Embed Size (px)
Citation preview

Leslie Partridge, RRA, MSRT(R)
Drawings by: Joshua Tussing, MSRT(R)(N), RRA

OBJECTIVES
Discuss patient screening, pre-procedure assessment and patient education
process.
Review intrathecal contrast administration
Medication interactions
Allergy issues
Selection of appropriate concentration and dosage
Risks
Analyze puncture and procedure techniques, contraindications and
complications
Present myelogram studies to examine anatomy, procedure technique and
pathology.
I have no disclosures.

HISTORY OF MYELOGRAPHY
1920s – air into subarachnoid space for X-ray eval of spinal tumors
1920s-1930s – oil-based lipiodol
1940s – oil based but less viscous iophendylate(Pantopaque)
1950s-1960s – Iodinated water-soluble, ionic
Methiodal (Abrodil), meglumine iothalamate (Conray), meglumineiocarmate (Dimer X)
1970s – first nonionic water-soluble, metrizamide(Amipaque), CT imaging
1980s – MRI use takes over much of spinal imaging
Today – nonionic water soluble
Iohexal (Omnipaque), iopamidol (Isovue)

INDICATIONS
Pathology contacting, displacing
or impinging on thecal sac,
spinal cord or nerve roots
Degenerative changes of disks,
vertebrae or ligamentum flavum
Examine arachnoid cysts,
arachnoiditis, perineural cysts
Preference of referring surgeon
Cannot have an MRI
Radiation therapy planning
Back or neck pain
Extremity weakness,
radiculopathy, paresthesia
Incontinence
Gait disturbance
Trauma


MRI VS MYELOGRAPHYMRI Myelography
Less invasive
No radiation
No intrathecal contrast
Often no contrast
Intramedullary lesions
Tumors, infarction, demyelination
Extramedullary lesions
Meningiomas, nerve sheath tumors
Negatives:
Low osseous detail, CSF pulsation
artifact, motion degradation,
surgical hardware, claustrophobia
Physician involvement
Improved look at osseous structures
Trauma, congenital anomaly, spinal column curvature
Stenosis by bone or soft tissue
Functional
Delayed passage of contrast across severe stenosis
Dynamic - upright, flexion, extension
Post-op spine
Brachial plexus injury
Radiation therapy planning
CSF leak evaluation
Negatives
Contrast, needles, pain, positioning, radiation

PATIENT SCREENING
History
Indication/symptoms, surgeries,
allergies, current status
Medications
Lab studies
Prior imaging studies
Potential contraindications
Elevated intracranial or intraspinal
pressure
Soft tissue infection at/near
puncture site
Systemic infection with likely
bacteremia
Coagulopathy
Uncooperative patient
Pregnancy
Hepatorenal insufficiency
Contrast allergy
History of seizures
PATIENT PREP
Call 2 days prior to exam
Hold blood thinners or meds that decrease seizure threshold
If contrast allergy, verify premedication
NPO for 4 hours before exam
Except necessary medications
Bring medications for after
Bring outside imaging studies or reports
Must have a driver and someone to help them at home for 24 hours
Arrival time
2 hours early if need coags day of
30 minutes early otherwise
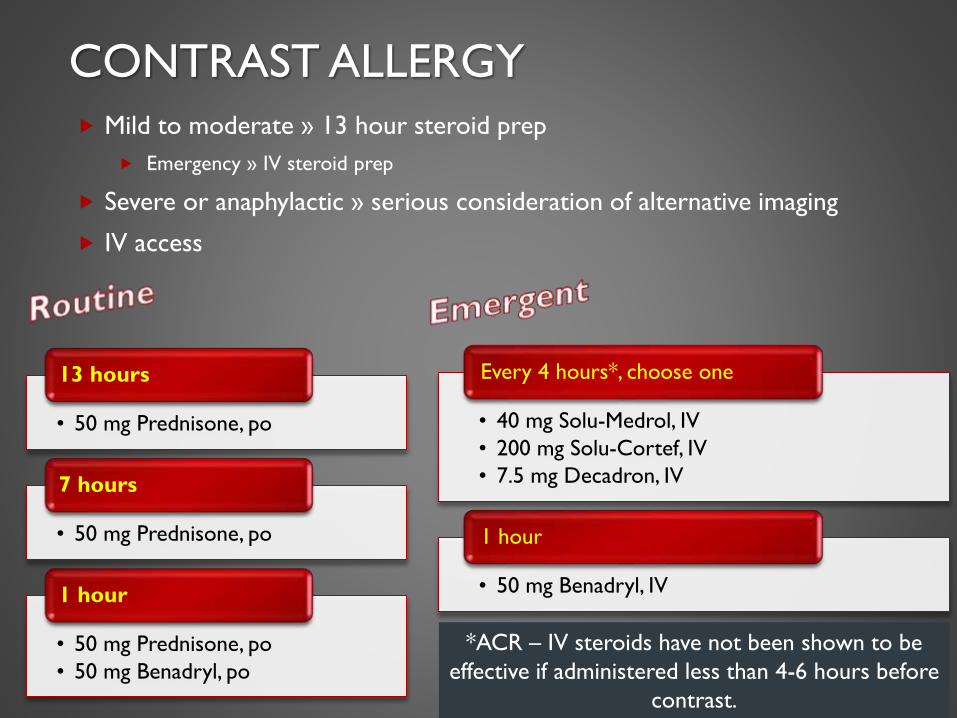
CONTRAST ALLERGY
Mild to moderate » 13 hour steroid prep
Emergency » IV steroid prep
Severe or anaphylactic » serious consideration of alternative imaging
IV access
• 50 mg Prednisone, po
13 hours
• 50 mg Prednisone, po
7 hours
• 50 mg Prednisone, po
• 50 mg Benadryl, po
1 hour
• 40 mg Solu-Medrol, IV
• 200 mg Solu-Cortef, IV
• 7.5 mg Decadron, IV
Every 4 hours*, choose one
• 50 mg Benadryl, IV
1 hour
*ACR – IV steroids have not been shown to be
effective if administered less than 4-6 hours before
contrast.

MEDICATION REVIEWMeds that reduce seizure threshold
Antipsychotics
Psychoactives
Muscle relaxants
Antidepressants
Phenothiazines
MAOIs
Tricyclic
CNS stimulants

MEDICATION REVIEW – BLOOD THINNERSMedication Hold
Warfarin/Coumadin/Jantoven 3-5 days, INR < 1.5
Heparin <10,000U no hold; >10,000U 2-4 hours + normal PTT
Restart 1 hour after
Enoxaparin/Lovenox 40mg QD 12 hours; Treatment dose (1-1.5mg/kg or 100mg
Q12 h) 24 hours before + after
Dalteparin/Fragmin Prophylaxis 12 hours; Treatment 24 hours before + after
Dabigatran/Pradaxa 5 days + normal PTT
Fondaparinux/Arixtra <2.5mg QD 48 hours; 5-10 mg 72 hours
Rivaroxaban/Xarelto Hold 18 hours
Apixaban/Eliquis, Abciximab/ReoPro,
Dipyridamole/Persantine
Hold 48 hours
Edoxaban/Savaysa Hold 24 hours
Bivalirudin/Angiomax Hold 2 hours
Aspirin No hold
Clopidogrel/Plavix, Prasugrel/Effient, Aggrenox Hold 7 days
Ticloplidine/Ticlid Hold 14 days
Tirofiban/Aggrastat, Eptifibatide/Integrilin Hold 8 hours
Alteplase/TPA 2 mg dose for catheter no hold; Full dose delay procedure
10 days

PRE PROCEDURE LAB STUDIES
INR <1.5
Platelet count >50,000
PTT <35
Urine pregnancy test

REVIEW OF PRIOR IMAGING
Anatomy
Optimal puncture level
Level and degree of spinal stenosis
Scoliosis or other deformity
Location of the conus
Postsurgical anatomy
Location of hardware
Post-op infection or abscess
Potential complications
Chiari malformation
Myelomeningocele
Low-lying posterior inferior cerebellar artery (PICA)
Tonsillar ectopia
PROCEDURE - INFORMED CONSENT
Explain procedure
Risks and side effects
Pain
Bleeding
Infection
CSF leak
Headache
N/V
Dizziness
Allergic or anaphylactic reaction
Nerve root injury
Seizures
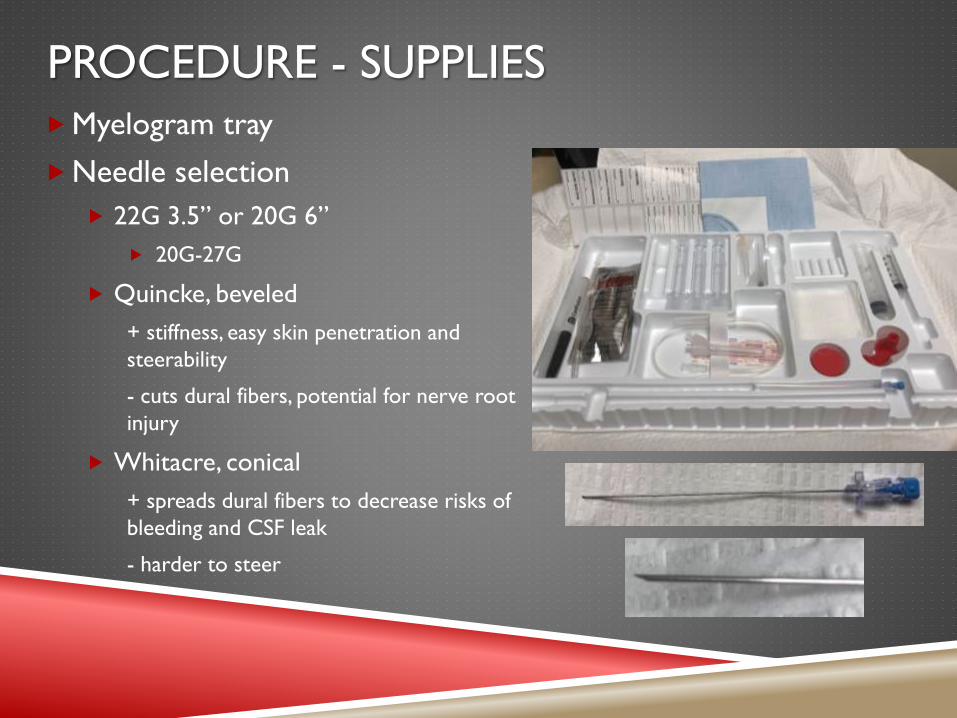
PROCEDURE - SUPPLIES
Myelogram tray
Needle selection
22G 3.5” or 20G 6”
20G-27G
Quincke, beveled
+ stiffness, easy skin penetration and
steerability
- cuts dural fibers, potential for nerve root
injury
Whitacre, conical
+ spreads dural fibers to decrease risks of
bleeding and CSF leak
- harder to steer

PROCEDURE – CONTRAST SELECTION
Non-ionic, iohexal – total volume up to 3g of iodine
17 mL 180
12.75 mL 240
10.2 mL 300
Ionic has potential for neurotoxicity
Lumbar
12-15 mL
Lumbar, Lumbar + Thoracic, Cervical w/CP
10-12 mL
Cervical w/LP, Thoracic + Cervical w/LP, Entire spine, Cisternogram
10 mL

LP PATIENT POSITIONING
Prone Prone, oblique
Less painful, avoiding
paraspinal musculature
Advanced spinal degeneration
or interspinous osteoarthritis
(Baastrup’s)

THORACIC, CERVICAL OR ENTIRE

LP TECHNIQUE
Dural “pop”
Stretches for 5-10 mm
before puncture
Less likely to feel with
smaller gauge needles
CSF flow
Slight, 1-2mm, advancement
after pop
Rotate bevel cranial
Tilt table head up

CONTRAST INJECTION
“Wet-to-wet” connection
Avoid air bubbles
CSF & contrast mixing
Confirms subarachnoid placement
Elevate head of table
Slow injection of 1-2 mL under
continuous fluoro
“wisp of smoke”
Flows freely away from needle
Finish slow injection with
intermittent fluoro looking for
visible nerve roots

CONTRAST INJECTION
Epidural Subdural
Starburst Linear

CERVICAL PUNCTURE
Higher risk of neurologic
complications
Puncture of cord, nerves or vessels
When?
Lumbosacral skin infection, abscess or
mass
Severe spinal stenosis resulting in a block
Lumbar posterior osseous fusion
Contraindications
Tonsillar ectopia
Chiari malformation
Low-lying PICA
Uncooperative patient
Positioning
Supine, prone or lateral
Head and neck stabilized
True lateral imaging
C1-C2 puncture
Posterior 1/3 meets the anterior 2/3
Advance to midline on AP view
Free flow of CSF to ensure subarachnoid
positioning
Intramedullary injection could cause
catastrophic cord injury
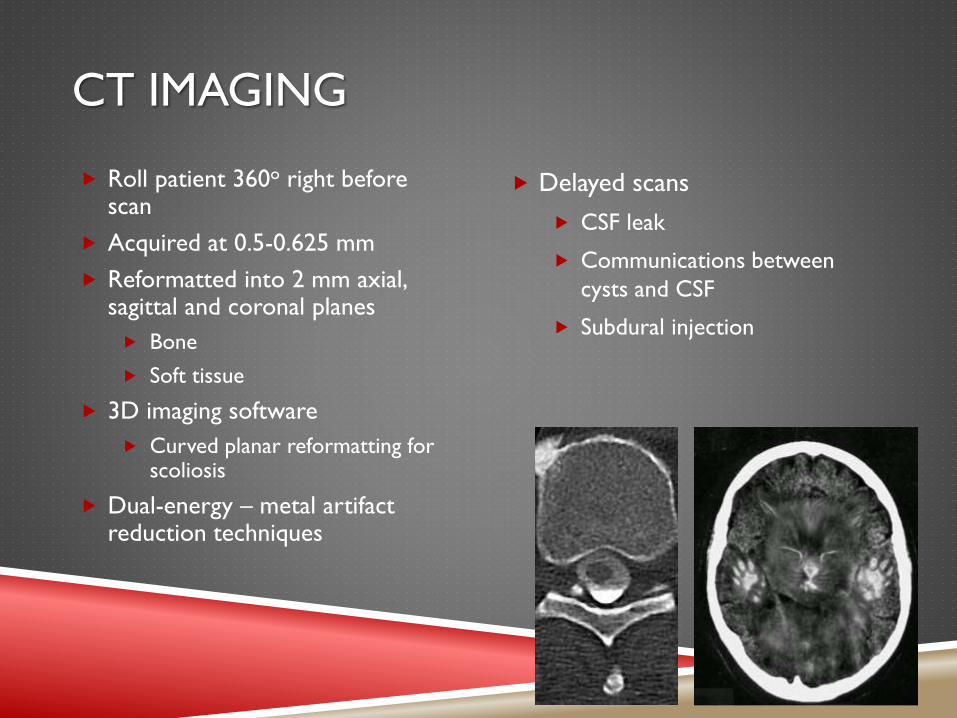
CT IMAGING
Roll patient 360o right before scan
Acquired at 0.5-0.625 mm
Reformatted into 2 mm axial, sagittal and coronal planes
Bone
Soft tissue
3D imaging software
Curved planar reformatting for scoliosis
Dual-energy – metal artifact reduction techniques
Delayed scans
CSF leak
Communications between
cysts and CSF
Subdural injection

POST MYELOGRAM PATIENT CARE
Post procedure care area At home
2 hours of bedrest (2-4 hours)
Head elevated 30-45o
Allowed up to bathroom
Back to normal diet
Encourage fluid intake
Medications
None if doing ok; may take personal
meds
Headache or pain
Tylenol or NSAIDs
Stronger if prescribed
N/V
Zofran
Avoid phenothiazines (Phenergan)
No driving for 24 hours
Lay around for 24 hours
Normal diet with extra fluids
Caffeine
Go to ED if
Fever
Stiff neck
Increased pain or N/V
Swelling or drainage at puncture site
Positional headache after 48 hours
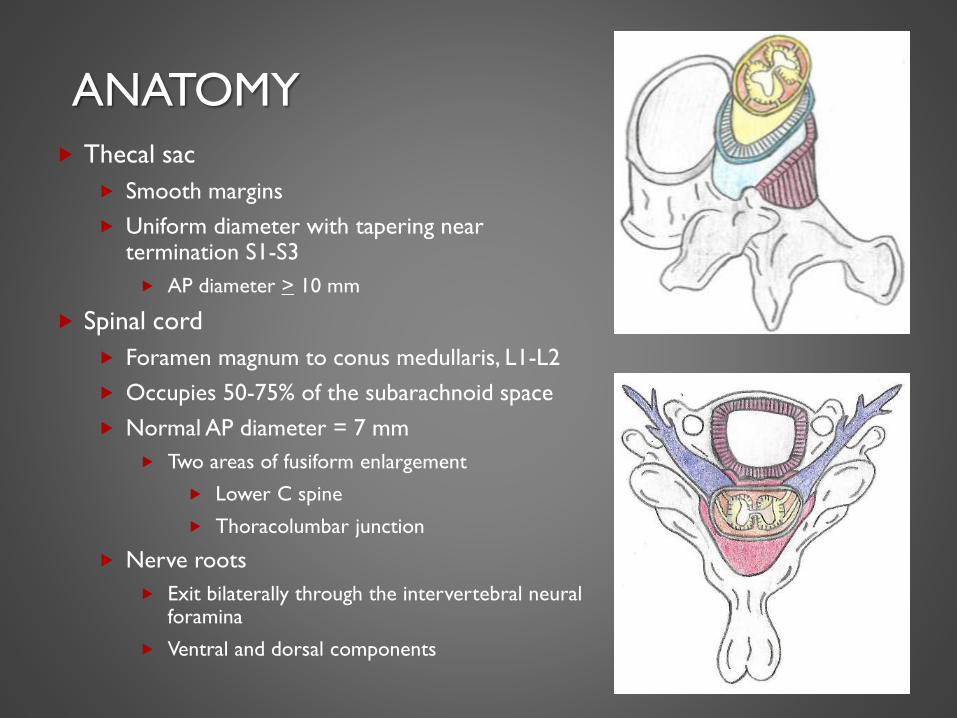
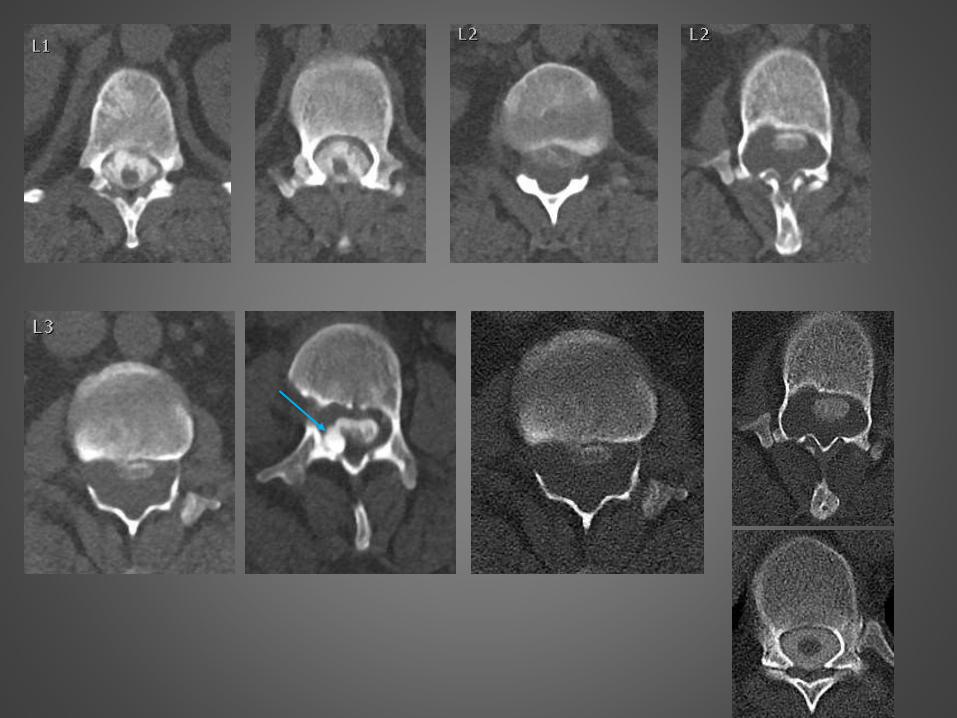
ANATOMY
Thecal sac
Smooth margins
Uniform diameter with tapering near termination S1-S3
AP diameter > 10 mm
Spinal cord
Foramen magnum to conus medullaris, L1-L2
Occupies 50-75% of the subarachnoid space
Normal AP diameter = 7 mm
Two areas of fusiform enlargement
Lower C spine
Thoracolumbar junction
Nerve roots
Exit bilaterally through the intervertebral neural foramina
Ventral and dorsal components
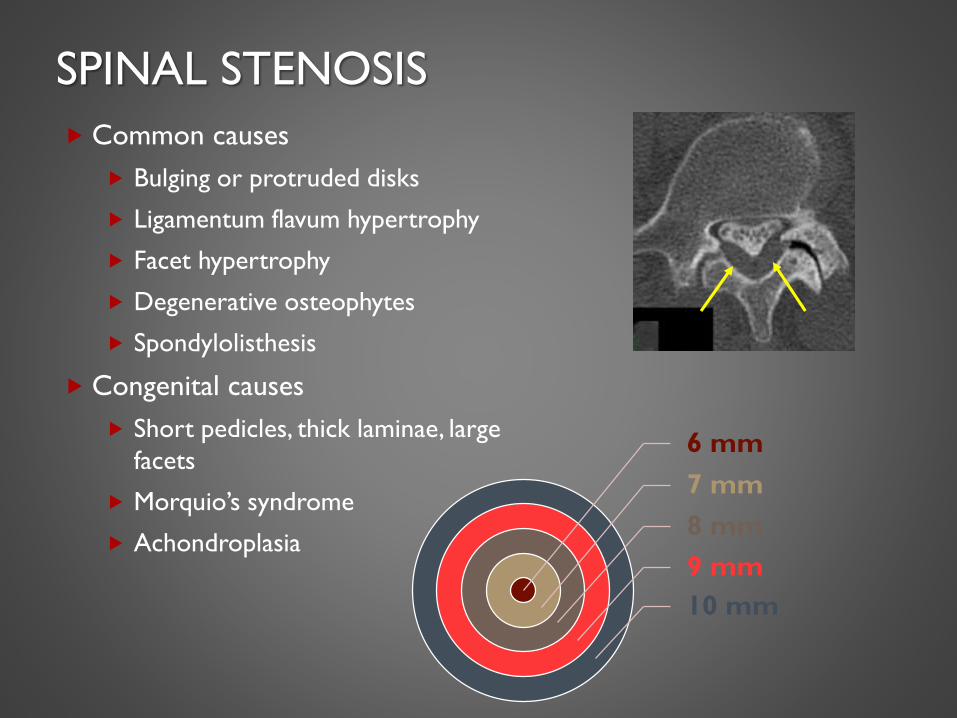
SPINAL STENOSIS
Common causes
Bulging or protruded disks
Ligamentum flavum hypertrophy
Facet hypertrophy
Degenerative osteophytes
Spondylolisthesis
Congenital causes
Short pedicles, thick laminae, large
facets
Morquio’s syndrome
Achondroplasia
6 mm
7 mm
8 mm
9 mm
10 mm

SPINAL CORD COMPRESSION
No CSF around the cord
Narrowed AP diameter <7mm
Deformity of cord
Causes
Infection (TB, pyogenic)
Fractures (malignancy, trauma)
Disk disease (HNP, ligament hypertrophy,
osteophytes, facet hypertrophy)
Primary bone disorders (Paget’s disease)
Benign tumors (cysts, lipoma)
Epidural hematoma

FORAMINAL STENOSIS
Common causes
Osteoarthritis of facet joints
Buckling/thickening of
ligamentum flavum
Spondylolisthesis
Lateral herniated discs
Fracture
Post-op scarring
Extradural masses
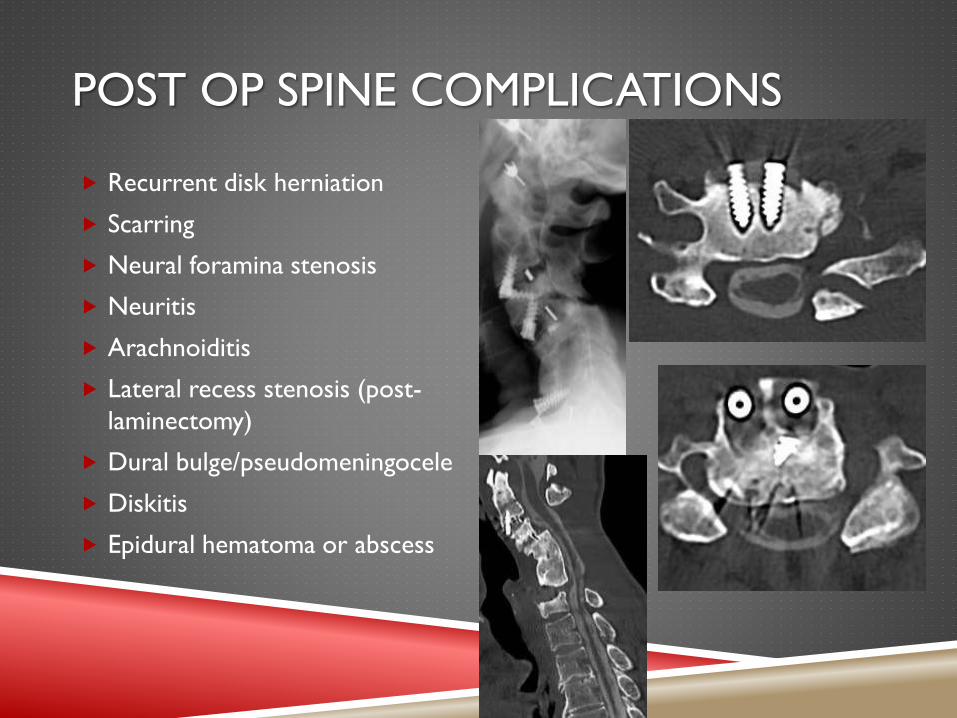
POST OP SPINE COMPLICATIONS
Recurrent disk herniation
Scarring
Neural foramina stenosis
Neuritis
Arachnoiditis
Lateral recess stenosis (post-
laminectomy)
Dural bulge/pseudomeningocele
Diskitis
Epidural hematoma or abscess

INTRAMEDULLARY LESIONS
Tumor
Astrocytoma
Ependymoma
Hemangioblastoma
Metastases
Demyelinating disease/myelitis
Syringohydromyelia (tumor or
Chiari malformation)
AVM
Trauma
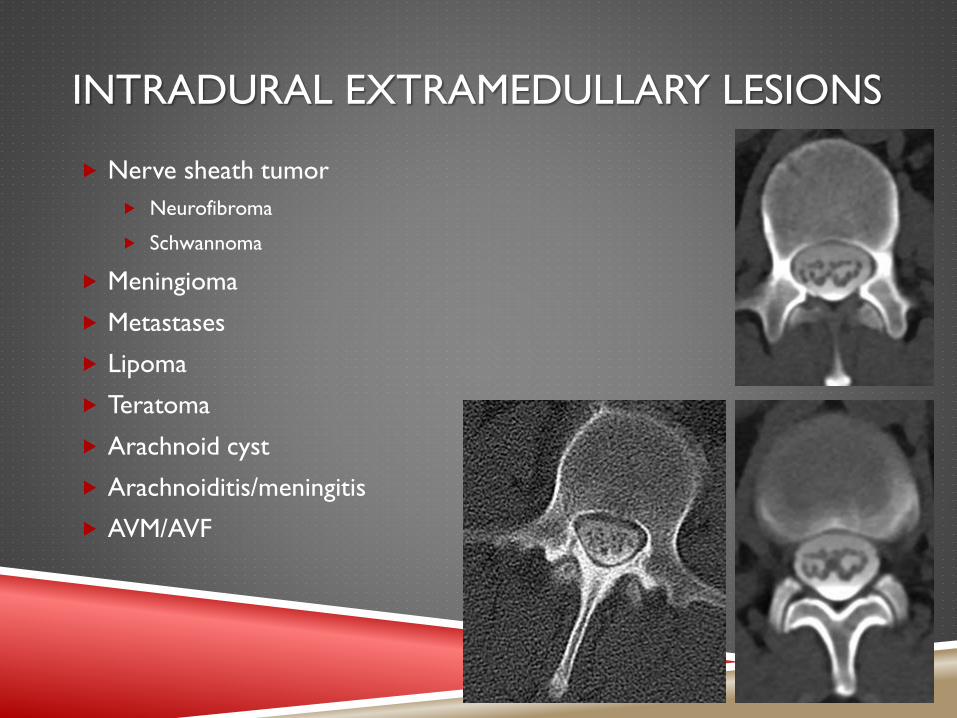
INTRADURAL EXTRAMEDULLARY LESIONS
Nerve sheath tumor
Neurofibroma
Schwannoma
Meningioma
Metastases
Lipoma
Teratoma
Arachnoid cyst
Arachnoiditis/meningitis
AVM/AVF

EXTRADURAL LESIONS
Disk
Metastases
Epidural abscess
Hematoma
Lipomatosis
Synovial cyst
Perineural cyst


1
2
3 4 5
6
7 8





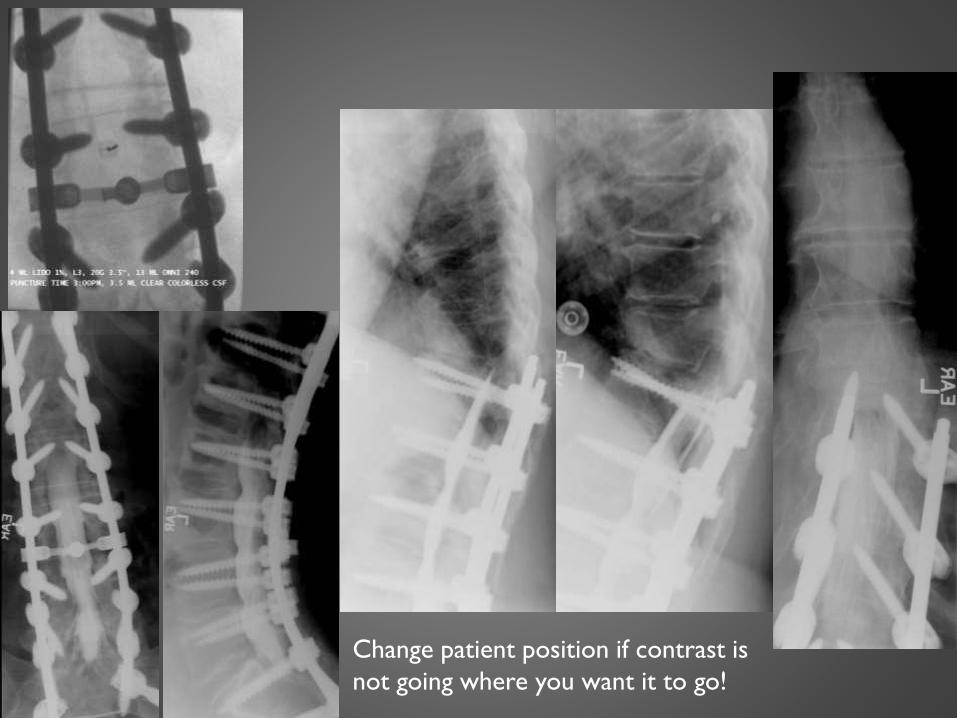
Change patient position if contrast is
not going where you want it to go!







REFERENCES
Boutin, RD, Rupp FW. Myelography.
Harisinghani, MG, Chen JW, et al. Primer of Diagnostic Imaging. Elsevier,
2019.
Harreld JH, McMenamy JM, et al. Myelography: A Primer. Current
Problems in Diagnostic Radiology July/August:149-157, 2011.
Pomerantz, SR. Myelography: modern technique and indications.
Handbook of Clinical Neurology, Vol. 135, p. 449-468. Elsevier, 2016.