Embed Size (px)
Citation preview

Late Outcome After Percutaneous Transluminal Coronary Angioplasty During Acute
Myocardial Infarction Brian O’Murchu, MB, MRCPI, Bernard J. Gersh, MB, ChB, DPhil, Guy S. Reeder, MD,
Kent R. Bailey, PhD, and David R. Holmes, Jr., MD
Early reperfusion for acute myocardial infarction (AMI) results in improved ventricular function and survival. There is a dearth of data on long-term survival (>J years) after percutaneous translumirr al coeonary mW~lasty (WCA) perfonnd dth~ as a primary procedure or in conjunction with thrombolytic therapy. We studied 150 patients who underwent PTCA durSng AMI between 1961 and 1997 either with (n = 101) or without (n = 59) streptokinase therapy. Mean time to reperfusion was 4.6 hours, and patency was achieved In 134 patients (64%). Mean discharge ejection fraction was 46 f 14%. Coronary artery bypass grafting was performed before dismissal in 34 patients (21%), including 21 of 130 patients (16%) with l- or 2-vessel disease and 13 of 30 patients (43%) wlth &vessel disease (p ~0.05). Eleven patients (7%) died in the hospiil. The 149 hospital survi- vors were followed for a mean of 69 + 21 months (median 72). During followup, 22 patients (15%) died, 21(14%) had reinfarction, 23 (15%) undelc went coronary artery bypass grafting, and 21 (14%) underwent repeat PTCA of the infarct- lated artery. On univariate analysis, age 262 years, multivessel disease, ejection fraction SO%, previous AMI, and being a nonsmoker at the time of AMI were predictive of late mortality (p *0.05 each variable). On multivariate analysis, only ejection fraction 240% and prior AMI were predictive of late death. In patients treated wlth PTCA for AMI, late survival is excellent. Early sur- gical revascularization of himsk patients may contribute to these encourting results.
(Am J Cardid 1993;72:63&639)
From the Division of Cardiovascular Diseases and Internal Medicine and the Section of Biostatistics, Mayo Clinic and Mayo Foundation, Rochester, Minnesota. Manuscript received October 8, 1992; revised manuscript received May 17, 1993, and accepted May 20.
Address for reprints: Bernard J. Gersh, MB,ChB, DPhil, Mayo Clinic, 200 First Street SW, Rochester, Minnesota 55905.
E arly reperfusion for acute myocardial infarction (AMI) results in improved ventricular function and in excellent hospital and l-year survival.1-7
However, there is a dearth of data on long-term survival (i.e., >5 years) after percutaneous transluminal coronary angioplasty (PTCA) performed either as a primary pro- cedure or in conjunction with thrombolytic therapy.7-10 Furthermore, few studies have examined risk factors for late events in this group of patients-lo We report the early and late outcomes of PTCA performed either alone or in conjunction with thrombolytic therapy at our in- stitution between April 1981 and April 1987 for AMI.
MmHODS Patients: All patients who underwent PTCA be-
tween April 1981 and April 1987 at our institution dur- ing evolving AMI were analyzed. Patients were select- ed for interventional therapy on the basis of the follow- ing criteria: symptoms that lasted for >30 minutes, myocardial injury pattern on electrocardiography con- sisting of ST-segment elevation of at least 1 mV, and evaluation within 4 hours from the onset of symptoms, or within 10 hours from onset of symptoms in the pres- ence of per-sistent or intermittent stuttering chest pain. One hundred forty-six patients who were enrolled in the National Heart, Lung, Blood Institute Thrombolysis in Myocardial Infarction (TIMJ) study at our institution during this time were excluded.
Procedure: After patients gave informed consent, left ventriculography, coronary angiography, PTCA, and intravenous or intracoronary streptokinase (or both) in- fusions were performed by standard techniques as pre- viously described.3
The decision to proceed with emergency angiogra- phy in this nonrandomized population was according to the preference of the attending cardiologist. The specif- ic treatment strategy was determined after consultation between the angiographer and the attending cardiologist and was based on the clinical situation and angiographic anatomy. In general, PTCA was chosen as the initial or sole therapy if thrombolytic therapy was relatively or ab- solutely contraindicated, hemodynamic instability was present, or PICA could be performed without delay. Short proximal stenoses or occlusions, those most suit- able for PTCA, were present in most but not all patients selected for initial PTCA therapy.
If initial PTCA produced a widely patent artery, no further therapy was given (group 1). In the absence of any contraindication, streptokinase was given if initial PICA was unsuccessful, i.e., if a high-grade stenosis re- mained or if a large amount of intraluminal thrombus
634 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 SEPTEMBER 15,1993

persisted (group 2). The remaining patients chosen for emergency angiography who did not undergo initial PTCA underwent intracoronary or intravenous strepto- kinase infusion as the initial mode of therapy (group 3). The duration of streptokinase infusion before it was deemed necessary to proceed to PTCA, performed gen- erally because of a residual high-grade stenosis or per- sistent occlusion in the infarct-related artery, varied and depended largely on the patient’s clinical status. The prevailing opinion at our institution during the period of enrollment for this study was that urgent PTCA was in- dicated in this setting. No attempt was made to dilate le- sions other than the infarct-related lesion in patients with multivessel disease. All patients underwent hepariniza- tion during PTCA and after intervention while hospital- ized. In the absence of any contraindication, patients were dismissed from the hospital taking aspirin, 325 mg/ day.
Initial left ventricular ejection fraction was calculat- ed with biplane ventriculography at the time of the ini- tial catheterization. Convalescent phase ejection fraction was determined by radionuclide ventriculography, echo- cardiography, or repeat biplane ventriculography.
Coronary artery stenoses were graded by visual esti- mation using 22 orthogonal views and expressed as the greatest stenosis in any view. Successful reperfusion was defined as angiographically demonstrated establishment of anterograde flow in the infarct-related artery (TIM1 grade 2 or 3). ‘I Time to reperfusion was defined as the interval between the onset of symptoms and the angio- graphic demonstration of anterograde blood flow through an arterial segment that was initially occluded. Patients whose infarct-related artery was patent before interven- tion were not included in data analysis when groups were divided by reperfusion times, but were included in the analysis of the results of reperfusion. Successful di- latation was defined as 220% increase in luminal diam- eter of a stenotic vessel.12
Follow-up data were obtained by means of a regis- try, with return clinic visits, telephone interviews, and questionnaires mailed to the patients. All deaths, myo- cardial infarctions, repeat PTCA procedures, episodes of severe angina, and coronary artery bypass grafting that occurred at our institution were confirmed by review of the medical records. If events occurred at outside insti- tutions, death certificates or other appropriate records were obtained for confirmation. Angina was graded by using the Canadian Cardiovascular Association criteria and was considered severe when class III or IV symp- toms were present. A “sedentary lifestyle” was defined as the absence of regular exercise before myocardial in- farction.
Statistical analysis: Continuous and discrete base- line variables were summarized by mean It: SD and by percentages, respectively. The 3 groups were compared by analysis of variance F tests for continuous variables and Pearson’s chi-square test. The univariate and multi- variate relation of variables with in-hospital mortality were assessed by simple and stepwise logistic regres- sion. Relations of baseline variables to discharge ejec- tion fraction were assessed by multiple linear regression. Late mortality or event-free survival were estimated by
TABLE I Baseline Characteristics of 160 Patients Who Underwent Percutaneous Transluminal Coronary Angioplasty During Acute Myocardial Infarction
Number of Patients (%)
Patient groups by initial therapy Group 1, PTCA alone Group 2, PTCA followed by streptokinase Group 3, streptokinase followed by PTCA
Women/men Previous myocardlal infarctlon Current smoker (at time of myocardial mfarction) Diabetes mellitus Systemic hypertension Total cholesterol > 250 mg/dl Location of myocardial infarctlon
Anterior/lateral Inferior/posterior
Q-wave myocardial infarction Cardiogenic shock
At presentation During PTCA
Number of coronary arteries narrowed > 50% in diameter
2 3
Infarct-related coronary artery Left anterior descending Left circumflex Right
Left main coronary artery stenosis > 50% Sedentary lifestyle (no regular exercise before
myocardial Infarction)
PTCA = percutaneous translumlnal coronary angioplasty.
59 38 63
241136 36 69 11 65 27
99 59
109
5 (3) 6 (4)
82 (51) 48 (30) 30 (19)
90 24 46
9
(15185) (23) (43) (7) (41) (17)
(62) (37) (68)
(56) (15) (29) (3) (6)
the Kaplan-Meier method. Relations with baseline vari- ables were assessed by log rank tests and by Cox regres- sion models.lJ (When 7-year event rates were compared between groups, p values still referred to log rank tests.) Statistical significance was judged using the 2-sided 0.05 significance level. Continuous variables were dichoto- mized for the purpose of looking at univariate and mul- tivariate relations with outcomes.
RESULTS Patient population: Baseline clinical characteristics
for the 160 patients who underwent PTCA during AMl are listed in Table I. The mean age was 59 + 11 years (range 34 to 85), and 109 patients (68%) were 165 years old. A postprocedure electrocardiogram was not avail- able for 5 patients. Left ventriculography was performed in 131 patients, yielding a mean calculated ejection frac- tion of 51 f 13% (range 9 to 80). At the start of the pro- cedure, 134 patients (84%) had total occlusion. The 3 groups of patients differed only in that cardiogenic shock during PTCA was a more frequent occurrence in group 1 patients (i.e., in 5 [8%] of the group 1 patients; 1 [3%] of the group 2 patients; and none of the group 3 pa- tients) (p = 0.044). Apart from this, no significant differ- ences in baseline characteristics were found among the 3 treatment groups.
Initial therapy: Of the 160 patients, 134 (84%) had a patent infarct-related artery at the end of the proce- dure. In addition, 8 patients underwent emergency coro-
PERCUTANEOUS TRANSLUMINAL CORONARY ANGIOPLASTY 635
”
0 1 2 3 4 5 6 7
Year
Overall Infarct-free
Event-free
nary artery bypass grafting because of unsuccessful PTCA, thus, 142 patients (89%) underwent successful reperfusion during the acute phase. The mean stenosis of the infarct vessel after therapy was 43 + 21% in those who had patent arteries. The mean time to reperfusion could be determined in 114 patients; it was 4.6 f 1.9 hours. Twenty-six patients had a patent infarct-related artery at the time of initial coronary artery injection; consequently, their reperfusion time could not be deter- mined.
Left ventricular ejection fraction was determined in 132 patients >4 days after the infarct; the mean conva- lescent ejection fraction was 46 f 14% (range 7 to 77), and was significantly higher in patients with an open (47 AI 14%; n = 113) than in those with a closed infarct-re- lated artery (38 + 13%; n = 19) (p = 0.01). Among pa- tients with an open infarct-related artery in whom time to reperfusion could be determined (n = 78), variables predictive by multivariate analysis of a better discharge ejection fraction were higher baseline ejection fraction (p <O.OOOl), earlier time to reperfusion (p = 0.0004), and undergoing PTCA alone (p = 0.04).
lrrhospttal molbiclity and mortalii: Eleven patients (7%) died before hospital dismissal, all of cardiovascu- lar causes: 4 of the 59 group 1 patients (7%), 6 of the
100
60
s i
60
2 2 3 40 02
- Open - Closed
01 I I I 1 I I I
0 1 2 3 4 5 6 7
Year
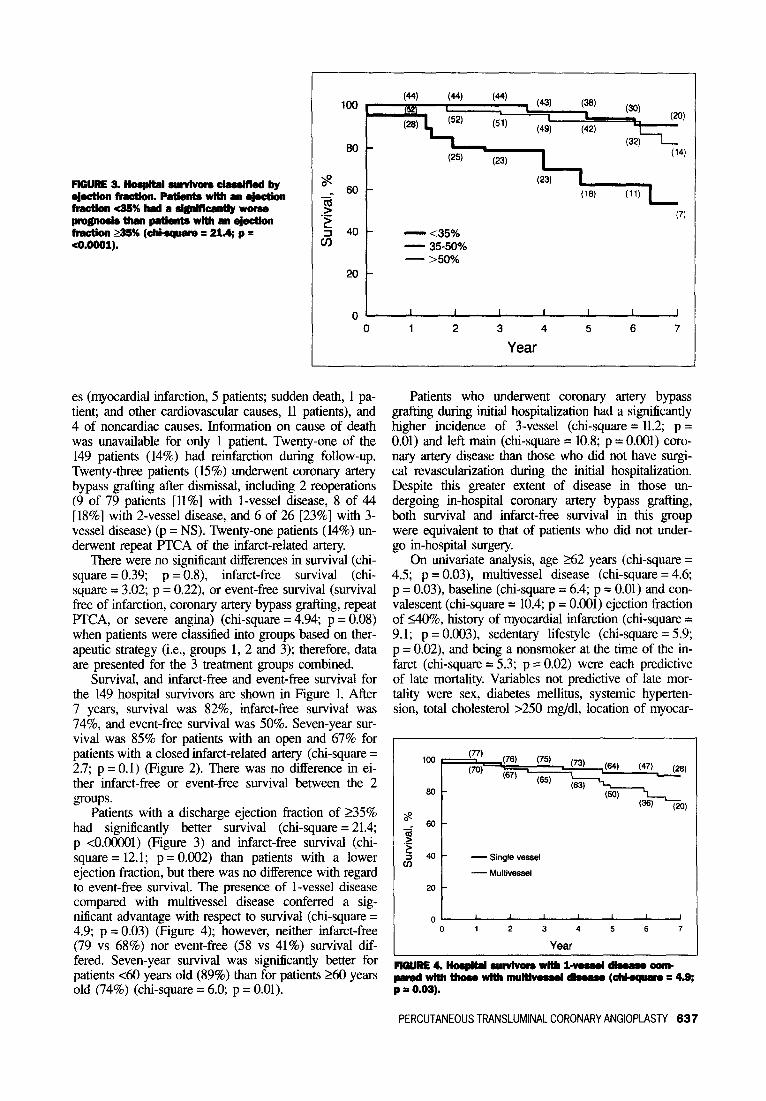
FlGURE 2. RospRal survivors wRh open compared with dosed Mar&related artarks (chkquam = 2.7; p = 0.1).
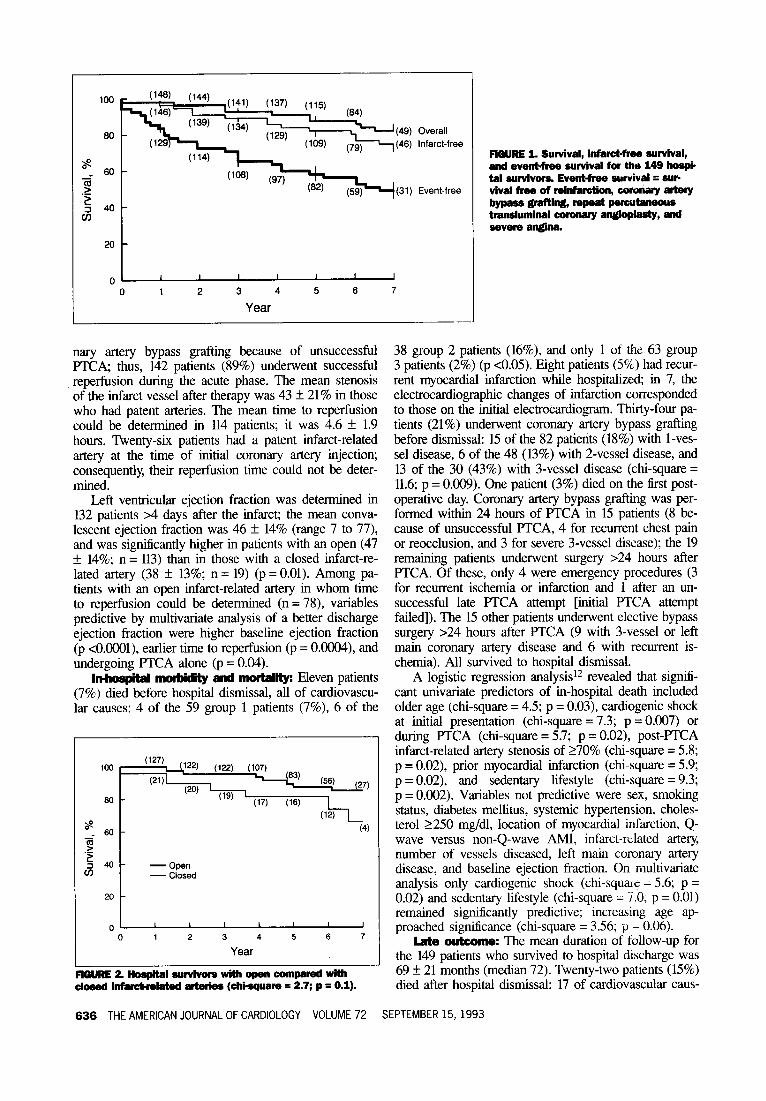
RGURE 1. Survival, infa~W~ survival, and evenbfres survival for the 149 hospi- tal survivors Event-fme survival = SW vlval frea of rainfercti, -wartery
-rYWD@-tY,- savera englne.
38 group 2 patients (16%), and only 1 of the 63 group 3 patients (2%) (p ~0.05). Eight patients (5%) had recur- rent myocardial infarction while hospitalized; in 7, the electrocardiographic changes of infarction cotresponded to those on the initial electrocardiogram. Thirty-four pa- tients (21%) underwent coronary artery bypass grafting before dismissal: 15 of the 82 patients (18%) with l-ves- sel disease, 6 of the 48 (13%) with 2-vessel disease, and 13 of the 30 (43%) with 3-vessel disease (&i-square = 11.6; p = 0.009). One patient (3%) died on the first post- operative day. Coronary artery bypass grafting was per- formed within 24 hours of FTCA in 15 patients (8 be- cause of unsuccessful FTCA, 4 for recurrent chest pain or reocclusion, and 3 for severe 3-vessel disease): the 19 remaining patients underwent surgery >24 hours after RCA. Of these, only 4 were emergency procedures (3 for recurrent ischemia or infarction and 1 after an un- successful late F’TCA attempt [initial FTCA attempt failed]). The 15 other patients underwent elective bypass surgery >24 hours after FTCA (9 with 3-vessel or left main coronary artery disease and 6 with recurrent is- chemia). All survived to hospital dismissal.
A logistic regression analysis12 revealed that signifi- cant univariate predictors of in-hospital death included older age (&i-square = 4.5; p = 0.03), cardiogenic shock at initial presentation (&i-square = 7.3; p = 0.007) or during FTCA (&i-square = 5.7; p = 0.02), post-F’TCA infarct-related artery stenosis of 270% (&i-square = 5.8; p = 0.02), prior myocardial infarction (&i-square = 5.9; p = 0.02), and sedentary lifestyle (&i-square = 9.3; p = 0.002). Variables not predictive were sex, smoking status, diabetes mellitus, systemic hypertension, choles- terol 2250 mg/dl, location of myocardial infarction, Q- wave versus non-Q-wave AMI, infarct-related artery, number of vessels diseased, left main coronary artery disease, and baseline ejection fraction. On multivariate analysis only cardiogenic shock (chi-squaic - 5.6; p = 0.02) and sedentary lifestyle (chi-square - i.0, p = 0.01) remained significantly predictive; increasing age ap- proached significance (cm-square = 3.56; p - 0.06).
I.&e outcome: The mean duration of follow-up for the 149 patients who survived to hospital discharge was 69 f 21 months (median 72). Twenty-two patients (15%) died after hospital dismissal: 17 of cardiovascular caus-
636 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 SEPTEMBER 15,1993
FlGuRE2.Hosp&alwrvlvors-by ~WtlOll-.-Wlth~ejectian
fracthcSS%hmla~worse PWP-~pstientrW~~~ fltwth 35% (chbsquara = 21.4; p = CO.0001).
20
t
”
0 1 2 3 4 5 6 7
Year
es (myocardial infarction, 5 patients; sudden death, 1 pa- tient; and other cardiovascular causes, 11 patients), and 4 of noncardiac causes. Information on cause of death was unavailable for only 1 patient. Twenty-one of the 149 patients (14%) had reinfarction during follow-up. Twenty-three patients (15%) underwent coronary artery bypass grafting after dismissal, including 2 reoperations (9 of 79 patients [ ll%] with l-vessel disease, 8 of 44 [18%] with 2-vessel disease, and 6 of 26 [23%] with 3- vessel disease) (p = NS). Twenty-one patients (14%) un- derwent repeat PTCA of the infarct-related artery.
There were no significant differences in survival (chi- square = 0.39; p = 0.8), infarct-free survival (chi- square = 3.02; p = 0.22) or event-free survival (survival free of infarction, coronary artery bypass grafting, repeat PTCA, or severe angina) (&i-square = 4.94; p = 0.08) when patients were classified into groups based on ther- apeutic strategy (i.e., groups 1, 2 and 3); therefore, data are presented for the 3 treatment groups combined.
Survival, and infarct-free and event-free survival for the 149 hospital survivors are shown in Figure 1. After 7 years, survival was 82%, infarct-free survival was 74%, and event-free survival was 50%. Seven-year sur- vival was 85% for patients with an open and 67% for patients with a closed infarct-related artery (&i-square = 2.7; p = 0.1) (Figure 2). There was no difference in ei- ther infarct-free or event-free survival between the 2 groups.
Patients with a discharge ejection fraction of 235% had significantly better survival (&i-square = 21.4; p <O.OOOOl) (Figure 3) and infarct-free survival (chi- square = 12.1; p = 0.002) than patients with a lower ejection fraction, but there was no difference with regard to event-free survival. The presence of l-vessel disease compared with multivessel disease conferred a sig- nificant advantage with respect to survival (&i-square = 4.9; p = 0.03) (Figure 4); however, neither infarct-free (79 vs 68%) nor event-free (58 vs 41%) survival dif- fered. Seven-year survival was significantly better for patients ~60 years old (89%) than for patients 260 years old (74%) (&i-square = 6.0; p = 0.01).
Patients who underwent coronary artery bypass grafting during initial hospitalization had a significantly higher incidence of 3-vessel (&i-square = 11.2; p = 0.01) and left main (chi-square = 10.8; p = 0.001) coro- nary artery disease than those who did not have surgi- cal revascularization during the initial hospitalization. Despite this greater extent of disease in those un- dergoing in-hospital coronary artery bypass grafting, both survival and infarct-free survival in this group were equivalent to that of patients who did not under- go in-hospital surgery.
On univariate analysis, age 262 years (&i-square = 4.5; p = 0.03), multivessel disease (chi-square = 4.6; p = 0.03), baseline (&i-square = 6.4; p = 0.01) and con- valescent (&i-square = 10.4; p = 0.001) ejection fraction of 140%, history of myocardial infarction (&i-square = 9.1; p = 0.003), sedentary lifestyle (&i-square = 5.9; p = 0.02), and being a nonsmoker at the time of the in- farct (&i-square = 5.3; p = 0.02) were each predictive of late mortality. Variables not predictive of late mor- tality were sex, diabetes mellitus, systemic hyperten- sion, total cholesterol >250 mg/dl, location of myocar-
100
8
ii 60-
.->
’ 40 - -Single vessel 4
- Multivessel
Flww4.lbapltd SWVhW8WMll-WS!lldabrruCO#Ib pamdwithtlmewithmulthwseldbase(~=4.9; p = 0.02).
PERCUTANEOUS TRANSLUMINAL CORONARY ANGIOPLASTY 637

dial infarction, non-Q-wave versus Q-wave AMI, car- diogenic shock, infarct-related artery, left main coronary artery disease, and postPICA infarct-related artery stenosis of 270%. On multivariate analysis, only conva- lescent ejection fraction of 140% (chi-square = 9.1; p = 0.003) and a history of myocardial infarction (chi- square = 4.0, p = 0.05) remained significantly predictive of late death.
DISCUSSION Early reperfusion during AM1 decreases infarct size,
increases myocardial salvage, and improves recovery of left ventricular function.3,7sJ4 Although numerous stud- ies clearly show excellent hospital and l-year survival,‘s4 others suggest that the benefits of thrombolytic therapy are maintained for up to 6 years of follow-up.10J5J6 Our study coniirms the low early morbidity and mortality as- sociated with PTCA alone or in combination with strep- tokinase as initial therapy for AMI. Moreover, we report long-term and event-free survival with follow-up for all patients.
Aggressive intervention in the form of thrombolytic therapy, PTCA, or both, has been shown to have a fa- vorable impact on early mortality and ischemic events.17 In-hospital mortality in these and other studies ranged from 7 to 12%2-4,7-9 and compares favorably with the 7% for our patients treated with PTCA alone. Howev- er, whereas recent studies have shown a reduction in recurrent ischemia,18 no randomized study has docu- mented a superiority of PTCA over thrombolytic thera- py for mortality reduction from AMI.18,19 Indeed, there are ample data supporting the lack of additional benefit from early PTCA after thrombolytic therapy for AMI.2o The better in-hospital survival in the present study among patients treated in this manner is likely to reflect their lower prevalence of cardiogenic shock, a powerful predictor of early death.
Previous reports3q7,8 found that patients treated with PICA have improved left ventricular function than pa- tients who received streptokinase. Our data suggest that, among patients with an open infarct-related artery, the major determinants of a favorable discharge ejection fraction are higher baseline ejection fraction and short- er time to reperfusion.
The low annual mortality rate of 2.5% among hospi- tal survivors is encouraging and deserves comment. In the current study, a convalescent ejection fraction of <40%, a history of prior myocardial infarction, multives- se1 coronary artery disease, and older age adversely af- fected late mortality. These data confirm those of pre- vious reports7,9*21; however, the l-year mortality in the present study is better than would be expected from ex- trapolation of the Multicenter Postinfarction Research Group21 data. The importance of an open compared with a closed infarct-related artery has been emphasized.22,23 In the present study, although patients with closed artery had a significantly lower discharge ejection fraction, they formed a minority (15%) of the cohort. Further- more, strong selection biases were reported in trials of thrombolytic therapy?4,25 where as few as 22 to 33% of patients with AM1 received lytic therapy. These biases, operating in the present study, may have contributed to
the selection of low-risk patients with lower mortality and adverse outcome rates.
The role of surgical revascularization in the setting of AMI is controversial? A high frequency (22 to 25%) of bypass grafting has been reported in trials of throm- bolytic therapy,2o*27 and despite older age, more exten- sive coronary disease, and lower ejection fraction, the mortality of patients who had undergone surgery was comparable to that of those who had no operation. A low incidence of 3-vessel disease (19%) was noted in our study group and surgical revascularization was per- formed more frequently within this group. That many of these higher risk patients underwent coronary bypass surgery may have had an additional and beneficial effect on mortality.
To our knowledge, being a current smoker at the time of infarction has not been reported as a favorable prognostic factor in late survival (>5 years) after AMI. Mueller et a128 found that the term “not current smok- er” was predictive of fatal and nonfatal reinfarction ear- ly after myocardial infarction; our data expand this ob- servation into late survival. It is possible that smokers have a coronary artery disease risk factor profile that is mom amenable to secondary prevention than do patients who have infarction in the absence of the smoking in- sult.
In patients treated with PTCA either alone or in com- bination with thrombolytic therapy, late survival and event rates are excellent. PTCA in AMI should be one aspect of a “sequential reperfusion strategy”27 that in- volves careful patient selection, observation for recurrent ischemia, and both catheter-based and surgical revascu- larization in high-risk subsets.
1. ISIS-2 (Second International Studv of Infarct Survival) Collaborative Grow. Randomised trial of intravenous streptbkinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. Lancer 1988;2: 349-360. 2. Holmes DR Jr, Smith HC, Vlietstm RJ?, Nishimwa RA, Reeder GS, Bove AA, Bresnahan JF. Chesebm JH. Piehler JM. Percutaneous transluminal coronarv an- -, gioplasty, alone or in combination with streptokinase therapy, during acute my- ocmiial infarction. Mayo Clin Proc 1985;60:44%456. 3. O’Neill W, Tiimis GC, Bourdiilon PD, Lai P, Ganghadzhan V, Walton I Jr, Ramos R, Laufer N, Gordon S, Schork MA, Pitt B. A prospective randomized clii- ical trial of intracoronary streptokinase versus coronary angioplwy for acute my- ocardial infarction. N Engl J Med 1986;314:812-818. 4. Stack RS, Califf RM, Hiiohara T, Phillips HR. Pryor DB, Simonton CA, Carl- son EB, Morris KG, Behar VS, Kong Y, Peter RH, Hlatky MA, O’Connor CM, Mark DB. Survival and cardiac event rates in the fmt year after emergency com- nary angioplasty for acute myccaxiial infarction. J Am CoU Cardiol 1988;ll: 1141-l 149. 1. Pepine CJ, Prida X, Hill JA, Feldman RL, Conti CR. Percutaneous transluminal coronary aneio~lastv in acute mvocardial infarction. Am Heart J 1984:107:82l&822. 6. H&ler 66, RutheTford BD: McConahay DR, Johnson WL Jr, Mbllister BD, Gum GM Jr, Corm RC, Crockett JE. Percutaneous tmnsluminal coronary angic- plasty with and without thrombolytic therapy for txeahnent of acute myocardi~in- farction. Am Heart J 1983;106:965-973. 7. Kahn JK, Rutherford BD, McConahay DR, Johnson WL, Giorgi LV, Shimshak TM, Ligon R, Hart&r GO. Results of primary angioplasty for acute myocmdial infarction in patients with multivessel coronary artery disease. J Am Coil Cardiol 1990;16:1089-1096. 8. O’Keefe JH Jr, Rutherford BD, McConahay DR. Ligon RW, Johnson WL Jr, Giorgi LV, Crockett JE, McCallister BD, Corm RD, Guru GM Jr, Good TH, Stein- haus DM, Bateman TM, Shimshak TM, Hartzler GO. Early and late results of corn- nary angioplasty without antecedent thmmbolytic therapy for acute myocardial in- faction. Am J Cardiol 1989;64:1221-1230. 9. Kander NH, O’Neill W, Top01 FJ, Gallison L, Mileski R, Ellis SG. Long-term follow-up of patients treated with coronary angioplasty for acute myocardial in- farction. Am Heart J 1989;118:22&233. 10. Taylor GJ, Moses HW, Katholi RE, Korsmeyer C, Kolm P, Dove JT, Mike11 FL, Sutton JM, Wellons HA, Schneider JA. Six-year survival after coronary throm- bolysis and early revascularization for acute myocardial infarction. Am J Cardiol
638 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 SEPTEMBER 15,1993

1992;70:26-30. 11. The TIMI Study Group. The Thrombolysis in Myocardial Infarction (TIMI) trial. Phase I fmdings. N Engl .I Med 1985;312:932-936. 12. Kent KM, Bentivoglio LG, Block PC, Cowley MJ, Dorms G, Goss&n AJ, Grunt& A, Myler RK, Simpson J, Stettzer SH, Williams Do, Fisher L, Gillespie MJ, Deue K, Kelsey S, Mullin SM, Mock MB. Percutaneous transluminal coro- nary angioplasty: report from the Registry of the National Heart, Lung, and Blood Institute. Am J Cardiol 1982;49:201 I-2020. 13. Cox DR. Regression methods and life-tables (with discussion). J R Star Sot (BJ 1972:34: 187-220. 14. Lee L, Bates ER, Pitt B, Walton JA, Laufer N, O’Neill WW. Percutaneous tmnsluminal coronary angioplasry improves survival in acute myocardial infarction complicated by cardiogenic shock. Circular~on 1988:78: 1345-135 1. 15. Simoons ML, Vos J, Tijssen JGP, Vermeer F, Verheugt FWA, Krauss XH, Cats VM. Long-term benefit of early thrombolytic therapy in patients with acute myocardial infarction: 5 year follow-up of a trial conducted by the Interuniversity Cardiology Institute of The Netherlands. J Am Co!/ Cardiol 19X9; 14:1609-1615. 16. Mathey DG. Schafer J, Sheehan FH, Krebber H-J, Justen M, Rodewald G. Dodge HT, Bleifeld W. Improved survival up to four years after early coronary rhmmbolysis. Am J Cardin/ 1988;61:52&529. 17. Top01 EJ. O’Neill WW, Langburd AB, Walton JA Jr, Bourdillon PDV, Bates ER, Grines CL, Schork AM, Kline E, Pitt B. A randomized, placebo-controlled trial of inmavenous recombinant tissue-type plasminogen activator and emergency coronaq angioplasty in acute myocardial infarction. Cimdarion 1987;75:42@428. 18. Grines CL, Bmwne KF, Marco J, Rothbaum D, Stone GW, O’Keefe J, Over- lie P, Donahue B, Chelliah N, Timmis GC, Vlietstra RE, Shzelecki M, Puchro- wicz-Ochocki S, O’Neill WW, for the Primary Angioplasty in Myocardial Infarc- tion Study Group. A comparison of immediate angioplasty with thrombolytic ther- apy for acute myocardial infarction. N Engl J Med 1993;328:67%79. 19. Gibbons RJ, Holmes DR, Reeder GS, Bailey KR, Hopfenspirger MR, Gersh BJ, for the Mayo Coronary Care Unit and Catheterization Laboratory Groups. Im- mediate angioplasty compared with the adminisuation of a thmmbolytic agent fol- lowed by conservative treatment for myocardial infarction. N En,@ J Mrd 1993
;328:68%691. 20. TIMI Study Group. Comparison of invasive and conservative strategies after treatment with intravenous tissue plasminogen activator in acute myocanlial in- farction: Results of the Thrombolysis in Myocardial Infarction (TIMI-II) Phase II Trial. N Engl J Med 1989;320:618-627. 21. The Multicenter Postinfarction Research Group. Risk stratification and survival after myocardial infarction. N Engl J Med 1983;309:331-336. 22. Braunwald E. Myocardial repezfusion, limitation of infarct size, reduction of left ventricular dysfunction, and improved survival. Should the paradigm be ex- panded? Circulation 1989;79:4414l4. 23. Califf RM, Top01 EI, Gersh BJ. From myocardial salvage to patient salvage in acute myocardial infarction: the role of reperfusion therapy. J Am CoN Cardiol 1989; 14: 1382-1388. 24. Pfeffer MA, Moye LA, Braunwald E, Basta L, Brown FJ Jr, Caddy TE, Da- genais GR, Flaker GC, Gelhnan EM, Gersh BJ, Goldman S, Lamas GA, Packer M, Rouleau JL, Rutherford JD, Steingart RM, Wertheimer JH, for the SAVE in- vestigators. Selection bias in the use of thnxnbolytic therapy in acute myocardial infarction. JAMA 1991;266:528-532. 25. Cragg DR, Friedman HZ, Bonema JD, Jaiyesimi IA, Ramos RG, Timmis GC, O’Neill WW, Schreiber TL. Outcome of patients with acute myocardial infarction who are ineligible for thrombolytic therapy. Ann Infern Med 1991;115:173-177. 26. Roten HS, Ahmad A, Swanson JS, Wood JA, Chapman RD, Fessler CL, Starr A. Long-term survival after postinfarction bypass operation: early versus late oper- ation. Ann Thorac Surg 1989:48:757-763. 27. Kereiakes DJ, Califf RM, George BS, Ellis S, Samaha J, Stack R, Martin LH, Young S, Topol EJ, and the TAM1 Study Group. Coronary bypass surgery im- proves global and regional left ventricular function following thmmbolytic therapy for acute myocardiai infarction. Am Heart J 1991;122:39(1-399. 28. Mueller HS, Cohen LS, Braunwald E, Fornun S, Feit F, Ross A, Schweiger M, Cabin H, Davison R, Miller D, Solomon R, Knattelud GL. Predictors of early morbidity and mortality after thrombolytic therapy of acute myocardial infarction: analyses of patient subgroups in the ‘Ihrombolysis in Myocardial Infa&on (TIMI) Trial, Phase II. Circzdation 1992;85:12541264.
PERCUTANEOUS TRANSLUMINAL CORONARY ANGIOPLASTY 639





























