Embed Size (px)
Citation preview

Slide 1
Chest X ray interpretation
David O’Neill MSc BSc RN NMP FHEA
Associate Lecturer Cardiff University (Non Medical Prescribing)
Respiratory Advanced Nurse Practitioner Royal Gwent Hospital Newport
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 2 Learning Outcomes
• Understand role of chest x-rays in acute care
• Review surface anatomy of the lungs
• Identify normal structures on an x-ray
• Recognise the types of densities in chest x-
ray
• Understand the steps involved in interpreting
a chest x-ray
• Interpret examples of X rays you may be
asked to review
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 3 Clinical Patient Assessment
• Clinical Patient Assessment (CPA) involves:
– Patient history (75-85% of diagnosis stems from this)
– Clinical examination
– Formulating a working diagnosis
– Differential diagnosis
– Choosing appropriate investigations
– EVALUATION OF THE ABOVE(Longmore et al 2002)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 4 X ray in acute care
• Used to evaluate for:
• NORMALITY
• Consolidation (Pneumonia)
• Pneumothorax
• Atelectasis
• Pleural effusion (including haemothorax)
• COPD
• TUBERCULOSIS
• MALIGNANCY
• POSITIONING OF MEDICAL DEVICES
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 5 Be systematic
• Some anatomical structures in the
chest should be assessed on every
chest x-ray
• Each of these anatomical structures
should be viewed using a systematic
approach
• There are also important structures that
are obscured or become visible only
when abnormal
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 6 Mnemonic
Some S=Skin
Body B=Bones
Lost L=Lungs and pleura
My M=Myocardium (Heart)
Toy T=Trachea
Dinosaur D=Diaphragm
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
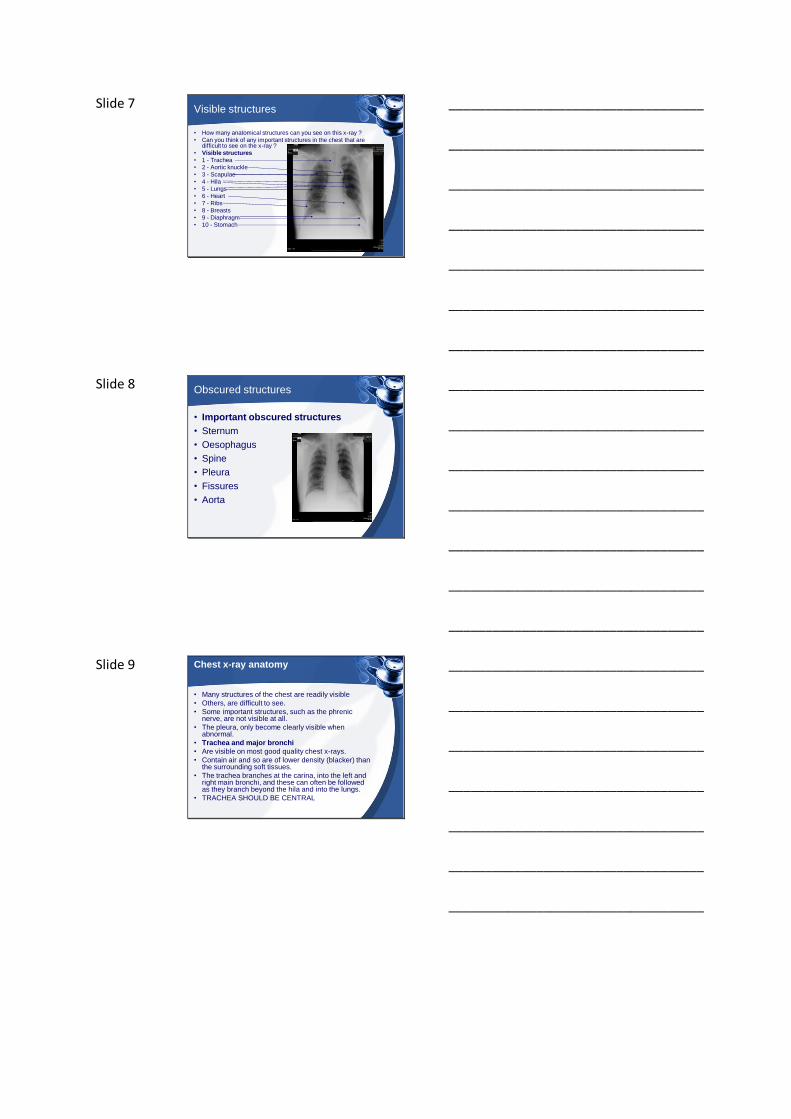
Slide 7 Visible structures
• How many anatomical structures can you see on this x-ray ?
• Can you think of any important structures in the chest that are difficult to see on the x-ray ?
• Visible structures
• 1 - Trachea
• 2 - Aortic knuckle
• 3 - Scapulae
• 4 - Hila
• 5 - Lungs
• 6 - Heart
• 7 - Ribs
• 8 - Breasts
• 9 - Diaphragm
• 10 - Stomach
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 8 Obscured structures
• Important obscured structures
• Sternum
• Oesophagus
• Spine
• Pleura
• Fissures
• Aorta
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 9 Chest x-ray anatomy
• Many structures of the chest are readily visible
• Others, are difficult to see.
• Some important structures, such as the phrenic nerve, are not visible at all.
• The pleura, only become clearly visible when abnormal.
• Trachea and major bronchi
• Are visible on most good quality chest x-rays.
• Contain air and so are of lower density (blacker) than the surrounding soft tissues.
• The trachea branches at the carina, into the left and right main bronchi, and these can often be followed as they branch beyond the hila and into the lungs.
• TRACHEA SHOULD BE CENTRAL
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
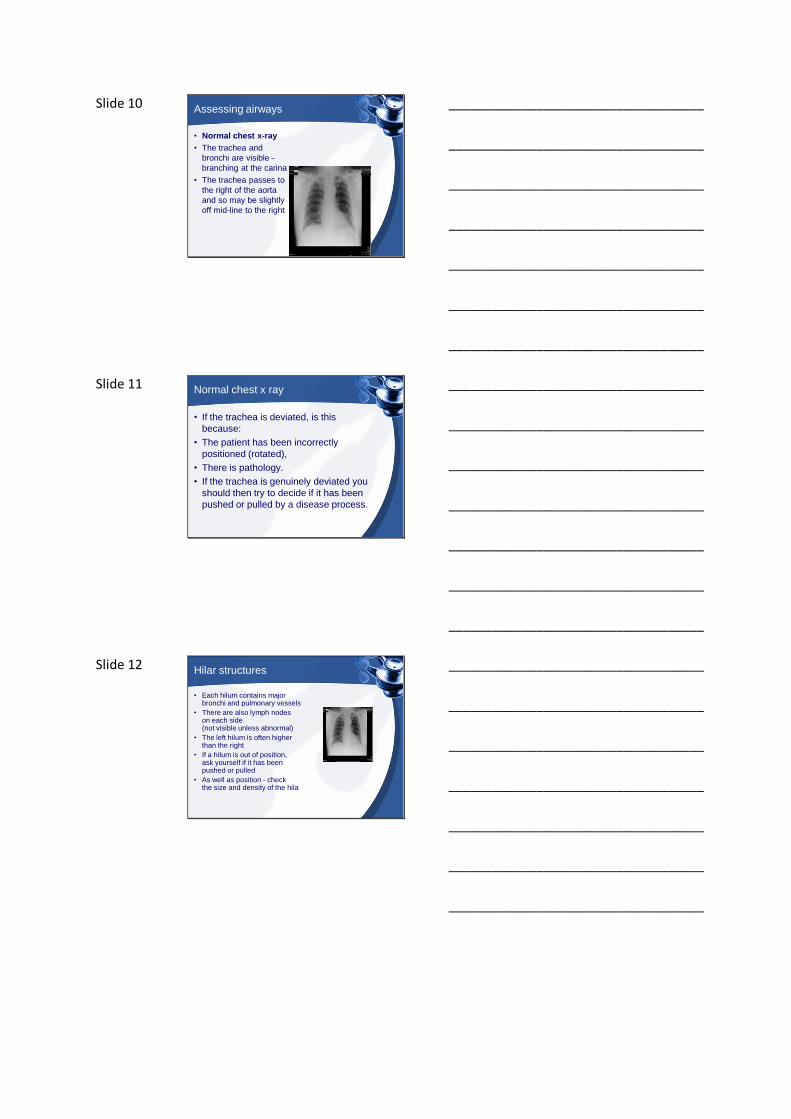
Slide 10 Assessing airways
• Normal chest x-ray
• The trachea and
bronchi are visible -
branching at the carina
• The trachea passes to
the right of the aorta
and so may be slightly
off mid-line to the right
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 11 Normal chest x ray
• If the trachea is deviated, is this
because:
• The patient has been incorrectly
positioned (rotated),
• There is pathology.
• If the trachea is genuinely deviated you
should then try to decide if it has been
pushed or pulled by a disease process.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 12 Hilar structures
• Each hilum contains major bronchi and pulmonary vessels
• There are also lymph nodes on each side (not visible unless abnormal)
• The left hilum is often higher than the right
• If a hilum is out of position, ask yourself if it has been pushed or pulled
• As well as position - check the size and density of the hila
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 13 Pleura & pleural spaces
• The pleura and pleural spaces are only visible when abnormal
• Lung markings should reach the thoracic wall
• Trace round the entire edge of the lung where pleural abnormalities are more readily seen
• Start and end at the hila
• Is there pleural thickening?
• Is there a pneumothorax? The lung markings should be visible to the chest wall
• Is there an effusion? The costophrenic angles and hemidiaphragms should be well defined
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 14 Chest X ray anatomy
• The left lung has two lobes
and the right has three
• Each lobe has its own
pleural covering
• The horizontal fissure
(right) is often seen on a
normal frontal view
• The oblique fissures are
often seen on a normal
lateral view
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 15 Surface anatomy R Lung
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 16 Costophrenic angles
• The costophrenic
angles are limited
views of the
costophrenic recess
• On a frontal view the
costophrenic angles
should be sharp
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 17 Diaphragm
• The hemidiaphragms are domed structures
• Each hemidiaphragm should be well defined
• The left hemidiaphragm should be visible behind the heart
• The hemidiaphragm contours do not represent the lowest part of the lungs
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 18 Cardiac assessment
• The heart size is
assessed as the
cardiothoracic ratio
(CTR)
• A CTR of >50% is
abnormal - PA view only
• The left hemidiaphragm
should be visible behind
the heart
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 19 Soft tissue
• Assess the soft tissues on every chest x-ray
• Thick soft tissue may obscure underlying structures
• Black within soft tissue may represent gas
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 20 Bones
• Assess the bones on every chest x-ray
• Check for abnormalities of single bones
and for diffuse bone disease
• The bones are helpful in assessing the
quality of the chest x-ray
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 21 Clavicles, spinous processes and ribs
• Clavicles are clearly seen on a chest x-ray.
• Spinous processes of the vertebrae (posterior structures) should lie midway between the medial ends of the clavicles (anterior structures).
• If the spinous processes are not central, the patient is rotated, that is, positioned obliquely to the x-ray beam.
• The anterior and posterior ends of the 5th rib are also shown.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 22 Ribs
• The anterior end of approximately 5-7 ribs should be visible above the diaphragm in the mid-clavicular line.
• Less than this indicates an incomplete breath in, and more than 7 ribs or flattening of the diaphragm, suggests lung hyper-expansion.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 23 Assessing the lungfields
• The lungs are assessed and described by dividing them into upper, middle and lower zones
• Refer to 'zones' not 'lobes'
• Compare left with right
• Compare an area of abnormality with the rest of the lung on the same side
• Note that the lower zones reach below the diaphragm. This is because the lungs pass behind the dome of the diaphragm into the posterior sulcus of each hemithorax.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 24 Densities
• Different tissues have
different density on X
ray
• Bones are white
• Lung tissue is 99% air
and is black
• Blood vessels give the
lacy pattern (1%)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 25 Interpretation of CXR
• Basic interpretation is EASY. They are
either:
– TOO WHITE
– TOO BLACK
– TOO LARGE
– IN THE WRONG PLACE
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 26 Technical details
• Check the patient name
• Date of X ray
• Whether its PA or AP
• Check Left/Right marker
• Check for Rotation
(clavicles not equally
positioned)
• Check
exposure/penetration
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 27 Consolidation
• Compare the left and right upper, middle and lower lung zones
• Decide which side is abnormal
• Compare an area of abnormality with the rest of the lung on the same side
• The whiter side is not always the abnormal side
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 28 Pleural disease- too white
• Pleura only
become visible
when diseased
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 29 Air fluid interface too white/black
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 30 Too black
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 31 Too large
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 32 Too large
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 33 In the wrong place
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 34 Pneumoperitoneum
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 35 Checklist 1
• Check patient name, position, technical quality.
• Soft tissue including breast, chest wall,
companion shadow.
• Review soft tissues and skeletal structures of
shoulder girdles and chest wall.
• Review abdomen for bowel gas, organ size,
abnormal calcifications, free air, etc.
• Review soft tissues and spine of neck.
• Review spine and rib cage: check alignment,
disc space narrowing, lytic or blastic regions,
etc.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 36 Checklist 2
• Review mediastinum:
– overall size and shape
– trachea: position
– margins: SVC, ascending aorta, right atrium, left subclavian artery, aortic arch, main pulmonary artery, left ventricle
– lines and stripes: paratracheal, paraspinal, paraesophageal (azygoesophageal), paraaortic
– retrosternal clear space
• Review hila:
– normal relationships
– size
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 37 Checklist 3
• Review lungs and pleura:
– compare lung sizes
– evaluate pulmonary vascular pattern: compare upper to lower lobe, right to left, normal tapering to periphery
– pulmonary parenchyma
– pleural surfaces
• fissures - major and minor - if seen
• compare hemidiaphragms
• follow pleura around rib cage
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 38 Examples 1
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 39 Examples 2
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 40 Examples 3
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 41 Examples 4
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 42 Examples 6
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 43 Examples 7
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 44 Example 8
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 45 Example 9
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 46 Example 10
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 47 Example 11
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 48 References
• Corne, D, J, Carroll M, Brown I, Delaney D (2002) Chest X ray Made Easy (2nd ed) Edinburgh Churchill Livingstone
• Longmore, M, Wilkinson, I, Torok, E (2001) Oxford Hnadbook of Clinical Medicine Oxford Oxford University Press.
• Medscape http://emedicine.medscape.com/pulmonology[Accessed 31/3/2010]
• McCance KL, Heuther, SE. (2006). Pathophysiology-The biologic basis for disease in adults and children. St Louis. Elsevier-Mosby
• Parson PE Heffner JE. (2002) Pulmonary/Respiratory Therapy Secrets (2nd Ed.) Philadelphia. Hanley & Belfus
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________