-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
1/17
Lecture 6: Spinal Cord; Cortex; Reflexes
Spinal Cord and Pathways
Objectives
1.
Be able to identify the components of the spinal cord: dorsal,
ventral and lateral grey horns,
anterior, posterior and lateral white columns, grey commissure
and central canal. Describe theirfunctional significance and
differences.
2.
Explain the functional significance of the dorsal root
ganglia.
3.
Explain the roles of white matter and gray matter in processing
and relaying sensory information
and motor commands.
4.
Identify and differentiate between the three somatic sensory
pathways: Dorsal ColumnMedial
Meniscus Pathway, Anterolateral Spinothalamic Tracts,
Spinocerebellar tracts.
5.
Identify somatic motor pathway and rationalize the types of
function losses from spinal cord
injuries.
1. Be able to identify the components of the spinal cord:
dorsal, ventral and lateral grey horns,
anterior, posterior and lateral white columns, grey commissure
and central canal. Describe their
functional significance and differences.
Central canalis a canal filled with CSF. The gray (grey)
commissureis a strip of gray matter that
connects left and right halves of the spinal cord and surrounds
the central canal.
Posterior (dorsal) gray hornscarry sensory information.
Anterior (ventral) gray hornscontain bodies of somatic motor
neurons.
Lateral gray hornscontain bodies of autonomic, presynaptic
neurons.
Anterior (ventral) white column (funiculus) isthe white
substance of the spinal cord lying on either
side between the anterior median fissureand the ventral root.
Anterior white column contains both
ascending and descending tracts.
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
2/17
Lateral white column (funiculus) is the white substance of the
spinal cord lying between the dorsal and
ventral horns. It also contains both ascending (e.g.
spinocerebellar tracts, lateral spinothalamic tract)
and descending tracts (e.g. lateral corticospinal).
Dorsal (posterior) white column (funiculus) is the white matter
of the spinal cord lying between the
posterior median sulcus and the dorsal root. It contains only
ascending (sensory) tracts: fasciculus
gracilis and fasciculus cuneatus.
Fasciculus gracilis
(slender one) brings
sensory signals from
the legs and lower part
of the body.
Fasciculus cuneatus
(wedge-shaped) brings
sensory information
from the arms and
upper body.
The fasciculus gracilis axons synapse in the gracile nucleus,
and the cuneates axons synapse in the
cuneate nucleus.
2. Identify the parts of the spinal cord and location of
different types of neurons in spinal cord,
spinal nerves and adjacent ganglia
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
3/17
Identify: the parts of spinal cord: anterior (motor) and
posterior (sensory) horns, ventral and dorsal
roots; the ganglia: sympathetic chain ganglionvs. dorsal root
ganglion; and the types of neurons (e.g.
sensory, motor, unipolar, multipolar) in the picture above.
The bodies of the sensory neurons are residing in the dorsal
root ganglia (please refer to the picture.)
There is one such ganglion for every spinal nerve. The sensory
neurons, which are located in these
ganglia, are unipolar. The paravertebral sympathetic chain
ganglia contain bodies of postganglionic
sympathetic neurons.
3. Explain the roles of white matter and gray matter in
processing and relaying sensory information
and motor commands.
White matter
(myelinated axons)
tracts propagate
sensory impulses
from receptors to
the brain and motor
impulses from thebrain to the
effectors.Gray
matter(bodies of
neural cells) receives
and integrates
incoming and
outgoing
information.
4. Identify and differentiate between the three somatic sensory
pathways: Dorsal Column Medial
Lemniscus Pathway, Anterolateral Spinothalamic Tracts,
Spinocerebellar tracts.
The somatosensory systemis a division allowing the perception of
different sensations from the body
(e.g. light touch, pain, pressure, temperature and
proprioception). Different sensations are referred to
different areas of the brain via three different somatosensory
(afferent) pathways:
1. Dorsal ColumnMedial Lemniscus Pathway carries the signals of
discriminative touch, which is a
perception of touch, pressure, vibration and texture. It allows
for the feeling of shape and texture of the
object.
2. Anterolateral Spinothalamic Tracts carry signals of pain,
temperature, tickling and itching.3. Spinocerebellar tracts carry
signals fromjoints, tendons and muscles (proprioception). It
allows
feeling the position of the body parts (stretch, tension,
movement) without looking at them. These
signals are referred to the cerebellum which receives
second-to-second feedback about the movement
of the body.
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
4/17
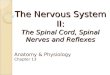
Dorsal ColumnMedian
Lemniscus Pathwayis presented
in the picture to the right. The
key to the picture is summarized
in the table below. Dorsal
columnMedial Lemniscus
pathway carries discriminative
touch signals from all the parts
of the body except face. These
types of signals from the face are
carried by the cranial nerves V
and VII.
The signals from the upper part
of the body including hand and
arm are going through the
fasciculus cuneatus of dorsal
column; the signals from lower
part of the body are comingthrough f. gracile. In medulla
axons synapse in corresponding
nuclei and the signals proceed
via medial lemniscus pathway,
which decussates in medulla.
Dorsal ColumnMedian Lemniscus Pathway consists of three
neurons:1st order neuron (red in the
image)2
ndorder neuron (blue) 3
rdorder neuron
(violet)
Sensation comes via sensory
axon of unipolar neuron.
Receives signals from 1st Receives signals
from 2nd
Body is located in Dorsal Root
Ganglion.
Body of the neuron is located in
medulla: Nucleus gracile or cuneate
nuclus.
Body is located in
thalamus (clearing
house of sensory
info)
Primary afferent axonssynapse in medulla (gracile
fasciculus in gracile nucleus,
cuneate fasciculus in cuneate
nucleus)
Axon (secondary afferent) decussatecrosses to the opposite side
of
medulla and then goes to synapse in
thalamus.
Axon synapse incerebral cortex
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
5/17
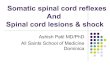
Anteriolateral Spinothalamic pathway carries signals of pain and
temperature.
Anterolateral Spinothalamic Tracts ( Pain and Temperature)
consists of three neurons:
1st order neuron2
nd
order neuron 3rd
order neuron
Collect signals from receptorsof pain and temperature.
Receives signals from 1st
Receives signals from2nd
Body in dorsal root ganglia Body is in dorsal horns. Body is
located in
thalamus (clearing
house of sensory info)
Synapse in dorsal horn of the
spinal cord.
Axon (secondary afferent)
crosses to the opposite side of
spinal cord to synapse in
thalamus.
Axon synapse in
cerebral cortex
Compare discriminative touch pathway to pain and temperature
pathway in the image above.
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
6/17
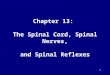
Spinocerebellar tracts carry signals of proprioception (position
of parts).
Compare discriminative touch pathway to pain and proprioception
pathway in the image above.
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
7/17
Spinocerebellar Tracts (proprioception) consists of two neurons
only:
1st order neuron 2nd
order neuron
Collect signals from muscles and tendons in
limbs and trunk
Receives signals from 1st
Body in dorsal root ganglia Body is in dorsal horns.
Synapse in dorsal horn of the spinal cord. Axon synapses in the
cerebellum on the
same side .
IPSILATERAL
Please identify locations of the three sensory pathways (blue)
in the image of spinal cord below.
In the summary:
Dorsal column - medial meniscus pathway decussates high in the
medulla oblongata. Thalamo-cortical
afferents go through internal capsule to primary somatosensory
cortex, postcentral gyrus.
Anterolateral Spinothalamic Tracts (Pain and Temperature)
decussates low in the spinal cord.
Spinocerebellar Tracts do not decussate at all.
5. Identify somatic motor pathway and rationalize the types of
function losses from spinal cord
injuries.
Somatic motor pathways (red in the image above) carry signals
from the CNS to skeletal muscles.
Initiation of movement is controlled by the prefrontal cortex,
supplementary motor area, premotor
cortex and basal ganglia in the brain. Then the signal (the
command to do) is communicated to the
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
8/17
motor cortex. Then the motor cortex sends the actual nervous
impulses to the muscles required to
perform the action, as well as a copy to the cerebellum.
The axons of Upper Motor Neuronscarrying this information travel
down through the brainstem and
spinal cord (primarily via the cortico-spinal tract, in the
white matter) until they reach the spinal
segment corresponding to the muscle(s) they innervate. Most of
these axons decussate high in the
brain before they reach the spinal cord.
The axons of upper motor neurons synapse with the cell bodies of
their corresponding Lower Motor
Neurons(LMN) in the anterior or lateral grey horns of the spinal
cord. The axons of LMN travel out
through the ventral roots to their destination, where they
stimulate the muscle fibers to contract.
http://medchrome.com/wp-content/uploads/2010/07/UMN-and-LMN.jpg
http://medchrome.com/wp-content/uploads/2010/07/UMN-and-LMN.jpghttp://medchrome.com/wp-content/uploads/2010/07/UMN-and-LMN.jpghttp://medchrome.com/wp-content/uploads/2010/07/UMN-and-LMN.jpg
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
9/17
Upper motor neurons (UMN)have their bodies in the motor cortex.
Their axons synapse in the medulla
oblongata or in the spinal cord. UMN are completely inside the
CNS. Damage to the UMN leads to
spasticity, increased muscular tone and exaggerated
reflexes.
Lower motor neurons (LMN)receive the signals from UMNs and carry
these signals to the skeletal
muscles via peripheral nerves (cranial or spinal).
About 90% of the axons of UMNs decussate to the contralateral
side in the medulla oblongata; the
remaining 10% eventually cross over at the spinal cord level
when they synapse with an interneuron or
LMN.
It is clinically important to distinguish between upper and
lower motor neuron weakness. The signs of
UMN damage versus LMN damage are summarized in the table on the
following page.
Lower motor neuron weakness (LMN) Upper motor neuron weakness
(UMN)
Flaccid Spasticity
Decreased tone Increased tone
Decreased muscle stretch reflexes Increased muscle stretch
reflexes
Profound muscle atrophy Minimal muscle atrophy
Fasciculations present Fasciculations absent
May have sensory disturbances May have associated sensory
disturbances
http://www.neuroanatomy.wisc.edu/SClinic/Weakness/Weakness.htm
Fasciculationsare irregular contractions of a group of muscle
fibers that belong to one fascicle.
Clinically, this appears as a small muscle twitch.
It is also helpful, to differentiate between the sites of the
LMN or muscle damage: body of neuron in the
anterior horn, myelination of axon (neuropathy), NMJ (myestenia
gravis) or muscle itself (myopathy).
Answer these practice questions:
Where would the sensory loss be, if you cut:
1). The left gracile fasciculus?2). The left dorsal columns
(gracile & cuneate)?
3). The right medial lemniscus, in the medulla?
Where the motor loss will be if the damage is:
4). In right side of the brain?
5). In the right anterior grey horn?
http://www.neuroanatomy.wisc.edu/SClinic/Weakness/Weakness.htmhttp://www.neuroanatomy.wisc.edu/SClinic/Weakness/Weakness.htmhttp://www.neuroanatomy.wisc.edu/SClinic/Weakness/Weakness.htm
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
10/17
Answers:
1) The left leg and lower left trunk. 2) The left side of the
body below the level of the cut. 3) The entire
left body, from the neck down. 4) The left side of the body. 5).
Muscles controlled by the peripheral
nerve at this level.
Cortex
Objectives
1.
Differentiate the major areas of the cerebral cortex:
somatosensory cortex, motor cortex and
selected Brodmanns areas.
The brain cortexis a thin (2-
4mm thick) layer of gray matter
overlying white matter. This
layer of gray matter is the
cerebral cortexand the
cerebellar cortex.The cortex forms convex folds
(gyri) and concave grooves (sulci
or fissures).
A longitudinal fissure separates the left & right cerebral
hemispheres. A big sulci divides each
hemisphere into 5 lobes: frontal, parietal, temporal, occipital
and insula. The Centralsulcusseparates
the frontal and parietal lobes. The Parieto-occipitalsulcus
separates the parietal and occipital lobes. The
Lateral sulcusseparates the temporal lobe from the frontal and
parietal lobes. The Insula (or insular
lobe) is a portion of the cortex that sits in the fold of the
lateral sulcus between the frontal and temporal
lobes.
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
11/17
The precental gyrus(anterior to the central sulcus) is the
primary motor area. The postcentral gyrus
(posterior to the central sulcus) is the primary sensory
area.
The primary sensory area receives input from the thalamus which
is a major relay station. The two
cerebral hemispheres usually receive information from the
contralateral side of the body. The special
senses (vision and hearing) are referred to special areas of the
cortex on the contaralateral side.
Early in the twentieth century, Dr. Brodmanncreated a map of the
areas of the cerebral cortex. These
studies were based on electrical stimulation of differrent areas
of the cortex during the surgery of
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
12/17
epileptic patients and recording their physiological and
behavioral reactions. Brodmann assigned
numbers to the areas with different functions. Now these areas
are known as Brodmanns areas.
Please note the location and function of: Primary somatosensory
area: postcentral gyrus = 1,2,3;
Primary visual area = 17, Primary auditory area = 41 and 42;
Primary gustatory area = 43. Wernickes
area 39-40, speech interpretation.
Reflection of the body parts in primary
sensory area (postcentral gyrus). The
size of the area is proportional to the
number of receptors in the
corresponding part of the body rather
than the size of this body part: e.g. lips
are better represented than the leg.
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
13/17
The motor areas of the cerebral cortexcontrol voluntary
movements. This control is also contralateral.
Please note the location and function of: Primary motor area
(precentral gyrus = 4) . The primary motor
area controls voluntary contractions of skeletal muscles on the
contralateral side; Motor speech
(Brocas) area = 44 & 45. Upper motor neurons are located in
this area.
Reflection of the body parts in
primary motor area depends on the
number of motor units controlled
by this area
Blue Boxesin M&A pp. 589- 592
Medical Imaging of Head.
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
14/17
Reflexes
Objectives
1.
Describe the steps in a neural reflex
2.
Classify the types of reflexes and explain the functions of
each.
1. Describe the steps in a neural reflex
http://www.answers.com/topic/reflex
-arc"Reflex arc." The Oxford Dictionary
of Sports Science. Oxford University
Press, 1998, 2006, 2007. Answers.com
10 Dec. 2010.
A reflexis a specific motor reaction to
a specific stimulus. A reflex arc is the
pathway followed by nerve impulses
that produce a reflex. An ideal reflex
arc consists of 5 steps: 1) receptor,
2) afferent fiber, 3) interneuron(s),
4) efferent fiber and 5) effector.
1. Receptors convert external or
internal stimulus (e.g. light, heat,
pressure, chemical changes) into the
action potentials.
2. Afferent (sensory) fibers transmit
these signals to the interneurons in
CNS.
3. Interneurons integrate and process the signals; it may be one
or few interneurons or no interneuron
at all.
4. Motor fibers transfer the AP from CNS to the effector.
5. Effectors (e.g. skeletal muscles, smooth muscles, glands)
perform the response.
2. Classify the types of reflexes and explain the functions of
each.
Reflexes can be classified by the site of processing: e.g.
spinal, brain stem, cerebral, etc.
Spinal reflexesare processed at the level of the spinal cord.
This allows the faster motor reaction
because the motor neuron is activated without sending signals to
the brain and back. Although, the
brain still receives the signal while the motor reaction is
occurring: e.g. myotatic stretch reflexes.
Brain reflexesare processed at the level of the brain. Their
absence indicates brain death; e.g. pupillary,
pharyngeal, cough reflexes. Cough reflex is coughing in response
to irritation of the airway linings.
Pupillary reflex is a contraction of the pupil in response to
the light. Pharyngeal reflex is a contraction of
pharyngeal constrictor muscle in response to touching the back
of the pharynx.
http://www.answers.com/topic/reflex-archttp://www.answers.com/topic/reflex-archttp://www.answers.com/topic/reflex-archttp://www.answers.com/topic/reflex-archttp://www.answers.com/topic/reflex-arc
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
15/17
Reflexes can be classified by the number of synapses:
polysynaptic vs. monosynaptic. Polysynaptic
reflexes involve more than one synapse. They are often complex
and take a longer time. Monosynaptic
reflexes involve just one synapse. There are no interneurons
involved and processing occurs in the
motor neuron. These reflexes are the most simple and
fastest.
Myotatic stretch reflexesare an example of a
spinal monosynaptic reflex. A stretch reflex is the
contraction of the muscle in response to the
stretching of the muscle spindles. Muscle
spindles are receptors inside the muscle that lie
parallel to muscle fibers. When a muscle spindle
is stretched the sensory neuron sends the signal
to the motor neuron in the ventral horn of the
spinal cord which in turn sends the signal back to
the muscle and the muscle contracts. Stretch
reflexes are very important to maintain posture
and balance. For the testing purposes the
myotatic stretch reflexes can be checked by brisktaping of the
tendon of the corresponding
muscle: knee jerk reflex (patellar ligament) ,
ankle jerk reflex (Achilles tendon), biceps reflex
(biceps tendon), brachioradialis reflex, jaw jerk,
finger jerk, etc.
http://thebrain.mcgill.ca/flash/d/d_01/d_01_cr/
d_01_cr_fon/d_01_cr_fon.html
Hyporeflexiaabsent or low response totapping (weak reflexes)
usually indicate the damage of the motor neuron within the reflex
arc (lower
neuron damage). Hyperreflexiarepeating or too strong response to
tapping indicates damage to the
descending tracts of the corticospinal
pathway (upper neuron damage). Even
if the reflex is monosynaptic information
is actually sent to the cortex as a
reference.
The Golgi tendon organ, which is
another receptor, is attached between
the muscle and the tendon. When
muscle contracts Golgi tendon organ
sends the signal to the spinal cord and
synapses on an inhibitory interneuron.
The inhibitory interneuron synapses on
an alpha motor neuron which goes to an
antagonist muscle and causes relaxation
of the antagonist. Information is also
conveyed from these receptors to the
cerebellum and cortex.13-16
Illustration of the Stretch Reflex
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
16/17
Reflexes can be classified by their development: innate vs.
acquired. Inborn or innate reflexes are
involuntary and unlearned. Withdraw reflex is pulling your body
part away from pain (e.g. hand away
from a hot surface when touched). Palatine reflex is a
swallowing in response to stimulation of the
palate. Grasp reflex is a flexion of the fingers (grasping) in
response to stimulation of the palm (in
infants). Rooting reflex; when an infant's cheek is stroked, the
baby responds by turning his or her head
in the direction of the touch and opening their mouth for
feeding. Learned or acquired reflexes are often
complex, learned motor patterns acquired during the lifetime;
e.g. walking on two extremities, biking,
swimming, driving the car, reading, writing, speech, languages,
following the traffic rules, etc.
Reflexes can be classified by the effector organs: somatic vs.
autonomic (visceral). Somatic Reflexes:
involve contractions of the skeletal muscles. Examples: Knee
Jerk reflex, biking. Babinski's
reflex dorsiflexion of the big toe results from firmly stroking
the lateral outer margin of the sole. In
adults positive Babinski is a sign of the lesions in the cortex
or in the pyramidal tract, although it is a
normal reflex in infants till one year old.
Autonomic or visceral reflexes: involve glands, smooth and
cardiac muscles, and generally are not
consciously perceived. The main integrating centers for most
autonomic reflexes are located in the
hypothalamus and brain stem. Some autonomic reflexes, e.g. for
urination and defecation, have
integrating centers in the spinal cord. Peristaltic reflex, when
a portion of the intestine is full (stretched
and irritated), the area just proximal contracts and the area
just distal relaxes. Pilomotor reflex, when
stroking or tickling the skin causing the activation of arrector
pili with formation of goose bumps.
Baroreceptor reflex, the response to stimulation of
baroreceptors of the carotid sinus and aortic arch,
regulating blood pressure by controlling heart rate, strength of
heart contractions, and diameter of
blood vessels. The steps of the visceral reflex arch are
essentially the same as somatic, but visceral has
two neurons in the motor branch: preganglionic and
postganglionic; while somatic reflex has only one
neuron in the motor branch.
Compare and contrast
steps of somatic and
visceral reflex in the image
to the right. Label each step
and structure.
http://people.eku.edu/ritch
isong/301notes2b.html
http://people.eku.edu/ritchisong/301notes2b.htmlhttp://people.eku.edu/ritchisong/301notes2b.htmlhttp://people.eku.edu/ritchisong/301notes2b.htmlhttp://people.eku.edu/ritchisong/301notes2b.htmlhttp://people.eku.edu/ritchisong/301notes2b.html
-
7/24/2019 Lecture 6 Spinal Cord Cortex Reflexes
17/17
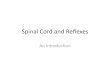
To perform Babinskis test, the sole of the foot must be firmly
stroked on the lateral side in the direction
from heel to toes as it shown in the image.
http://medical-
dictionary.thefreedictionary.com/Babinski+reflex
A and B normal adult plantar reflex causes aflexion of the
hallux and toes ( Negative Babinskis
sign).
C is positive Babinskis sign, when the big toe moves
toward the dorsum of the foot and the other toes
fan out in response to the foot stroke.
Positive Babinskis is normal in babies. Positive
Babinskis after age 2 is a sign of damage to the nerve paths
connecting the spinal cord and the brain
(the corticospinal tract).
Underlying causes of positive Babinskis test may be head trauma,
stroke, meningitis, multiple sclerosis,
brain tumor etc. A Babinski's reflex can occur on one side or on
both sides of the body. Patients withpositive Babinskis may
complain of poor coordination and muscle spasms or weakness.
http://what-when-how.com/neuroscience/the-upper-motor-neurons-motor-systems-part-3/
http://medical-dictionary.thefreedictionary.com/Babinski+reflexhttp://medical-dictionary.thefreedictionary.com/Babinski+reflexhttp://medical-dictionary.thefreedictionary.com/Babinski+reflexhttp://what-when-how.com/neuroscience/the-upper-motor-neurons-motor-systems-part-3/http://what-when-how.com/neuroscience/the-upper-motor-neurons-motor-systems-part-3/http://what-when-how.com/neuroscience/the-upper-motor-neurons-motor-systems-part-3/http://medical-dictionary.thefreedictionary.com/Babinski+reflexhttp://medical-dictionary.thefreedictionary.com/Babinski+reflex