Embed Size (px)
Citation preview
Laparoscopic Hysterectomy: Total, supracervical, robotic, single port ?
Tommaso Falcone, M.D.Professor an Chair
Learning ObjectivesLearning Objectives
Select patients appropriately for Select patients appropriately for Laparoscopic hysterectomyLaparoscopic hysterectomy
Understand the advantages and limitations Understand the advantages and limitations of different surgical approaches of different surgical approaches
Understand the advantages and limitations Understand the advantages and limitations of robotic hysterectomyof robotic hysterectomy

DUB 20%DUB 20%(120,000/year)(120,000/year)
Fibroids 30%Fibroids 30%
Endometriosis/Endometriosis/Adenomyosis 20%Adenomyosis 20%
((Pre) cancer Pre) cancer 10%10%
Chronic pelvic pain 10%Chronic pelvic pain 10%Prolapse 15%Prolapse 15%
Hysterectomy in the US for DUB Hysterectomy in the US for DUB

Procedure of ChoiceProcedure of Choice
Johnson N, Barlow D, Lethaby, et al. Johnson N, Barlow D, Lethaby, et al. Surgical approach to hysterectomy for Surgical approach to hysterectomy for benign gynecological disease. Cochrane benign gynecological disease. Cochrane Database Syst Rev 2006; CD 003677.Database Syst Rev 2006; CD 003677.
This review included 3643 patients from This review included 3643 patients from 27 randomized trials. 27 randomized trials.
Vaginal hysterectomy is the procedure of Vaginal hysterectomy is the procedure of choice choice

Preoperative ConsiderationsPreoperative Considerations
Prophylactic oophorectomy in women without Prophylactic oophorectomy in women without riskrisk– A decision analysis by Parker et al suggested that A decision analysis by Parker et al suggested that
the age for prophylactic oophorectomy should be the age for prophylactic oophorectomy should be closer to 65 years (Obstet Gynec 2005).closer to 65 years (Obstet Gynec 2005).
– Vitonis et al Obstet Gynecol May 2011Vitonis et al Obstet Gynecol May 2011Risk: Jewish ethnicity, less than 1 year of OCs, nulliparity, no Risk: Jewish ethnicity, less than 1 year of OCs, nulliparity, no breastfeeding, no tubal ligation, endometriosis, PCOS or breastfeeding, no tubal ligation, endometriosis, PCOS or obesity, talc useobesity, talc use
0-1 score lifetime risk 1.2 %0-1 score lifetime risk 1.2 %
5 or more 6.6%5 or more 6.6%
Total vs. Supracervical Total vs. Supracervical HysterectomyHysterectomy
Learman et al Obstet Gynecol 2003 (RCT 135 Learman et al Obstet Gynecol 2003 (RCT 135 patients)patients)No differenceNo difference– ComplicationsComplications– Length of stayLength of stay– Postoperative painPostoperative pain– Total convalescenceTotal convalescence– Reduction of preoperative symptoms (including Reduction of preoperative symptoms (including
urinary symptoms)urinary symptoms)– In urinary symptoms or incontinence at 24 monthsIn urinary symptoms or incontinence at 24 months

ReadmissionsReadmissions
Readmissions: TAH 6% & SCH 12% (NS) Readmissions: TAH 6% & SCH 12% (NS)
Post-supracervical hysterectomy cyclic Post-supracervical hysterectomy cyclic vaginal bleeding: 5%vaginal bleeding: 5%
RCT: Thakar et al NEJM 2002RCT: Thakar et al NEJM 2002
No difference in outcomeNo difference in outcome– Sexual function, urinary symptoms all improvedSexual function, urinary symptoms all improved
More blood loss in TAH ( 422mL) vs. SCH More blood loss in TAH ( 422mL) vs. SCH (320mL); no difference in blood transfusion(320mL); no difference in blood transfusion
Time difference: 11 minutesTime difference: 11 minutes
Postoperative complicationsPostoperative complications– Pyrexia higher TAH groupPyrexia higher TAH group– Cyclic vaginal bleeding or cervical prolapse: 7%Cyclic vaginal bleeding or cervical prolapse: 7%

Post-hysterectomy bleeding Post-hysterectomy bleeding
Danish study- N=136 19 % experienced Danish study- N=136 19 % experienced bleeding but only 2 patients required a bleeding but only 2 patients required a trachelectomytrachelectomy
British study-N= 140 7 % bleeding & 2 % British study-N= 140 7 % bleeding & 2 % had prolapsehad prolapse
American study N=68 5 % bleeding only 1 American study N=68 5 % bleeding only 1 patient required a trachelectomypatient required a trachelectomy
Quality of LifeQuality of Life
Einarsson et al 2011Einarsson et al 2011– Prospective trial TLH vs. TSHProspective trial TLH vs. TSH
QOL scores better with TSHQOL scores better with TSH
No difference in postoperative pain, No difference in postoperative pain, nausea, use of opoids, or return to daily nausea, use of opoids, or return to daily activityactivity
Patients want choicesPatients want choicesPatients want choicesPatients want choices
Decisions are a Decisions are a partnership between partnership between doctor & patientdoctor & patient

Patients want choicesPatients want choices
Evidence based medicine does not imply Evidence based medicine does not imply giving one option-the one with the highest giving one option-the one with the highest Odds Ratio in the Cochrane reviews Odds Ratio in the Cochrane reviews
Impact of HysterectomyImpact of Hysterectomy
Emotional and perceptional impact of Emotional and perceptional impact of hysterectomyhysterectomy
Patient resourcesPatient resources
Web sitesWeb sites– Attest to the “damage” of hysterectomyAttest to the “damage” of hysterectomy
Amazon.com Amazon.com – Myriad of booksMyriad of books
Supracervical hysterectomySupracervical hysterectomy
Perceived as a “hysterectomy alternative”Perceived as a “hysterectomy alternative”
Allows preservation of what is perceived to Allows preservation of what is perceived to be the most important part of the organbe the most important part of the organ
Patient SelectionPatient SelectionExclusion of malignancy or pre-malignant Exclusion of malignancy or pre-malignant statestate
Realistic expectationsRealistic expectations– Do they want 100 % guarantee of amenorrhea?Do they want 100 % guarantee of amenorrhea?
– 24 % had residual endometrium in the stump24 % had residual endometrium in the stump
Endometriosis patientsEndometriosis patients– 23 % who had a trachelectomy had endometriosis 23 % who had a trachelectomy had endometriosis
Prolapse ?Prolapse ?
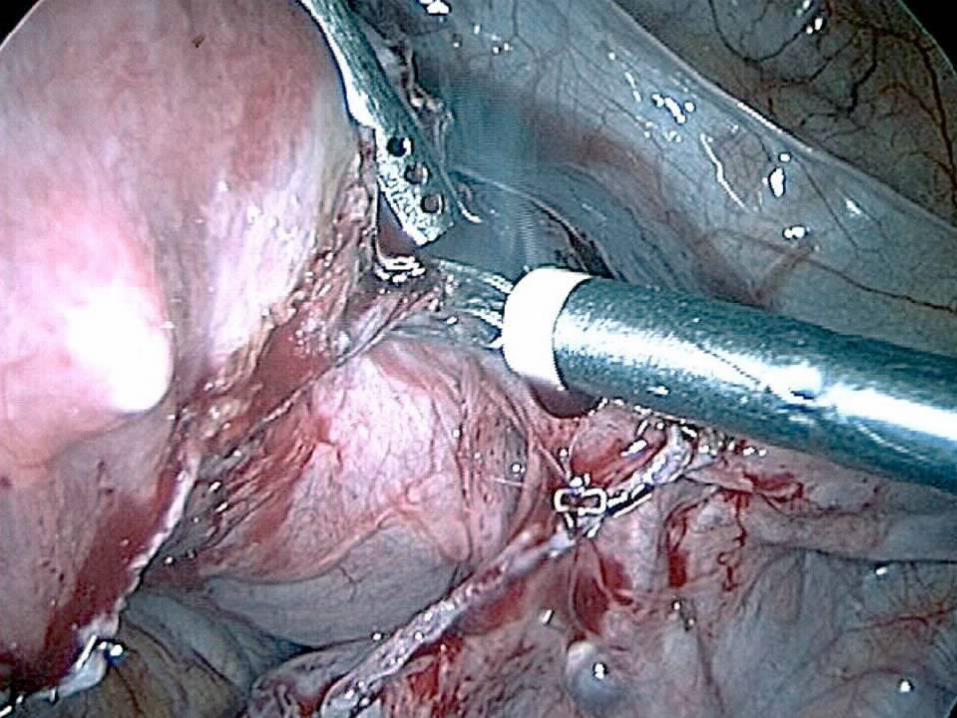
How to convert an abdominal How to convert an abdominal hysterectomy into a less hysterectomy into a less
invasive procedureinvasive procedure
Supracervical is far less complex than a Supracervical is far less complex than a laparoscopic or LAVHlaparoscopic or LAVH
Supracervical is technically easier and Supracervical is technically easier and fasterfaster
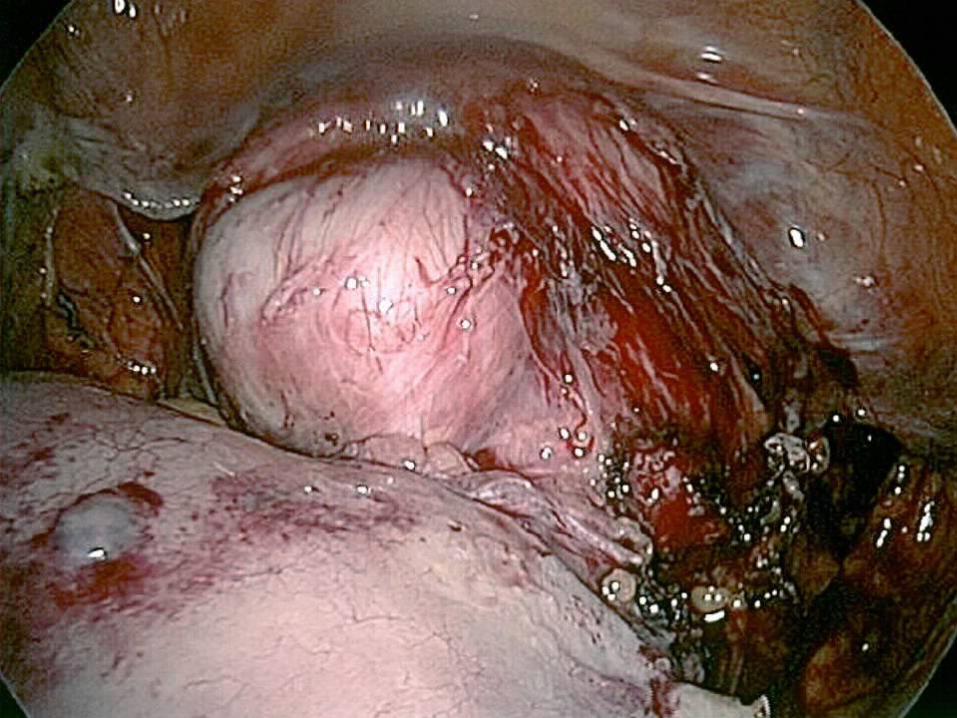
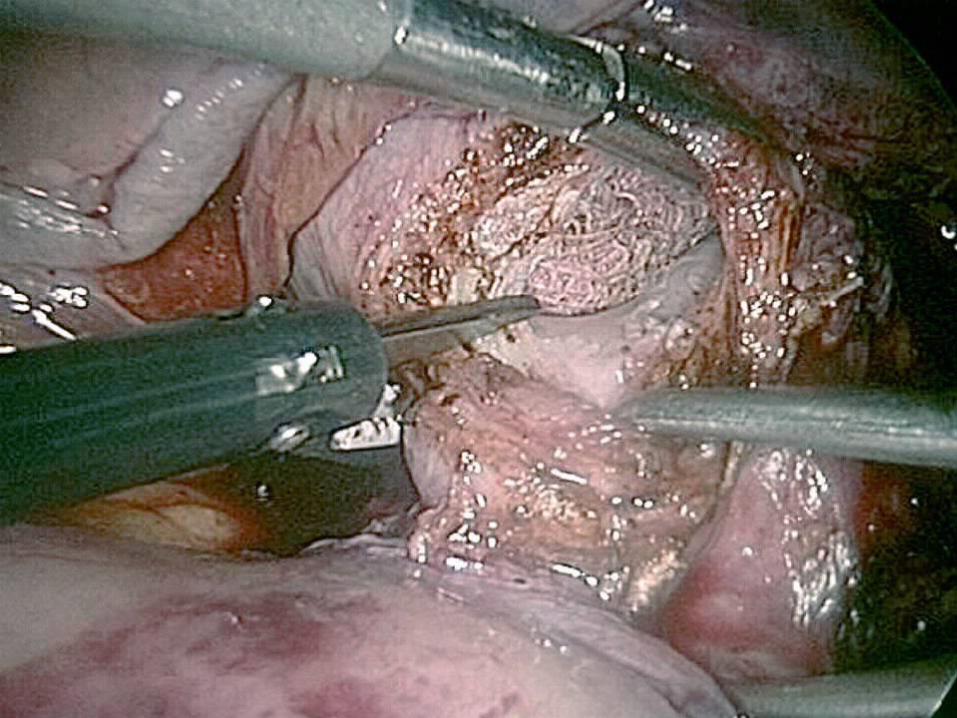
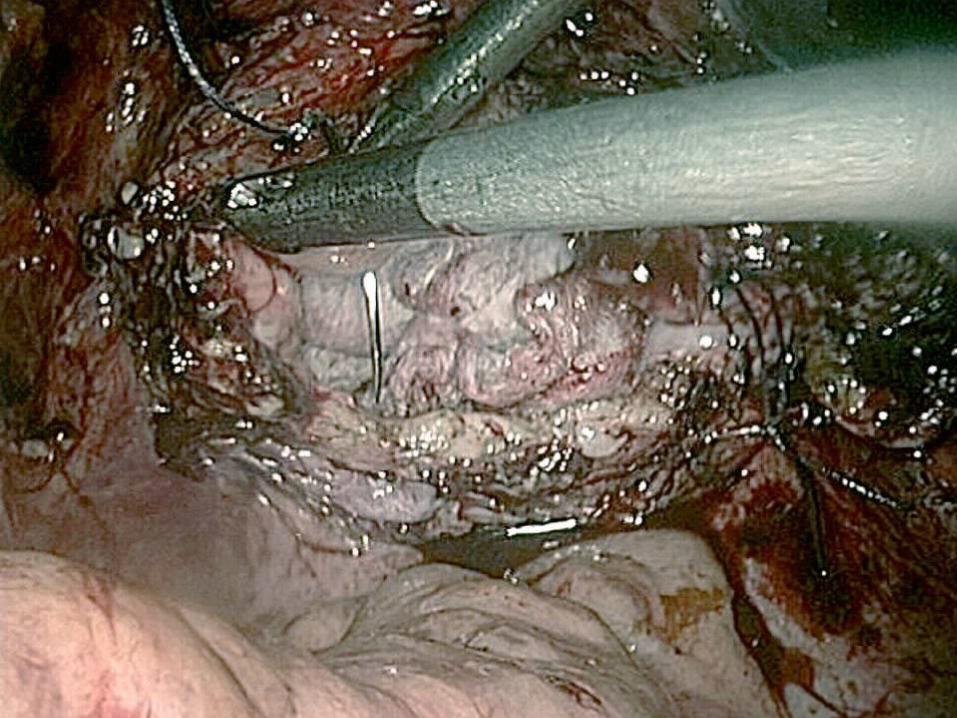
InjuryInjury
Cochrane database-Urinary Tract injuryCochrane database-Urinary Tract injury– LAVH associated with more injury than LAVH associated with more injury than
abdominal hysterectomyabdominal hysterectomyRelated to the dissection required around the Related to the dissection required around the paracervical areaparacervical area
– Supracervical is probably associated with less Supracervical is probably associated with less urinary tract injuryurinary tract injury
The RCT were not powered to assess injuryThe RCT were not powered to assess injury
To detect a 2 % difference- 2000 subjects To detect a 2 % difference- 2000 subjects randomizedrandomized

Abdominal Abdominal Hysterectomy Hysterectomy
Laparoscopic Laparoscopic HysterectomyHysterectomy
Vaginal Vaginal HysterectomyHysterectomy
Laparoscopic HysterectomyLaparoscopic Hysterectomy
At least one At least one complication complication
6.2 %6.2 % 7.2 %7.2 % 5.4 %5.4 % 6.7 %6.7 %
Conversion to Conversion to laparotomylaparotomy
3.9 %3.9 % 4.2 %4.2 % 2.7 %2.7 %
Major Major hemorrhagehemorrhage11
2.4 %2.4 % 4.6%4.6% 2.9%2.9% 5.1%5.1%
Bowel injuryBowel injury 1%1% 0.2%0.2% 0%0% 0%0%
Ureter injuryUreter injury 0%0% 0.9%0.9% 0%0% 0.3%0.3%
Bladder injuryBladder injury 1%1% 2.1%2.1% 1.2%1.2% 0.9%0.9%
Other Other 22 2.1%2.1% 2.4 %2.4 % 1.8 %1.8 % 3.9 %3.9 %
Perioperative ConsiderationsPerioperative Considerations
Prophylactic antibiotics initiated within one Prophylactic antibiotics initiated within one hour of incisionhour of incision
Use of first or second generation Use of first or second generation cephalosporinscephalosporins
Discontinuing prophylactic antibiotics Discontinuing prophylactic antibiotics within 24 hourswithin 24 hours
VTE prophylaxisVTE prophylaxis
unfractionated heparin (5000 units every 12 unfractionated heparin (5000 units every 12 hours) or low molecular weight heparin hours) or low molecular weight heparin (ex.enoxaparin 40 mg or 2500 units of (ex.enoxaparin 40 mg or 2500 units of dalteparin) or intermittent pneumatic dalteparin) or intermittent pneumatic compression device compression device Patients over 40 years of age or those under 40 Patients over 40 years of age or those under 40 years of age who have risk factors (such as years of age who have risk factors (such as obesity)- unfractionated heparin (5000 units obesity)- unfractionated heparin (5000 units every 8 hours) or low molecular weight heparin every 8 hours) or low molecular weight heparin ( 5000 units of dalteparin or similar dose of ( 5000 units of dalteparin or similar dose of enoxaparin 40 mg). enoxaparin 40 mg).




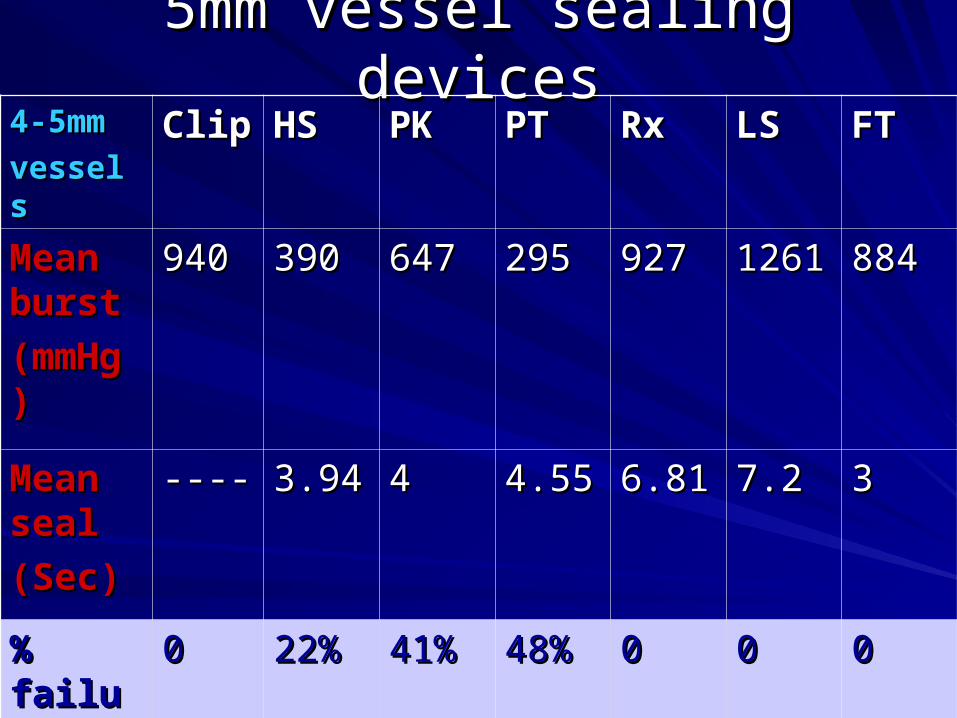
5mm vessel sealing devices5mm vessel sealing devices4-5mm4-5mm
vesselsvesselsClipClip HSHS PKPK PTPT RxRx LSLS FTFT
Mean Mean burstburst
(mmHg(mmHg))
940940 390390 647647 295295 927927 12611261 884884
Mean Mean sealseal
(Sec)(Sec)
-------- 3.943.94 44 4.554.55 6.816.81 7.27.2 33
% % failuresfailures
00 22%22% 41%41% 48%48% 00 00 00






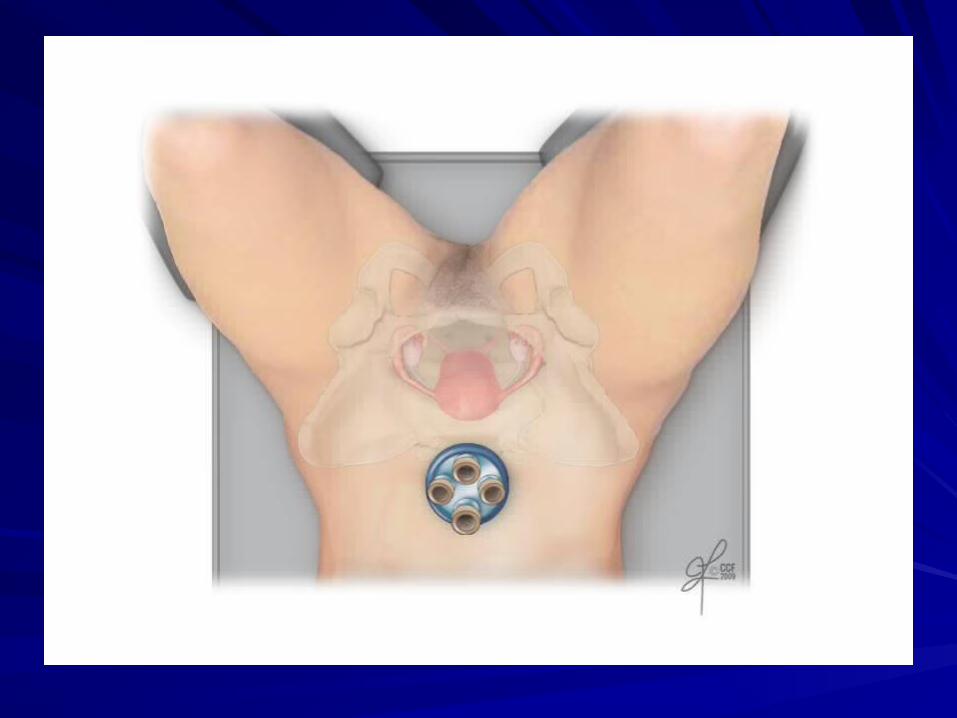

LESS ( Single Site) HysterectomyLESS ( Single Site) Hysterectomy
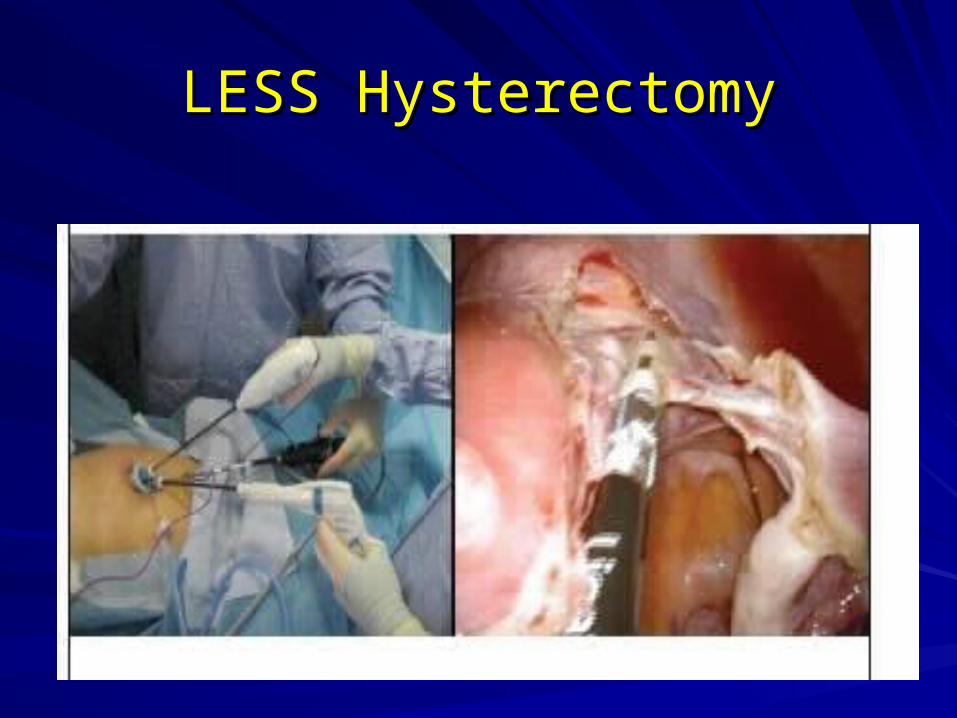
LESS HysterectomyLESS Hysterectomy
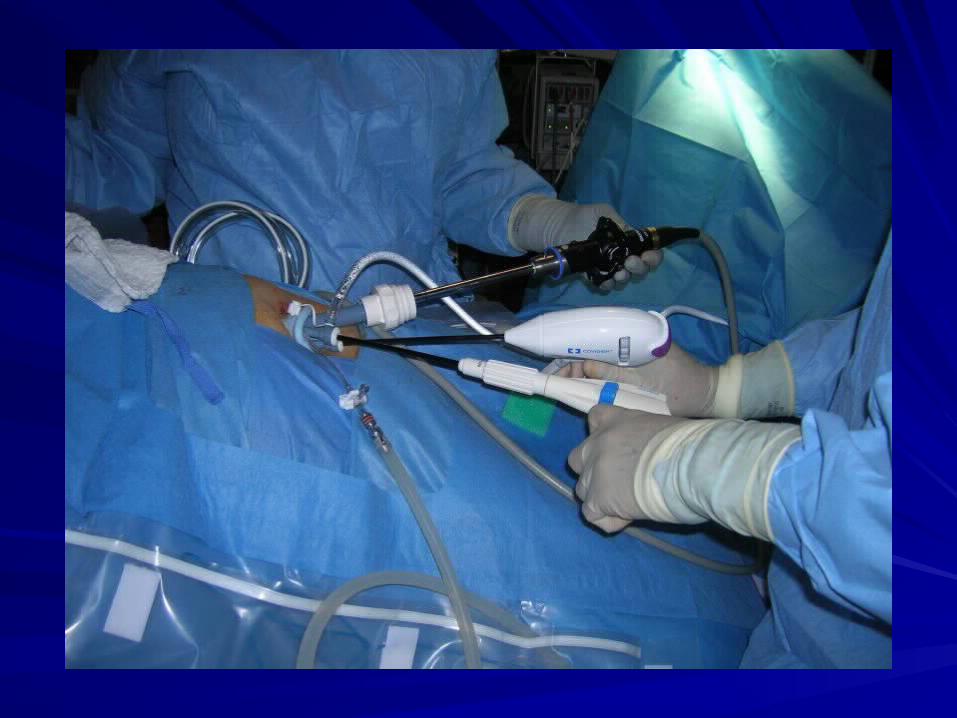
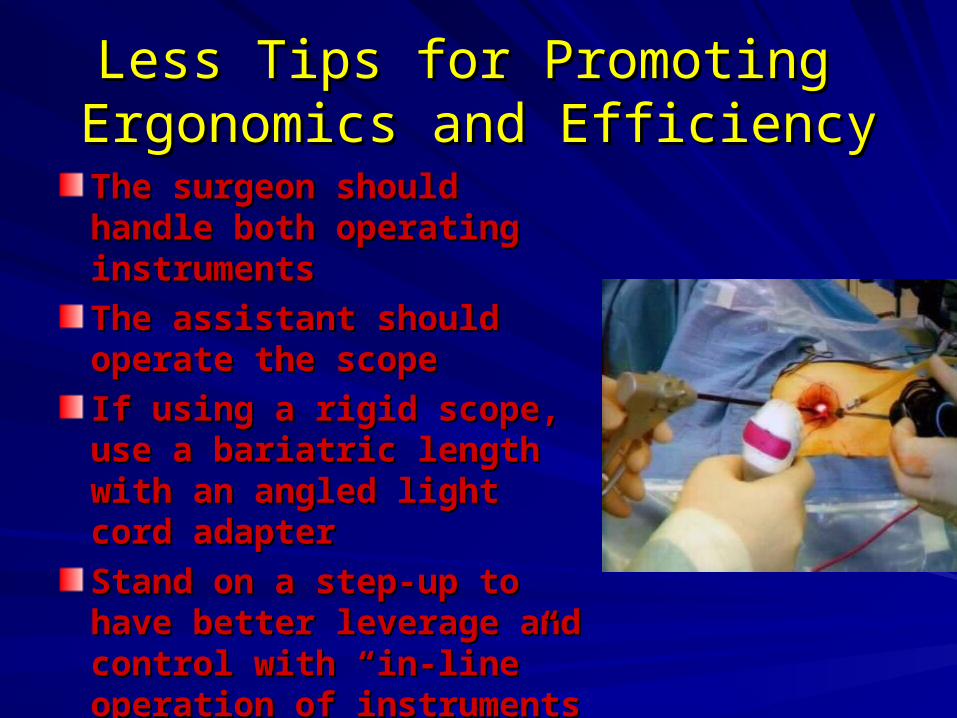
Less Tips for Promoting Less Tips for Promoting Ergonomics and EfficiencyErgonomics and Efficiency
The surgeon should handle The surgeon should handle both operating instrumentsboth operating instruments
The assistant should The assistant should operate the scopeoperate the scope
If using a rigid scope, use a If using a rigid scope, use a bariatric length with an bariatric length with an angled light cord adapterangled light cord adapter
Stand on a step-up to haveStand on a step-up to have better leverage and control better leverage and control with “in-line” operation of with “in-line” operation of instrumentsinstruments

OpticsOptics
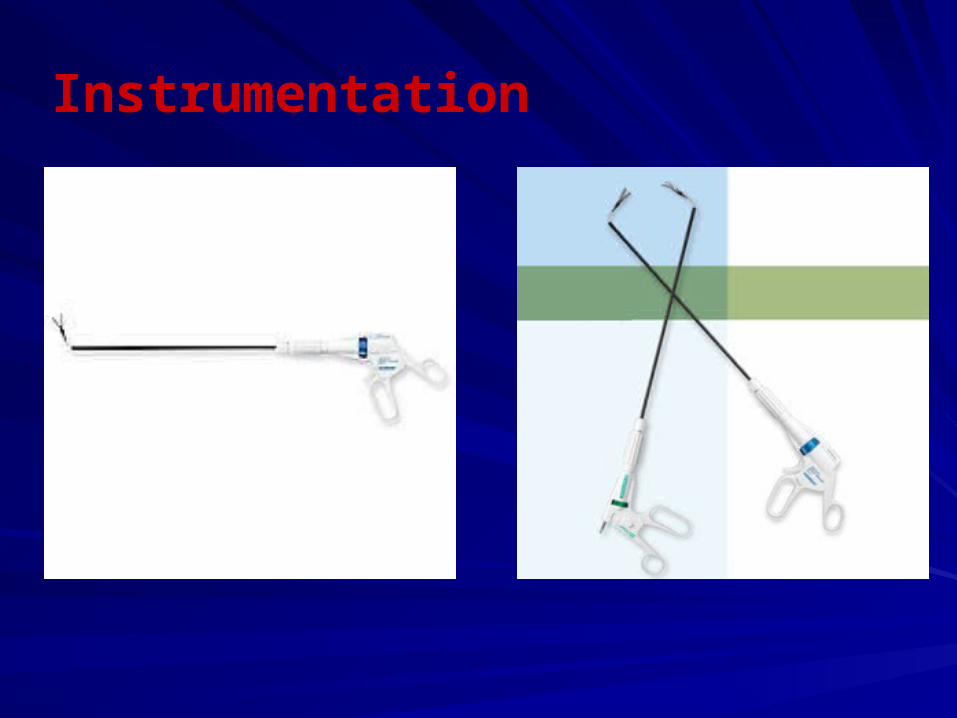
Instrumentation
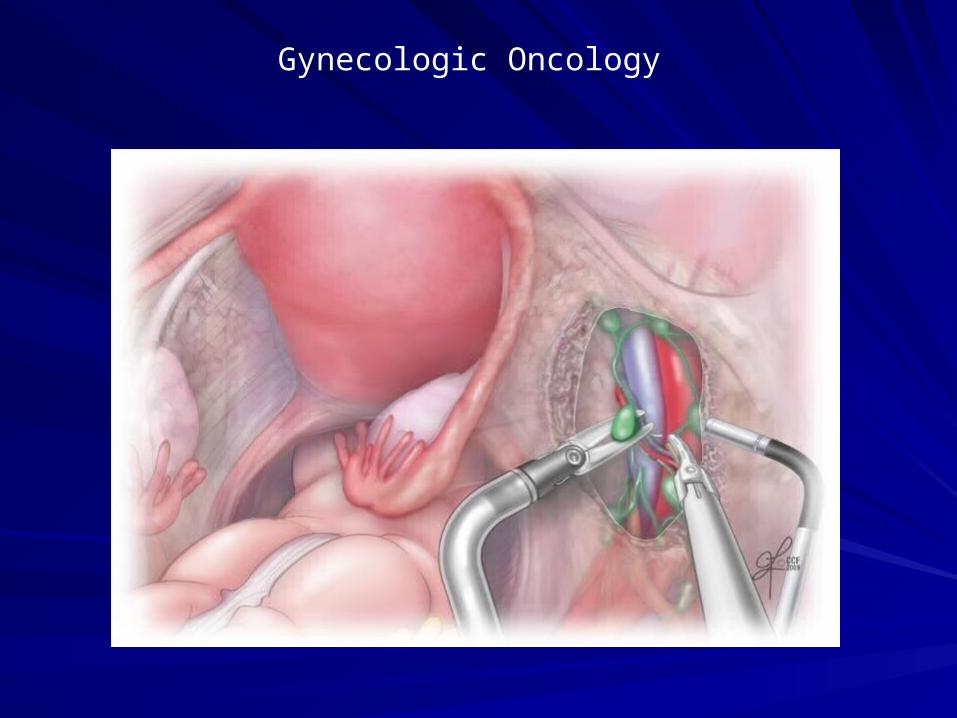
Gynecologic Oncology
RCT: Conventional vs. Single Port RCT: Conventional vs. Single Port HysterectomyHysterectomy
Chen et al April 2011 Obstet GynecolChen et al April 2011 Obstet Gynecol– N=100N=100– Uterine weight 284 gramsUterine weight 284 grams– OR time 122-127 minutesOR time 122-127 minutes– Cuff closed through the vaginaCuff closed through the vagina– Pain score at 24 hours & 48 hours was Pain score at 24 hours & 48 hours was
significantly different ( 3.6 vs. 5.1; 1.9 vs. 2.8)significantly different ( 3.6 vs. 5.1; 1.9 vs. 2.8)– Total Meperidine dose difference 25 mgTotal Meperidine dose difference 25 mg
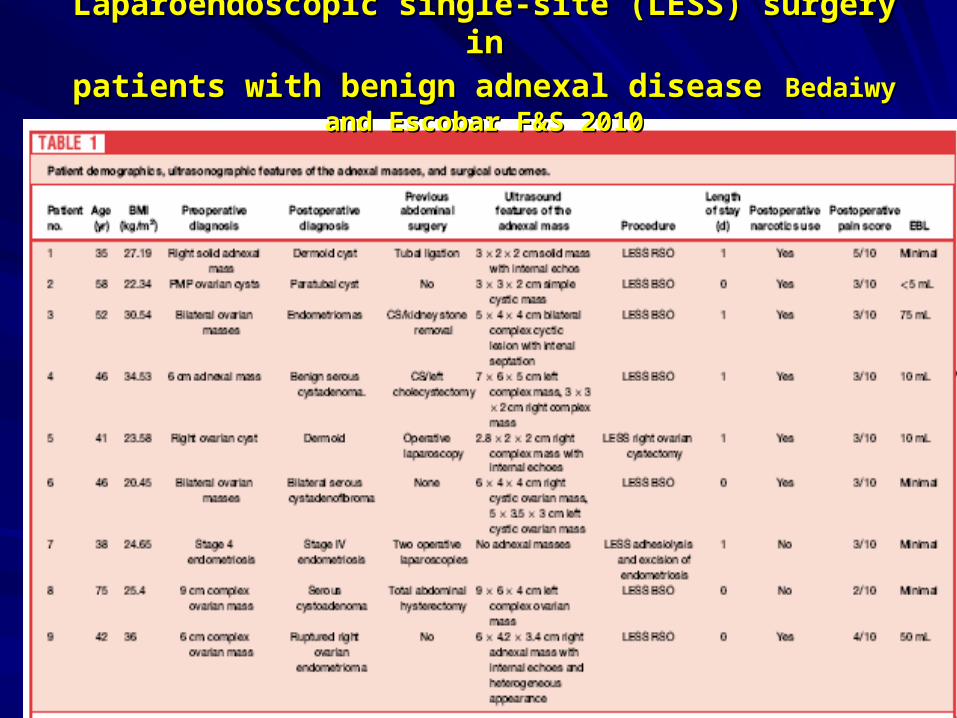
Laparoendoscopic single-site (LESS) surgery inLaparoendoscopic single-site (LESS) surgery in
patients with benign adnexal diseasepatients with benign adnexal disease Bedaiwy and Escobar Bedaiwy and Escobar F&S 2010F&S 2010
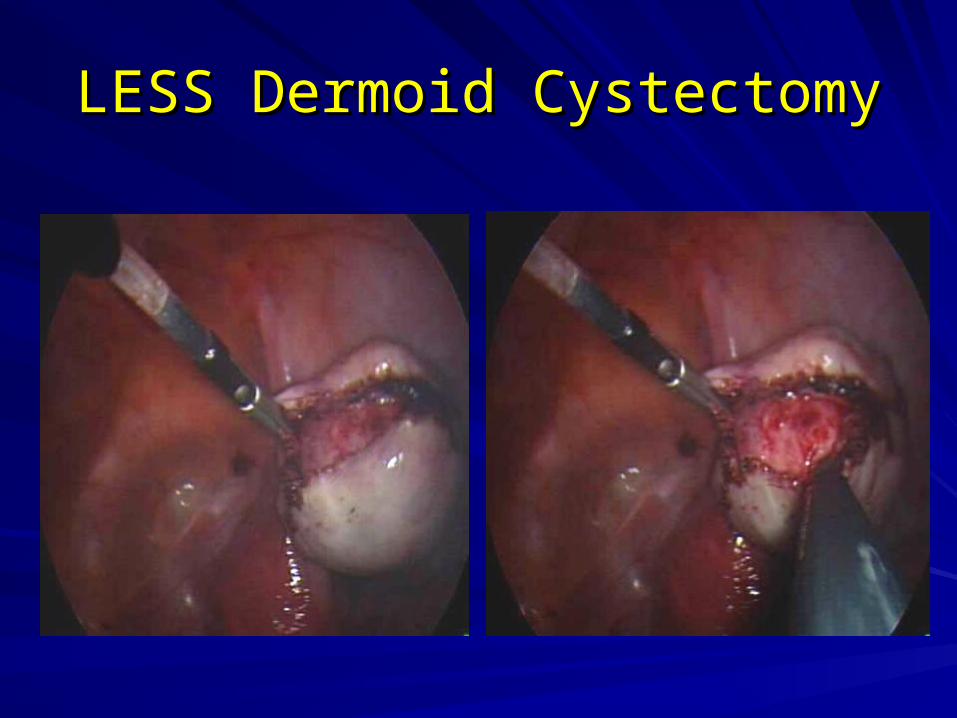
LESS Dermoid CystectomyLESS Dermoid Cystectomy



Women’s Preferences in Minimally Women’s Preferences in Minimally Invasive IncisionsInvasive Incisions
Bush et al JMIG 2011Bush et al JMIG 2011
Preference was traditional 4 puncture Preference was traditional 4 puncture configuration over single site and robotic 5 configuration over single site and robotic 5 puncture techniques.puncture techniques.