Embed Size (px)
Citation preview

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 1 of 109 Last printed 05/02/2020 12:10:00
Division of Laboratory Medicine
Wythenshawe Hospital
Laboratory Medicine Handbook
Table of Contents
Table of Contents............................................................................................................... 1
1 Introduction .............................................................................................................. 5
1.1 Accreditation .................................................................................................................... 5
1.2 Quality assurance ............................................................................................................ 6
1.3 Key performance indicators ............................................................................................. 7
1.4 Protection of personal information ................................................................................... 7
1.5 Patient information ........................................................................................................... 7
1.6 Sample acceptance ......................................................................................................... 7 1.6.1 Samples failing acceptance criteria ......................................................................................... 7 1.6.2 Exceptions ............................................................................................................................... 8 1.6.3 Two-Sample Rule .................................................................................................................... 8 1.6.4 Patient consent ........................................................................................................................ 9
1.7 Requesting and reporting of laboratory tests ................................................................... 9
1.8 What to do when there is an IT failure ............................................................................. 9
1.9 Sample containers ........................................................................................................... 9
1.10 Sample transportation ................................................................................................... 11 1.10.1 Hospital requirements ....................................................................................................... 12 1.10.2 GP requirements ............................................................................................................... 12 1.10.3 Postal samples .................................................................................................................. 12
1.11 Requesting further tests on samples already in the laboratory (‘add-on’ tests) .............. 12 1.11.1 Biochemistry ...................................................................................................................... 12 1.11.2 Haematology ..................................................................................................................... 12 1.11.3 Mycology Reference Centre .............................................................................................. 12
1.12 Turnaround times .......................................................................................................... 13
How to use this document:
Do not print it. It may change, the most up-to-date version will always be available on the Trust
internet/intranet
Click on items in this table of contents to navigate to the required section
Click to navigate between sections / open hyperlinks in a browser / email addresses to send a message
Use bookmarks in the navigation pane in your PDF viewer to move around the document
Ctrl +F to perform a word search
Click for an A-Z list of tests

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 2 of 109 Last printed 05/02/2020 12:10:00
1.13 Complaints or comments ............................................................................................... 13
2 DLM general contact details ................................................................................. 13
3 Phlebotomy ............................................................................................................ 14
3.1 Inpatient service ............................................................................................................ 14
3.2 Outpatient service .......................................................................................................... 14
3.3 General Practitioner service .......................................................................................... 14
4 Sample reception ................................................................................................... 16
5 Biochemistry .......................................................................................................... 17
5.1 Contact details ............................................................................................................... 18
5.2 Working hours ............................................................................................................... 18 5.2.1 Outside routine hours ............................................................................................................ 18
5.3 Urgent Requests............................................................................................................ 19
5.4 Examinations offered by Biochemistry ........................................................................... 19
5.5 Sample transportation ................................................................................................... 20
5.6 Add-on Tests ................................................................................................................. 20
5.7 Sample Information ....................................................................................................... 20
5.8 Test library ..................................................................................................................... 21
5.9 Factors known to significantly affect performance of tests/interpretation of results ........ 54
5.10 Effect of haemolysis, lipaemia and icterus: .................................................................... 55
5.11 Measurement uncertainty .............................................................................................. 55
5.12 Point of Care ................................................................................................................. 55
6 Haematology .......................................................................................................... 56
6.1 Contact details ............................................................................................................... 56
6.2 Routine Haematology .................................................................................................... 57 6.2.1 Test library ............................................................................................................................. 57
6.3 Coagulation ................................................................................................................... 61 6.3.1 Test library ............................................................................................................................. 61 6.3.2 Factors affecting the results or processing of coagulation tests ........................................... 62
6.4 Immunology ................................................................................................................... 62 6.4.1 Immunology test library ......................................................................................................... 63
6.5 Blood transfusion ........................................................................................................... 63 6.5.1 Two sample rule .................................................................................................................... 63 6.5.2 Test library ............................................................................................................................. 64
7 Cellular Pathology ................................................................................................. 67
7.1 Contact details ............................................................................................................... 67
7.2 General information ....................................................................................................... 69
7.3 Sample acceptance ....................................................................................................... 69
7.4 Clinical information ........................................................................................................ 69
7.5 Sample containers ......................................................................................................... 70

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 3 of 109 Last printed 05/02/2020 12:10:00
7.6 Histology sample collection ........................................................................................... 71
7.7 Supply of sample containers .......................................................................................... 71
7.8 Factors that prevent a detailed accurate diagnosis ........................................................ 71
7.9 Frozen sections ............................................................................................................. 71 7.9.1 Booking cardiothoracic frozen section requests .................................................................... 71 7.9.2 Booking other frozen section requests .................................................................................. 71 7.9.3 Once specimen has been taken ............................................................................................ 72
7.10 Bone Marrow Trephine specimens. ............................................................................... 72
7.11 Skin immunofluorescence specimens ............................................................................ 72
7.12 Oral immunofluorescence specimens ............................................................................ 72
7.13 Amputated limb specimens ............................................................................................ 73
7.14 Cytology samples .......................................................................................................... 73 7.14.1 Broncho-alveolar lavages (BAL) ....................................................................................... 76 7.14.2 Endobronchial ultrasound guided aspirate specimens (EBUS) ........................................ 76 7.14.3 Joint Fluids ........................................................................................................................ 76
7.15 Cervical Cytology ........................................................................................................... 76
7.16 Andrology ...................................................................................................................... 76 7.16.1 Infertility ............................................................................................................................. 76 7.16.2 Post vasectomy ................................................................................................................. 77
7.17 Sample transport ........................................................................................................... 79
7.18 Reports .......................................................................................................................... 80
7.19 RCPath cancer standards and data sets ....................................................................... 80
7.20 Multidisciplinary Team Meetings (MDT’s) ...................................................................... 81
7.21 Turnaround times .......................................................................................................... 81
7.22 Material sent away for further tests ................................................................................ 81
7.23 Return of tissues............................................................................................................ 81
7.24 Disposal of tissues ......................................................................................................... 82
7.25 Errors happen ................................................................................................................ 82
7.26 Manchester Cancer Research Centre Tissue Bank ....................................................... 82
7.27 Measurement uncertainty .............................................................................................. 82
8 Mortuary ................................................................................................................. 83
8.1 Contact details ............................................................................................................... 83
8.2 Opening hours: .............................................................................................................. 83
8.3 Adult post mortems ........................................................................................................ 83
8.4 Infectious bodies............................................................................................................ 85
8.5 Medical Devices ............................................................................................................ 85 8.5.1 Pacemakers and defibrillators ............................................................................................... 85 8.5.2 Fixion
TM intramedullary nails .................................................................................................. 85
8.6 Stillbirths and foetuses, post mortems and disposal ...................................................... 85 8.6.1 Wythenshawe Hospital patients ............................................................................................ 85 8.6.2 Tameside patients ................................................................................................................. 86
9 Microbiology .......................................................................................................... 87

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 4 of 109 Last printed 05/02/2020 12:10:00
9.1 Urgent requests out of hours ............................................ Error! Bookmark not defined.
9.2 Contact details .................................................................. Error! Bookmark not defined.
10 Mycology Reference Centre, Manchester ............................................................ 88
10.1 Contact Details .............................................................................................................. 88
10.2 Additional Tests ............................................................................................................. 89
10.3 Measurement Uncertainty .............................................................................................. 89
10.4 Antifungal Drug Levels................................................................................................... 89 10.4.1 Indications for monitoring .................................................................................................. 89
10.4.2 References ..................................................................................................................... 89
10.5 Identification and susceptibility testing of medically important fungi ............................... 89
11 Appendix A – A-Z List of tests ............................................................................ 103
Standards covered by this document:
ISO 15189:2012 5.4.2 Information for patients and users
MHRA QMS
specifications 5.4.1 There is an up to date user manual
HTA 2004

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 5 of 109 Last printed 05/02/2020 12:10:00
1 Introduction
The Division of Laboratory Medicine (DLM) at Manchester University NHS Foundation Trust (MFT)
Wythenshawe Hospital provides diagnostic services to Wythenshawe and Withington Hospitals as
well as General Practitioner surgeries in the South Manchester area and beyond. The Histopathology
Department also provide a service to Tameside and Glossop Integrated Care Organisation. There
are four departments within Division of Laboratory Medicine based at Wythenshawe Hospital;
Biochemistry, Haematology, Cellular Pathology (including provision of mortuary services), and the
Mycology Reference Centre Manchester (MRCM).
Laboratory Medicine (except MRCM) is housed in the Clinical Sciences Building on the
Wythenshawe Hospital site, shown in the bottom right corner of the map below. The Mycology
Reference Centre is based in the Education and Research Centre; also shown below, in orange.
This handbook relates to DLM services located at Wythenshawe Hospital. Information on laboratory
medicine services located at the Oxford Road Campus can be found here. The Microbiology
laboratory is based at the Oxford Road Campus.
1.1 Accreditation
Each department within Laboratory Medicine has undergone external accreditation by the United
Kingdom Accreditation Service, UKAS. Current accreditation status can be checked on the UKAS
website, using the UKAS numbers in the table. The accreditation process requires annual inspection
to ensure there is a system of quality management in place to give assurance that the results
released and advice given by the laboratory are of a high standard.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 6 of 109 Last printed 05/02/2020 12:10:00
Laboratory UKAS Number
Biochemistry 9063
Haematology 9072
Histopathology 9083
Microbiology 8393
Mycology 10196
The Blood Transfusion laboratory, also known as blood bank, conforms to the UK Blood Safety and
Quality Regulations and is deemed compliant with these by the Medicines & Healthcare products
Regulatory Agency (MHRA). This compliance is assessed annually.
In England, Wales and Northern Ireland, mortuaries where post-mortem examinations take place are
licensed and inspected by the Human Tissue Authority (HTA). The HTA help mortuaries improve the
standard of care they provide, so the public can have confidence that deceased people are treated
with dignity and respect. The mortuary at MFT Wythenshawe is licenced by the HTA and is inspected
on a regular basis to ensure we are complying with all the relevant regulations.
1.2 Quality assurance
Test performed in the laboratories are enrolled either in a national/international External Quality
Assurance (EQA) scheme or a similar local scheme where no national scheme is available. This
ensures that our tests are performing well. We also use Internal Quality Assurance (IQA) and
Internal Quality Control (IQC) to monitor the performance of our tests.
Our clinical and some scientific staff are also enrolled on proficiency testing EQA schemes, where
they are tested on their interpretation of case studies involving pathology test results. This ensures
that the reports issued are correctly interpreted and the right advice is given.
Each laboratory is approved by the Institute of Biomedical Science for training of Biomedical
Scientists, which has its own quality assurance programme.
The Biochemistry and Histopathology Departments at Wythenshawe Hospital are recognised for
training Specialty Trainees (STs) in each discipline. The training programmes are recognised and
approved by the Royal College of Pathologists (and the General Medical Council) and are quality-
assured by Health Education England North West. The Biochemistry and Mycology departments are
approved training centres for the Scientific Trainee Programme (STP), which is accredited by the
National School of Healthcare Science.
As part of this training approval we have comprehensive training programmes for all grades of staff to
ensure that they have all the required knowledge and skills to perform their duties to the highest
level. This includes the provision of expert clinical advice to our users and interpretive comments on
reports.
We also have Quality Managers within the laboratories who are employed to oversee all aspects of
quality and ensure that we meet the requirements of our accrediting and regulatory bodies.
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 7 of 109 Last printed 05/02/2020 12:10:00
1.3 Key performance indicators
We use Key Performance Indicators (KPIs) to monitor the quality of the service we provide. There is
a Laboratory Medicine dashboard that contains all of these KPIs, which is reviewed monthly to
ensure we are performing to the required standard.
1.4 Protection of personal information
The laboratory adheres to the Trust-wide Policies on information governance for the protection of
patient information, including the Trust “Data Protection Policy”.
1.5 Patient information
The Pathology Handbook is available to patients online.
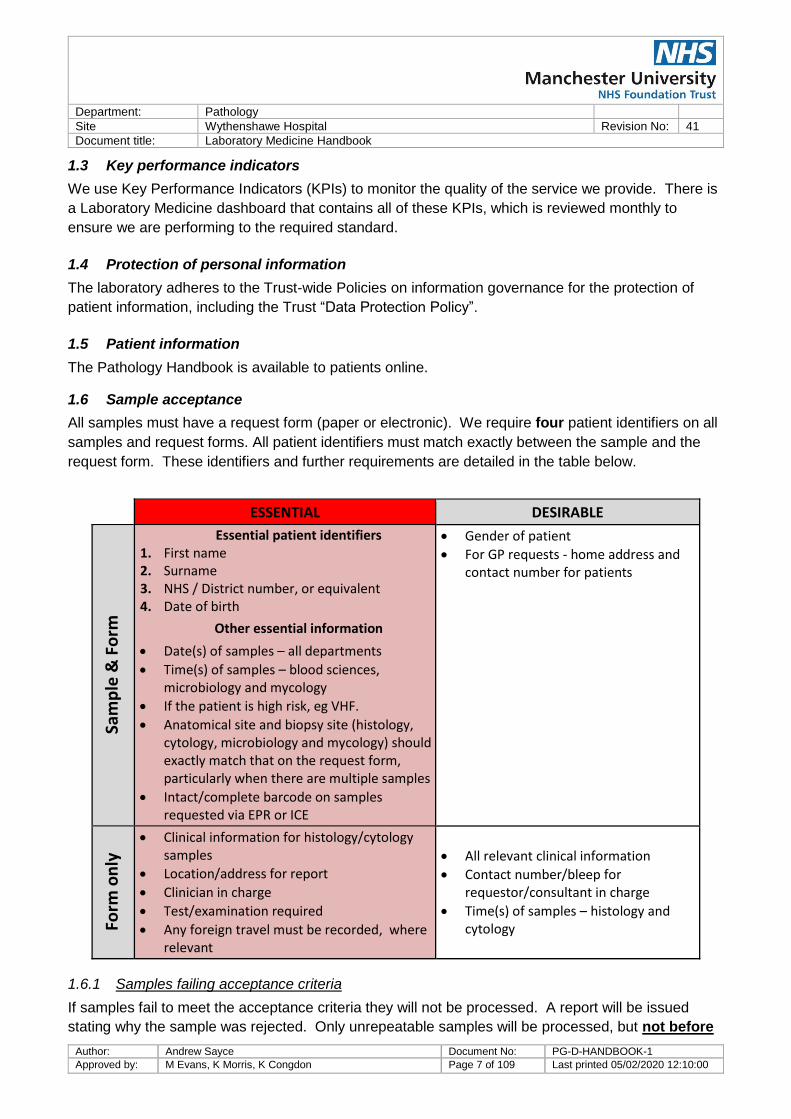
1.6 Sample acceptance
All samples must have a request form (paper or electronic). We require four patient identifiers on all
samples and request forms. All patient identifiers must match exactly between the sample and the
request form. These identifiers and further requirements are detailed in the table below.
ESSENTIAL DESIRABLE
Sam
ple
& F
orm
Essential patient identifiers 1. First name 2. Surname 3. NHS / District number, or equivalent 4. Date of birth
Other essential information
Date(s) of samples – all departments
Time(s) of samples – blood sciences, microbiology and mycology
If the patient is high risk, eg VHF.
Anatomical site and biopsy site (histology, cytology, microbiology and mycology) should exactly match that on the request form, particularly when there are multiple samples
Intact/complete barcode on samples requested via EPR or ICE
Gender of patient
For GP requests - home address and contact number for patients
Form
on
ly
Clinical information for histology/cytology samples
Location/address for report
Clinician in charge
Test/examination required
Any foreign travel must be recorded, where relevant
All relevant clinical information
Contact number/bleep for requestor/consultant in charge
Time(s) of samples – histology and cytology
1.6.1 Samples failing acceptance criteria
If samples fail to meet the acceptance criteria they will not be processed. A report will be issued
stating why the sample was rejected. Only unrepeatable samples will be processed, but not before

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 8 of 109 Last printed 05/02/2020 12:10:00
the requestor has attended the relevant laboratory to complete a “Specimen Labelling Amendment
Form”. This form becomes part of the patient’s record.
Examples of unrepeatable samples:
Sterile body fluids (ie peritoneal, CSF, pleural)
Bone marrow
Fine needle aspirates (FNA)
Tissue biopsies/surgical specimens/cytology samples (with the exception of sputum, urine and
andrology samples)
Blood cultures
Mycology isolates from any of the above specimens
Bronchoscopy/endoscopy specimens
Drug levels timed for treatment (peak and trough), as well as any from neonatal patients
Blood samples from patients with no venous access (ie femoral stabs)
Arterial samples
All other samples will be rejected if they fail to meet the acceptance criteria. It is in everyone’s
interest, particularly the patients’, that all samples and forms are correctly labelled before they are
sent to the laboratory.
Please do not use addressograph labels on blood tubes or other small containers. These stickers
are too large and the extra bulk they add means the samples will not pass through the automated
analysers in the laboratories. Small labels can be used, except for transfusion samples.
1.6.2 Exceptions
In certain circumstances, patient identification details are intentionally hidden or substituted with
particular ID numbers (e.g. Sexual Health, Clinical trials, donor samples) in such instances, a
properly coded identifier must be used.
During a major incident, patients presenting through A&E will be allocated a MAJAX identification.
This consists of a MAJAX number in the place of a district number, forename number in text format
(e.g. THIRTEEN) and a surname from the phonetic alphabet with a MAJAX pre-fix (MAJAX HOTEL).
1.6.3 Two-Sample Rule
In line with current BCSH guidelines, two samples will be required to determine the blood group of a
patient before cross-matched components are released. If a patient has a historical blood group on
record, just one sample for the current request is required.
Any patient that does not have a Transfusion history (a known Blood Group on the laboratory
computer system) will require a second Group and Antibody Screen. The Transfusion Laboratory will
inform the clinician if a second sample is required. Two samples (with two separate request forms)
are required. These samples should be taken by two different people, or if bled by the same person
must be taken at a different time e.g. two independent separate phlebotomies.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 9 of 109 Last printed 05/02/2020 12:10:00
1.6.4 Patient consent
It is important that as well as the above, patient and family information is provided on the request
form, where relevant (e.g. for interpreting genetic examination results). We may have to refer
samples for testing to other laboratories if we are unable to perform the testing in-house. In these
cases we will have to send patient identifiers, such as name, date of birth and the clinical details we
have been given to enable these laboratories to perform appropriate testing and interpret results
correctly.
The patient presenting to the point of sample collection, or providing a sample themselves to their
healthcare provider implies consent. The individual requesting the tests has responsibility for
obtaining informed consent for these tests. Informed consent should cover all the tests requested,
the implications of any results and that personal details and clinical information will be shared with
the requesting organisation and any other organisations involved in providing the tests and results.
1.7 Requesting and reporting of laboratory tests
Electronic requesting must be used to request pathology investigations where it is available. Hand
written requests are more prone to sample labelling errors, transcription errors, sample collection
errors and reporting errors. Do not use hand written requests unless absolutely necessary.
Handwritten request forms are accepted in Histology because these have been designed to allow
annotation of anatomical diagrams.
Each request accepted by the laboratory for examination(s) shall be considered an agreement.
1.8 What to do when there is an IT failure
When there is a failure of the electronic requesting system and it is not possible to request pathology
tests electronically, handwritten request forms can be used. If required, blank request forms can be
sent from the laboratory via the pneumatic tube system. Wards should take the forms they need and
leave a stock of forms next to the pod station for other departments to use. If you require more
forms, please call the laboratory on ext. 4765.
Critical/urgent results will be telephoned by Laboratory staff to the requesting departments. Please
leave the Laboratory phone lines free for us to do this and do not contact us unnecessarily during
these times.
1.9 Sample containers
BD/Becton Dickinson sample collection tubes are used for adults and Sarstedt for paediatric patients.
The lid colours are shown in the table below.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 10 of 109 Last printed 05/02/2020 12:10:00
Container type Colour Description Use
Fluoride
Grey Fluoride oxalate
Blood glucose
Ethanol
Lactate
Serum gel
Gold Serum gel
Routine biochemistry
Immunology
Please note these tubes MUST
NOT be used for mycology
tests
EDTA
(4ml tube)
Purple EDTA
Haematology
HbA1c
Immunology
Li Hep
Green Lithium heparin
gel
Serum
Red Clotted
Bacteriology
Viral serology
Immunology
Mycology
Some transfusion tests
EDTA
Pink EDTA
Blood group
Cross match
Please note these tubes MUST
NOT be used for routine
haematology tests
Citrate
Blue Citrate
Coagulation studies
D-Dimer
Fibrinogen
Trace metal
Royal
Blue
Trace metal
serum Zinc and Selenium
Rapid
Serum
Orange
Thrombin-
based clot
activator
Only for routine biochemistry
samples from A&E department
Paediatric tubes (1.3ml):
Glucose
fluoride Yellow Fluoride oxalate
Blood glucose
Ethanol
Lactate

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 11 of 109 Last printed 05/02/2020 12:10:00
Container type Colour Description Use
Serum gel
Brown Serum gel
Routine biochemistry
Immunology
Please note these tubes MUST
NOT be used for mycology
tests
EDTA
Red EDTA Haematology
Blood transfusion
Li Hep
Orange Lithium Heparin
Citrate
Green Citrate Coagulation
Serum (no
gel)
White Serum (no gel) Mycology only
Other sample containers:
Plain
universal
White Sterile container
Microbiology
CSF samples for biochemical
analysis
CSF samples for mycological
analysis
Cytology samples
Plain
universal with
scoop
Blue
Sterile container
with scoop for
collecting faeces
Microbiology culture
Biochemical analysis
24 hour urine
collection
24 hour urine
Return to Examinations offered by biochemistry
For containers relating to histology and cytology please see the histopathology sample container
section.
1.10 Sample transportation
Each sample or set of samples must be placed in the plastic bag that accompanies the request
form. This bag must be sealed to prevent any leakage or loss of samples in transit. Please do not
use staples to seal these bags. Please ensure that the request sticker is placed on the paper form
that is attached to the sample bag and NOT placed directly on to the plastic bag.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 12 of 109 Last printed 05/02/2020 12:10:00
Samples must NOT be stored but should be sent to the laboratory immediately via porter or air tube
or, for off-site users, by the next available transport. Users must consider the time of the next
transport as delays may compromise certain results - if unsure, contact the relevant department.
1.10.1 Hospital requirements
Delivery in person to laboratory:
Samples must be sealed in plastic bags and must also be placed in an appropriate carrier, e.g. sturdy
carry box, sealed strong bag or other approved container whilst being carried to the laboratory.
Pneumatic tube:
Samples in sealed bags may be placed directly into the pods and sent through the system. See
below for more information on sample types that can and cannot be sent in a pod.
1.10.2 GP requirements
Samples collected from GP practices are gathered into strong polythene bags which are sealed. The
hospital transport drivers place these bags in the secure rigid sample transport boxes with sealable
lids that they carry in their vans.
These boxes must be labelled as “Diagnostic Specimens – UN3373” and have the department and
hospital name and contact telephone number.
1.10.3 Postal samples
Samples that are sent via the Royal Mail must be packed in special containers purchased from the
Royal Mail that conform to regulation UN No 3373 – Packing instructions for Diagnostic specimens
and Infectious substances (Packing instruction P650). This states that the ‘packaging must be of
good quality, strong enough to withstand the shocks and loadings normally encountered during
carriage’.
1.11 Requesting further tests on samples already in the laboratory (‘add-on’ tests)
1.11.1 Biochemistry
If you wish to request further tests on blood samples that you have already sent to us please call us
on ext. 4765 with the patient identifiers and the tests you require.
1.11.2 Haematology
If you wish to request further tests on blood samples that you have already sent to us please call us
on;
Haematology ext. 2141
Coagulation ext. 2127
Transfusion ext. 2160
1.11.3 Mycology Reference Centre
Please call us on ext. 2124 to request any additional tests, with patient identifiers. The addition of
extra tests is dependent on sufficient sample volume and date of original sample collection.
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 13 of 109 Last printed 05/02/2020 12:10:00
1.12 Turnaround times
Turnaround times that appear in this handbook are from time of receipt into the laboratory information
system (LIMS) to the time of reports being issued, except for histopathology turnaround times which
are from the date of sample collection to date of report issue.
Where possible the time of receipt in the laboratory is recorded on the request form and corrected in
the LIMS. This information is monitored monthly by each laboratory and is available on request.
1.13 Complaints or comments
We would hope that you do not have reason to complain about the service we provide. However, if
you do, please use the contact details below or the specific departmental contact details to raise this
with us in the first instance. Patient complaints can be made through the Trust website.
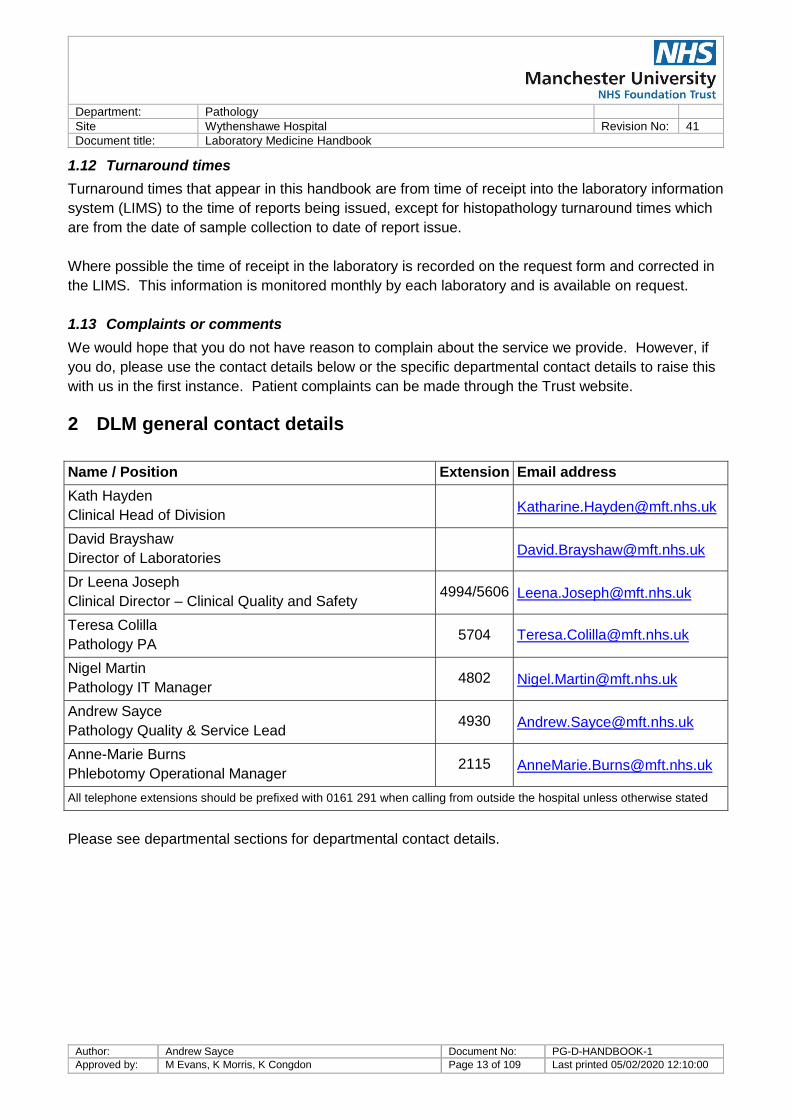
2 DLM general contact details
Name / Position Extension Email address
Kath Hayden
Clinical Head of Division [email protected]
David Brayshaw
Director of Laboratories [email protected]
Dr Leena Joseph
Clinical Director – Clinical Quality and Safety 4994/5606 [email protected]
Teresa Colilla
Pathology PA 5704 [email protected]
Nigel Martin
Pathology IT Manager 4802 [email protected]
Andrew Sayce
Pathology Quality & Service Lead 4930 [email protected]
Anne-Marie Burns
Phlebotomy Operational Manager 2115 [email protected]
All telephone extensions should be prefixed with 0161 291 when calling from outside the hospital unless otherwise stated
Please see departmental sections for departmental contact details.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 14 of 109 Last printed 05/02/2020 12:10:00
3 Phlebotomy
The Phlebotomy Service is provided by the Division of Laboratory Medicine.
3.1 Inpatient service
A time limited service is provided to all medical and surgical wards Monday - Friday from between
8am and 12 noon for routine blood collection.
A restricted phlebotomy service is provided to the wards over the weekend and bank holidays to
assist in the collection of routine blood samples between 7.30am and 11.30am.
All requests must be made on EPR by 7am Monday - Friday and 7:15am Saturday/Sunday and Bank
holidays. EPR request forms should not be pre-printed. If EPR is unavailable, Biochemistry
Haematology request forms should be used. Please complete the forms in full.
Phlebotomists must have access to the blood collection cart upon arrival to the ward. All users are
responsible for the cleaning and maintenance of the blood collection carts. Blood collection carts
should be re-stocked and put back on charge when finished with and left on charge when not in use.
Faults or defects are to be reported to the IT helpdesk by the user as soon as possible.
All urgent blood requests must be taken by the doctor/nurse. Urgent requests should not be left for
the phlebotomist’s routine blood collection round.
3.2 Outpatient service
There is a drop-in phlebotomy service for out-patients. Please note this service is not for in-patient
use.
Site Location Days Hours
Wythenshawe
Hospital
Phlebotomy suite opposite first floor
Out-patient Department Monday - Friday
09:00 am - 16:45
pm
Withington
Community Hospital
Main Out-patients Department,
ground floor
Monday -
Thursday
08:30 am - 16:45
pm
Friday 08:30 am - 16:00
pm
Please note - all hospital patients must have a request on EPR or bring the appropriate request
forms with them. If it is known that a patient has restricted venous access and the volume of sample
taken may not be sufficient for full analysis the priority of the tests will need to be indicated on the
request.
3.3 General Practitioner service
General Practitioner patients must use the appointment system and call 0800 092 4020 or
0161 947 0770 to book an appointment. Please note - patients must attend phlebotomy with a blood
request form.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 15 of 109 Last printed 05/02/2020 12:10:00
Site Location Days Hours
Wythenshawe
Hospital
Phlebotomy suite opposite first floor
Out-patient Department Monday - Friday
08:15am –
09:25am
Withington
Community Hospital
Main Out-patients Department,
ground floor Monday - Friday
08:30 am – 12:25
pm
Burnage Health
Centre
347 Burnage Ln, Manchester
M19 1EW Friday
09:00 am – 10.55
am

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 16 of 109 Last printed 05/02/2020 12:10:00
4 Sample reception
Pathology sample reception is open 24 hours a day, every day. Samples can be delivered directly to
the hatch at specimen reception at the front of the Clinical Sciences Building or sent via the
pneumatic tube. There are restrictions on samples that can be sent via the pneumatic tube, as
detailed below:
This sign should be on every pod station. If your pod station does not have this sign please contact
Sodexo on ext 5430.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 17 of 109 Last printed 05/02/2020 12:10:00
5 Biochemistry
Clinical Biochemistry is the study of the chemical and biochemical processes of the body in relation
to disease. This is a laboratory-based service which exists to help clinicians in the prevention,
diagnosis, treatment and management of disease. Diseases such as diabetes, thyroid problems,
kidney disease, heart attacks and cystic fibrosis can be diagnosed and monitored by the analysis of
body fluids such as blood, urine, saliva and CSF.
The department uses a fully automated analyser to analyse the majority of routine samples. This
analyser has a sophisticated sample tracking system which incorporates online decapping,
aliquotting, sealing and storage of samples within the analysing process. This system allows a high
throughput of samples with fast turnaround times. The department is also a specialist centre for
mass spectrometry, analysing samples from around the world for immunosuppressants, steroid
hormones, and markers of neuroendocrine tumours on six state-of-the-art mass spectrometers.
The Biochemistry department also actively promotes and supports Point-of-Care Testing (POCT),
managing blood gas analysers, blood glucose, ketone, urinalysis, haemoglobin, HbA1c and INR
testing meters throughout the Trust.
The majority of routine biochemistry results are returned within 24 hours, with a high percentage
being turned around within four hours. Exceptions include the more specialised tests which may
require batching, manual preparation or periods of incubation. Turnaround times are recorded for
each of the tests in the test library below. The test library is split into several sections:
Arterial blood gases Tumour markers Pleural fluid
Routine biochemistry CSF Other fluids
Therapeutic drug monitoring Faeces Specialist tests
Endocrinology Urinalysis Dynamic function tests
Specific proteins
Tests not available within the department are referred to specialist accredited laboratories. See
Referred Tests.
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 18 of 109 Last printed 05/02/2020 12:10:00
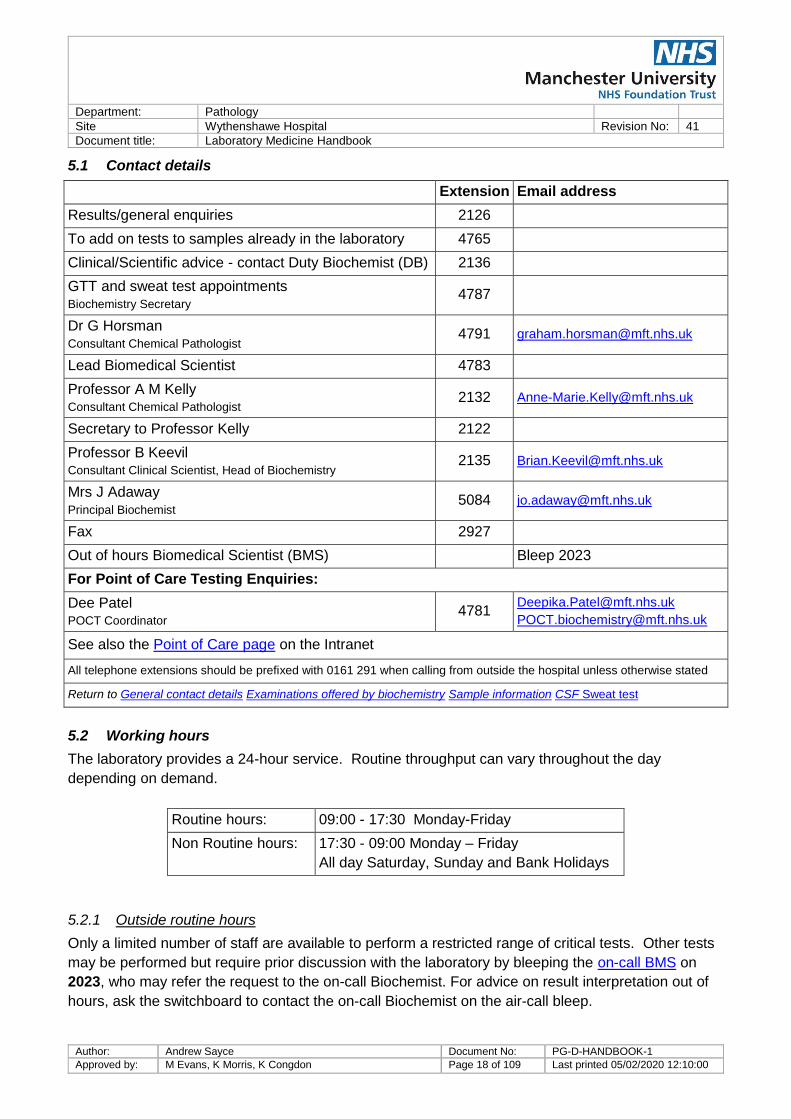
5.1 Contact details
Extension Email address
Results/general enquiries 2126
To add on tests to samples already in the laboratory 4765
Clinical/Scientific advice - contact Duty Biochemist (DB) 2136
GTT and sweat test appointments Biochemistry Secretary
4787
Dr G Horsman Consultant Chemical Pathologist
4791 [email protected]
Lead Biomedical Scientist 4783
Professor A M Kelly Consultant Chemical Pathologist
2132 [email protected]
Secretary to Professor Kelly 2122
Professor B Keevil Consultant Clinical Scientist, Head of Biochemistry
2135 [email protected]
Mrs J Adaway Principal Biochemist
5084 [email protected]
Fax 2927
Out of hours Biomedical Scientist (BMS) Bleep 2023
For Point of Care Testing Enquiries:
Dee Patel POCT Coordinator
4781 [email protected]
See also the Point of Care page on the Intranet
All telephone extensions should be prefixed with 0161 291 when calling from outside the hospital unless otherwise stated
Return to General contact details Examinations offered by biochemistry Sample information CSF Sweat test
5.2 Working hours
The laboratory provides a 24-hour service. Routine throughput can vary throughout the day
depending on demand.
Routine hours: 09:00 - 17:30 Monday-Friday
Non Routine hours: 17:30 - 09:00 Monday – Friday
All day Saturday, Sunday and Bank Holidays
5.2.1 Outside routine hours
Only a limited number of staff are available to perform a restricted range of critical tests. Other tests
may be performed but require prior discussion with the laboratory by bleeping the on-call BMS on
2023, who may refer the request to the on-call Biochemist. For advice on result interpretation out of
hours, ask the switchboard to contact the on-call Biochemist on the air-call bleep.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 19 of 109 Last printed 05/02/2020 12:10:00
The following tests are available at all times without prior arrangement:
General Biochemistry
U & E (Sodium, potassium, urea, creatinine, eGFR) Lipase
LFT (Total protein, albumin, ALT, ALP, globulin & bilirubin), AST,
conjugated bilirubin, GGT
Uric Acid
Bone profile (Total protein, albumin, globulin, calcium, phosphate) Chloride
Arterial Blood gas (also available as point of care testing in the
hospital)
Venous Bicarbonate
CRP Lipids (Cholesterol, HDL, triglycerides,
LDL)
Troponin T & cardiac enzymes (CK, LDH, AST)
Glucose Ethanol
Lactate Vitamin B12 & folate
Ammonia Iron studies (Fe, ferritin, transferrin)
Magnesium
Bilirubin
Endocrinology & Tumour
markers
Drug monitoring CSF/Fluid
analysis
Thyroid function tests (TSH & fT4) Paracetamol & Salicylate Protein
Gonadotrophins (LH/FSH) Antiepileptic drugs – carbamazepine & phenytoin, valproate Glucose
Oestradiol Theophylline Lactate
hCG Antibiotics – gentamicin, vancomycin, tobramycin & amikacin
AFP Digoxin
PSA
Progesterone
Prolactin
5.3 Urgent Requests
Urgent requests need to be marked clearly on the request form.
For A&E and samples marked urgent, the above tests that are available at all times will be available
within 1 hour of receipt in sample reception 90% of the time. Please call the laboratory for results of
urgent endocrinology tests or tumour markers out of routine hours as these require extra
interpretation and may take longer to appear on EPR.
5.4 Examinations offered by Biochemistry
Please note: separate blood samples for each laboratory discipline are required – Mycology,
Microbiology, Immunology, Biochemistry and Haematology.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 20 of 109 Last printed 05/02/2020 12:10:00
All routine serum biochemistry tests can be analysed on one filled 5ml tube (gold top). For non-
routine tests please see the individual test information in the Test Library for sample type (or
Appendix A for a full A-Z list of tests from all departments).
Further details for non-routine tests: contact the Duty Biochemist.
5.5 Sample transportation
CSF, precious samples and samples that must reach the laboratory within a set time must not be
transported by pneumatic tube.
5.6 Add-on Tests
The majority of tests can be added onto an initial collection within 24 hours. Some tests are more
stable and can be added on up to 5 days. Urine samples are stored for 2 days, all other samples are
stored for a minimum of 5 days and then discarded. Please contact the add-on line on ext. 4765 to
request any additional tests.
5.7 Sample Information
Age and sex related reference ranges are available from the laboratory and will be provided with
reports, providing sufficient patient information is given when requesting.
Biochemistry samples should be filled to the line to allow enough sample for analysis.
Turnaround times are for routine samples. If tests are urgently required then please contact the Duty
Biochemist during routine working hours or, outside these times, bleep the on-call BMS.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 21 of 109 Last printed 05/02/2020 12:10:00
5.8 Test library
Arterial Blood Gases Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
pH
1 hour
Heparinised
syringe
7.38 - 7.42
pCO2 4.7 - 6.0 kPa
pO2 12.0 - 14.6 kPa
Bicarbonate 21 - 25 mmol/L
Methaemoglobin <1.0% of total Hb
Base Excess -2 to +2 mmol/L
Carboxyhaemoglobin Non-smokers <5% Smokers 2 - 15%
Routine Biochemistry Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Sodium 4 hours
133 - 146 mmol/L Guidelines for management of hyponatraemia can be
found in the MFT Wythenshawe site formulary.
Potassium 4 hours
3.5 - 5.3 mmol/L
Neonate (1-3 weeks): 3.6 - 5.8 mmol/L
Guidelines for management of hypokalaemia /
hyperkalaemia can be found in the MFT Wythenshawe
site formulary.
Chloride 4 hours
95 - 108 mmol/L

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 22 of 109 Last printed 05/02/2020 12:10:00
Routine Biochemistry Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Venous
Bicarbonate 4 hours
22 - 29 mmol/L
Urea 4 hours
2.5 - 7.8 mmol/L
Creatinine 4 hours
Female 45 - 84 µmol/L
Male 59 - 104 µmol/L
0 No evidence of AKI
1
An increase of serum creatinine >26 umol/L
from baseline in 48 hrs OR more than 1.5 to 2
fold from baseline
2 An increase of serum creatinine of more than
or equal to 2-3 fold from baseline
3
An increase of serum creatinine more than 3
fold from baseline OR serum creatinine >355
umol/L with an acute rise of at least 45 umol/L
More details are available http://uhsm-
intranet/imt/ICE/Pages/AKIAlerts.aspx
Also from the think Kidneys website -
https://www.thinkkidneys.nhs.uk/
eGFR 4 hours
≥60 mL/min/1.73m2
Results above 90 will be reported as > 90 ml/min/1.73m2
eGFR is only an estimate and is not validated for use in

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 23 of 109 Last printed 05/02/2020 12:10:00
Routine Biochemistry Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
the following: children, pregnancy, acute renal failure,
oedematous states, muscle wasting disease states,
amputees and malnourished patients. This measurement
is for Caucasian patients only. There is a correction factor
to be applied for Afro-Caribbean patients, and this will be
published on the report form.
Also refer to http://www.renal.org/information-
resources/the-uk-eckd-guide or the Think Kidneys
website
Glucose (fasting) * 4 hours
3.0 - 6.0 mmol/L
*Low/High glucose measurements using Point of Care
Testing equipment need to be verified by sending a
specimen to the laboratory.
Bilirubin 4 hours
<21 µmol/L
Calcium
(Amended) 4 hours
2.20 - 2.60 mmol/L
Amended calcium is calculated using a formula from local
population data, and which is monitored and updated
wherever required
Guidelines for management of hypercalcaemia and
hypocalcaemia can be found in the MFT Wythenshawe
site formulary.
Magnesium 4 hours
0.7 - 1.0 mmol/L Guidelines for management of hypomagnesaemia can be
found in the MFT Wythenshawe site formulary.
Phosphate 4 hours
0.80 - 1.50 mmol/L Guidelines for management of hypophosphataemia can
be found in the MFT Wythenshawe site formulary.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 24 of 109 Last printed 05/02/2020 12:10:00
Routine Biochemistry Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Total protein 4 hours
60 - 80 g/L
Albumin 4 hours
35 - 50 g/L
Globulin 4 hours
25 - 42 g/L
Iron 4 hours
5.8 - 34.5 µmol/L
Transferrin 4 hours
2.0 - 3.6 g/L
Urate 4 hours
Male: 200 - 430 µmol/L
Female: 140 - 360 µmol/L
CRP 4 hours
< 5 mg/L
ALP 4 hours
Adult: 30 - 130 IU/L
Lipase 4 hours
13 - 60 U/L

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 25 of 109 Last printed 05/02/2020 12:10:00
Routine Biochemistry Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
AST 4 hours
Male: <50 IU/L
Female: <35 IU/L
ALT 4 hours
Male: <50 IU/L
Female: <35 IU/L
GGT 4 hours
Male: 10 - 71 IU/L
Female: 6 - 42 IU/L
CK 4 hours
Male: <320 IU/L
Female: <200 IU/L
LDH 4 hours
≤250 U/L
Total cholesterol 4 hours
Dependent on coronary risk factors. See BNF for details
HDL cholesterol 4 hours
Male: >1.0 mmol/L
Female: >1.2 mmol/L
Fasting
triglycerides 4 hours
<1.7 mmol/L
Lactate 2 hours
Age related
Adult 0.6 - 2.5 mmol/L

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 26 of 109 Last printed 05/02/2020 12:10:00
Routine Biochemistry Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
ACE (Angiotensin
converting
enzyme)
72 hours
≤65 IU/L for patients above 14 years of age
Alcohol (Ethanol) 4 hours
Not detected
Ammonia 4 hours
Adult: 10-50 µmol/L
Ensure sample received in lab within 30 minutes
of collection. Air tube transport is not suitable,
deliver sample directly to lab
Osmolality 36 hours
275 - 295 mOsm/kg

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 27 of 109 Last printed 05/02/2020 12:10:00
Routine Biochemistry Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
HbA1c 96 hours
NON-DIABETIC 25 - 36 mmol/mol IFCC (equivalent to 4.5 - 5.5% DCCT)
GOOD Control: <49 mmol/mol IFCC (equivalent to
6.5% or less DCCT)
POOR Control >64 mmol/mol IFCC (equivalent to
8.1% or above DCCT)
BORDERLINE: 49 - 64 mmol/mol IFCC (equivalent to
6.6 - 8.0% DCCT)
An HbA1c of 48 mmol/mol is recognised as the cut point
for diagnosing diabetes mellitus (WHO 2011).
Diabetes mellitus is not excluded by an HbA1c < 48
mmol/mol.
An HbA1c of 42 - 47 mmol/mol indicates a high risk of
diabetes mellitus.
HbA1c is not appropriate for the diagnosis of diabetes
mellitus in some situations e.g increased red cell
turnover.
High Sensitivity
Troponin T 2 hours
Reference range: ≤14 ng/L
A change of 50% or more between the 0 and 3 hour
samples is significant (increase or decrease)
ICE will alert any change of 50% or more (whether
increasing or decreasing)
Click on the alert icon for details
The Chest Pain Pathway should be followed in all cases.
Send blood for troponin T measurement at 0 and 3 hrs
post admission if coming in to hospital or post chest pain
if already an inpatient.
B12 24 hours
197 - 771 ng/L

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 28 of 109 Last printed 05/02/2020 12:10:00
Routine Biochemistry Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Ferritin 24 hours
Male: 30 - 400 µg/L
Female: 13 - 150 µg/L
Folate 24 hours
3.9 - 20 µg/L
Therapeutic Drug Monitoring Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Paracetamol 4 hours
Not detected
It is recommended to measure paracetamol 4 hour post
suspected overdose if an accurate history is possible.
Paracetamol levels may be falsely low when sample is
taken after starting treatment with N-acetyl cysteine.
Salicylate 4 hours
No reference range
If the patient has taken other drugs toxicity may be
enhanced. For advice contact the local poisons
information service: 0344 892 0111
Amikacin 4 hours
See comments. (Ranges from microbiology)
Antimicrobial interpretation should be directed to a
consultant microbiologist
Once daily dosing: Trough <5mg/L
Multiple daily dosing: Trough <10 mg/L Peak 25-30 mg/L
Carbamazepine 4 hours
4.0 - 12.0 mgl/L concern level: 25 mgl/L

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 29 of 109 Last printed 05/02/2020 12:10:00
Therapeutic Drug Monitoring Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Cyclosporin 24 hours
Variable
Target ranges depend on specific use of the drug.
Suggest consult local specialist for advice.
Digoxin 4 hours
0.6 - 1.2 µg/L; concern level: 3.0 µgl/L
Results are only meaningful if taken > 6 hours after
previous dose.
Hypokalaemia and/or hypothyroidism can potentiate
toxicity.
Everolimus 24 hours
3 – 8 µg/L
Gentamicin 4 hours
See comments, reference ranges from microbiology
Once daily dosing:
Trough level: < 1 mg/L
Peak level: not required to assess therapy
Multiple daily dosing
Trough level: < 1 mg/L
Peak level: not usually required to assess therapy
Lithium 24 hours
0.4 - 1.0 mmol/L pre-dose or >12 hrs post dose
Mycophenolate 192
hours
2.5-4.5 mg/L trough level for heart and lung transplant
patients Pre-dose
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 30 of 109 Last printed 05/02/2020 12:10:00
Therapeutic Drug Monitoring Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
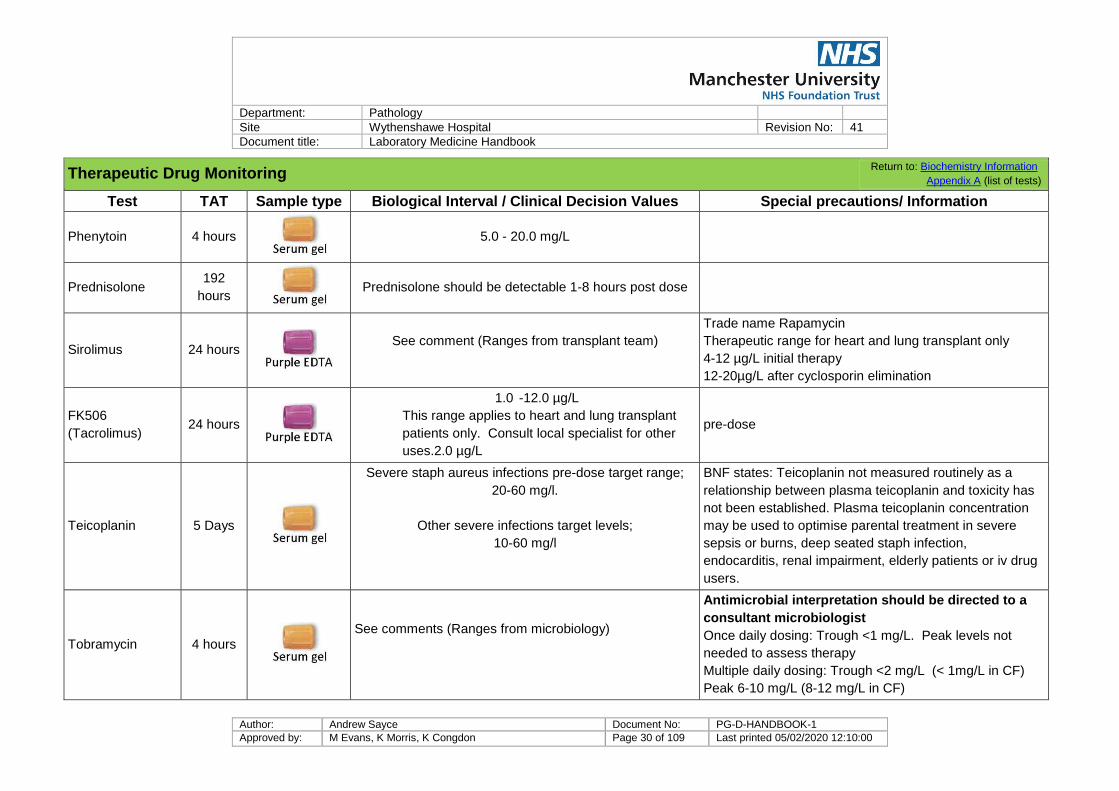
Phenytoin 4 hours
5.0 - 20.0 mg/L
Prednisolone 192
hours
Prednisolone should be detectable 1-8 hours post dose
Sirolimus 24 hours
See comment (Ranges from transplant team)
Trade name Rapamycin
Therapeutic range for heart and lung transplant only
4-12 µg/L initial therapy
12-20µg/L after cyclosporin elimination
FK506
(Tacrolimus) 24 hours
1.0 -12.0 µg/L
This range applies to heart and lung transplant
patients only. Consult local specialist for other
uses.2.0 µg/L
pre-dose
Teicoplanin 5 Days
Severe staph aureus infections pre-dose target range;
20-60 mg/l.
Other severe infections target levels;
10-60 mg/l
BNF states: Teicoplanin not measured routinely as a
relationship between plasma teicoplanin and toxicity has
not been established. Plasma teicoplanin concentration
may be used to optimise parental treatment in severe
sepsis or burns, deep seated staph infection,
endocarditis, renal impairment, elderly patients or iv drug
users.
Tobramycin 4 hours
See comments (Ranges from microbiology)
Antimicrobial interpretation should be directed to a
consultant microbiologist
Once daily dosing: Trough <1 mg/L. Peak levels not
needed to assess therapy
Multiple daily dosing: Trough <2 mg/L (< 1mg/L in CF)
Peak 6-10 mg/L (8-12 mg/L in CF)

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 31 of 109 Last printed 05/02/2020 12:10:00
Therapeutic Drug Monitoring Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Finger prick samples are also accepted.
Theophylline 4 hours
Adult: 10 - 20 mg/L Pre-dose
TPMT
(Thiopurine S-
methyltransferase)
192
hours
Deficient: <10 mU/L
Low: 20-67 mU/L
Normal: 68-150 mU/L
High: >150 mU/L
Recent blood transfusions may mask a deficient TPMT
result
Vancomycin 4 hours
Trough level: 10 – 15 mg/L
Trough level: 15 – 20 mg/L for severe MRSA infections.
Antimicrobial interpretation should be directed to a
consultant microbiologist
Pre-dose
Endocrinology Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Free T4 4 hours
10 - 25 pmol/L
Free T3 72
hours
3.1 - 6.8 pmol/L

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 32 of 109 Last printed 05/02/2020 12:10:00
Endocrinology Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
TSH 4 hours
0.27 - 4.20 mU/L
TPO 96
hours
<34 IU/mL
LH 24
hours
Variable. See report
FSH 24
hours
Variable. See report
Progesterone 24
hours
Variable. See report
Oestradiol 24
hours
Variable. See report Mass spectrometry assay for oestradiol also available
with TAT of 10 days . Contact 2136 for details
Prolactin 24
hours Variable. See report
Testosterone
240
hours See report
Salivary
testosterone
744
hours
Saliva (passive
drool). Contact
See report Samples collected onto salivette swabs are NOT suitable.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 33 of 109 Last printed 05/02/2020 12:10:00
Endocrinology Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
lab
SHBG 240
hours
See report
17-
hydroxyprogesterone
240
hours
Variable. See report Part of female testosterone profile
Androstenedione 240
hours
0.8-4.7 nmol/L Part of female testosterone profile
DHEAS 240
hours
Variable. See report Part of female testosterone profile
Metanephrines 240
hours
Metanephrine <510 pmol/L
Normetanephrine <1180 pmol/L
3-methoxytyramine (3-MT) <180 pmol/L
Sample must reach lab and be separated & frozen within
1 hour of collection.
Preferably take sample with patient recumbent after
overnight fast.
Macroprolactin 5 days
See report Usually added to requests by laboratory staff as required
PTH 24
hours
1.6 - 6.9 pmol/L for normocalcaemic patients
Renin 240
hours
0.3-2.2 nmol/L/hr
Aldosterone 240
hours
up to 630 pmol/L

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 34 of 109 Last printed 05/02/2020 12:10:00
Endocrinology Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Cortisol 36
hours
Shows variation across day
0830-1130: 100-500 nmol/L
Salivary cortisol 240
hours (Contact lab)
See report
Vitamin A & E 360
hours
Vitamin A 1.05 – 2.97 µmol/L
Vitamin E 13.9 – 47.0 µmol/L
Vitamin D 168
hours
See report
Dexamethasone 360
hours
Dexamethasone concentrations <3.0 nmol/L suggest
impaired absorption or excess metabolism of
dexamethasone and an alternative biochemical screening
test to investigate hypercortisolism should then be
considered
Conversely, dexamethasone concentrations ≥3.0 nmol/L
suggest adequate absorption and metabolism of
dexamethasone
Several drugs/medications have been identified as
potential inducers or inhibitors of the CYP3A4 enzyme
resulting in accelerated or impaired metabolism of
dexamethasone. For further information contact the Duty
Biochemist.
Human chorionic
gonadotrophin
(hCG)
24
hours
Non-pregnant < 2.0 U/L

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 35 of 109 Last printed 05/02/2020 12:10:00
Specific Proteins Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Alpha-1-
antitrypsin 96 hours
0.9 - 2.0 g/L
Assay performed Tuesday and Friday.
Low Alpha-1-antitrypsin results (< 1.1 g/L) and samples
from patients < 1 years will be sent away for phenotyping.
IgA 72 hours
See report
IgG 72 hours
See report
IgM 72 hours
See report
Protein
Electrophoresis
168
hours
Qualitative interpretation
The main use of this test is to exclude the presence of a
monoclonal protein, which may indicate myeloma, MGUS
or a lymphoproliferative disorder.
A urine sample for analysis of Bence Jones proteins is
also required to exclude the above disorders.
Polyclonal increases in immunoglobulins can be
associated with infection, inflammation or connective
tissue disease and do not indicate myeloma.
Rheumatoid
factor 4 hours
<14 IU/mL
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 36 of 109 Last printed 05/02/2020 12:10:00
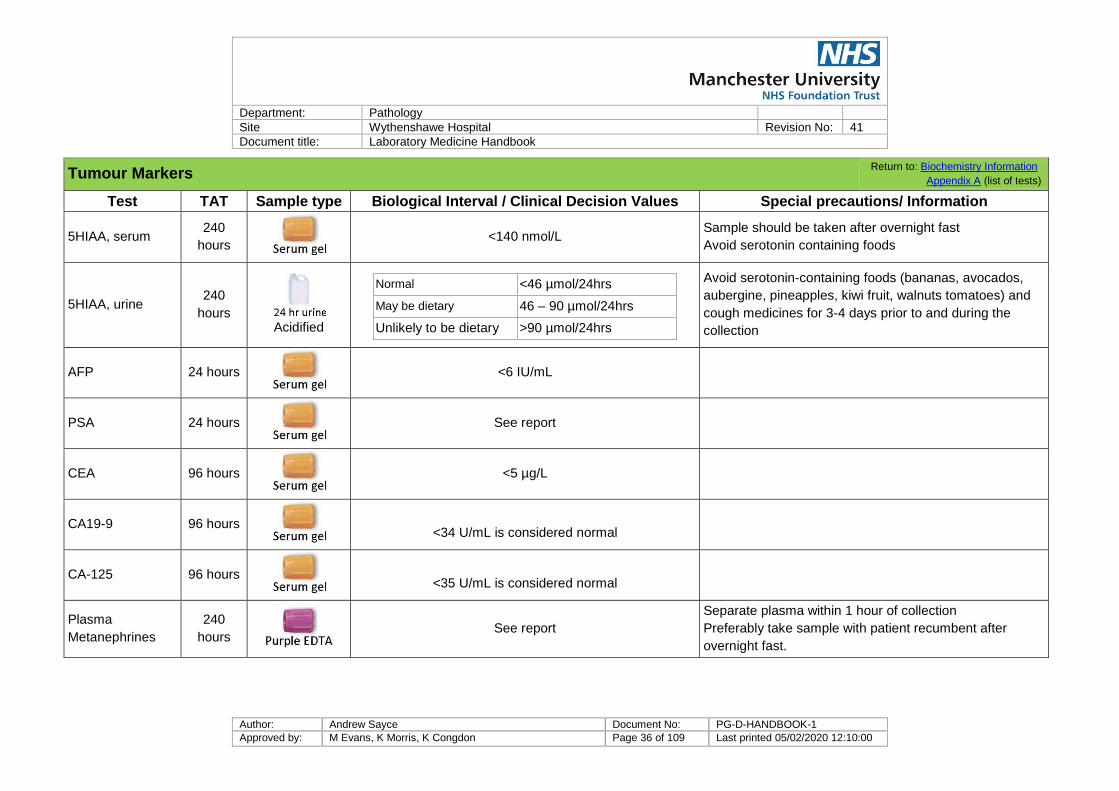
Tumour Markers Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
5HIAA, serum 240
hours
<140 nmol/L Sample should be taken after overnight fast
Avoid serotonin containing foods
5HIAA, urine 240
hours Acidified
Normal <46 µmol/24hrs
May be dietary 46 – 90 µmol/24hrs
Unlikely to be dietary >90 µmol/24hrs
Avoid serotonin-containing foods (bananas, avocados,
aubergine, pineapples, kiwi fruit, walnuts tomatoes) and
cough medicines for 3-4 days prior to and during the
collection
AFP 24 hours
<6 IU/mL
PSA 24 hours
See report
CEA 96 hours
<5 µg/L
CA19-9 96 hours
<34 U/mL is considered normal
CA-125 96 hours
<35 U/mL is considered normal
Plasma
Metanephrines
240
hours
See report
Separate plasma within 1 hour of collection
Preferably take sample with patient recumbent after
overnight fast.
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 37 of 109 Last printed 05/02/2020 12:10:00
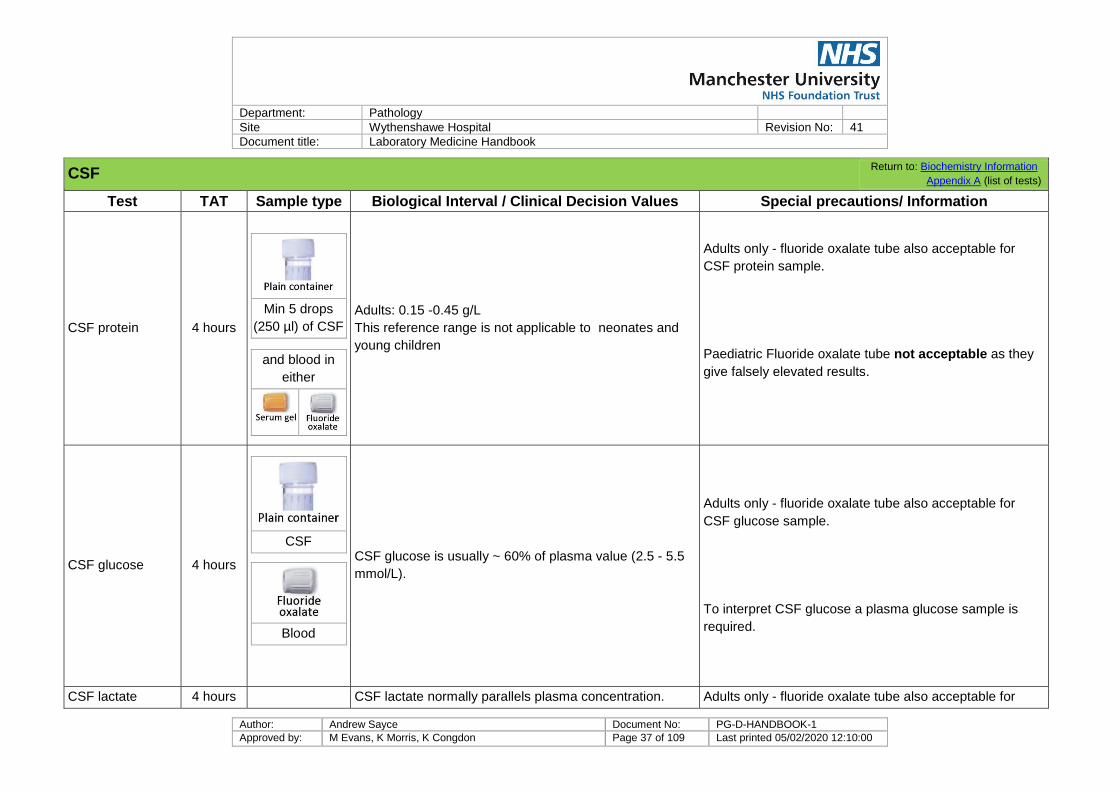
CSF Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
CSF protein 4 hours
Min 5 drops
(250 µl) of CSF
and blood in
either
Adults: 0.15 -0.45 g/L
This reference range is not applicable to neonates and
young children
Adults only - fluoride oxalate tube also acceptable for
CSF protein sample.
Paediatric Fluoride oxalate tube not acceptable as they
give falsely elevated results.
CSF glucose 4 hours
CSF
Blood
CSF glucose is usually ~ 60% of plasma value (2.5 - 5.5
mmol/L).
Adults only - fluoride oxalate tube also acceptable for
CSF glucose sample.
To interpret CSF glucose a plasma glucose sample is
required.
CSF lactate 4 hours CSF lactate normally parallels plasma concentration. Adults only - fluoride oxalate tube also acceptable for

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 38 of 109 Last printed 05/02/2020 12:10:00
CSF Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
CSF
Blood
CSF lactate sample.
To interpret CSF lactate a plasma lactate sample is
required.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 39 of 109 Last printed 05/02/2020 12:10:00
CSF Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Xanthochromia
Analysed
8am-
8pm*
4th sample of
LP (min 0.5ml)
CSF (total
protein)
Blood for
bilirubin
Xanthochromia Collection packs are available from
Biochemistry.
Xanthochromia test should only be requested in CT-scan
negative patients.
Sample must be 12 h post-onset of symptoms and within
14 days of symptoms.
CSF must be protected from light.
*Samples received outside of these times can be sent to an
external laboratory if result required urgently (minimum 700 µL
of sample required).

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 40 of 109 Last printed 05/02/2020 12:10:00
Faeces Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Faecal elastase
(pancreatic)
336
hours
Random
faeces
(minimum pea
sized amount)
Severe insufficiency < 100 µg/g
Moderate insufficiency 100-200 µg/g
Normal > 200 µg/g normal
Watery/runny or mucousy stool samples may have falsely
low results due to dilution. Send a formed stool sample
where possible.
Urinalysis Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Bence-Jones
protein
192
hours
10ml urine
Screening test, Pos or Neg Early morning sample preferred
Calcium 4 hours
Acidified
2.5 - 7.5 mmol/24hrs
Citrate 240
hours Acidified
1680-6450 µmol/24hrs

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 41 of 109 Last printed 05/02/2020 12:10:00
Urinalysis Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Cortisol 192
hours
No preservative
Up to 165nmol/24 hours
Cotinine 192
hours
See report Nicotine metabolite – may also be positive if patient is on
nicotine replacement therapy
Creatinine
Clearance 24 hours
No preservative
Blood for U&E
Age dependent. See report For most patients e-GFR is used to estimate glomerular
filtration
Cystine 240
hours
No preservative
<100 mg/24hrs

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 42 of 109 Last printed 05/02/2020 12:10:00
Urinalysis Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Magnesium 24 hours
Acidified
2.4 - 6.6 mmol/24hr
Microalbumin
(ACR) 24 hours
10 ml EMU
ACR >2.9 mg/mmol should be regarded as clinically important proteinuria in all patients (NICE CG182)
Also known as albumin:creatinine ratio (ACR)
Osmolality 24 hours
10 ml random
Relative to hydration status
Oxalate 240
hours Acidified
See report Contact Duty Biochemist for paediatric reference ranges
Phosphate 24 hours
Acidified
15-50 mmol/24h Random urine phosphate also available
Potassium 24 hours
No preservative
25 - 125 mmol/L
Contact Duty Biochemist for further information
Random urine phosphate also available
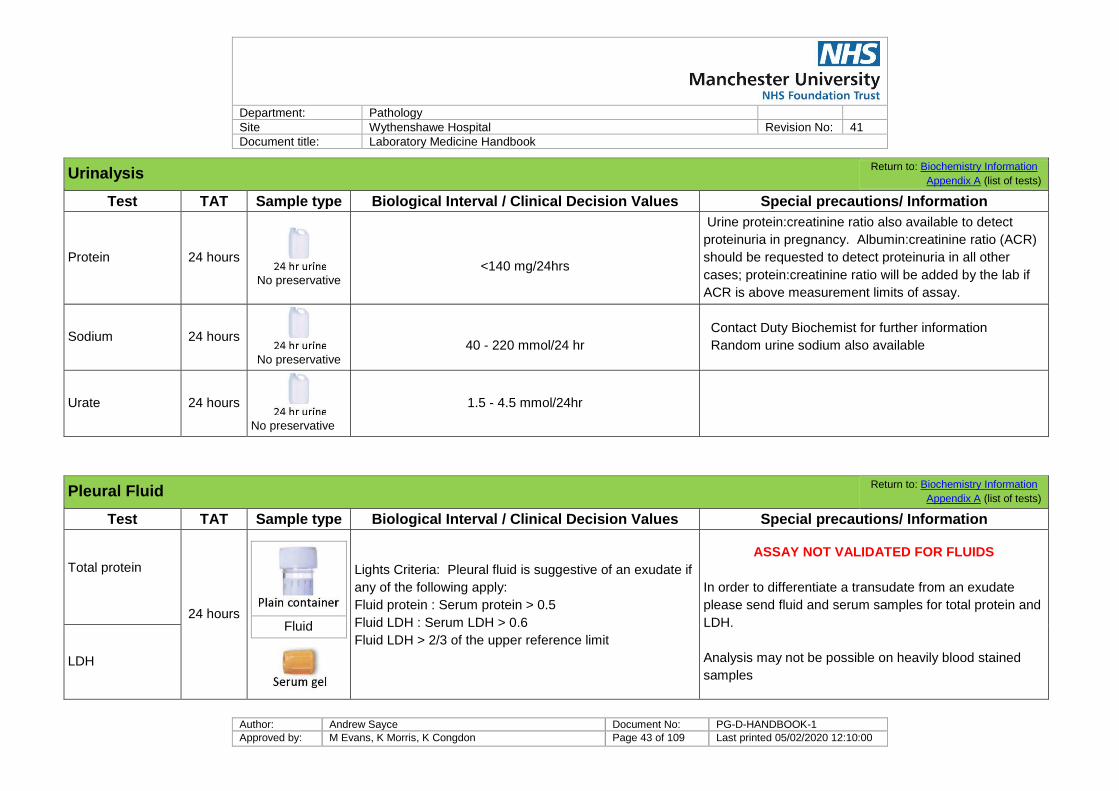
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 43 of 109 Last printed 05/02/2020 12:10:00
Urinalysis Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Protein 24 hours
No preservative
<140 mg/24hrs
Urine protein:creatinine ratio also available to detect
proteinuria in pregnancy. Albumin:creatinine ratio (ACR)
should be requested to detect proteinuria in all other
cases; protein:creatinine ratio will be added by the lab if
ACR is above measurement limits of assay.
Sodium 24 hours
No preservative
40 - 220 mmol/24 hr
Contact Duty Biochemist for further information
Random urine sodium also available
Urate 24 hours
No preservative
1.5 - 4.5 mmol/24hr
Pleural Fluid Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Total protein
24 hours
Fluid
Lights Criteria: Pleural fluid is suggestive of an exudate if
any of the following apply:
Fluid protein : Serum protein > 0.5
Fluid LDH : Serum LDH > 0.6
Fluid LDH > 2/3 of the upper reference limit
ASSAY NOT VALIDATED FOR FLUIDS
In order to differentiate a transudate from an exudate
please send fluid and serum samples for total protein and
LDH.
Analysis may not be possible on heavily blood stained
samples LDH

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 44 of 109 Last printed 05/02/2020 12:10:00
Pleural Fluid Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Glucose 24 hours
Fluid
Glucose < 2.2 mmol/L is associated with empyema,
rheumatoid arthritis, tuberculosis or malignancy. This cut
off may not apply in patients with elevated plasma
glucose.
ASSAY NOT VALIDATED FOR FLUIDS
To interpret fluid glucose a plasma glucose sample is
required. Please contact the duty biochemist for further
advice.
pH 24 hours
Heparinised
syringe
pH < 7.3 is associated with empyema, TB, malignancy,
collagen vascular disease or haemothorax.
ASSAY NOT VALIDATED FOR FLUIDS
Please REMOVE needle and cap syringe prior to sending
sample to lab.
Analysis may not be possible on heavily blood stained
samples
Triglyceride 24 hours
Fluid
Fasting
> 1.26 mmol/L Suggestive of a Chylous effusion
< 0.57 mmol/L Not suggestive of a Chylous
effusion
0.57 – 1.26 mmol/L equivocal
ASSAY NOT VALIDATED FOR FLUIDS
To interpret fluid triglycerides a fasting serum sample is
required. Interpret fluid triglycerides with caution in
patients on TPN or those with hypertriglyceridemia. For
further information contact the Consultant Chemical
Pathologists.
Analysis may not be possible on heavily blood stained
samples

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 45 of 109 Last printed 05/02/2020 12:10:00
Pleural Fluid Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Lipase 24 hours
Fluid
Blood
Fluid lipase higher than serum lipase may be suggestive
of pancreatic involvement.
ASSAY NOT VALIDATED FOR FLUIDS
This test should only be requested if a pancreatic cause
of pleural effusion is suspected.
To interpret fluid lipase a serum sample is required.
NOT TO BE USED FOR PANCREATIC CYST FLUID.
For further advice contact the duty biochemist
Albumin 24 hours
Fluid
An albumin gradient (serum albumin – fluid albumin) < 12
g/L is suggestive of a transudate and > 12 g/L is
suggestive of an exudate.
ASSAY NOT VALIDATED FOR FLUIDS
In order to differentiate a tansudate from an exudate
please request a fluid and serum samples for total
protein and LDH
Analysis may not be possible on heavily blood stained
samples
Other Fluids Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
For fluids other than CSF, Pleural effusions and urine please contact duty biochemist for advice on appropriate test selection.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 46 of 109 Last printed 05/02/2020 12:10:00
Specialist Tests Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Cryoglobulins 192
hours
Normal result – cryoglobulins NOT detected.
Samples need to be sent to the laboratory at 37°C.
Sample must be collected into a pre-warmed tube and
transported to the laboratory in a vacuum flask
containing warm sand. Collect pre-warmed flask/tube
from Specimen Reception (Clinical Sciences Building) or
Out-patient phlebotomy.
Sweat test 34 hours Sweat
For child of 6 months of age or older:
Abnormal consistent with CF Chloride > 60 mmol/L
Equivocal Chloride 40 - 60 mmol/L
Normal Chloride < 40 mmol/L
For a child <6 months of age please contact the
laboratory or refer to the report.
These are performed in the Paediatric Outpatients
department on Thursday mornings.
A prior appointment is needed. Please contact the
Consultant Chemical Pathologists’ secretary.
A request form or referral letter with full patient details
must be sent to the department.
Renal stone
analysis 17 days Stone (calculi) See report
Please include information on the location the stone was
removed from.
Check www.UKAS.com for up to date accreditation status of referral laboratories.
Referred Tests Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval /
Clinical Decision Values Special precautions/ Information
Referral Lab and Accreditation Number
ACTH 24 days
See report Must be received in lab within 15 minutes of
collection.
Clinical Biochemistry, The
Christie Hospital (8697)

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 47 of 109 Last printed 05/02/2020 12:10:00
Referred Tests Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval /
Clinical Decision Values Special precautions/ Information
Referral Lab and Accreditation Number
Acyl
carnitines/free
carnitine/MCADD
profile
2 weeks
Dried blood
spot or
See report Willink Laboratory (UKAS 9865)
Amino acids
(plasma) 35 days
See report CSF amino acids also available Willink Laboratory (UKAS 9865)
Amino acids
(urine) 35 days
5 mL random
urine sample
See report Willink Laboratory (UKAS 9865)
Β2 microglobulin 14 days
See report Department of Immunology,
MFT Oxford Road (UKAS 8195)
β-OH
butyrate/free fatty
acids
17 days
See report
Separate sample required. Take at time of
hypoglycaemia. Must be received in the lab
within 20 minutes of collection.
Paediatric Biochemistry, MFT
Oxford Road (UKAS 8651)
Caeruloplasmin 10 days
See report Requested with copper for investigation of
?Wilson’s disease
Biochemistry, MFT Oxford Road
( UKAS 8651)
Cholinesterase/ac
etylcholinesterase
4-6
weeks
See report
For investigation of suxamethonium/mivacurium
sensitivity (scoline apnoea). Apnoea
investigations should wait until patient is fully
recovered.
Biochemistry, MFT Oxford Road
(UKAS 8651)

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 48 of 109 Last printed 05/02/2020 12:10:00
Referred Tests Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval /
Clinical Decision Values Special precautions/ Information
Referral Lab and Accreditation Number
Chromium and
cobalt 5 weeks
See report
Take serum sample through needle first and
discard. Then take sample into trace element
tube through the same needle and send to lab.
Biochemistry, MFT Oxford Road
(UKAS 8651)
Copper (serum) 10 days
See report
Copper increases during the acute phase
response, and should not be measured in
patients with acute infection/inflammation. Fasting
samples preferred.
Biochemistry, MFT Oxford Road
(UKAS 8651)
Copper (urine) 4 weeks
24h urine
collection See report
No preservative or pre-treatment of the container
required
Biochemistry, MFT Oxford Road
(UKAS 8651)
Complement C3 7 days
See report Department of Immunology,
MFT Oxford Road (UKAS 8195)
Complement C4 7 days
See report Department of Immunology,
MFT Oxford Road (UKAS 8195)
Down’s syndrome
screening 5 days
Risk factor provided. Refer to
report. Reports sent directly to requestor.
Blood Sciences, Royal Bolton
Hospital (UKAS 9925)
Drugs of abuse
screen (urine) 14 days
Random urine
sample
See report Indicate on request form if cannabis and/or urine
ethanol are required.
Clinical Biochemistry, Salford
Royal Hospital (UKAS 8331)
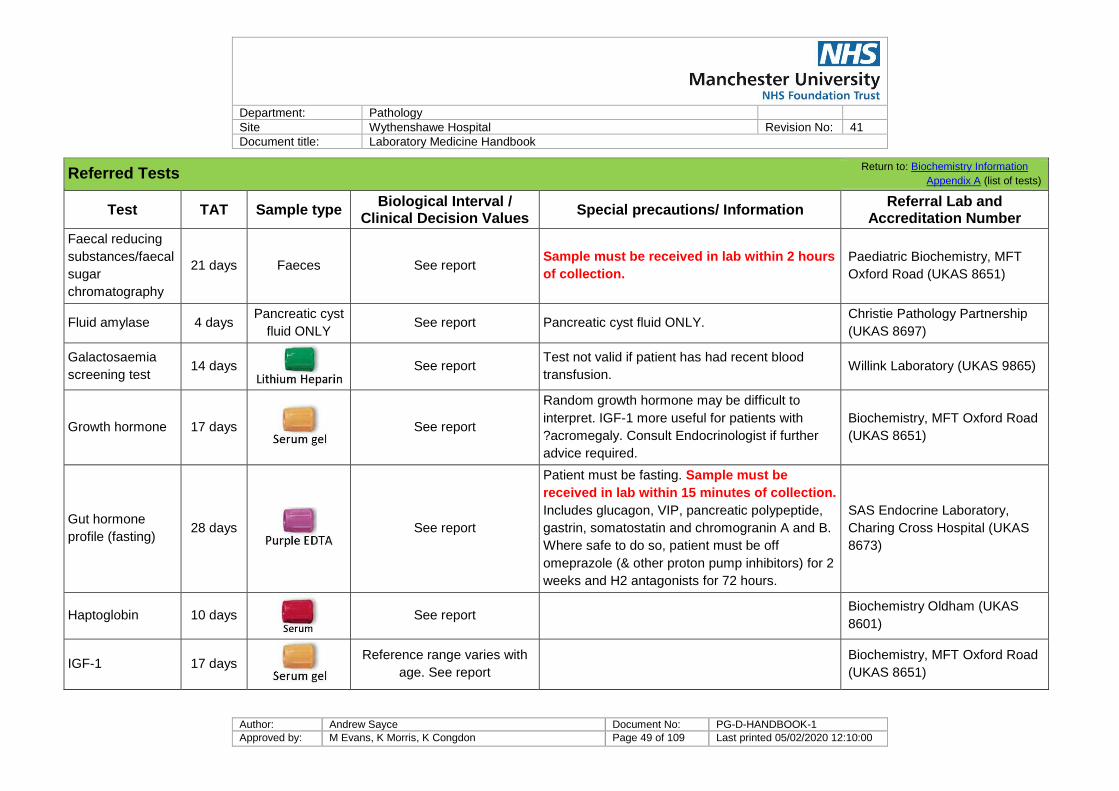
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 49 of 109 Last printed 05/02/2020 12:10:00
Referred Tests Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval /
Clinical Decision Values Special precautions/ Information
Referral Lab and Accreditation Number
Faecal reducing
substances/faecal
sugar
chromatography
21 days Faeces See report Sample must be received in lab within 2 hours
of collection.
Paediatric Biochemistry, MFT
Oxford Road (UKAS 8651)
Fluid amylase 4 days Pancreatic cyst
fluid ONLY See report Pancreatic cyst fluid ONLY.
Christie Pathology Partnership
(UKAS 8697)
Galactosaemia
screening test 14 days
See report
Test not valid if patient has had recent blood
transfusion. Willink Laboratory (UKAS 9865)
Growth hormone 17 days
See report
Random growth hormone may be difficult to
interpret. IGF-1 more useful for patients with
?acromegaly. Consult Endocrinologist if further
advice required.
Biochemistry, MFT Oxford Road
(UKAS 8651)
Gut hormone
profile (fasting) 28 days
See report
Patient must be fasting. Sample must be
received in lab within 15 minutes of collection.
Includes glucagon, VIP, pancreatic polypeptide,
gastrin, somatostatin and chromogranin A and B.
Where safe to do so, patient must be off
omeprazole (& other proton pump inhibitors) for 2
weeks and H2 antagonists for 72 hours.
SAS Endocrine Laboratory,
Charing Cross Hospital (UKAS
8673)
Haptoglobin 10 days
See report Biochemistry Oldham (UKAS
8601)
IGF-1 17 days
Reference range varies with
age. See report
Biochemistry, MFT Oxford Road
(UKAS 8651)

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 50 of 109 Last printed 05/02/2020 12:10:00
Referred Tests Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval /
Clinical Decision Values Special precautions/ Information
Referral Lab and Accreditation Number
IgG subclasses
(IgG4 can also be
requested
separately)
10 days
See report
Investigation of suspected immunodeficiency, or
autoimmune pancreatitis which can be associated
with raised IgG4 levels.
Department of Immunology,
MFT Oxford Road (UKAS 8195)
Insulin and c-
peptide (adult
patients >16 years
of age, for
investigation of
hypoglycaemia)
17 days
See report
Sample must be received in the lab within 20
minutes of collection. Collect at time of
hypoglycaemia. Also send sample for glucose.
SAS Peptide Hormone
Laboratory, Royal Surrey
County Hospital (UKAS 9732)
Lamotrigine 1 working
day
See report Pre-dose Biochemistry, MFT Oxford Road
(UKAS 8651)
Mannose binding
lectin 17 days
See report Protein Reference Unit,
Sheffield (UKAS 8494)

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 51 of 109 Last printed 05/02/2020 12:10:00
Referred Tests Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval /
Clinical Decision Values Special precautions/ Information
Referral Lab and Accreditation Number
Oligoclonal bands
(CSF) 20 days
CSF with paired
serum sample
CSF
Blood
See report For diagnosis of multiple sclerosis Biochemistry, Salford Royal
Hospital (UKAS 8331)
Organic acids
(urine) 35 days
5 mL random
urine sample
See report Investigation of suspected inherited metabolic
disorders Willink Laboratory (UKAS 9865)
Orosomucoid
(Alpha-1 acid
glycoprotein)
17 days
See report Biochemistry, MFT Oxford Road
(UKAS 8651)
Phenobarbital 48 hours
See report Pre dose.
Biochemistry, MFT Oxford Road
(UKAS 8651)

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 52 of 109 Last printed 05/02/2020 12:10:00
Referred Tests Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval /
Clinical Decision Values Special precautions/ Information
Referral Lab and Accreditation Number
Porphyrin screen 17 days
Random urine
Blood
See report
Samples must be protected from light
immediately after collection. Provide full
clinical details. If acute porphyria is
suspected, sample should be collected at the
time of symptoms.
Porphyria Service, Medical
Biochemistry, University
Hospital of Wales, Cardiff
(UKAS 8989)
Procalcitonin 14 days
See report Biochemistry, MFT Oxford Road
(UKAS 8651)
PIIINP (Type III
procollagen
peptide)
35 days
See report Sample must be received within 4 hours of
collection. For patients on methotrexate therapy.
Biochemistry, MFT Oxford Road
(UKAS 8651)
Selenium 10 days
See report
Selenium is decreased in the acute phase
response, and should not be measured in
patients with acute infection/inflammation.
Results also affected by low albumin. Fasting
samples preferred.
Biochemistry, MFT Oxford Road
(UKAS 8651)

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 53 of 109 Last printed 05/02/2020 12:10:00
Referred Tests Return to: Biochemistry Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval /
Clinical Decision Values Special precautions/ Information
Referral Lab and Accreditation Number
Urine light chain
quantification 15 days
No preservative
See report Used in the monitoring of patients with myeloma Protein Reference Unit,
Sheffield (UKAS 8494)
Urine reducing
substances 21 days
Random urine
See report Sample must be received in the lab within 2 hours
of collection Willink Laboratory (UKAS 9865)
Valproate 48 hours
There are no evidence based
therapeutic ranges for serum
valproate concentrations.
There is not a clear
relationship between serum
valproate concentration and
efficacy and toxicity.
Pre-dose Biochemistry, MFT Oxford Road
(UKAS 8651)
Very long chain
fatty acids
(VLCFA)
35 days
See report Willink Laboratory (UKAS 9865)
Zinc 10 days
See report
Zinc is decreased in the acute phase response,
and should not be measured in patients with
acute infection/inflammation. Results also
affected by low albumin. Fasting samples
preferred.
Biochemistry, MFT Oxford Road
(UKAS 8651)

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 54 of 109 Last printed 05/02/2020 12:10:00
Protocols are available from the Department directly for the following dynamic tests. If these need to be discussed, please contact the Duty Biochemist.
Dynamic Function Tests Return to: Biochemistry Information
Appendix A (list of tests)
Combined pituitary function test Insulin stimulation test
Dexamethasone suppression test Prolonged fasting test
Glucose tolerance test Short Synacthen test
Glucose tolerance test with GH suppression Water deprivation test
GnRH Stimulation test
5.9 Factors known to significantly affect performance of tests/interpretation of results
Problem Common Causes Affected Analyte
Delay in processing Overnight storage
>6 hour delay in separation Increased potassium, phosphate, LDH, AST.
Incorrect storage Storing unseparated sample in the fridge Increased phosphate and potassium
Decreased bicarbonate
Haemolysis
Expelling blood through needle
Vigorous shaking
Extreme temperature
Increased potassium, phosphate, LDH, AST.
Inappropriate Collection Site Sample taken from drip arm Increased drip analyte e.g. sodium, glucose
Decreased analytes - dilutional effect
Incorrect container or anticoagulant No fluoride oxalate Decreased glucose
K-EDTA contamination
Increased potassium
Decreased calcium, magnesium, alkaline
phosphatase
Lithium heparin tube Increased lithium

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 55 of 109 Last printed 05/02/2020 12:10:00
5.10 Effect of haemolysis, lipaemia and icterus:
Haemolysis, lipaemia and icterus may cause false elevations or reductions in the measured
concentrations of several biochemistry analytes. The presence of haemolysis, lipaemia or icterus will
be detected in the laboratory and the affected analytes will be flagged. In cases where there is
significant interference, the affected analyte will not be reported. Further information can be obtained
from the Duty Biochemist.
5.11 Measurement uncertainty
All assays have a margin of error associated with the calculation of the numerical value. This is
referred to as the measurement uncertainty and is usually expressed as a percentage of the reported
figure. This calculation allows the user to understand the uncertainty of any numerical results and
can be assured with 95% confidence that the true result lies plus or minus the measurement
uncertainty around the reported value. Further information on the measurement of uncertainty for all
our laboratory assays is available by contacting the Duty Biochemist within routine working hours.
5.12 Point of Care
The relationship between values obtained in the laboratory and POCT are established and available
upon request.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 56 of 109 Last printed 05/02/2020 12:10:00
6 Haematology
6.1 Contact details
Extension Fax Email address
Dr Simon Watt Consultant Haematologist, Head of Haematology
2114
2125
Dr Sumaya El-Hanash Consultant Haematologist
2114 [email protected]
Dr Shiva Natarajan Consultant Haematologist
4797 [email protected]
Haematology secretaries 2114/4789
Medical emergencies Contact
switchboard
For non-urgent advice - haematology [email protected]
For non-urgent advice – immunology [email protected]
Results/general enquiries 2126
Laboratories:
Blood transfusion 2160/2161 2130
Haematology 2141
Coagulation 2127
Immunology 4762
Gareth Davies Lead Biomedical Scientist - Haematology
4777 [email protected]
Maggie Evans Lead Biomedical Scientist – Blood transfusion
4719 [email protected]
Out of hours Biomedical Scientist (BMS) Bleep 2033
All telephone extensions should be prefixed with 0161 291 when calling from outside the hospital unless otherwise stated
Return to: A-Z list of tests,

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 57 of 109 Last printed 05/02/2020 12:10:00
6.2 Routine Haematology
6.2.1 Test library
Routine Haematology Return to: Haematology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Full Blood Count
Urgent 1 hr
See table below
Minimum sample volume (Purple EDTA) 1.5ml
Minimum Paediatric sample volume 0.5ml
Specimens for FBC should be sent to the laboratory as
soon as possible after being taken. A FBC specimen
should be analysed no more than 24 hours after being
bled from the patient.
Extremes of temperature can affect FBC specimens –
where storage is required store between 2oC and 25oC –
Note that if a plasma viscosity is to be performed on the
same specimen, it must remain at ambient temperature.
Other factors that can affect FBC results include
lipaemia, haemolysis, hyperbilirubinemia,
Clotted specimens and sample volumes lower than the
specified minimum volume will not be processed
Routine 4 hrs
Plasma Viscosity 24 hours
See table below Minimum sample volume 1.5ml
DO NOT REFRIGERATE

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 58 of 109 Last printed 05/02/2020 12:10:00
Routine Haematology Return to: Haematology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Haemoglobinopathy
(Hb Variant
/thalassaemia)
5 days
See table below
FBC sample will be used
Please send sample for ferritin also. Recent transfusion
will interfere with test interpretation.
Note – abnormal variants will require further testing,
adding 2 weeks to the stated TAT.
Malaria screen 2 hours
See report FBC sample will be used. Give details of area visited.
Glandular Fever
screening test 24 hours
Screening test – reported as positive or negative FBC sample will be used
G6PD screening
test 5 days
See report FBC sample will be used
Sickle Cell Test Urgent 1 hour
Screening test – reported as positive or negative
FBC sample will be used
The lab must be contacted by phone for any urgent
requests.
Emergency pre-op only. Recent transfusion will interfere
with test interpretation
ESR 2 hours
See table below
PMR, GCA/Temporal arteritis/Takayasu’s arteritis only
Minimum sample volume 2ml
Reticulocytes Urgent 1 hr
See table below FBC sample will be used Routine 4 hrs
Blood film 72 hours
See table below FBC sample will be used

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 59 of 109 Last printed 05/02/2020 12:10:00
Routine Haematology Return to: Haematology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Bone Marrow
Examination 2 weeks
See report
Reported by Consultant Haematologists
Must be arranged with Consultant Haematologist
Pyruvate
Kinase (PK) 2 weeks
See report
Minimum sample volume 1ml
Referred to Kings, London for analysis
Must be arranged with Consultant Haematologist

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 60 of 109 Last printed 05/02/2020 12:10:00
Haematology Adult Reference Ranges Return to: Haematology Test library
Male Female Units
Haemoglobin (Hb) 130 - 180 115 - 165 g/L
White Cell Count (WBC) 4.0 -15.0 4.0 - 15.0 109/L
Platelet Count (PLT) 150 - 400 150 - 400 109/L
Red Blood Count (RBC) 4.5 - 6.5 3.8 - 5.8 1012
/L
Mean Cell Volume (MCV) 80 - 97 80 - 97 fl
Packed Cell Volume (PCV)/Haematocrit (HCT) 0.40 - 0.54 0.37 - 0.47 L/L
Mean Cell Haemoglobin Concentration (MCHC) 300 - 360 300 - 360 g/L
Neutrophil Count 2.0 - 7.5 2.0 - 7.5 109/L
Lymphocyte Count 1.5 - 4.0 1.5 - 4.0 109/L
Monocyte Count 0.2 - 0.8 0.2 - 0.8 109/L
Eosinophil Count 0 - 0.4 0 - 0.4 109/L
Basophil Count 0 - 0.1 0 - 0.1 109/L
Reticulocytes 0.2 - 2.0
<100
0.2 - 2.0
<100
%
109/L
Plasma Viscosity 1.5 - 1.72 1.5 - 1.72 mPa
HbA2 2.3 - 3.4 2.3 - 3.4 %.
HbF 0 - 1.5 0 - 1.5 %
Erythrocyte Sedimentation Rate (ESR) 01 - 10.0 01 - 12.0 mm/hr
Adult reference ranges have been locally adapted from Haematology literature including Dacie and
Lewis Practical Haematology. The current age and sex specific ranges are included with each
report.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 61 of 109 Last printed 05/02/2020 12:10:00
6.3 Coagulation
6.3.1 Test library
Coagulation Return to: Haematology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Coagulation screen Urgent 90 min
Clinical decision values are subject to change. Current
ranges available on report. Contact lab for any queries.
Routine 4 hrs
D-Dimer Urgent 90 min
Clinical decision values are subject to change. Current
ranges available on report. Contact lab for any queries.
Routine 4 hrs
Unfractionated (UF)
Heparin
Urgent 90 min
Clinical decision values are subject to change. Current
ranges available on report. Contact lab for any queries.
Send to lab urgently. Must be processed within
4 hours of collection. Routine 4 hrs
Oral anticoagulants Urgent 90 min
Clinical decision values are subject to change. Current
ranges available on report. Contact lab for any queries.
For dosing contact the Anticoagulant Clinic on
Ext 4747 Routine 4 hrs
Thrombophilia
screen 4 weeks 3x
Clinical decision values are subject to change. Current
ranges available on report. Contact lab for any queries.
Factor V Leiden and Prothrombin G20210A
mutation screen sent to referral laboratory. Testing
will be carried out in accordance with BCSH
guidelines.
Lupus
anticoagulant
2 weeks
2x
Clinical decision values are subject to change. Current
ranges available on report. Contact lab for any queries.
Anti 10a assay Urgent 4 hrs
Clinical decision values are subject to change. Current
ranges available on report. Contact lab for any queries.
Sample should be taken 3 to 4 hours post dose Routine ≤72 hrs
Factor Assays Urgent 4 hrs
2x
Clinical decision values are subject to change. Current
ranges available on report. Contact lab for any queries.
Must be arranged with Consultant
Haematologist Routine 4 wks

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 62 of 109 Last printed 05/02/2020 12:10:00
Coagulation Return to: Haematology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Von Willebrand
assays 4 weeks 2x
Clinical decision values are subject to change. Current
ranges available on report. Contact lab for any queries.
Must be arranged with Consultant
Haematologist
Direct Oral
Anticoagulants
(DOAC)
Clinical decision values are subject to change. Current
ranges available on report. Contact lab for any queries.
Contact laboratory first
Normal reference ranges For PT , APTT and Fibrinogen are re calculated with each new lot of reagent using known normal samples. All other
reference ranges have been adapted from Haematology literature including Dacie and Lewis Practical Haematology. The current age and sex related
ranges are included with each report.
6.3.2 Factors affecting the results or processing of coagulation tests
Problem with sample Laboratory comment
Under-filled Will not be processed
Haemolysed Will be processed, depending on degree of haemolysis
Clotted Will not be processed
Lipaemic Will be processed, depending on degree of lipaemia
6.4 Immunology
Immunology would recommend non urgent samples that require special treatment should not be sent on a Friday, especially if the Monday following is a
Bank Holiday.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 63 of 109 Last printed 05/02/2020 12:10:00
6.4.1 Immunology test library
All immunology tests should be requested electronically. This is because the request forms generated by this process state the number and type(s) of
sample tubes required to perform all the testing. Please contact the laboratory if the test you require is not available via electronic requesting.
Our immunology samples are referred to other laboratories for testing. The majority of our samples are sent to the Immunology Department at MFT
Oxford Road. It is not possible for us to maintain a list of tests performed at other laboratories, so they are not listed in this handbook.
6.5 Blood transfusion
6.5.1 Two sample rule
In line with current British Committee for Standards in Haematology (BCSH) guidelines, two samples will be required to determine the blood group of a
patient before cross matched components are released. If a patient has a historical blood group on record, just one sample for the current request is
required.
Any patient that does not have a transfusion history (a known blood group on the laboratory computer system) will require a second group and antibody
screen. The transfusion laboratory will inform the clinician if a second sample is required.
Two samples (with two separate request forms) are required. These samples should be taken by two different people, or if bled by the same person
must be taken at a different time e.g. two independent separate venepunctures.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 64 of 109 Last printed 05/02/2020 12:10:00
6.5.2 Test library
Transfusion Return to: Haematology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Group and Save
Urgent 45 min
Valid for 3 days.
Patient ID stickers MUST NOT be used for transfusion
samples. Labels MUST be handwritten.
Two sample rule applies (see above)
Routine 24 hrs
Crossmatch
Urgent 45 min
Must have a valid Group and Save
Patient ID stickers MUST NOT be used for transfusion
samples. Labels MUST be handwritten. Routine 6 hrs
Direct Antiglobulin
Test (DAT) 24 hours
Not suitable for cord samples
Foetal cell count 48 hours
Kleihauer 48 hours Mate
rnal
Samples must be received in the lab within 24 hours of
delivery
Co
rd
Cold agglutinin titre 2 days
Telephone blood bank for advice

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 65 of 109 Last printed 05/02/2020 12:10:00
Transfusion Return to: Haematology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
HLA specific
antibody screen 10 days
Request form 3A – Diagnostic Laboratory FRM745
http://hospital.blood.co.uk/media/27701/frm745-hi-
request-form-3a-diagnostic-lab.pdf
HLA B27 10 days
Request form 3A – Diagnostic Laboratory FRM745
http://hospital.blood.co.uk/media/27701/frm745-hi-
request-form-3a-diagnostic-lab.pdf
HLA type Class 1
10 days
Request form 3A – Diagnostic Laboratory FRM745
http://hospital.blood.co.uk/media/27701/frm745-hi-
request-form-3a-diagnostic-lab.pdf
Platelet antibodies 9 days
3x
Patient leaflet -
http://hospital.blood.co.uk/media/27109/inf283.pdf
Request form 3D – Platelet Immunology FRM999
http://hospital.blood.co.uk/media/27703/frm999-hi-
request-form-3d-platelet-immunology.pdf 1x
Neonatal
alloimmune
thrombocytopenia
9 days
Mu
m
Patient leaflet –
http://hospital.blood.co.uk/media/27109/inf283.pdf
Request form 3D – Platelet Immunology FRM999
http://hospital.blood.co.uk/media/27703/frm999-hi-
request-form-3d-platelet-immunology.pdf
Dad
Ch
ild
>0.5ml

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 66 of 109 Last printed 05/02/2020 12:10:00
Transfusion Return to: Haematology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Heparin induced
thrombocytopenia
(HIT)
9 days
Patient Leaflet -
http://hospital.blood.co.uk/media/1881/b45bc8e7-af47-
473d-87e8-8f3e96d811b9.pdf
Request form 3D – Platelet Immunology FRM999
http://hospital.blood.co.uk/media/27703/frm999-hi-
request-form-3d-platelet-immunology.pdf
Anti-neutrophil
antibodies 30 days

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 67 of 109 Last printed 05/02/2020 12:10:00
7 Cellular Pathology
The Histology and Cytology laboratory (jointly referred to as Cellular Pathology) at the Wythenshawe
Site offers a diagnostic service for tissue and body fluid samples. The department provides a service
to the patients, clinicians and General Practitioners of the South Manchester and Tameside area
including Tameside and Glossop Integrated Care Organisation. The department specialises in
cardio-thoracic, breast, skin and gastrointestinal pathology.
Contact details for clinical or laboratory staff are available below for advice / interpretation of reports
or to enquire about further investigations, should the information you require not be in this handbook.
7.1 Contact details
Generic contact details Location Extension Information
Report enquiries Office 4813
At times, this number may have an
answering machine: please leave a
clear request and a number for us to
call you back
Report Fax Number Office 4809
Departmental nhs.net email address [email protected]
Return to Andrology, Histology sample collection, Frozen Sections, Booking frozen sections,
Consultant Name and Speciality Office Secretary Email address
Dr M Scott
Co-Head of Histopathology Gynaecology, Gastrointestinal, Urology
2144 2123 [email protected]
Dr N Ali Breast, Skin, Gynaecology, Gastrointestinal cytology
5663 4812 [email protected]
Dr P Bishop Cardiothoracic, Skin, Head & Neck, Haematolymphoid
Andrology 2159 2121 [email protected]
Dr A Davenport (part-time)
Co-Head of Histopathology Gastrointestinal
5311 2143 [email protected]
Dr H M Doran (part-time) Cardiothoracic
2138 2121 [email protected]
Dr V Howarth Skin, Gastrointestinal, Urology
2598 2123 [email protected]
Dr M Howe Breast, Urology
4806 4812 [email protected]
Dr R. Hunt Breast, Gastrointestinal, Gynaecology, Urology,
Gastrointestinal cytology 4807 4812 [email protected]
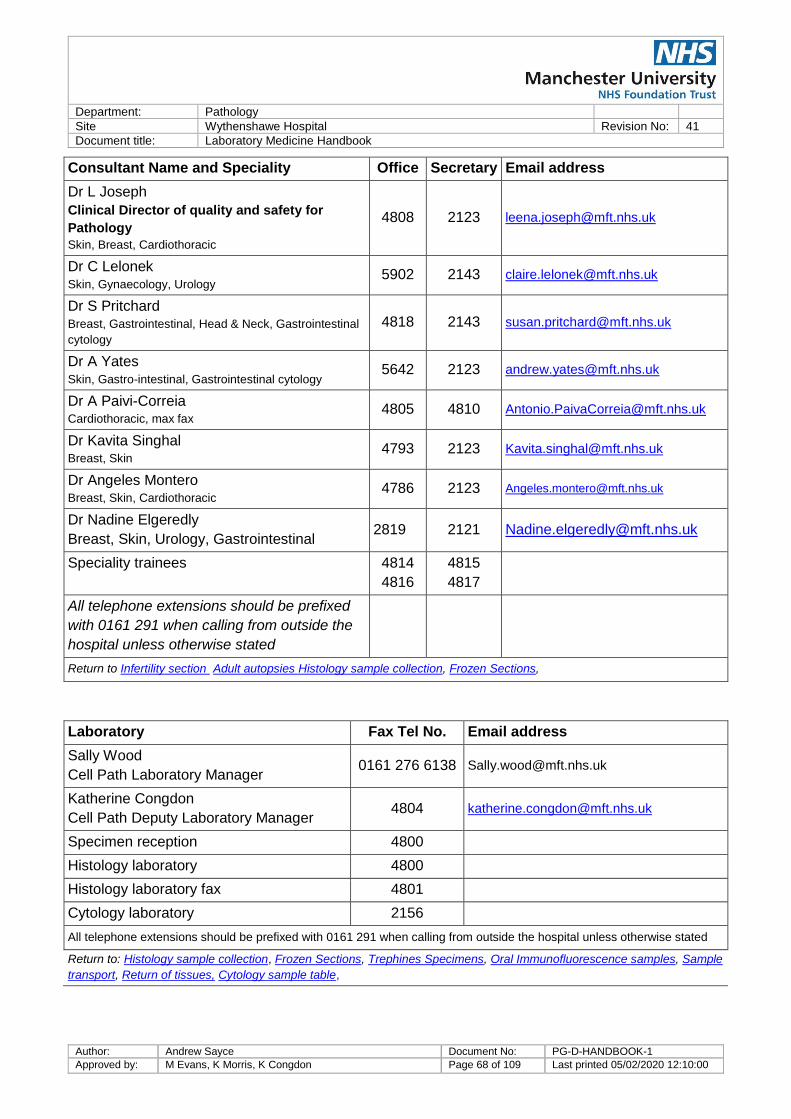
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 68 of 109 Last printed 05/02/2020 12:10:00
Consultant Name and Speciality Office Secretary Email address
Dr L Joseph
Clinical Director of quality and safety for
Pathology
Skin, Breast, Cardiothoracic
4808 2123 [email protected]
Dr C Lelonek Skin, Gynaecology, Urology
5902 2143 [email protected]
Dr S Pritchard Breast, Gastrointestinal, Head & Neck, Gastrointestinal
cytology
4818 2143 [email protected]
Dr A Yates Skin, Gastro-intestinal, Gastrointestinal cytology
5642 2123 [email protected]
Dr A Paivi-Correia Cardiothoracic, max fax
4805 4810 [email protected]
Dr Kavita Singhal Breast, Skin
4793 2123 [email protected]
Dr Angeles Montero Breast, Skin, Cardiothoracic
4786 2123 [email protected]
Dr Nadine Elgeredly
Breast, Skin, Urology, Gastrointestinal 2819 2121 [email protected]
Speciality trainees 4814
4816
4815
4817
All telephone extensions should be prefixed
with 0161 291 when calling from outside the
hospital unless otherwise stated
Return to Infertility section Adult autopsies Histology sample collection, Frozen Sections,
Laboratory Fax Tel No. Email address
Sally Wood
Cell Path Laboratory Manager 0161 276 6138 [email protected]
Katherine Congdon
Cell Path Deputy Laboratory Manager 4804 [email protected]
Specimen reception 4800
Histology laboratory 4800
Histology laboratory fax 4801
Cytology laboratory 2156
All telephone extensions should be prefixed with 0161 291 when calling from outside the hospital unless otherwise stated
Return to: Histology sample collection, Frozen Sections, Trephines Specimens, Oral Immunofluorescence samples, Sample
transport, Return of tissues, Cytology sample table,

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 69 of 109 Last printed 05/02/2020 12:10:00
7.2 General information
The histology / cytology laboratory is open from 8am until 5.30pm. Outside these hours relevant
personnel are on call for dealing with urgent cardio-thoracic transplant biopsies. Notice needs to be
given to the Consultant Histopathologist and the Biomedical Scientist of the intention to perform a
biopsy and to the Biomedical Scientist when the specimen is dispatched for transport to pathology.
All tissue taken for histological analysis will initially be stained with routine haematoxylin and eosin
(H&E) stain. Following this, additional staining tests may be performed to aid or confirm the initial
diagnosis. All cellular fluid samples are stained with H&E, papanicolaou, or giemsa stain, depending
on specimen type.
The Mortuary is open from 8.30am until 4pm and Anatomical Pathology Technicians operate a
limited on call service. They can be contacted via the duty manager in the first instance.
7.3 Sample acceptance
All specimens need to be accompanied by a correctly completed histology / cytology request form.
Please see sample acceptance criteria for more information.
It is recognised that histology samples are often not repeatable therefore the department has
protocols in place to deal with specimens and accompanied request forms that do not meet the
specimen acceptance criteria. A final report will not been issued until such details have been
corrected. The requesting clinician will be required to attend either the Laboratory at Wythenshawe
or Tameside. Samples from General Practitioners will be returned for amendment. All specimen
and/or request form amendments will need to have a specimen amendment form completed. If
amendments are not addressed within seven calendar days then an incident will be raised in
Ulysses.
7.4 Clinical information
In producing a final diagnostic histopathology or cytopathology report the Pathologists are essentially
looking to provide guidance and answers to clinical queries. Therefore it is essential that all relevant
clinical information is provided on the request form (paper based or electronic) so that the histological
and cytological features of the specimen can be interpreted within the clinical context. Rather than
simply repeating oneself under each heading give relevant clinical details, procedure details, medical
history and the clinically suspected (differential) diagnosis. This should include all previous
malignancies, whether in the same or any other organ system. Under Specimen Details, give the
precise anatomical site of the specimens sent. If there are multiple specimens, there should be a
one-to-one correspondence between the specimens listed on the card and the labelling of the
specimen pots. State any markers / sutures / clips, and their significance. Record any features of
the specimen that are likely to be difficult to interpret after fixation, particularly for complex resections.
If the relevant, appropriate clinical information is not provided this may lead to a delay in the final
report being issued.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 70 of 109 Last printed 05/02/2020 12:10:00
7.5 Sample containers
Container type Description Use
Fixed or air-
dried slides
Slide carrier
If alcohol spray fixative is required
(see cytology sample table), this
available from the cytology
laboratory.
Cytology samples
Plain
container
Sterile container
If MEM, cytology green collection
fluid, or cytorich red preservative
are required (see cytology sample
table), these are available from the
cytology laboratory.
Cytology samples
Plain
universal
Sterile container
If MEM,cytology green collection
fluid, or cytorich red preservative
are required (see cytology sample
table), these are available from the
cytology laboratory.
Cytology samples
CellPath
CellStor
Container prefilled with formalin
Available from the histology
laboratory
Small histopathology
samples
Bucket
Bucket prefilled with formalin
Available from the histology
laboratory .
Unfilled specimen containers for
specific, lung specimens to be
received fresh also available from
histology.
Larger
histopathology
samples
One-Piece
Microbiopsy
Cassette
Tissue Cassette For small tissue
biopsy samples.
Return to Cytology samples table

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 71 of 109 Last printed 05/02/2020 12:10:00
7.6 Histology sample collection
The majority of specimens for histology need to be placed in an appropriately sized container with
adequate amount of formalin (ideally 10x the volume of the sample) as soon as removed from the
patient. Specimen containers of all sizes, pre-filled with formalin, are available from histology, please
contact the laboratory. For specimens to be sent to the department not in formalin, empty specimen
containers of all sizes are also available.
7.7 Supply of sample containers
We supply prefilled containers of all sizes to departments at Wythenshawe Hospital and empty
buckets and prefilled biopsy pots to Tameside Hospital.
The exceptions to this rule are specimens requiring an urgent frozen section report, lung wedges and
resection specimens and specimens being transferred to the department by the Biobank team for
which they will have explicit patient consent for sampling. These specimens should not be sent in
formalin.
Prefilled specimen pots are only to be transported by the Trust transport department using the
dedicated barrels.
Any formalin that is identified as out of date and therefore shouldn't be used should be returned to the
Histology department at Wythenshawe site so that the fluid can be safely disposed of.
7.8 Factors that prevent a detailed accurate diagnosis
There are several factors that prevent a detailed accurate diagnosis:
Insufficient tissue sent
Insufficient formalin or lack of formalin
Insufficient space within specimen container
Delay in placing specimen in formalin
Specimen being placed in a unsuitable solution, for example saline
Should any of these factors affect the issuing of a final report, then an incident may be raised in
Ulysses. If a final report is able to be issued, factors that may have affected this result will be
included in this report.
7.9 Frozen sections
7.9.1 Booking cardiothoracic frozen section requests
To book a cardiothoracic frozen please liaise with the cardiothoracic booking clerks who can access
the shared electronic diary for booking such requests. The laboratory access the electronic diary
regularly to see what frozen sections are booked. Any changes to these booking should be
communicated to the Cellular Pathology department as soon as these changes are known.
7.9.2 Booking other frozen section requests
Frozen section requests, from either Wythenshawe or Tameside, need to be booked 24 hours in
advance by calling the secretarial service.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 72 of 109 Last printed 05/02/2020 12:10:00
Should the notice for a frozen section be less than 24 hours, the service may be unavailable.
7.9.3 Once specimen has been taken
Once taken, the specimens should be delivered to the department fresh (not in formalin) as soon as
practically possible, together with the receipt book to audit the delivery of the specimen to the
department. Wythenshawe frozen sections requests are delivered directly to the Histopathology
department at Wythenshawe: specimens taken at Tameside are taken directly to the Tameside
Pathology laboratory. Delay in delivery of the specimen will delay the issuing of the frozen section
report.
If the frozen section service is no longer required please ring the laboratory as soon as possible to
notify us of the cancellation.
A preliminary report will be issued stating the diagnosis obtained from the frozen section. To ensure a
timely report is available, please provide contact details of where this report should be issued. A full
report will follow once the tissue has been formalin fixed and paraffin sections examined by a
Pathologist.
7.10 Bone Marrow Trephine specimens.
All bone marrow trephine specimens should be placed in formalin and referral request made on the
HODS database to be referred into the Manchester Haematological Cancers Diagnostic Partnership
(HCDP). These specimens are sent from the clinic to Central Specimen Reception at Oxford Road
Campus via the Haematology department at Wythenshawe Hospital.
7.11 Skin immunofluorescence specimens
Skin biopsies requiring immunofluorescence need two samples to be taken from the same area. One
is to be placed in formalin; the other for immunofluorescence should be placed in Mikel’s medium
which is obtainable from the Histopathology Department at Salford Royal Hospital. Specimens
should be sent to Wythenshawe hospital histopathology; these will be booked onto the Trust
laboratory system and then packaged by laboratory staff for hospital transport to Salford Royal
hospital. Reports are returned to Wythenshawe histopathology, where they are then uploaded onto
the laboratory information system.
7.12 Oral immunofluorescence specimens
The Oral Pathology Department at Oxford Road Campus has special gel tubes to preserve the
specimens. Please contact them for advice on how to source the relevant specimen containers and
any instructions that need to be adhered to for taking the specimen. Specimens should be sent to
Wythenshawe hospital histopathology in the gel tubes; these will be booked onto the Trust
laboratory system and then packaged by laboratory staff for hospital transport to Oxford Road
Campus. Reports are returned to Wythenshawe histopathology, where they are then uploaded onto
the laboratory information system.
If the specimen taken is larger than the containers in use then please contact the histopathology
department at Oxford Road Campus for further advice.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 73 of 109 Last printed 05/02/2020 12:10:00
7.13 Amputated limb specimens
If the patient would like their amputated limb returning to them following surgery, please contact the
histology department for further information. Amputated limbs for disposal should not be sent to
either the Mortuary or Histopathology for disposal. Should any limbs be received for disposal, the
requesting theatre will be contacted and arrangements made for the limb to be returned immediately.
7.14 Cytology samples
Cytology specimens are either fluid based or received as smears of fine needle aspirations (FNA) or
imprints of tissue biopsies on glass slides.
Cytology specimens should be sent in sample containers of an appropriate size to adequately hold
the specimen. Some specimens are received fresh, with no additives and therefore should be
delivered to the department as soon as collected to prevent deterioration of the sample (see table
below). Other specimens are received in cell collection fluid or a preservative such as cytorich red.
These preservatives assist with preservation of the cells within the sample. In the case of thyroid
aspirates some slides should be fixed using the alcohol based fixative spray and some air dried. The
air dried slides are for Giemsa staining.
Cytorich red and alcohol spray fixative are both available from cytology by contacting the cytology
laboratory.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 74 of 109 Last printed 05/02/2020 12:10:00
Cytology samples
Test TAT Sample type Biological Interval / Clinical
Decision Values Special precautions/ Information
Serous fluid 7 days
N/A N/A
Urine 7 days
Bronchial washings 7 days
Bronchial-alveolar
lavage 7 days
Sputum 7 days
Bladder washings 7 days
Urethral washings 7 days
Ureteric washings 7 days
Cyst fluid 7 days
Serous fluid 7 days
Urine 7 days
Bronchial washings 7 days
Bronchial-alveolar
lavage 7 days
FNA 7 days
N/A Cytorich red or cytology green collection fluid
required, available from the cytology laboratory.
EBUS 7 days
EUS 7 days
Bronchial brushings 7 days
Bile brushings 7 days
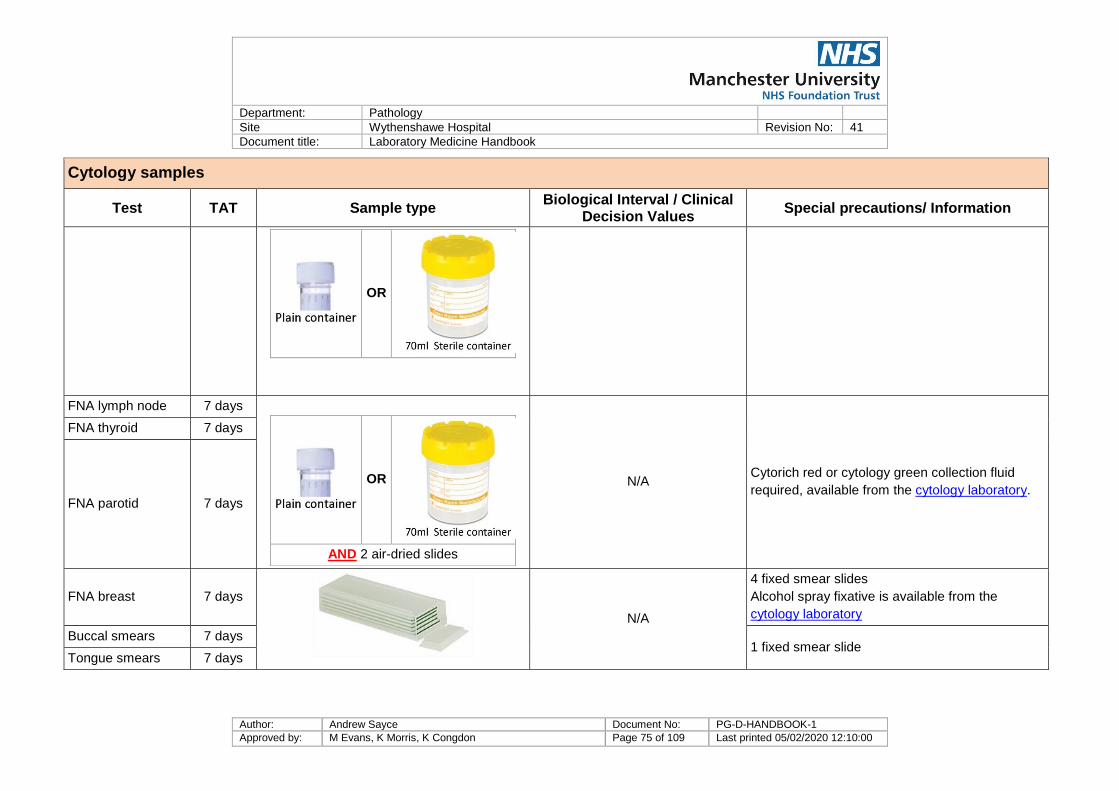
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 75 of 109 Last printed 05/02/2020 12:10:00
Cytology samples
Test TAT Sample type Biological Interval / Clinical
Decision Values Special precautions/ Information
OR
FNA lymph node 7 days
OR
AND 2 air-dried slides
N/A Cytorich red or cytology green collection fluid
required, available from the cytology laboratory.
FNA thyroid 7 days
FNA parotid 7 days
FNA breast 7 days
N/A
4 fixed smear slides
Alcohol spray fixative is available from the
cytology laboratory
Buccal smears 7 days 1 fixed smear slide
Tongue smears 7 days

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 76 of 109 Last printed 05/02/2020 12:10:00
7.14.1 Broncho-alveolar lavages (BAL)
These specimens requiring a differential cell count should be received on ice and by 5pm on working
days only. This is to ensure the appropriate slide preparations can be made. The cytology
department can examine for Pneumocystis carinii on Broncho-alveolar lavage specimens if required
however, the preferred method is for the sample to be sent to microbiology.
7.14.2 Endobronchial ultrasound guided aspirate specimens (EBUS)
These should be delivered to the department as soon as possible so that preparation of the samples
can be undertaken. It is appreciated that reports are wanted on these specimens in a timely fashion
for MDT discussion.
7.14.3 Joint Fluids
Joint fluids should be sent to Cytology. For any cases where microbiology testing is also required,
two separate samples should be collected and two requests made; one for cytology testing and the
other for microbiology testing. Failure to request separate testing will result in a delay in cytology
testing as the sample will first be sent to microbiology based at Oxford Road Campus, before being
returned to the Cytology department at Wythenshawe Hospital for testing. This may lead to an
erroneous result due to the delay in testing and potential degradation of the specimen.
7.15 Cervical Cytology
Cervical cytology is sent to Oxford Road Campus for reporting. The contact details are:
Jacquelyn Medlock [email protected] Cytology Manager Adanna Ehirim [email protected] Lead BMS Cytopathology Richard Lambert [email protected] Lead BMS Cytopathology
Manchester Cytology Centre Clinical Science Building 2 Manchester Royal Infirmary Oxford Road Manchester M13 9WL
Tel: 0161 276 5119 Fax: 0161 276 5113
7.16 Andrology
The Cytology department offers infertility and post vasectomy testing.
7.16.1 Infertility
Infertility services are performed at both the MFT Wythenshawe site and Tameside site on an
appointment based system. Appointments are available at Wythenshawe on Wednesday and Friday
and at Tameside on a Tuesday morning. Please contact the secretarial team at Wythenshawe for
information. Once a patient has made an appointment a kit will be posted, via Royal Mail, which
contains a specimen pot and instructions.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 77 of 109 Last printed 05/02/2020 12:10:00
Instructions for both Tameside and South Manchester patients are provided by the laboratory to GPs
and clinicians who wish to request these tests.
The bottom of this information leaflet needs to be completed by the patient when the sample has
been produced to inform the laboratory of information that may affect the quality of the result.
Infertility samples without a correctly completed request form from the requesting clinician / GP and
no or incomplete information sheet will be rejected. Infertility samples, which are not received in the
specimen pot provided, will also be rejected. The patient will then be expected to make another
appointment and produce another sample.
Reports are issued, in line with the fifth edition of the “WHO laboratory manual for the examination
and processing of human semen”.
In case of difficulty interpreting the new ranges below, please contact a consultant specialising in
andrology.
7.16.2 Post vasectomy
Vasectomy Analysis services are performed at Tameside on a Thursday morning. At Wythenshawe
they are undertaken every working day, during 8.30am until 3.30 pm. No appointment for this service
is required. Patients are required to be given the relevant information leaflet, which is provided by
the laboratory to GPs and clinicians who wish to request these tests.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 78 of 109 Last printed 05/02/2020 12:10:00
Infertility Reports Return to: Andrology expert
Infertility section
Test TAT Sample
type Biological Interval / Clinical Decision Values
Special precautions/ Information
Infertility
testing 3 weeks Semen
Volume: Although we may measure the weight of the sample but we report by
volume, the lower reference limit being 1.5 ml.
Sperm concentration The lower reference limit has been reduced to 15.106 per ml
Total sperm number The WHO editorial committee considered that total sperm number per
ejaculate provides a more accurate assessment of testicular function than
does sperm concentration. There is now a lower reference limit for the total
sperm number of 39.106 per ejaculate: we will calculate this.
pH: Lower reference range is 7.2. No upper limit is defined.
Motility: There are three categories: progressive motility (PR, spermatozoa moving
actively), non-progressive motility (NP, all other patterns of motility with an
absence of progression) and immotile (IM, no movement). The lower
reference limits are Total motility (PR + NP); 40%, Progressive motility
(PR); 32%.
Vitality 58% of spermatozoa are alive. Vitality will be assessed if the total motility is
less than 50%.
Sperm morphology The lower reference limit, which is 4% normal forms.
Infertility specimens to
be received in the
department 45 minutes
from production.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 79 of 109 Last printed 05/02/2020 12:10:00
7.17 Sample transport
Specimens for histology or cytology are not allowed to be transported via the pneumatic tube system.
The transport of the specimens to the department is undertaken by the respective hospital transport
from both the Wythenshawe and the Tameside site. Dedicated barrels are provided, by the histology
department, as the secondary packaging for use to transport the samples. The primary packaging
being the container the specimen is in. Urgent samples may be delivered to the department ad hoc;
these should be transported in an appropriate container, with a tightly fitting lid. Specimens should
not be transferred to the department without appropriate packaging. All specimens should be
received with a documented tracking sheet detailing the patient identifiers, specimen type and where
the specimen has been taken. These tracking sheets are checked on arrival in the histology
department and returned to the department or area the specimen was taken from for staff to record
that the specimen has been received safely in Histology.
For specimens received from hospitals where there is not a routine transport service arranged, a
courier service is used. This includes specimens transported from Stepping Hill Hospital. Transport
between Wythenshawe Histopathology and Oxford Road Campus is in place at regular intervals
throughout the day to ensure timely transport of specimens to be processed at each site.
If you have any queries or should extra transport be required for any reason please contact the Trust
transport department via switchboard.
Transport of the Tameside samples occurs twice daily. The transport collects specimens from
theatres, endoscopy and then pathology before leaving pathology at 9.30 am and 3.30 pm for
delivery to Wythenshawe Site histopathology. This transport also delivers samples from GP
surgeries within the Tameside borough. This transport also delivers supplies from Wythenshawe Site
back to Tameside for the relevant theatres and clinics.
Samples received from both Trusts are recorded using a paper based system and in some cases
electronically. Please ensure such records are completed before dispatch of samples. For paper
based requesting, only specimen request forms provided by histopathology should be used to
request specimen testing. These forms should not be photocopied, for a supply of forms, please
contact the laboratory.
Samples from the GP surgeries within the South Manchester District are delivered to the main
pathology reception area and then collected by histology staff on an ad hoc basis. Some of these
samples are requested electronically others are accompanied by hand written request forms. For
paper based requesting, only specimen request forms provided by histopathology should be used to
request specimen testing. These forms should not be photocopied, for a supply of forms, please
contact the laboratory.
If samples from Wythenshawe Site cannot be accepted due to failing the specimen acceptance
criteria, the requesting Clinician will be contacted and asked to attend the laboratory as soon as
possible to make the necessary amendments and complete a Specimen Labelling Amendment form.
This will form part of the record of this sample.
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 80 of 109 Last printed 05/02/2020 12:10:00
If samples are from GP’s within the Wythenshawe borough, these are returned to the GP practice for
amendments and completion of a Specimen Labelling Amendment Form. The specimen can then be
returned to the Wythenshawe Histology department for processing.
If samples from Tameside Hospital cannot be accepted due to failing the specimen acceptance
criteria, the requesting Clinician will be contacted and informed the sample will be returned to
Tameside Pathology Specimen Reception. The Clinician should then attend the department to make
any necessary amendments and complete a Specimen Labelling Amendment form. This will form
part of the record of this sample. The sample is then returned to Histology at Wythenshawe Site for
processing.
If samples are from GP’s within the Tameside borough, these are returned to Tameside Specimen
Reception to then be sent to the GP practice for necessary amendments to be made and Specimen
Amendment Form. This is then returned to Wythenshawe Histology via Specimen Reception at
Tameside.
If specimens received from Stepping Hill Hospital cannot be accepted due to failing specimen
acceptance criteria, the requesting Clinician will be contacted and asked to attend the laboratory as
soon as possible to make the necessary amendments and complete a specimen amendment form.
This will form part of the record for this sample.
Please be aware that a final report will not be made available until the necessary amendments have
been made. Failure to amend the specimen request form of specimen pot in a timely fashion will lead
to a delay in the final report and if the specimen is not amended in 7 days, a Ulysses record will be
raised.
7.18 Reports
All reports issued by the department are available on the relevant Trusts’ electronic systems. This
will be EPR at Wythenshawe site and Lorenzo within Tameside. For primary care reports are
distributed to the GP practice systems.
Paper reports are still sent to the users at Tameside and some GP practices. Tameside reports,
including those for the Tameside GP practices, are transported back to the Pathology Department at
Tameside site using the twice daily transport. They are then distributed as required from Tameside
Pathology. Paper reports for GP practices within the Wythenshawe Site catchment area are sent via
second class post.
7.19 RCPath cancer standards and data sets
For cancer resections, the Department follows guidelines and reporting templates recommended in
the Royal College of Pathologists Cancer Data Sets.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 81 of 109 Last printed 05/02/2020 12:10:00
7.20 Multidisciplinary Team Meetings (MDT’s)
Histopathologists participate in MDT meetings as required, on both the Wythenshawe Tameside
sites. Participation in the Tameside MDTs and links into multi-centre MDTs is often via video
conferencing.
7.21 Turnaround times
The Cellular Pathology department monitors turnaround times in line with the RCPath key
performance indicators – proposals for implementation July 2013. This document states that 80% of
diagnostic cases should be reported within 7 calendar days and 90% within 10 calendar days.
For up to date information on the department’s current turnaround figures, please contact the Deputy
Manager.
7.22 Material sent away for further tests
The laboratory on occasion refers material (paraffin embedded blocks or stained slides) to the
Manchester Haematological Cancers Diagnostic Partnership. This is a joint partnership between
Manchester Foundation Trust and the Christie Hospital for confirmation and classification of
lymphomas and to the Christie Hospital for opinion and / or confirmation of pathology in a small
number of cases.
Material may also be referred to St. Marys Genetics department for Genetic / molecular testing which
quotes a 10 day turnaround time for results. This includes EGFR, BRAF and KRAS.
A very small number of cases are referred to other Specialist Histopathologists for expert second
opinion or review.
7.23 Return of tissues
On occasion, patients request the return of tissues following a surgical procedure. This may be for
various cultural or religious reasons. Patients have a right to have their tissues returned to them.
1. If there is no need for the tissue to be examined histologically and the patient wishes to take it
away immediately, then it does not need to be sent to the Pathology Department.
2. In some cases, the tissue needs to be examined histologically. The remaining tissue will then
be returned to the patient by the Pathology Department. Sometimes the patient is
hospitalised or is uncertain as to what he wants done with the tissue, in which case it will be
stored by the Pathology Department. In such cases, please speak to the Deputy Laboratory
Manager or a senior Biomedical Scientist to ensure that the patient’s wishes are met with
regard retention and return of their tissue sample. Please be aware that failure to inform the
department that the patient wishes to have their tissue sample retained and returned to them
may result in the specimen being disposed of as tissue samples are only kept in the
department for 4 weeks following the issue of a histology report. If the specimen is returned to
the patient, written advice as to the hazards of the formalin fixative used will be provided.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 82 of 109 Last printed 05/02/2020 12:10:00
7.24 Disposal of tissues
Specimens are not permitted to be sent to histology for disposal purpose. We provide a diagnostic
service, not a disposal service. Any specimens received where disposal is indicated will be
processed and a report issued. Only POC specimens may be disposed of without histological
examination if indicated by the patient on consent form 9.
7.25 Errors happen
There is evidence that the rate of clinically significant reporting errors for Histopathologists is 1 to 2%.
Since histology often provides the definitive diagnosis, error in histology may have a profound impact
on patient management. There are things that you can do to reduce the occurrence and impact of
errors:
Make sure that request cards and specimen pots meet the requirements of the sample
acceptance criteria with unambiguous and correct patient demographics.
Provide clinical information on the request card, including details of previous specimens,
whether here or in another hospital.
Question cases where there is an apparent discrepancy between the clinical, radiological and
pathological diagnosis.
Review cancers at an MDT
7.26 Manchester Cancer Research Centre Tissue Bank
The Manchester Cancer Research Centre (MCRC) Tissue Bank is an initiative to collect and bank
tissue samples from cancers to facilitate research. The project started collecting in April 2008. To
contact the team please ring 0161 446 3659 or click on the hyperlink above.
7.27 Measurement uncertainty
For information regarding measurement uncertainty for specimens in Cellular Pathology please
contact the laboratory.
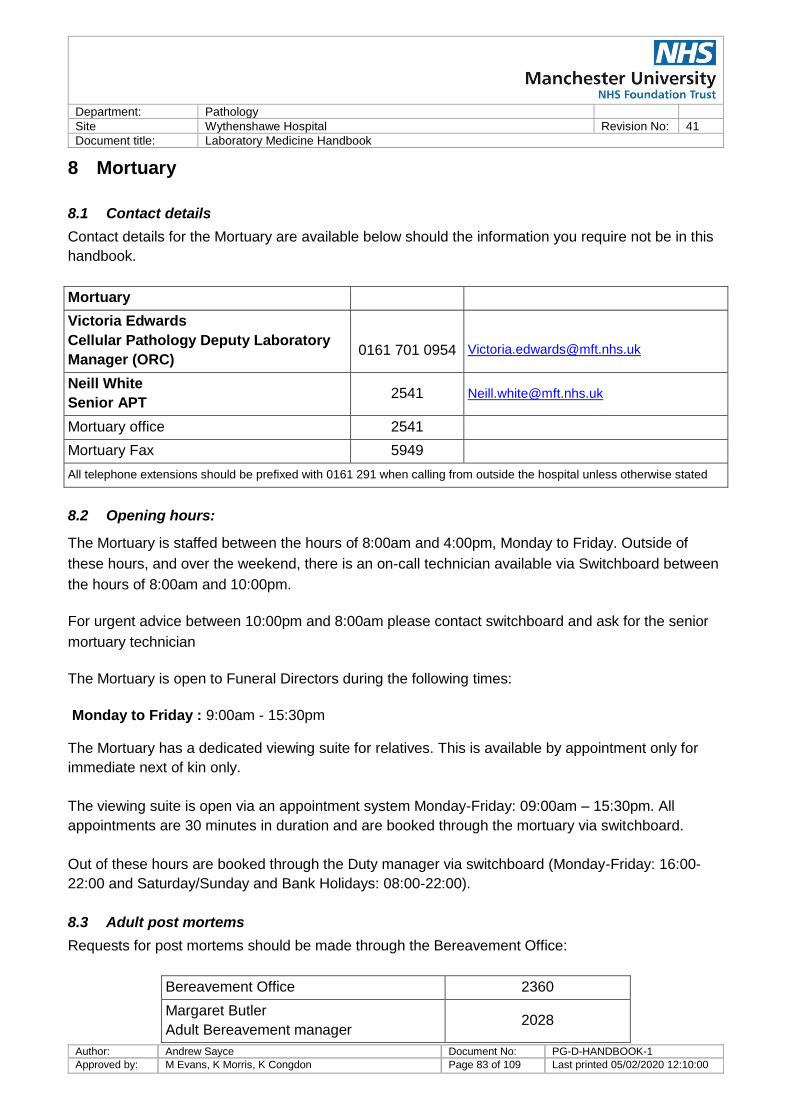
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 83 of 109 Last printed 05/02/2020 12:10:00
8 Mortuary
8.1 Contact details
Contact details for the Mortuary are available below should the information you require not be in this
handbook.
Mortuary
Victoria Edwards
Cellular Pathology Deputy Laboratory
Manager (ORC)
0161 701 0954
Neill White
Senior APT 2541 [email protected]
Mortuary office 2541
Mortuary Fax 5949
All telephone extensions should be prefixed with 0161 291 when calling from outside the hospital unless otherwise stated
8.2 Opening hours:
The Mortuary is staffed between the hours of 8:00am and 4:00pm, Monday to Friday. Outside of
these hours, and over the weekend, there is an on-call technician available via Switchboard between
the hours of 8:00am and 10:00pm.
For urgent advice between 10:00pm and 8:00am please contact switchboard and ask for the senior
mortuary technician
The Mortuary is open to Funeral Directors during the following times:
Monday to Friday : 9:00am - 15:30pm
The Mortuary has a dedicated viewing suite for relatives. This is available by appointment only for
immediate next of kin only.
The viewing suite is open via an appointment system Monday-Friday: 09:00am – 15:30pm. All
appointments are 30 minutes in duration and are booked through the mortuary via switchboard.
Out of these hours are booked through the Duty manager via switchboard (Monday-Friday: 16:00-
22:00 and Saturday/Sunday and Bank Holidays: 08:00-22:00).
8.3 Adult post mortems
Requests for post mortems should be made through the Bereavement Office:
Bereavement Office 2360
Margaret Butler
Adult Bereavement manager 2028
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 84 of 109 Last printed 05/02/2020 12:10:00
Bereavement office fax 2665
Please be clear as to whether you wish to request a hospital (consent) post mortem, or you need to
refer a death to the coroner. The Coroner has indicated that he would like all deaths associated with
a hospital acquired infection reported to him: it would be appropriate for the reporting doctor to advise
whether the deceased died with the infection or of the infection, or that this is uncertain.
Please do not make promises to relatives that a post mortem will be done the next day. Post
mortems are performed in a timely fashion but there are multiple factors determining when they are
done. Refer the relatives to the bereavement office for this information.
The consent form for a hospital post mortem is extensive but logical. You need to familiarize yourself
with it before meeting with the next of kin.
In the event of the coroner ordering a post mortem examination, no consent from the next of kin is
required. However, the coroner's view of the information that is required from the post mortem is
likely to be narrower than that of a clinician. For example, the coroner will be satisfied with a
diagnosis of "carcinomatosis", where a clinician will want to know the tumour type and the site of the
primary. Once the pathologist is able to give a cause of death to the satisfaction of the coroner, there
is no authority for further investigation. In particular, the coroner has no authority to allow tissue to be
taken for histology, once a natural cause of death has been given. In order to satisfy the needs of
medical audit and education, it is necessary to obtain consent from the next of kin for investigations
over and above those authorised by the coroner. For this purpose, you need to ask the next of kin to
complete the consent form. Annotate it to indicate that this consent is being taken to supplement a
coroner's post mortem.
For hospital post mortem examinations, not under the authorisation of the coroner, consent must be
sought from the person in the highest ranking qualifying relationship as per the Human Tissue Act. A
member of the Consultant body who undertakes autopsies or the bereavement manager should be
present when consent is taken to ensure that this is taken in line with the Human Tissue Act.
The coroner has restricted the release of post mortem findings to clinicians. If you want to know
about a post mortem, permission needs to be obtained from the coroner. Phone: 0161 219 2222,
Fax: 0161 274 7329, [email protected].
Information relating to the Manchester coroner is available at www.manchester.gov.uk/coroners
The Wythenshawe Site holds a license from the Human Tissue Authority for the storage of bodies,
the making of a post-mortem examination and the removal of tissues at post mortem: we are listed at
the HTA web site under Wythenshawe Hospital. There is extensive advice from the Human Tissue
Authority at www.hta.gov.uk/guidance/codes_of_practice.cfm
Human Tissue Authority Designated 0161 291 5663 / 4812

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 85 of 109 Last printed 05/02/2020 12:10:00
Individual
Dr Nisha Ali, Consultant Histopathologist
8.4 Infectious bodies
We inform undertakers of infectious risks by issuing an Infection control notification sheet. You will
be asked to complete this form at the same time as you complete a death certificate. The staff of the
Bereavement Office will advise, but if necessary, consult a histopathologist or microbiologist.
8.5 Medical Devices
8.5.1 Pacemakers and defibrillators
Implantable devices such as pacemakers and defibrillators contain batteries which explode on
incineration. It is therefore essential that they are removed from bodies prior to cremation. If you
know that a body contains such a device, please inform the Mortuary APT’s. If you are completing
the first part of the cremation form, you are required to state if a device is present
Defibrillators pose an additional hazard, in that they are liable to be triggered by the act of removing
them from the body if they have not first been inactivated. Increasingly, they are indistinguishable
from pacemakers on external inspection of the body. If you know that the device is a defibrillator, you
must inform the Mortuary APT’s specifically so that we can ask an ECG technician to inactivate the
device.
8.5.2 FixionTM intramedullary nails
FixionTM intramedullary nails have a saline-filled chamber. On incineration, the steam pressure is
sufficient to cause an explosion. You need to state on the first part of the cremation form if such an
implant is present. At the time of implantation, the next of kin should have been advised of this
hazard.
Removal of the above devices are completed by the Funeral Directors.
8.6 Stillbirths and foetuses, post mortems and disposal
Any live born baby that dies should be referred to a paediatric pathologist at St Mary’s Hospital for a
post mortem.
For post mortems on stillbirths and non-viable foetuses, please contact the bereavement midwife on
the maternity unit at Wythenshawe hospital on ext 2930 or 2963.
8.6.1 Wythenshawe Hospital patients
For first trimester miscarriages, any pregnancy remains should be sent to the histology department
accompanied by a Consent Form 9 “Consent for Histopathological Examination and Disposal of
Tissue Following Early Pregnancy Loss Up To 12 Weeks 6 Days” signed by the mother and
indicating her wishes for the remains from her miscarriage/ectopic pregnancy. Note Consent Form 9
solicits consent to histological examination of the non-fetal tissues only. The fetus will not be

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 86 of 109 Last printed 05/02/2020 12:10:00
dissected or examined microscopically but may be commented as to the presence of it within the
specimen.
The specimen cannot be examined without appropriate consent; lack of an accompanying
appropriately completed or legible consent form will result in delay to reporting which may have
adverse effects on the patient's management. In such cases, staff in histopathology will contact the
clinicians, whom this patient is under, requesting a consent form to be sent as soon as possible
before the specimen can be examined. If no consent is received within seven calendar days, an
incident report will be raised in Ulysses.
If you have any questions, please speak to the laboratory or to the specialist midwife on maternity.
8.6.2 Tameside patients
For first trimester miscarriages, from patients’ at Tameside, any pregnancy remains should be sent to
the histology department accompanied by a Dukinfield cremation form. This is completed and signed
by the mother indicating her understanding of the specimen being sent for cremation following
histological examination.
Only non-fetal tissue is examined; any fetus will not be dissected or examined microscopically, but
may be commented as to the presence of it within the specimen. Should a cremation form be
received without parental signature, the form and specimen pot will be returned to the mortuary at
Tameside.
Staff at Tameside mortuary will then liaise with clinicians to ensure a cremation form is completed. If
no cremation form is received, a report may still be issued, however, staff from Wythenshawe Site
histology will contact clinicians at Tameside requesting a form to be sent. If this is received prior to
disposal, the form can be sent to Wythenshawe Site and matched with the specimen pot. If not
received prior to disposal, the specimen is returned to the Mortuary at Tameside, where staff will
continue to liaise with clinicians for completion of the cremation form.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 87 of 109 Last printed 05/02/2020 12:10:00
9 Microbiology
The Microbiology Laboratory service for Wythenshawe Hospital is provided by the Manchester
Medical Microbiology Partnership (MMMP), situated at the Oxford Road Campus. All information
regarding the microbiology service is available on the MFT Laboratory Medicine website. Click on the
MMMP User Manual link. The manual includes information on how to request samples out-of-hours
and a list of contact details.
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 88 of 109 Last printed 05/02/2020 12:10:00
10 Mycology Reference Centre, Manchester
The UK NHS Mycology Reference Centre Manchester (MRCM) is situated on the second floor of the
Education & Research Centre at Wythenshawe Hospital. The MRCM provides specialist mycology
diagnostic services for Manchester University NHS Foundation Trust, and hospitals throughout
Greater Manchester and the UK.
Antifungal and mycological advice can be offered on the diagnosis of disease, clinical management
and care of patients.
The MRCM laboratory is open from 08:30 to 17:00 hours Monday to Friday. Urgent medical advice
can be obtained by contacting Wythenshawe Hospital switchboard and asking for the on-call
Infectious Diseases Consultant.
10.1 Contact Details
Member of staff Location Extension Email address
Professor MD Richardson Director of MRCM and Consultant Clinical
Scientist in Mycology
Office 5914
[email protected] Secretary 5839
Mobile 07545 994 936
Dr CB Moore Deputy Director of MRCM, and Principal
Clinical Scientist
Office 4223 [email protected]
[email protected] Secretary 5839
Dr R Richardson Consultant Medical Mycologist
Office 5941 [email protected]
General enquiries Office 5839 [email protected]
Test enquiries/results Laboratory 2124 [email protected]
Website www.mycologymanchester.org
All Wythenshawe Hospital samples should be sent to the Clinical Sciences Building, Wythenshawe
Hospital where appropriate transportation to the Mycology Reference Centre Laboratory will be
ensured.
External samples can be sent using the DX System. Our details are DX 332601 MANCHESTER
96M.
Alternatively samples may be posted, ensuring appropriate packaging (see 1.10.3), to:
Mycology Reference Centre Manchester 2nd Floor Laboratories Education and Research Centre Wythenshawe Hospital Southmoor Road Manchester M23 9LT
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 89 of 109 Last printed 05/02/2020 12:10:00
10.2 Additional Tests
Additional tests can be requested by contacting the laboratory, although it must be recognised that
the archive sample available will have a limited volume. Furthermore, samples may be beyond the
validation period for particular tests.
10.3 Measurement Uncertainty
All assays have a margin of error associated with the calculation of the numerical value. This is
referred to as the measurement uncertainty. Further information on the measurement of uncertainty
for our laboratory assays is available by contacting the laboratory.
10.4 Antifungal Drug Levels
Please ensure that details of all antifungal drugs the patient is receiving are given - this information is
essential to ensure appropriate testing is performed.
Please record the date and time the specimen is taken, together with the time of last dose. These
details ensure correct interpretation of results.
10.4.1 Indications for monitoring
All patients receiving flucytosine
Patients receiving itraconazole - to check drug absorption and to monitor compliance
Patients receiving posaconazole - to check drug absorption and to monitor compliance
Patients receiving isavuconazole – to check drug absorption and to monitor compliance
All patients receiving voriconazole – a pre-dose sample is required
Fluconazole in patients on dialysis/haemofiltration
Patients failing azole therapy
If drug interactions are suspected
10.4.2 References
Richardson MD and Warnock DW. Fungal Infection: Diagnosis and Management. 4th Ed.
Oxford, Wiley-Blackwell, 2012.
Ashbee HR, Barnes RA, Johnson EM, Richardson MD, Gorton R, Hope WW.
Therapeutic drug monitoring (TDM) of antifungal agents: guidelines from the British
Society for Medical Mycology. J Antimicrob Chemother 2014; 69: 1162–1176.
10.5 Identification and susceptibility testing of medically important fungi
Respiratory, vaginal and oral swabs will be cultured within our laboratory. Identification and/or
susceptibility testing will be performed as appropriate.
Other original specimens will be processed by the Microbiology Department, MFT Manchester Royal
Infirmary. If fungus is isolated, the Microbiology Department will then send the culture on to the
Mycology Reference Centre for identification and/or susceptibility testing.
Please ensure that the request form states that mycological investigations (identification and
susceptibility testing) are required.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 90 of 109 Last printed 05/02/2020 12:10:00
10.5.1 Indications for testing
All life-threatening fungal infections, to ensure that the optimal therapy is administered
Isolates from patients at increased risk of fungal infection, such as those infected with HIV,
immunosuppressed or on ICU, so that appropriate antifungal therapy can be given
Mucosal candidosis not responding to therapy
Clinically significant non-Candida albicans species due to increasing incidences of both infection
and fluconazole resistance
Rare pathogens because of an increased incidence of resistance and unpredictability of
resistance patterns

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 91 of 109 Last printed 05/02/2020 12:10:00
10.6 Test library
Antifungal Drug Levels Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision
Values Special precautions/ Information
Antifungal drug
levels See below
Specimens should be transported to the laboratory as soon as possible. If
a delay is anticipated, samples should be refrigerated. Assays validated for
transportation of samples at room temperature for up to and including 5
days.
For all drugs, the time of previous dose and time of sampling should
be recorded accurately to allow correct interpretation.
Flucytosine
Generally
next
working
day
Adult 5ml Neonate
0.5ml
Adult Pre-dose 30-40 mg/L
Post-dose 70-80 mg/L
Neonate:
(<3 months)
Pre-dose 20-40 mg/L
Post-dose 50-80 mg/L
Levels >100mg/L are potentially toxic
Therapeutic Drug Monitoring is essential for clinical management
Pre-dose: Oral and IV: Just before dose*
Post dose: Oral: 2 hours post dose*
IV: 30 minutes post dose*
Commence: Around second/third dose
Frequency: Twice weekly, or more often if renal function is changing
Lab assay runs:
Day of receipt as required Samples must be notified or received before 1pm

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 92 of 109 Last printed 05/02/2020 12:10:00
Antifungal Drug Levels Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision
Values Special precautions/ Information
Itraconazole 1-2 days
Adult 5ml Neonate
0.5ml
Target level:
Prophylaxis: pre 0.5–1.0mg/L
Therapy: pre 1.0-2.0mg/L
Commence monitoring only after steady
state has been reached (1-2 weeks on
oral therapy, little variation through the
day)
Therapeutic Drug Monitoring is essential for clinical management
Pre-dose: Oral: not needed
Post dose: Oral: random*
Commence: Only after steady state has been reached.
Frequency: Dependent on patient - seek advice - usually monthly for the first three months and then every three months. Check levels two weeks after any dose change or if there might be a possible drug interaction. Repeat levels if concern about poor compliance / poor absorption.
Lab assay runs:
Each weekday
Posaconazole
1-2 days
Adult 5ml Neonate
0.5ml
Target level:
Prophylaxis: pre 0.7-1.5mg/L
Therapy: pre 1.0-3.75mg/L
Consider reduction if > 3.0mg/L
Commence monitoring only after steady
state has been reached (1-2 weeks on
oral therapy, little variation through the
day)
Therapeutic Drug Monitoring is essential for clinical management
Pre-dose: Oral: not needed
Post dose: Oral: random*
Commence: Only after steady state has been reached.
Frequency: Dependent on patient - seek advice - usually monthly for the first three months and then every three months. Check levels a few weeks after any dose change or if there may be a drug interaction. Repeat levels if concern about poor compliance / poor absorption.
Lab assay runs:
Each weekday

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 93 of 109 Last printed 05/02/2020 12:10:00
Antifungal Drug Levels Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision
Values Special precautions/ Information
Voriconazole 1-2 days
Adult 5ml Neonate
0.5ml
Pre-dose level target range 1.3 -
5.7mg/L
Dose escalation is advised for any level
less than 1.3mg/L
Due to the non-linear kinetics of the drug
in adults, informed clinical judgement
regarding target range is not possible on
any sample except pre-dose samples
Therapeutic Drug Monitoring is essential for clinical management
Pre-dose: Oral: 10-14h post-dose window* (ie pre-dose as BD dosing) IV: Just before dose*
Post dose: Not required
Commence: after 3 days of therapy
Frequency: Dependent on patient - seek advice. If patient has suspected invasive disease or very unwell, do a level at day 5 of treatment and repeat at least weekly until therapeutic levels obtained. If IV to oral switch done, repeat level about 5 days after switch. Once therapeutic levels achieved, repeat levels at 2, 4, 8 and 12 weeks, and every three months thereafter. For other diagnoses, do a level at week 2, 4, 8 and 12 of treatment and every three months thereafter. Repeat levels two weeks after any dose change or if a drug interaction is suspected. Repeat levels if concern about poor compliance / poor absorption.
Lab assay runs:
Each weekday

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 94 of 109 Last printed 05/02/2020 12:10:00
Antifungal Drug Levels Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision
Values Special precautions/ Information
Isavuconazole
1-2 days
Adult 5ml Neonate
0.5ml
Target levels not yet established and
informed clinical judgement is required
for dose adjustments. Consult Mycology
Reference Centre for advice.
Pre: 1-4mg/L.
The mean half-life of isavuconazole in
plasma is 130 hours and it has linear
kinetics.
Therapeutic Drug Monitoring is essential for clinical management
Pre-dose: Oral: 10-24 hours post-dose window* (ie pre-dose as BD dosing) IV: Just before dose*
Post dose: Not required
Commence: after 3 days of therapy
Frequency: Dependent on patient - seek advice. If patient has suspected invasive disease or very unwell, do a level at day 5 of treatment and repeat at least weekly until therapeutic levels obtained. Once therapeutic levels achieved, repeat levels at 2, 4, 8 and 12 weeks, and every three months thereafter. For other diagnoses, do a level at week 2, 4, 8 and 12 of treatment and every three months thereafter. Repeat levels two weeks after any dose change or if a drug interaction is suspected. Repeat levels if concern about poor compliance / poor absorption.
Lab assay runs:
Each weekday
* these samples are most useful for clinical management
Itraconazole, Posaconazole and Voriconazole TDM are performed by Biochemistry, Wythenshawe Hospital (UKAS 9063).
Isavuconazole TDM is performed by Antimicrobial Reference Laboratory, Bristol (UKAS 8099).
Check www.UKAS.com for up to date accreditation status of referral laboratories.
Fluconazole levels can be assayed to test compliance or absorption. Contact Mycology Reference Centre.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 95 of 109 Last printed 05/02/2020 12:10:00
Identification and Susceptibility Testing of Yeasts and Moulds Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample
type
Biological Interval / Clinical Decision
Values Special precautions/ Information
Full identification
and susceptibility
testing of all
medically
important yeasts
and moulds
Identification:
Yeast: 2-5 days
Mould: 2-7 days
Longer if molecular sequence-
based identification is required.
Susceptibility testing:
Yeast: 1-5 days
Longer for some yeasts and
drugs.
Mould: 3-7 days
Longer if culture requires
incubation.
As per Microbiology guidelines
N/A The following susceptibility tests are routinely performed :
Yeasts Moulds
Flucytosine Itraconazole
Fluconazole Amphotericin
Amphotericin Voriconazole
Itraconazole Posaconazole
Voriconazole Isavuconazole
Micafungin Micafungin
Anidulafungin Terbinafine
Posaconazole
Other drugs, including caspofungin, are available upon request

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 96 of 109 Last printed 05/02/2020 12:10:00
Cryptococcal antigen latex agglutination test Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval /
Clinical Decision Values
Special precautions/ Information
Latex
agglutination test
for cryptococcal
antigen.
Collection is not
time dependent.
Generally
same day
CSF by lumbar puncture, serum
and urine
Minimum 500 l
N/A
Indications for testing:
Testing for Cryptococcus neoformans capsular antigen is one of the
most reliable methods for the diagnosis of cryptococcosis.
Suspected cryptococcosis, including cryptococcal meningitis,
pulmonary and disseminated disease, in both immunocompromised,
e.g. HIV-positive, and immunocompetent patients.
With appropriate controls, a positive test is indicative of infection.
Perform repeat lumbar puncture after 2 weeks of treatment. Repeated
testing can be used to monitor response to treatment, monitor for
duration of treatment course, especially in HIV-positive patients.
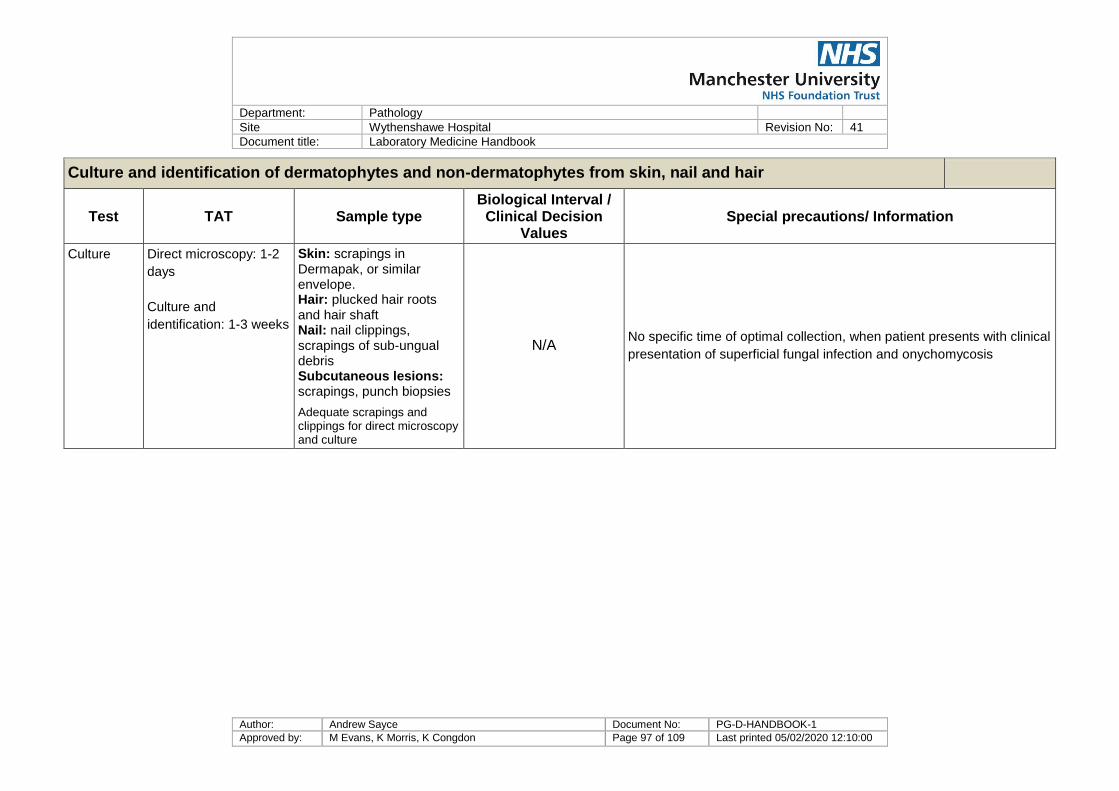
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 97 of 109 Last printed 05/02/2020 12:10:00
Culture and identification of dermatophytes and non-dermatophytes from skin, nail and hair
Test TAT Sample type Biological Interval /
Clinical Decision Values
Special precautions/ Information
Culture Direct microscopy: 1-2
days
Culture and
identification: 1-3 weeks
Skin: scrapings in Dermapak, or similar envelope. Hair: plucked hair roots and hair shaft Nail: nail clippings, scrapings of sub-ungual debris Subcutaneous lesions: scrapings, punch biopsies
Adequate scrapings and clippings for direct microscopy and culture
N/A No specific time of optimal collection, when patient presents with clinical
presentation of superficial fungal infection and onychomycosis

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 98 of 109 Last printed 05/02/2020 12:10:00
Aspergillus galactomannan assay Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
PLATELIA
assay for
Aspergillus
galactomannan
circulating
antigen in serum
and other body
fluids: this test is
indicated for
presumptive
diagnosis of
Aspergillus
infection
This assay
is
performed
every day,
Monday-
Friday.
TAT:
95% within
one
weekday.
Serum 700 µl
or 5 ml clotted
blood
The Platelia galactomannan (GM) test results are
expressed as an index value and are reported as negative,
weak positive, or positive – with the index value given.
Interpretation of values depend on the sample type:
Blood: GM index values of >0.5 are interpreted as positive
Bronchoalveolar lavage fluid: GM index values >1.0 are
interpreted as positive.
Index values 0.5-1.0 have a lower predictive value than
values >1.0 and are interpreted as weakly positive. Further
sampling is recommended.
Sputum: The test is not validated for sputum samples. GM
index values of >1.0 are interpreted as positive.
Specificity of the test is improved if two or more
consecutive specimens are positive.
No specific time of optimal collection. First clinical
indication of pulmonary or invasive aspergillosis.
Prospective screening twice weekly to monitor for evidence
of elevated and rising levels of galactomannan which
provides a convenient surrogate marker for invasive or
pulmonary Aspergillus disease (depending on sample type
tested).
This test should be used in conjunction with other
diagnostic procedures.
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 99 of 109 Last printed 05/02/2020 12:10:00
Pan-fungal glucan assay Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
FUNGITELL
assay for -1-3-D-
glucan: the
fungal glucan
test is indicated
for presumptive
diagnosis of
fungal infection
This assay
is
performed
most days,
Monday-
Friday.
TAT:
95% within
two
weekdays,
generally
available
within one
weekday.
5 ml clotted
blood
Samples are
easily
contaminated
- it is
recommended
that blood is
not separated
before
sending.
The Fungitell test results are expressed in pg/ml of serum
and range from undetectable (<31.250 pg/ml) to >500
pg/ml.
Glucan values of <60 pg/ml are interpreted as negative
results.
Values 80 pg/ml are interpreted as positive.
Values from 60 to 79 pg/ml are interpreted as
indeterminate results and suggest possible fungal infection.
Additional sampling is recommended.
The glucan test has a very high negative predictive
value.
This is the possibility that patients with a negative
screening test result do not have the disease (true
negative).
No specific time of optimal collection. First clinical
indication of invasive fungal infection.
Prospective screening twice weekly to monitor for evidence
of elevated and rising levels of glucan which provides a
convenient surrogate marker for invasive fungal disease.
This test should be used in conjunction with other
diagnostic procedures. The Fungitell –1-3-D Glucan assay
does not detect certain fungal species such as the genus
Cryptococcus, which produces very low levels of 1-3-D-
glucan. This assay also does not detect the Zygomycetes,
such as Lichtheimia, Mucor and Rhizopus, which are not
known to produce 1-3-D-glucan.
Aspergillus precipitin test Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Agar gel double
diffusion for
Aspergillus
precipitins
against
Aspergillus
fumigatus
7-10 days
Serum 700 µl
or 5 ml clotted
blood
No specific time of optimal collection. When patient
presents with aspergilloma (mycetoma, fungal ball),
allergic bronchopulmonary aspergillosis or other pulmonary
manifestations of aspergillosis.
Serial samples during treatment.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 100 of 109 Last printed 05/02/2020 12:10:00
Aspergillus PCR on respiratory samples Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Elitech
Aspergillus PCR
Seven
days
Respiratory
secretions
(BAL, sputum)
1-2 ml
minimum,
daily if
Aspergillus
infection is
suspected.
See report No specific time of optimal collection. First clinical
indication of pulmonary or invasive aspergillosis.
Assay for the quantitative detection of Aspergillus species
genomic DNA extracted from respiratory specimens from
the lower respiratory tract, as an aid to the diagnosis of
pulmonary and invasive Aspergillus infection. The results
need to be taken in context of the clinical condition of the
patient and other diagnostic test results.
Aspergillus fumigatus Cyp51A pyrosequencing Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval /
Clinical Decision Values
Special precautions/ Information
Aspergillus
fumigatus
Cyp51A
pyrosequencing
assay
2 - 3
weeks.
Sometimes
DNA
amplificatio
n fails, and
no result is
possible.
Respiratory secretions (BAL,
sputum, 1-2 ml minimum), or
Aspergillus fumigatus isolates.
See report No specific time of optimal collection.
Assay for the pyrosequencing-based detection of triazole resistance-
associated polymorphisms of the Cyp51A gene in Aspergillus fumigatus. All
specimens are initially processed for Aspergillus PCR to determine
suitability. Please contact MRCM for further information.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 101 of 109 Last printed 05/02/2020 12:10:00
Pneumocystis PCR Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval / Clinical Decision Values Special precautions/ Information
Pneumocystis
PCR assay 4 days
Respiratory
secretions
(BAL, sputum)
1-2 ml
minimum,
daily if
Pneumocystis
infection is
suspected.
See report No specific time of optimal collection. First clinical
indication of Pneumocystis infection.
This test is performed by Virology at MRI.
Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 102 of 109 Last printed 05/02/2020 12:10:00
Molecular identification of fungi from culture negative, microscopy positive specimens Return to: Mycology Information
Appendix A (list of tests)
Test TAT Sample type Biological Interval /
Clinical Decision Values
Special precautions/ Information
DNA extraction
and molecular
sequencing
Two
weeks.
Sometimes
DNA
extraction
fails, and
no result is
possible.
Original specimen, if a fluid
specimen, such as pus, BAL,
pleural fluid, peritoneal fluid,
transported at room
temperature and stored at 4°C,
-20°C or -80°C.
Fixed paraffin section (5-10
normal or thick sections placed
together in a sterile container
and transported at room
temperature)
Fungal identification
provided
Indications for testing: clinically significant fungal infection, with negative
culture and serology.
Using sophisticated DNA extraction technology, fungal DNA can be obtained
from most samples in which fungal hyphae are seen, including fixed paraffin
sections. In some cases, no sample was submitted for culture, in other
cases, culture is negative.
Cases should be discussed with the MRCM staff, who will advise.
Surveillance of hospital environments, homes, public buildings, for Aspergillus species and allergenic moulds
Test TAT Sample type Biological Interval / Clinical
Decision Values Special precautions/ Information
Culture of air
samples, culture
of dust and
material
samples.
5-7 days
Air samples,
settled dust,
surface
samples,
material
samples
N/A
No specific time. Surveillance during hospital construction, maintenance,
demolition and renovation, water damage, faulty air filtration and conditioning, and
outbreaks.
Minimum: one air sample and one dust sample from patients' rooms and general
hospital areas. More intensive sampling where reservoir of Aspergillus is most
likely to occur.
Sampling availability, processing of submitted samples, identification and
interpretation: please contact the laboratory for further information.

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 103 of 109 Last printed 05/02/2020 12:10:00
11 Appendix A – A-Z List of tests
Test Department
5HIAA (urine) Biochemistry
5HIAA (serum) Biochemistry
17-hydroxyprogesterone Biochemistry
HbA1c Biochemistry
ACE (Angiotensin converting enzyme) Biochemistry
ACTH Biochemistry
Acyl carnitines/free carnitine/MCADD profile Biochemistry
AFP Biochemistry
Albumin (serum) Biochemistry
Albumin (pleural fluid) Biochemistry
Alcohol (Ethanol) Biochemistry
Aldosterone Biochemistry
ALP (adult) Biochemistry
Alpha-1-antitrypsin Biochemistry
ALT Biochemistry
Amino acids (plasma) Biochemistry
Amino acids (urine) Biochemistry
Ammonia Biochemistry
Lipase (serum) Biochemistry
Lipase (fluid) Biochemistry
Androstenedione Biochemistry
Anti 10a assay Haematology
Antifungal Drug Levels Mycology
Anti-neutrophil antibodies Haematology
Arterial Blood Gases Biochemistry
Aspergillus galactomannan Mycology
Aspergillus PCR Mycology
Aspergillus precipitin test Mycology
AST Biochemistry
B12 Biochemistry
B2 microglobulin Biochemistry
Base Excess Biochemistry
Bence-Jones protein Biochemistry
Bicarbonate (arterial blood gas) Biochemistry
Bicarbonate (serum) Biochemistry
Bilirubin Biochemistry
Blood film Haematology
Bone Marrow Examination Haematology
CA-125 Biochemistry
CA19-9 Biochemistry

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 104 of 109 Last printed 05/02/2020 12:10:00
Test Department
Caeruloplasmin Biochemistry
Calcium Biochemistry
Calcium (Amended) Biochemistry
Carbamazepine Biochemistry
Carboxyhaemoglobin Biochemistry
Catecholamines Biochemistry
CEA Biochemistry
Chloride Biochemistry
Cholinesterase/acetylcholinesterase Biochemistry
Chromium and cobalt Biochemistry
Citrate Biochemistry
CK Biochemistry
Coagulation Haematology
Coagulation screen Haematology
Cold agglutinin titre Haematology
Combined pituitary function test Biochemistry
Complement C3 Biochemistry
Complement C4 Biochemistry
Copper (serum) Biochemistry
Copper (urine) Biochemistry
Cortisol (blood) Biochemistry
Cortisol (urine) Biochemistry
Cotinine Biochemistry
Creatinine Biochemistry
Creatinine Clearance Biochemistry
Crossmatch Haematology
CRP Biochemistry
Cryoglobulins Biochemistry
Cryptococcal antigen latex agglutination test Mycology
CSF Biochemistry
CSF glucose Biochemistry
CSF lactate Biochemistry
CSF protein Biochemistry
Culture and identification of dermatophytes and non-dermatophytes from skin, nail and hair
Mycology
Cyclosporin Biochemistry
Cystine Biochemistry
D-Dimer Haematology
Dexamethasone Biochemistry
Dexamethasone suppression test Biochemistry
DHEAS Biochemistry
Digoxin Biochemistry
Direct Antiglobulin Test (DAT) Haematology

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 105 of 109 Last printed 05/02/2020 12:10:00
Test Department
Direct oral anticoagulants (A10a) Haematology
Down’s syndrome screening Biochemistry
Drugs of abuse screen (urine) Biochemistry
Dynamic Function Tests Biochemistry
eGFR Biochemistry
Endocrinology Biochemistry
ESR Haematology
Everolimus Biochemistry
Factor Assays Haematology
Faecal elastase (pancreatic) Biochemistry
Faecal reducing substances Biochemistry
Faeces Biochemistry
Fasting triglycerides Biochemistry
Ferritin Biochemistry
FK506 (Tacrolimus) Biochemistry
Fluconazole Mycology
Flucytosine Mycology
Foetal cell count Haematology
Folate Biochemistry
Free T3 Biochemistry
Free T4 Biochemistry
FSH Biochemistry
Full Blood Count Haematology
G6PD screening test Haematology
Galactosaemia screening test Biochemistry
Gentamicin Biochemistry
GGT Biochemistry
Glandular Fever screening test Haematology
Globulin Biochemistry
Glucose Biochemistry
Glucose (fasting) Biochemistry
Glucose tolerance test Biochemistry
Glucose tolerance test with GH suppression Biochemistry
GnRH Stimulation test Biochemistry
Group and Save Haematology
Growth hormone Biochemistry
Gut hormone profile (fasting) Biochemistry
Haemoglobinopathy (Hb Variant /thalassaemia) Haematology
Haptoglobin Biochemistry
hCG Biochemistry
HDL cholesterol Biochemistry
Heparin induced thrombocytopenia (HIT) Haematology
High Sensitivity Troponin T Biochemistry

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 106 of 109 Last printed 05/02/2020 12:10:00
Test Department
HLA B27 Haematology
HLA specific antibody screen Haematology
HLA type Class 1 Haematology
Identification and Susceptibility Testing of Yeasts and Moulds Mycology
IgA Biochemistry
IGF-1 Biochemistry
IgG Biochemistry
IgG subclasses (IgG4 can also be requested separately) Biochemistry
IgM Biochemistry
Immunology - There are too many tests to list here and it is subject to change. Please contact the laboratory for further information.
Haematology
Infertility reports Histopathology
Insulin and c-peptide Biochemistry
Insulin stimulation test Biochemistry
Iron Biochemistry
Isavuconazole Mycology
Itraconazole Mycology
Kleihauer Haematology
Lactate Biochemistry
Lamotrigine Biochemistry
LDH (serum) Biochemistry
LDH (pleural fluid) Biochemistry
LH Biochemistry
Bio_Urine_Light_chains Biochemistry
Lithium Biochemistry
Lupus anticoagulant Haematology
Macroprolactin Biochemistry
Magnesium (serum) Biochemistry
Magnesium (urine) Biochemistry
Malaria screen Haematology
Mannose binding lectin Biochemistry
Metanephrines Biochemistry
Methaemoglobin Biochemistry
Microalbumin (ACR) Biochemistry
Molecular identification of fungi from culture negative, microscopy positive specimens
Mycology
Mycophenolate (MPA) Biochemistry
Neonatal alloimmune thrombocytopenia Haematology
Oestradiol Biochemistry
Oligoclonal bands (CSF) Biochemistry
Oral anticoagulants Haematology
Organic acids (urine) Biochemistry
Orosomucoid (Alpha-1 acid glycoprotein) Biochemistry

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 107 of 109 Last printed 05/02/2020 12:10:00
Test Department
Osmolality (serum) Biochemistry
Osmolality (urine) Biochemistry
Other Fluids Biochemistry
Oxalate Biochemistry
Pan-fungal glucan assay Mycology
Paracetamol Biochemistry
pCO2 Biochemistry
pH (blood) Biochemistry
pH (pleural fluid) Biochemistry
Phenobarbital Biochemistry
Phenytoin Biochemistry
Phosphate (serum) Biochemistry
Phosphate (urine) Biochemistry
PIIINP (Type III procollagen peptide) Biochemistry
Plasma Metanephrines Biochemistry
Plasma Viscosity Haematology
Platelet antibodies Haematology
Pleural Fluid Biochemistry
Pneumocystis PCR Mycology
pO2 Biochemistry
Porphobilinogen/ urobilinogen / Porphyria screen Biochemistry
Porphyrin screen Biochemistry
Posaconazole Mycology
Potassium (serum) Biochemistry
Potassium (urine) Biochemistry
Prednisolone Biochemistry
Procalcitonin Biochemistry
Progesterone Biochemistry
Prolactin Biochemistry
Prolonged fasting test Biochemistry
Protein Biochemistry
Protein Electrophoresis Biochemistry
PSA Biochemistry
PTH Biochemistry
Pyruvate Kinase (PK) Haematology
Referred Tests Biochemistry
Renal stone analysis Biochemistry
Renin Biochemistry
Reticulocytes Haematology
Rheumatoid Factor Biochemistry
Routine Biochemistry Biochemistry
Routine Haematology Haematology
Salicylate Biochemistry

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 108 of 109 Last printed 05/02/2020 12:10:00
Test Department
Salivary cortisol Biochemistry
Salivary Testosterone
Selenium Biochemistry
SHBG Biochemistry
Short Synacthen test Biochemistry
Sickle Cell Test Haematology
Sirolimus Biochemistry
Sodium (serum) Biochemistry
Sodium (urine) Biochemistry
Specialist Tests Biochemistry
Specific Proteins Biochemistry
Surveillance of hospital environments, homes, public buildings, for Aspergillus species and allergenic moulds
Mycology
Sweat test Biochemistry
Teicoplanin Biochemistry
Testosterone Biochemistry
Theophylline Biochemistry
Therapeutic Drug Monitoring Biochemistry
Thrombophilia screen Haematology
Tobramycin Biochemistry
Total cholesterol Biochemistry
Total protein (serum) Biochemistry
Total protein (pleural fluid) Biochemistry
TPMT (Thiopurine S-methyltransferase) Biochemistry
TPO Biochemistry
Transferrin Biochemistry
Transfusion Haematology
Triglyceride Biochemistry
TSH Biochemistry
Tumour Markers Biochemistry
Unfractionated Heparin Haematology
Urate (serum) Biochemistry
Urate (urine) Biochemistry
Urea Biochemistry
Urinalysis Biochemistry
Urine reducing substances Biochemistry
Valproate Biochemistry
Vancomycin Biochemistry
Very long chain fatty acids (VLCFA) Biochemistry
Vitamin A & E Biochemistry
Vitamin D Biochemistry
Von Willebrand assays Haematology
Voriconazole Mycology

Department: Pathology
Site Wythenshawe Hospital Revision No: 41
Document title: Laboratory Medicine Handbook
Author: Andrew Sayce Document No: PG-D-HANDBOOK-1
Approved by: M Evans, K Morris, K Congdon Page 109 of 109 Last printed 05/02/2020 12:10:00
Test Department
Water deprivation test Biochemistry
Xanthochromia Biochemistry
Zinc Biochemistry
β-OH butyrate/free fatty acids Biochemistry





























