0
3.0
2.0
Cox regression adjusting for age (time scale), gender, & education.
Hyper-tension
HighCholest
CoronaryArtery
Disease
Arrhyth-mia
TransientIschemic
Attack
MyocardialInfarction
Diabetes Stroke HeartValve
Disease
CongestiveHeart
Failure
• In people who reach age 90+ without dementia:– Decreased risk - Hypertension
– Increased risk - Congestive heart failure, stroke, and heart valve disease
• The association with dementia changes with age for some but not all vascular diseases.
Conclusions

9/10/2018
16
• Our results are consistent with other studies
• Hypertension at older ages may be necessary to sustain adequate cerebral perfusion in the oldest-old
• Survival bias is an unlikely explanation for the association between hypertension and a decreased risk of dementia; finding is specific to hypertension and not other vascular diseases.
Discussion
Qiu, Winblad, & Fratiglioni, Lancet Neurol, 2005; Jani and Rajkumar, Post Grad Med J, 2006; de la Torre, Stroke, 2002; Siennicki-Lantz et al., Eur. J. Neurol, 2007
Risk of Dementia in Relation toAge of Onset of Hypertension
1.00
0.88
1.13
0.59
0.45
0.2
2.0
No hx <70 70-79 80-89 90+
Rel
ativ
e R
isk
(95%
CI)
(lo
g sc
ale)
Age of Onset of Hypertension
1.0
low
er r
isk
hig
her
ris
k
Adjusted for age & education Corrada, et al. AAIC 2014
Blood Pressure & DementiaPotential Interpretations
1. “Normal” blood pressure may be different for 90+ year olds
2. Elderly torturous cerebral vessels may require increased pressure for adequate perfusion
3. Low blood pressure may be a marker for other diseases
4. Medication effects – ACE-inhibitors, Ca-channel blockers, others
5. Differential medical care

9/10/2018
17
The 90+ Autopsy Study
Enrolled 506
Longitudinal follow-up every 6 months
305 have come to autopsy
90+ Autopsy Study Participants
Not Demented Demented
Median
Age (years) 97 97
MMSE 27 12
Brain Weight (g) 1150 1117
Normal BrainAlzheimer’s Brain

9/10/2018
18
AD Pathological Features
Neuritic Plaques
Extracellular depositsof beta-amyloid
Neurofibrillary Tangles
Intracellular deposits of hyperphosphorylated tau
Pathological Diagnoses by Dementia Status
No Dementia(N=85)
Dementia(N=98)
AD=Intermediate/High NIA Reagan Criteria
None or InsufficientPathology
40%
ADPathology
60%
None or InsufficientPathology
58%
ADPathology
42%
Other pathologies that may contribute to dementia in the
oldest old
9/10/2018
19
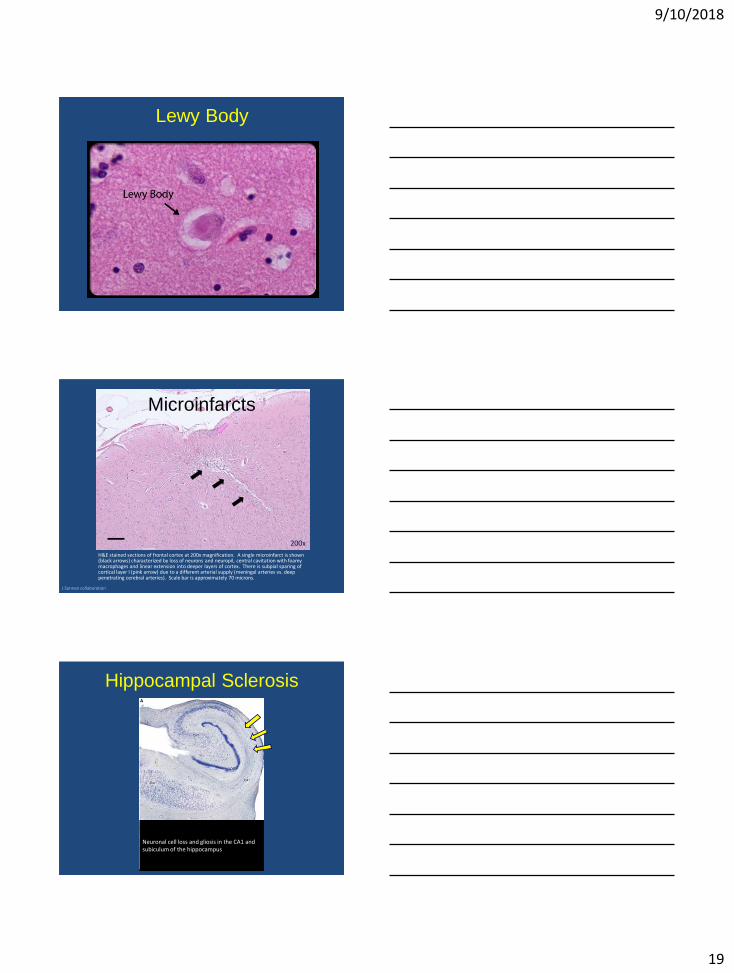
Lewy Body
H&E stained sections of frontal cortex at 200x magnification. A single microinfarct is shown (black arrows) characterized by loss of neurons and neuropil, central cavitation with foamy macrophages and linear extension into deeper layers of cortex. There is subpial sparing of cortical layer I (pink arrow) due to a different arterial supply (meningal arteries vs. deep penetrating cerebral arteries). Scale bar is approximately 70 microns.
200x
J Sonnen collaboration
Microinfarcts
Hippocampal Sclerosis
Neuronal cell loss and gliosis in the CA1 and subiculum of the hippocampus

9/10/2018
20
Frequency of Dementia by Number of Pathologies (N=183)
Kawas, et al. (under revision)
OBJECTIVE
To explore the relationshipbetween risk of falling at age 90+ and physical activity at
ages 60-70s

9/10/2018
21
Methods
• Time spent exercising (at ages 60 -70s) was self-reported in 1980s and categorized as none, 15 minutes, 30-45 minutes, or 1+ hour / day.
• 1536 participants (or their informant) of The 90+ Study provided information on falls in the previous year.
• Mean age = 94 years; 78% female; 99% Caucasian
RESULTS
• 52% had fallen in the prior year
• 32% had fallen more than once
• 21% had had a severe fall
• Falling at age 90+ was significantly related to:
–Medical hx: heart disease, TIA/stroke, arthritis, vision disease, dementia, depression
–Medications: hypnotics, anti-psychotics, anti-depressants
–Assistive Devices: cane, walker, wheelchair
RESULTS
• Regular physical activity (30+ minutes /day) at ages 60 -70s was associated with a 35% lower odds of falling in the previous year at age 90+.
• Regular physical activity (30+ minutes /day) at ages 60 -70s was associated with a 45% lower odds of repeated falls in the previous year at age 90+ .

9/10/2018
22
Conclusion and Relevance
• Falls are extremely common among the oldest-old and often lead to serious injury.
• Prior exercise of 30+ minutes /day was related to a decreased risk of falling at age 90+ even the presence of co-morbidities, certain medications and assistive devices.
• This work is the first to show an association between exercise at ages 60 -70s and lower risk of falling at age 90+.
• Remarkable increase in longevity and numbers
of oldest old world-wide
• Risk of dementia continues to increase with age
• Risk factors change with age
• Multiple pathologies (and risk factors specific to
each) are likely to be important in the
development of dementia in aging
Summary
Did you hear? 95 is the new 65!
The Laguna Beach Independent - O’Malley - 2/1/08

9/10/2018
23
Acknowledgements
UCI Our CollaboratorsClaudia Kawas Tom Montine - Stanford UniversityMaría Corrada John Trojanowski - U PennAnnlia Paganini Hill Virginia Lee - U PennSandy Pittman Juan Troncoso - JHUNadim Madi Ronald Brookmeyer - UCLARonald Kim Charles DeCarli - UC DavisJaime DeMoss Josh Sonnen - U of UtahChristina WhittleZara MelikyanFarah MozaffarNatalie BryantSzofia BullainShawna PerryMaria KirkwoodColette AquirreMontez HesterMiyoung Kim
Supported by: NIA R01AG21055, P50AG016573, T32AG000096, and the Al and Trish Nichols Chair in Clinical Neuroscience
60 Minutes - May 4, 2014
The 90+ Study Team
.

9/10/2018
24