Embed Size (px)
DESCRIPTION
anatomy
Citation preview

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 1/42
© 2013 Pearson Education, Inc.
West Beach, South Australia

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 2/42
Slides includes material (direct or modified) from © 2013 Pearson Education, Inc. Human Anatomy & Physiology, Ninth Edition and materialsupplied by Dr J Carnegie and other sources as referenced
The Respiratory System
Lectures 1&2
ANP 1105A&EAnthony Krantis, [email protected]
These slides contain material to be presented in lecture*.The information from the lecture should be used in combination with the
relevant chapters of the recommended Text book(s).Throughout this presentation, there are references to and use of figures
from the text book. In addition, specific animations/videosare also referenced and can be used by the student forstudy purposes, if they wish.*Slides marked with a STAR will not be covered in the lecture but are
provided as additional learning material

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 3/42
Basics of the Respiratory SystemFunctional Anatomy
•
What structural aspects must be considered in theprocess of respiration? –
The conduction portion
–
The exchange portion
–
The structures involved withventilation
• Skeletal & musculature•
Pleural membranes
• Neural pathways
•
All divided into
–
Upper respiratory tract•
Entrance to larynx
–
Lower respiratory tract• Larynx to alveoli (trachea
to lungs)

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 4/42
© 2013 Pearson Education, Inc.
Figure 22.1 The major respiratory organs in relation to surrounding structures
Nasal cavity
Nostril
Larynx
Trachea
Carina oftrachea
Right main(primary)bronchusRightlung
Oral cavity
Pharynx
Left main(primary)
bronchusLeft lung
Diaphragm

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 5/42
•
Conducting zone-conduits to gas exchange sites
– Includes all other respiratory structures;
cleanses, warms, humidifies air
•
Respiratory zone-site of gas exchange – Microscopic structures-respiratory
bronchioles, alveolar ducts, and alveoli
•
Diaphragm and other respiratory muscles promoteventilation
© 2013 Pearson Education, Inc.
Functional Anatomy

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 6/42
© 2013 Pearson Education, Inc.
Figure 22.3b The upper respiratory tract.
Pharyngeal tonsil
Oropharynx
Cribriform plateof ethmoid bone
Sphenoid sinus
Posterior nasalaperture
Nasopharynx
Opening ofpharyngotympanic tube
Uvula
Palatine tonsil
Isthmus of thefauces
Laryngopharynx
Esophagus
Trachea
Frontal sinus
Nasal cavityNasal conchae(superior, middleand inferior)
Nasal meatuses(superior, middle,and inferior)
Nasal vestibule
Nostril
Hard palate
Soft palate
Tongue
Lingual tonsil
Hyoid boneLarynx
EpiglottisVestibular fold
Thyroid cartilage
Vocal fold
Cricoid cartilage
Thyroid gland

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 7/42© 2013 Pearson Education, Inc.
Nasal Cavity
•
Olfactory mucosa contains olfactory epithelium
• Respiratory mucosa
– Pseudostratified ciliated columnarepithelium
–
Mucous and serous secretions containlysozyme and defensins
– Cilia move contaminated mucusposteriorly to throat
– Inspired air warmed by plexuses ofcapillaries and veins
– Sensory nerve endings trigger sneezing
Within and posterior to external nose
• During inhalation, conchae & nasal mucosa
– Filter, heat, & moisten air
• During exhalation these structures – Reclaim heat & moisture

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 8/42© 2013 Pearson Education, Inc.
Paranasal Sinuses
Lighten skull; secrete mucus; help to warm and moisten air
• Rhinitis
– Inflammation of nasal mucosa
– Nasal mucosa continuous with mucosa ofrespiratory tract ! spreads from nose ! throat
! chest
– Spreads to tear ducts and paranasal sinusescausing
• Blocked sinus passageways! air absorbed! vacuum ! sinus headache

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 9/42© 2013 Pearson Education, Inc.
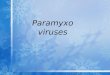
Pharynx
Connects nasal cavity and mouth to larynx and esophagus
–
Composed of skeletal muscle
–
Three regions
Nasopharynx
Oropharynx
Laryngopharynx
Pharynx
Figure 22.3c The upper respiratory tract.

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 10/42
© 2013 Pearson Education, Inc.
Larynx
• Continuous with trachea
–
Provides patent airway
– Routes air and food intoproper channels
– Voice production
Nine cartilages : All hyaline
cartilage except epiglottis
Epiglottis-elastic cartilage;covers laryngeal inlet duringswallowing; covered in taste
bud-containing mucosa
Body of hyoid bone
Thyroid cartilage
Laryngeal prominence(Adam’s apple)
Cricothyroid ligament
Cricotracheal ligament
Thyrohyoidmembrane
Cricoid cartilage
Tracheal cartilages
Epiglottis
Figure 22.4a The larynx.
Trachea

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 11/42

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 12/42
© 2013 Pearson Education, Inc.
• Pulmonary ventilation (breathing)-movement of air into and out
of lungs
• External respiration-O2 and CO2 exchange between lungs and blood
• Transport-O2 and CO2 in blood
• Internal respiration-O2 and CO2
exchange between systemic blood
vessels and tissues
Respiratorysystem
Circulatorysystem
Processes of Respiration

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 13/42
© 2013 Pearson Education, Inc.
Trachea
Esophagus
Trachealis
muscle
Lumen oftrachea
Posterior
Mucosa
Submucosa
Hyaline cartilage
Adventitia
Seromucous glandin submucosa
Anterior
Cross section of the tracheaand esophagus
• Windpipe –from larynx into
mediastinum• 3 layers
– Mucosa-ciliated pseudo-stratified epithelium withgoblet cells
– Submucosa-connective tissue
– Adventitia-outermost layer ofconnective tissue; encases C-
shaped rings of hyaline
cartilage
Figure 22.6a Tissue composition of the tracheal wall.

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 14/42
© 2013 Pearson Education, Inc.
Figure 22.10c Anatomical relationships of organs in the thoracic cavity.
Transverse section through the thorax, viewed from above. Lungs, pleuralmembranes, and major organs in the mediastinum are shown.
Posterior
Parietal pleura
Visceral pleura
Pleural cavity
Pericardial
membranesSternum
Vertebra
Esophagus
(in mediastinum)Root of lungat hilum
• Left mainbronchus• Left pulmonaryartery
• Left pulmonaryvein
Thoracic wall
Heart (in mediastinum)
Anterior mediastinum
Anterior
Left lung
Pulmonary trunk
Right lung

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 15/42
© 2013 Pearson Education, Inc.
Figure 22.7 Conducting zone passages
Superior lobe
of right lung
Middle lobe
of right lung
Inferior lobe
of right lung
Trachea
Superior lobe
of left lung
Left main(primary)bronchus
Lobar (secondary)bronchus
Segmental (tertiary)bronchus
Inferior lobeof left lung

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 16/42
© 2013 Pearson Education, Inc.
Conducting Zone Structures
• Trachea! right and left main (primary) bronchi
•
Each main bronchus enters hilum of one lung
– Right main bronchus wider, shorter, morevertical than left
• Each main bronchus branches into lobar
(secondary) bronchi (three on right, two on left)
– Each lobar bronchus supplies one lobe
•
Air passages undergo 23 orders of branching !
bronchial (respiratory) tree •
From tips of bronchial tree ! conducting zonestructures ! respiratory zone structures

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 17/42
© 2013 Pearson Education, Inc.
Figure 22.11 A cast of the bronchial tree.
Right lung Left lung
Left superiorlobe(4 segments)
Left inferiorlobe(5 segments)
Rightinferior lobe(5 segments)
Right
middlelobe (2segments)
Rightsuperiorlobe (3segments)
• Lobar bronchus branches into segmental (tertiary) bronchi
–
segmental bronchi divide repeatedly
• Branches become smaller
Bronchioles- <1 mm in diameter Terminal bronchioles - < 0.5 mm

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 18/42
© 2013 Pearson Education, Inc.
Respiratory ZoneBegins as terminal bronchioles ! respiratory bronchioles !
alveolar ducts ! alveolar sacs
–
Alveolar sacs contain clusters of alveoli
•
~300 million alveoli make up most of lung volume
•
Sites of gas exchange
Alveolar duct
Respiratory bronchioles
Terminalbronchiole
Alveoli
Alveolar duct
Alveolarsac
Figure 22.8a Respiratory zone structures.

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 19/42
© 2013 Pearson Education, Inc.
Figure 22.9a Alveoli and the respiratory membrane.
Terminal bronchiole
Respiratory bronchiole
Smooth
muscle
Elasticfibers
Alveolus
Capillaries
Diagrammatic view of capillary-alveoli relationships
Alveolar and capillary walls and
their fused basement membranes
~0.5µm thick; gas exchange by
simple diffusion

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 20/42
© 2013 Pearson Education, Inc.
Figure 22.9c Alveoli and the respiratory membrane
Red bloodcell incapillary
Alveoli(gas-filledair spaces)
Type IIalveolarcell
Type Ialveolarcell
Capillary
Macrophage
Endothelial cellnucleus
Respiratorymembrane
Alveolarepithelium
Fused basementmembranes ofalveolarepithelium and
capillaryendothelium
Capillaryendothelium
Capillary
Alveolus
Nucleus of type Ialveolar cell
Alveolar pores
Red bloodcell
Alveolus
secrete surfactant and
antimicrobial proteins

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 21/42
© 2013 Pearson Education, Inc.
Blood Supply
• Pulmonary circulation (low P, high V)
–
Pulmonary arteries deliver systemic venous blood to lungs foroxygenation
• feed into pulmonary capillary networks
– Pulmonary veins carry oxygenated blood from respiratory zones toheart
• Bronchial arteries provide oxygenated blood to lung tissue
– Arise from aorta and enter lungs at hilum
– Part of systemic circulation (high P, low V)
– Supply all lung tissue except alveoli
–
Bronchial veins anastomose with pulmonary veins•
Pulmonary veins carry most venous blood back to heart

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 22/42
22
Lungs and Pleura
Pleural cavity – slit-like potential space filled with pleuralfluid
"
Lungs can slide but separation from pleura is resisted(acts like film between 2 plates of glass)
" Lungs cling to thoracic wall and are forced to expand
and recoil as volume of thoracic cavity changesduring breathing
Around each lung is a flattenedsac of serous membrane called pleura
Parietal pleura – outer layer
Visceral pleura – directly on lung

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 23/42
© 2013 Pearson Education, Inc.
Pressure Relationships in the Thoracic Cavity
• Atmospheric pressure (Patm)
–
P exerted by air surrounding body
– 760 mm Hg at sea level = 1 atmos
• Respiratory pressures described relative to Patm
–
Negative respiratory pressure- less than Patm – Positive respiratory pressure- greater than Patm
– Zero respiratory pressure = Patm

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 24/42
© 2013 Pearson Education, Inc.
Intrapulmonary Pressure
• Intrapulmonary (intra-alveolar) pressure (Ppul)
–
Pressure in alveoli
–
Fluctuates with breathing
– Always eventually equalizes with Patm

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 25/42
© 2013 Pearson Education, Inc.
Intrapleural Pressure
• Intrapleural pressure (Pip)
–
Pressure in pleural cavity
– Fluctuates with breathing
– Always negative
–
Fluid level must be minimal• Pumped out by lymphatics
• If accumulates! positive Pip ! lung collapse
Disruption of the integrity of the pleuralmembrane will result in a rapid
equalization of pressure and loss ofventilation function = collapsed lung or
pneumothorax

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 26/42
© 2013 Pearson Education, Inc.
Figure 22.12 Intrapulmonary and intra-pleural pressure relationships.
Atmospheric pressure (P atm) 0 mm Hg (760 mm Hg)
Thoracic wall
Parietal pleura
Visceral pleura
Pleural cavity
Transpulmonarypressure 4 mm Hg(the differencebetween 0 mm Hgand !4 mm Hg)
Intrapleuralpressure (P ip) !4 mm Hg(756 mm Hg)
Intrapulmonarypressure (P pul) 0 mm Hg(760 mm Hg)
Diaphragm
Lung
0
– 4
• If Pip = Ppul or Patm ! lungs collapse
• (Ppul – Pip) = transpulmonary pressure
– Keeps airways open
– Greater transpulmonary pressure! larger lungs

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 27/42
© 2013 Pearson Education, Inc.
Figure 22.13 Changes in thoracic vol. and sequence of events duringinspiration
Inspiratory musclescontract (diaphragmdescends; rib cage rises).
Thoracic cavity Vincreases.
Lungs are stretched;intrapulmonary Vincreases.
Intrapulmonary Pdrops (to –1 mm Hg).
Air (gases) flows intolungs down its P gradientuntil intrapulmonaryP is 0 (= Atmos P).
I n s p i r a t i o n
SequenceChanges in anterior-posterior &
superior-inferior dimensions
Changes in lateral dimensions
(superior view)
1
2
3
4
5 Diaphragmmoves inferiorlyduringcontraction.
Ribs areelevated andsternumflares as
externalintercostalscontract.
Externalintercostalscontract
*** ACTIVE PROCESS
During deep or forced inspiration,
additional muscles recruited:
Scalenes
Sternocleidomastoid
Pectoralis minor
Quadratus lumborum on 12th rib
Erector spinae

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 28/42
© 2013 Pearson Education, Inc.
Figure 22.13 Changes in thoracic vol. and sequence of events during expiration
1
E x p i r a t i o
n
SequenceChanges in anterior-posterior and
superior-inferior dimensions
Changes in lateral dimensions
(superior view)
2
3
4
5 Diaphragmmovessuperiorlyas it relaxes.
Ribs andsternum aredepressed
as externalintercostalsrelax.
Externalintercostalsrelax
Inspiratory muscles relax(diaphragm rises; rib cagedescends due to recoil ofcostal cartilages).
Thoracic cavity volumedecreases.
Elastic lungs recoilpassively; intrapulmonaryVolume decreases.
Intrapulmonary P rises(to +1 mm Hg).
Air (gases) flows out oflungs down its P gradientuntil intrapulmonarypressure is 0.
PASSIVE PROCESS….but forced expiration- is active process; usesabdominal (oblique and transverse) and internal intercostal muscles

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 29/42
© 2013 Pearson Education, Inc.
Figure 22.14 Changes in intrapulmonary and intrapleural pressures during inspiration and expiration.
Intrapulmonary PPressure inside lung
decreases as lung volincreases duringinspiration; pressureincreases during expiration.
Intrapleural P Pleural cavity pressure
becomes more negative aschest wall expands duringinspiration. Returns to initial
value as chest wall recoils.
Volume of breath. Duringeach breath, the pressure
gradients move 0.5 liter ofair into and out of the lungs.
P r e s s u r e r e l a t i v e t o
a t m o s
p h e r i c p r e s s u r e
( m m H
g )
V o l u m
e ( L )
Inspiration Expiration
Intrapulmonarypressure
Trans-pulmonarypressure
Intrapleuralpressure
Volume of breath
5 seconds elapsed
+2
0
–2
–4
–6
–8
0.5
0

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 30/42
© 2013 Pearson Education, Inc.

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 31/42
© 2013 Pearson Education, Inc.
Pulmonary Ventilation: Inspiration and Expiration
Mechanical processes due to volume changes in thoracic
cavity –
Volume (V) changes! P changes
–
P changes! gases flow to equalize P
Boyle's LawPressure (P) varies inversely
with volume (V): P1V1 = P2V2
Three factors hinder
air passage & pulmonary ventilation;
1. Airway resistance
2. Alveolar surface tension
3. Lung compliance

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 32/42
© 2013 Pearson Education, Inc.
Airway Resistance
• Friction- major nonelastic source of resistance to
gas flow; occurs in airways
• Relationship between flow (F), pressure (P), and
resistance (R) is:
– !P - pressure gradient between atmosphere and
alveoli (2 mm Hg or less during normal quiet
breathing)
–
Gas flow changes inversely with resistance

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 33/42
© 2013 Pearson Education, Inc.
Conductingzone
Respiratoryzone
Medium-sizedbronchi
R
e s i s t a n c e
Terminal
bronchioles
1 5 10 15 20 23
Airway generation(stage of branching)
Figure 22.15 Resistance in respiratory passageways

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 34/42
© 2013 Pearson Education, Inc.
Homeostatic Imbalance
• As airway resistance rises, breathing
movements become more strenuous
- Severe constriction or obstruction of
bronchioles
- Can prevent ventilation –
Eg. acute asthma attacks; stops ventilation
• Epinephrine dilates bronchioles, reduces air
resistance

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 35/42
© 2013 Pearson Education, Inc.
Alveolar Surface Tension
•
Surface tension
–
Attracts liquid molecules to one another at gas-liquidinterface
–
Resists any force that tends to increase surface area
of liquid
–
Water–high surface tension; coats alveolar walls !
reduces them to smallest size
• Surfactant
–
Detergent-like lipid protein complex produced by type II alveolarcells
–
Reduces surface tension of alveolar fluid and discouragesalveolar collapse
–
Insufficient quantity in premature infants causes infant
respiratory distress syndrome ! alveoli collapse after each
breath

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 36/42
© 2013 Pearson Education, Inc.
Lung Compliance
• Measure of change in lung V that occurs
with given change in transpulmonary P
• Higher lung compliance! easier to
expand lungs
•
Normally high due to
–
Distensibility of lung tissue
– Alveolar surface tension

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 37/42
© 2013 Pearson Education, Inc.
Pulmonary Function Tests
• Spirometer- measures respiratory volumes and
capacities
• Spirometry can distinguish between
– Obstructive pulmonary disease —increasedairway resistance (e.g., bronchitis)
•
TLC, FRC, RV may increase
– Restrictive disorders —reduced TLC due todisease or fibrosis
• VC, TLC, FRC, RV decline

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 38/42
© 2013 Pearson Education, Inc.
Figure 22.16a Respiratory volumes and capacities.
5000
4000
3000
2000
1000
0
M i l l i l i t e r s ( m l )
Spirographic record for a male
6000
Inspiratoryreserve volume
3100 ml
Expiratoryreserve volume
1200 ml
Residual volume1200 ml
Inspiratorycapacity3600 ml
Functionalresidualcapacity2400 ml
Vitalcapacity4800 ml
Total lungcapacity6000 ml
Tidal volume 500 ml

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 39/42
© 2013 Pearson Education, Inc.
Figure 22.16b Respiratory volumes and capacities.
Measurement
Adult male
ave value
Adult female
ave value Description
Respiratoryvolumes
Respiratorycapacities
Summary of respiratory volumes and capacities for males and females
Tidal volume (TV)
Inspiratory reservevolume (IRV)
Expiratory reservevolume (ERV)
Residual volume (RV)
500 ml 500 ml
3100 ml
1200 ml
1200 ml
1900 ml
700 ml
1100 ml
Amount of air inhaled or exhaled with each breath under restingconditions
Amount of air that can be forcefully inhaled after a normal tidalvolume inspiration
Amount of air that can be forcefully exhaled after a normal tidalvolume expiration
Amount of air remaining in the lungs after a forced expiration
Maximum amount of air contained in lungs after a maximuminspiratory effort: TLC = TV + IRV + ERV + RV
Maximum amount of air that can be expired after a maximuminspiratory effort: VC = TV + IRV + ERV
Maximum amount of air that can be inspired after a normal tidalvolume expiration: IC = TV + IRV
Volume of air remaining in the lungs after a normal tidal volumeexpiration: FRC = ERV + RV
6000 ml
4800 ml
3600 ml
2400 ml
4200 ml
3100 ml
2400 ml
1800 ml
Total lung capacity (TLC)
Vital capacity (VC)
Inspiratory capacity (IC)
Functional residualcapacity (FRC)

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 40/42
© 2013 Pearson Education, Inc.
Dead Space
• Anatomical dead space
–
No contribution to gas exchange
– Air remaining in passageways; ~150 ml
•
Alveolar dead space –non-functional alveoli
due to collapse or obstruction
•
Total dead space-sum of anatomical andalveolar dead space

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 41/42
© 2013 Pearson Education, Inc.
AVR = frequency X (TV – dead space)
(ml/min)
(breaths/min)
(ml/breath)
Alveolar Ventilation
• Good indicator of effective ventilation
•
Alveolar ventilation rate (AVR)-flow of gases into and out ofalveoli in one minute - rough estimate of respiratory efficiency
• Dead space normally constant
• Rapid, shallow breathing decreases AVR
AVR – Normal at rest = ~ 6 L/min
– Normal with exercise = up to 200 L/min

7/21/2019 Lec 12 - pt.1 - Rsystem
http://slidepdf.com/reader/full/lec-12-pt1-rsystem 42/42
Table 22.2 Effects of Breathing Rate and Depth on Alveolar ventilation