-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
1/70
The Digestive Tract
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
2/70
2
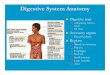
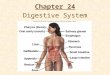
The GI tract(gastrointestinal tract)
The muscular alimentary canal
Mouth
Pharynx
Esophagus
Stomach
Small intestine
Large intestine Anus
The accessorydigestive organs
Supply secretions contributingto the breakdown of food Teeth
& tongue
Salivary glands
Gallbladder
Liver
Pancreas
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
3/70
3
The Digestive Process
Ingestion Taking in food through the mouth
Propulsion (movement of food) Swallowing
Peristalsis propulsion by alternatecontraction
&relaxation
Mechanical digestion Chewing
Churning in stomach
Mixing by segmentation
Chemical digestion By secreted enzymes: see later
Absorption Transport of digested end products into
blood and lymph in wall of canal
Defecation Elimination of indigestible substances from
body as feces
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
4/70
4
Chemical digestion
Complex food molecules (carbohydrates,
proteins and lipids) broken down into
chemical building blocks (simple sugars,amino acids, and fatty
acids and glycerol)
Carried out by enzymes secreted by digestive
glands into lumen of the alimentary canal
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
5/70
5
Ways to divide.
The more common
Plus:
epigastric
periumbilical
suprapubic
flank
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
6/70
6
Histology of alimentary canal wall
Same four layers from esophagus to anal canal
1. Mucosa
2. Submucosa
3. Muscularis
externa
4. Serosa
from lumen (inside) out
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
7/70
7
Inner layer: the mucosa*(mucous membrane)
Three sub-layers
1. Lining epithelium
2. Lamina propria
3. Muscularis
mucosae
*
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
8/70
8
More about the mucosa
Epithelium: absorbs nutrients, secretes mucus Continuous with
ducts and secretory cells of intrinsic
digestive glands (those within the wall)
Extrinsic (accessory) glands: the larger ones such as
liver and pancreas
Lamina propria
Loose connective tissue with nourishing and
absorbing capillaries
Contains most of mucosa-associated lymphoid tissue
(MALT)
Muscularis mucosae
Thin layer of muscle producing only local movements
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
9/70
9
Second layer: the submucosa*
Connective tissuecontaining majorblood and
lymphatic vesselsand nerves
Many elastic fibersso gut can regainshape after foodpasses
*
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
10/70
10
Next in, the muscularis externa*(AKA just muscularis)
Two layers of smoothmuscle responsiblefor peristalsis
andsegmentation
Inner circular layer(circumferential) Squeezes
In some places formssphincters (act asvalves)
Outer longitudinallayer: shortens gut
*
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
11/70
11
Last (outer), the serosa*(the visceral peritoneum)
Simple squamousepithelium(mesothelium) Thin layer of areolar
connective tissueunderneath
Exceptions: Parts not in peritoneal
cavity have adventitia,
lack serosa Some have both, e.g.
retroperitoneal organs
*
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
12/70
12
Smooth muscleSmooth muscle
Muscles are spindle-shaped cellsOne central nucleus
Grouped into sheets: often running
perpendicular to each other
Peristalsis
No striations (no sarcomeres)
Contractions are slow, sustained and
resistant to fatigue
Does not always require a nervous signal:
can be stimulated by stretching or hormones6 major locations:1.
inside the eye 2. walls of vessels 3. respiratory tubes
4. digestive tubes 5. urinary organs 6. reproductive organs
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
13/70
13
Nerves
Enteric nervous system: the guts own Visceral plexuses within
gut wall controlling the
muscles, glands and having sensory info
Myenteric: in muscularis
Submucosal
100 million neurons! (as many as the spinal cord)
Autonomic input: speeds or slows the system
Parasympathetic
Stimulates digestive functions
Sympathetic
Inhibits digestion
Largely automatic
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
14/70
14
Review of some definitions.
Peritoneum: serous membranes of the
abdominopelvic cavity
Visceral peritoneum: covers external
surfaces of most digestive organs
Parietal peritoneum: lines body wall
Peritoneal cavity: slit-like potential spacebetween visceral and
parietal peritoneum
Serous fluid lubricating
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
15/70
15
New definitions
Mesentery Double layer of peritoneum
Extends to digestive organs from body wall
Hold organs in place
Sites of fat storage Route by which circulatory vessels and
nerves reach
organs
Most are dorsal
Extend dorsally from gut to posterior abdominal wall Ventral
mesentery from stomach and liver to
anterior abdominal wall
Some mesenteries are called ligaments though nottechnically
such
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
16/70
16
Mesenteries
Note dorsal, ventral and formation ofretroperitoneal
position
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
17/70
17
Mesenteries
Two ventral mesenteries
Falciform ligament
Binds anterior aspect of liver
to anterior abdominal walland diaphragm
Lesser omentum (=fatty
skin) see diagram*
All other mesenteries are
dorsal (posterior)
*
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
18/70
18
Mesenteries continued (all these are dorsal)
Greater omentum Connects stomach to posterior abdominal wall
very roundabout
Wraps around spleen: gastrosplenic ligament
Continues dorsally as splenorenal ligament
A lot of fat
Limits spread of infection by wrapping around inflamed e.g.
appendix
Mesentery or mesentery proper Supports long coils of jejunum and
ileum (parts of small intestine)
Transverse mesocolon Transverse colon held to posterior
abdominal wall
Nearly horizontal sheet fused to underside of greater
omentum
Sigmoid mesocolon Connects sigmoid colon to posterior abdominal
wall
see next slides for pics
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
19/70
19
Note mesenteries: falciform ligament, lesser
omentum, greater omentum
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
20/70
20
Note: greater omentum, lesser omentum, falciform ligament,
transverse mesocolon, mesentery, sigmoid mesocolon
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
21/70
21
Some organs are retroperitoneal
Are behind the peritoneum
Fused to posterior (dorsal) abdominal wall
Lack a mesentery
Include: Most of duodenum (1st part of small intestine)
Ascending colon
Descending colon
Rectum
Pancreas
Tend to cause back pain, instead of abdominal pain
(This is as opposed to the organs which are intraperitoneal,
or just peritoneal)
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
22/70
22
Mouth = oral cavity
Lining: thick
stratified squamous
epithelium
Lips- orbicularis
oris muscle
Cheeksbuccinator muscle
The Mouth
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
23/70
23
Vermillion border or redborder Between highly
keratinized skin of face
and mucosa of mouth Needs moisture
Note frenulums (folds ofmucosa)
Palate roof of mouth Hard plate anteriorly
Soft palate posterioly
Uvula
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
24/70
24
Tongue Mostly muscles
Grip and reposition food
Forms bolus of food (lump)
Help in swallowing Speech help form some consonants
Note frenulum on previous slide: can be too tight
Taste buds contained by circumvallate and fungiform papillae
Lingual tonsil back of tongue
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
25/70
25
Teeth
Called dentition (like dentist)
Teeth live in sockets (alveoli) in the gum-
covered margins of the mandible andmaxilla
Chewing: raising and lowering themandible and moving it from
side to sidewhile tongue positions food between teeth
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
26/70
26
Teeth
Two sets
Primary or deciduous Baby teeth
Start at 6 months
20 are out by about 2 years
Fall out between 2-6 years
Permanent: 32 totalAll but 3rd set of molars by
end of adolescence
3rdset = wisdom teeth Variable
Some can be impacted(imbedded in bone)
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
27/70
27
Teeth are classified according to
shape and function
Incisors: chisel-shaped forchopping off pieces
Canines: cone shaped totear and pierce
Premolars (bicuspids) and
Molars - broad crownswith 4-5 rounded cusps forgrinding
incisor
canine
premolar
molar
Cusps are surface bumps
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
28/70
28
Tooth structure Two main regions
A. Crown (exposed)
B. Root (in socket)
C. Meet at neck
Enamel
99% calcium crystals
Hardest substance inbody
Dentin bulk of thetooth (bone-like but
harder than bone, withcollagen and mineral)
Pulp cavity with vesselsand nerves Root canal: the part of
the pulp in the root
A
B
C
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
29/70
29
Tooth structure
Cementum bonelayer of tooth root Attaches tooth to
periodontal ligament
Periodontal l igament
Anchors tooth in boneysocket of the jaw
Continuous with ging iva(gums)
Cavities orcaries- rot
Plaque film of sugar,bacteria and debris
A
B
C
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
30/70
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
31/70
31
Extrinsic salivary glands
Parotids* - largest (think mumps)
Facial nerve branch at risk during surgery here
Submandibular # - medial surface mandible
Sublingual + - under tongue; floor of mouth
Compound = duct branches
Tubo = tubes
Alveolar = sacs
*
#
+
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
32/70
32
Pharynx
Oropharynx andlaryngopharynx Stratified squamous
epithelium
Three constrictormuscles* Sequentially squeeze
bolus of food intoesophagus
Are skeletalmuscles
Voluntary action
Vagus nerve (X)
___oropharynx
___laryngopharynx
*
*
*
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
33/70
33
Esophagus
Continuation of pharynx in
mid neck Muscular tube collapsed
when lumen empty
Descends through thorax On anterior surface of
vertebral column
Behind(posterior to) trachea
Esophagus___________
*
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
34/70
34
Esophagus continued
Passes through esophageal hiatus in the diaphragm toenter the
abdomen
Abdominal part only 2 cm long Joins stomach at cardiac
orifice*
Cardiac sphincter at cardiac orifice to prevent regurgitation
(foodcoming back up into esophagus)
Gastroesophageal junction and GERD
___________________esophageal hiatus
(hiatus means opening)
*
Mi i t f h
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
35/70
35
Contains all 4
layers (see right)
Epithelium: nonkeratinized stratified squamous epithelium
At GE junction thin simple columnar epithelium Mucus glands in
wall
Muscle (muscularis externa) changes as it goes down Superior 1/3
of esophagus: skeletal muscle (like pharynx)
Middle 1/3 mixture of skeletal and smooth muscle
Inferior 1/3 smooth muscle (as in stomach and intestines)
When empty, mucosa and submucosa lie in longitudinal folds
Microscopic anatomy of esophagus
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
36/70
36
Esophagus histology
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
37/70
37
Stomach J-shaped; widest part of alimentary canal
Temporary storage and mixing 4 hours Into chyme
Starts food breakdown Pepsin (protein-digesting enzyme needing
acid
environment) HCl (hydrochloric acid) helps kill bacteria
Stomach tolerates high acid content but esophagusdoesnt why it
hurts so much when stomachcontents refluxes into esophagus
(heartburn; GERD)
Most nutrients wait until get to small intestine tobe absorbed;
exceptions are: Water, electrolytes, some drugs like aspirin
and
alcohol (absorbed through stomach)
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
38/70
38
Stomach
Lies mostly in LUQ But pain can be epigastric or
lower
Just inferior to (below)diaphragm
Anterior (in front of) spleenand pancreas
Tucked under left lowermargin of liver
Anchored at both ends butmobile in between
Main regions in drawing
toright--------------------------------
Capacity: 1.5 L food; maxcapacity 4L (1 gallon)
epigastrium
junction with
esophagus
funnel shaped
contains pyloric
sphincter
dome
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
39/70
39
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
40/70
40
Stomach Regions
Cardiac region Fundus (dome shaped)
Body
Greater curvature
Lesser curvature
Pyloric region
Antrum
Canal
Sphincter
junction with
esophagus
funnel shaped
contains pyloric
sphincter
dome
Rugae: longitudinal folds
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
41/70
41
Rugae: longitudinal foldson internal surface
(helpsdistensibility)
Muscular is: additionalinnermost oblique layer(along with
circular andlongitudinal layers)
Histology of
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
42/70
42
Histology of
stomach
Simple columnar
epithelium: secretebicarbonate-bufferedmucus
Gastric pits openinginto gastric glands
Mucus neck cells Parietal cells
HCL
Intr ins ic factor(forB12 absorption)
Chief cells Pepsinogen
(activated to pepsinwith HCL)
Stimulated by gastr in:a stomach hormone
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
43/70
43
Small intestine
Longest part of alimentary canal (2.7-5 m) Most enzymatic
digestion occurs here
Most enzymes secreted bypancreas, not
small intestine
Almost all absorption of nutrients
3-6 hour process
Runs from pyloric sphincterto RLQ
Small intestine___________
S ll i t ti h 3 bdi i i
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
44/70
44
Small intestine has 3 subdivisions Duodenum 5% of length
Jejunum almost 40%
Ileum almost 60%
Blood supp ly : super io r
mesenter ic artery;
Veins drain in to hepat ic
po rtal vein
Duodenum is retroperitoneal (stuck down under peritoneum);
others are loose
Duodenum receives
bile from liver and gallbladder via bile duct*
enzymes from pancreas via main pancreatic duct*
*
*
Small intestine designed for absorption
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
45/70
45
Small intestine designed for absorption Huge surface area
because of great length
Structural modifications also increase absorptive area Circular
folds (plicae circulares)
Villi (fingerlike projections) 1 mm high simple columnar
epithelium: velvety
Microvilli
Lacteal*: network of bloodand lymph capillaries-Carbs and prote
ins into b lood to
l iver via hepat ic por ta l vein
-Fat into lymp h:fat-solub le toxins
e.g. pest ic ides circu late
sys temical ly before going to l iverfor detoxi f icat ion
*
Absorpt iv ie cel l
with microv i l l i to
increase surface
area & m any
mitochondr ia:
nutr ient up take is
energy-
demanding
Intest inal cryp ts* (of Lieberkuhn) inbetween villi
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
46/70
46
Intest inal cryp ts(of Lieberkuhn) inbetween villi Cells here
divide every 3-6 days to renew epithelium (most rapidly dividing
cells of the
body)
Secrete watery intestinal juice which mixes with chyme (the
paste that food becomesafter stomach churns it)
Intest inal f lo ra the permanent normal bacteria Manufacture
some vitamins, e.g. K, which get absorbed
Mucus to counteract acidity
from stomach
Hormones:
Cholecystokin in(stimulates GB
to release stored bile, also pancreas)
Secretin(stimulates pancreaticducts to release acid
neutralizer)
*
-have many
mitochondr ia:
nutr ient uptakeis energy-
demanding
-produce
mucus
Duodenal glands* *
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
47/70
47
General histology of digestive tract
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
48/70
48
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
49/70
49
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
50/70
50
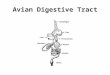
Large intestine
Subdivisions
CecumAppendix
Colon
RectumAnal canal
Digested residue reaches it
Main function: to absorb waterand electrolytes
1. Teniae coli (3 longitudinal
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
51/70
51
Three special
features
1. Teniae coli (3 longitudinalmuscle strips)
2. Haustra (puckering into sacs)
3. Epiploic appendages (omental
or fat pouches)
1.
2.
3.
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
52/70
52
Between ileum
and cecum
1stpart
Bl ind tube
Colon has segments: ascending , transverse and descending c
olon; then sigm oid colon
Right angle turns:hepatic f lexure* in RUQan dsplenic f lexure*
in LUQ
*
*
S-shaped
Movement sluggish and weak except for a few mass peristaltic
movements per day to force feces toward rectum powerfully
Rectum
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
53/70
53
In pelvis
No teniae
Strong longitudinal musclelayer
Has valves
Anal canal Pectinate line*
Inferior to it: sensitive topain
Hemorrhoids (enlargedveins) Superior to pectinate
line: internal
Inferior to pectinate line:external
Sphincters (close opening) Internal*
smooth muscle
involuntary
External* skeletal muscle
voluntary
*
*
*
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
54/70
54
Defecation
1. Triggered by stretching ofwall, mediated by spinalcord
parasympathetic reflex
2. Stimulates contraction ofsmooth muscle in wall and
relaxation of internal analsphincter
3. If convenient to defecatevoluntary motor neuronsstimulate
relaxation ofexternal anal sphincter
(aided by diaphragm andabdominal wall muscles -called Valsalva
maneuver)
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
55/70
55
Histology large intestine
No villi Fewer nutrients
absorbed
Columnar cells in pic
= absorptive cells Take in water and
electrolytes
A lot of goblet cells formucus Lubricates stool
More lymphoid tissue A lot of bacteria in stool
Th Li
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
56/70
56
The Liver
Largest gland in the body
(about 3 pounds) Over 500 functions
Inferior to diaphragm inRUQ and epigastric areaprotected by
ribs
R and L lobes Plus 2 smaller lobes
Falciform ligament Mesentery binding liver to
anterior abdominal wall
2 surfaces Diaphragmatic
Visceral
Covered by peritoneum Except bare area fused to
diaphragm
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
57/70
57
anterior
poster ior
Fissureon visceral surface
Porta hepat is: major vessels and nervesenter and leave - see
pics
Ligamentum teres: remnant of
umbilical vein in fetus, attaches to navel
see next slide
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
58/70
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
59/70
59
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
60/70
60
Just some of the livers repertoire
Produces bile
Picks up glucose from blood
Stores glucose as glycogen
Processes fats and amino acids
Stores some vitamins
Detoxifies poisons and drugs
Makes the blood proteins
Li hi t l
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
61/70
61
Liver histology Liver lobules (about one million of them)
Hexagonal solid made of sheets ofhepatocytes(liver
cells) around a central vein
Corners of lobules have portal triads
(see next pic)
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
62/70
62
Portal tr iad
Portal arteriole
Portal venule Branch of hepatic
portal vein Delivers substances
from intestines forprocessing byhepatocytes
Bile duct Carries bile away
Liver sinusoids Large capillaries
between plates ofhepatocytes
Contribute to centralvein and ultimately to
hepatic veins and IVC Kupffercells
Liver macrophages
Old blood cells andmicroorganismsremoved
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
63/70
63
Hepatoc tes (li er cells)
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
64/70
64
Hepatocytes (liver cells)
Many organelles
Rough ER manufactures blood proteins Smooth ER help produce bile
salts and detoxifies
blood-borne poisons
Peroxisomes detoxify other poisons, includingalcohol
Golgi apparatus packages Mitochondria a lot of energy needed for
all this
Glycosomes - role in storing sugar and regulation ofblood
glucose (sugar) levels
Produce 500-1000 ml bile each day Secrete into bile canaliculi
(little channels) then ducts
Regeneration capacity through liver stem cells
Gallbladder*
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
65/70
65
Gallbladder Bile is produced in the liver
Bile is stored in the gallbladder
Bile is excreted into theduodenum when needed (fattymeal)
Bile helps dissolve fat andcholesterol
If bile salts crystallize, gallstones are formed
Intermittent pain: ball valveeffect causing
intermittentobstruction
Or infection and a lot of pain,fever, vomiting, etc.
*
PancreasLies in LUQ kind of behind stomach
Is retroperitoneal
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
66/70
66
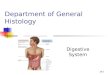
Pancreas
(exocrine and
endocrine)
Is retroperitoneal
Has a head, body and tail
Head is in C-shaped curve of duodenum
Tail extends left to touch spleen
Main pancreatic duct runs thelength of thepancreas, joins bile
duct
http://upload.wikimedia.org/wikipedia/commons/1/15/Gray1100.pnghttp://upload.wikimedia.org/wikipedia/commons/1/15/Gray1100.pnghttp://upload.wikimedia.org/wikipedia/commons/1/15/Gray1100.png
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
67/70
67
Pancreaticone acinus
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
68/70
68
Pancreatic
exocrine function
Compound acinar(sac-
like) glands opening into
large ducts (therefore
exocrine) Acinarcells make 22
kinds of enzymes
Stored in zymogen
granules Grape-like arrangement
Enzymes to duodenum,
where activated
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
69/70
-
7/27/2019 Lecture 22 - The Digestive Tract (Histology)
70/70
Endocrine cells: