Embed Size (px)
Citation preview

Carlo Vancheri
Centro Riferimento Regionale Malattie Rare del Polmone
Università di Catania
Le nuove terapie della UIP

Quanti sono i pazienti con IPF?
• In Europa ci sono tra 80.000 e 120.000pazienti con IPF
• Ogni anno si ammalano di IPF circa 35.000cittadini europei
• La malattia è lievemente più frequente nelsesso maschile
• L’IPF colpisce soggetti adulti con un piccomassimo intorno ai 65 anni
1. Meltzer EB and Noble PW. Orphanet J Rare Dis 2008;3:822.
2. Hodgson U et al. Thorax 2002;57:338342.
3. Coultas DB et al. Am J Respir Crit Care Med 1994;150:967997.
Orphanet 2010; www.orphanet.net; Eurostat News Release. 110/2010

Incidenza IPF (solo UIP) in ITALIA
Abitanti = 60.000.000
Pazienti con IPF 4.800-9.200

Popolazione residente in Sicilia = 5.042.781 abitanti
Seguendo il modello di calcolo proposto
da Raghu negli USA, si stima che
in Siciliadovrebbero esserci
da 400 a 800casi di IPF ogni
anno !!!
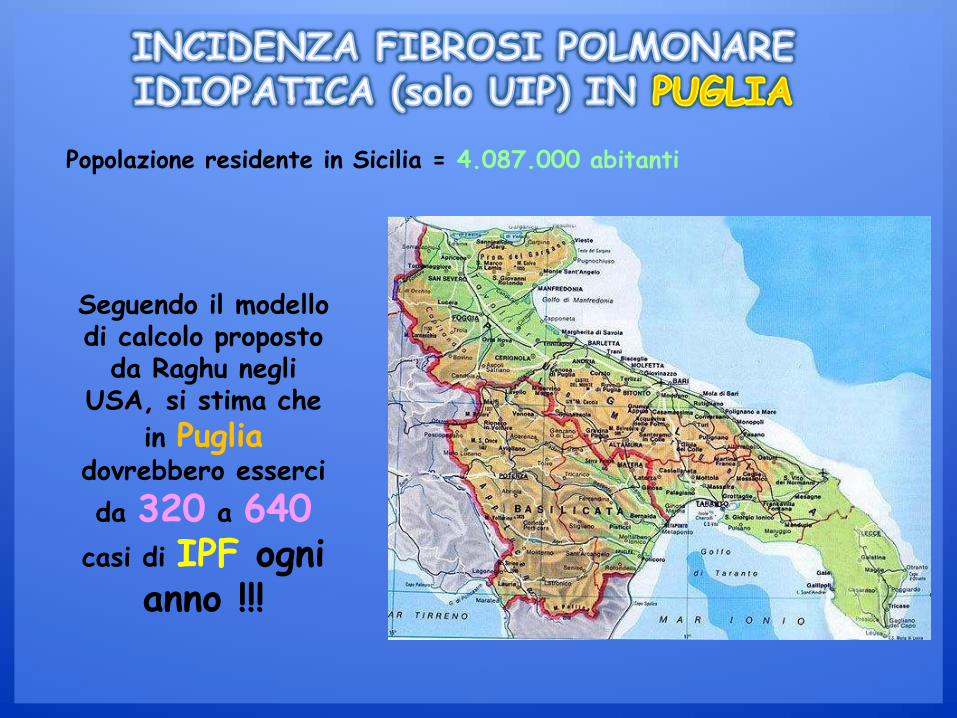
Popolazione residente in Sicilia = 4.087.000 abitanti
Seguendo il modello di calcolo proposto
da Raghu negli USA, si stima che
in Pugliadovrebbero esserci
da 320 a 640casi di IPF ogni
anno !!!

•Modified from: American Thoracic Society/European Respiratory Society. Am J Respir Crit Care Med 2002;165:277304;•Ryerson CJ and Collard HR. Curr Opin Pulm Med 2013;19:453459. PRC-2184
Interstitial Lung Disease (ILD)
ILD of known causes
(e.g. drugs, collagen vascular disease, exposures, genetic)
Idiopathic interstitial pneumonias (IIPs)
IPF: idiopathic pulmonary
fibrosis
Other IIPs
NSIP: non-specific interstitial pneumonia
RB-ILD: respiratory bronchiolitis interstitial
lung disease
AIP: acute interstitial pneumonia
DIP: desquamative interstitial pneumonia
COP: cryptogenic organising pneumonia
LIP: lymphocytic interstitial pneumonia
AFOP: acute fibrinous and organising
pneumonia
Granulomatous ILDs
(e.g. sarcoidosis, fungal, mycobacterial)
Unique entities
(e.g. PAP, EG and EP, LAM, capillaritis, idiopathic PPFE,
unclassifiable ILD)
55%
25%
<2%
5% <1%
10
15
%
rare

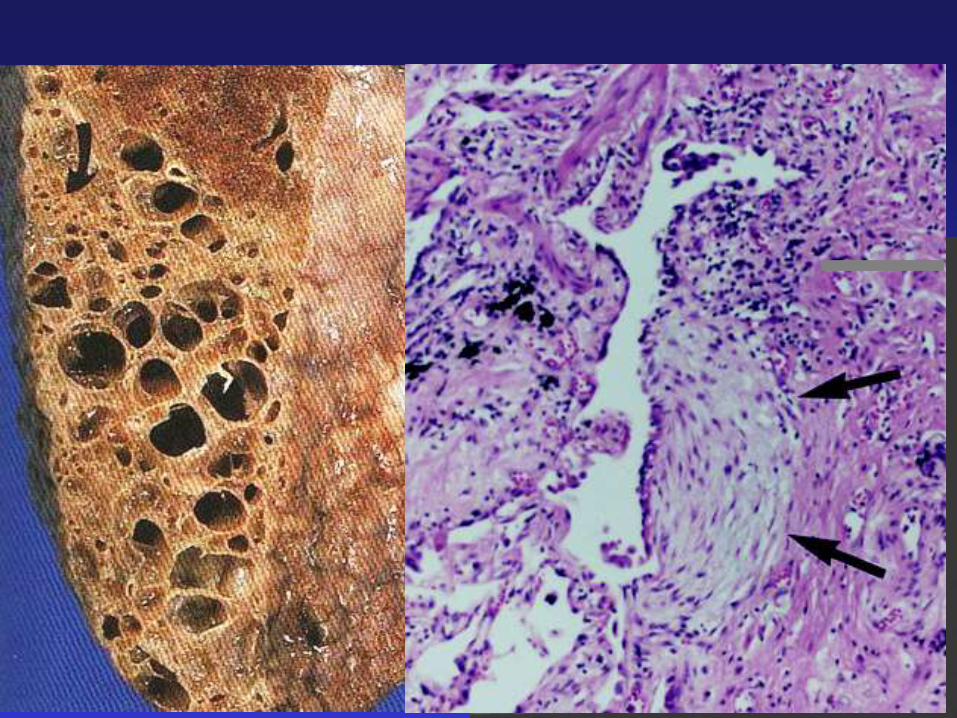
UIP

fibroblasti
spazio alveolare
pneumociti tipo I
pneumociti tipo II
macrofagi alveolari
membrana basale
cellule endoteliali
surfattante
interstizio
globuli rossi

fibroblasti

Idiopathic Pulmonary Fibrosis
Normal Lung Usual Interstitial Pneumonia


IL-1, TNF-
IL-8, RANTES
IL-5, GM-CSF
APC T-Linfocita
MHC II TCR
CD28
CD40
CD40L
Noxa patogena B7.2
B7.1
Proteasis, oxidants
Damage and repair
STEROIDS
IMMUNOSUPPRESSORS

PANTHER 2012 Interim Results
• Triple therapy has no benefit for FVC
• Increased risk of death
Primary Triple Therapy Placebo P-value
FVC (liters) -0.24 -0.23 0.85
Raghu G, et al. N Engl J Med. 2012;366:1968-1977.
Pro
bab
ility
Time to DeathKaplan–Meier Analysis
Weeks Since Randomization
HR 9.26 (95% CI 1.16-74.1)
P = 0.01
ATS 2011
2011-2013 2014Pre-2011

Genetic background
ACTIVATION OF FIBROBLASTS AND FIBROSIS
smoking
Alveolar cells
Altered response to damageloss of epithelial integrity Apoptosis, ER stress
Aging
The importance of a proper substrate
Come si è arrivati alla terapia dell’IPF con Pirfenidone?
PRC-2063

Possible Mechanisms of Pirfenidone Action
Hilberg O, et al. Clin Respir J. 2012;6:131-143.
TNF-αIL-6
Pirfenidone
TGF-βIL-6
MMPsCollagenases
ROIs
Collagen
• Antifibrotic
• Molecular target unclear
• Active in several animal models of fibrosis (lung,
liver, kidney)

ASCEND 2014
ATS 2011
2011-2013Pre-2011 2014

Pirfenidone Reduces Loss of FVC
<0.000001King TE, et al. N Engl J Med. 2014;370(22):2083-2092.
235 ml
428 ml
Rank ANCOVA P-value < 0.00001 at each indicated time point
Me
an C
han
ge (
ml)
Week

Riduzione del declino funzionale e poi?
PRC-2063

Pirfenidone Increased Progression-Free Survival*
King TE, et al. N Engl J Med. 2014;370(22):2083-2092.
*Progression is first occurrence of death, 10% ↓ FVC, or 50 m ↓ 6MWD
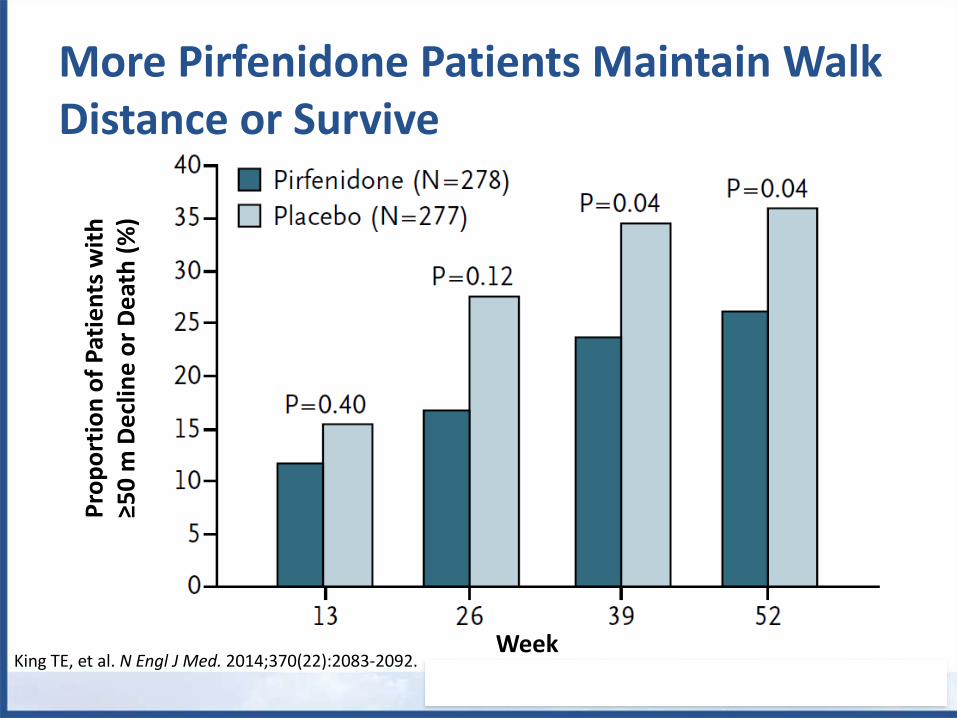
More Pirfenidone Patients Maintain Walk Distance or Survive
King TE, et al. N Engl J Med. 2014;370(22):2083-2092.
Pro
po
rtio
n o
f P
atie
nts
wit
h
≥50
m D
ecl
ine
or
De
ath
(%
)
Week

0 3 6 9 12
Month
0.0
2.5
5.0
7.5
De
ath
s (
%)
Placebo (N=624)
Pirfenidone 2403 mg/d (N=623)
Patients at Risk, n
Pirfenidone
Placebo
623 618 609 596 509
624 619 603 586 490
10.0
HR 0.52 (95% CI 0.31, 0.87)*
P=0.011†
* Cox proportional hazards model)
† Log-rank test
Pooled All-cause Mortality (Week 52): Treatment
group curves diverge early and continue separating
throughout the study period
25
MRC-2161King TE et al. N Engl J Med 2014 May 18. doi:10.1056/NEJMoa1402582

Quando dobbiamo iniziare a trattare con pirfenidone?
PRC-2063
“Wait and see or early treatment?”


Roche Medical Affairs 29
Confidential for internal use only
Natural history of disease progressionPooled placebo population
6MWD, 6-minute walk distance; FVC, forced vital capacity; HR, hazard ratio;
UCSD SOBQ, University of California—San Diego Shortness of Breath Questionnaire.
FVC < 80%
Event/TotalFVC ≥ 80%
Event/Total
FVC decline ≥ 10%
or death
99/450 (22.0%) 30/168 (17.9%)
6MWD decline ≥ 50 m
or death150/450 (33.3%) 36/168 (21.4%)
UCSD total score change
≥ 20 points or death
141/451 (31.3%) 22/169 (13.0%)
0.1 1 10
↑ Risk for FVC ≥ 80% ↑ Risk for FVC < 80%
2.68 (1.71-4.21) < 0.0001
1.67 (1.16-2.41) 0.0049
1.28 (0.85-1.92) 0.2403
HR (95% CI)
Between-
Subgroup
P Value
The risk of disease progression (especially FVC decline ≥ 10% or death) is comparable
in patients with FVC above versus below 80%

5-YEAR SURVIVAL OF IPF AND CANCER
Leukaemia
IPF
Lung
Pancreas
Skin
Thyroid
Bladder
Prostate
Lymphoma
Uterus
Kidney
Colon
Breast
1008060402005-year survival (%)
Modified by Richeldi L.

Risk factors for IPF
Susceptible individuals
Environmental and/or
occupational factors?
Cigarette smoking?
Viral infection? (Epstein-Barr)
Chronic injury? (GERD and
tractional injury)

Risk factors for cancer
Susceptible individuals
Environmental and/or
occupational factors?
Cigarette smoking?
Viral infection? (Epstein-Barr)
Chronic injury?
(wound that doesn’t heal)

• Tumour suppressor gene mutations
• Telomere shortening
Genetic alterations
• Hypermethylation of the Thy-1 promoter regionEpigenetic alterations
• Myofibroblasts recruitment and differentiation
• Myofibroblasts infiltrative ability
• Expression invasive molecules
Tissue invasion
• Self-sufficiency in growth signals• Insensitivity to growth inhibitory signals• Evasion of apoptosis• Altered cell-to-cell communications
Uncontrolled proliferation
• Activation Wnt/β-catenin pathway
• Activation PI3K/PTEN-AKT pathway
• Activation of tyrosine kinases
Signal transduction
pathways
• P53, FHIT, microsatellite instability, microRNA alterations, MUC5B
• (Loss of Thy-1 protein) invasive behaviour of fibroblasts
• Myofibroblasts behaviour• Invasive molecules
(HSP-27, laminin, fascin)
• Autocrine TGF-β production• Connexin 43 reductio
• Proliferation, differentiation, activation
Common pathways in IPF and cancer
Vancheri and Du Bois ERJ 2013

Activation of Wnt/β-catenin pathway
Activation of PI3K/AKT pathway
Activation of tyrosine kinase pathway
Common pathways in IPF and cancer
Signal transduction pathways

Overall survivalPatients with adenocarcinoma histology
100
80
60
40
20
0
322 263 203 163 131 96 72 46 25 10
336 269 184 139 101 73 55 33 15 7
Pro
bab
ilit
y o
f su
rviv
al
(%)
Nintedanib + docetaxel
Placebo + docetaxel
Median, mo 12.6 10.3
HR (95% CI) 0.83 (0.70 to 0.99)
p-value 0.0359
52.7%
44.7% 25.7%
19.1%
No. at risk
Nintedanib
Placebo
0 4 8 12 16 20 24 28 32 36
Time (months)
Presented at ASCO 2013
Effect of the kinase inhibitor nintedanib on NSCLC

Various tyrosine kinases play key roles in the pathologic activation of fibroblasts during
fibrogenesis, rendering them attractive molecular targets in the treatment of fibrosis
FIBROGENESIS

Rationale for investigating nintedanib (BIBF 1120) in IPF
• PDGF is implicated in the fibrotic process1
• Liver fibrosis was decreased in FGF-1/FGF-2 deficient mice2
• Experimental evidence in rats suggests that inhibition of VEGFR may reduce fibrosis3
1. Selman M et al. Am J Respir Cell Mol Biol 20032. Yu C et al. Am J Pathol 20033. Hamada N et al. J Immunol 2005
PDGF
Collagen deposition
FIBROSIS
Alveolar epithelial cells
Myofibroblast differentiation
FGF VEGF
4. Hilberg F et al. Cancer Res 20085. Chaudhary NI et al. Eur Respir J 2007
• Nintedanib is a kinase inhibitor that targets PDGF, FGF and VEGF receptors4
• Nintedanib prevented development of lung fibrosis in a bleomycin rat model5
• Nintedanib reduces TGF-β-induced fibroblast to myofibroblast transformation5
N Engl J Med 2011

INPULSIS 2014ATS
20112011-2013Pre-2011 2014

PRIMARY EFFICACY ENDPOINT IN INPULSIS-1
125.3 mL/year
(95% CI: 77.7, 172.8)
p<0.0001
Nintedanib 150 mg bid (n=309)
Placebo (n=204)
Ad
juste
d a
nnua
l ra
te (
SE
) o
f d
eclin
ein
FV
C (
mL
/ye
ar)
2 4 6 12 24 36 52
Week
No. of patients
Nintedanib 303 301 298 292 284 274 250
Placebo 202 198 200 194 192 187 165
0
Placebo
Nintedanib 150 mg bid
Me
an
(S
E)
ob
se
rve
d c
ha
nge
fro
m b
ase
line in F
VC
(m
L)

TIME TO FIRST ACUTE EXACERBATION (INVESTIGATOR-REPORTED) IN POOLED DATA
Nintedanib 150 mg bid
(n=638)
Placebo (n=423)
Patients with ≥1 acute exacerbation, n
(%)
31 (4.9) 32 (7.6)
Placebo
Nintedanib 150 mg bid
HR 0.64
(95% CI; 0.39, 1.05)
p=0.0823

EFFECT OF NINTEDANIB ON PATIENTS WITH BASELINE FVC>80%
Pooled INPULSIS® data; post hoc subgroup analysis of patients with baseline FVC >
80% versus ≤ 80% predicted
To assess the impact of baseline lung function impairment on the effect of nintedanib using an FVC threshold relevant for treatment reimbursement in several countries
Annual rate of decline in FVC similar in patients in both subgroups. Nintedanib slowed the decline in lung function independent of degree of lung function impairment at baseline
Most exacerbations reported in patients with baseline FVC ≤ 80% predicted
Time to first acute exacerbation and change in SGRQ total score was not significantly different between the subgroups by baseline FVC % predicted and was consistent with the results in the overall pooled population.
FVC = forced vital capacity; SGRQ = St George's Respiratory Questionnaire.Maher T, Oral presentation, Session 462, ERS 2015.
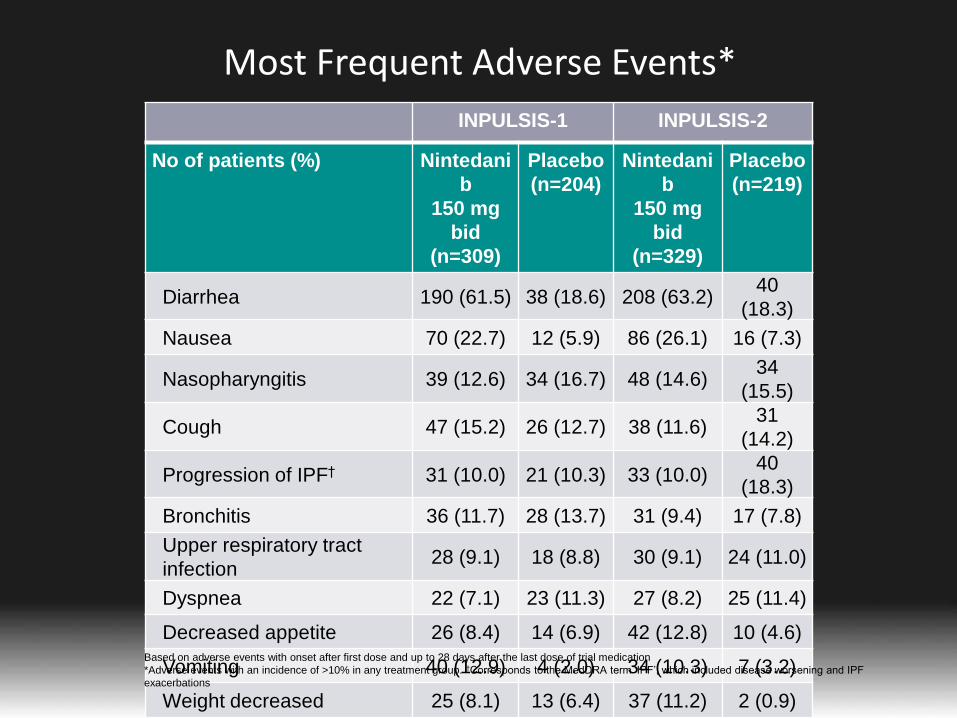
Most Frequent Adverse Events*
INPULSIS-1 INPULSIS-2
No of patients (%) Nintedani
b
150 mg
bid
(n=309)
Placebo
(n=204)
Nintedani
b
150 mg
bid
(n=329)
Placebo
(n=219)
Diarrhea 190 (61.5) 38 (18.6) 208 (63.2)40
(18.3)
Nausea 70 (22.7) 12 (5.9) 86 (26.1) 16 (7.3)
Nasopharyngitis 39 (12.6) 34 (16.7) 48 (14.6)34
(15.5)
Cough 47 (15.2) 26 (12.7) 38 (11.6)31
(14.2)
Progression of IPF† 31 (10.0) 21 (10.3) 33 (10.0)40
(18.3)
Bronchitis 36 (11.7) 28 (13.7) 31 (9.4) 17 (7.8)
Upper respiratory tract
infection28 (9.1) 18 (8.8) 30 (9.1) 24 (11.0)
Dyspnea 22 (7.1) 23 (11.3) 27 (8.2) 25 (11.4)
Decreased appetite 26 (8.4) 14 (6.9) 42 (12.8) 10 (4.6)
Vomiting 40 (12.9) 4 (2.0) 34 (10.3) 7 (3.2)
Weight decreased 25 (8.1) 13 (6.4) 37 (11.2) 2 (0.9)
Based on adverse events with onset after first dose and up to 28 days after the last dose of trial medication
*Adverse events with an incidence of >10% in any treatment group. †Corresponds to the MedDRA term ‘IPF’, which included disease worsening and IPF
exacerbations

ASCEND Study: GI and skin-related events were more commonin the pirfenidone group
Occurring in ≥10% of patients in either treatment group †Coded to preferred terms in the Medical Dictionary for Regulatory Activities, version 11.0
Patients (%)
Pirfenidone
(N=278)
Placebo
(N=277)
Cough 25.2 29.6
Nausea 36.0 13.4
Headache 25.9 23.1
Diarrhea 22.3 21.7
Upper Respiratory Tract Infection 21.9 20.2
Fatigue 20.9 17.3
Rash 28.1 8.7
Dyspnea 14.7 17.7
Dizziness 17.6 13.0
Idiopathic pulmonary fibrosis 9.4 18.1
Bronchitis 14.0 13.0
Constipation 11.5 13.7
Back pain 10.8 13.4
Dyspepsia 17.6 6.1
Nasopharyngitis 11.9 10.8
Anorexia 15.8 6.5
Vomiting 12.9 8.7
Weight decreased 12.6 7.9
Gastroesophageal reflux 11.9 6.5
Insomnia 11.2 6.5
King TE et al. N Engl J Med 2014 May 18. doi:10.1056/NEJMoa1402582

Our real life experience on 220 patients treated
with pirfenidone and 40 with nintedanib

35%
65%no ADR
ADR
Adverse drug reactions (ADR) related to pirfenidone treatment
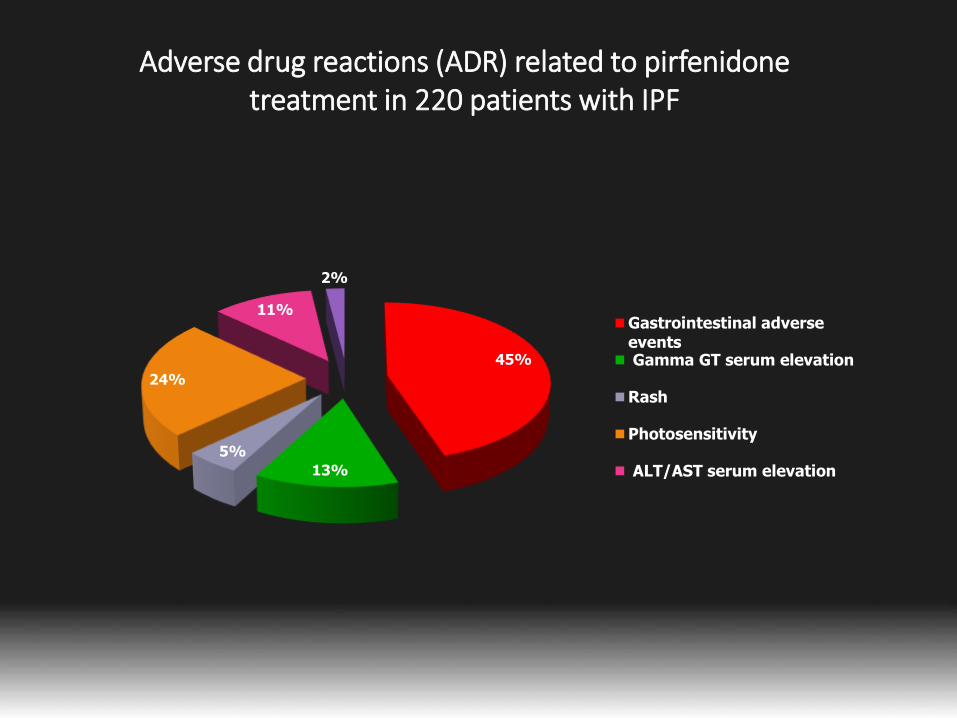
45%
13%
5%
24%
11%
2%
Gastrointestinal adverseevents Gamma GT serum elevation
Rash
Photosensitivity
ALT/AST serum elevation
Adverse drug reactions (ADR) related to pirfenidone treatment in 220 patients with IPF

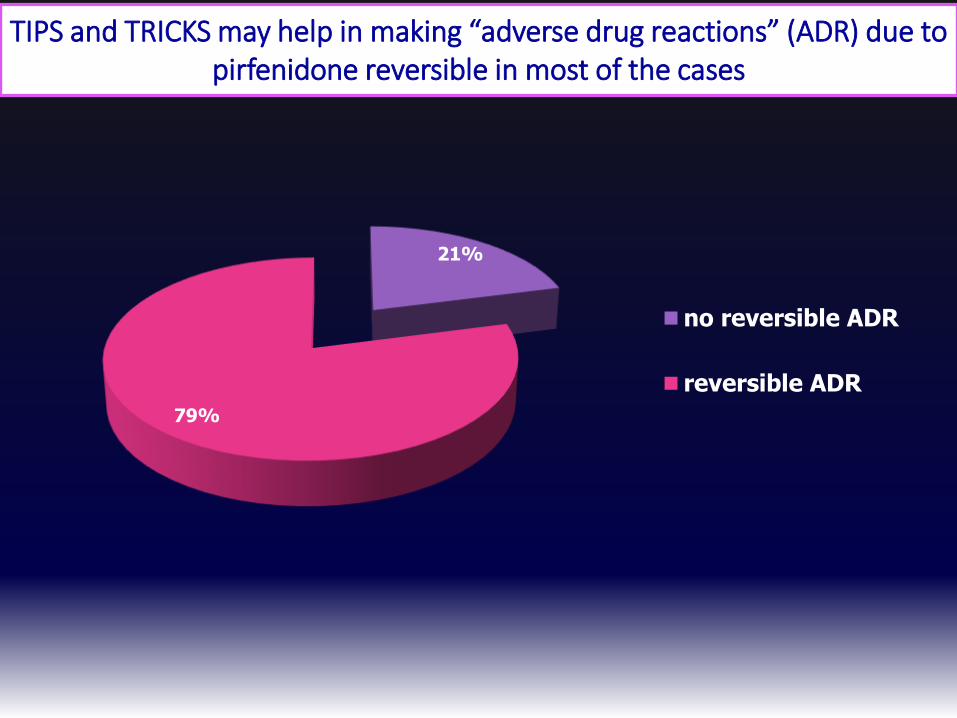
21%
79%
no reversible ADR
reversible ADR
TIPS and TRICKS may help in making “adverse drug reactions” (ADR) due to pirfenidone reversible in most of the cases
In conclusione le attuali terapie consentono di:
1.Ridurre il declino funzionale dei pazienti con IPF
2.Ridurre la mortalità
3.Ridurre le esacerbazioni?
4.Trattare i pazienti fin dalle fasi iniziali
5.Trattare con un buon profilo di sicurezza
PRC-2063






![Original Article Artigo Original phonological development ... · epenthesis (e.g..: bruxa – [bu’ɾuʃa]), merger (e.g..: cravo – [´davu]), compensatory stretching (e.g.: planta](https://img.dokumen.tips/doc/110x75/5c5d165109d3f2a1498c572b/original-article-artigo-original-phonological-development-epenthesis-eg.jpg)