Embed Size (px)
Citation preview

Lauren Cobbs, M.D.Medical Director, Standardized Patient Program
Assistant Professor, Department of Humanities in MedicineTexas A & M Health Science Center College of Medicine
Elizabeth H. Sinz, M.D.Director, PennState Simulation Development & Cognitive Science Laboratory
Professor of Anesthesiology & NeurosurgeryImmediate Past-president, Society for Simulation in Healthcare
Robin Wootten, M.B.A., R.N.Director, Russell D. and Mary B. Shelden Clinical Simulation Center and
Standardized Patient ProgramUniversity of Missouri School of Medicine
Board of Directors, Society for Simulation in Healthcare
2008 ASPE PanelSponsored by:

Combining Standardized Patients with Simulators for Teaching and Assessment
Lisa Sinz, M.D.

“To me, the three greatest joys in medicine are:
1. learning how to save a life
2. saving a life
3. teaching others how to save lives
You get to do all three.What a wonderful thing.”
-LTC Christian Macedonia, M.D.
We get to teach important things to people who really want to learn!

Benefit of Simulators and Standardized Patients
• Student can practice key skills in a safe environment
• Teacher can break down the task into components
• Student can receive immediate feedback
• Teacher can create the same situation to assess performance repeatedly

Standardized Patients vs. Simulators
• Standardized patients great for teaching and assessing:– Communication skills– Exploration of emotional component– Examination skills– Sensitivity
• Not great for:– Technical skills– Certain pathology– Treatment

Simulators vs. Standardized Patients• Simulators great for teaching and assessing:
– Procedural skills– Treatment/interventions– Invasive monitoring
• Not great for:– 2-way communication skills– Treating the patient as a person– Representing family/staff/other team members

Solution: Select the best components of each
1. Determine skills to be taught or assessed
2. Deconstruct task into components
3. Determine best tools to meet goals
4. Build on previously acquired knowledge, skills, and experience
5. Separate summative and formative sessions

Roger Kneebone on teaching Procedural Skills
• Need– Technical skills– Communication– Professionalism
• Must be integrated but are often taught separately
• Conditions for holistic professional practice

Example:Suturing
Roger Kneebone

Roger Kneebone

Roger Kneebone

Example: Foley Catheter Insertion• Provide an explanation of what they are going to learn-
reading, video, lecture, etc.• Teaching points: Basic “mechanics” of placing a Foley
catheter, Sterile technique for this procedure, Different types of catheter

Practice placement of catheter with a task trainer
• Psychomotor skills, sterile technique, experience with the equipment and procedure

Practice catheter placement with a standardized patient
Student should explain:
• steps of procedure• reason for
procedure• treat patient
respectfully• maintain patient’s
privacy

Finding the level of the student
• Initial step of simply placing the catheter occurs before any patient encounters
• Students observe and possibly perform procedure in patients
• Return to lab for more complex encounters
Advanced Cases:• Difficult patient-dementia, pain, refuses
procedure– Teaching point: managing the situation and the procedure
concurrently
• Difficult procedure-catheter will not pass– Teaching points: Call for additional expertise, procedural
complications
• Difficult situation-trauma bay, new admission– Teaching points: Multitasking, assigning responsibility,
triage

Crisis Management
• Focus on medical management
• Crisis resource management skills are reinforced
• Increased complexity
• Videotaped for review and reflection– “What will you do differently next time?”

Trauma and Awareness: ED
• Patient arrives in trauma bay following motorcycle accident
• Initially conscious, he deteriorates due to a pneumothorax and requires a chest tube and intubation
Case Report-Singh, Shashank, Sinz, Elizabeth, Henry, Jody, Murray, Bosseau: Trauma and Awareness. Simulation in Healthcare 1(4):240-245, Winter 2006

Trauma and Awareness: OR
• Patient arrives in OR for semi-urgent procedure
• During case, conflict occurs when patient deteriorates

Trauma and Awareness-Clinic• Patient returns to follow-up clinic complaining
of “awareness” with symptoms of post-traumatic stress disorder
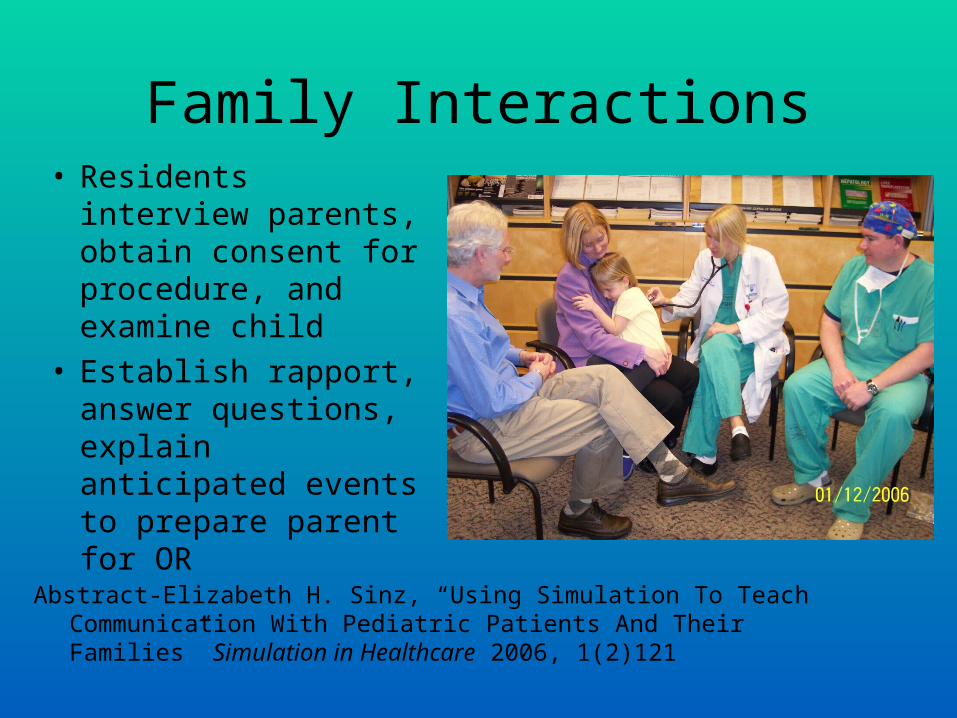
Family Interactions• Residents interview
parents, obtain consent for procedure, and examine child
• Establish rapport, answer questions, explain anticipated events to prepare parent for OR
Abstract-Elizabeth H. Sinz, “Using Simulation To Teach Communication With Pediatric Patients And Their Families” Simulation in Healthcare 2006, 1(2)121
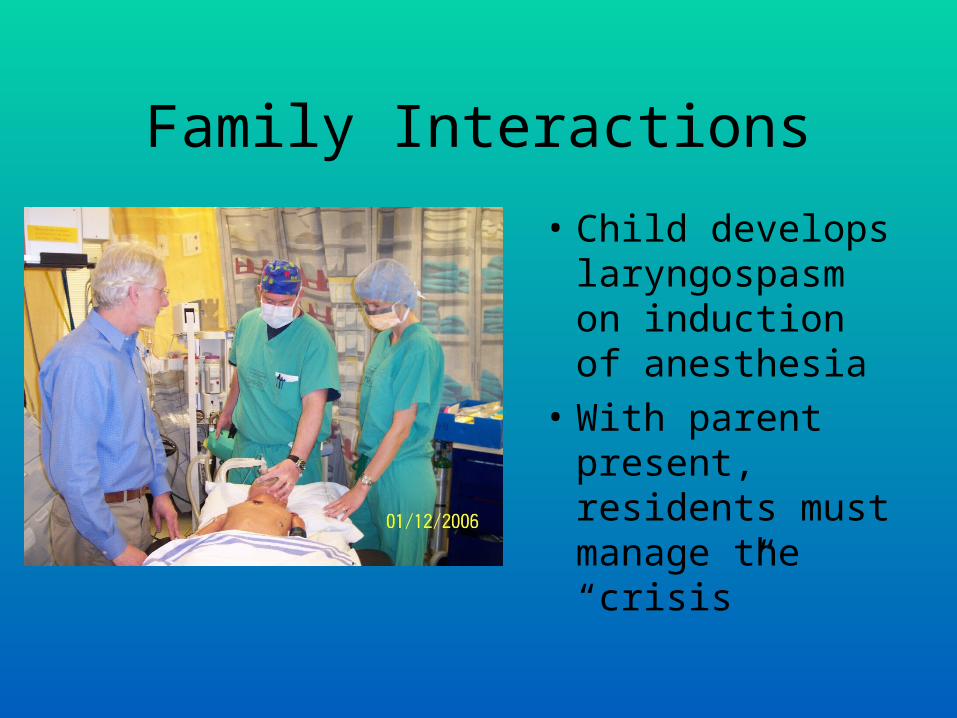
Family Interactions
• Child develops laryngospasm on induction of anesthesia
• With parent present, residents must manage the “crisis”

Feedback that encourages self-reflection
• Videotape is frequently used
• Students are asked how they thought the scenario went
• Leading questions probe the students’ thought processes

Assessment using Simulation?
• Against – Simulator technology not good enough– Wasteful-adult learners need formative
education more than educators need assessment
• For– Already using Standardized Patients for
assessment– Procedural Skills vs. Team training

Assessment: Stroke Management• Manikin can provide physiologic signs that
can be treated
• SP can provide history, emotion
• “Brain Attack” invokes a standardized, consensus-based approach that can be scored
Doug Bower, Miland Kothari, Jansie Prozesky, Lisa Sinz

Immediate Diagnostic Studies: Evaluation of a Patient With Suspected
Acute Ischemic Stroke-AHA• All patients
– Noncontrast brain CT or brain MRI – Complete blood count, incl. plt count, PT, PTT– Serum electrolytes/renal function tests – Markers of cardiac ischemia – EKG – Blood glucose – Oxygen saturation– Blood pressure

AssessmentPatient Care• Raise head of bed • Measure/Treat Blood Glucose• Measure/Treat Hypertension• Measure/Treat HypoxemiaProfessionalism• Obtain pertinent history• Explain diagnosis & next stepsSystems• Order head CT• Alert stroke team

Systems Assessment:Acute Myocardial Infarction
• Example: Use of Standardized Patient and Simulator to evaluate “door-to-drug” time for acute myocardial infarction
• Standardized patient presents
to ED with complaint of chest pain– History obtained– Explanation given

Systems Assessment
• Patient deteriorates, requires intubation– Patient now represented by manikin– Supportive therapy initiated
• Manikin taken to cardiac catheterization laboratory
Process involving many
individuals and several
departments

Systems Assessment:Process evaluation
• Standardized patient provided practice and assessment for triage, communication, and staff-patient interaction
• Simulator allowed staff to practice and obtain feedback on crisis management, changing conditions, and medical management
• Improvements to the “system” were made based on the experience of the simulation

Conclusion
• Standardized patients and simulators have converged to create broader applications for simulation than ever before
• Each enhances the effectiveness and scope of the other
• Simulation centers will increasingly incorporate all modes of simulation

Lauren Cobbs, M.D.
Simulation of Ethical, Cultural, and Professionalism Issues
In Health Care

Why try?
Why are the traditional methods for teaching health care ethics and professionalism in medicine “not enough”?

A Brief Tour of Ethics Education in Medicine
• Apprenticeship model of medical education
• Teaching methods have remained relatively unchanged over the years
• “Poor progression of [ethical] concepts. Students do well in the first years but unable to deepen their learning [due to] limited teaching capacity”1
1Mattick, K., Bligh, J. J Med Ethics 2006; 32:181-185

When it comes to ethics and professionalism education
Are we doing what we think we were doing?
How well are we in fact doing it?

The ACGME Competencies Issue
• Does simple exposure to medical ethics and professionalism = competency?
• ACGME Outcomes Project
– Patient care– Medical knowledge– Practice based learning and improvement– Interpersonal and communication skills– Professionalism – Systems based practice

Three Phase Professionalism Curriculum
• Identify specific learning objectives
– What are the expected professional behaviors?
– What exactly does role modeling and leadership as a health care professional entail?
– To whom are we role models?– What are the repercussions of not exhibiting
professional behaviors?

Three Phase Professionalism Curriculum
• Phase 1– Introduction to the foundational
principles of health care ethics
• Large group didactic/case discussion • Ensure each learner has exposure to same
basic level of knowledge in this content area

Three Phase Professionalism Curriculum
• Phase 2– Work in small groups with neutral facilitators in
discussion of paradigm cases
• Participants think through with colleagues how they would address specific professionalism challenges
• Mixture of different levels of clinical training/experience• Use of neutral discussion facilitator

Three Phase Professionalism Curriculum
• Phase 3– Health care provider placed in simulated
clinical situations• Expected to demonstrate how they resolve ethical
dilemmas, respond to professionalism challenges, and/or address cultural/diversity related issues
– Health care provider can observably (and ideally competently) integrate all aspects of their clinical training

What’s the point?
• Using a reflective learning model and the debriefing process, participants should be better able to:
– Understand– Respond to– Justify
The mental models used in their medical decision making and patient care, and in their overall role as medical professionals

Jehovah’s Witness Scenario
Mrs. Right has been chronically taking OTC NSAIDS due to a long h/o severe osteoarthritis.
She presented to her PCP’s office for a knee arthrocentesis and while having the procedure c/o abdominal pain. She then vomited up coffee ground emesis and some frank blood.
Mrs. Right was admitted to the hospital for further management.

Jehovah’s Witness Scenario
• Scenario objectives:– Medical decision making
• Utilize appropriate criteria for surrogate decision making for an incapacitated patient
• Awareness of criteria for clinical decision making in life threatening situations when patient wishes are unknown
• Recognize Jehovah Witness’ beliefs regarding receiving blood products
– Technical skills
• Management of acute blood loss• Management of potentially lethal arrhythmias

What do I get for my time and effort?
What can incorporating hybrid simulations into a medical education curriculum for the purpose of professionalism training realistically achieve?

What does hybrid simulation add to medical ethics education?
• Builds upon already acquired knowledge • Challenges and exposes areas where there may
be no or limited knowledge
– Push participants to become aware of a potential gap in their:
• Knowledge• Technical proficiency• Behavior or attitudes
Regarding a situation they are likely to face in their professional futures

What won’t I get for my time and effort?
What can’t hybrid simulations for ethics, professionalism, and cultural competence education achieve?

No “Ah Ha!” Moment
• Non-technical skills education is much harder for health care providers to immediately grasp
– Any differences in thinking, way of approaching medical decision making, or general attitudes toward patient care is likely not recognized until they are challenged to use those skills at some later point
– Regardless of the teaching method, issues related to ethics, professionalism and cultural competency generally do not have clearly defined “answers”
• To say, “If you approach it this way every time you will be OK” does
not exist

Using Simulation to Enhance Resident Learning of
Ethics, Professionalism and Cultural AwarenessL. Cobbs, M.D., J. Song, Ph.D., M. Howell, M.Ed., C. Mirkes, D.O.
• 53 IM residents participated in 3 phased curriculum study 8/07 – 12/07
• Anonymous 12 question self assessment survey was administered following phases 2 and 3

Using Simulation to Enhance Resident Learning of
Ethics, Professionalism and Cultural AwarenessL. Cobbs, M.D., J. Song, Ph.D., M. Howell, M.Ed., C. Mirkes, D.O.
• Residents self assessed confidence level (specifically defined as “your belief in your ability to perform the described task”) in their ability to:– Identify, make a decision, justify their decision for a patient
who:• Will require difficult airway management• Is at severe medical risk (i.e. at risk for imminent death)
– Identify, make a decision, justify their decision for resolving: • An ethical dilemma in the clinical management of a patient• A cultural/religious/ethnic value difference between the resident
and their patient
• Verbal anchors of no, low, some, good or strong confidence were used for rating purposes

Table 1ODDS RATIO ANALYSIS
Confidence level rating of “Good” or “Strong”
Make decision managing
difficult airway
PRE POST
Make decision managing patient at severe medical
risk
PRE POST
Make decision resolving
ethical dilemma
PRE POST
Make decision resolving
cultural/value difference
PRE POST
PGY 2 vs. PGY 1 8.38 9.44 29.71 10.31 7.08 6.25 3.25 15.99
PGY 3 vs. PGY 1 73.14 7.79 31.99 26.24 8.50 7.50 2.86 1.95

One way to look at this…
• The immediacy of the post simulation reflective learning process may provide residents with a more “realistic” snapshot of their abilities in certain clinical areas
– For some this =
– For others this = impetus for further self assessment/new learning in those areas that are perceived as being less than optimal or below expectation

…and my parting shot
Multidimensional simulation exercises which require full integration of medical management skills may help residents/residency programs obtain more accurate assessments of a resident’s overall clinical abilities
The strength of incorporating hybrid simulations into this area of medical education (and assessment) is as an enhanced way of addressing not only the technical, but the more elusive cognitive competencies of professionalism, ethical decision making and cultural awareness

Bridging the Gap
Utilizing a Community of Practice
Model to Enhance
Inter-Professional, Hybrid
Simulation
Robin Wootten, MBA, RN

Today’s Marketplace
• Fueled by knowledge
• Organizing it all is a challenge
• Technology is not enough
• Requires an effective knowledge strategy
• Limited resources
• Time is money

Communities of Practice
• Common interests and expertise
• Create, share and apply knowledge– Within and across boundaries
• Provide a concrete path toward creating a true knowledge organization
» Wegner, McDermott, Snyder –
“Cultivating Communities of Practice, 2002”

Social Learning Theorist:Dr. Etienne Wenger
• Activities of a Community of Practice– Problem solving
– Requests for information
– Seeking experience
– Re-using assets
– Coordination and synergy
– Discussing developments
– Documentation projects
– Visits
– Mapping knowledge and identifying gaps
http://www.ewenger.com/theory/index.htm

The power of The power of communitycommunity
Enabling emergence
Enabling emergence
Connecting people
Connecting people
Shar
ing
lead
ersh
ip
Shar
ing
lead
ersh
ip
Inviting participation
Inviting participation
Mod
elin
g a
spiri
t of i
nqui
ry
Mod
elin
g a
spiri
t of i
nqui
ry
Opening identities
Opening identities
Inspiring new meanings
Inspiring new meanings Building tru
st
Building trust
PersonalPersonal
EngagedEngaged
EmotionalEmotional
ChallengingChallenging
GratifyingGratifying
UnseenUnseen
Used with Permission, Wenger, 2007
Social Artists: The Work of Leadership

Gaining Leverage
• Drive overall simulation strategy– Including SP / Hybrid Encounters
• Generate new business opportunities
• Tie personal development to organizational goals
• Transfer Best Practices
• Recruit and Retain Top Talent

Mission StatementUniversity of Missouri
Simulation Community of Practice
• Train and evaluate health care practitioners to provide continuous, safe, effective patient-centered care from entry to exit using excellent communication and teamwork skills

What is possible?
• Joint Grants– Missouri Hospital Association grant for
mannequins• HRSA National Bioterrorism Hospital
Preparedness Program• Trailer for Outreach Hybrid Simulation
Experiences
– Technology Innovations Grant• Hybrid Crisis Simulation in Sim Center

Possibilities• Disaster Training
– NDLS Training Site Designation• ATLS
• BDLS
– Hybrid Simulation• Additional funding for participants and facility fees
Possibilities
• Service Learning– Nursing / Health Professions Students
– Theater Students• Participate as Standardized Patients• Play role in addition to mannequin
– Win – Win• Saves the center money• Inter-professional communication• Learning occurs for all participants

Possibilities
• Team Training– Monday Morning Code Blue Sessions
• Open to anyone interested– Staff, Faculty, Residents, Students
• Now being required by some departments– IM / Pediatric / Family Medicine Residents
– Students – RT, Medical, Nursing
– SP plays family member• Breaking Bad News After Code• Disclosure

Possibilities• Video Policy and Procedure Manuals
• Digital Library of Procedures– Rural Track Students
• CME Opportunities
• Joint Department Endeavors– Law School – Vet School– Journalism
• Video Conferencing of Events


Hershey Learning Center


Questions? Comments? Contact Information:
Elizabeth Sinz, M.D.
Lauren Cobbs, M.D.
Robin Wootten, M.B.A., R.N





![William Allan Kritsonis, PhD - PhD Dissertation Advisor.Rochelle Cobbs Prospectus.4.10.13.1[1]](https://img.dokumen.tips/doc/110x75/577c87921a28abe054c4a010/william-allan-kritsonis-phd-phd-dissertation-advisorrochelle-cobbs-prospectus4101311.jpg)























