Embed Size (px)
DESCRIPTION
AHM 540 Chapter 3
Citation preview
AHM Medical Management: Environmental Influences on Medical Management
Objectives:
After completing Environmental Influences on Medical Management, you should be able to:
Describe the types of environmental factors that affect medical management of healthplans
Discuss the expectations of purchasers, providers, and plan members for medicalmanagement
Describe the major federal and state regulatory requirements that affect medicalmanagement
Describe how environmental factors influence a health plan's delegation of medicalmanagement functions
Identify the main accrediting agencies and explain the impact of accreditation on medicalmanagement
Introduction
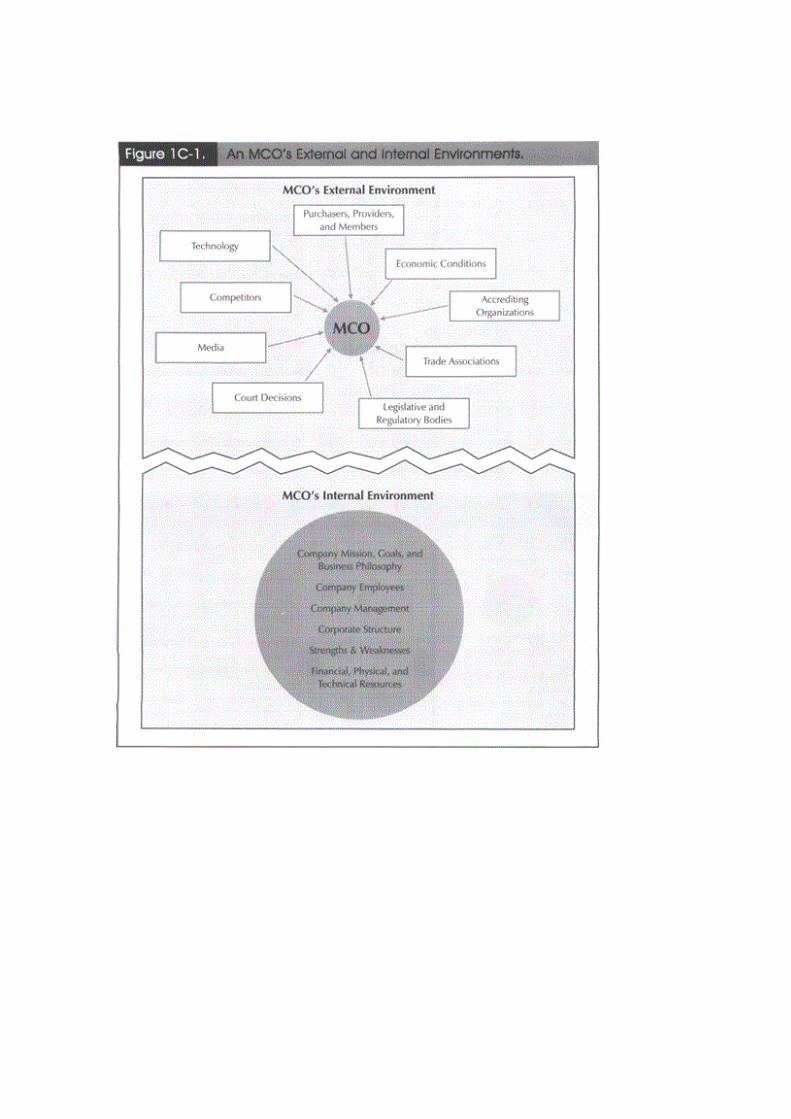
Health plans operate within an increasingly complex environment that consists of both internaland external factors. A health plan's internal environment includes all those elements within thecompany that affect the company's business functions and over which the company has control. Ahealth plan's external environment includes all those elements that are outside the company'scontrol. Figure 1C-1 shows some of the elements that constitute a health plan's external andinternal business environments.
Environment factors have a direct impact on a health plan's medical management policies,strategies, and decision making processes. For example, consider the situation facing a healthplan that is trying to decide whether to add a disease management program to its medicalmanagement function. In order to make a decision, the health plan must not only satisfy itsmedical management goals, it must also accommodate a variety of external demands. Purchasers,providers, and health plan members all have expectations related to healthcare services and to thehealth plans that deliver those services. Competitive pressures influence how plans develop andmarket their products. Federal and state laws and regulations specify how plans must operate, thekinds of benefits they may or must offer, and even the quality standards with which they mustcomply. Accreditation organizations direct how plans measure and improve the quality of theirservices. Media coverage often determines the health plan's public image. As Figure 1C-2illustrates, the issues that affect the health plan's decision can be complex.

In this lesson, we will describe how a health plan's external environment influences its medicalmanagement decisions. We will focus our discussion on the following factors: (1) purchaser,provider, and plan member expectations; (2) legal and regulatory requirements; and (3)accreditation standards.
Medical Management and Expectations of Purchasers, Providers, and Plan Members
Purchasers, providers, and plan members all have expectations related to the healthcare servicesthey want and need and to the health plans that arrange the delivery of those services. Someexpectations are shared by all of these customer groups; others are not. All have an impact on ahealth plan's medical management decisions.
Purchaser Expectations
The major purchasers of health plan services are private employers and federal and stategovernment programs. As a group, these purchasers want to see that all health plans underconsideration:
Provide quality healthcare benefits that are accessible, yet affordable. Operate efficiently so that administrative costs are minimized. Maintain satisfactory member service patterns. Comply with applicable laws, regulations, and industry standards.
Employers, federal governments, and state governments also have their own individualexpectations.

Employers
Employers-especially large employers-are key purchasers of healthcare benefits, and their abilityto recruit and retain competent employees often depends on the type and level of healthcarebenefits they offer. Although cost is an important part of their purchase decision, employers arealso concerned with the quality of care and services the plan delivers. For example, one largeemployer is requesting that health plans comply with specified clinical goals for preventive care,such as prenatal care, mammography screenings, and child immunization rates1. Employersconsider employee satisfaction as well. No employer wants to be inundated with employeecomplaints about inadequate treatment, long wait times for appointments, lack of access toappropriate specialists or preferred providers, poor quality of provider/patient interactions, andthe share of costs they must pay.
Employers can address these concerns, in part, by evaluating and comparing quality data from allhealth plans under consideration. For HMO plans, accreditation by one of the major accreditingorganizations provides evidence that the plan meets certain quality and customer satisfactionstandards. Performance measurement programs provide additional information. These sourcesmay be less helpful in evaluating the quality of non-HMO plans because fewer non-HMO planscurrently seek accreditation or report specific performance results.
If employers are not satisfied with the quality or cost of services available through health plans,they can minimize or even eliminate the role of health plans by contracting directly withproviders or by establishing self-funded plans. Direct contracting allows employers to reduceadministrative costs and see that employees have a sufficient level of provider choice. However,it also requires employers to manage complex provider relationships. So far, the challenges of thisrole have prevented direct contracting from becoming a dominant model. Under self-fundedarrangements, employers assume the financial risk associated with providing healthcare benefits.In some cases, employers also assume responsibility for administering the program; in othercases, employers contract with health plans to provide administrative support throughadministrative services only (ASO) agreements.
In all self-funded programs, directly in the delivery and financing of healthcare benefits and havea voice in determining the type, quality, and cost of healthcare services.
Federal Government
The federal government serves as both a regulator and a purchaser of healthcare benefits. As aregulator of health plans, the federal government exerts regulatory and legislative influence overhealth plans and expects health plans to fully comply with all applicable laws and regulatoryrequirements. In addition, the federal government seeks input from health plans when draftinglegislation or developing regulations to implement laws enacted by Congress. For example, as wewill discuss later in this lesson, many health plans have participated in the federal government'sefforts to develop regulations implementing electronic data security and privacy standards asrequired by the Health Insurance Portability and Accountability Act of 1996.
As the largest purchaser of healthcare benefits in the United States, the federal government has animpact on the medical management functions of individual health plans. Through programs suchas Medicare, the Federal Employee Health Benefits Program (FEHBP), and TRICARE, thefederal government sets standards for the quality and types of benefits it expects health plans to
offer to qualified beneficiaries. Many of these standards and expectations are eventually adoptedby purchasers and consumers in the private sector as well.
In the following sections we discuss some of the federal government's expectations related toMedicare, FEHBP, and TRICARE programs. We will discuss the programs in more detail in laterassignments.
Medicare. As you recall from Healthcare Management: An Introduction, Medicare+Choiceexpanded the types of entities that are allowed to offer managed healthcare plans to Medicarebeneficiaries. During the last few years, the federal government's major quality and costinitiatives have been to encourage Medicare beneficiaries to enroll in managed healthcare plansas part of Medicare+Choice.
The federal government expects Medicare+Choice plans to:
Medicare+Choice Plans Should
Offer a variety of specialty care providers Accommodate the special access and healthcare needs of the Medicare population (e.g.,
transportation, disability coverage) Accommodate the unique utilization patterns of the Medicare population (e.g., use of
emergency departments) Provide services and plan information in a linguistically and culturally sensitive manner
In order to see that health plans satisfy these expectations, the federal government hasimplemented a variety of quality assessment and improvement initiatives. The government hasalso revised reimbursement methods for managed healthcare plans in an effort to reduce costs.However, as a result of these cost-cutting efforts, some health plans have withdrawn from theMedicare program.
On December 8, 2003, President George W. Bush signed into law the Medicare ModernizationAct of 2003 (MMA), creating short-term reforms to designed to both improve benefits and reduceout-of-pocket costs for millions of Medicare beneficiaries who are covered by health plans in theMedicare Advantage program, previously known as the Medicare+Choice programs, and to effectpayment reform to encourage more health plans to offer medicare Advantage programs.
See Editor's Note.Editor's NoteThe Medicare Modernization Act of 2003
On December 8, 2003, President George W. Bush signed into law the Medicare ModernizationAct of 2003 (MMA), taking steps to expand private sector health care choices for current andfuture generations of Medicare beneficiaries. The MMA proposes short-term and long-termreforms that build upon more than 30 years of private sector participation in Medicare.
The centerpiece of the legislation is the new voluntary prescription drug benefit that will be madeavailable to all Medicare beneficiaries in 2006. Additional changes to the M+C program include:
M+C program’s name is changed to Medicare Advantage (MA); Increased funding is provided for MA plans in 2004 and 2005;

MA regional plans are established effective 2006.
On January 16, 2004 CMS announced new county base payment rates for the MA program.Beginning March 1, 2004, all county MA base rates received an increase which plans are requiredto use for enhanced benefits. Plans may use the extra money in one of four ways:
Reduce enrollee cost sharing; Enhance benefits for enrollees; Increase access to providers; Utilize the stabilization fund.
The short-term reforms have already improved benefits and reduced out-of-pocket costs formillions of Medicare beneficiaries who are covered by health plans in the Medicare Advantageprogram, previously known as the Medicare+Choice program. These coverage improvementsbecame effective on March 1, 2004.
On June 1, 2004, beneficiaries saw additional improvements in Medicare under another importantMMA initiative, the Medicare-Endorsed Prescription Drug Discount Card Program, which willremain in effect through the end of 2005. This program gives beneficiaries the option ofpurchasing prescription drug discount cards—sponsored by private sector entities and endorsedby Medicare—which offer discounted prices on prescription drugs. Furthermore, the discountcard program is providing low-income Medicare beneficiaries with up to $600 annually inassistance, in both 2004 and 2005, to help cover their prescription drug costs.
Beginning in 2006, the MMA will provide beneficiaries with a broader range of private healthplan choices similar to those that are available to working-age Americans and federal employees.In addition to the locally-based health plans that currently cover more than 4.6 million Medicarebeneficiaries, regional PPO-style plans will be available as a permanent option under theMedicare Advantage program.
Beginning in 2006, all beneficiaries will have the option of choosing prescription drug coveragedelivered through private sector entities. This coverage will be available as a stand-alone drugbenefit or, in other cases, as part of a comprehensive benefits package offered by MedicareAdvantage health plans.
Other important provisions of the MMA address Medigap choices and specialized MedicareAdvantage plans for beneficiaries with special needs.
Public comments on the regulations are currently in review, and changes to the draft regulationsare anticipated. Final regulations are expected in the spring of 2005, and content updates will bemade after the release of the final regulations.
The Federal Employee Health Benefits Program. The Federal Employee Health BenefitsProgram (FEHBP) is a voluntary health coverage program for federal employees, retirees, andtheir dependents and survivors.3 The Office of Personnel Management (OPM) oversees theFEHBP, which offers plan members a choice among fee-for-service (FFS) plans and HMOs.Because of its size and membership, plan design requirements for the FEHBP often influenceplan design in the private sector. The OPM has generated several requirements for mandatedbenefits, including no limits on annual coverage for behavioral health benefits. Some healthcare
analysts have proposed the FEHBP as a model for a national healthcare plan. It has already beenused as a model for various quality assessment and improvement initiatives.
Tricare
TRICARE is the healthcare benefit program offered by the federal government to active andinactive military personnel and their families. It is the result of the federal government'sconscious decision to incorporate health plans into its traditional FFS program. TRICARE offerseligible members three plan options:
1. TRICARE Prime-a capitated HMO;2. TRICARE Extra-a PPO; and3. TRICARE Standard-a fee-for-service plan.4
Coordination of services between civilian and military providers is an important focus ofTRICARE because civilian providers now deliver many healthcare services to the militarypopulation.
State Governments
Like the federal government, state governments serve as both healthcare regulators andpurchasers. For example, states act as purchasers of healthcare coverage for state and localgovernment employees. Expectations for these populations parallel expectations established forfederal programs. The influence of state governments as purchasers, however, is focused on twomajor programs: Medicaid and workers' compensation. This section provides a brief descriptionof Medicaid and workers' compensation. More detailed discussions are presented later in the text.
Medicaid is a joint federal/state program designed to provide healthcare benefits to low-incomefamilies, children, and certain other groups of disabled and medically needy individuals. Thefederal government determines minimum eligibility standards, benefits, and providerreimbursement rates. It also provides funding for state programs. State governments provideadditional funding and oversee the administration of Medicaid at the state level. Currently, all butone of the states offers a health plan option to Medicaid recipients. A growing number of statesare making enrollment in health plans mandatory.
Health plans participating in state Medicaid programs are expected to accommodate the uniqueaccess needs of the Medicaid population, including locating appropriate providers at sitesconvenient to program recipients. In addition, states expect participating plans to address thespecial language, culture, education, and health/disability needs of the Medicaid population.
Workers' Compensation
Workers' compensation, often referred to as workers' comp, is a state-mandated insuranceprogram that provides benefits for medical expenses that are incurred and wages that are lost byworkers who suffer work-related injury or illness.5 Purchasers expect health plans participating inworkers' comp programs to address both of these issues.
An effort is underway in several states to combine healthcare coverage with disability incomecoverage and on-the-job accident coverage into one program, called 24-hour coverage. Wheneverhealth plan principles are applied to this combined coverage, the resulting plan is called 24-hour

health plan. The main effect of 24-hour health plan programs on a health plan's medicalmanagement function is that coverage for work-related injuries or illnesses and incomereplacement for the time period out of work are mandatory.
Provider Expectations
Providers working with health plans have three major concerns. First, providers want thehealthcare services that they deliver to meet proper medical and quality standards. In a traditionalFFS system, providers determine which services are provided and under what conditions. In ahealth plan environment, health plans may influence some of these decisions. For example, ahealth plan may establish standards for the types of tests authorized under certain circumstancesor for certain conditions.
Providers sometimes perceive that health plans make such decisions on the basis of cost ratherthan appropriateness of care and fear that this practice will have a detrimental effect on quality.Providers sometimes also perceive that nonmedical personnel are involved in making medicaldecisions and that health plans are practicing medicine without a license-a practice referred to asthe corporate practice of medicine. Health plans can alleviate these concerns, in part, byencouraging provider participation in defining what constitutes best medical practices and indeveloping clinical practice guidelines for medical services.
Second, providers want to retain a certain level of authority and autonomy in providing medicalcare. Providers feel that they, and not the health plan, should be the final authorities for medicaldecision making. Providers also want to have access to due process procedures in the event of aconflict between a provider and the health plan. Timely, well-documented, and objectiveprocedures in an appeals process are critical to allaying providers' concerns about theirparticipation in health plans.
Finally, providers want to know that health plans can provide necessary financial andadministrative support for their practices. For example, providers want health plans to establisheasy claims submission and reimbursement procedures, to provide timely payment of their fees,and to require providers to follow as few administrative procedures as possible. Ideally, providerswould welcome an integrated information system that would enable them to expeditecorrespondence and administrative record keeping. Providers want ready access to plan memberrecords, medical journals and research studies, and laboratory results. Providers also want theirhealth plan contracts to result in a steady stream of plan members and dependable income results.
Because of their growing negotiating power and their ability to articulate concerns andexpectations, providers can exert substantial influence over a health plan's medical managementfunction. For example, physicians and other providers may choose not to contract with a healthplan that does not meet their needs. A significant reduction in the number of providers in thenetwork can force a health plan to reduce the number of services it offers, which can, in turn,cause plan members and purchasers to look elsewhere for healthcare, perhaps following theproviders who have left the plan.
Plan Member Expectations
Plan members' expectations for health plans have evolved as members have become betterinformed about healthcare issues and have refined their ideas about what constitutes quality,
affordable, and accessible healthcare benefits. Today, health plan members expect health plans tooffer the following benefits and services:
Benefits and Services
Provider choice. Plan members want freedom of choice with respect to the primary careprovider (PCP) network, hospitals, specialists, and ancillary service providers, such aspharmacies, laboratory services, and behavioral health services. In some cases, planmembers desire direct access to specialty care providers without obtaining a PCP referral.
High quality care. Plan members expect providers to be competent and to deliverappropriate, quality healthcare.
High quality service. Plan members expect health plans to provide courteous and promptresponses to requests for information, quick resolution of coverage issues, and customer-service-oriented providers at all levels.
Low cost. Plan members expect plans to minimize the amount of out-of-pocket expensesmembers are required to pay for care and services.
Information on plans. Plan members expect their health plans to provide informationabout covered healthcare services, treatment options, and network providers andlocations.
Medical information. Members are becoming interested in obtaining information via theInternet, including information on illnesses, medical procedures, and chronic conditions,online health assessments, e-mail addresses of network providers, and prescription refills.
Healthcare benefit options. Members often want healthcare options that includecomplementary and alternative medicine choices (for example, chiropractic services,acupuncture, biofeedback, and therapeutic massage).
Confidentiality of medical records. Confidentiality is becoming increasingly importantas healthcare information is transmitted and stored electronically and as plan membersdemand instant access to their medical records and to information concerning variousillnesses and conditions.
Grievance and appeals processes. Members want health plans to provide explicitprocesses for resolving disputes over nonauthorization of payment for specified medicalservices or providers, and appropriate medical treatment. Health plans that fail to provideplan members with appropriate avenues of due process leave themselves potentiallyliable for breach of fiduciary duty under ERISA at the federal court level, civil lawsuitsfor negligence or medical malpractice at the state court level, and increased pressure byconsumer groups for Congress to pass a patients' bill of rights concerning healthcareservices.
Health plans are responding to increased awareness and expectations of plan members byadjusting their medical management functions to meet members' needs. In the past, health planslooked to employers and government programs as their primary market for purchasers. Recently,health plans have begun to see individual plan members as purchasers. As plan members seekmore customization in their healthcare benefits and as their employers become more willing toallow it, individual healthcare plans within a group environment become a possibility.
For example, an employer can allot a specified dollar amount for healthcare benefits for eachemployee and then allow employees to contract for their own coverage. If the cost of anemployee's selected healthcare coverage exceeds the dollar amount of the employer allotment,then the employee makes up the difference. In this way, the employee's coverage shifts from a"defined benefit" (i.e., employer contribution depends on the number and type of benefits
included in the plan) to a "defined contribution" (i.e., employer contributes a specified dollaramount and employee contributes any additional dollar amounts to pay for healthcare coverage).
Other trends in meeting plan member expectations include: (1) a shift in marketing efforts towardwomen, who utilize healthcare services more frequently than men and who often make thehealthcare decisions in a family; (2) more emphasis on long-term, chronically disabling illnessesin a population that is growing older; and (3) an increased awareness of the language, cultural,and economic barriers that affect healthcare in a culturally diverse population.
Legal and Regulatory Requirements That Affect Medical Management
Purchasers, providers, and plan members influence the perceived need for laws and regulations tosupport the quality of medical care available through health plans. Over the years, public interestin healthcare has increased dramatically. Consumers, many of whom have been enrolled in healthplan programs without choice and are unfamiliar with the system, have expressed concern overthe quality of healthcare services available to them. Because of the human interest appeal ofhealthcare issues, media coverage of health plans have also grown. As a result, a number of lawsand regulations designed to support quality medical care have been enacted at both the federaland state levels. Many of these laws and regulations have a direct impact on medicalmanagement.
To see that their interests are properly represented and that legislators are adequately educatedabout health plan principles and practices, health plans must be aware of and participate in thelegislative process. Health plans must also comply with all applicable federal and state regulatoryrequirements.
In the following sections, we will look first at laws and regulations that apply at the federal leveland then at state requirements and case law requirements. Keep in mind that federal and stategovernments often share jurisdiction over health plans and that regulatory requirements mayoverlap, or even conflict.
Federal Laws and Regulations that Affect Medical Management
A variety of federal laws and regulations affect medical management. Those laws related toemployee benefits, health insurance, budget reconciliation, and patient protection, are especiallyimportant.
Employee Retirement Income Security Act of 1974
Employee health benefit plans, except those maintained by government employers, are currentlysubject to regulation under a federal law called the Employee Retirement Income Security Act(ERISA) of 1974, which is designed to maintain the proper funding and administrativemanagement of pension and employee welfare benefit plans.6 The Act includes a preemptionprovision which states that ERISA takes precedence over any state laws that regulate employeewelfare benefit plans.
ERISA has important implications for medical management, especially in cases in which anemployee raises questions of noncoverage of benefits related to medical appropriateness. Planmembers and their families who obtain healthcare benefits through employee benefit plans must
file legal challenges involving coverage issues or administration of the plan at the federal level,and ERISA is generally the governing law for such cases.
Unlike most state laws, ERISA limits damage awards in lawsuits to the cost of denied treatment;it does not allow plan members to obtain compensatory or punitive damages. For example, a planmember who brings a lawsuit for nonauthorization of payment based on the health plan's decisionthat the service was not medically necessary can recover benefits that a court of law determineswere inappropriately denied. However, the plan member cannot recover monetary amounts forpain and suffering or awards designed to deter employers or health plans from makinginappropriate decisions in the future. As a result of these ERISA provisions, it is in a health plan'sbest interest to have a case tried at the federal level.
Fast Definition
Compensatory damages are monetary amounts that the law awards as compensation for alegal wrong. In most tort cases, damages are the amount of money that will compensatethe injured party for his or her injuries.
Punitive damages are monetary amounts that are awarded to punish or make an exampleof the wrongdoer in order to dissuade others from similar behavior.
Currently, plaintiffs are challenging ERISA's preemption provision in many cases in the federalcourts. Such cases question the intent of the U. S. Congress to preempt state laws via federal lawssuch as ERISA. The judicial system has not yet defined a clear direction regarding whetherlitigation against ERISA plans is to be pursued through federal or state court. The system has alsonot defined the remedies that are available to members of managed healthcare plans covered byemployee benefit plans subject to ERISA regulation. Some recent court decisions on ERISApreemption, however, indicate that ERISA may not provide health plans with automaticprotection from damages, especially in cases dealing with the quality of care arranged by theplan.
Also, federal legislators are considering changing ERISA, particularly its preemption clause. Iflegislation is passed to eliminate the ERISA preemption, then plan members may sue health plansand group purchasers in state court for remedies that include compensatory and punitive damages.
Health Insurance Portability and Accountability Act
The Health Insurance Portability and Accountability Act (HIPAA) of 1996, which increases thecontinuity and portability of healthcare coverage in the group and individual health care markets,specifies that a group health plan may not deny coverage or discriminate against individuals onthe basis of their health status.7
HIPAA provides additional patient protections through the following standards:
HIPAA's patient protections through amendments and standards.8
Provisions for long-term care coverage, which define insurance contracts that containlong-term care coverage as accident and health plans and specify that premiums paid andbenefits received are medical care expenses that are excluded from the insured's grossincome for tax purposes.
Standards for privacy of individually identifiable health information, which prohibithealthcare organizations from releasing identifiable patient health information forpurposes other than medical treatment, payment, quality assurance, or utilization review,without the patient's consent. Standards apply only to electronically transmittedinformation, and regulation is, in some cases, superseded by pre-existing state and federallaws.
Standards for electronic data security, which define the security measures health careorganizations must take to protect the confidentiality of electronically stored andtransmitted patient information. Measures endorsed by HIPAA regulations include accesscontrols, callback procedures to verify the identify of users, passwords, authenticationprocedures to verify the identity of entities using the system, automatic logoffs afterperiods of inactivity, and recording audit trails.
HIPAA provisions and standards affect both the benefits health plans provide to their membersand the ways in which those benefits are administered. For example, health plans are required toinform plan members about HIPAA provisions and to issue certificates of creditable coverage toall plan members. Plans may not delegate this responsibility to a third party administrator. Healthplans must also establish special open enrollment periods for individuals who lose other healthcoverage or who become eligible for coverage as dependents. In addition, health plans mustdevelop information systems that support electronic claims processing and comply withconfidentiality and information security standards.
Complying with HIPAA mandates requires not only planning, but additional allocation ofresources, especially in the area of information management. Some health plans worry thatHIPAA requirements will create administrative nightmares and make the collection of qualitydata expensive or even impossible. Noncompliance, however, is likely to result in serioussanctions. Violators face the possibility of civil penalties of up to $25,000 and criminal penaltiesof up to $250,000 and up to 10 years in prison per violation.
Balanced Budget Act of 1997
The Balanced Budget Act (BBA) of 1997 facilitated the enrollment of beneficiaries ofgovernment-sponsored health programs in health plans and allocated funding for health insurancefor uninsured children.
The BBA established the Medicare+Choice program, the social health maintenance organization(SHMO) program, and the Programs of All-Inclusive Care for the Elderly (PACE). Each programhas specified coverage, solvency, and organizational requirements that directly affect a healthplan's medical management function. The BBA also requires health plans to develop qualityimprovement programs in areas such as healthcare outcomes, utilization review, and coordinationof care. The Balanced Budget Refinement Act (BBRA) of 1999 modifies some of therequirements and implementation schedules established in the BBA for these programs. Theimpact of the BBA on Medicare and Medicaid programs is discussed in more detail in the lessonsMedicare and Medicaid.
Federal Agency Requirements
Health plans are also subject to a variety of requirements established by regulatory agencies. Thefollowing sections highlight the impact that several key federal agencies have on medicalmanagement. A more complete discussion of these programs is included in later assignments.
Department of Health and Human Services
The Department of Health and Human Services (HHS) oversees many government healthcareprograms. In addition to Medicare and Medicaid, HHS has authority over Programs of All-Inclusive Care for the Elderly (PACE), a joint federal-state program designed to provide personsaged 55 or older who require a nursing-facility level of care with an alternative to institutionalcare, and the State Children's Health Insurance Program (SCHIP), a federal-state programdesigned to enable states to initiate and expand child health assistance to uninsured, low-incomechildren by providing initial and matching funding over time. The Centers for Medicare andMedicaid Services (CMS), a division of HHS, is responsible for administering these programs.
One important goal of CMS' administration of the Medicare and Medicaid programs is to supportthe delivery of quality healthcare services to eligible beneficiaries. Toward this goal, CMSrequires Medicare health plans to document improvements in clinical procedures and to collectand report on quality measures for comparison purposes. CMS has developed a quality initiativecalled the Quality Assessment Performance Improvement that is designed to strengthen healthplans' efforts to protect and improve the health and satisfaction of Medicare and Medicaidenrollees. Compliance with QAPI is mandatory for Medicare+Choice plans. For Medicaid, QAPIstandards serve as a model that states can use at their discretion to develop quality requirementsfor Medicaid health plans. QAPI standards cover the following broad domains:
Quality assessment and performance improvement Enrollee rights Health services management
In addition, CMS establishes delegation guidelines with which health plans that serve a Medicarepopulation must comply. The CMS requirements for delegation oversight are similar to those oftwo prominent accrediting agencies, NCQA and URAC, which we discuss later in this lesson. Ingeneral, delegated functions are held to the same CMS standards as the functions actuallyperformed by the health plan, and CMS will hold the health plan accountable for any deficienciesin the delegate's performance. CMS is also directly involved in the development of standards forelectronic medical record (EMR) transactions as they relate to the Medicare and Medicaidprograms.
The healthcare needs of medically underserved populations are also addressed through suchprograms as the National Health Service Corps, Federally Qualified Health Centers, and theIndian Health Service. These programs are administered by the Health Resources and ServicesAdministration (HRSA) division of HHS. Decisions of agencies such as the CMS and HRSAdirectly affect health plans that serve these populations.
Department of Defense
The Department of Defense (DOD) oversees all military healthcare programs, which are amongthe largest in the United States. In addition, the DOD frequently establishes minimum benefit andadministrative requirements that health plans must meet if they want to serve the military market.The DOD's decisions regarding quality, access, and program choice directly influence how ahealth plan designs and implements its medical management activities. The evolution ofhealthcare benefit programs for active and retired military personnel and their dependents fromthe Civilian Health and Medical Program of the Uniformed Services (CHAMPUS), which was anindemnity-based plan, to TRICARE, which offers an indemnity plan but also a PPO plan and an
HMO plan, has also affected medical management. We discuss healthcare benefits programs forthe military in Other Government Programs.
Office of Personnel Management
The Office of Personnel Management (OPM) conducts human resources functions on behalf offederal government employees. One of its major functions is to oversee the Federal EmployeesHealthcare Benefits Program (FEHBP), which is the largest group healthcare plan in the nation.Healthcare benefits under the FEHBP are generally broader than those of most employer-sponsored group health plans.
Coverage decisions established for the FEHBP often set a precedent for coverage in the privatesector as well. For example, as a result of an executive order issued by the president, health plansthat serve federal employees must be in compliance with the Consumer Bill of Rights andResponsibilities recommended by the Advisory Commission on Consumer Protection and Qualityin the Health Care Industry. This directive is likely to have a significant effect on medicalmanagement in both FEHBP plans and private sector plans.
Federal Trade Commission
The Federal Trade Commission (FTC), along with the Department of Justice, enforces federalantitrust statutes. These statutes have a direct effect on health plans' provider contractingactivities. For example, in contracting with providers, a health plan must avoid creating tyingarrangements, which require a provider to purchase the health plan's healthcare benefits in orderfor the provider to participate in the health plan's network. Health plans must also guard againstengaging in horizontal group boycotts, in which two or more competing health plans decide toexclude a particular provider because the provider also contracts with another health plan.
Department of Justice
In addition to its involvement in antitrust matters in conjunction with the FTC, the Department ofJustice (DOJ) also oversees fraud and abuse matters as they relate to medical management.Because the costs associated with fraud and abuse can be extremely high, health plans activelyfocus on reducing the occurrence of fraud and abuse of healthcare benefits.
Health plans have noted two medical management conditions in particular that may signalpotential fraud and abuse: (1) purposeful underutilization of medically necessary healthcareservices in health plans that capitate their providers, and (2) purposeful overutilization of, andinappropriate billings for, services in plans that pay their providers on an FFS basis. Althoughutilization management of healthcare services helps reduce a health plan's medical service costs,underutilization of medically necessary services is detrimental to members' health and will likelylead to higher costs over the long term.
A number of other federal agencies also influence medical management. For example, the Officeof the Inspector General (OIG) is often involved along with the Department of Justice in dealingwith fraud and abuse issues. The Federal Drug Administration (FDA) and National Institute ofHealth (NIH) are important contributors to the development of medical policy. The Office ofMinority Health, a division of HHS, has proposed standards addressing the development ofculturally and linguistically appropriate services.

State Laws and Regulations
State governments typically regulate health plans through the state department of insuranceand/or department of health. Like federal laws and regulations, state laws and regulations and therequirements of specific organizations have a significant impact on a health plan's medicalmanagement programs. For example, many states have laws that require health plans to:
Laws Require Health Plans to:
Arrange for adequate access to healthcare providers and facilities Have specific quality management programs and take appropriate action to improve
quality deficiencies Follow specified guidelines, procedures, and registration requirements for utilization
review Report specified utilization and grievance information Provide plan members with adequate information about covered benefits, how to obtain
those benefits, and how to pursue grievances Have formal grievance processes in place for members and providers
In the following sections, we describe some of the areas in which state laws and regulations havethe greatest impact on medical management.
Benefit/Provider Mandates
One way in which state governments impact medical management is through mandated benefitlaws. Mandated benefit laws are state laws or federal laws that require health plans to arrange forthe financing and delivery of particular benefits, such as coverage for a stay in a hospital for aspecified length of time.10 The Newborns' and Mothers' Health Protection Act (NMHPA) is anexample of a federal law that mandates benefits. State laws have been enacted that require healthplans to provide for benefits including
Direct member access to certain specialists, such as OB/GYNs, dermatologists, or doctorsof chiropractic, without first going through a primary care provider
Coverage for emergency department visits, even if a subsequent diagnosis determinesthat the condition was not an emergency, if the presenting symptoms that caused a planmember to go to the emergency department appeared to be an emergency, such as chestpains
Hospice and home health benefits Mental health and chemical dependency services (behavioral healthcare) Benefits for specialized services such as post-mastectomy reconstructive surgery,
transplants, temporomandibular joint treatment, and infertility treatment
These mandates not only require that the benefits be covered, they also imply that particular typesof providers such as behavioral healthcare professionals must be included in the network.
In some cases, federal and state mandated benefit laws conflict with a health plan's goals formanaging the costs of delivering healthcare services. For example, mandated length-of-stay lawsfor maternity and mastectomy patients increase the costs of providing those healthcare benefitsand may not actually be medically beneficial in all cases.
Access to Quality Care and Service
Many of the state laws related to the quality of healthcare services are based on model lawsdeveloped by the National Association of Insurance Commissioners (NAIC), an organization ofstate insurance commissioners established to encourage uniformity in insurance regulation. In1996, the NAIC introduced a series of Health Plan Accountability Models. The following NAICModels specifically address the issue of quality in health plans:
Health Care Professional Credentialing Verification Model Act: specifies therequirements health plans must satisfy to see that network providers meet minimumstandards of professional qualification
Quality Assessment and Improvement Model Act: requires health plans to establishand report on systems for assessing the quality of care and services
Network Adequacy and Accessibility Model Act: specifies standards health plans mustmeet in developing and managing provider networks
Health Carrier Grievance Procedure Model Act: requires health plans to establishwritten procedures for handling member grievances
The NAIC has also developed model laws on health information privacy and state licensure. Statelaws and regulations based on these model acts apply to all health plans operating in those states.
Delegation
State governments and regulatory agencies have developed a variety of laws and regulations thatapply to the use of delegation by health plans. These regulations and laws help determine whichactivities, if any, a health plan may delegate and the nature of the delegation arrangement. Forexample, more than half the states have laws-based in whole or in part on the NAIC's HMOModel Act-requiring HMOs to include a description of their contractual arrangements fordelegation in their written quality improvement program. As we discuss later in this lesson, healthplans that seek accreditation must also meet the delegation-related standards of the relevantaccrediting agency. Because health plans are accountable for all delegated activities, regardless ofthe terms of the agreement for delegation, a high level of review and monitoring by the healthplan is required for all delegated activities.
Some states have more specific requirements for the delegation of medical management functionsby health plans. For instance, in Alabama, credentialing activities may be delegated only toentities that have been approved by the state for this purpose. Fourteen states require health plansto maintain oversight of delegated utilization review activities.11 Because state laws on delegationvary, a health plan must monitor the requirements of each state in which the health plan operatesand adjust its delegation programs accordingly.
Patient Protection
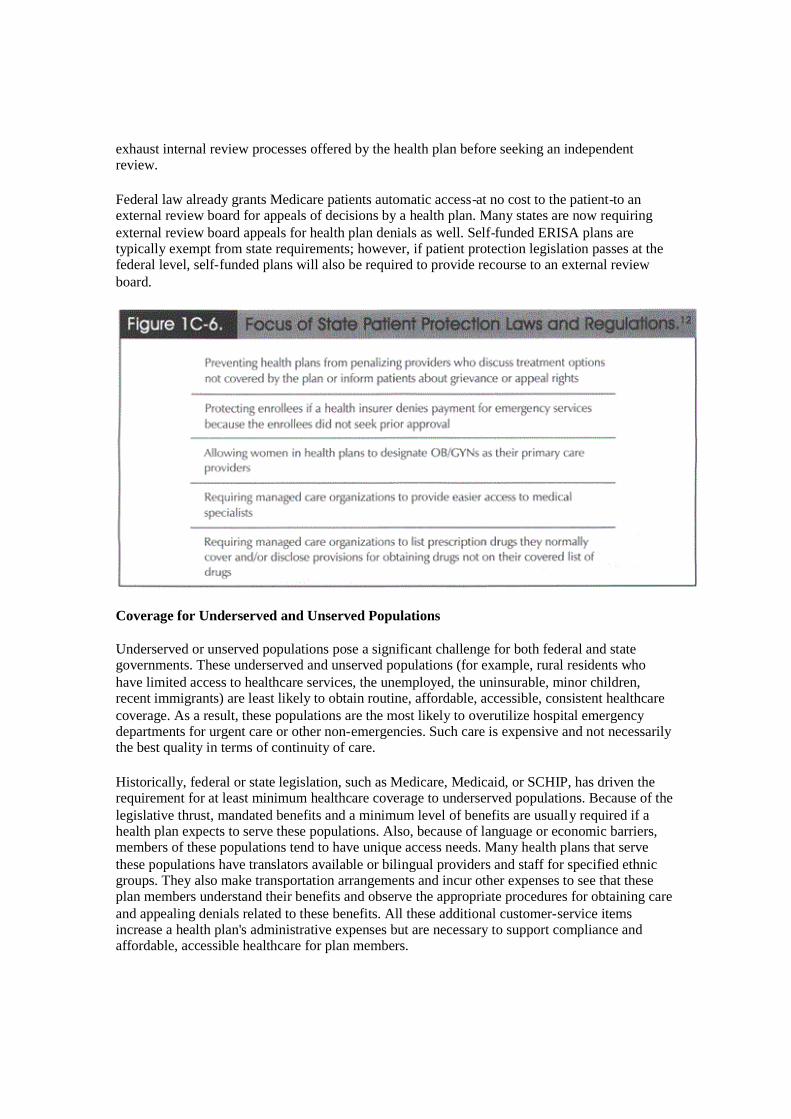
Patient protection has become an important issue at the state as well as the federal level. Figure1C-6 summarizes some of the major issues addressed by recent state legislative and regulatoryefforts.
Proposed patient protection bills also include provisions for the use of an external review board toserve as a second medical opinion or, in cases of claims denials or nonauthorization of paymentfor treatment, as an arbitration review panel. Most health plans currently require plan members to
exhaust internal review processes offered by the health plan before seeking an independentreview.
Federal law already grants Medicare patients automatic access-at no cost to the patient-to anexternal review board for appeals of decisions by a health plan. Many states are now requiringexternal review board appeals for health plan denials as well. Self-funded ERISA plans aretypically exempt from state requirements; however, if patient protection legislation passes at thefederal level, self-funded plans will also be required to provide recourse to an external reviewboard.
Coverage for Underserved and Unserved Populations
Underserved or unserved populations pose a significant challenge for both federal and stategovernments. These underserved and unserved populations (for example, rural residents whohave limited access to healthcare services, the unemployed, the uninsurable, minor children,recent immigrants) are least likely to obtain routine, affordable, accessible, consistent healthcarecoverage. As a result, these populations are the most likely to overutilize hospital emergencydepartments for urgent care or other non-emergencies. Such care is expensive and not necessarilythe best quality in terms of continuity of care.
Historically, federal or state legislation, such as Medicare, Medicaid, or SCHIP, has driven therequirement for at least minimum healthcare coverage to underserved populations. Because of thelegislative thrust, mandated benefits and a minimum level of benefits are usually required if ahealth plan expects to serve these populations. Also, because of language or economic barriers,members of these populations tend to have unique access needs. Many health plans that servethese populations have translators available or bilingual providers and staff for specified ethnicgroups. They also make transportation arrangements and incur other expenses to see that theseplan members understand their benefits and observe the appropriate procedures for obtaining careand appealing denials related to these benefits. All these additional customer-service itemsincrease a health plan's administrative expenses but are necessary to support compliance andaffordable, accessible healthcare for plan members.
Case Law
The laws outlined in the previous sections were developed and passed as federal and statestatutory laws. Case law also influences medical management. Case law, also called commonlaw, is a body of law that consists of federal and state court decisions.13 Monitoring case law iscritical because the outcome of a court case may clarify ambiguous sections of a particularstatute. Court decisions may also establish precedents that must be followed if a health plan is tocomply with the law. For example, the outcome of specific court cases under consideration invarious state courts may determine whether plan members can directly sue their health plans inthose states. Insight 1C-1 describes some of these cases.
Health Plan Liability and Medical Management Activities
As a result of federal and state regulation of health plans and other laws and regulations thataffect the daily operations of service businesses, health plans have legal obligations to planmembers and providers. These legal obligations often impact medical management activities.
Plans that violate these obligations can be held directly liable for any harm that results from theiractions. This would be the case if a court ruled that a health plan had made an inappropriateutilization management or provider credentialing decision and that decision had resulted in harm.
Plans may also be held accountable for the actions of other parties through vicarious liability.Vicarious liability is a kind of liability that arises when one party is held responsible for theactions of another party because of the existence of a special relationship between those twoparties.14 A claim for vicarious liability may arise in connection with a health plan's delegation ofcertain medical management activities.
For example, suppose that a health plan contracts with a utilization review organization (URO)for utilization review services and that URO improperly recommends denial of payment forservices to a plan member. The health plan can be directly liable if the health plan failed toadequately investigate the quality of the URO's services and the qualifications of its personnelprior to establishing the delegation arrangement or to provide proper oversight of the delegatedactivities.15 The health plan may also be liable for the URO's actions under state law if the UROis determined to be an agent-that is, the authorized representative-of the health plan or if the UROis determined to be an apparent, or ostensible, agent of the health plan.
Under the legal doctrine of apparent agency, also called ostensible agency, a health plan may beliable for the actions of a delegate if the following three conditions are true:
Health plan may be liable for actions of a delegate if
1. The health plan fails in some way to establish that the delegate is not the health plan'sagent.
2. A plan member perceives the delegate as an agent.3. In relying on this perception, the member suffers physical or financial harm.
To avoid the appearance that the delegate is an agent of the health plan, any documents that referto the delegation arrangement, including marketing materials and written agreements between thehealth plan and the delegate, should specify that the delegate is an independent contractor and notan agent.16
Vicarious liability may also arise in connection with medical malpractice committed by a planphysician or other healthcare provider against a plan member if the health plan is deemed liablebecause of the contractual relationship between the health plan or plan and the provider.
One way that health plans can protect themselves from the prospect of litigation based on theliabilities discussed above is to structure utilization review, case management, and diseasemanagement programs so that the cost of treatment has no bearing on what is consideredmedically appropriate. In subsequent lessons, we discuss Utilization Review, Case Managementand Disease Management.
Impact of Accreditation on Medical Management
Accreditation organizations independently evaluate the quality of a health plan's services. Theinformation provided by the accreditation process is intended to help purchasers and possiblyconsumers make well-informed decisions when choosing and contracting with a health plan.However, the process itself presents challenges for health plans.
Participation in the accreditation process is voluntary, and health plans are responsible forgathering and submitting the data needed for accreditation purposes. For most plans, the processof gathering accreditation information is both time consuming and expensive. For example, thedecentralized structure of some managed healthcare plans makes it necessary to collect data fromseparate physical locations including administrative offices, physician offices, labs, and hospitals.In many cases, the costs of obtaining the information technology needed to amass extensiveperformance data can be prohibitive.
In addition, despite the value of accreditation ratings for the comparison of quality among healthplans, few purchasers and fewer consumers review the results of accreditation in makingdecisions to purchase or enroll in a specified health plan. Instead, purchasers tend to make healthplan choices on the basis of cost, which is easier to measure than quality. Plan members often rateplan quality on the basis of whether a particular provider is in the plan's network and whether aspecified healthcare benefit is covered.
As a result, many health plans elect not to participate in the accreditation process. However, asquality standards and accreditation results increasingly focus on evidence-based medicine-forexample, positive outcomes realized from disease management programs-as an indicator ofquality, purchasers and plan members may rely more on the reported results of the accreditationprocess. As purchaser demand for comparative quality data increases, more health plans-particularly plans that serve the large employer market-may find it necessary, despite the costs, toparticipate in the accreditation process.
Accreditation Organizations
Accreditation is typically conducted by independent, not-for-profit organizations, which are notaffiliated with federal or state governments. The following sections introduce several keyaccreditation organizations in the health plan industry. These organizations and their standardsand guidelines are discussed in more detail in lesson Quality Management.
National Committee for Quality Assurance
The National Committee for Quality Assurance (NCQA), an independent, not-for-profitorganization, serves as the primary accrediting agency for most HMOs and similar health plans,managed behavioral healthcare organizations (MBHOs), credentials verification organizations(CVOs), and physician organizations. NCQA's accreditation is a rigorous and comprehensiveevaluation process through which the quality of all key systems and processes that make up thehealth plan are assessed. Accreditation and certification results are available through NCQA'sWeb site. NCQA also has developed the Health Plan Employer Data and Information Set(HEDIS), which is used as a factor in the accreditation process as we discuss later in this lesson.
National Committee for Quality Assurance
NCQA reports health plans' accreditation results publicly using the following five categories, allof which have a direct impact on a health plan's medical management functions:
Access and service Qualified providers Staying healthy Getting better Living with illness17
The NCQA also surveys the systems and processes of health plans against the following sixcategories:
Quality improvement Utilization management Credentialing Member rights Preventive health Medical records
Results in these categories are not publicly reported.
CVOs are evaluated on the basis of such categories as malpractice insurance, liability claimshistory, and sanctions concerning Medicare, Medicaid, and the appropriate medical board.
American Accreditation HealthCare Commission/URAC
The American Accreditation HealthCare Commission/URAC (URAC) is an accrediting agencythat promotes consistent standards in the application of utilization procedures and providernetwork standards. URAC's standards focus on five key areas:
Network management Utilization management Quality management Credentialing Member participation and protection18
URAC has also developed accreditation programs for case management programs, CVOs, healthplan telephone call centers, and workers' compensation services.
Accreditation Standards for Delegation
NCQA and URAC all consider a health plan's management of delegated activities whenevaluating a health plan for accreditation. These three agencies have established specificstandards for the oversight of delegated activities. Although all three accrediting agencies'standards have the same intent-to see that the delegated activities are performed in accordancewith the delegating health plan's standards-the specific requirements of their standards aresomewhat different. For example, URAC place no restrictions on the types of functions that canbe delegated. NCQA allows health plans to delegate authority for almost all functions, butrequires that the health plan itself conduct all delegation oversight activities rather than delegatingthe responsibility for oversight to another entity.21
Although health plans that seek accreditation typically design their delegation oversight programaccording to the standards of the relevant accrediting agency, most programs include provisionsrelated to accountability and documentation.
Accountability
Accountability is the process by which one party is required to justify its actions and policies toanother party. When a health plan delegates authority for a function, it transfers the power toconduct the function on a day-to-day basis, but not the ultimate accountability for the function.Although the delegate assumes the authority to plan and carry out the function within specifiedparameters, the health plan retains the responsibility for making sure that the delegate acts inaccordance with the health plan's standards and those of NCQA or URAC. If the delegate'sperformance fails to meet these standards, the health plan is responsible for developing correctiveaction requirements to guide the delegate in making a plan to remedy the deficiencies. The healthplan is also accountable for maintaining coordination and continuity between the delegatedfunctions and the functions that are conducted by the health plan.
Documentation
All three accrediting agencies require documentation showing that the health plan is conductingappropriate oversight of the delegated function. Such oversight typically includes regular reportsfrom the delegate to the health plan and formal site visits and audits by the health plan on anannual basis or more frequently. In addition, both URAC and NCQA require writtendocumentation of the agreement between the health plan and the delegated entity.
In some cases, accreditation standards for delegation oversight are reduced if the delegate hasalready been certified or accredited by the health plan's accrediting agency. For example, if thedelegating health plan adheres to NCQA standards and the delegate is an NCQA-accreditedhealth plan or MBHO or an NCQA-certified CVO or physician organization, the delegatinghealth plan's oversight obligations are reduced. Although NCQA still requires an appropriatewritten agreement between the health plan and the delegate, the health plan is not obliged toconduct a formal, annual oversight review of the accredited entity on any elements for which thedelegate has been certified.23 Similarly, if a health plan accredited by URAC delegates activitiesto a URAC-certified CVO or utilization management organization, URAC does not require thehealth plan to perform annual oversight reviews of elements already certified for that delegate.
Additional Quality Initiatives
Besides the quality measures from accreditation organizations discussed in the previous sections,various other attempts to measure quality have been developed. The following sections discussseveral of these additional quality initiatives.
Health Plan Employer Data and Information Set
NCQA developed the Health Plan Employer Data and Information Set (HEDIS), which is aperformance measurement tool designed to help healthcare purchasers and consumers comparethe quality offered by different health plans.23 Since 1999, NCQA has integrated HEDISmeasures into its accreditation standards, and CMS now requires Medicare plans to reportNCQA-audited data on HEDIS performance measures.
Health Plan Employer Data and Information Set
HEDIS measures comprise eight domains as listed below. Note that not all of these domains areconsidered in the accreditation process.
Effectiveness of care (e.g., cancer screening, childhood immunizations) Access/availability of care (e.g., prenatal care, adults' and children's access to preventive
and primary care services) Satisfaction with the experience of care (e.g., plan member satisfaction) Health plan stability (e.g., financial strength, provider and plan member turnover) Use of services (e.g., hospital utilization, mental health utilization) Cost of care (e.g., premium rate trends) Informed healthcare choices (e.g., language translation services, information provided
during enrollment, plan member education services) Health plan descriptive information (e.g., board-certification of physicians, case
management, quality improvement)
The National Forum for Health Care Quality Measurement and Reporting
The National Forum for Health Care Quality Measurement and Reporting, also called theQuality Forum, is a not-for-profit organization that was established to develop and implement anational strategy for quality measurement and reporting. The Quality Forum develops standardsfor measuring healthcare service quality. Although initially established as a result of apresidential advisory commission recommendation, the Quality Forum's funding is obtained fromthe private sector. A secondary objective of developing quality standards is for the benefit ofproviders, who can use standard measures of quality to improve their performance. Thepresidential advisory commission originally proposed the following categories for the QualityForum:
Objectives for the Quality Forum25
Identify core sets of quality measures for standardized reporting by all sectors of thehealthcare industry
Establish a framework and capacity for quality measurement and reporting Support the focused development of quality measures that enhance and improve the
ability to evaluate and improve care
Make recommendations regarding an agenda for research and development needed toadvance quality measurement and reporting
See that comparative information on healthcare quality is valid, reliable, comprehensible,and widely available in the public domain
Agency for Healthcare Research and Quality (AHRQ)
The Agency for Healthcare Research and Quality (AHRQ), formerly the Agency for Health CarePolicy and Research (AHCPR), is an organization that performs research functions for HHS. In1999, Congress changed the focus of the agency from medical treatment research and thecollection of health statistics to research on healthcare delivery and quality measurement andimprovement. This new focus, along with an increased budget, expands the agency's impact onimproving healthcare quality.
One of AHRQ's major contributions to healthcare quality is the Consumer Assessment of HealthPlans Survey (CAHPS™), which gathers comparative data on healthcare service quality acrosspopulations. CAHPS measures consumer satisfaction with specified aspects of health planservices, including access to care and the relationship between consumers and their physicians.Specific questions address consumer experiences with treatments for chronic conditions or withMedicare or Medicaid managed plans26. NCQA and AHRQ recently merged CAHPS with theHEDIS Member Satisfaction Survey.
Conclusion
As you can see, medical management goes far beyond a health plan's internal considerationsregarding the quality and cost of healthcare services. It is a complex process that requires healthplans to understand the needs and expectations of its purchasers, providers, and plan members aswell as the requirements of various legislative, regulatory, and accrediting bodies. In order todevelop successful medical management programs, health plans must understand the dynamics ofthe environment in which they operate and consider how the environment affects the delivery ofhealthcare services.
Endnotes
1. Margaret Ann Cross, "Employers Starting to Hold HMOs Accountable for Quality,"Health Plan (May 1999): 42A.
2. Nicholas L. Desoutter and Kenneth Huggins, eds., LOMA's Glossary of Insurance Terms,3rd edition (Atlanta, GA: LOMA, 1997)
3. Academy for Healthcare Management, Managed Healthcare: An Introduction, 2ndedition (Washington, DC: Academy for Healthcare Management, 1999), 11-29.
4. Academy for Healthcare Management, Managed Healthcare: An Introduction, 2ndedition (Washington, DC: Academy for Healthcare Management, 1999), 11-30.
5. Academy for Healthcare Management, Network Management in Health Plans(Washington, DC: Academy for Healthcare Management, 1999), 7-48.
6. Academy for Healthcare Management, Network Management in Health Plans(Washington, DC: Academy for Healthcare Management, 1999), 1-19-1-21.
7. Academy for Healthcare Management, Network Management in Health Plans(Washington, DC: Academy for Healthcare Management, 1999), 1-20.
8. W. Reece Hirsch, "Call the Lawyers: Making Web Sites HIPAA-Compliant,"healthcarebusiness (January/February 2000): 58.
9. Muriel L. Crawford, Life and Health Insurance Law (Boston, MA: Irwin/McGraw-Hill,1998), 61.
10. Academy for Healthcare Management, Health Plans: Governance and Regulation(Washington, DC: Academy for Healthcare Management, 1999), 9-2-9-3.
11. Academy for Healthcare Management, Health Plan Finance and Risk Management(Washington, DC: Academy for Healthcare Management, 1999), 3-8.
12. American Accreditation HealthCare Commission/Utilization Review AccreditationCommission (URAC), Survey of State Utilization Laws and Regulations, 1999 ed.(Washington, DC: American Accreditation HealthCare Commission/Utilization ReviewAccreditation Commission, 1998), 7.
13. Academy for Healthcare Management, Health Plans: Governance and Regulation(Washington, DC: Academy for Healthcare Management, 1999), 4-4.
14. Academy for Healthcare Management, Health Plans: Governance and Regulation(Washington, DC: Academy for Healthcare Management, 1999), 12-8.
15. Cynthia Conner, et al., "Basis for Liability," in Health Plan Law Manual (Gaithersburg,MD: Aspen Publishers, 1999), 2: 4.
16. Cynthia Conner, et al., "Utilization Management," in Health Plan Law Manual(Gaithersburg, MD: Aspen Publishers, 1999), 1: 6-7.
17. Academy for Healthcare Management, Network Management in Health Plan(Washington, DC: Academy for Healthcare Management, 1999), 1-28-1-29.
18. Academy for Healthcare Management, Network Management in Health Plans(Washington, DC: Academy for Healthcare Management, 1999), 6-52.
19. Academy for Healthcare Management, Network Management in Health Plans(Washington, DC: Academy for Healthcare Management, 1999), 1-30.
20. Academy for Healthcare Management, Network Management in Health Plans(Washington, DC: Academy for Healthcare Management, 1999), 1-29.
21. Academy for Healthcare Management, Network Management in Health Plans(Washington, DC: Academy for Healthcare Management, 1999), 1-30.

22. National Committee for Quality Assurance (NCQA), 1998 Surveyor Guidelines for theAccreditation of Health Plans (Washington, DC: National Committee for QualityAssurance, 1998), 369.
23. National Committee for Quality Assurance (NCQA), 1998 Surveyor Guidelines for theAccreditation of Health Plans (Washington, DC: National Committee for QualityAssurance, 1998), 369.
24. Academy for Healthcare Management, Managed Healthcare: An Introduction, 2ndedition (Washington, DC: Academy for Healthcare Management, 1999), 8-15.
25. Academy for Healthcare Management, Managed Healthcare: An Introduction, 2ndedition (Washington, DC: Academy for Healthcare Management, 1999), 8-14. Used withpermission; all rights reserved.
26. "Quality Forum Planning Committee Schedules Meeting," 4 May 1999,http://www.uhfync.org/intro/qfpc.htm (11 May 1999).
27. Agency for Healthcare Research and Quality, "Consumer Assessment of Health Plans(CAHPS™): Fact Sheet," http:www.ahcpr.gov/qual/cahpfact.htm (15 June 1999).





























