Embed Size (px)
Citation preview

Modena 6 Ottobre 2017
Marcello MaggioUOC Clinica Geriatrica
Dipartimento Medico Geriatrico RiabilitativoDipartimento di Medicina e Chirurgia
AOU Parma-Università di Parma
La revisione della terapia farmacologica

Outline
• Demenza e Delirium: la necessità di una visione integrata
• La necessità di una rivisitazione farmacologica guidata
• L’appropriatezza prescrittiva ed il deprescribing: necessità di Algoritmi guida con focus sugli antipsicotici e PPI


Date of download: 11/12/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
A unifying model of aging, frailty, and the geriatric syndromes.
Legend :
From: Chapter 72. Clinical Problems of AgingHarrison's Principles of Internal Medicine, 18e, 2 012From: Chapter 72. Clinical Problems of AgingHarrison's Principles of Internal Medicine, 18e, 2 012




Delirium Epidemiology: Risk Factors
Predisposing Precipitating
Age (esp > 80y) Infection
Dementia → 5x ↑ risk Metabolic ∆ (esp dehydr)
Severe med dz > 3 new meds/24 hrs
Major surgery Immobilization
Polypharm (> 4 meds) Use of bladder catheter
Sensory impairment Car/CNS events

Delirium Mnemonic
D rugs
E lectrolytes, O2
L ack of drugs (withdrawal)
I nfection
R educed sensory input
I ntracranial, injury/pain
U rinary retention
M yocardial




Inouye. N Engl J Med 2006; 354:1157-1165
All’ Ammissione in Ospedale

Fagherazzi et al. G Gerontol 2015;63:205-220

Fagherazzi et al. G Gerontol 2015;63:205-220

MedicationsAlcohol withdrawal
Medications, medical ilnesses, surgery
Hepatic failureBenzodiazepines

Lauretani F, Ceda GP, Maggio M et al. Aging Clin Ex Res 2010; 354:1157-1165


Medications and Risk of Delirium
Drug Class Relative RiskAnticholinergic drugs 4.5-11.7
Sedative-hypnotics 3.0-11.7
Any antipsychotic 3.9
Narcotics 2.6
Number Drugs2-3 rxes 2.7
4-5 rxes 9.3
6+ rxes 13.7
Am J Med 1999;106:565
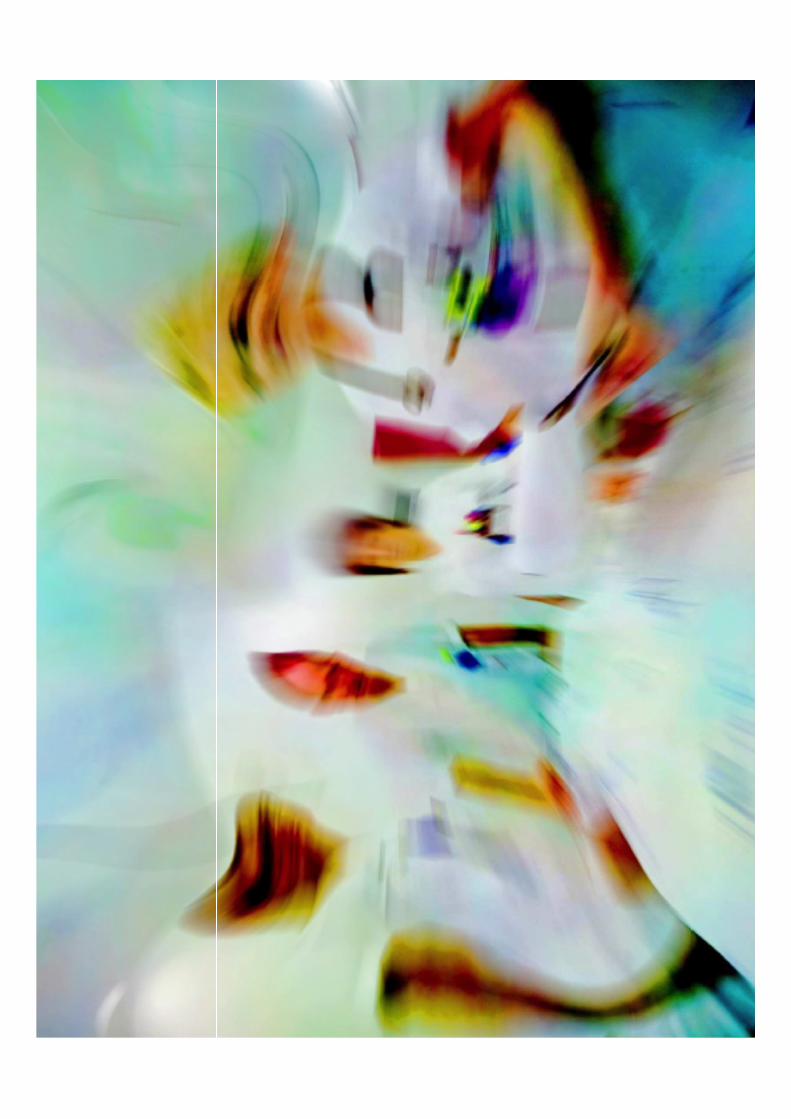
Common Meds Anticholinergic Drug Activity
Medication Anti-Ach activity (ng/ml atropine eq)Furosemide 0.22Digoxin 0.25Theophylline 0.44Warfarin 0.12Prednisolone 0.55Nifedipine 0.22Isosorbide 0.15Codeine 0.11Ranitidine 0.22
Am J Psych 1992;149:1393

LowLow

Lauretani F, Ceda GP, Maggio M et al. Aging Clin Ex Res 2010; 354:1157-1165

Lauretani F, Ceda GP, Maggio M et al. Aging Clin Ex Res 2010; 354:1157-1165

CHOLINERGIC DEFICIENCY AND DELIRIUM
1st CASE
HYPOREACTIVE DELIRIUM
ACETYLCHOLINE
MONOAMINEDA, NE, SE
HYPERREACTIVE DELIRIUM
ACETYLCHOLINE
DA
2nd CASE

Scott IA et al. MJA 2014 6 October; 201 (7)


Scott IA et al. JAMA Intern Med 2015; 175: 827-834



JAMA Int Med 2016 Feb 1;176(2):238-46.
Prevalence of PPI use from 2006 to 2011

Number of older persons exposed to PPI (in red)
Amos TB, Keith SW, Del Canale S, Orsi P, Maggio M, Baccarini S, Gonzi G, Liu M, Maio V.
J Clin Pharm Ther. 2015 Feb;40(1):7-13.


34
N. and % of older persons according to duration of PPI use
Uso IP
Parma Fidenza Valli Taro Sud-Est Totale
N % N % N % N % N %
<=60 gg 4961 30.5 2464 32.9 1191 30.3 1489 29.7 10105 30.9
61-180 gg 4356 26.8 1925 25.7 1105 28.1 1419 28.3 8805 26.9
181-360 gg 4962 30.5 2210 29.5 1189 30.2 1567 31.2 9928 30.4
>360 gg 1971 12.1 899 12.0 448 11.4 543 10.8 3861 11.8
Totale16250 7498 3933 5018 32699
Amos TB, Keith SW, Del Canale S, Orsi P, Maggio M, Baccarini S, Gonzi G, Liu M, Maio V.
J Clin Pharm Ther. 2015 Feb;40(1):7-13.

Ampio utilizzo di PPI nella popolazione anziana
Increased riskof GI disease
High prevalenceof
multimorbidity
Polifarmacotherapy (ASA,
Corticosteroids, NSAID, OAC)
LARGE USE IN OLDER PERSONS
Inappropriate use of PPI in older italian hospitalized patients (Study REPOSI) 66% at admission and 64% at
discharge
Pasina L et al. on Behalf of Reposi Investigators Eur J Intern Med 2011;22:205-210
25-70% of patients receiving PPI: not appropriateForgacs I, et al BMJ 2008; 336:2-3
Data coming from dAustralia, New Zealand, Ireland and Great Bretain : 63%, 33% and 67% of hospitalized patients were taking PPI without specific indication
Aunton M, J Clin Pharm Ther 2000; 25:333-40Mat Saad AZ, et al. Int J Clin Pract 2005; 59:31-4
Walker NM, et al. Pharm World Sci 2001;

Complications of chronic PPI therapy
Pulmonary and gastrointestinal infections (pneumonia, Clostridiumdifficile infections)
Pharrmacological interactions (Clopidogrel, Aspirina, DIFOSFONATI)
Skeletal scheletriche: fractures
Abrahamsen et al, Arch Intern Med 2011; 171 (11):998-1004
Elaine WY et al. Am J Med 2011; 124:519-526
Sandra Dial et al, JAMA 2005; 294 (23): 2989-2995Laheij RJ et al JAMA 2004; 292: 1955-1960
Recker RR, NEJM 1985; 313: 70-73Broeren MA et al, 2009 Ann Intern Med; 151: 755-756
Marcuard SP et al, 1994 Ann Intern Med; 120: 211-215
�
�
�
� Potential interference on micronutrient adsorbtion (Vit B12,iron, Calcium, Sodium, Magnesium)

Badiola et al. PlosOne 2013

Gomm W et al. Jama Neurology. 2016

Observational Study «PharmacosurVeillance in the elderly Care – PVC» conducted in Italian Community Hospitals and University-Hospitals, to evaluate drug consumption, drug adverse reactions and quality of hospital care in 506 older patients admitted in 11
acute wards in the period of time between April 1°and June 30 2007, discharged and followed during
1-year follow-up period
Methods PharmacosurVeillance Study
Maggio M, Corsonello A, et al. JAMA Intern Med. 2013 Apr 8;173(7):518-23

Chronic use of PPI is associated with higher risk of adverse events
Functional Decline
RehospitalizationMortalityCombinedEnd-Point


Maggio M et al. JAMA Intern Med. 2013 Apr 8;173(7):518-23

Relationship between use of PPI and adverseoutcomes
Maggio M et al. JAMA Intern Med. 2013 Apr 8;173(7):518-23

JAMA Intern Med. 2013 Apr 8;173(7):518-23

Linsky et al. 2013 JAMA Intern Med.
Katz MH. Arch Intern Med. 2011 Jun 13;171(11):1004-5.



1. La polifarmacoterapia è un marker di fragilità e declino funzionale anche nel soggetto con demenza/delirium;
2. La ricognizione farmacologica all’ingresso in ospedale è tra i momenti topici della «good clinical practice» multiprofessionale del paziente anziano ospedalizzato spt se affetto da demenza;
3. La « Medication list biopsy» non può prescindere da un peso attento del carico anticolinergico dei farmaci utilizzati e dell’appropriatezza prescrittiva
4. Il descripribing dei farmaci non appropriati costituisce un vero atto clinico che sempre di più si basa su algoritmi precisi (Canadesi) come dimostra l’esempio degli antipsicotici e dei PPI e di una formazione integrata Ospedale-Territorio
Take Home Messages