Embed Size (px)
Citation preview

12/21/2013
1
Lab and Imaging Interpretation Primary Eye Care
James L. Fanelli, OD, FAAO Visiting Professor of Clinical Medicine
Pa College of Optometry
AOA Meeting, 2014
Goals of the Presentation
• One Goal, and One Goal Only:
• To give you one nugget of information that you can take home and actually use in your practice, maybe two.
– Use that information to make you a better clinician
What the Goals are NOT:
• To have you become a hematologist
• To have you become a radiologist
This is a CEE/TQ Course
• It comes with an examination! – Exciting, yes?
• Pay attention to information presented in either red or gray font, as you may see that information again
• You can fill out your course evaluation at this point
Interpretation of Diagnostic Tests: A
Synopsis of Laboratory Medicine
Jacques Wallach MD
Little, Brown and Co
Clinical Implications of Laboratory
Tests
Tilkian, Conover & Tilkian
Mosby Co

12/21/2013
2
Interpreting Lab and Imaging Studies
• This is a Lab Study:
• This is an Imaging Study:
Why order Lab & Image Testing? • Objective measurment
• Helpful in DDx
• Dx confirmation
• Screening for unsupected illness
• Monitor compliance to therapy
• Monitor response to condition/treatment
• Medico-legal justification of Tx
Why Order Testing???
Clinical Confirmation
confirmatory diagnosis
Adjunct to Thorough Examination
covering the bases
Co-Management vs. Direct Involvement
refer vs. orchestrate
Can I Order Lab/Image Test? • Yes, most states allow ODs to order;
–Diagnostic Laboratory test for eye related conditions
–Radiological Imaging test for eye related conditions
What Are My Options?
• Hospital
• In-office
• Reference Laboratory
• Imaging Center
– Hospital based
– Private imaging center

12/21/2013
3
Typical Laboratory Tests • Complete Blood Count (CBC)
• Blood Chemistry/Profiles
• Urine Analysis
• Serology
Profile Examples
• Autoimmune Profile
– Anti-ANA antibodies, ANA, Complement C3
• Lipid Profile (VAP Cholesterol)
– Cholesterol, HDL, LDL,Triglycerides
• Thyroid Function Profile
– Free Thyroxin index (FTI), T4, T3 Uptake, Thyroid Stimulating Hormone (TSH)
Imaging Tests Available
• Plain Film X-Ray
• Computed Tomography (CT)
• CT Angiography (CTA)
• Magnetic Resonance Imaging (MRI)
• Magnetic Resonance Angiography (MRA)
• Magnetic resonance Venography (MRV)
• Carotid Doppler Ultrasonography
• Temporal Artery Ultrasonography
Lecture Format
Anatomy/Physiology Pathophysiology PEARLS
Lab/Image Results
Case Example SOAP
Lab/Image Test
Complete Blood Count (CBC) • WBC w/ Differential
• RBC Count
• Hematocrit
• Hemoglobin
• RBC Indices (MCV, MCH, MCHC)
• Peripheral Blood Smear
• Red Cell Distribution
• Reticulocyte Count
• Platelet Count

12/21/2013
4
CBC - Retinal Hemorrhage (Subjective)
• 41 YOWF secretary c/o Blur @ Near resulting in daily fatigue @ work
• First Eye Exam
• MHx: Unremarkable, 10 yrs since last physical
• Meds: None
• NKDA
CBC - Retinal Hemorrhage (Objective)
• BVA: 20/20 OD, OS w/ +1.00 ADD
• Neuro: PERRLA (-) APD; EOM-I
• SLE: Unremarkable
• DFE: Isolated Intraretinal Hemorrhage/CWS
• BP: 118/70
CBC - Retinal Hemorrhage (Objective)
CBC - Retinal Hemorrhage (Assessment)
1. Presbyopia
2. Retinal Hemorrhage with microinfarction
Additional History
• Fatigue also on weekends and has noted SOB and palpitations upon exertion
CBC - Retinal Hemorrhage (Plan)
1. Prescribe PAL w/ Adjustment to Work Station
2. -Physical Exam
-Laboratory Investigation ( Include CBC, SMA, ESR, ANA)
-RTC 1 month F/U DFE
CBC - Retinal Hemorrhage Lab Results/Final Assessment
Elevated
MCV
Low
RBCs
Hemoglobin
Hematocrit
Additional Labs
Low Fasting B12
(dietary lack or absorption?)
Normal Serum Folate (B8)
Schilling Test Stage I: known marked amount of B 12
ingested/excreted
Stage II: admin of ‘intrinsic factor’ followed by oral B12 ingestion and clearance
Final Dx: Pernicious Anemia

12/21/2013
5
CBC - Retinal Hemorrhage Discussion
Anatomy RBCs (erythrocytes)- # Red Cells in mL of Venous
Blood
Hemoglobin- O2 Carrying Pigment of RBCs
Hematocrit- Column of RBCs in 100 mL of Blood
MCV- Avg. Volume of individual cells in cubic Microns. Hematocrit X 10 divided by RBCs
Retinal NFL or capillary bed
CBC - Retinal Hemorrhage Discussion
Physiology • RBCs- Carries Hemoglobin
• Hemoglobin- Transports O2 to Tissue and CO2 to Lungs
• Hematocrit- measure of volume occupied by RBC’s
• MCV- individual cell volume elevated to increase O2 transport
CBC - Retinal Hemorrhage Discussion
• Physiology
–individual cellular effects occur at level of capillary bed
–Vitamin B-12
• co enzyme utilized in amino acid metabolism
• stimulates erythropoiesis
CBC - Retinal Hemorrhage Discussion
Pathophysiology • Pernicious anemia - precipitated by a gastric
condition that interferes with B12 absorption which results in ineffective erythropoiesis.
• Retinal hemorrhage/infarct from tissue hypoxia
• Decreased oxygen transport results in fatigue, dyspnea, angina, and syncope.
CBC - Retinal Hemorrhage Discussion
PEARLS
• 70-80% of Hematologic Disorders Dx by CBC
• B12 Absorption Defect not Dietary Lack
• Rare Before Age 35
• More Common in Scandinavian, English, and Irish. Rare in Orientals
• Treated w/ B12 (cyanocobalamin) Injections
Atherosclerosis Risk in Communities Study ARIC
• Initiated by the National Heart Blood and Lung Institute – Investigate factors that are involved with the
development of atherosclerosis and the incidence of CHD, stroke and other cardiovascular diseases
– Measure cardiovascular disease rates in communities over time
– 15,792 initial participants
12/21/2013
6
ARIC and Retinopathy
• What is incidence and prevalence of retinopathy?
– 3.8% chance of developing retinopathy
– 7.7% prevalence rate
– Retinopathy related to: • Fasting serum glucose
• Cholesterol
• Mean arterial blood pressure
• Plasma fibrinogen
• In non diabetics, incidence and prevalence are halved, with BP being the leading risk factor
Wong et al. Three-year incidence and cumulative prevalence of retinopathy: the atherosclerosis risk in communities study. Am J Ophthalmol. 2007 Jun;143(6):970-6. Epub 2007 Apr 2.
CBC - Retinal Hemorrhage Discussion
• ARIC (Atherosclerosis Risk in Communities) Study – Wong et al
– 1684 participants
– One arm of study compared MR findings with retinopathy in the context of STROKE
– retinopathy included: • microaneurysms, retinal hemorrhages, soft exudates, hard
exudates, macular edema and optic disc swelling
ARIC Prelim Results
• The overall incidence of stroke was found to be related to:
– 1: MR findings of white matter lesions
– 2: presence of “retinopathy”
Atherosclerosis Risk in Communities
• Findings:
– The 5-year cumulative incidence of clinical stroke:
– (-) white matter lesions 1.4%
– (+) white matter lesions 6.8%
– (-) retinopathy 1.4%
– (+) retinopathy 8.0%
Atherosclerosis Risk in Communities
• Higher Incidence of Clinical Stroke was related to ‘retinopathy’ and + MR findings independently.
• Was there a link between the two distinct clinical signs?
Atherosclerosis Risk in Communities
• Findings:
– No retinopathy:
• 9.9% chance of having MR lesions
• 1 out of 10
– With retinopathy:
• 22.9% chance of having MR lesions
• 1 out of 4 !!!
What about both together in a patient???
12/21/2013
7
Atherosclerosis Risk in Communities
• Findings: – 5year cumulative incidence of stroke:
• (-) white matter lesions and (-) retinopathy: 1.4%
• (+) white matter lesions and (+) retinopathy: 20.0%
– The study suggests that healthy people with white
matter lesions detected by MRI may benefit from a retinal examination to assess their risk of stroke.
Blood Chemistry (SMA or Profiles)
• Quick survey of body systems with an overall appreciation for the patients general condition as well as detection of abnormalities in specific systems
• Glucose, Lipid/Cholesterol, Electrolytes, Renal Function, Liver Function, Mineral/Bone Metabolism, Protein, Cardiac Function, Thyroid Profile, etc.
Blood Chemistry- Retinal Emboli (Subjective)
• 57 YOWM c/o decreased VA X 3 wks.
• POHx: Unremarkable; LEE: 2+ yrs.
• PMHx: S/P MI w/ CABG X 3, NIDDM X 16 mos.
• MEDS: Plavix, Lipitor, Glucophage
• NKDA
Blood Chemistry-Retinal Emboli (Objective)
• BVA: OD 20/30; OS 20/50 w/ -1.00 & -1.50 Refractive Shift
• Ta: OD 19 mmHg; OS 18 mmHg
• SLE: Clear OD, OS
• DFE: 1/3 AV with Nicking, Stage II AS, Multiple Arterial Plaques; Multiple Mid-peripheral Intraretinal Hemes.
• BP 140/85 LAS
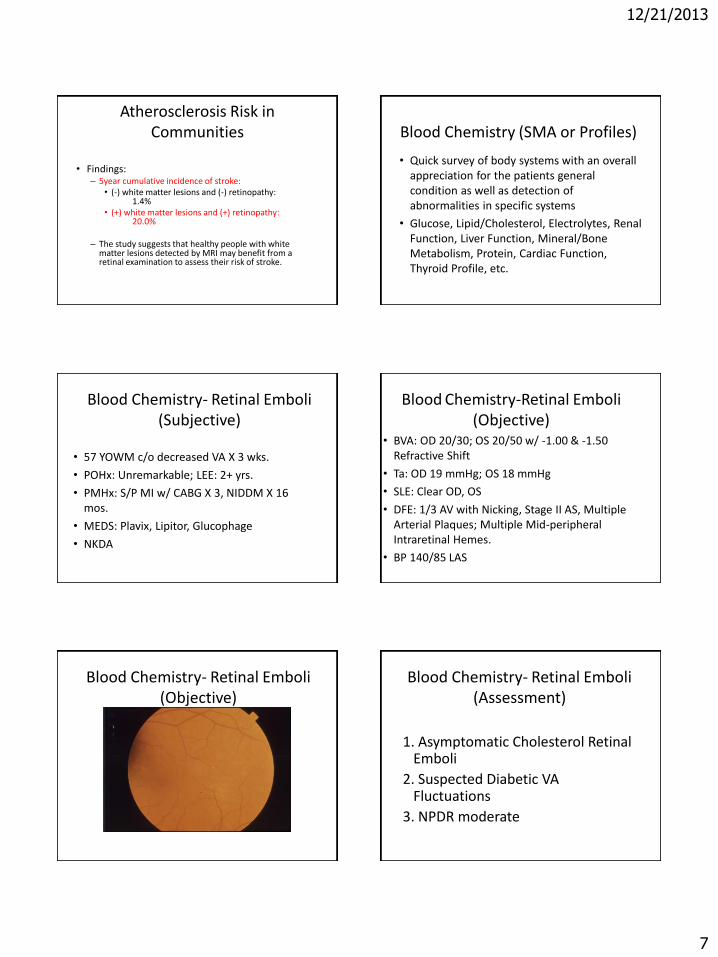
Blood Chemistry- Retinal Emboli (Objective)
Blood Chemistry- Retinal Emboli (Assessment)
1. Asymptomatic Cholesterol Retinal Emboli
2. Suspected Diabetic VA Fluctuations
3. NPDR moderate

12/21/2013
8
Blood Chemistry- Retinal Emboli (Plan)
CBC w/ Diff, ESR, Diabetic Profile
VAP Cholesterol Profile
– Lipid profile (total, LDL, HDL, VLDL,triglycerides, cardio risks)
– Lipoprotein A Cholesterol
– Homocysteine levels
– CRP
VAP Cholesterol Test Vertical Auto Profile
http://www.atherotech.com
VAP Cholesterol
• Global Cardiometabolic Risk stratification
• Total, HDL, LDL, triglycerides
• Also measures cholesterol subclasses that play a major role in the development of ASCVD
• Benefits: – More accurate risk profile
– Provides basis for patient specific treatment
Blood Chemistry- Retinal Emboli (Plan)
• Carotid Doppler
• IM Communication
• Educate & Follow q 1 month
Blood Chemistry- Retinal Emboli Labs
High
• Fasting Glucose (133 mg/dl), Hgb A1C (10.2), Cholesterol (296 mg/dl), LDL, homocysteine
Low
• HDL
Risk 2.5/1
Doppler 80% Blockage @ Bifurcation
Blood Chemistry- Retinal Emboli Final Diagnosis/Plan
1. Hypercholesterolemia
2. Type II DM w/ NPDR
3. Carotid Occlusive Dz
4. Hyperhomocysteinemia
1. & 2. Medicate
3. Consider Endarterectomy
4. ????

12/21/2013
9
Blood Chemistry- Retinal Emboli Discussion
Anatomy/Physiology
• Carotid to Retinal Arteriole Vasculature & Blood Flow
• Serum Cholesterol, HDL, LDL,
Hgb A1C & Glucose
Blood Chemistry- Retinal Emboli Discussion
Blood Chemistry- Retinal Emboli Discussion
Pathophysiology • Hypercholesterolemia/Plaque Formation
• Arteriosclerosis
• Carotid Stenosis
• Hyperglycemia
Blood Chemistry- Retinal Emboli Discussion
Blood Chemistry- Retinal Emboli Discussion
PEARLS
• Moniter Hgb A1c
• Eye w/ MHx Significance
• Profile vs. Individual Test
• Systemic Risk of Retinal Emboli
• Hyperglycemia also Seen w/ Certain Medications(ie. Cortisone) and Trauma
Lipoproteins
• 5 categories
– HDL (high density lipoproteins)
– LDL (low density lipoproteins)
– Chylomicrons
– VLDL (very low density lipoproteins)
– IDL (intermediate density lipoproteins)
12/21/2013
10
Associated Markers of ASCVD
• Low density lipoproteins
• Lipoprotein (a)
• Apolipoprotein A1
• Apolipoprotein B
• Ratio of A1 / B
Low Density Lipoprotein
• One type of lipoprotein that transports cholesterol and triglycerides from liver to peripheral tissues
• Serum is water based; LDL’s allow fats and cholesterol to circulate
• LDL particles vary in size and density
– Subtype A • Larger, less dense
– Subtype B • Smaller, more dense
LDL Subtypes A and B
• Subtype B is more likely to penetrate vascular endothelium
– More highly associated with risk of CAD
• normal vascular endothelial gaps are about 26nm
Measurements of LDL
• Measurement of LDL is widely available and relatively inexpensive
• Not very well correlated with development of atherosclerosis
• Measurement of sub types of LDL are more correlated with cardiovascular disease
LDL and Cardiovascular Risk
• LDL may be low, but in presence of elevated LDL particles, AS increases
• LDL may be high, and in cases where LDL particles are low, so too is incidence of AS
• Typical lipid panels do NOT directly measure LDL; Friedenwald Formula is used to calculate LDL
Pathophysiology
• PDAYS Study
– Pathobiological Determinants of Atherosclerosis in Youth Study
– Lesions in the intimal lining of ALL the aortas and 50% of the Right Coronary Arteries are present by age 9

12/21/2013
11
A Rhetorical Question Homocysteine
• Homocysteine is: – 1: an amino acid that has protective properties in
patients at risk of cardiovascular disease
– 2: an amino acid that is a significant risk factor for MI, ischemic stroke, and thromboembolism
– 3: an amino acid whose levels are genetically determined and is not altered by dietary intake
– 4: an enzyme responsible for increased clotting times
Homocysteine
• Homocysteine is: – 1: an amino acid that has protective properties in
patients at risk of cardiovascular disease
– 2: an amino acid that is a significant risk factor for MI, ischemic stroke, and thromboembolism
– 3: an amino acid whose levels are genetically determined and is not altered by dietary intake
– 4: an enzyme responsible for increased clotting times
Homocysteine
• Elevated plasma levels of homocysteine is an established risk factor for ASCVD, Cerebrovascular disease, perpheral vascular occlusive disease
• Hcy levels are lower in premenopausal women than in men and post menopausal women
– May be related to the increased incidence of ASCVD in postmenopausal women
Homocysteine
• Elevated plasma levels of Hcy can be reduced by therapy with folate and vitamins B6 & B12
• Elevated Hcy levels are reduced by HRT, estrogens and tamoxifen
More to Think About
• Since elevated Hcy levels are associated with a significant increase in ASCVD and stroke:
– 1: lowering Hcy by folate and vitamins has a significant effect in lowering the risk of stroke
– 2: lowering of Hcy by folate and vitamins has a moderate effect in lowering the risk of stroke
– 3: lowering of Hcy by folate and vitamins has no clinical effect in lowering the risk of stroke
– 4: lowering Hcy by folate and vitamins further increases the risk of stroke

12/21/2013
12
More to Think About
• Since elevated Hcy levels are associated with a significant increase in ASCVD and stroke:
– 1: lowering Hcy by folate and vitamins has a significant effect in lowering the risk of stroke
– 2: lowering of Hcy by folate and vitamins has a moderate effect in lowering the risk of stroke
– 3: lowering of Hcy by folate and vitamins has no clinical effect in lowering the risk of stroke
– 4: lowering Hcy by folate and vitamins further increases the risk of stroke
VISP Study
• Vitamin Intervention for Stroke Prevention
• Double blind, randomized, controlled study
• 4000 participants
• Does administration of high doses of folate, B6 and B12 reduce the risk of stroke?
Vitamin in Stroke Prevention
• High doses or low doses of folate, B6 and B12 did not differ in effect on stroke outcomes
• Neither high nor low doses of folate, B6 and B12 had a clinically significant effect on vascular outcomes
2004, JAMA
Homocysteine and the Eye
• Include Hcy levels in work up of patients with:
– ASCVD
– emboli
– TIA, TVB
– retinal vascular disease,
– neuro visual field defects,
– vascular diplopia
Homocysteine and the Eye
• If clinical findings are present and Hcy levels elevated, IM prophylaxis with folate, B6 and B12 and anti-platelet therapy is warranted
Even More to Think About
• If lowering Hcy levels by supplementation does not decrease risk of stroke, why recommend it in patients at risk?
– 1: current research shows Hcy is intimately linked to vascular endothelial disease
– 2: high levels of folate increase libido in the elderly
– 3: high levels of folate are associated with a decreased incidence of Alzheimer’s Disease
– 4: two of the above

12/21/2013
13
Even More to Think About
• If lowering Hcy levels by supplementation does not decrease risk of stroke, why recommend it in patients at risk?
– 1: current research shows Hcy is intimately linked to vascular endothelial disease
– 2: high levels of folate increase libido in the elderly
– 3: high levels of folate are associated with a decreased incidence of Alzheimer’s Disease
– 4: two of the above
Homocysteine
• Elevated levels are associated with:
– Alzheimer’s Disease
– Neovascular AMD
• Not dry AMD
– Increased risk of cervical cancer
Serology for Inflammatory Disease
• Erythrocyte Sedimentation Rate (ESR, Sed Rate)
• C-Reactive Protein (CRP)
• Rheumatoid Factor (RF)
• Anti-Nuclear Antibody Titer (ANA)
• Human Leukocyte Antigen Test (HLA Typing)
• Immunoglobulins (IgM, IgG, IgA)
Inflammatory Disease - AION (Subjective)
• 61 YOWF c/o Sudden, Painless OD Decreased VA X 5 d, “Dimming of Vision”
• POHx: ? OS Problem 10+ yrs. Ago
• PMx: HTN, RA, Anxiety
• FMHx: Non-contributory
• Meds:Diazide, Macrobid, Naprosyn, Lorazepam
• NKDA
Inflammatory Disease - AION (Objective)
• BVA: 20/100 OD, 20/70 OS
• Neuro: PERRLA (-)APD; CF Constricted to 20 Degrees, EOM FROM, CV 4/10 OD, 8/10 OS w/ 25% Red Desatuation OD
• SLE: Unremarkable except 2+ NS OD, OS
• DFE: Moderate Sectoral Disc Edema w/ NFL Heme OD, Pale Atrophy OS
• Formal Visual Fields
Inflammatory Disease - AION (Objective)

12/21/2013
14
Inflammatory Disease - AION (Assessment)
1. AION OD
2. Optic Atrophy OS from Previous AION
(Foster-Kennedy Syndrome doubt)
Inflammatory Disease - AION (Plan)
1. STAT Laboratory Investigation
(CBC, SMA, ESR, CRP, RPR,RF, ANA, FTA-ABS)
2. STAT Imaging Study
(MRI of Head and Orbits R/O Mass Lesion)
Inflammatory Disease - AION Lab Results (Plan)
Lab Results
• Elevated ESR- 63 mm/hr
• Elevated CRP
Image Results
• Normal MRI
Plan Continued
• Schedule TA Biopsy
• Rx Prednisone 80mg po qd in Divided Doses (Co-Manage w/ IM/Rheumatologist)
• Follow ESR, VF, VA, CRP & ONH
Inflammatory Disease - AION Discussion
Anatomy/Physiology
• Optic Nerve Head
• Lamina Cribrosa
• Vasa Vasorum of Optic Nerve
Inflammatory Disease - AION Discussion
Inflammatory Disease - AION Discussion
12/21/2013
15
Ischemic Optic Neuropathy
Arteritic vs Non Arteritic
temporal artery biopsy
Arteritic
elevated sed rate (Westergren)
elevated CRP
associated symptoms of malaise, claudication, headache
Non-Arteritic
look for top 5 CV/IHD risk factors
C Reactive Protein
• C Reactive Protein levels:
– 1: are a marker of vascular inflammation
– 2: if elevated, are a risk factor for cardiovascular disease
– 3: if elevated, are more sensitive in determining AAION than ESR
– 4: all of the above
C Reactive Protein
• C reactive Protein levels:
– 1: are a marker of vascular inflammation
– 2: if elevated, are a risk factor for cardiovascular disease
– 3: if elevated, are more sensitive in determining AAION than ESR
– 4: all of the above
Ischemic Optic Neuropathy
Hayreh et al
AJO March 1997
ascertained reliability, sensitivity and specificity of signs, symptoms and diagnostic tests for early diagnosis of GCA
Findings most strongly suggestive of GCA:
1: jaw claudication
2: C-reactive protein > 2.45mg/dl
3: neck pain
4: ESR > 47mm/hr
Ischemic Optic Neuropathy
Hayreh et al, AJO March 1997
Sensitivity of CRP: 100%
Sensitivity of ESR: 90%
ESR + CRP gave best specificity (97%)
On to Part 2!




























