Embed Size (px)
Citation preview

IMAGES IN CARDIOTHORACIC SURGERY
Left Ventricular Outflow Tract Obstruction Due toMitral Valve AnomalyRaffaele Calabro, MD, Giuseppe Santoro, MD, Carlo Pisacane, MD,Maria Giovanna Russo, MD, Giuseppe Pacileo, MD, Giuseppe Caianiello, MD, andYves LeCompte, MDPediatric Cardiology and Cardiac Surgery, A.O. “Monaldi”, II University of Naples, Naples, Italy, and Unite Medico-Chirurgicalede Cardiologie Pediatrique, Institut Cardiovasculaire Paris Sud, Paris, France
A14-year-old patient was referred to our center due todyspnea and syncope from moderate effort. At
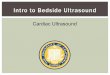
clinical examination a systodiastolic murmur at the mid-sternal level was recorded. A chest roentgenogramshowed mild cardiac enlargement and normal pulmo-nary markings. An electrocardiogram showed left ven-tricular (LV) hypertrophy. At echocardiography a severeLV outflow tract obstruction (Doppler peak pressuregradient of 100 mm Hg), associated with both aortic andmitral valve regurgitation, was imaged. Left ventricularoutflow tract obstruction was due to a “windsock-like”
accessory mitral valve tissue that expanded during LVejection period (Fig 1). At operation, this anomalous tissue,rising from the top of the posteromedial papillary muscleand extending just beneath the aortic valve (Fig 2), wascarefully excised, thereby relieving the LV obstruction.
This work was supported by the Programma Operativo delPiano CCCN-5 B006 of the Ministero dell’Universita e RicercaScientifica (MURST) and the European Community (711/1998).
Address reprint requests to Dr Santoro, Ospedale V. Monaldi, Facolta diMedicina e Chirurgia, Servizio di Cardiologia Pediatrica, Via Vito Lembo,14, 84131 Salerno, Italy; e-mail: [email protected].
Fig 1. Echocardiographic long axis view of the left ventricle (LV)showing the accessory mitral valve tissue arising from the top of theposteromedial papillary muscle (arrow) and crossing the LV outflowtract to attach just beneath the aortic valve. (Ao � aorta; LA � leftatrium.)
Fig 2. (A, B) Surgical view of the left ventricular outflow tractthrough the aortic cusps (asterisks) showing the accessory mitralvalve tissue (cross) arising from the top of the posteromedial papil-lary muscle (arrows). (C) Surgical resection of the muscular stalk(arrow) of the accessory mitral valve tissue (cross).
A videoclip of this procedure can be viewed on theInternet at http://www.sts.org/section/atsvideo.
© 2001 by The Society of Thoracic Surgeons Ann Thorac Surg 2001;72:1762 • 0003-4975/01/$20.00Published by Elsevier Science Inc PII S0003-4975(00)01479-X