Embed Size (px)
Citation preview

Ophthalmic Genetics, 30:13–18, 2009Copyright c© Informa Healthcare USA, Inc.ISSN: 1381-6810 (print) / 1744-5094 (online)DOI: 10.1080/13816810802502970
Lack of Association Between Optineurin Gene VariantsT34T, E50K, M98K, 691 692insAG and R545Q andPrimary Open Angle Glaucoma in Brazilian Patients
Cristiano Caixeta-UmbelinoGlaucoma Service, Department of Ophthalmology, Faculty of Medical Sciences, Irmandade da SantaCasa de Misericordia de Sao Paulo, Sao Paulo, SP, Brazil
Jose Paulo Cabral de Vasconcellos and Vital Paulino CostaGlaucoma Service, Department of Ophthalmology, Faculty of Medical Sciences, University of Campinas- UNICAMP, Campinas, SP, Brazil
Niro Kasahara, Maurıcio Della Paolera, Geraldo Vicente de Almeida,Ralph Cohen, and Carmo Mandia Jr.Glaucoma Service, Department of Ophthalmology, Faculty of Medical Sciences, Irmandade da SantaCasa de Misericordia de Sao Paulo, Sao Paulo, SP, Brazil
Mylene Neves Rocha, Flavio Richeti, and Carlos Alberto LonguiLaboratory of Molecular Medicine, Department of Physiology, Faculty of Medical Sciences, Irmandadeda Santa Casa de Misericordia de Sao Paulo, Sao Paulo, SP, Brazil
Monica Barbosa de MeloLaboratory of Human Molecular Genetics, Center for Molecular Biology and Genetic Engineering(CBMEG), University of Campinas - UNICAMP, Campinas, SP, Brazil.
Purpose: To verify the frequencies of T34T, E50K, M98K, 691 692insAG, and R545Q variantsin the optineurin (OPTN) gene in Brazilian subjects with primary open-angle glaucoma (POAG)and controls. Patients and Methods: Ninety-nine patients with POAG and 100 normal controlswere enrolled in this study. The frequency of alterations in the OPTN gene was analyzed bydirect sequencing and enzymatic digestion of PCR products. Results: None of the five alterationsevaluated was significantly associated with POAG when compared to controls. However, theT34T silent change was present in greater frequency in POAG patients (37.37% vs. 23.00%in controls), while the R545Q change was more prevalent in controls (23.00% vs. 10.10% inPOAG). The M98K and 691 692insAG presented with low frequencies in POAG patients (1.01%and 2.02%, respectively) and controls (2.00% and 2.00%, respectively). The E50K substitutionwas not observed. Conclusion: Our data show no association between the five evaluated variantsand POAG in the Brazilian population.
Keywords Optineurin; variants; mutations; primary open angle glaucoma
INTRODUCTIONGlaucoma is a group of eye disorders characterized by pro-
gressive degeneration of retinal ganglion cells (RGC), resulting
Received 30 July 2008; accepted 21 September 2008.Address correspondence to Monica Barbosa de Melo, Laboratory
of Human Molecular Genetics, Center for Molecular Biology and Ge-netic Engineering (CBMEG), University of Campinas - UNICAMP,Campinas, SP, Brazil, Zip Code: 13083-875 — P.O.Box: 6010. E-mail:[email protected]
in correspondent visual field loss. The process of RGC apoptosisin glaucoma is accelerated compared with the natural age-relatedloss.1
Adult primary open angle glaucoma (POAG) is a major formof glaucoma worldwide. Although its molecular basis is notcompletely understood, it is probably a genetically heteroge-neous disorder attributed to the interaction of multiple genesand environmental influences.2,3 Elevated intraocular pressure(IOP) is a primary risk factor for glaucoma.1 Other risk fac-tors, including family history, age, smoking, and myopia are
13
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 0
8/28
/14
For
pers
onal
use
onl
y.

14 C. CAIXETA-UMBELINO ET AL.
also implicated in the pathogenesis of POAG.4,5 Thirteen locihave been associated with POAG (GLC1A to GLC1M) (MIM —Mendelian Inheritance in Man), and three genes were identified.The first described gene was myocilin (MYOC, MIM 601652),followed by optineurin (OPTN or Optic Neuropathy InducedProtein, MIM 602432) and WD-repeat-containing protein 36(WDR36, MIM 609669). Among the three known genes, onlyMYOC has proven to have a causative role in POAG, whereasthe participation of OPTN and WDR36 is still unclear.6
OPTN was first identified as a gene associated with glaucomaby Rezaie and colleagues in 2002. It is localized on the GLC1Elocus (chromosome 10q15-p14) and is composed by 16 exons,three of which are non-coding (5′UTR), and 13 exons that cod-ify a 577 aminoacid protein. Four sequence alterations in theOPTN gene were described in 16.7% of the families with hered-itary POAG, with most patients presenting with normal tensionglaucoma (NTG). The E50K mutation in exon 4 (458G>A) wasidentified in seven families and segregated in 124 members, in-cluding 38 affected; a mutation in exon 6, characterized by theinsertion of two base pairs “AG” between positions 691 692 seg-regated in a family with normal tension glaucoma (NTG); theR545Q mutation in exon 16 (1944G>A) was present in anotherfamily with NTG; and, finally, a fourth sequence change (M98K)in exon 5 (603T>A), was present in both POAG (13.6%) andcontrols (2.1%).7
Since the pioneering work performed by Rezaie andcolleagues,7 the frequency of OPTN mutations has been evalu-ated in different populations. When these studies are considered,OPTN mutations do not appear to be a common cause of POAG,as observed for the MYOC gene. Although these reports suggesta role for OPTN in glaucoma, its participation is not definitelyproven for all implicated alleles in different populations.8
To our knowledge, the frequency of OPTN mutations has notbeen studied in the Brazilian population. The purpose of thisanalysis was to evaluate the frequency of five OPTN alterationsin Brazilian patients with POAG. These include the variantsreported by Rezaie et al. in 2002 (E50K, M98K, 691 692insAG,R545Q) and the T34T (412G>A) silent change, which has alsobeen shown to be associated with POAG in Japanese patients.9
PATIENTS AND METHODSSamples
The study was approved by Santa Casa de Sao Paulo andState University of Campinas Ethics Committee and adhered tothe tenets of the Declaration of Helsinki. All individuals signedan informed consent in order to participate in the study.
Subjects underwent a complete eye examination and glau-coma patients were included only if they had wide open angleon gonioscopy, typical optic disc changes (localized or diffuseneural rim thinning, disc hemorrhage), typical visual field de-fects, defined according to Hodapp and colleagues10 and IOPhigher than 21 mmHg (individuals who presented with IOPless than 21 mmHg due to clinical or surgical treatment were
also included in the study). Patients with other forms of glau-coma (either secondary or developmental glaucoma) were notincluded.
The control group comprised individuals with IOP ≤ 15mmHg, cup-to-disc ratio ≤ 0.3, absence of localized rim loss,disc hemorrhage or cup/disc asymmetry < 0.2 in both eyesand full visual fields on the FDT screening program. Subjectswith any ocular and systemic disease that might simulate visualfield defects or optic disc atrophy were not included, as well assubjects with a positive family history for glaucoma or blindnessfrom unknown causes.
Mutation ScreeningGenomic DNA was isolated from peripheral leukocyte us-
ing the phenol and chloroform method. OPTN mutations wereevaluated through direct sequencing and restriction fragmentlength polymorphism (RFLP). DNA was amplified by poly-merase chain reaction (PCR) using 4 primer pairs for re-gions 4, 5, 6, and 16, designed based upon OPTN gene se-quence (GenBank accession numbers AF420371 to AF420373)(Invitrogen Life Technologies, Carlsbad, CA, USA), usingthe “primer 3 program,” available at www.broad.mit.edu/cgi-bin/primer/primer3 www.cgi.
A 25 µL reaction volume for PCR included approximately100 ng of genomic DNA, 20 pmol of each primer, 1X enzymebuffer (10X buffer = 20 mM Tris-HCl [pH 8,4], 50 mM KCl,0,01% gelatine), 1,5 mM MgCl2,200 µM nucleotides (dATP,dCTP, dTTP, dGTP), 0.5 U of Taq DNA polymerase (InvitrogenLife Technologies, Carlsbad, CA, USA), and sterile deionizedwater. Samples were amplified on the “MasterCycler EP Gradi-ent S” thermalcycler (Eppendorf, Hamburg, Germany) accord-ing to the following conditions: exon 4 — initial denaturationfor 5 minutes at 94◦C, 35 cycles at 94◦C for 30 seconds, 60◦Cfor 1 minute, 72◦C for 1 minute and 30 seconds with a finalextension at 72◦C for 7 minutes; exons 5, 6 and 16 - initialdenaturation at 94◦C for 5 minutes, followed by 35 cycles at94◦C for 30 seconds, 58◦C for 1 minute, 72◦C for 2 minuteswith a final extension of 72◦C for 7 minutes. Primer sequences,fragment size and annealing temperatures are depicted inTable 1.
After the confirmation of amplification, PCR products en-compassing T34T and E50K variants in exon 4 were analyzedby direct sequencing using the “Big Dye Terminator Cycle Se-quencing Ready Reaction Kit” version 3.1 (Applied Biosystems,Foster City, CA, USA) according to manufacturer’s instruc-tions and electrophoresed in the DNA automatic analyzer “ABIPRISM 310” (Applied Biosystems, Foster City, CA, EUA).M98K (exon 5 - 603T>A), 691 692insAG (exon 6 — prematurestop codon) and R545Q (exon 16 —1944G>A) variants wereevaluated through digestion with StuI, BslI, e BbvI enzymes(New England Biolabs, Ipswich, MA, USA), respectively, ac-cording to manufacturer’s instructions. The results of enzymaticdigestion were compared to positive independent controls fromthe Molecular Ophthalmic Genetics Laboratory, University of
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 0
8/28
/14
For
pers
onal
use
onl
y.

LACK OF ASSOCIATION BETWEEN OPTINEURIN GENE VARIANTS 15
TABLE 1Primer sequences, fragment size and annealing temperature for mutation screening of the OPTN gene
Exon Fragment size (bp) Forward primer sequence Reverse primer sequence AT
4 224 5′ GGGGGACAGCTCTATTTTCA 3′ 5′ CTGCTCACCTTTCAGCTGGT 3′ 60◦C5 218 5′ TCCACTTTCCTGGTGTGTGA 3′ 5′ TTTTCCAAGCTCTTCCTTCAA 3′ 58◦C6 201 5′ ATGGTGCCCAGCCTTAGTTT 3′ 5′ CGCTGGAGTTCAGCTTGAG 3′ 58◦C
16 232 5′ CGCCATCTGTTCTTCAAGTG 3′ 5′ ACCAACAGTTTTGGGGAGGT 3′ 58◦C
bp: base pairs, AT: annealing temperature.
Connecticut Health Center, Farmington, Connecticut, USA, andalso evaluated by direct sequencing for confirmation.
Statistical AnalysisThe frequencies of OPTN gene mutations between patients
and controls were compared using the Chi-square test, correctedby Yates when appropriate. Statistical analysis was performedusing the “Epi Info Version 3.3.2” statistical package software.Statistical significance was assumed at P < 0.05, and significantstatistical associations were corrected by the Bonferroni test formultiple comparisons. The Hardy-Weinberg equilibrium for theobserved frequencies was calculated.
RESULTSThe study group comprised 99 patients with POAG; 46
(46.4%) were female and 53 (53.4%) were male. The controlgroup included 100 subjects: 62 (62.0%) were female, and 38(38.0%) were male. The mean age was 63.6 ± 12.9 years (range:35.0 to 87.0 years) for the POAG patients and 69.0 ± 6.5 years(range: 52.0 to 94.0 years) for the controls. Sixty-eight (68.7%)patients were white, 17 (17.1%) mulatto and 14 (14.1%) wereblack. In the control group, 75 (75.0%) individuals were white,15 (15.0%) mulatto and 10 (10.0%) were black. The mean IOPsat diagnosis for POAG patients were 24 ± 8.5 mmHg for righteyes (RE) and 25 ± 8.4 mmHg for left eyes (LE). In the controlgroup, mean IOPs were 12 ± 2.1 mmHg for RE and 12 ± 1.7for LE. In the POAG group the mean cup-to-disc ratios were0.8 ± 0.2 for RE and 0.8 ± 0.2 for LE, the mean number ofeye surgeries was 1.3 ± 1.2 and the mean number of glaucomamedications was 2.4 ± 1.0.
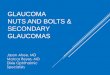
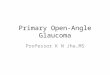
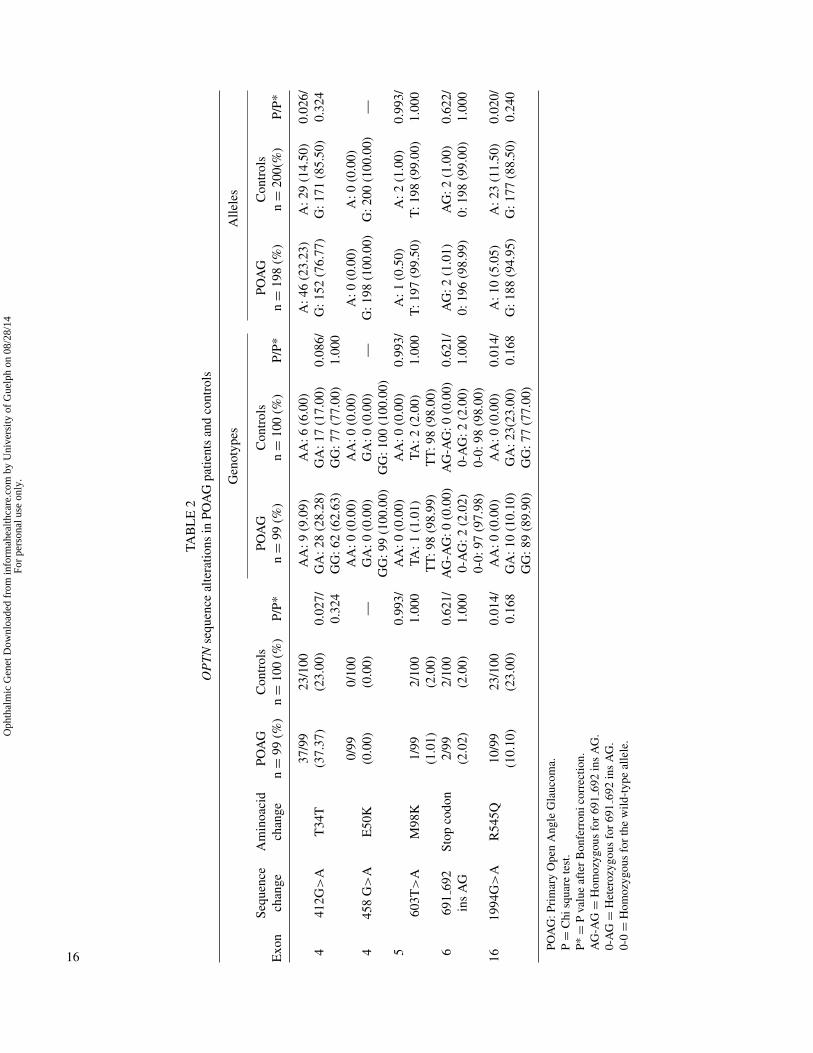
In relation to the distribution of OPTN variants, all data andcomparisons are depicted in Table 2. The E50K mutation wasnot observed in either group. The T34T (412G>A) silent changewas present more frequently in the POAG group than in controls(P = 0.027; Bonferroni adjusted, P = 0.324). No correlation wasobserved between genotypes and the development of POAG, butwhen the alleles were analyzed we can see a tendency of the Aallele to be more frequent in the POAG than in the control group(P = 0.026; Bonferroni adjusted, P = 0.324).
Both the M98K and the 691 692insAG mutations wereequally distributed between groups. However, the R545Q mu-tation was present in a greater frequency in the control groupthan in the POAG group (P = 0.014; Bonferroni adjusted, P =
0.168). Similar results were observed when groups were strat-ified according to genotypes and alleles, showing that the GAgenotype and the A allele were present more frequently in thecontrol group (P = 0.014; Bonferroni adjusted, P = 0.168 andP = 0.020; Bonferroni adjusted, P = 0.240, respectively).
The frequencies of the T34T and R545Q genotypes werein Hardy-Weinberg (HW) equilibrium in the POAG group. Inthe control group, the R545Q genotypes followed HW equilib-rium, but the T34T genotypes did not. The same analysis wasinconclusive for the other variants.
DISCUSSIONPOAG is a complex disease and its molecular basis is at-
tributed to the interaction of multiple genes and environmentalfactors. Although the mechanisms through which alterations inthe OPTN gene lead to glaucoma are not clarified, its expres-sion in the neuronal and ganglion cells of the retina and opticnerve indicates that it could affect retinal ganglion cell survivalby means of interaction with proteins related to the apoptosisprocess.8 Several studies involving different populations havebeen performed in an attempt to find associations between OPTNmutations and POAG/NTG. Since the direct sequencing of theentire gene would be time consuming, this study investigatedthe most frequently reported coding sequence variants in theOPTN gene among glaucoma patients.
The frequency of the T34T silent change was higher in thestudy group than in the control group, but it did not reach sta-tistical significance after Bonferroni correction (P = 0.324), thesame occurring with the higher frequency of the A allele (P =0.324). In a study involving Japanese patients with glaucoma,Funayama et al.9 observed this change in 35.6% of POAG pa-tients, 31.8% of NTG patients and 23.9% of controls. The dif-ference was significant only for POAG patients (P = 0.009).However, other authors, in agreement with our data, could notfind a higher frequency of the T34T alteration when comparedto controls.11–18
In this study, the E50K mutation was not observed in eithergroup, different from the observation of Rezaie and colleagues,7
who found the mutation in 13.5% of glaucoma patients and inno control subject. The authors have included patients with bothPOAG and NTG. Our study is in accordance with several othergroups, who were unable to identify the E50K substitution inthe OPTN gene in different populations,14,17,19–23
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 0
8/28
/14
For
pers
onal
use
onl
y.
TAB
LE
2O
PT
Nse
quen
ceal
tera
tions
inPO
AG
patie
nts
and
cont
rols
Gen
otyp
esA
llele
s
Exo
nSe
quen
cech
ange
Am
inoa
cid
chan
gePO
AG
n=
99(%
)C
ontr
ols
n=
100
(%)
P/P*
POA
Gn
=99
(%)
Con
trol
sn
=10
0(%
)P/
P*PO
AG
n=
198
(%)
Con
trol
sn
=20
0(%
)P/
P*
441
2G>
AT
34T
37/9
9(3
7.37
)23
/100
(23.
00)
0.02
7/0.
324
AA
:9(9
.09)
GA
:28
(28.
28)
GG
:62
(62.
63)
AA
:6(6
.00)
GA
:17
(17.
00)
GG
:77
(77.
00)
0.08
6/1.
000
A:4
6(2
3.23
)G
:152
(76.
77)
A:2
9(1
4.50
)G
:171
(85.
50)
0.02
6/0.
324
445
8G
>A
E50
K0/
99(0
.00)
0/10
0(0
.00)
—A
A:0
(0.0
0)G
A:0
(0.0
0)G
G:9
9(1
00.0
0)
AA
:0(0
.00)
GA
:0(0
.00)
GG
:100
(100
.00)
—A
:0(0
.00)
G:1
98(1
00.0
0)A
:0(0
.00)
G:2
00(1
00.0
0)—
560
3T>
AM
98K
1/99
(1.0
1)2/
100
(2.0
0)
0.99
3/1.
000
AA
:0(0
.00)
TA:1
(1.0
1)T
T:9
8(9
8.99
)
AA
:0(0
.00)
TA:2
(2.0
0)T
T:9
8(9
8.00
)
0.99
3/1.
000
A:1
(0.5
0)T
:197
(99.
50)
A:2
(1.0
0)T
:198
(99.
00)
0.99
3/1.
000
669
169
2in
sA
GSt
opco
don
2/99
(2.0
2)2/
100
(2.0
0)0.
621/
1.00
0A
G-A
G:0
(0.0
0)0-
AG
:2(2
.02)
0-0:
97(9
7.98
)
AG
-AG
:0(0
.00)
0-A
G:2
(2.0
0)0-
0:98
(98.
00)
0.62
1/1.
000
AG
:2(1
.01)
0:19
6(9
8.99
)A
G:2
(1.0
0)0:
198
(99.
00)
0.62
2/1.
000
1619
94G
>A
R54
5Q10
/99
(10.
10)
23/1
00(2
3.00
)0.
014/
0.16
8A
A:0
(0.0
0)G
A:1
0(1
0.10
)G
G:8
9(8
9.90
)
AA
:0(0
.00)
GA
:23(
23.0
0)G
G:7
7(7
7.00
)
0.01
4/0.
168
A:1
0(5
.05)
G:1
88(9
4.95
)A
:23
(11.
50)
G:1
77(8
8.50
)0.
020/
0.24
0
POA
G:P
rim
ary
Ope
nA
ngle
Gla
ucom
a.P
=C
hisq
uare
test
.P*
=P
valu
eaf
ter
Bon
ferr
onic
orre
ctio
n.A
G-A
G=
Hom
ozyg
ous
for
691
692
ins
AG
.0-
AG
=H
eter
ozyg
ous
for
691
692
ins
AG
.0-
0=
Hom
ozyg
ous
for
the
wild
-typ
eal
lele
.
16
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 0
8/28
/14
For
pers
onal
use
onl
y.

LACK OF ASSOCIATION BETWEEN OPTINEURIN GENE VARIANTS 17
The M98K mutation was identified in only one of 99 POAGpatients and in two of 100 controls (P = 1.000). Our results differfrom the observation by Rezaie et al.,7 who found the mutationin 17.8% of glaucoma subjects and in 2.1% of controls. Thisdifference can be explained in part by the fact that the authorsincluded NTG patients in their analysis.
Several studies evaluated the frequency of the M98K variantin POAG patients and controls, however the majority of thesestudies did not reach any statistically significant difference. TheM98K frequency among these POAG patients ranges from 4.5%in a Swedish population to 30.6% in Chinese patients, whereas incontrols it ranged from 4.5% in the French population to 28.8%in Chinese subjects.9,12,15,16,18,19,22,24 Few studies have shownan association between the M98K alteration and POAG. Fuse etal. (2004), evaluating Japanese patients and controls, observed asignificantly higher frequency of this mutation in POAG patients(16.9%) than in controls (5.0%) (P = 0.09).14 Willoughby et al.11
reported a frequency of 16.3% of this mutation in a mixedpopulation of POAG patients and 3.9% in controls (P = 0.02).Independently of the absence of association between this changeand POAG, our numbers indicate that this is a rare variant in ourpopulation.
The premature stop codon (691 692insAG) mutation in exon6 was present in a low frequency in this study (2.0% in bothgroups, P = 1.000). This observation, in part, agrees with theresults of Rezaie et al.,7 who found the mutation in only oneglaucoma patient (2.2%) and in no subject pertaining to thecontrol group. Other studies were not able to find this changein either POAG patients or controls.14,19,20,23 However, its pres-ence in two individuals belonging to the control group raises adiscussion regarding its functional consequence.
Although this alteration creates a premature stop codon,truncating the protein by 76%,7 the remaining product mightmaintain its properties. Also, mutations in other genes and/orenvironmental factors could be modulating OPTN function. Thisobservation strengthens the need of functional analysis, as ex-pression studies and intracellular localization by immunocyto-chemistry, that could guide researchers to a better comprehen-sion of the role of this insertion.
In our study, the R545Q mutation in exon 16 was observed in10.1% of glaucoma patients and 23.0% of controls, results notstatistically significant after Bonferroni correction, (P = 0.168).This is in agreement with several previous studies that evalu-ated POAG patients and observed similar frequencies betweenpatients and controls.9,11,12,14,16,18,19,21,23 The exception is thestudy reported by Mukhopadhyay et al.16 in Indian patients withPOAG, which identified the R545Q mutation in 3% of glaucomapatients and in no normal control (P < 0.05). In opposition toE50K and M98K, which were rare sequence variants in our pop-ulation, the R545Q was present in a relatively high frequencycompared to other studies.
In summary, there was no significant association betweenthe evaluated coding sequence alterations in the OPTN gene inPOAG Brazilian patients. One of the limitations of this study is
that we did not include NTG patients in our analysis. Althoughmost studies observe OPTN gene variations associated withNTG, this analysis is difficult to be performed in the Brazilianpopulation, due to the small number of patients with this condi-tion in our country, as observed by Urbano et al. who found 3%of NTG among 329 glaucoma patients.25 POAG is a complexdisease, in which different genes, associated to environmentalinteractions, may contribute in a greater or lesser extension tothe development of the glaucomatous damage depending on theethnic background. This equation explains why the frequencyof OPTN mutations is variable among different studies.
ACKNOWLEDGMENTSThe authors would like to thank Mansoor Sarfarazi and
Tayebeh Rezaie from the Molecular Ophthalmic Genetics Labo-ratory, University of Connecticut, and Rodrigo Secolin from theMolecular Genetics Laboratory, Department of Medical Genet-ics, FCM - UNICAMP for their contribution to this work. Thisstudy was supported by grants from FAP-SCSP and FAPESP(02/11575-0).
DECLARATION OF INTERESTThe authors report no conflicts of interest. The authors alone
are responsible for the content and writing of the paper.
REFERENCES1. Weinreb RN. Glaucoma neuroprotection: What is it? Why is it
needed? Can J Ophthalmol. 2007;42:396–398.2. Raymond V. Molecular genetics of the glaucomas: mapping of the
first five “GLC” loci. Am J Hum Genet. 1997;60:272–277.3. Sarfarazi M. Recent advances in molecular genetics of glaucomas.
Hum Mol Genet. 1997;6:1667–1677.4. Wilson MR, Hertzmark E, Walker AM, Childs-Shaw K, Epstein
DL. A case-control study of risk factors in open angle glaucoma.Arch Ophthalmol. 1987;105:1066–1071.
5. Drance S. Chronic open angle glaucoma: risk factors in additionto intraocular pressure. Acta Ophthalmol Scand. 2001;79:545.
6. Monemi S, Spaeth G, DaSilva A, Popinchalk S, Ilitchev E, Lieb-mann, Ritch R, Heon E, Crick RP, Child A, Sarfarazi M. Iden-tification of a novel adult-onset primary open glaucoma (POAG)gene on 5q22.1. Hum Mol Genet. 2005;14:725–733.
7. Rezaie T, Child A, Hitchings R, Brice G, Miller L, Coca-PradosM, Heon E, Krupin T, Ritch R, Kreutzer D, Crick RP, Sarfarazi M.Adult-onset primary open-angle glaucoma caused by mutations inoptineurin. Science. 2002;295:1077–1079.
8. Libby RT, Douglas B. Gould DB, Anderson MG, John SM. Com-plex Genetic of Glaucoma Susceptibility. Annu Rev Genomics HumGenet. 2005;6:15–44.
9. Funayama T, Ishikawa K, Ohtake Y, Tanino T, Kurosaka D,Kimura I, Suzuki K, Ideta H, Nakamoto K, Yasuda N, Fujimaki T,Murakami A, Asaoka R, Hotta Y, Tanihara H, Kanamoto T,Mishima H, Fukuchi T, Abe H, Iwata T, Shimada N, Kudoh J,Shimizu N, Mashima Y. Variants in optineurin gene and theirassociation with tumor necrosis factor-alpha polymorphisms inJapanese patients with glaucoma. Invest Ophthalmol Vis Sci.2004;45:4359–4367.
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 0
8/28
/14
For
pers
onal
use
onl
y.

18 C. CAIXETA-UMBELINO ET AL.
10. Hodapp E; Parrish RK II, Anderson DR: Clinical decisions inglaucoma. St Louis, The C.V, Mosby Co., 1993. pp.52–61.
11. Willoughby CE, Chan LL, Herd S, Billingsley G, Noordeh N,Levin AV, Buys Y, Trope G, Sarfarazi M, Heon E. Defining thepathogenicity of optineurin in juvenile open-angle glaucoma. In-vest Ophthalmol Vis Sci. 2004;45:3122–3130.
12. Fan BJ, Wang DY, Fan DS, Tam PO, Lam DS, Tham CC, LamCY, Lau TC, Pang CP. SNPs and interaction analyses of myocilin,optineurin, and apolipoprotein E in primary open angle glaucomapatients. Mol Vis. 2005;11:625–631.
13. Tang S, Toda Y, Kashiwagi K, Mabuchi F, Iijima H, TsukaharaS, Yamagata Z. The association between Japanese primary open-angle glaucoma and normal tension glaucoma patients and theoptineurin gene. Hum Genet. 2003;113:276–279.
14. Fuse N, Takahashi K, Akiyama H, Nakazawa T, Seimiya M, Kuwa-hara S, Tamai M. Molecular genetic analysis of optineurin gene forprimary open-angle and normal tension glaucoma in the Japanesepopulation. J Glaucoma. 2004;13:299–303.
15. Jansson M, Wadelius C, Rezaie T, Sarfarazi M. Analysis of rarevariants and common haplotypes in the optineurin gene in Swedishglaucoma cases. Ophthalmic Genet. 2005;26:85–89.
16. Mukhopadhyay A, Komatireddy S, Acharya M, Bhattacharjee A,Mandal AK, Thakur SK, Chandrasekhar G, Banerjee A, ThomasR, Chakrabarti S, Ray K. Evaluation of Optineurin as a candidategene in Indian patients with primary open angle glaucoma. MolVis. 2005;11:792–797.
17. Hauser MA, Sena DF, Flor J, Walter J, Auguste J, Larocque-Abramson K, Graham F, Delbono E, Haines JL, Pericak-VanceMA, Rand Allingham R, Wiggs JL. Distribution of optineurinsequence variations in an ethnically diverse population of low-tension glaucoma patients from the United States. J Glaucoma.2006;15:358–363.
18. Leung YF, Fan BJ, Lam DS, Lee WS, Tam PO, Chua JK, ThamCC, Lai JS, Fan DS, Pang CP. Different optineurin mutation pat-tern in primary open-angle glaucoma. Invest Ophthalmol Vis Sci.2003;44:3880–3884.
19. Toda Y, Tang S, Kashiwagi K, Mabuchi F, Iijima H, Tsukahara S,Yamagata Z. Mutations in the optinurin gene in Japanese patientswith primary open angle glaucoma and normal tension glaucoma.Am J Med Genet A. 2004;125A:1–4.
20. Baird PN, Foote SJ, Mackey DA, Craig J, Speed TP, Bureau A.Evidence for a novel glaucoma locus at chromosome 3p21-22.Hum Genet. 2005;117:249–257.
21. Alward WL, Kwon YH, Kawase K, Craig JE, Hayreh SS, JohnsonAT, Khanna CL, Yamamoto T, Mackey DA, Roos BR, AffatigatoLM, Sheffield VC, Stone EM. Evaluation of optineurin sequencevariations in 1048 patients with open angle glaucoma. Am J Oph-thalmol. 2003;136:904–910.
22. Aung T, Rezaie T, Okada K, Viswanathan AC, Child AH, BriceG, Bhattacharya SS, Lehmann OJ, Sarfarazi M, Hitchings RA.Clinical features and course of patients with glaucoma with theE50K mutation in the optineurin gene. Invest Ophthalmol Vis Sci.2005;46:2816–2822.
23. Weisschuh N, Neumann D, Wolf C, Wissinger B, Gramer E.Prevalence of myocilin and optineurin sequence variants in Ger-man normal tension glaucoma patients. Mol Vis. 2005;11:284–287.
24. Melki R, Belmouden A, Akhayat O, Brezin A, Garchon HJ. TheM98K variant of the OPTINEURIN (OPTN) gene modifies initialintraocular pressure in patients with primary open angle glaucoma.J Med Genet. 2003;40:842–844.
25. Urbano AP, Freitas TG, Arcieri ES, Urbano AP, Costa VP.Avaliacao dos tipos de glaucoma no Servico de Oftalmologia daUnicamp. Arq Bras Oftalmol. 2001;64:P052 [Abstract].
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 0
8/28
/14
For
pers
onal
use
onl
y.