Embed Size (px)
Citation preview

Knowledge of General Practitioners in Irelandon Female Genital Mutilation
EGIDE DHALA. February 2013
SURVEY

AkiDwA would like to thank:All the General Practitioners who responded to the research.
HSE- Social Inclusion Unit for funding AkiDwA FGM work and in particular this researchPat Guerin for proof reading and editing draft document
© Copyright 2013 AkiDwAPublished by AkiDwA, Unit 2, Killarney Court, Upper Buckingham Street, Dublin 1, Republic of Ireland.
Telephone: (+1 353) 01 834 9851 • Mobile: (+353 87) 4150906• E-mail: [email protected] • Visit: www akidwa.ie

Knowledge of General Practitioners in Irelandon Female Genital Mutilation
SURVEY

2
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY
Executive Summary
AkiDwA conducted this survey following its campaign and advocacy work aimed at ending Female Genital Mutilation(FGM), and at supporting women and girl victims of this harmful practice. A total of 64 GPs (general practitioners)from all counties in the Irish Republic participated in the survey. It revealed that a large majority of GPs are not familiarwith FGM or its effects on the health of women.
The results show that almost 80% of surveyed GPs in Ireland have no knowledge of FGM or its associated issues,and the same percentage of GPs have never encountered women or girls who have undergone FGM. However 25FGM patients attended clinics to 12 of the 64 respondent GPs.
As the first point of contact in Irish healthcare services, it is reasonable to expect that GPs would have anunderstanding of key issues relating to the health of the immigrant population. This was suggested by the HSENational Intercultural Health Strategy (2007-2012). Surprisingly, however, this survey shows that over 65% of GPswere unable to identify symptoms presented by FGM patients. And, as the research reveals, none of these GPs wereaware of the referral pathways for providing support and/or information to FGM clients patients who had been victimsof FGM. On a positive note, however, almost 80% of surveyed GPs expressed a desire to receive a list of servicesto which FGM patients could be referred.
The limit or lack of GPs knowledge on FGM and its associated issues has been also noticed in relation to FGMprevalence in Ireland (almost 60% did not know), the Irish law that prohibit it (80% did not know) and even thesafeguarding procedures when it’s about protecting girls at risk of FGM (25% were unable to answer the question).
This survey is a real step forward as almost 80% of the respondent GPs have shown great interest in being up skilledon FGM. As AkiDwA has been planning to progress further its work on FGM, the present research is a clear evidenceof the need among the General Practitioners in Ireland to be trained on FGM health related issues. Also it has beenclearly shown that there is a need of a dedicated service as a referral point for the FGM patients.
Table of contents
I. Introduction ............................................................................................................................4
1. Background....................................................................................................................4
a. Definition ........................................................................................................................4
b. History............................................................................................................................4
c. Prevalence ....................................................................................................................4
d. Health consequences ....................................................................................................4
2. AkiDwA work on FGM ..................................................................................................5
3. Objective of the Survey..................................................................................................6
4. Methodology ................................................................................................................6
a. Design ............................................................................................................................6
b. Study area and Data collection......................................................................................6
c. Structure of the questionnaire........................................................................................6
d. Data analysis..................................................................................................................6
II. Survey Outcomes....................................................................................................................7
III. Conclusion ............................................................................................................................12
IV. Recommendations ................................................................................................................13
V. References ............................................................................................................................14
VI. Appendix ..............................................................................................................................15
3
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY
I. Introduction
1. Background
a. Definition
Female Genital Mutilation (FGM), also known as Female Genital Cutting or Female Circumcision is defined by theWorld Health Organisation as any procedure involving partial or total removal of the external female genitalia or otherinjury to the female genital organs for non-medical reasons (WHO, 2012).
Expanding on this definition, the WHO classified FGM into 4 different types, including:
- Type 1: Partial or total removal of the clitoris and/or the prepuce (clitoridectomy)
- Type 2: Partial or total removal of the clitoris and the labia minora, with or without excision of the labiamajora (excision)
- Type 3: Narrowing of the vaginal orifice with creation of a covering seal by cutting and repositioning thelabia minora and/or the labia majora, with or without excision of the clitoris (infibulation)
- Type 4: All the other harmful procedures to the female genitalia for non-medical purposes, e.g. pricking,piercing, incising, scraping and cauterisation.
b. History
It is not known where the tradition of FGM originated. This practice has been occurring for thousands of years,starting long before the establishment of both Christianity and Islam. Ancient Egyptian mummies were foundcircumcised, indicating that the practice dates from as far back as the fifth century B.C. (Dunsmuir & Gordon, 1999).
FGM has been performed by different cultures for centuries. The ‘reasons’ for the practice, include tradition, rite ofpassage into womanhood, preservation of virginity until marriage, social acceptance among peers, and on aestheticgrounds (WHO, 2008). These strong cultural factors have seen the traditional practice of FGM maintained acrosstime despite the negative health implications for the girls and women on whom it is performed.
c. Prevalence
FGM is practiced in at least twenty-eight countries in Africa, and can also be found in the Middle East and Asia. Theprevalence of FGM varies widely within countries and often depends on tribal and regional traditions and the criteriagoverning marriage. Globally, it is estimated that between 100 million and 140 million women and girls haveundergone FGM and more than three million girls are at risk of FGM every year in Africa alone (WHO, 2008).
The European Parliament’s Committee on Women’s Rights and Gender Equality estimates that about 500,000 girlsand women living in Europe have undergone FGM (Amnesty International, 2009). Using population data from CentralStatistics Office (CSO 2011) and global Female Genital Mutilation prevalence statistics, AkiDwA estimates that 3,780women living in Ireland have undergone FGM.
d. Health consequencesFGM has no health benefits. It involves removing or damaging healthy body parts. This results in damage to a girl’sor women reproductive organs. Some of the immediate health consequences of FGM include (WHO, 2008):
• Severe pain, shock and bleeding
• Difficulty passing urine
• Psychological trauma
• Infection
• Death as a result of the above.
4
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY

Long-term complications include:
• Chronic urinary and menstrual problems
• Chronic pain
• Pelvic inflammatory disease
• Cysts
• Increased risk of HIV transmission
• Infertility
• Serious problems for mother and baby during childbirth
2. AkiDwA work on FGM
Akina Dada wa Africa (AkiDwA), Swahili for sisterhood, is a national network of migrant women living in Ireland andwas established in 2001 by a group of African women to address isolation, racism and Gender Based Violence thatthey were experiencing at that time. The organisation has been working on the issue of FGM since 2001, throughraising awareness, promoting migrant women’s health, and campaigning for legislation to prohibit the practice. In2005, consultations with women from communities where FGM is being practiced led to a partnership with the IrishFamily Planning Association (IFPA). Both Organisations agreed to develop a National Plan of Action to address FGMin Ireland in 2008. This was supported by a steering committee of diverse stakeholders including children’s advocacygroups, women and human rights organisations.
Since 2001 AkiDwA have been campaigning tirelessly for a law to be put into place in Ireland that Ban practice ofFGM. In 2009, AkiDwA and the IFPA made representations to the Joint Oireachtas Committee on Health and Childrenon the need for legislation to prohibit FGM and for the promotion of health services related to FGM. After a decadeof campaigning and lobbying The Criminal Justice (Female Genital Mutilation) Act 2012 was signed into law on April2012, and became effective on September 2012. The act also creates an innovative offence of removal from theState of a girl for the purpose of FGM. The legislation takes a human rights perspective and stipulates that the rightto practice one's cultural traditions and beliefs cannot be used to justify FGM, which has been internationallyrecognised as a form of gender-based violence. Punishment is up to 14 years imprisonment and/or a fine; for asummary conviction, the penalty is a fine of up to €5,000 and/or imprisonment for up to 12 months or both.
AkiDwA and the Royal College of Surgeon’s published an information handbook - Female Genital Mutilation:Information for Healthcare Professionals Working in Ireland - to raise awareness among healthcare professionals,second edition of this publication is in the process of been published.
In 2008 AkiDwA produced the first initial statistics of the prevalence of FGM in Ireland this was done by Using Irish2006 census data from the Central Statistics Office and synthesising it with global FGM prevalence data, a figure of2,585 women living in Ireland who have undergone FGM was derived, this figure was updated in 2010 and in 2013after the 2011 census, there are currently 3780 women in Ireland who have undergone through FGM. The currentdata has shown that despite a decline in inward migration to Ireland the figure of the prevalence of FGM in Irelandcontinue to increase.
An Bord Altranais Practice Standards for Midwives, which is sent to all registered midwives in Ireland, came intoforce in July 2010 and now includes a section on FGM, with a reference to AkiDwA website for further information
AkiDwA lobbied to have Female Genital Mutilation (FGM) included in the new Irish national standardized maternityhospital chart under Risk Factors. FGM is now listed in the National Maternity Healthcare. This new form will beused for all women booking for maternity care and includes for the first time at a national level FGM as a risk factorfor obstetric care.
To date AkiDwA have delivered awareness raising and training to over 3000 health care professionals, that includemedical student and AkiDwA has and continue to raise awareness on FGM at local regional and national level throughmedia, seminars, workshops, conferences and publications
Since 2009 AkiDwA has been the Irish partner on European END FGM Campaign led by Amnesty International
In 2010 AkiDwA established two community forums for dialogue on FGM in Cork and Galway and in February 2013the organisation established the Community Health Ambassadors- these are dedicated volunteers who are raisingawareness on health related issues that pertain to migrant women. AkiDwA had offered training to six women frommigrant community that are currently doing outreach work mainly raising awareness on FGM around the country.
In 2012 AkiDwA published an information leaflet for the public- Female Genital Mutilation and the law in Ireland.
5
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY
3. Objective of the survey
Ireland’s National Action Plan to address FGM states that: “many health care professionals and other organisationssupporting migrant women are not yet aware of the existence of FGM, the health implications of FGM particularlyas they relate to childbirth and/or an appropriate referral pathway including child protection pathways. As a result,women and girls are not able to access the care and services they need and health care professionals and otherscharged with supporting migrant women are unsure of how to provide appropriate support” (INAP, p.9).
The purpose of the present survey is to ascertain the knowledge of FGM amongst the General Practitioners in Irelandin order to help inform the planning of awareness programmes and support the needs of migrant women and girlswho are at risk or affected by FGM in Ireland.
Three specific objectives form the basis of the work that AkiDwA is willing to pursue on FGM, that is:
• To identify training needs of GP / Practice Nurses and gaps in service provision
• To provide information regarding referral agencies for support and counselling
• To improve GPs and Practice Nurse’s knowledge and implications of FGM.
4. Methodology
a. Design
This is a narrative study carried out by collecting quantitative data through a designed questionnaire.
b. Study area and data collection
There are approximately 2,600 practicing GPs in Ireland. In order to achieve the survey objectives, a questionnairewas sent to 218 GPs by post with stamped returned envelopes. In addition, questionnaires were sent to 600 GPsby e-mail. The questionnaire probed their level of knowledge on issues related to FGM and thus their ability to makean appropriate health intervention.
Accessing GPs for the purpose of carrying out this research was done through a GP contact list published in theIrish Medical Directory (2012-2013). A random selection of GPs was made throughout all the counties in the Republicof Ireland. More questionnaires were sent to GPs based in places where the population of migrants was greater,using the RIA designated accommodation centres for people seeking asylum as a guideline. Also female GPs wereprioritised as female matters are mostly referred to female GPs in Ireland.
Sixty-two of the 218 GPs surveyed by post completed the questionnaire within a month, representing almost a 30% return. The return from GPs surveyed by email achieved a much smaller return. Of the 600 GPs who receivedtheir questionnaires by email, only two responded. The survey outcomes are based on a total of sixty-four completedquestionnaires.
c. Structure of the questionnaire
The questionnaire specifically designed for this study is in the appendix. To make the collected data standardisedand easy to analyse, closed questions were mostly used. And in order to allow GPs to respond freely, thequestionnaire was anonymous and did not request that respondents identify their gender.
d. Data analysis
Data was summarised manually by counting how many respondents chose each option on each item and the countwas recorded.
6
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY

II. Survey Outcomes
In Ireland, General Practitioners are the first point for accessing heath care. In most surgeries GPs have contractednurses who may deal from time to time with health issues related to women. On the first question asking to whatcapacity the participants responded to the survey, it resulted that all 64 respondents were GPs themselves. Howeverit cannot be concluded that practicing nurses have never had to deal with FGM cases in GP surgeries.
Responding on their knowledge of FGM, the majority of GPs, sixty-three, were aware of its existence but only few,thirteen, were able to identify its different types.
Table 1: Knowledge of FGM and its different types by GPs
7
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY
The above figures show that despite knowing what FGM is, the majority of GPs are not able to identify its differentcharacteristics. Is it because of the fact that they have never had to deal with FGM cases in their clinics? Such anassumption cannot be made with certainty. The following section will inform whether or not good knowledge of FGMdepends on the encountering experience with women and girls who were victims of the practice.
Through this survey, AkiDwA was able to get an idea on a sampling number of clients with FGM that have attendedGP clinics in Ireland. Figures below show whether or not respondent GPs have seen women or girls who haveundergone FGM and the total numbers of women who attended GP surgeries in Ireland.
Table 2: GPs who have seen FGM clients and the number of people who attended GP surgeries
Knowledge of What FGM is Knowledge of different types of FGM
a. GPs who have seen FGM clients
No: 52 Yes: 12
b. Number of FGM clients who attended GP clinics in Ireland: 25
A total of twenty-five migrant women who have undergone FGM attended clinics in Ireland to eleven out of sixty-four GPs who responded to the questionnaire.

It is curious to note that the number of GPs who have knowledge of the different types of FGM directly correspondswith the number who has seen clients with FGM in their clinics. One may be attempted to deduct that GPs’ deepknowledge of the FGM features depends on their experience of having to deal with the issue. This is not necessarilytrue, however. Of the twelve respondents who met with FGM patients, only three could differentiate between typesof FGM. In addition, one GP had dealt with FGM cases abroad but not in Ireland. Thus only one-third of GPs whomet FGM clients can recognize the different types of FGM. The other two-thirds of GPs who had to deal with FGMcases were not aware of its different types. This is likely to cause a deficiency in terms of providing proper care andsupport.
FGM victims present different types of complications which GPs must be aware of in order to identify the appropriatereferral pathways. In fact, according to the World Health Organisation, the symptoms range from physicalcomplications to psychological/emotional ones (WHO, 2008). Asking whether FGM clients presented with physicalor psychological/emotional complications, the majority of respondents – forty-two- did not answer the question andtwelve of the twenty-two participants who responded to that question were those who have met FGM clients in theirclinics.
Table 3: Complications presented by women who have undergone FGM
8
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY
Type of Complication GPs with GPs with no Total %experience of FGM experience of FGM
Physical 1 1 1.5%
Psychological/Emotional 3 3 4.7%
Both 6 10 16 25%
None 2 2 3.1%
No Answer 42 42 65.6%
The above figures show clearly that the GPs surveyed have little exposure to FGM cases perhaps explaining theirlimited knowledge on the issue. The majority of GPs (65.6%) were unable to identify the kind of symptoms FGMvictims can present with, reflecting their inexperience of FGM patients. This interpretation is suggested by the factthat 83.3% of GPs who have been exposed to FGM cases could identify either physical or psychological/emotionalsymptoms, or both in some instances.
Despite the WHO assertion, it appears that the impact of FGM on women has not yet captured the attention of GPsin Ireland and thus limits their capacity to make effective referrals, thereby allowing patients to access adequatesupport from specialist services.
When asked whether or not they had referral pathways for providing support or information to the FGM clients, allthe respondent answered in the negative. This also supports the interpretation that GPs largely remain unaware ofthe impact of FGM on those women subjected to the practice. On the positive side, a large majority of therespondents (76.6%) were keen to have a referral list that they could use whenever FGM clients attend their clinics.
Table 4: GPs willing to get a referral list for support/information to FGM clients
Yes No No Answer
GPs with experience of FGM 8 2 2
GPs with no experience of FGM 41 9 2
Total 49 11 4
As it appears on the above table, the majority of GPs are in favour of receiving a referral list that they would usewhenever they see clients who have undergone FGM and who may have sustained marks. Even respondents whohave met with FGM clients in their clinics have expressed the need for a referral list (67.7%). Of the respondentswho either did not show interest in getting a referral list or did not answer the question, two commented that theywould refer FGM clients to local Gynaecology or counselling services and one said that there were very few migrantsliving in their area.
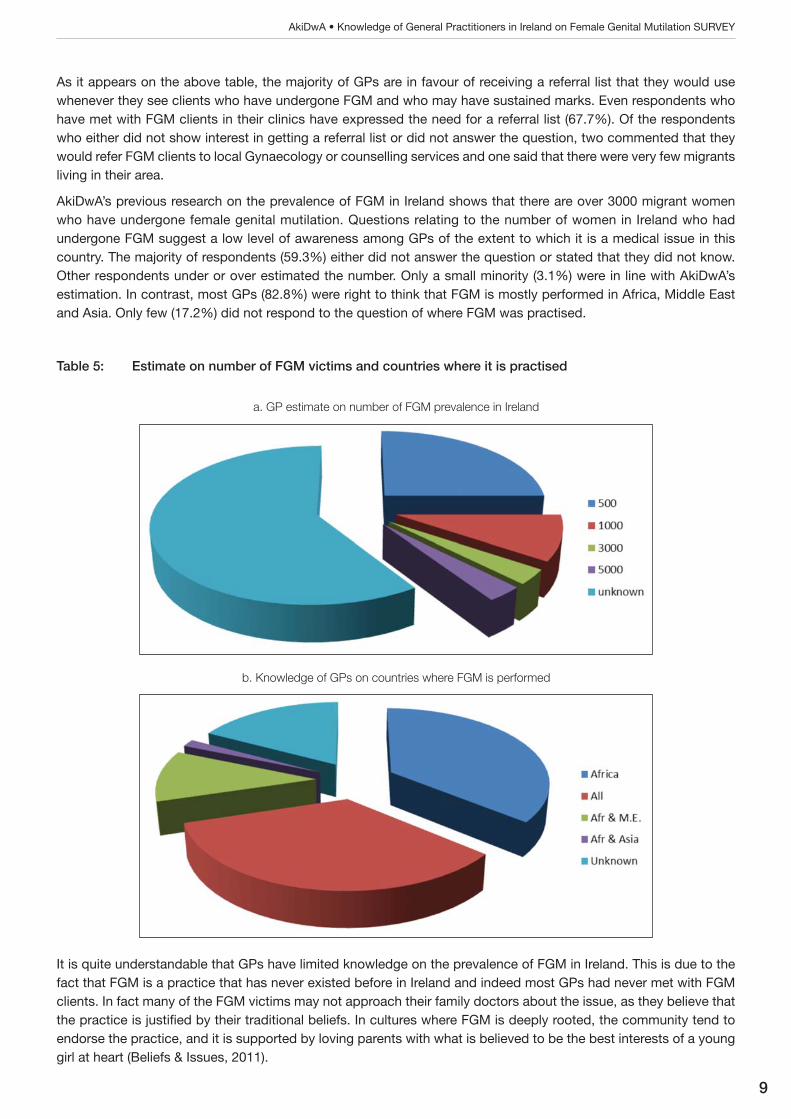
AkiDwA’s previous research on the prevalence of FGM in Ireland shows that there are over 3000 migrant womenwho have undergone female genital mutilation. Questions relating to the number of women in Ireland who hadundergone FGM suggest a low level of awareness among GPs of the extent to which it is a medical issue in thiscountry. The majority of respondents (59.3%) either did not answer the question or stated that they did not know.Other respondents under or over estimated the number. Only a small minority (3.1%) were in line with AkiDwA’sestimation. In contrast, most GPs (82.8%) were right to think that FGM is mostly performed in Africa, Middle Eastand Asia. Only few (17.2%) did not respond to the question of where FGM was practised.
Table 5: Estimate on number of FGM victims and countries where it is practised
9
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY
a. GP estimate on number of FGM prevalence in Ireland
b. Knowledge of GPs on countries where FGM is performed
It is quite understandable that GPs have limited knowledge on the prevalence of FGM in Ireland. This is due to thefact that FGM is a practice that has never existed before in Ireland and indeed most GPs had never met with FGMclients. In fact many of the FGM victims may not approach their family doctors about the issue, as they believe thatthe practice is justified by their traditional beliefs. In cultures where FGM is deeply rooted, the community tend toendorse the practice, and it is supported by loving parents with what is believed to be the best interests of a younggirl at heart (Beliefs & Issues, 2011).
However with regard to countries where FGM is performed, it is clearly demonstrated that GPs are well aware of thefact that African, Middle East and Asian countries have kept very traditional practices which may impact on humanhealth. As underlined by the NIHS, Ireland has embraced cultural diversity and this must be acknowledged byhealthcare professionals in order to ensure equality of access to health services.
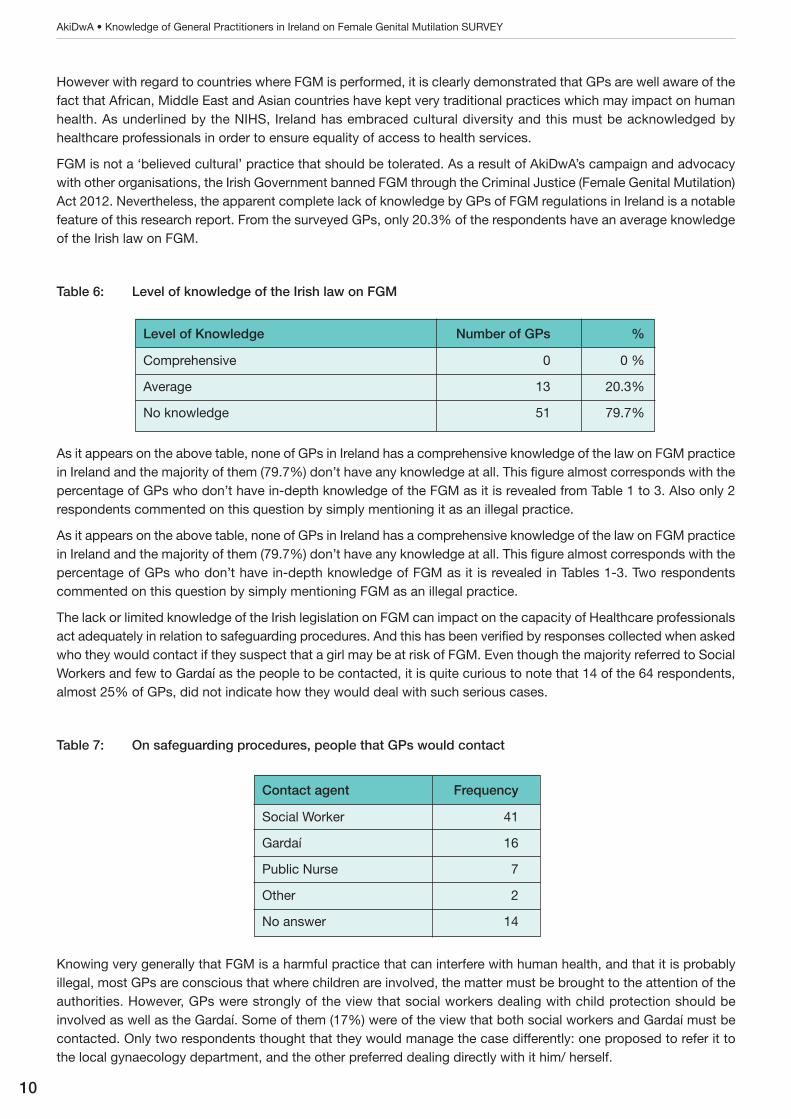
FGM is not a ‘believed cultural’ practice that should be tolerated. As a result of AkiDwA’s campaign and advocacywith other organisations, the Irish Government banned FGM through the Criminal Justice (Female Genital Mutilation)Act 2012. Nevertheless, the apparent complete lack of knowledge by GPs of FGM regulations in Ireland is a notablefeature of this research report. From the surveyed GPs, only 20.3% of the respondents have an average knowledgeof the Irish law on FGM.
Table 6: Level of knowledge of the Irish law on FGM
10
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY
Contact agent Frequency
Social Worker 41
Gardaí 16
Public Nurse 7
Other 2
No answer 14
As it appears on the above table, none of GPs in Ireland has a comprehensive knowledge of the law on FGM practicein Ireland and the majority of them (79.7%) don’t have any knowledge at all. This figure almost corresponds with thepercentage of GPs who don’t have in-depth knowledge of the FGM as it is revealed from Table 1 to 3. Also only 2respondents commented on this question by simply mentioning it as an illegal practice.
As it appears on the above table, none of GPs in Ireland has a comprehensive knowledge of the law on FGM practicein Ireland and the majority of them (79.7%) don’t have any knowledge at all. This figure almost corresponds with thepercentage of GPs who don’t have in-depth knowledge of FGM as it is revealed in Tables 1-3. Two respondentscommented on this question by simply mentioning FGM as an illegal practice.
The lack or limited knowledge of the Irish legislation on FGM can impact on the capacity of Healthcare professionalsact adequately in relation to safeguarding procedures. And this has been verified by responses collected when askedwho they would contact if they suspect that a girl may be at risk of FGM. Even though the majority referred to SocialWorkers and few to Gardaí as the people to be contacted, it is quite curious to note that 14 of the 64 respondents,almost 25% of GPs, did not indicate how they would deal with such serious cases.
Table 7: On safeguarding procedures, people that GPs would contact
Knowing very generally that FGM is a harmful practice that can interfere with human health, and that it is probablyillegal, most GPs are conscious that where children are involved, the matter must be brought to the attention of theauthorities. However, GPs were strongly of the view that social workers dealing with child protection should beinvolved as well as the Gardaí. Some of them (17%) were of the view that both social workers and Gardaí must becontacted. Only two respondents thought that they would manage the case differently: one proposed to refer it tothe local gynaecology department, and the other preferred dealing directly with it him/ herself.
Level of Knowledge Number of GPs %
Comprehensive 0 0 %
Average 13 20.3%
No knowledge 51 79.7%
FGM is a sensitive, hidden and private issue. It is therefore very difficult to identify whether or not it is occurring inIreland. Currently there is no evidence of the practice happening here. AkiDwA is engaged in an on-going awarenessraising programme, and in the training of healthcare professionals, to enable a better understanding of the issue andto ensure future generations are fully protected from this barbaric practice.
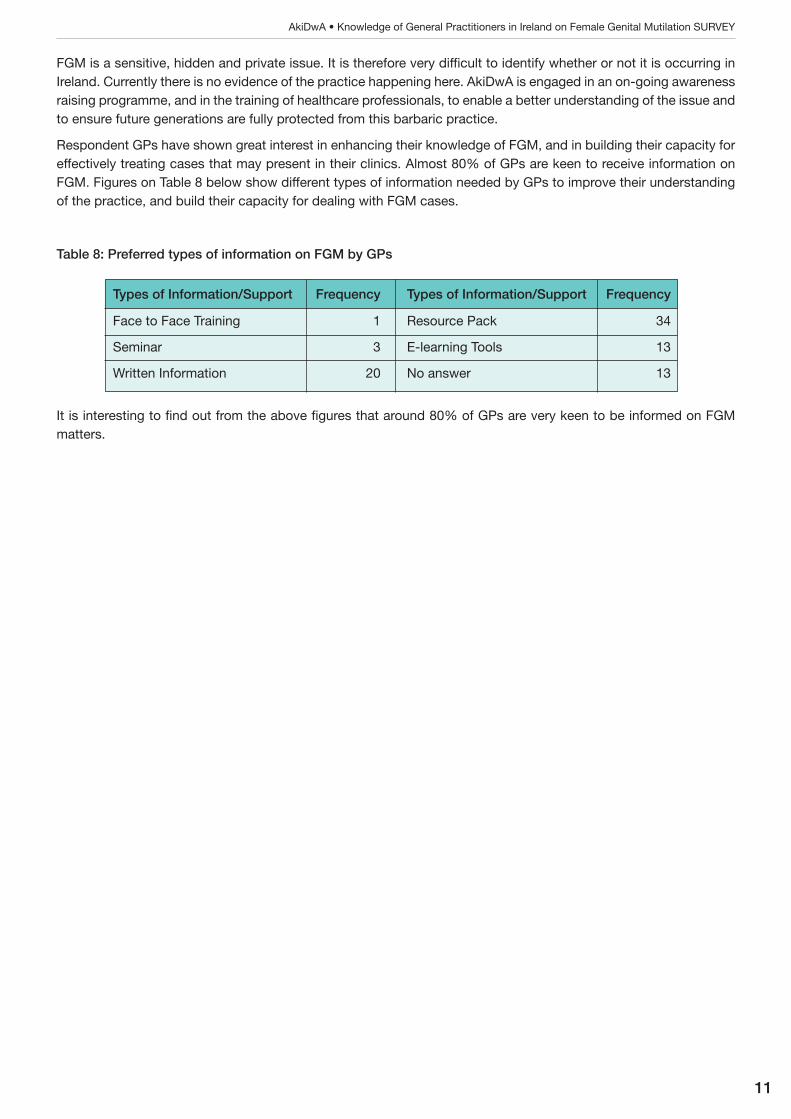
Respondent GPs have shown great interest in enhancing their knowledge of FGM, and in building their capacity foreffectively treating cases that may present in their clinics. Almost 80% of GPs are keen to receive information onFGM. Figures on Table 8 below show different types of information needed by GPs to improve their understandingof the practice, and build their capacity for dealing with FGM cases.
Table 8: Preferred types of information on FGM by GPs
11
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY
Types of Information/Support Frequency Types of Information/Support Frequency
Face to Face Training 1 Resource Pack 34
Seminar 3 E-learning Tools 13
Written Information 20 No answer 13
It is interesting to find out from the above figures that around 80% of GPs are very keen to be informed on FGMmatters.

III. Conclusion
In the past fifteen years or so, Ireland has become an increasingly diverse multicultural society. This is reflected inthe 2002 Census where for the first time a question on nationality was included. The 2011 Census revealed that12% of the population is comprised of people born abroad. For this reason the HSE adopted a National InterculturalHealth Strategy in 2007 to address equality in accessing healthcare for all citizens living in Ireland. Among thosecitizens, over 2% came from Africa, the Middle East and Asia, all places where FGM is practiced (CSO 2012).
Immigration is indeed a recent phenomenon in Ireland. According to Gilmartin, 1996 marked the first year of asustained period of net in-migration to Ireland, which lasted until 2009 (Gilmartin, 2012). This explains the lack ofexperience of service providers when dealing with issues related to the immigrant population, which FGM is one ofthe most prominent as the results of the survey reveal.
After leading a campaign to protect migrant women and children from FGM, and to support victims, AkiDwA identifiedGPs as key players, being the first point of contact for most victims.
In general eleven points questioned the knowledge of GPs on FGM, its prevalence in Ireland, its effects on womenand girls, the related law or regulation, the referral pathways and safeguarding procedures. The overwhelming majorityof GPs who participated in the survey are not aware of FGM related issues and keen to up-skill in this area.
As both the Ireland Health Intercultural Strategy 2007-2012 and the Ireland’s National Plan of Action to AddressFemale Genital Mutilation have reached the planned years of implementation, the present survey is an importantpiece of research that would enhance the need of building capacity of healthcare service providers, especially theGeneral Practitioners, on issues that impact on the health of immigrants which the Female Genital Mutilation is oneof the most preponderant.
12
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY
IV. Recommendation
Based on findings through this survey and in line with health related policies for the immigrant population living inIreland as well as best model of practice in other European countries, the following recommendations are made:
• Organisations must work with communities not only in dissuading parents from countries where FGMis practised from continuing this inhuman custom, but also in encouraging women who were subjectedto the practice to inform their GPs.
• Information and training materials should be developed to support GPs and other healthcareprofessionals up skilling on healthcare issues specific to immigrant communities, specifically on FGM.
• As part of an Intercultural Health Module, FGM should be mainstreamed as a subject in the curriculumfor University students in Medicine. Provision should also be made for training all medical doctors,healthcare professionals, social workers, counsellors, Gardaí etc.
• Ireland needs to establish a One Stop Clinic for provision of services to the victims of FGM that wouldbe based in one of the existing maternity hospitals. This kind of initiative will make the referral pathwaystraight forward and easier for women to access.
• A co-ordinated approach is needed in addressing FGM to ensure that awareness raising programmeson the issue reach as wide an audience as possible. Similarly, a co-ordinated approach is needed tomonitor the effectiveness of the legislation prohibiting FGM.
• An Induction or welcoming pack that includes information on FGM should be made available to all newimmigrants arriving in the country.
• In order to achieve the HSE, NIHS and the NAP recommendations, work on FGM needs to be properlyresourced.
13
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY

V. References
- AKIDWA (2012), We Lived to Tell, Migrant Women’s Personal Experiences of Domestic Violence,Ireland, 23p.
- AKIDWA (2008), Female Genital Mutilation, Information for Health-Care Professionals Working inIreland, 24p.
- AMNESTY INTERNATIONAL (2009), End FGM, European Campaign run by Amnesty InternationalIreland in partnership with NGOs. [online] Available at: http://www.endfgm.eu/en/ [Accessed 1February 2013].
- BELIEFS & ISSUES (2011), Female Genital Mutilation, Information for Health & Child ProtectionProfessionals. [online] Available at: http://www.fgm.co.nz/beliefs-and-issues [Accessed 31 January2013]
- CSO (2012), Profile 6. Migration and Diversity. [online] Available at:http://www.cso.ie/en/media/csoie/census/documents/census2011profile6/Profile%206%20Migration%20and%20Diversity%20entire%20doc.pdf [Accessed 31 January 2013]
- DAPHNE, Ireland’s National Plan of Action to Address Female Genital Mutilation. Ireland, 23p.
- DUNSMUIR, W.D., & GORDON, E.M (1999), The history of Circumcision, in BJU International, Vol. 83,Suppl. 1, pp. 1-12. [online] Available at: http://www.cirp.org/library/history/dunsmuir1/ [Accessed 31January 2013]
- GILMARTIN, M (2012), The changing landscape of Irish migration, 2000-2012, in NIRSA, n. 69.[online] Available at:http://www.nuim.ie/nirsa/research/documents/WP69_The_changing_face_of_Irishmigration_2000_2012.pdf. [Accessed 31 January 2013]
- HSE, National Intercultural Health Strategy 2007-2012. [online] Available at:http://www.hse.ie/eng/services/Publications/services/SocialInclusion/National_Intercultural_Health_Strategy_2007_-_2012.pdf [Accessed 20 January 2013]
- Irish Medical Directory, The Directory of Irish Healthcare, 2012-2013.
- RECEPTION AND INTEGRATION AGENCY (RIA), http://www.ria.gov.ie/en/RIA/Pages/2011_Statistics
- THE ROYAL COLLEGE OF MIDWIVES, Female Genital Mutilation: Report of a Survey on Midwives‘views and knowledge. [online] Available at:https://www.google.ie/search?q=The+Royal+College+of+Midwives%2C+Female+Genital+Mutilation%3A+Report+of+a+Survey&rlz=1C1AFAB_enIE496IE499&oq=The+Royal+College+of+Midwives%2C+Female+Genital+Mutilation%3A+Report+of+a+Survey&aqs=chrome.0.57.43959&sourceid=chrome&ie=UTF-8 [Accessed 20 January 2013]
- WHO (2012) Female Genital Mutilation, Fact sheet n. 241, February 2012. [online] Available at:http://www.who.int/mediacentre/factsheets/fs241/en/ [Accessed 21 January 2013]
- WHO (2008) Eliminating female genital mutilation: an interagency statement. Geneva: World HealthOrganization; 2008. [online] Available at:http://whqlibdoc.who.int/publications/2008/9789241596442_eng.pdf [Accessed 22 January 2013]
14
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY
VI. Appendix
FGM Survey Questions
1. Please indicate in what capacity you are responding to this survey
GP nn Practice Manager nn Other (please specify) nn
2. Do you know what is FGM?
Yes nn No nn
3. Would you be able to identify different types of FGM?
Yes nn No nn
4. Have you seen women or girls in your practice who have undergone FGM?
Yes nn No nn
b) If yes, state how many:
5. What symptoms or complications do they present with?
Physical Complications nn Psychological/emotional nn
Other (please specify) nn
6. Do you have referral pathways for providing support/ information to FGM client?
A. If yes, please explain:
B. if not would you be interested to get a referral list? Yes nn No nn
Comments:
7. What do you think the prevalence of FGM is here in Ireland?
500 nn 1000 nn 3000 nn 5000 nn
8. In which of the following countries / areas is FGM practised?
Africa nn Asia nn Middle East nn All of the above nn
9. What is your level of knowledge of the Irish law on FGM?
No knowledge nn Average nn Comprehensive nn
Comment:
10. Safeguarding procedures – who would you contact if you suspect that a girl may be at risk of FGM?
Gardaí nn Public Health Nurse nn Social-worker nn
11. Would you be interested in receiving any of the following on FGM as an individual or for your staff?
Face to face training nn Seminars nn Written information nn Resource pack nn
E learning Tools on FGM nn if yes please write your email here:
Please use space below if you have any further comment.
Please use the enclosed envelope to send back the questionnaires.
THANK YOU!
15
AkiDwA • Knowledge of General Practitioners in Ireland on Female Genital Mutilation SURVEY

Unit 2, Killarney Court, Upper Buckingham Street, Dublin 1, Republic of Ireland.Telephone: (+1 353) 01 834 9851 • Mobile: (+353 86) 309 6859 • E-mail: [email protected] • Visit: www akidwa.ie


![Collaborative Knowledge Translation: Application of a Wiki Model for Primary Care Practitioners [4 Cr2 1530 Shachak]](https://img.dokumen.tips/doc/110x75/55c073c1bb61ebdb158b45a0/collaborative-knowledge-translation-application-of-a-wiki-model-for-primary-care-practitioners-4-cr2-1530-shachak.jpg)


























