Embed Size (px)
Citation preview

1
GIT APPLIED/CLINICAL
ASPECTSLecture – 10
Dr. Zahoor Ali Shaikh

2
GIT APPLIED/CLINICAL ASPECTS We will look at some important
conditions/diseases that can affect GIT. This lecture will introduce you to the
applied/clinical aspects, details of these conditions you will do later.

3
APPLIED ASPECTS Topics Vomiting Hunger Contraction Gastro Oesophagal Reflux Disorder Peptic Ulcer Jaundice Hepatitis [Viral] Liver Transplant Pancreatitis Celiac Disease [Gluten Entropathy] Irritable Bowel Syndrome Inflammatory Bowel Disease Food Poisoning Traveler's Diarrhea Parasitic Infections of Intestine

4
VOMITING
It is forceful expulsion of gastric contents through mouth.
Major force of expulsion comes from contraction of diaphragm and abdominal muscles.
There is vomiting center in Medulla, it co-ordinates the act of vomiting.
Contracting diaphragm descends downwards on the stomach.
5
VOMITING (cont) At the same time, abdominal muscles
compress the abdominal cavity and increase the intra-abdominal pressure.
Stomach is squeezed between the diaphragm above and compressed abdominal cavity below.
The gastric contents are forced upwards through relaxed sphincter and esophagus, out through the mouth.
6
CAUSES OF VOMITING
Touching the back of throat e.g. seeing the throat using the tongue depressor.
Distension of stomach.
Increased intracranial pressure e.g. head injury causing intra cerebral hemorrhage.

7
CAUSES OF VOMITING (cont) Motion sickness.
Drugs.
Renal Failure.
Psychogenic e.g. emotional factors

8
HUNGER CONTRACTION Gastric Contraction can sometimes be
felt and may be mildly painful [peristaltic wave].
Hunger Contraction are associated with sensation of hunger and play role in regulation of appetite.
9
Gastro Esophagal Reflux Disorder [GERD]
Patient with reflux has persistent symptoms.
It occurs when lower Esophagal sphincter tone fails to increase when patient is lying down or when intro-abdominal pressure increases.
Patient complains of heart burn.

10

11

12
PEPTIC ULCER
Duodenal Ulcer [D.U] are more common than Gastric Ulcer.
10 - 15% of population may suffer from D.U.
Patient complains of epigastric pain, relationship of pain with food is variable and may not be helpful in diagnosis.
13
PEPTIC ULCER (cont)
D.U pain is more when patient is hungry.
If long standing symptoms investigation like test for H.Pylori and Endoscopy can be done.

14

15
JAUNDICE
We have already discussed three types of Jaundice.
(i). Prehepatic or Hemolytic Jaundice
(ii). Hepatic e.g. Viral
(iii). Post-hepatic or Obstructive e.g. Gall stones

16
HEPATITIS-VIRAL

17
LIVER TRANSPLANT
It is established treatment for number of diseases.
Acute Liver Failure. Chronic Liver Failure.

18
GALL STONES
We have already discussed Gall Stones. Ultrasound is helpful in diagnosis. Cholecystectomy – Laparoscopic is
done now in requires 48hours stay in hospital.

19
Image showing Normal Gall bladder

20
Gallstones

21

22
Ultrasound showing normal gallbladder

23
Ultrasound showing gallstones

24
PANCREATITIS
Patient complains of pain in epigastric region.
Pain radiates to back. Acute Pancreatitis can be due to gall
stones, alcohol, viral infection e.g. mums, hyperlipidaemia.
Chronic Pancreatitis can be due to alcohol, hypercalcaemia.
25
PANCREATITIS (cont)
Investigation which help in Diagnosis Blood test e.g. Serum Amylase will be
raised. Abdominal ultrasound.
26
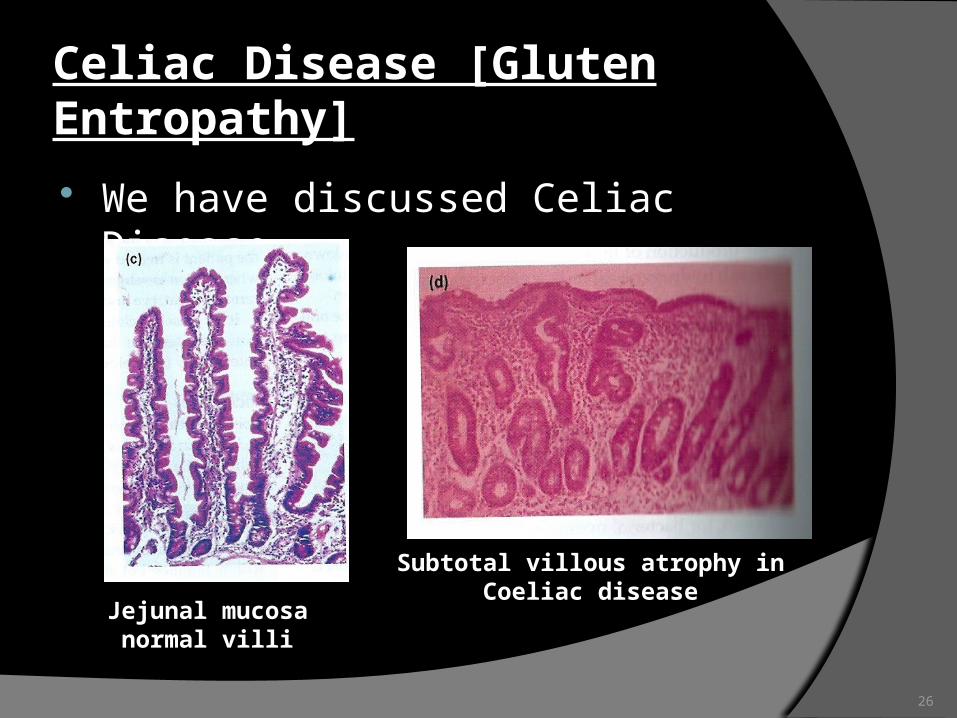
Celiac Disease [Gluten Entropathy] We have discussed Celiac Disease.
Jejunal mucosa normal villi
Subtotal villous atrophy in Coeliac disease

27
Irritable Bowel Syndrome
It is functional Bowel disorder.
More common in female than male.
Anxiety factor is common.
28
Irritable Bowel Syndrome (cont) Patient gives history of
- Abnormal Stool Frequency – more than 3/day.
- Abnormal Stool Form – watery, loose or hard stool.
- Feeling of incomplete evacuation.
- Passage of mucus.
- Abdominal Distension.

29
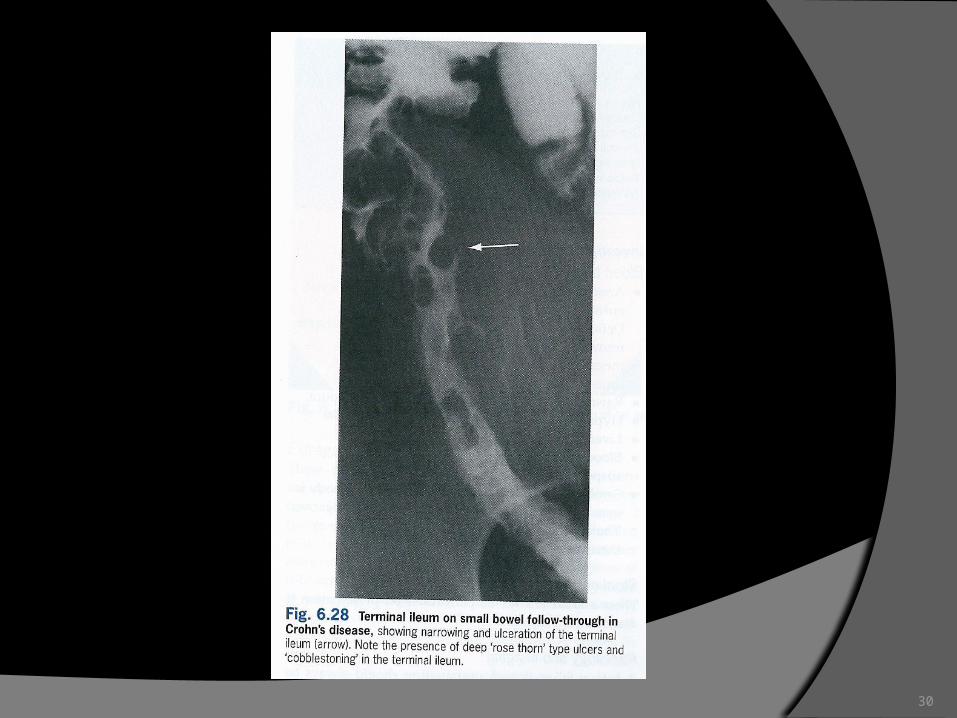
Inflammatory Bowel Disease [IBD] Two major diseases are
- Crohn’s Disease [CD] – it can affect any part of GIT.
- Ulcerative Colitis [UC] – it affects large intestine.
30

31
Inflammatory Bowel Disease

32
FOOD POISONING

33
Traveler's Diarrhea [TD]

34
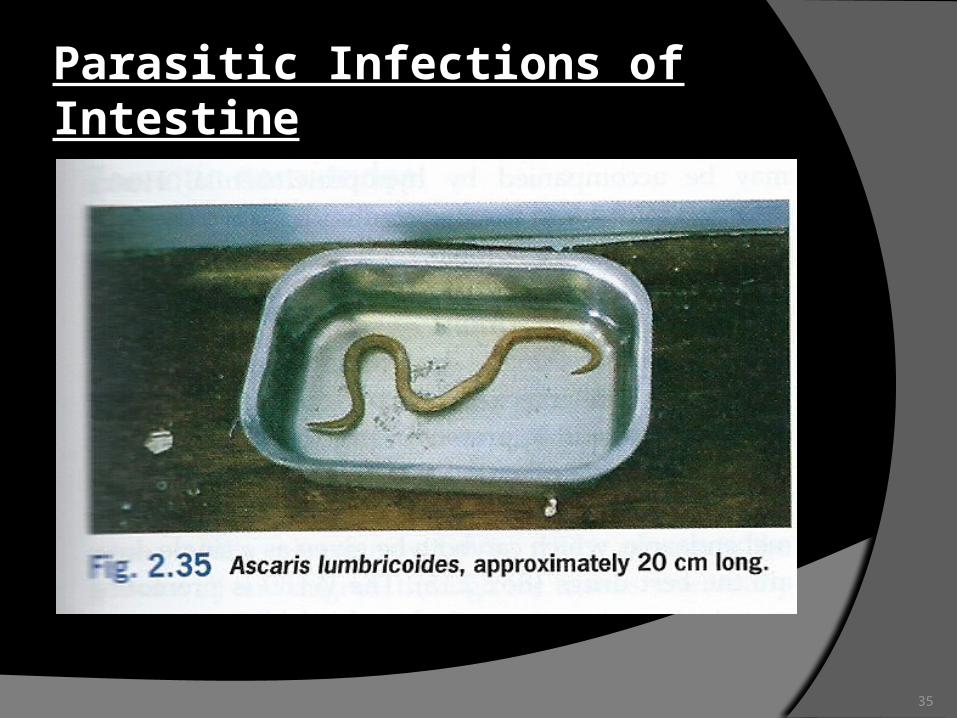
Parasitic Infections of Intestine GIT Parasites
- Entamoeba Histolytica – Amoebiasis
- Giardiasis Intestinal Worms
- Thread worm – Entrobius Vermicularis
- Round worm – Ascaris Lumbricoides
- Hook worm – Ancylostoma Duodenal
35
Parasitic Infections of Intestine
36
Thank you








![ERYTHROCYTES [RBCs] Lecture – 2 Dr. Zahoor Ali Shaikh 1](https://img.dokumen.tips/doc/110x75/56649dc45503460f94ab688e/erythrocytes-rbcs-lecture-2-dr-zahoor-ali-shaikh-1.jpg)