Embed Size (px)
Citation preview

British Journal of Plasfic Surgery (1982) 35,41752 0 1982 The Truslees of British Association of Plastic Surgeons
0007-l226/82~O277-o047 $02.00
Latissimus dorsi muscle free flaps BRUCE N. BAILEY and ALAN M. GODFREY Plastic Surgery and Jaw Injury Service, Stoke Mandeville Hospital, A ylesbury
Summary-We have used free latissimus dorsi muscle flaps in nine patients to cover a variety of defects. The muscle has been covered with unexpanded meshed split-skin. The method is a reliable means of providing skin cover with a minimal donor site morbidity and less flap bulk than in conventional myocutaneous flaps. Our one “failure” was not related to the fact that the muscle was taken without its overlying skin, it was due to avulsion of the vascular anastomosis.
Muscle flaps have assumed an important place in the treatment of defects of the lower leg. Their use has been described in several articles by Ger (ii) (1966 to 1976). The applications and limitations of muscle flaps have been well summarised by Pers and Medgyesi (1973) and Vasconez and (iii) McGraw (1979).
We have used free latissimus dorsi muscle flaps covered with split-skin for defects where pedicled muscle or myocutaneous flaps were contraindi- (iv) cated (Bailey, 1979). The method evolved from the use of pedicled latissimus dorsi muscle flaps in order to avoid the discomfort of dorsal skin grafts particularly in a hot climate. We first used (v) this technique for muscle free flaps at Stoke Mandeville Hospital on an obese patient (Case 1) (vi) in whom the thick layer of fat was too bulky to allow a myocutaneous design of flap.
The procedure has several advantages:
tension free suture line than on a grafted area. The flap is far less bulky than a myocut- aneous flap and becomes even thinner as the muscle component atrophies. There are no difficulties in closing the donor site and the entire latissimus dorsi muscle may be used to cover massive defects. The flap may be placed with the superficial muscle surface inverted (i.e. “upside down”) if this allows a better lie of the vascular pedicle. The flap can be raised if secondary work is needed. The bulky muscle atrophies within 6-12 months leaving a mobile layer separating skin from bone very much like the normal subcutaneous tissue in the pre-tibia1 region of an undamaged leg.
(i) Donor site morbidity is reduced as there is no skin-grafted posterior skin defect. Post-
To date (December 1980) we have used latis-
operative chest managment is simplified and simus dorsi muscle free flaps in nine cases. The basic clinical details are itemised in the Table
the patient is more comfortable lying on a below.
NO. Sex Site of defect Size offlap Length offollow-up in months
1 26 JC
20 AH 19 PD 18 MC 16 SC
49 JV 30 TM 56 W 35 GF
M Knee
M M M F
M M M M
Lower leg Lower leg HtXl Lower leg
Ankle Both lower legs Head Hand
4” base 5” side
Isosceles triangle 9” x 5” 8” x 5” 8” x 5” 9” x4”
5” x 3” 15” x 8” 8” x 8” lo” x 3”
36112
18112 17112 11112
9112 Flap lost between one and two weeks
x/12 l/l 2 6112 6112
47

48
Case 1
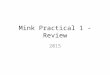
An obese muscular man sustained severe damage to his knee joint and capsule (Fig. 1). The patellar tendon and capsule of the joint had been sutured but the skin became necrotic and flap cover was requested to facilitate healing. A free latissimus dorsi muscle flap and split-skin were used (Figs. 2 and 3). After one year he had achieved full extension of the knee, 90” of active flexion and was playing football (Fig. 4).
Case 2
A motor-cyclist sustained a compound fracture of the tibia and fibula with denuded bone, a small bone defect and non-united fracture (Fig. 5). Cancellous bone chips were packed into the bone gap deep to a free latissimus dorsi muscle flap which was covered with a meshed split-skin graft (Fig. 6). The fracture united solidly in four months (Fig. 7).
Fig. 1 Loss of soft tissues with disruption of the capsule of the knee joint.
BRITISH JOURNAL OF PLASTIC SURGERY
Case 3
A motor-cyclist presented with unstable scars and sinuses over a plated ununited fracture of the mid-shaft of the tibia. The unstable area was excised and resurfaced with a free latissimus dorsi muscle flap covered with a meshed split-skin graft. The plate was removed after one month and three months later the fracture had healed solidly.
Case 4
A motor-cyclist degloved his heel exposing a shattered OS calcis which was pinned and covered with a free latissimus dorsi muscle flap and a meshed split-skin graft. He is now walking with a stick.
Case 5
A girl sustained multiple pelvic injuries and compound fractures of the right femur and mid-shaft of the tibia.
Fig. 2 Latissimus dorsi free flap in position.

LATISSIMUS DORSI MUSCLE FREE FLAPS
Fig. 3 Muscle flap covered with a split-skin graft.
Fig. 4 Nine months later the wound is soundly healed
The large area of bare bone was covered by a free latissimus dorsi muscle flap and a meshed split-skin graft. At one week the flap was healthy and the meshed skin had taken well. At the next dressing one week later the flap had failed. On exploration the vascular pedicle was found avulsed from the end-to- side popliteal anastomosis despite immobilization in a long leg plaster. The flap had revascularised the bed as a “crane flap” (Millard, 1969) and the underlying bone was protected by granulation tissue. The bone plate was removed and a few days later the granulating area was split-skin grafted. Five months later there was solid union.
Case 6
This man suffered ten years of persistent ulceration of the lower leg after trauma. Repeated skin grafting was
JPS D
unsuccessful. The area is now stable and soundly healed following a free latissimus dorsi muscle flap and a meshed split-skin graft.
Case 7
A lorry driver’s legs were crushed when he was trapped in his cab. He sustained bilateral compound com- minuted fractures of the tibia and tibuta with skin loss and a right sided femoral fracture. After excision of the devitalised tissue a single large free latissimus dorsi muscle flap was used to cover both defects, vascula- rised from the left femoral vessels. Meshed split-skin was applied to the latissimus dorsi muscle covering the leg defects and to the anterior and posterior surfaces of the muscle bridge. The flap was divided five weeks later and showed vigorous bleeding from both sides.

50 BRITISH JOURNAL OF PLASTIC SURGERY
An X-ray at six weeks showed abundant callus Case 9 formation. He is now walking with a stick.
An engineer’s right hand was degloved in a printer’s roller. Removal of the in-driven ink and damaged
Case 8 tissue exposed all the denuded metacarpals along with
A grossly overweight man (23 stone) had a massive Ringert’s tumour arising in the right frontal sinus invading the frontal lobe of the eye. It recurred after excision of the eye, bone and dura and ulcerated through the scalp flap covering the defect. Further wide excision was carried out, removing part of the frontal lobe and all the previous flap. The defect was
the flexor and extensor tendons. Following multiple neurovascular repairs the defect was covered with a free latissimus dorsi muscle flap placed inside-out to facilitate the pedicle attachment and meshed un- expanded split-skin was applied (Figs. 8 and 9). He has now regained full extension and flexion of the digits to one inch from the palm (Figs. 10 and 11).
made good with a fascia iata graft fo; dural repair and a free latissimus dorsi muscle flap with meshed skin Note on technique cover. He went home fully healed one month later and is undergoing prophylactic radiotherapy as an out- We dress the muscle graft with a layer of Vaseline
patient. If a standard free myocutaneous flap had been gauze to prevent adherence and a thick pad of used in this obese man the flap would have been b surgical gauze soaked in normal saline. This 7 cm thick. prevents desiccation of the meshed graft, reduces
Fig. 5 Compound fracture of the tibia and fibula with Fig. 6 Latissimus dorsi muscle flap covered with meshed denuded bone. split-skin.

LATISSIMUS DORSI MUSCLE FREE FLAPS 51
blood clot formation and allows free drainage. After three or four days when the skin has taken the dressing is replaced by a single layer of Vaseline gauze.
Discussion
The latissimus dorsi myocutaneous free flap is the safest and simplest free flap because of its long pedicle and large calibre vessels. Using muscle alone, donor site morbidity is reduced and the flap itself is less bulky. Skin cover is provided by unexpanded meshed split-skin which allows drainage of any haematoma or exudate. A 100% “take” is almost the rule and after a year the meshed graft pro- vides a matt surface which looks less conspicuous than the shiny appearance often seen when a sheet of split-skin graft is used.
A difficulty encountered with these cases is monitoring the muscle flap circulation before the skin-graft circulation has become visible. It is overcome by separating one of the splits in the meshed graft when the vascular muscle surface can be inspected. If there is still doubt the muscle surface may be scratched to make it bleed and
Figs. 8 and 9 Crush&gloving injury of the right hand
Fig. 7 covered with a latissimus dorsi muscle flap. A meshed split-
Eight months later the wound is soundly healed. skin graft.

52 BRITISH JOURNAL OF PLASTIC SURGERY
Figs. 10 and 11 Six months later to show the range of movement.
confirm that the circulation is intact. It may be easier to preserve a small patch of dorsal skin on the muscle flap as an indicator. This would show the familiar changes in the circulation of a skin flap and make a convenient “observation point” for the nursing staff. The island of skin could be excised after the muscle flap had “pinked up”.
Acknowledgement
We would like to thank Mr M. D. Poole, FRCS for permission to publish Case No. 8, who was admitted to the Churchill Hospital, under his care.
References
Bailey, B. N. (1979). Latissimus dorsi flaps-a practical approach. Annals of the Academy of Medicine of Singapore, 8,447.
Ger, R. (1966). Operative treatment of an advanced stasis ulcer: a preliminary communication. American Journal of Surgery, 111, 659.
Ger, R. (1968). The management of pretibal skin loss. Surgery, 63,751.
Ger, R. (1971). The technique of muscle transposition in the operative treatment of traumatic and ulcerative lesions of the leg. Journal of Trauma, 11, 502.
Ger, R. (1972). Surgical management of ulcerative lesions of the leg. Current Problems in Surgery, 1, 52.
Ger, R. (1975). The surgical management of ulcers of the heel. Surgery, Gynecology and Obstetrics, 140, 909.
Ger, R. (1976). Management of chronic ulcers of the dorsum of the foot by muscle transposition and split-skin graft. British Journal of Plastic Surgery 29, 199.
Ger, R. (1977). Closure of defects of lower extremities by muscle flaps. In Reconstructiue Plastic Surgery. Ed. J. M. Converse, 2nd Edition. Philadelphia. W. B. Saunders Company.
Millard, D. R. (1969). The “Crane” principle for the treat- ment of subcutaneous tissue. Plastic and Reconstructive Surgery, 43,45 1.
Pers, M. and Medgyesi, S. (1973). Pedicle muscle flaps and their applications in the surgery of repair. British Journal of Plastic Surgery, 26, 313.
Vasconez, L. 0. and MeCraw, J. B. (1979). Reconstruction procedures of the lower extremity. In Plastic Surgery. Ed. W. C. Grabb and J. W. Smith. Third Edition. Boston. Little Brown and Company.
The Authors
Bruce N. Railey, FRCS, Consultant Plastic Surgeon, Stoke Mandeville Hospital, Aylesbury.
Alan M. Godfrey, FRCS Ed, Senior Registrar in Plastic Surgery, Stoke Mandeville Hospital, Aylesbury.
Requests for reprints to: B. N. Bailey, FRCS, Plastic and Jaw Surgery Centre, Stoke Mandeville Hospital, Aylesbury, Bucks HP21 8AL.