Embed Size (px)
Citation preview

KOL Lunch: Regulation of Drugs that Regulate Glucose: Cardiovascular Effects of
Drugs for Type 2 Diabetes
Updates for Cardiologists
Chicago, Illinois September 12, 2012
Content Collaborator

Session 4
Session 4: KOL Lunch: Regulation of Drugs that Regulate Glucose: Cardiovascular Effects of Drugs for Type 2 Diabetes Learning Objectives
1. Compare and contrast the potential risks, benefits, and safety profiles of pharmacotherapies frequently utilized in the management of type 2 diabetes.
2. Summarize key ongoing clinical trials that will yield data to guide clinical practice around the use of glucose-regulating drugs in patients with or at risk for cardiovascular disease.
Faculty
Darren K. McGuire, MD, MHSc Associate Professor of Medicine Division of Cardiology University of Texas Southwestern Medical Center Dallas, Texas
Dr Darren McGuire is an associate professor of medicine at the University of Texas (UT) Southwestern Medical Center, Dallas, in the division of cardiology, where he holds the Dallas Heart Ball Chair for Heart Disease Research in Women. Dr McGuire’s expertise is in large-scale clinical trial design and execution, and in drug registration/regulation, with a focus on diabetes and cardiovascular disease. Dr McGuire earned his medical degree from the Johns Hopkins University, and completed his internship and residency at UT Southwestern. He underwent fellowship training in cardiology at Duke University School of Medicine and received a Master in Health Sciences in Clinical Research from Duke Medicine’s Clinical Leadership Program. Dr McGuire joined the UT Southwestern faculty August 2001, where he is currently director of both the Cardiovascular Clinical Research Unit and the Parkland Hospital and Health System Outpatient Cardiology clinics. His research centers on the prevention of cardiovascular complications of diabetes, with broader interests in global cardiovascular risk–reduction strategies. He is actively involved in the leadership of numerous international clinical outcomes trials. Dr McGuire, who has published over 150 peer-reviewed manuscripts, reviews, editorials, and book chapters, is a senior editor of Diabetes and Vascular Disease Research and an associate editor of the American Heart Journal. He is a fellow of the American Heart Association (AHA) and the American College of Cardiology (ACC); immediate past chair of the AHA Diabetes Committee; co-chair of the ACC Diabetes Education Initiative; and a standing member of the US Food and Drug Administrations’ Cardiovascular and Renal Drugs Advisory Committee.
Peter Libby, MD, FACC Chief, Cardiovascular Medicine Brigham and Women’s Hospital
Mallinckrodt Professor of Medicine Harvard Medical School Boston, Massachusetts
Dr Peter Libby is chief of cardiovascular medicine at the Brigham and Women’s Hospital (BWH) in Boston. He also serves as the Mallinckrodt Professor of Medicine at Harvard Medical School, where he directs the D. W. Reynolds Cardiovascular Clinical

Session 4
Research Center. His current research focus is the role of inflammation in vascular diseases such as atherosclerosis. His areas of clinical expertise include general and preventive cardiology. An author and lecturer on cardiovascular medicine and atherosclerosis, Dr Libby has published extensively in medical journals, including Circulation, the Journal of Clinical Investigation, Proceedings of the National Academy of Sciences, the New England Journal of Medicine, and Nature. He is editor-in-chief of the new ninth edition of Braunwald’s Heart Disease. Dr Libby has also contributed chapters on the pathogenesis, treatment, and prevention of atherosclerosis to Harrison’s Principles of Internal Medicine. He has frequently served as a consultant to the National Heart, Lung, and Blood Institute, including a five-year term on its Board of Scientific Councilors, and was the recipient of the organization’s MERIT Award. Dr Libby has held numerous visiting professorships and has been selected to deliver over 50 named or keynote lectures throughout the world. Dr Libby’s professional memberships include the Association of American Physicians, the American Society for Clinical Investigation, and honorary membership in the British Atherosclerosis Society. The current president of the Association of University Cardiologists, Dr Libby has served in many volunteer roles for the American Heart Association (AHA), as chairman of several research committees and as member of AHA’s executive committee councils on arteriosclerosis, circulation, and basic science. Dr Libby earned his medical degree at the University of California, San Diego, and completed his training in internal medicine and cardiology at the Peter Bent Brigham Hospital (now the BWH). He has received recognition and numerous awards for his research accomplishments, including the 2006 Distinguished Scientist Award of the American College of Cardiology. He also holds an honorary Master of Arts from Harvard University. Faculty Financial Disclosure Statements The presenting faculty reports the following: Dr McGuire is a consultant for Genentech, Inc.; Roche; Pfizer Inc.; Daiichi Sankyo; Takeda Pharmaceutical Company Limited; Orexigen Therapeutics, Inc.; and Novo Nordisk Inc.
Dr Libby is a scientific advisory board member for Athera Biotechnologies, BIND Biosciences, Carolus Therapeutics, and Interleukin Genetics. He also serves as an unpaid consultant and/or is involved in clinical trials with AstraZeneca Pharmaceuticals LP; GlaxoSmithKline; Merck & Co., Inc.; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Pronova BioPharma; and Sigma-Tau Pharmaceuticals, Inc. Suggested Reading List Buse JB, Ginsberg HN, Bakris GL, et al. Primary prevention of cardiovascular diseases in people with diabetes mellitus: a scientific statement from the American Heart Association and the American Diabetes Association. Circulation. 2007;115(1):114-126.
Gore MO, McGuire DK. Cardiovascular disease and type 2 diabetes mellitus: regulating glucose and regulating drugs. Curr Cardiol Rep. 2009;11(4):258-263.
Inzucchi SE, McGuire DK. New drugs for the treatment of diabetes: part II: Incretin-based therapy and beyond. Circulation. 2008;117(4):574-584.
McGuire DK, Inzucchi SE. New drugs for the treatment of diabetes mellitus: part I: Thiazolidinediones and their evolving cardiovascular implications. Circulation. 2008;117(3):440-449.

1
Regulation of Drugs that Regulate Glucose:CV Safety Assessment of Diabetes Drugs
Darren K. McGuire, MD, MHSc
Associate Professor
Donald W. Reynolds Cardiovascular Clinical Research Center
University of Texas Southwestern Medical Center at Dallas
Disclosures
• Consultancy• F. Hoffmann La Roche
• Daiichi Sankyo
• Genentech
• Sanofi-Aventis
• Novo Nordisk
• Pfizer
• Regeneron
• Clinical Trial Leadership– Roche/Genentech
– Merck
– Eli Lilly/Daiichi Sankyo
– Novo Nordisk
– BMS/AstraZeneca
– Boehringer Ingelheim
– Takeda
– Orexigen
Entire presentation is “off label” since no glucose-lowering drugs have a cardiovascular indication or claim
Diabetes in Cardiology Cohorts
Am Heart J. 2003;145:285-91; Am Heart J. 2003;146:351-8; Circ. 2005;112:2397-2402; Lancet. 2002;359:2140;
2007 ADA Scientific Sessions-646-P
1997-1999(n=3266)
1994-1998(n=1612)
1996-2003(n=7310)
1998-2000(n=181)
2007(n=580)
Early Type 2 Diabetes Mellitus: A Cardiovascular Disease
0
5
10
15
20
25
30
Blindness ESRD Amputation Net Micro-vasc
CVA CAD Macro-vasc
10-yearrisk(%)
United Kingdom Prospective Diabetes Study (n=3867)Mean f/u=10 years
UKPDS Investigators. Lancet. 1998;352:837.
High Residual Risk of Diabetes: Observations from the Statin Trials
0%
10%
20%
30%
40%Statin No T2DMStatin T2DM
Inc
ide
nc
e o
f C
V E
ve
nts
1HPS Collaborative Group. Lancet. 2003;361:2005-2016; 2Sacks FM, et al. N Engl J Med. 1996;335:1001-1009, 3LIPID Study Group. N Engl J Med. 1998;339:1349-1357; Shepherd J, et al. Lancet. 2002;360:1623-1630; 5Sever PS, et al. Lancet. 2003;361:1149-1158.
HPS CARE LIPID PROSPER ASCOT-LLA
Coronary Calcium According to Glucose Status: The Dallas Heart Study
Chi-square trend: P < 0.0001
Das SR, et al. Am Heart J. 2006;151:1087-1093.

2
CHD Risk Appears to Begin at Low Blood Glucose Levels
N = 17,869 men, age 40 – 64 years; follow-up 33 years
*Relative to baseline group of all men with blood glucose < 83 mg/dL
83 mg/dL
1.6
1.2
0.8
0.4
0.0
−0.4
CH
D m
ort
ali
ty (
log
ha
zard
ra
tio
s)*
54 72 10890 126 144 162 180
OGTT blood glucose (mg/dL)
Brunner EJ, et al. Diabetes Care. 2006;29:26-31.
Mortality Impact of Glycemic Control: UGDP
0
5
10
15
20
0 1 2 3 4 5 6 7 8
Cardiovascular Causes
Years of Follow-up
TOLB (n=204)IVAR (n=204)ISTD (n=210)PLBO (n=205)
n=823
0
5
10
15
20
0 1 2 3 4 5 6 7 8
Years of Follow-up
All Causes
TOLB (n=204)IVAR (n=204)ISTD (n=210)PLBO (n=205)
Mo
rta
lity
Ra
te(%
)
21
1820
30
TotalDeaths
10
1213
26
TotalCV Deaths
UGDP Investigators. Diabetes. 1970;19(Suppl 2):789-830.
0.88 (0.79,0.99)Any diabetes-related endpoint
0.84 (0.71,1.00)Myocardial infarction
1.11 (0.81,1.51)Stroke
0.75 (0.60,0.93)Microvascular disease
Relative risk (95% CI)
Relative risk
0.1 0.5 2.0 10
Favors more intensive
Favors less intensive
UKPDS Group. Lancet. 1998;352:837-853.
Blood Glucose and Vascular Risk in Diabetes: UKPDS Findings
UKPDS Metformin Sub-Study: CHD Events
Myocardial infarction
Inci
den
ce p
er 1
,000
pat
ien
t-ye
ars
Coronary deaths
0
5
10
15
20 P = 0.01
NS
39%reduction
0
2
4
6
8
10 P = 0.02
50%reduction
Conventional Insulin Metformin Conventional Metformindiet SU’s diet
N = 411 951 342 411 342Events (n) 73 139 39 36 16
UKPDS Group. Lancet. 1998;352:854-865.
Guidance for Diabetes Drug Development Through 2008
• ICH Guidelines:– 1500 subjects
exposed
– 300-600 x 6 mos
– 100 x 1y
Off Target Adverse Drug Effects….
• Troglitazone– FDA Approval 3/1997
– 1.8 million patients treated in 3 years
– Post-marketing surveillance
• Acute liver failure in 94 patients
• 61 deaths
Troglitazone withdrawn from the market 3/2000

3
PROactive 1° EndpointDeath, MI, CVA, ACS, Leg Revasc. / Amputation, PCI, or CABG
Kap
lan
–Mei
er e
ven
t ra
te
Time from randomization (months)
0.25
0.20
0.15
0.10
0.05
0.0
Pioglitazone (514 events)Placebo (572 events)
HR 0.90P 0.095 CI 0.80 – 1.02
0 6 12 18 24 30 36
N at risk: 5,238 5,018 4,786 4,619 4,433 4,268 693 (228)
Dormandy JA, et al. Lancet. 2005;366:1279-1289.
ADOPT: Treatment effect on glucose control
Kahn SE, et al. N Engl J Med. 2006;355:2427-43.
GlyburideN=1441
MetforminN=1454
RosiglitazoneN=1456
0110
120
130
140
150
160
543210Years
FPG (mg/dL)
*
A1C(%)
7.2
7.6
6.8
6.4
6.0
00 1 2 3 4 5
8.0
Years
*
*p<0.05
N=4360 with new DM
ADOPT: Cardiovascular events
Kahn SE, et al. N Engl J Med. 2006;355:2427-43. Nissen S. N Engl J Med. 2007; 356: 2457-2471.
Rosiglitazone and CVD risk: Nissen Meta-analysis
*P=0.03†P=0.06
3.02.0
Odds Ratio
1.0 1.5
Myocardialinfarction
Cardiovasculardeath1.64†
1.43*
n=158 events
n=61 events
• Meta-analysis of 42 trials– Summary level data
• Inclusion criteria– Duration >24 weeks
– Randomized control
– Data for MI or CV death
• N = 27,843– 15,560 on rosiglitazone
– 12,283 on control
• Included 5 registration studies, DREAM and ADOPT
Summary of RCT & Meta-Analysis Data on TZDs and MI Risk
Risk ratios (95% CI)
Rosiglitazone Pioglitazone
0.1 1.0 10.0
ADOPT
DREAM
RECORD
Nissen
Singh
GSK
58
25
89
158
177
256
1.40
1.78
1.23
1.43
1.42
1.31
Events (n) Estimate Events (n) Estimate
0.1 1.0 10.0
263
290
0.83
0.81
PROactive
Lincoff
Rohatgi A, McGuire DK. Cardiovasc Drugs Ther. 2008;22:233-240.
CV Effects of Glucose Control in Recent Large-Scale Trials
Events (n): 572 vs. 514 371 vs. 352 590 vs. 557 264 vs. 235 319 vs. 678 126 vs. 81RRR 0.9 0.9 0.94 0.88 0.85 0.67
95% CI 0.8-1.02 0.78-1.04 0.84-1.06 0.74-1.05 0.74-0.97 0.51-0.89
Dormandy JA, et al. Lancet. 2005;366:1279-1289; ACCORD Study Group. N Engl J Med. 2008;358:2545-2559ADVANCE Collaborative Group. N Engl J Med. 2008;358:2560-2572; Holman RR, et al. N Engl J Med. 2008;359:1577-1589.

4
Intensive Glycemic Control and CVD Outcomes
CHD Events
All-causeMortality
Ray KK, et al. Lancet. 2009;373:1765-72.
2009 ADA/AHA/ACC Statement Recommendations
• Goal of A1C <7% remains reasonable – uncomplicated patients-Class I (A)
– with macrovascular disease-Class IIb (A)
• Incremental microvascular benefit may be obtained from even lower goals-Class IIa (C)
• Less stringent goals may be appropriate for those with advanced micro- or macrovasculardisease-Class IIa (C)
Circulation. 2009;119:351-357.
Cautions for Diabetes Medications in CHD Patients: Beware the Product Label• All sulfonylureas
– “….oral hypoglycemic drugs have been reported to be associated with increased cardiovascular mortality….”
• Metformin– Temporarily withhold at the time of or prior to and 48 hours
following iodinated contrast administration; resume after confirming baseline renal function
– Contraindicated with CKD≥2– No longer contra-indicated with heart failure
• Thiazolidinediones– Observe for signs/symptoms of heart failure– Caution for use with any HF (NYHA Class I-IV)– Initiation contra-indicated in Class III-IV
• Rosiglitazone (but not pioglitazone)– Because of the potential increased risk of myocardial infarction,
[rosiglitazone] is available only through a restricted distribution programMcGuire DK, Inzucchi SE. Circulation. 2008;117:440-9.
Inzucchi SE, McGuire DK. Circulation. 2008;117:574-84.http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/021071s040lbl.pdf
ADA/EASD Consensus Algorithm for Treatment of Type 2 Diabetes
Nathan DM, et al. Diabetologia. 2009;52:17-30.
Associations between Insulin Secretagogues and Mortality
N=107,806 Danish Adults Initiating Glucose-lowering TherapyF/U up to 9 yrs (mean 3.3 yrs)
9505 Deaths for Analysis
Schramm TK, et al. Eur Heart J. 2011, ePub April 6
Proposed Algorithm for Glucose Treatment in T2DM Patients With/At risk for CVD
Metformin
+ Pioglitazone
+ Secretagogue,α-glucosidase
inhibitor,DPP-4 inhibitor,
or GLP-1 analogue
Insulin
HbA1c ≥ 7.0%
HbA1c ≥ 7.0%
HbA1c ≥ 7.0%
HbA1c ≥ 7.0%
HbA1c ≤ 7.0%
HbA1c ≤ 7.0%
HbA1c ≤ 7.0%
Inzucchi SE & McGuire DK. Circulation. 2008;117:574-584.

5
Proposed Algorithm for Glucose Treatment in T2DM Patients With/At risk for CVD
Metformin
+ Pioglitazone
+ Secretagogue,α-glucosidase
inhibitor,
Insulin
HbA1c ≥ 7.0%
HbA1c ≥ 7.0%
HbA1c ≥ 7.0%
HbA1c ≥ 7.0%
HbA1c 7.0%
HbA1c 7.0%
HbA1c 7.0%
Adapted from: Inzucchi SE & McGuire DK. Circulation. 2008;117:574-584.
GLP-1analogue,or DPP IV inhibitor
HbA1c 7.0%
HbA1c ≥ 7.0%
Converging Pressures for Regulatory Change: Beyond A1C• Diabetes common and increasing
– Approaching 10% of US adult population and 300 million worldwide
• Morbid and mortal disease– Especially cardiovascular– Clear graded associations with severity of hyperglycemia
• Proliferation of glucose-lowering therapeutic alternatives– Before 1995: insulin, sulfonylureas, glucosidase inhibitors– 1995: metformin– Now: 33 formulations representing 11 classes
• Discordance in clinical trials– Bi-directional invalidation of A1C as target for CVD risk reduction
• Failure of hypothesis?• On target adverse effects?• Off target adverse effects?• Too little, too late?
Summary of Revised Guidance for Diabetes Drug Development
• ICH Guidelines:– 1500 subjects
exposed
– 300-600 x 6 mos
– 100 x 1y
• FDA Revised Guidance (2/2008)– Phase 2/3 data on 2500
subjects exposed to Investigational Agent
– 1300-1500 for 1y
– 300-500 for 18 mo or more
New FDA Regulatory Guidance for Drugs for Type 2 Diabetes
http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2008/ucm116994.htm
– “…sponsors should demonstrate that the therapy will not result in an unacceptable increase in cardiovascular risk.”
• Advocates meta-analysis strategy for non-inferiority assessment
• Blinded central adjudication of CVD events in Phase 2 & 3• Inclusion of high-risk subjects: advanced CVD; elderly; CKD• Minimum exposure of 2 years
Novel Drugs & Targets in Development for Diabetes
• Bromocriptine• Long-acting GLP-1 receptor
agonists• DPP IV inhibitors• Ranolazine• Dual PPAR/ agonists• Pan PPARα// agonists• Sodium-GLucose coTransporter
(SGLT) 1 and 2 antagonists• Salicylate derivatives• Glucagon receptor antagonists• Fructose 1,6 Bisphosphatase
inhibitors• Glucokinase activators
• 11β-hydroxysteroiddehydrogenase (HSD)-1 inhibitors
• Protein tyrosine phosphatase 1B inhibitors
• Acetyl CoA carboxylase-1 and -2 inhibitors
• G-protein coupled receptor (GPR)-40 & -119 Agonists
• Protein Tyrosine Phosphatase(PTB)-1b inhibitors
• Carnitine Palmitoyltransferase(CPT)-1 inhibitors
• Acetyl CoA Carboxylase (ACC)-1 & -2 inhibitors
Inzucchi SE & McGuire DK. Circulation. 2008;117:574-584. Not FDA approved for treatment of diabetes
• Long-acting GLP-1 receptor agonists
• DPP IV inhibitors• Ranolazine• Salicylate derivatives• Dual PPAR/ agonists• Pan PPARα// agonists• Sodium-GLucose coTransporter
(SGLT) 1 and 2 antagonists• Glucagon receptor antagonists• Fructose 1,6 Bisphosphatase
inhibitors• Glucokinase activators
• 11β-hydroxysteroiddehydrogenase (HSD)-1 inhibitors
• Protein tyrosine phosphatase 1B inhibitors
• Acetyl CoA carboxylase-1 and -2 inhibitors
• G-protein coupled receptor (GPR)-40 & -119 Agonists
• Protein Tyrosine Phosphatase(PTB)-1b inhibitors
• Carnitine Palmitoyltransferase(CPT)-1 inhibitors
• Acetyl CoA Carboxylase (ACC)-1 & -2 inhibitors
Inzucchi SE & McGuire DK. Circulation. 2008;117:574-584.
Novel Drugs & Targets in Development for Diabetes

6
Toward Establishing Non-inferiority of Diabetes Drugs: MACE Analyses
1.8
Premarketing AnalysesUpper CL of 95% CI <1.8At HR=1.0; ~120 events
1.0
*MID=minimally important difference
1.3
Post-marketing AnalysesUpper CL of 95% CI <1.3At HR=1.0; ~1200 events
GLP-1: Multiple Effects That Regulate Glucose Homeostasis
Drucker DJ. Cell Metabolism. 2006;3:153-165.
GLP-1 Receptors in the Cardiovascular System
Ban, et al. Circulation. 2008;117:2340-2350.
C: Mesenteric artery SM cell
F:Cardiomyocytes
G: Endocardium
H: Vascular endothelium &
SM cells
Early and Sustained BP Reduction with Liraglutide
*p=0.0030; **p=0.0001
0
127
128
129
130
131
132
133
134
0 2 4 6 8 10
LS
me
an
s S
BP
(m
mH
g)
Time (weeks)
Liraglutide 1.2 mg, n=896Liraglutide 1.8 mg, n=1363
Placebo, n=524
12 14 16 18 20 22 24 26
LEAD-1–6: meta-analysis (repeated measure analysis)
***
Fonseca, et al. Diabetes. 2009;58 (Suppl. 1): A146.
GLP-1 Agonist Effects on Selected CV Biomarkers
Parameter Liraglutide Rosiglitazone Glimepiride Glargine Exenatide Placebo
BNP (%) -11.9 30.9 0.1 10.2 -3.9 1.4
hsCRP (%) -23.9 -42.6 -12.3 2.8 -15.6 -3.0
Plutzky et al. Diabetologia. 2009;52 (Suppl. 1): S299.
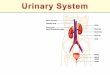
SGLT2 receptors
• SGLT2 - high-capacity, low-affinity glucose transporter
• SGLT1 is a low-capacity, high-affinity glucose transporter
– Highly expressed in the small intestine
SGLT2SGLT1
proximal
convoluted tubule distal convoluted tubule
collecting duct
Urine
glomerulus
loop of Henle
collecting
Glucose reabsorbed to systemic circulation
Courtesy , Bruce Neal, MD

7
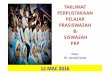
SGLT2 inhibitors
Specific inhibition of SGLT2
• Loss of ~80 grams of glucose/day in T2DM subjects
• lowers plasma glucose with minimal hypoglycemia
• Loss of ~ 300-400 cal/day
SGLT2SGLT1
proximal
convoluted tubule distal convoluted tubule
collecting duct
glomerulus
loop of Henle
collecting
Glucose reabsorbed to systemic circulation
GlycosuriaCourtesy , Bruce Neal, MD
Present Landscape of CVD Outcomes Trials in Type 2 DM
Trial Drug Sample Size Stage
ORIGIN Insulin glargine 12,500 Started 9/2003
TECOS Sitagliptin 14,000 Started 12/2008
ACE Acarbose 7500 Started 2/2009
TIDE Rosi/Pio 16,000 Halted
EXAMINE Alogliptin 5,400 Started 09/2009
CANVAS Canagliflozin 4500 Started 11/2009
T-emerge 8 Taspoglutide 2,000 Halted
AleCardio Aleglitazar 7,000 Started 2/2010
SAVOR TIMI-53 Saxagliptin 16,500 Started 4/2010
ELIXA Lixisenatide 6000 Started 6/2010
EXSCEL Exenatide LAR 12,000 Started 6/2010
C-SCADE 8 Empagliflozin 12,500 Started 7/2010
CAROLINA Linagliptin 6000 Started 10/2010
LEADER Liraglutide 8723 Started 8/2010
>144,000 patients http://www.clinicaltrials.gov
Present Landscape of CVD Outcomes Trials in Type 2 DM
Trial Drug Sample Size Stage
ORIGIN Insulin glargine 12,500 Started 9/2003
TECOS Sitagliptin 14,000 Started 12/2008
ACE Acarbose 7500 Started 2/2009
TIDE Rosi/Pio 16,000 Halted
EXAMINE Alogliptin 5,400 Started 09/2009
CANVAS Canagliflozin 4500 Started 11/2009
T-emerge 8 Taspoglutide 2,000 Halted
AleCardio Aleglitazar 7,000 Started 2/2010
SAVOR TIMI-53 Saxagliptin 16,500 Started 4/2010
ELIXA Lixisenatide 6000 Started 6/2010
EXSCEL Exenatide LAR 12,000 Started 6/2010
C-SCADE 8 Empagliflozin 12,500 Started 7/2010
CAROLINA Linagliptin 6000 Started 10/2010
LEADER Liraglutide 8723 Started 8/2010
>144,000 patients http://www.clinicaltrials.gov
Present Landscape of CVD Outcomes Trials in Type 2 DM
Trial Drug Sample Size Stage
ORIGIN Insulin glargine 12,500 Started 9/2003
TECOS Sitagliptin 14,000 Started 12/2008
ACE Acarbose 7500 Started 2/2009
TIDE Rosi/Pio 16,000 Halted
EXAMINE Alogliptin 5,400 Started 09/2009
CANVAS Canagliflozin 4500 Started 11/2009
T-emerge 8 Taspoglutide 2,000 Halted
AleCardio Aleglitazar 7,000 Started 2/2010
SAVOR TIMI-53 Saxagliptin 16,500 Started 4/2010
ELIXA Lixisenatide 6000 Started 6/2010
EXSCEL Exenatide LAR 12,000 Started 6/2010
C-SCADE 8 Empagliflozin 12,500 Started 7/2010
CAROLINA Linagliptin 6000 Started 10/2010
LEADER Liraglutide 8723 Started 8/2010
>144,000 patients http://www.clinicaltrials.gov
Present Landscape of CVD Outcomes Trials in Type 2 DM
Trial Drug Sample Size Stage
ORIGIN Insulin glargine 12,500 Started 9/2003
TECOS Sitagliptin 14,000 Started 12/2008
ACE Acarbose 7500 Started 2/2009
TIDE Rosi/Pio 16,000 Halted
EXAMINE Alogliptin 5,400 Started 09/2009
CANVAS Canagliflozin 4500 Started 11/2009
T-emerge 8 Taspoglutide 2,000 Halted
AleCardio Aleglitazar 7,000 Started 2/2010
SAVOR TIMI-53 Saxagliptin 16,500 Started 4/2010
ELIXA Lixisenatide 6000 Started 6/2010
EXSCEL Exenatide LAR 12,000 Started 6/2010
C-SCADE 8 Empagliflozin 12,500 Started 7/2010
CAROLINA Linagliptin 6000 Started 10/2010
LEADER Liraglutide 8723 Started 8/2010
>144,000 patients http://www.clinicaltrials.gov
Present Landscape of CVD Outcomes Trials in Type 2 DM
Trial Drug Sample Size Stage
ORIGIN Insulin glargine 12,500 Started 9/2003
TECOS Sitagliptin 14,000 Started 12/2008
ACE Acarbose 7500 Started 2/2009
TIDE Rosi/Pio 16,000 Halted
EXAMINE Alogliptin 5,400 Started 09/2009
CANVAS Canagliflozin 4500 Started 11/2009
T-emerge 8 Taspoglutide 2,000 Halted
AleCardio Aleglitazar 7,000 Started 2/2010
SAVOR TIMI-53 Saxagliptin 16,500 Started 4/2010
ELIXA Lixisenatide 6000 Started 6/2010
EXSCEL Exenatide LAR 12,000 Started 6/2010
C-SCADE 8 Empagliflozin 12,500 Started 7/2010
CAROLINA Linagliptin 6000 Started 10/2010
LEADER Liraglutide 8723 Started 8/2010
>144,000 patients http://www.clinicaltrials.gov

8
ADA Standards of Medical Care: Cardiovascular Risk Modification
• Lifestyle• Aspirin (75-162mg daily) for those with
– CVD; or– 1 CRF in men >50 or women >60
• Lipids– For age>40 with 1 CRF, statin regardless of baseline LDL
• Target a) LDL<100 mg/dl (<70 mg/dl optional); OR 30-40% reduction
• TGs <150 and HDL>40/50 for men/women
• Blood pressure target of <130/80 mmHg• ACEI or ARB; thiazide, BBlocker, CCB• ACEI-independent of BP for age>55 + another CRF
Diabetes Care. 2011;34 Suppl 1:S11-61.
Benefit of Comprehensive, Intensive Management: STENO 2 Study
• Treatment Goals:– Intensive TLC
– HgbA1c <6.5%
– Cholesterol <175
– Triglycerides <150
– BP <130/80
Gæde P. N Engl J Med. 2008;258:580-591.
CV Risk Modification in Diabetes: Results from the Dallas Heart Study
0
20
40
60
80
100
ASA* ACEI* Statin* BP Rx BP<130/80
Lipid Rx LDL<100
*Proportion meeting 2005 ADA guideline criteria
N=410 with prevalent diabetes
Das S, et al. Am Heart J. 2006;151:1087-93.
ACCF Education Initiative
• A– A1C (<7%)– ASA daily (age > 50
(men) or 60 (women)
• B– Blood pressure
(< 130/80 mm Hg)
• C– Cholesterol
• LDL < 100 mg/dL(optional < 70 mg/dL)
• Non-HDL < 130 mg/dL(optional < 100 mg/dL)
– Cigarette abstinence
• D– Diabetes prevention and
education
• E– Exercise
• Daily moderate intensity aerobic physical activity
• F– Food choices
• Limit caloric intake/portion size
• Limited saturated and no trans-fats
http://www.cardiosource.com/GenSAPX/UserAgreement.asp?productID=134
Conclusions
• Diabetes is common and increasing• Principal complication is cardiovascular disease• Clear graded association of risk with hyperglycemia
• Diabetes is associated with increased risk for adverse CV outcomes despite best available therapies
• Role of glucose control in CVD risk mitigation remains uncertain
• What drugs/strategies; what intensity; what timing• Side effects-both on- and off-target
• A number of plausible therapeutic targets in T2DM continue to hold promise
• Many presently under RCT investigation
Questions & Answers
?