Embed Size (px)
Citation preview

Welcome!
Heinen + Löwenstein GmbHArzbacher Straße 80D-56130 Bad EmsTel. +49 (0) 2603 9600-0Fax +49 (0) 2603 960050
www.hul.de

Leoni Ventilators
Leoni mobil Leoni 2
Leoni plus

Mode of Operation
• The Leoni neonatal and pediatric ventilator functions according to the constant flow generator principle. • A constant gas flow of mixed Oxygen/Air is delivered to the patient via a hose system. • The desired concentration of the inhaled gas mixture is produced by a valve bank. • During the inspiration phase, the expiratory valve on the end of the hose system is closed, so that the flow must go towards the patient. • Exhalation is effected by opening the expiratory valve. The lung then deflates due to the pressure decrease.

Specifications
Leoni mobil Leoni 2 Leoni plus
O2 Monitor x x x
Electronic gas blender x x x
VIVE x x x
Integrated battery x x x
LCD Display x x
TFT Colour screen x
Touch screen, removeable x
Volume trigger x x
Curves: Pressure x
Curves: Pressure / Volume / Flow x x
Lopps: F/P, V/P, F/V x x

Ventilation modes
Leoni mobil Leoni 2 Leoni plus
CPAP x x x
IPPV x x x
SIPPV x x
SIMV x x
SIPPV - PSV x x
SIMV - PSV x x
HFOV x
Volume Limit x x
Volume Guarantee x
Manual Ventilatory Drive x x x

Leoni plus Ventilation modes
CPAP
IPPV / IMV
SIPPV
SIMV
PSV SIPPV
PSV SIMV
HFOV

CPAP Ventilation mode
Demand-CPAP
With support frequency

IMV/IPPV Ventilation mode
IMV

IPPV Ventilation mode
IPPV

SIPPV Ventilation mode
Leakage com- pensated volume trigge- ring Trigger sensi- tivity related to VTi (5 – 30 %)

SIMV Ventilation mode
Leakage com- pensated volume
triggering

PSV Ventilation mode
PSV SIPPV
PSV SIMV

HFOV Ventilation mode
HFOV on the membrane prin- ciple with recruit- ment breath function

Setting ranges
IPPV/IMV
SIMV SIPPV CPAP
Breath rateFREQUENCY [BPM]
6 .. 200 2 .. 100 2 .. 100 -
Inspiration timeI-TIME [sec]
0.10 .. 2.00
0.10 .. 2.00
0.10 .. 2.00
-
Expiration timeE-time [sec]
0.20 .. 10.00
0.50 .. 30.00
0.20 .. 30.00
-
Inspiratory FlowINSP FLOW [l/min]
1 .. 32 1 .. 32 1 .. 32 -
Expiratory Flow E Flow [l/min]
2 .. 10 2 .. 10 2 .. 10 -

Setting ranges
IPPV/IMV
SIMV SIPPV CPAP
Inspiratory PressureP INSP [cmH2O]
6 .. 60 6 .. 60 6 .. 60 -
Backup PressureP-BACK [cmH2O]
- - - 6 .. 60
Positive End Expiratory PressurePEEP [cmH2O]
0 .. 20 0 .. 20 0 .. 20 -
CPAP [cmH2O]- - - 1 .. 20

Setting ranges
IPPV/IMV
SIMV SIPPV CPAP
O2 Concentration
OXYGEN [%]21 .. 100 21 .. 100 21 .. 100 21 .. 100
O2 Concentration Oxygen
flushO2-Flush [%]
23 .. 100 23 .. 100 23 .. 100 23 .. 100
Volume triggerTRIGGER [% VTi]
- 10 .. 30 10 .. 30 -

Setting ranges
HFOV
Mean PressurePmean [cmH2O]
10 .. 30
High FrequencyHFFreq [Hz]
5 .. 20
High Frequency AmplitudeHFAmpl [cmH2O]
5 .. 80
Recruitment FrequencyFreqRec [1/min] 0 .. 10
Recruitment Inspiration TimeTI Rec [s]
0.1 .. 3

Casing front
1) Control Panel
2) Touch Screen
3) Rotary Pulse Encoder
4) Inspiratory Connection
5) Expiratory Connection
6) Pressure Gauge
Connection
7) HFOV- Connection
2
1 3
5 7 6 4

Casing rear
1) Earth Connection
2) Serial Interface
3) Ethernet Connection
4) Flow Sensor Connection
5) Oxygen Connection
6) O2Sensor Access
7) Compressed Air Connection
8) Mains Connection
9) Nurse Call
3 2
1
9
56
7
8
4

Accessories
1) Proximal Pressure Line
2) Expiration Hose
3) Inspiration Hose
4) Y-Piece
5) Flow Sensor
6) Test Lung
7) Flow Sensor Cable
8) HFOV Hose with Filter
8

Control panel
Mode / Home
Loops
Curves
Alarm Limits
Power Failure LED
Battery Operation LED
Alarm LED
Alarm Mute Button
StandBy
Manual VentilatoryDrive
Rotary Encoder
ON/OFF
Start Ventilation
Numerical ValuesSwitch-Over

Start Screen
1) Flow Sensor
2) Flow Sensor Calibration
3) Oxygen Sensor Calibration
4) Main Menu Bar
5) Calibration Button

Main Sreen
1) Alarm Bar
2) Curves
3) Softkeys
4) Numerical Values

Curve Display
1) Flow Curve
2) Pressure Curve
3) Volume Curve
Curves freelyscalable
3 Curves at the same time

Loop Screen
1) Flow over Pressure
2) Flow over Volume
3) Volume over Pressure
Full-screen presentation possible
Loops freely scalable
Up to 3 loops at the same time

Alarm limits
1) Manual Adjustment
2) Autoset Adjustment
3) Alarm Logbook Function

Simultaneous Presentation
Simultaneous Presentation of:
Loops Curve Screen Alarm Limits Monitoring

HFO Leoni plus
High-frequency ventilation (HFV) as a ventilatory therapy hasreached increasing clinical application over the past ten years. Theterm comprises several methods. High-frequency jet ventilationmust be differentiated from high-frequency oscillatory ventilation(HFOV or HFO). In this booklet I concentrate on high-frequencyoscillatory ventilation. Therefore, the difference in meaning notwithstanding,I use both acronyms, HFV and HFO, interchangeably.

Indications for HFV
Since the early eighties results on oscillatory ventilation have beenpublished in numerous case reports and studies. Yet there areonly few controlled studies based on large numbers of patients.
In newborns HFV has first beenemployed as a rescue treatment. The goal of this type of ventilationis to improve gas exchange and at the same time reduce pulmonarybarotrauma.
Oscillatory ventilation can be tried when conventional ventilationfails, or when barotrauma has already occurred or is imminent. In the first place this applies to pulmonary diseases with reducedcompliance. The efficacy of HFV for these indications has beenproven in the majority of clinical studies. In severe lung failure,HFV was a feasible alternative to ECMO
When to switch from conventional ventilation to HFV must certainlybe decided by the clinician in charge, according to their experience.Some centres meanwhile apply HFV as a primary treatmentfor RDS in the scope of studies. Likewise, in cases of congenital hernia and during surgical correction, HFV has been successfully used as a primary treatment

Indications; HFV+IMV
Also in different kinds of surgery, especially in the region of the larynx and the trachea, HFV has proven its worth. Moreover, in primary pulmonary hypertension of the newborn HFV can improve oxygenation and Ventilation.
Always observing the contraindications in our NICU we follow this proven procedure: If conventionalventilation* fails, we will switch over to HFV. We will assumefailure of conventional ventilation, if maintaining adequate bloodgas tensions (pO2 > 50mmHg, SaO2 > 90%; pCO2 < 55 to65 mmHg) requires peak inspiratory pressures (PIP) in excess ofcertain limits. Those depend on gestational age and bodyweight:In small prematures we consider using HFV at PIP higher than22 mbar. With PIP going beyond 25 mbar we regard HFV evenas a necessity.
In more mature infants the pressure limits are somewhat higher

Combining HFV and IMV, and sustained inflation
Oscillatory ventilation on its own can be used in the CPAP mode,or with superimposed IMV strokes, usually at a rate of 3 to 5strokes per minute.
The benefit of the IMVbreaths is probably due to the opening of uninflated lung units toachieve further ‘volume recruitment’.Sometimes very long inspiratory times (15 to 30 s) are suggestedfor these sustained inflations (SI). By applying them about every20 minutes compliance and oxygenation have been improved andatelectases prevented.

Combining HFV and IMV, and sustained inflation
Especially after volume loss by deflation during suctioningthe lung soon can be reopened with a sustained inflation. However,whether these inflation manoeuvres should be employedroutinely is subject of controversial discussions.
In most of the clinical studies no sustained inflations were applied. In animal trials no increased incidence of barotrauma was found.Prevention of atelectases, which might occur under HFV withinsufficient MAP, is the primary benefit of combining HFV and IMV.
HFV superimposed to a normal IMV can markedly improve CO2 washout (‘flushing the deadspace’ by HFV) at lower peak pressures

Indications; HFV+IMV
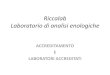
Effect of a sigh manoeuvres through sustained inflation (SI):prior to the SI the intrapulmonary volume equals V1 at the MAP level (point a);
the SI manoeuvres temporarily increases pressure and lung volume according to the pressure-volume curve; when the pressure has returned to the previous MAP level, pulmonary volume remains on a higher level, V2(point b),
because the decrease in pressure occurred on the expiratorylimb of the PV loop.PressureVolume

Standard Accessories
Flow Sensor / Y-Piece / Connecting cable
Expiration valve / Expiration membrane
Oxygen cell
Hose system, heated and non-heated
HFOV Hose

Total System

Thank you very much for your open interest
Heinen + Löwenstein GmbHArzbacher Straße 80D-56130 Bad EmsTel. +49 (0) 2603 9600-0Fax +49 (0) 2603 960050
www.hul.de