Embed Size (px)
Citation preview

structive cardiomyopathy. Circulation 1978;58:402-408. 15. Shapiro LM, Zeznlka A. Hypertrophic cardiomyopathy: a common disease with a good prognosis. Five-year experience of a district genera1 hospital. Br Heart J 1983;50:530-533. 16. Frank S, Braunwald E. Idiopathic hypertrophic subaortic stenosis: clinical analysis of 126 patients with emphasis on the natural history. Circulation 1968;37:759-788. 17. Lazzeroni R, Domenicucci S, Finardi A, Dodi C, Francescon P, Botti C. Severity of arrhythmias and extent of hypertrophy in hypertrophic cardiomyopa-
thy. Am Heart J 1989;118:734-738. 18. Goodwin JF. The frontiers of cardiomyopathies. Br Heart J 1982;48:1-18. 19. Maron BJ, Roberts WC, Eduards JE, McAllister HA Jr, Foley DD, Epstein SE. Sudden death in patients with hypertrophic cardiomyopathy: characterization of 26 patients without functional limitation. Am J Cardiol 1978;41:803-810. 20. Fananapazir L, Tracy CM, Leon MB, Winkler JB, Cannon RC III, Bonow RO, Maron BJ, Epstein SE. Electrophysiologic abnormalities in patients with hypertrophic cardiomyopathy: a consecutive analysis in 155 patients. Circulation 1989;80:1259-1268.
Left Ventricular Function in Patients >20 Years of Age with Ebstein’s Anomaly of the Tricuspid Valve Anita Saxena, DM, Lance V. Fong, FRACP, Maria Tristam, PhD, Duncan M. Ackery, FRCR, and Barry R. Keeton, FRCP
T here have been few reports of left ventricular (LV) abnormalities in patients with Ebstein’s anomaly of
the tricuspid valve.‘>* We studied LV function by echo- cardiography and radionuclide imaging in 8 patients >20 years of age with this abnormality.
Eight patients (4 men and 4 women) aged 21 to 54 years with Ebstein’s anomaly of the tricuspid valve as the isolated lesion proven by echocardiography were re- viewed. Each patient underwent a clinical cardiac assess- ment, electrocardiography and a chest x-ray.
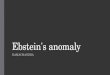
Two-dimensional echocardiography, Doppler and color flow mapping were performed. The size of the atrialized right ventricle and the degree of the tricuspid valve displacement (the ratio of mitral valve-to-apex versus tricuspid valve-to-apex distance) was estimated from the apical I-chamber view (Figure 1). The motion of the ventricular septum and LV posterior wall were
From the Wessex Cardiothoracic Centre, Southampton General Hospi- tal, Southampton, United Kingdom SO9 4XY. Manuscript received April 30, 1990; revised manuscript received and accepted September 10, 1990.
FtGURE 1. Apical 4cham- bered view (/eff) and illustra- tion (fight) showing echocar- diographic mea-. ARV = atrialized right ventri- ck;LA=leftatrium;LV= left ventrick; NIV = mitral vaive; RA = right atrium; RV = right ventricle; l-v = trl- cuspid valve.
analyzed. LV dimensions were measured, although shorteningfractions could not be meaningfully calculat- ed because ofparadoxical ventricular septal motion. The degree of tricuspid regurgitation was quantified on Doppler and color flow mapping and the right ventricu- lar systolic pressure estimated from the regurgitant jet velocity.
A multigated radionuclide cardiac blood pool study of the left ventricle was carried out using technetium- 99m in vivo labeled autologous red blood cells. Images were acquired with a gamma camera in the left anterior oblique view with craniocaudal tilt to separate the 2 ventricles. Gating of the cardiac images was obtained at the R wave and a resting LVejection fraction was calcu- lated.
Regional wall motion abnormalities were detected by tine loop images together with phase and amplitude studies. In the amplitude image, the amplitude of the time activity curve is assigned a value that is plotted on a color scale (a red-colored area indicates greatest ampli- tude and a blue area indicates least movement). Poorly contractile regions of the left ventricle have disturbance
Echocardiographlc Parameters in Ebstein’s Abnor m lality
MV-APEX TV displacement ratio TV-APEX
THE AMERICAN JOURNAL OF CARDIOLOGY JANUARY 15, 1991 217

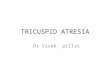
FIGURE 2. Radionucfide lefl ventricubgraphy from 3 study patients showing normal function, regional dyskinesia and global hy-
in the normal color distribution. The phase image is color-coded according to the timing of movement rela- tive to the R wave of the electrocardiogram. The atria are therefore distinguishable from the ventricles and dyskinetic regions can be ident.ij?ed.
On echocardiography the size of the atrialized right ventricle varied from 15 to 44 mm. The tricuspid valve displacement, estimated as a ratio, ranged from 1.5 to 2.8. Moderate to severe tricuspid regurgitation waspres- ent in dpatients and mild in 2. The regurgitant jet veloci- ty was X2.5 m/s in each patient. The ventricular septal motion was markedly paradoxical in all patients at the level of the atrialized right ventricle and was flat or greatly reduced below the level of displaced tricuspid valve attachment. LVposterior wall motion was signif?- cantly reduced in 2 patients, although the end-diastolic dimensions were within the normal range for body sur- face area in all patients.3
The resting LVejection fraction by radionuclide scin- tigraphy varied from 28 to 71% (median 46%) and was subnormal (<50?6) in 5 patients. A low ejection fraction could not be correlated with either the severity of tricus- pid valve displacement or tricuspid regurgitation by echocardiography. Amplitude andphase image analysis detected global hypokinesia in 2 patients and regional
dyskinesia of the upper septal and lateral wall in 5 (Figure 2). Two of these 5 patients had normal LV ejec- tion fractions. Thus, 7 of 8 patients in this study had either a subnormal ejection fraction or regional wall motion abnormalities.
One patient in this series died suddenly. He had had a low LV ejection fraction (28%) and global hypokinesia on radionuclide imaging. An autopsy revealed extensive myocardialfibrosis of the left ventricle with wide sepa- ration of remaining myocardialfibers in addition to the typical features of Ebstein’s anomaly of the tricuspid valve. The coronary arteries were normal.
It is now well established that volume overloading of the right ventricle may affect LV function.4,5 This has also been reported in Ebstein’s anomaly1,2 but it has been difficult to recognize on a routine clinical basis. Echocar- diography has not proved as helpful for assessing LV function in patients with volume overloading of the right ventricle.6 In Ebstein’s anomaly, the abnormal ventricu- lar septal motion makes assessment of LV performance difficult. In this study there was no echocardiographic parameter that permitted correlation with a subnormal LV ejection fraction on radionuclide imaging.
Radionuclide imaging is a valuable technique for as- sessing LV function in this group of patients despite wall
218 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 67

ST-Segment Depression After Cardiac Transplantation and Its Usefulness as an Indicator of Acute Rejection Bernd Heublein, MD, Jot-g Winter, Josef Kemnitz, MD, PhD, Thorsten Wahlers, MD,
motion abnormalities. Over 60% of our patients have suboptimal LV ejection fractions. A similar study of 7 adult patients also found low ejection fractions in 5.2
Regional wall motion abnormalities occur often in these patients. They are observed even in patients with normal resting LV ejection fractions. Anomalies of LV contour and contraction pattern have also been described previously in 12 of 13 patients with Ebstein’s anomaly studied by angiography.’ In our series, because 5 of 7 patients with regional wall motion abnormalities were <40 years, LV dysfunction is unlikely to be related to coronary artery disease. These findings indicate an im- portant LV problem, as was recognized in 1 of our pa- tients at autopsy.
We conclude that LV function may be significantly altered in older patients with Ebstein’s anomaly of the tricuspid valve and can be difficult to recognize clinically
or on echocardiography. Radionuclide imaging of the left ventricle is the investigation of choice.
1. Monibi AA, Neches WH, Lenox CC, Park SC, Mathews RA, Zuberbuhler JR. Left ventricular anomalies associated with Ebstein’s malformation of the tricuspid valve. Circulation 1978;57:303-306. 2. Benson LN, Child JS, Schwaiger M, Perloff JK, Schelbert HR. Left ventricu- lar geometry and function in adults with Ebstein’s anomaly of the tricuspid valve. Circulation 1987;75:353-359. 3. Feigenbaum H. Echocardiography. In: Braunwald E, ed. Heart Disease-a Textbook of Cardiovascular Medicine. Philadelphia: WB Saunders, 1980:96- 146. 4. Bemis CE, Setur JR, Borkenhagen D, Sonnenblick EH, Urschel CW. Influ- ence of right ventricular filling pressure on left ventricular pressure and dimension. Circ Res 1974;34:498-504. 5. Mathew R, Thilenius OG, Arcilla RA. Comparative response of right and left ventricles to volume overload. Am J Cardiol 1976;38:209-217. 6. Bonow RO, Borer JS, Rosing DR, Bacharach SL, Green MV, Kent KM. Left ventricular functional reserve in adult patients with atria1 septal defect-pre- and postoperative studies. Circulation 1981;63:1315-1322.
and Axe1 Haverich, MD
1 he so-called Hannover classification of rejection in cardiac allografts’ describes degrees of acute rejec-
tion with different frequencies of conversion into the forms of rejection that require therapy, where AO, Al, A2, A3, A4, A5a and A5b denote no rejection, mild rejection, mild rejection with premyocytolysis, moderate rejection, severe rejection, early-resolving phase and late- resolving phase, respectively. During episodes of acute rejection, the small coronary vessels frequently show an inflammatory response. The presence of the more severe degrees of concomitant vasculopathy implies an aug- mented risk of conversion into the form of acute rejection that requires therapy in the resolving and the late-resolv- ing phases.2 Various and different vasoactive mecha- nisms are obviously involved in the process of rejection, especially during the acute phase. Mediators of the eico- sanoid pathway3 and of cY-adrenergic stimulation4 might be responsible for episodes of reduction in blood flow. ST- segment depression after transplantation should there- fore be expected, especially during active infiltrating pro- cesses in the myocardium. Based on these hypotheses, we studied heart transplant recipients using 24-hour ambu- latory electrocardiographic recordings to determine the frequency and time of ST-segment depression after heart transplantation in relation to postoperative intervals, and to reveal a possible correlation with active rejection-relat- ed processes (acute rejection at various histologic stages).
From the Divisions of Cardiology and Cardiothoracic Surgery, Institute of Pathology, Hannover Medical School, Konstanty-Gutschow-Strasse 8, D-3000 Hannover 61, Federal Republic of Germany. Manuscript received July 13, 1990; revised manuscript received and accepted Sep- tember 6, 1990.
Seventy-seven patients (68 men, 9 women: mean age f standard deviation 45 f 19 years) were examined 7 I X I I,1 98 days after orthotopic heart transplantation. Patients were not treated with digitalis and all had a constant supraventricular rhythm. Duration of the QRS complex never exceeded 0.11 second. A total of 144 ambulatory 24-hour electrocardiographic record- ings were analyzed using a 2-channel recording sys- tem (Spacelabs Arrhythmia Master I 90201, frequency spectrum 0.05 to 100 cycles). Endomyocardial biopsy specimens obtainedfrom the right ventricle the same day served as a histologic reference.’ Localization of the bi- polar electrodes corresponded roughly with leads V, or V5; the 2 negative electrodes were positioned at both sides of the sternum at the level of the manubrium. Visual monitor-supported control of electrocardiograms were used to identify the most suitable lead for ST- segment monitoring before fixation of the electrodes. Signal analysis was performed after the classification of the electrocardiogram had been corrected by the observ- er. The calibrated STsegment, measured 60 ms after the Jpoint, was printed as a mean value at 10 minutes or l- minute intervals in parallel to the actual heart rate. An additional control was achieved by printing the electro- cardiogram before, during and after the ST-segment depression (Figure 1). ST-segment depression was de- fined as a downward shift or slope of the ST segment from the baseline (21 mV) lastingfor >5 minutes. To examine the influence of ongoing drug therapy (angio- ten&?-converting enzyme inhibitors, calcium antago- nists) and of extracellular electrolyte concentrations caused by immunosuppression and concomitant diuretic
THE AMERICAN JOURNAL OF CARDIOLOGY JANUARY 15, 1991 219