Embed Size (px)
Citation preview

Vol. 106 No. 3 September 2008
ORAL AND MAXILLOFACIAL PATHOLOGY Editor: Mark W. Lingen
Labial salivary gland biopsies in Sjögren’s syndrome: still thegold standard?Carol M. Stewart, MS, DDS, MS,a Indraneel Bhattacharyya, DMD, MSD,b
Kathleen Berg, PhD,c Donald M. Cohen, DMD, MS, MBA,d Christine Orlando, DO,e
Peter Drew, MD,f Nadim M. Islam, BDS,g Junu Ojha, BDS,h Westley Reeves, MD,i
Gainesville, FL; Indianapolis, IN; Detroit, MIUNIVERSITY OF FLORIDA, INDIANA UNIVERSITY, AND UNIVERSITY OF DETROIT MERCY
Objectives. The accuracy and diagnostic benefits of the labial salivary gland (LSG) biopsy for Sjögren’s syndrome (SS)have received mixed reviews. This study was conducted to assess (1) the inter-rater agreement among 5 pathologists,and (2) the relationship between biopsy findings and clinical disease parameters.Study design. Three oral pathologists (OP) and two surgical pathologists (SP) provided independent diagnoses, focusscores, and plasma cell characterizations for 37 LSG biopsies. Inter-rater reliability was assessed using percentage ofoverall agreement and intraclass correlation coefficients. Relationships between diagnoses and clinical parameterswere assessed by nonparametric correlations.Results. Overall agreement among the pathologists was poor, although the intra-specialty agreement was good. Theratings of OP were most highly correlated with serological measures, while those of SP were correlated with salivaryflow rate and disease damage.Conclusion. Since the LSG biopsy can be the determining factor in SS diagnoses, these demonstrated inconsistencies
merit further consideration. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:392-402)Sjögren’s syndrome (SS) is a chronic autoimmune dis-ease characterized by lymphocytic infiltration of theexocrine glands and symptoms of persistent oral andocular dryness. Symptoms may be limited to a localeffect on the salivary and lacrimal glands, or extend toinclude widespread involvement of multiple organ sys-tems.1 For many years, the labial salivary gland (LSG)biopsy has been considered an important consideration
This project was funded by the University of Florida Center forAutoimmune Diseases.aAssociate Professor, Department of Oral and Maxillofacial Surgeryand Diagnostic Sciences, University of Florida College of Dentistry;Co-Director, University of Florida, Center for Autoimmune Diseases.bAssistant Professor, Department of Oral and Maxillofacial Surgeryand Diagnostic Sciences, University of Florida College of Dentistry.cResearch Coordinator, Center for Orphaned Autoimmune Disorders;Department of Department of Oral and Maxillofacial Surgery andDiagnostic Sciences, University of Florida College of Dentistry.dProfessor, Department of Oral and Maxillofacial Surgery and Diag-nostic Sciences, University of Florida College of Dentistry.eClinical Assistant Professor, University of Florida, College of Med-
icine.392
among other parameters to help confirm the SS diag-nosis.2-4 The LSG biopsy is performed on the lower lipfollowing administration of local anesthesia. A 1.5- to2.0-cm horizontal incision is made on clinically normallabial mucosa, parallel to the vermillion border andlateral to the midline. Five or more accessory salivaryglands are harvested, formalin fixed, and embedded inparaffin. Sections of 5 �m are stained with hematoxylinand eosin and examined histopathologically. A charac-
fClinical Associate Professor, University of Florida, College of Medicine.gAssistant Professor, Department of Oral Pathology, Medicine andRadiology, Indiana University School of Dentistry.hAssistant Professor, Department of Diagnostic Sciences, School ofDentistry University of Detroit Mercy.iProfessor and Chair, Rheumatology and Clinical Immunology, Col-lege of Medicine; Co-Director, University of Florida, Center forAutoimmune Diseases.Received for publication Jan 18, 2008; returned for revision Mar 26,2008; accepted for publication Apr 18, 2008.1079-2104/$ - see front matter© 2008 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2008.04.018
sy con
OOOOEVolume 106, Number 3 Stewart et al. 393
teristic histopathologic feature in minor salivary glandsin SS is focal lymphocytic sialadenitis.3-7 Historically,the identification of more than one focus (a focus is acluster of 50 or more lymphocytes) within a 4 mm2 areaof glandular tissue has been considered supportive of adiagnosis of SS.4-6 However, according to criteria re-cently proposed by the 2002 American-European Con-sensus group (AECG), a more liberal criterion of one ormore lymphocytic foci is recommended.7 In early re-ports, the labial salivary gland biopsy was one of sev-eral criteria used in conjunction with other parametersto establish a definitive diagnosis. With time, the diag-nostic significance of the labial salivary gland biopsyhas increased and it has been anecdotally referred to as“the gold standard” by some physicians. The AECGcriteria7 require either positive auto-antibodies (antiRo/SS-A or anti-La/SS-B) or a positive LSG biopsy toconfirm a primary SS diagnosis.
In the past few years, the accuracy of the biopsyinterpretation, impact on disease classification, and di-agnostic benefits of this procedure have been reviewedwith mixed findings.8-16 To further investigate these
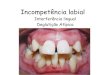
Fig. 1. A, Labial salivary gland biopsy consistent with Sjögreunits (H&E, magnification �5). B, Labial salivary gland biop
Table I. Characteristic histopathological features of SjSjögren’s syndrome
Patchy, focal periductal or perivascular mononuclear infiltrates withplasma cells, and macrophages
One or more foci per 4 mm2 of tissue adjacent to intact, normal-appFoci are seen consistently throughout the lobules in the specimenLack of ductal dilitationLack of fibrosis
important issues, this retrospective study was con-
ducted with 2 specific aims. The first aim was to assessthe concordance (inter-rater reliability) of histopatho-logical interpretations of labial salivary gland biopsiesamong 5 boarded histopathologists: 3 oral and maxil-lofacial pathologists (OP) and 2 surgical pathologists(SP). In addition, the inter-rater reliability among the 2groups of pathologists, as well as the potential impacton treatment from lack of agreement, was reviewed.The second aim was to assess predictive relationshipsbetween the labial salivary gland histopathologicalfindings and clinical disease parameters.
METHODSSubjects
The study group consisted of 37 female patientsreferred to the University of Florida College of Den-tistry Oral Medicine Clinic for evaluation of siccasymptoms of longer than 3 months’ duration, with apossible diagnosis of SS. The review of the medicalhistory, patient signs and symptoms, an unstimulatedwhole salivary flow rate,17 and the labial minor salivarygland biopsy were performed in the Oral Medicine
ndrome, showing multiple lymphocytic foci and intact acinarsistent with Sjogren’s syndrome (H&E, magnification �10).
’s syndrome and chronic sialadenitisChronic sialadenitis
mphocytes, Scattered and diffuse lymphocytic andplasmacytic infiltration
mucous acini Acinar atrophy
Ductal dilitationDiffuse interstitial fibrosis
n’s sy
ögren
�50 ly
earing
Clinic. The subject’s medical record provided by the

OOOOE394 Stewart et al. September 2008
referring rheumatologist was reviewed to confirm thereview of systems, diagnostic tests, and serologicallaboratory results. The rheumatologic diagnostic eval-uation included a Schirmer’s test, detection of serumANA, anti-Ro/SS-A, anti-La/SS-B, rheumatoid factor,anti-ds DNA, anti-RNP, anti Sm, anti-HCV, sedimen-tation rate, gammaglobulins, and thyroid profile. Alllaboratory tests were performed through the ShandsHospital clinical lab and their reference ranges wereapplied. The Schirmer test was considered abnormal orpositive if 5 mm or less of tear fluid was measured in 5minutes without the use of local anesthesia. In addition,an index of disease damage18 was completed for eachparticipant using information from the medical record.The histopathological report for the labial salivarygland biopsy had been completed and treatment hadbeen initiated by the referring rheumatologist at least 6months prior to beginning this retrospective analysis.All procedures were approved by the University of
Table II. Demographic and clinical data for 37 patientsDiagnosis SS (n � 23) CS (n � 14)
Age, yMean 56.6 59.1SD 15.5 9.6
Duration of symptoms, yMean 5.6 6.8SD 5.3 5.2
Race, nWhite 18 13Non-white 5 1
Schirmer test, n� 5 mm in 5 min 11 5� 5 mm in 5 min 12 8
Presence of autoantibodies, nANA 21 11Anti-Ro/ SS-A 14 2Anti-La/ SS-B 9 0
Erythrocyte sedimentation rateMean 33.5 21.0SD 27.3 21.1
White blood cell countMean 5715 6535SD 1379 2710
Salivary flow rate (mL/min)Mean 0.11 0.13SD 0.16 0.08
Disease damage indexMean 2.7 2.3SD 2.2 1.6
Smoking, nCurrently smoking 1 1Quit 9 5Never smoked 13 8
SS, Sjögren’s syndrome; CS, chronic sialadenitis.
Florida Institutional Review Board.
ProceduresIn a blinded fashion, the 5 pathologists (I.B., J.O.,
N.I., C.O., P.D.) independently reviewed the same he-matoxylin and eosin (H&E) sections from the 37 LSGbiopsies. All slides were de-identified and labeled witha random numerical code. The pathologists were in-formed that the slides were LSG biopsies from patientsreferred for sicca with a possible SS diagnosis. Bothgroups were instructed to treat these as if they wereroutine cases in their histopathology service. The his-topathological assessment was conducted according toaccepted criteria listed in Table I.5,6,19 RepresentativeH&E sections from our SS subjects are shown in Fig. 1.
Using a standardized score sheet, the pathologistswere asked to provide a diagnosis and, if appropriate, afocus score from 0 to 12 in 6 ordered categories. Thepathologists were asked to further define their assess-ments by noting descriptive categories that appeared tobe characteristic of the plasma cell distribution through-out the tissue. These categories were: (1) plasma cellsscattered among lymphocytic foci, (2) presence of plas-macytic foci, and (3) no comment regarding plasma cellpresence. A plasmacytic focus was defined as an ag-gregate of 10 to 30 plasma cells. The assessment ofplasma cells was included in this study as their distri-bution in labial salivary gland tissue and recognition inLSG biopsies by histopathologists has been un-clear.5,20-22 Plasma cells have been reported as beingpresent in interstitial tissue, but few are recognizedwithin the lymphocytic foci or appreciated as plasmacell aggregates. While it is known that they produceantibodies, their role in SS pathogenesis is not defined.Similarly, B cells are immunologically active and havebeen shown to produce immunoglobulins locally.23,24
Quantitative immunohistologic examination based onthe percentages of IgA-containing and IgG-containingplasma cells have been shown to help distinguish be-tween patients with SS and patients with rheumatoidarthritis without SS.25 Speight et al.26 reported a sig-nificant increase in IgG-and IgM-containing plasmacells and concluded that quantification and isotyping ofplasma cells might be of diagnostic significance. Thesetechniques were not performed in our study. Due to therole of plasma cells in antibody production, the char-acterization of distribution of plasma cells was includedto assess to what extent plasma cells were observed inroutine histopathologic interpretations of LSG biopsies.
To confirm the H&E assessment and distribution ofplasma cells in these sections, an extra section fromeach specimen was immunostained with CD-138, anantibody that recognizes human plasma cells and epi-thelial cells. To establish the distribution of plasmacells in reference to T and B lymphocytes in SS and CS,
representative CD-3 and CD-20 stains were performed
0.3
dard d
OOOOEVolume 106, Number 3 Stewart et al. 395
as well. All CD-138-, CD-3-, and CD-20-stained sec-tions were reviewed by pathologists I.B. and C.S. inblinded fashion.
Statistical analysisInter-rater reliability was calculated for 3 compo-
nents of the histopathological assessment: (1) diag-nosis, (2) focus score, and (3) plasma cell distribu-tion. One pathologist (D.C.) reported the initialhistopathological diagnoses on all subjects. Diag-
0
10
20
30
40
50
60
70
80
90
100
a b c d eRater
Perc
ent A
gree
men
t with
the
Stan
dard
D
iagn
osis
Fig. 2. Percentage agreement with the standard diagnosis.
Table III. Percent positive diagnoses and means andcategory ratings for each of 5 raters judging 37 sample
Sjögren’s d
Percent SS positive
Oral pathologistsRater a 59.5Rater b 56.8Rater c 64.9
Surgical pathologistsRater d 32.4Rater e 32.4
Table IV. Pairwise percent agreement between ratingdiagnosis for 37 samples
Rater a Rater b
p(o) p(�) p(�)a p(o) p(�) p(�)
Rater b .89 .91 .87Rater c .92 .94 .89 .86 .89 .83Rater d .70 .69 .72 .76 .73 .78Rater e .70 .69 .72 .76 .73 .78Standardb .92 .94 .89 .86 .89 .83
ap(o), p(�), and p(�) represent the percent of agreement overall, fobValues represent percent agreement between each rater and the stan
noses were reviewed the following day by a second
pathologist and no revisions to the initial report werenecessary. For this retrospective study, the 37 caseswere reevaluated by the same pathologist (D.C.) inblinded fashion to serve as the standard for thestatistical analysis. The reassessment occurred be-tween 7 months to 3 years from the initial report.One hundred percent agreement was demonstratedbetween the initial histopathological report and thesubsequent blinded review by pathologist D.C. Forthe diagnosis and focus score assessments, agree-ment among the 5 raters (pathologists) was deter-mined by computing the average percentage agree-ment across all possible rater pairs for both overallagreement and for positive and negative diagnosesconsidered separately. Inter-rater reliability was alsoassessed using the Intraclass Correlation Coefficient(ICC), a statistic that represents the ratio of thevariance between raters to the total variance ofscores.27 This coefficient ranges from 0 to 1.0, withvalues greater than 0.7 generally considered to rep-resent good agreement. For judgments of histologicalfeatures, inter-rater agreement was assessed usingthe generalized kappa coefficient for multiple rat-ers.28 Differences among raters were assessed usingthe Friedman analysis of variance by ranks, andrelationships between histopathological evaluationsand clinical disease parameters were examined using
rd deviations of Sjögren’s diagnoses and focus score
s Focus score
ating SD Mean rating SD
9 0.50 2.7 1.77 0.50 2.6 1.65 0.48 2.4 1.4
2 0.48 1.3 0.52 0.48 1.3 0.5
diagnostic status made by 5 raters plus the standard
Rater c Rater d Rater e
p(�) p(�) p(o) p(�) p(�) p(o) p(�) p(�)
.67 .68
.67 .68 1.0 1.0 1.0
.92 .85 .68 .67 .68 .68 .67 .68
ve ratings, and for negative ratings, respectively.iagnosis.
standasiagnosi
Mean R
0.50.50.6
0.3
s of
p(o)
.68
.68
.89
r positi
nonparametric correlation analysis. The impact of

OOOOE396 Stewart et al. September 2008
the LSG diagnosis on treatment was determined byC.S. following consultation with the referring physi-cian. The impact was either supportive or definitive.A supportive impact indicated that the LSG biopsywas one of several diagnostic parameters consideredin establishing the diagnosis of Sjögren’s syndrome.A definitive impact indicated that the LSG biopsywas the pivotal criterion in establishing the SS diag-nosis. Descriptive statistics were applied to this anal-ysis.
RESULTSSubjects
Specimens evaluated were LSG sections obtainedfrom 37 female patients ranging in age from 21 to 76years, with a mean age of 57 years. Fourteen of theLSG specimens had been diagnosed as chronic sialad-enitis (CS), not consistent with SS, and 23 had been
Fig. 3. A, Labial salivary gland biopsy consistent with SS (H(magnification �5). C, Same tissue, CD-20, demonstrating Bplasma cells in clumps and scattered (magnification �5).
interpreted as consistent with Sjögren’s syndrome. Ad-
ditional demographic and clinical data for these sub-jects are shown in Table II.
Inter-rater agreement for a diagnosisThe histopathological diagnoses included 2 entities:
(1) consistent with SS, and (2) CS. For statistical anal-ysis, SS was scored as 1, and CS was scored as 0. Asshown in Table III, mean ratings for the 2 SP wereapproximately half those of the OP, suggesting that theformer were less likely to interpret a given sample asconsistent with SS. A comparison of the percentage ofcases diagnosed as SS indicated that approximately60% were diagnosed as SS by oral pathologists and32% were diagnosed as SS by the surgical pathologists.Pairwise comparisons for the 5 raters are shown inTable IV. The percentage of overall agreement in di-agnosis was 79.5%, and the single-rater ICC for thesedata was 0.60 (95% CI � 0.44–0.75). Inter-rater agree-
gnification �5). B, Same tissue, CD-3 demonstrating T cells(magnification �5). D, Same tissue, CD-138, demonstrating
&E macells
ment within specialty was considerably better: the ICC

g foci,
OOOOEVolume 106, Number 3 Stewart et al. 397
for the 3 OP considered separately was 0.89, whileagreement between the 2 SP was perfect (ICC � 1.0).Comparisons with the standard diagnosis indicated thatthe overall percent agreement with the standard aver-aged 89% for the OP and 68% for the SP. Differencesin percent agreement for positive and negative diag-noses were small, and showed no consistent patternacross rater pairs (Fig. 2).
The lack of agreement with the standard diagnosishad the potential to adversely impact care for severalsubjects. Unanimous disagreement with the standarddiagnosis (SS in both cases) was noted for 2 subjects. In7 other cases, the disagreement was evenly dividedamong the OP and SP subgroups. If an SP instead of anOP had rendered the sign-out diagnosis, 5 subjectswould have received the diagnosis of CS as opposed toconsistent with SS. In 2 of these 5 cases, the LSGbiopsy was the determining diagnostic factor and treat-
Fig. 4. A, Labial salivary gland biopsy, consistent with SS (H�10). C, Same section as A, CD-20, demonstrating distributidemonstrating plasma cells in foci (white arrow), surroundin
ment would have been impacted.
Inter-rater agreement for focus scoreMeans and standard deviations of focus score ratings
are shown for each of the 5 raters in Table III. Resultsfor focus scores were similar to those for diagnosis.Both the mean and standard deviations of ratings madeby the SP were considerably smaller than those of theOP, suggesting again that the former may have beenmore conservative in their judgments. This impressionwas confirmed by a Friedman analysis of variance byranks, which indicated that there was a significant dif-ference in the distribution of focus scores across raters(P � .001). The percentage of overall agreement, com-puted as the average percent agreement across all pos-sible rater pairs, was 52.1%. The single-rater ICC was0.48 (95% confidence interval � 0.26–0.67) for acriterion of absolute agreement. This was increased to0.62 (95% CI � 0.48–0.75) for a criterion of consis-tency, which assesses relative, rather than absolute
agnification �10). B, Same tissue, SS CD-3 (magnificationB cells (magnification �10). D, Same section as A, CD-138,
and scattered (magnification �10).
&E, mon of
agreement among judges.27 Both coefficients are well

OOOOE398 Stewart et al. September 2008
below the range of agreement (� 0.7) typically consid-ered acceptable for estimates of inter-rater reliability.29
Percent agreement between each rater and the standardfocus score was also examined. The average percentagreement with the standard focus score was 75% forthe 3 oral pathologists, and 38% for the surgical pa-thologists.
Inter-rater agreement for plasma cell distributionFeatures of plasma cell infiltration were considered
in 3 descriptive categories: (1) plasma cells scatteredamong lymphocytic foci, (2) presence of plasmacyticfoci, and (3) no comment regarding plasma cell pres-ence. The overall generalized kappa for these ratingswas 0.11 (95% CI � 0.03–0.19), indicating that agree-ment among the 5 raters was very nearly at chance.Kappa coefficients were also computed separately foreach of the 3 descriptive categories. These valuesranged from 0.07 to 0.22, with ratings for category 1,scattered distribution of plasma cells, showing the high-est level of agreement. Additional chi square tests wereconducted to determine if pathologists’ descriptivejudgments were related to their diagnosis. These resultsrevealed a significant association between the judgedpresence of scattered plasma cells and rendering an SSdiagnosis for raters b, d, and e (P � .05). No significanttrends were evident in the judgments of the remaining2 raters.
The distribution of the plasma cells was verified withCD-138 immunostaining to confirm presence of fociand plasma cell distribution. Panels in Figs. 3, 4, 5, and6 show staining with H&E (section A), CD-3 (sectionB), CD-20 (section C), and CD-138 (section D). Plasmacell foci were seen in 13 of the 37 cases: 10 in SS and3 in CS. Examples are shown in the D sections of Figs.3–6 and in Fig. 7. Plasma cells were seen rimming theperiphery of the lymphocytic foci in 5 cases of SS asdemonstrated in Fig. 4, D, and Fig. 7. They wereobserved inside lymphocytic foci in 3 SS cases asdemonstrated in Fig. 4, D, and Fig. 7 and designated bythe white arrow. Scattered plasma cells were seen inboth SS (20 of 24) cases and CS (5 of 13) tissues aspictured in Figs. 3, D, and 4, D, and in Fig. 7, and inFigs. 5, D, and 6, D, respectively (Fig. 7).
Correlations with clinical measuresRelationships between clinical disease parameters
and judgments of diagnosis and focus score are shownfor each of the 5 pathologists in Tables V and VI,respectively. The pattern of results was similar for bothtypes of ratings. Of the various clinical measures ex-amined, ANA titer was most consistently associatedwith pathologists’ ratings; correlations between ANA
titer and ratings of both diagnosis and focus score werepositive and statistically significant for all 5 judges.However, patterns of association between the ratings oforal and surgical pathologists were markedly differentfor a number of clinical measures. In general, the rat-ings of OP were most highly correlated with serologicalvariables (anti-SSA, anti-SSB, ESR), while those of SPwere most highly correlated with salivary flow rate anddisease damage. There were no significant correlationsinvolving the Schirmer test or white blood cell count.Correlations involving duration of symptoms alsofailed to reach significance. However, the average du-ration of symptoms was longer for patients diagnosedas positive for SS by surgical pathologists than forthose diagnosed as negative (7.3 versus 5.0 years). Asimilar comparison for ratings of oral pathologists in-dicated that there was no difference in symptom dura-tion for patients receiving SS or CS diagnoses.
DISCUSSIONThe LSG biopsy is an integral component of SS
criteria.5-7,9 However, it is recognized that lymphocyticfoci may be seen in non-SS patients, healthy patients,and as part of the aging process.30-33 Conversely, sev-eral studies report that significant focal infiltrates willnot be present unless a connective tissue disease ispresent.2,3,34,35
In an examination of inter-rater reliability for a groupof 5 board-certified pathologists interpreting the sameseries of labial salivary gland biopsies, we found agree-ment to be uniformly poor for judgments of diagnostic
Fig. 5. Labial salivary gland biopsy, consistent with SS,CD-138 showing plasma cells within foci (white arrow), alsosurrounding lymphocytic foci, and scattered (magnification�10).
status, focus scores, and histological characteristics of

issue, C
OOOOEVolume 106, Number 3 Stewart et al. 399
biopsy specimens. This lack of agreement among pa-thologists and between pathologists and the standarddiagnosis is troubling as it has the potential to impactpatient management. The 80% overall agreement be-tween oral and surgical pathologists may reflect the useof different criteria in the assessment and interpretationof focus scores. The pattern of results suggests that thesurgical pathologists may have used the criteria whichrequired more than 1 focus per 4 mm2 to render adiagnosis “consistent with SS,” whereas the oral pa-thologists counted total foci and applied diagnosticcriteria more liberally. In this study, 2 instances ofunanimous disagreement with the standard diagnosiswere demonstrated. In both cases the standard diagno-sis was consistent with SS, and focus scores of 2 werereported. Because the autoantibodies were positive inboth cases, in addition to other AECG criteria, the LSGbiopsy played a supportive role. It is unlikely thattreatment would have been adversely affected if the
Fig. 6. A, Labial salivary gland biopsy, chronic sialadenitis�10). C, Same tissue, CD-20 (magnification �10). D, Same t
diagnosis of CS had been reported. The exact reason for
the marked discrepancy cannot be explained. It was notsurprising that the SP rejected a SS diagnosis due to thelow focus score. The reasons for the OP to reject a SSdiagnosis could be not determined. C.S. reviewed all 37cases blindly, and concurred with the standard diag-noses. In 7 cases, there was a split between the 2 groupsas to the diagnosis. For these 7 cases, the interpretationprovided by the 3 oral pathologists was consistent withSS, in agreement with the standard diagnosis, and thesurgical pathologists’ interpretation was chronic sialad-enitis. In 5 of these cases, the LSG biopsy played asupportive diagnostic role as the autoantibodies werealso positive (Anti-SSA/Ro positive in 7 and Anti-SSBB/La positive in 4). A diagnosis of CS might nothave impacted treatment. Again, the difference betweenthe 2 groups was interpretation of focus scores. In 2 of the7 cases, the oral signs, oral symptoms, and ocular signswere positive, but the autoantibodies were negative. For 1patient, the standard focus score designation was 3 and
, magnification �10). B, Same tissue, CD-3 (magnificationD-138, showing scattered plasma cells (magnification �10).
(H&E
responses were 2, 2, 3 from OP, and 1, 1 from SP. For the

CD-13
OOOOE400 Stewart et al. September 2008
second patient, the standard focus score was 5. The OPdesignations were 5, 3, 4, and the SP designations were 1,1. Both patients demonstrated hyposalivation as the wholeunstimulated flow rate was 1.5 mL/15 min or less. A
Fig. 7. A, Labial salivary gland biopsy, chronic sialadenitis (HC, Same tissue, CD-20 (magnification �5). D, Same tissue,
Table V. Correlations between clinical measures and astandard
Measures Rater a Rater
1. Unstimulated salivary flow rate �.11 �.172. Schirmer test � 5mm in 5 min �.26 �.103. Disease Damage Index �.04 .084. ANA titer .48† .485. Anti-Ro/ SS-A antibodies .34* .326. Anti-La/ SS-B antibodies .30 .367. Erythrocyte sedimentation rate .25 .278. White blood cell count �.20 �.15
*P � .05†P � .01
diagnosis of CS versus SS would have impacted treat-
ment. The LSG biopsy had a definitive impact on care inthese 2 cases. Both of these cases have been treated as SSand the patients are doing well.
The presence of focal lymphocytic/plasmacytic infil-
agnification �5). B, Same tissue, CD-3 (magnification �5).8, showing scattered plasma cells (magnification �5).
ren’s syndrome diagnosis for each of 5 raters plus the
Rater c Rater d Rater e Standard
�.11 �.33* �.33* �.19�.16 .16 .16 .08�.12 .38† .38† .00
.54† .49† .49† .56†
.30 .21 .21 .41*
.41* .14 .14 .43*
.40* .27 .27 .22�.12 �.08 �.08 �.15
&E, m
Sjög
b
†
*
trates has been a key feature in the diagnosis of SS for

OOOOEVolume 106, Number 3 Stewart et al. 401
over 50 years, but an abundance of plasma cells hasbeen considered of uncertain significance. It has beensuggested that an abundance of plasma cells is found inLSG of SS patients and can be helpful in differentiatinginfiltrates of SS from other causes of focal sialadeni-tis.21 In this postmortem study, the authors noted thatinfiltrates from non-SS patients demonstrated very fewplasma cells. In our study, plasma cells were foundrandomly scattered throughout the tissues, formingplasma cell aggregates, rimming the periphery of lym-phocytic foci, and sometimes within the lymphocyticfoci in SS tissues. Hence the presence of plasma cells inany of these configurations should not negate an SSdiagnosis if other diagnostic features are present. Theresults of the CD-138 staining in our study indicatedthat plasma cells are present in both SS and CS labialsalivary gland tissues, but more abundant in SS tissues.
Another important aspect of our study was the correla-tion of diagnosis with clinical measures. Previous studiesexamining the relationships among clinical, laboratory,and histopathological findings have shown varying re-sults. While a number of investigators have reported sig-nificant correlations between biopsy findings and serolog-ical or salivary measures,14-16 others have suggested morecaution in interpretation of these measures.12,36,37 In thepresent study, we found that the pattern of correlationsbetween clinical measures and biopsy results differedacross pathologists by subgroups. The surgical patholo-gists’ interpretation of an SS diagnosis correlated mosthighly with measures of salivary flow rate and diseasedamage, and judgments of the oral pathologists correlatedmost highly with serological features. These findings raisethe possibility that much of the reported inconsistency incorrelations between clinical measures and biopsy resultsmay be attributable to variability in the interpretation ofbiopsies. Given that surgical pathologists rated fewercases as consistent with SS, and that those patients diag-nosed with SS by surgical pathologists had experiencedsymptoms longer, it is likely that these patterns of asso-
Table VI. Correlations between clinical measures andMeasures Rater a Rater
1. Unstimulated salivary flow rate �.24 �.202. Schirmer test � 5mm in 5 min �.03 �.113. Disease Damage Index .12 .064. ANA titer .61† .645. Anti-Ro/ SS-A antibodies .41† .446. Anti-La/ SS-B antibodies .34* .447. Erythrocyte sedimentation rate .33 .318. White blood cell count �.18 �.12
*P � .05†P � .01
ciation also reflect differences in the diagnostic criteria
used by the 2 groups. Surgical pathologists, using thehistorical more stringent criteria (focus score �1) mayhave judged only the more advanced cases as positive forSS. These patients might be more likely than those earlierin the disease process to demonstrate symptoms such asreduced salivary flow rate and organ damage. In contrast,the ratings of oral pathologists would be more likely todemonstrate an association with clinical measures, such asserological variables, that become manifest earlier in thecourse of the disease. If so, an emphasis on early diagnosisand treatment of SS patients would favor the use of lessstringent focus score criteria such as that published by theAECG. Application of the AECG criteria allows classifi-cation of SS for patients with primary SS, but withoutsubjective complaints (excluding those that are negativefor both LSG histopathology and autoantibodies) with asensitivity of 89.5% and specificity of 95.2%.7
Based on the results of this study, how do the authorsanswer the question, “Is the LSG biopsy for Sjögren’ssyndrome still the ‘gold standard’?” The authors believethat among well calibrated histopathologists who carefullyapply the criteria, the answer is a “qualified yes.” TheLSG biopsy is an integral, and often a pivotal diagnosticcomponent of SS. However, as the literature indicates,9
supported by our results, there is room for concern. Otherinvestigators have suggested reviewing more glands andmore levels of sections to improve accuracy.8,10
CONCLUSIONLack of diagnostic agreement between pathologists
reflects the need to determine ways to improve theconsistency of histological interpretations. Our datasuggest that a standardized formula for determinationof a focus score was not consistently applied. Greaterconsistency in definition and application of SS criteriaare essential for physicians to maintain confidence inthe reliability of the procedure and for correct diag-noses and treatment. Eventually, the development of
scores for each of 5 raters plus the standardRater c Rater d Rater e Standard
�.28 �.40* �.40* �.22�.06 .16 .16 .01
.06 .44† .44† .11
.56† .55† .55† .70†
.38* .21 .21 .48†
.45† .14 .14 .38*
.39* .33 .33 .36*�.20 �.09 �.09 �.20
focusb
†††
salivary or serum biomarkers for greater prognostic and

OOOOE402 Stewart et al. September 2008
diagnostic accuracy may allow clinicians to place lessemphasis on this procedure.
REFERENCES1. Delaleu N, Jonsson R, Koller MM. Sjogren’s syndrome. Eur
J Oral Sci 2005;113:101-13.2. Chisholm DM, Mason DK. Labial salivary gland biopsy in
Sjogren’s disease. J Clin Pathol 1968;21:656-60.3. Greenspan JS, Daniels TE, Talal N, Sylvester RA. The histopa-
thology of Sjögren’s syndrome in labial salivary gland biopsies.Oral Surg Oral Med Oral Pathol 1974;37:217-29.
4. Daniels TE. Labial salivary gland biopsy in Sjögren’s syndrome.Assessment as a diagnostic criterion in 362 suspected cases.Arthritis Rheum 1984;27:147-56.
5. Daniels TE. Salivary histopathology in diagnosis of Sjögren’ssyndrome. Scand J Rheumatolol 1986;61(Suppl):36-43.
6. Fox RI, Robinson CA, Curd JG, Kozin F, Howell FV. Sjögren’ssyndrome. Proposed criteria for classification. Arthritis Rheum1986;29(5):577-85.
7. Vitali C, Bombardieri S, Jonsson R, Moutsopoulos HM, Alex-ander EL, Carsons SE, et al. Classification criteria for Sjögren’ssyndrome: a revised version of the European criteria proposed bythe American-European Consensus Group. Ann Rheum Dis2002;61:554-8.
8. Al-Hashimi I, Wright JM, Cooley CA, Nunn ME. Reproducibil-ity of biopsy in Sjogren’s syndrome. J Oral Pathol Med2001;30:408-12.
9. Vivino FB, Gala I, Hermann GA. Change in final diagnosis insecond evaluation of labial minor salivary gland biopsies.J Rheumatol 2002;29:938-44.
10. Morbini P, Manzo A, Caporali R, Epis O, Villa C, Tinelli C, etal. Multilevel examination of minor salivary gland biopsy forSjogren’s syndrome significantly improves diagnostic perfor-mance of AEGC classification criteria. Arthritis Res Ther2005;7(2):R343-8.
11. Manthorpe R. Sjogren’s syndrome criteria: American-Europeanand Japanese group’s criteria compared and contrasted. AnnRheum Dis 2002;61:482-4.
12. Langerman AJ, Blair EA, Sweiss NJ, Taxy JB. Utility of lipbiopsy in the diagnosis and treatment of Sjogren’s syndrome.Laryngoscope 2007;117(6):1004-8.
13. Katz J, Yamase H, Parke A. A case of Sjögren’s syndrome withrepeatedly negative findings on lip biopsy. Arthritis Rheum1991;34(10):1325-8.
14. Wise CM, Woodruff RD. Minor salivary gland biopsies in pa-tients investigated for primary Sjogren’s syndrome. A review of187 patients. J Rheumatol 1993;20:1515-8.
15. Gerli R, Muscat C, Giansanti M, Danieli MG, Sciuto M, Gabri-elli A, et al. Quantitative assessment of salivary gland inflam-matory infiltration in primary Sjogren’s syndrome: its relation-ship to different demographic, clinical and serological features ofthe disorder. Br J Rheumatol 1997;36:969-75.
16. Brennan MT, Sankar V, Leakan RA, Kleiner D, Atkinson JC,Wilkinson WE, et al. Risk factors for positive minor salivarygland biopsy findings in Sjögren’s syndrome and dry mouthpatients. Arthritis Rheum 2002;47(2):189-95.
17. Navazesh M, Christensen CM. A comparison of whole mouthresting and stimulated salivary measurement procedures. J DentRes 1982;61:1158-62.
18. Vitali C, Palombi G, and the study group of the Italian Society ofRheumatology. Sjögren’s Syndrome Disease Damage Index andDisease Activity Index. Arthritis Rheum 2007;56:2223-31.
19. Blitzer A. Inflammatory and obstructive disorders of salivary
glands. J Dent Res 1987;66(Suppl):675-9.20. Matthews JB, Deacon EM, Wilson C, Potts AJC, Hamburger J.Plasma cell populations in labial salivary glands from patientswith and without Sjogren’s syndrome. Histopathology 1993,23:399-407.
21. Yarom N, Dayan D, Buchner A, Vered M. Immunoprofile oflymphocytic infiltration in minor salivary glands of healthy in-dividuals. Oral Dis 2007;13:274-8.
22. Daniels TE, Aufdemorte TB, Greenspan JS. Histopathology ofSjögren’s Syndrome. In: Talal N, Moutsopoulos HM, Kassan SS,editors. Sjögren’s syndrome: clinical and immunological aspects.Berlin: Springer-Verlag; 1987. p. 41-52.
23. Anderson LG, Cummings NA, Asofsky R, Hylton MB, TarpleyTM Jr, Tomasi TB Jr, et al. Salivary gland immunoglobulin andrheumatoid factor synthesis in Sjögren’s syndrome. Am J Med1972;53:456-63.
24. Fox PC, Speight PM. Current concepts of autoimmune exocri-nopathy: immunologic mechanisms in the salivary pathology ofSjogren’s syndrome. Crit Rev Oral Biol Med 1996;7(2):144-58.
25. Bodeutsch C, de Wilde PCM, Kater L, van Houwelinger JC, vanden Hoogen F, Kruize AA, et al. Quantitative immunohistologiccriteria are superior to the lymphocytic focus score criterion forthe diagnosis of Sjogren’s syndrome. Arthritis Rheum 1992;35(9):1075-87.
26. Speight PM, Cruchley A, Williams DM. Quantification of plasmacells in labial salivary glands: increased expression of IgM inSjögren’s syndrome. J Oral Pathol Med 1990;19(3):126-30.
27. McGraw K, Wong S. Forming inferences about some intraclasscorrelation coefficients. Psychological Methods 1996;1:30-46.
28. Fleiss, JL. Statistical methods for rates and proportions. 2nd ed.New York: John Wiley; 1981. p. 36-46.
29. Landis R, Koch G. The measurement of observer agreement forcategorical data. Biometrics 1977;33:159-74.
30. Lindahl G, Hedfors E. Focal lymphocytic infiltrates of salivarygland are not confined to Sjögren’s syndrome. Scand J Rheuma-tol Suppl 1986;61:52-5.
31. Takeda Y, Komori A. Focal lymphocytic infiltration in the hu-man labial salivary glands: a postmortem study. J Oral Pathol1986;15:83-6.
32. Radfar L, Kleiner DE, Fox PC, Pillemer SR. Prevalence andclinical significance of lymphocytic foci in minor salivary glandsof healthy volunteers. Arthritis Rheum 2002;47:520-4.
33. DeWilde PCM, Baak JPA, van Houwelingen JC, Kater L, SlootwegPF. Morphometric study of histological changes in sublabial sali-vary glands due to aging process. J Clin Pathol 1986;39:406-17.
34. Cifarelli PS, Bennett MJ, Zaino EC. Sjögren’s syndrome: a casereport with an additional diagnostic aid. Arch Intern Med1966;117:429-31.
35. Chisholm DM, Waterhouse JP, Mason DK. Lymphocytic sialad-enitis in the major and minor glands: a correlation in postmortemsubjects. J Clin Pathol 1970;23:690-4.
36. Segerberg-Kontinnen M. A postmortem study of focal adenitis insalivary and lacrimal glands. J Autoimmun 1989;2(4):553-8.
37. Manthorpe R. How should we interpret the lower lip biopsyfinding in patients investigated for Sjögren’s syndrome? ArthritisRheum 2002;47(2):114-5.
Reprint requests:
Carol M. Stewart, MS, DDS, MS, Co-DirectorUniversity of Florida Center for Autoimmune DisordersPO Box 100414 JHMHCUniversity of Florida College of DentistryGainesville, FL 32610
[email protected]