Embed Size (px)
Citation preview

Klinische Onkologie
• Abschnitte der Tumortherapie– Induktionstherapie
• Meist intensive Therapie bis zur CR– Konsolidierungstherapie
• Therapie nach CR zur CR-Verlängerung– Erhaltungstherapie
• Wenig intensive Dauertherapie– Salvage Therapie
• Zweit- oder Drittlinientherapie , meist experimentell– Rezidivtherapie
Klinische Onkologie
• Kombination von Therapiemodalitäten, wenn synergistische oder additive Effekte zu erhoffen sind
• Adjuvante Therapie– Systemische Therapie im Anschluß an „kurative“
chirurgische (R0-Resektion) Tx• Neoadjuvante Therapie
– Systemische Therapie vor Lokaltherapie• Additive Therapie
– Kombination von Chemo- und Strahlentherapie, sequentiell oder kombiniert („sensitizing“)

Klinische Onkologie
• Klinische Studien– Phase I
• Ermittlung der MTD einer Substanz oder eines Schemas, die bei Probanden zu reversiblen Nebenwirkungen (max Grad III/IV nach WHO) führt
– Phase II• Ermittlung der Wirksamkeit an einem kleinen
Patientenkollektiv– Phase III
• Vergleich der Wirksamkeit mit der etablierten Standardtherapie

Klinische Onkologie
• Klinische Studien: „Good Clinical Practice“• Regelt die Rechte von Probanden nach der
Deklaration von Helsinki• Regelt die Durchführung von klinischen Studien und
die Dokumentationspflichten• Standardisierung des Reporting
– SV=Survival oder OS=overall survival– FFTF=freedom from treatment failure– DFS=disease free survival– RFS=relapse free survival– Intent to treat analysis (Vollständigkeit der Analyse!!!!)

Gesamtüberleben alle Patienten (n = 959)2x2 armige Studie (1999-2000)
Auswertung 05/2000
CHOP-21 (n=232) CHOEP-21 (n=244)CHOP-14 (n=238)CHOEP-14 (n=245)
M o n a t e4035302520151050
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.10.0
COX-Modelrel.
Risikop
Etoposid 0.7 0.0314 d 0.7 0.03Etoposidund 14 d
1.3 0.25

Klinische Onkologie
• Nebenwirkungen von Tumortherapien– Substanz- und prozedurspezifisch– Dosisabhängig (in der Regel)– Rationale für kombinierte Systembehandlungen
(Auswahl von Medikamenten mit nicht-identischem NW-Spektrum
• Graduierung nach– WHO-Klassifikation– NCI-C Klassifikation– Bearman Klassifikation für Hochdosistherapie– ARO Klassifikation für Strahlentherapie

Klinische Onkologie
• Therapieverfahren in der Onkologie– Lokale Therapieverfahren
• Chirurgie• Strahlentherapie
– Systemische Therapieverfahren• Chemotherapie• Antikörpertherapie• Targeted Therapie• Hormontherapie• Immuntherapie

12
Tumor cellnumber
Skippers Modell des Tumorwachstums

Klinische Onkologie
• Wirkungsmechanismus der Chemotherapie– Erhöhte Empfindlichkeit gegenüber zytotoxischen
Substanzen (Zytostatika) von Tumorgewene vs Normalgewebe
– Kombination, zeitliche Abfolge, Applikationsmodus und supportive Maßnahmen schonen nichtmalignes Gewebe
– Zytostatika wirken• Phasenspezifisch (G1, S, G2, M)• Zyklusspezifisch auf alle proliferierenden Zellen• zyklusunabhängig

Klinische Onkologie
• Klassen von Zytostatika– Alkylanzien: Aktivierung im Organismus; Vernetzung der
DNA, phasenunspezifisch– Interkalatoren/Anthrazykline/Topoisomerase II Ihibitoren
Klasse I: zellzyklusspezifisch , Konformationsänderung der DNA, Membrantoxizität
– Antimetabolite: Folsäure, Basenantagonisten. Zyklusspezifisch; Hemmung von Enzymen oder falscher Baustein
– Mitosehemmstoffe: Spindelgifte– Epipodophyllotoxine: G2-Phasenhemmung durch Blockade
der Topoisomerase (Reparaturenzym)
Klinische Onkologie
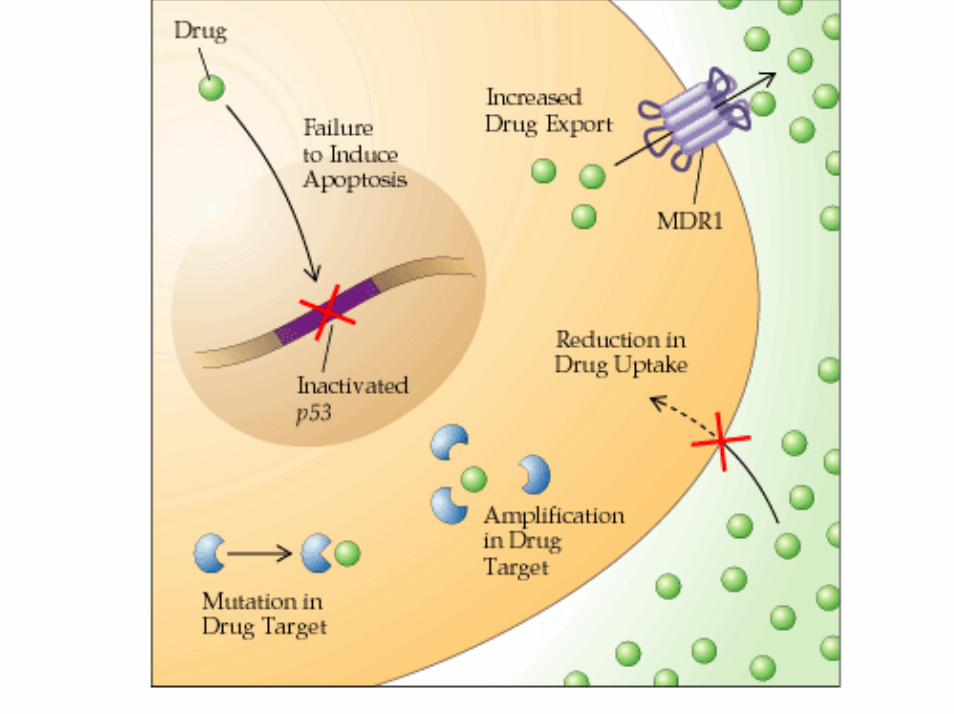
• Mechanismen der Zytostatikaresistenz– Temporäre Resistenz
• Dormancy = G0-Zellen• %-Satz bestimmt Empfindlichkeit gegenüber Chemo
– Primäre Resistenz• Chemonaive Zellen – ca 1 auf 100.000 – 1.000.000
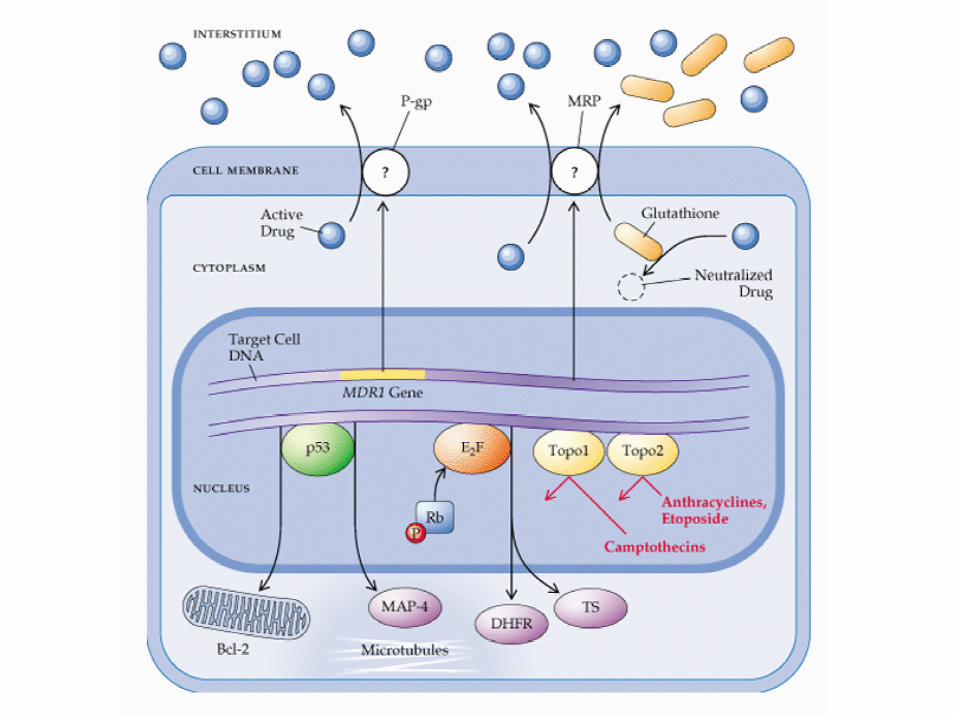
– Sekundäre Resistenz• Entsteht nach Exposition• Erhöhter Efflux: MDR-1 Gen induziert• Ungenügende Aktivierung• Genamplifikation von Bindungsproteinen• Induktion von DNA-Reparaturmechanismen

Klinische Onkologie
• Prinzipien der Polychemotherapie– Dient der Optimierung der Chemotherapie– Ist heute Standard in der Behandlung – Prinzip
• 1. Früher Beginn• 2. Hoher Einzelzell-Kill• 3. Frühe Wiederholung• 4. Damit hohe Dosis pro Zeit• 5. ? Chronobiologische Optimierung• 6. Einsatz mehrerer unterschiedlich wirkender Substanzen• 7. Kombination unterschiedlicher Nebenwirkungsspektra!

Cyclophosphamid (Endoxan®)
i.v. oder p.o., 90% BioverfügbarkeitElimination über MetabolisierungHWZ 4-8 hTox: KM-Tox, Alopezie, Lunge, Leber, Haut, Blase (hämorrhagische Zystitis) (Abbau!)First pass Effekt in der Leber, p450 Aktivierung
IndikationImmunsuppression, akute lymphatische Leukämie, CLL, NHL, solide Tumore
Cytarabin -Alexan®Pyrimidinantagonist (Antimetabolit)i.v., i.m. s.c.MetabolisierungHWZ biphasisch, 10 Min und 2 StdTox: KM-Tox, Mukositis, Diarrhoe, pulmonal, Konjunktivitis,Alexan-Syndrom mit Fieber, Myalgie, Knochenschmerzen, Hautausschlag
Ind.: akute Leukämien, MDS, Lymphome (2nd line)

Doxorubicin - Adriblastin®
Interkalator-Substanz (Anthrazyklin/Topo II Inh. I
Streng i.v. (Paravasat!!!)Resistenz: MDR-Amplifikation, Verminderung der Topo-II-AktivitätElimination biliär, Metabolisierung hepatisch
HWZ triphasisch: 12 min, 30 min, 3 Std
Tox: Herzmuskel, KM-Tox, Alopezie
Ind.: solide Tumore (Mammaca., SCLC), Leukämien, Lymphome, Sarkome
Methotrexat, Permetrexat, Alimta
Antimetabolit (kompetitiver Hemmer der DHFR), Gabe von Folin-Säure antagonisiert Wirkung
i.v.,i.m., i.th., p.o.Elimination: renal, wenig MetabolisierungTox: Hand-Fuß Syndrom, Mukositis, KM, Diarrhoe, Leber
Ind.: akute lymphatische Leukämie, agressive Lymphome, menigealer Befall durch alle Tumore
Klinische Onkologie
• „Supportivtherapie“ bei Chemotherapie– Antiemese
• Risikofaktoren = emetogene Potenz• Akutes vs. Verzögertes Erbrechen• Med: Serotoninrezeptorantagonisten, Neuroleptika, Corticosteroide
– Schmerztherapie• Ursachenabklärung
– Tumorbedingt, tumorassoziiert, Therapiefolge, begleitende
– Prophylaxe von Infektionen• Antibiotika, G-CSF
– Psycho-Onkologische Unterstützung

Cis Platin
CisplatinDNA-Interkalator: Reaktion mit Guanin und Adenosin, Induktion von Strangbrüchen, protrahierte S-Phase, G2 Arresti.v.Metabolisierungüber die NiereTox: KM-Tox mäßig, Nephrotoxizität, Ototoxizität, Neurotoxizität, Übelkeit
Ind.: alle große Tumore, Ausnahme Colonkarzinome (Oxaliplatin) 2nd oder 3rd line Lymphome
Paclitaxel - Taxol®
Paclitaxel, DocetaxelMitosehemmstoff/Spindelgifti.v. Über die Niere
Tox: KM-Tox, Hypersensitivitätsreaktion, Neurotoxizität, Kardiotox(Rhythmusstörungen), Ergüsse, Ödeme, capillary leak, Myalgie/Athralgie
Ind.: alle große Tumoren (außer Kolonkarzinome)
Antibody-Based TherapyPart 1: Basic Principles
Table of Contents:
• Monoclonal Antibodies (moAbs)• Mechanisms
– Immune Mobilization • Antibody – Dependent Cell Mediated Cytotoxicity (ADCC)• Complement – Dependent Cytotoxicity (CDC)
– Apoptosis– Cytokine-Fusion Antibodies– Antibody-Radionuclides– Antibody-Toxins

Antibodies are ImmunoglobulinMolecules
Heavy chainLight chain
Fc
Fab
Ant
igen
bin
ding
Med
iate
s bi
olog
ic a
ctiv
ity
CH2
CH3
Carbohydrates
VH
CH1
VK
CK
Complement binding region
Binds to Fc receptor
Hypervariableregions
Hinge



Monoclonal Antibodies
Mouse MoAb
Chimeric Ab
Humanized Ab
scFv(single chain
Fragment variable)
Fab-fragment

Monoclonal Antibodies Nomenclature (suffix)
• Murine antibody: “momab”
• Chimeric antibody: “ximab”
• Humanized antibody: “zumab”

BispecificBispecificBispecific MonoclonalMonoclonalMonoclonal AntibodiesAntibodiesAntibodies(((BsAbsBsAbsBsAbs)))
QuadromaHybrid-Hybridoma
scFv-Diabody
F(ab´)2Fragment
Mouse MoAb

From Murine to Reshaped MoAbs
Murine Chimeric Humanized Human
% Murine Protein 100% ≈25% <5% 0%HAMA Induction +++ + + -
Half-life short long long longEffectiveness in ADCC
++ +++ +++ ND

Mechanisms of Action
MTTCMTTCMTTC

Monoclonal Antibodies: Mechanisms of MoAbs
Immune Mobilization: Effector cells (ADCC) & Complement (CDC)
Induction ofApoptosis
Radiation/Radionuclide
Toxin/Drug
Target cell
Synergy of cytokine-MoAb
with Chemotherapy
MTTCMTTCMTTC
© PW Dec 2002
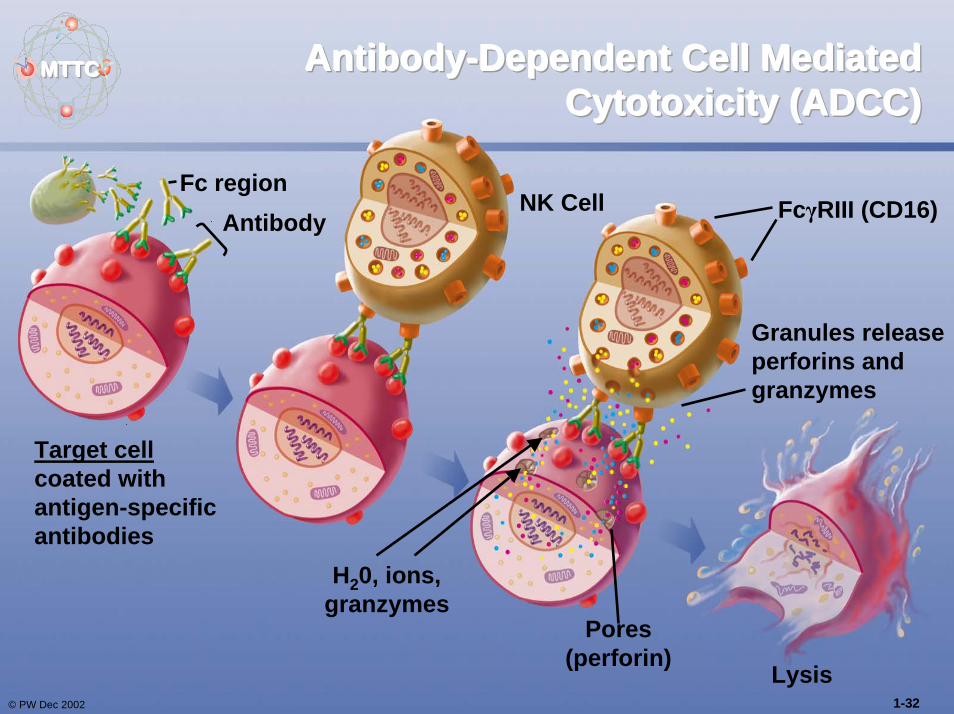
AntibodyAntibodyAntibody---Dependent Cell Mediated Dependent Cell Mediated Dependent Cell Mediated Cytotoxicity (ADCC)Cytotoxicity (ADCC)Cytotoxicity (ADCC)
Fc region
Target cell coated with antigen-specific antibodies
AntibodyNK Cell FcγRIII (CD16)
Granules release perforins and granzymes
Pores(perforin)
H20, ions,granzymes
Lysis1-32

MTTCMTTCMTTC ComplementComplementComplement---Dependent Cytotoxicity Dependent Cytotoxicity Dependent Cytotoxicity (((CDC)CDC)CDC)
Antibody
C1 ComplexC1rC1sC1q
Antigen
Target cell
Pores (C9s proteins)
H2O
Lysis© PW Dec 2002 1-33

ApoptosisApoptosisApoptosisMTTCMTTCMTTC
Antibody
Antigen
Macrophage
© PW Dec 2002 1-34

Importance of Antigen Density
• The clinical effect is often related to the intensity of antigen expression
HER2/neu
Trastuzumab
Strong HER2/neuexpression only
CD20 Rituximab Major activity in FCC and MCL and less active in CLLCD52 Alemtuzum
abCLL, T-cell NHL, and T-PLL

Monoclonal Antibodies: Mechanisms of MoAbs
Immune Mobilization: Effector cells (ADCC) & Complement (CDC)
Induction ofApoptosis
Radiation/Radionuclide
Toxin/Drug
Target cell
Synergy of cytokine-MoAb
with Chemotherapy

Immunocytokines (ICs) are MoAbs Combined with
Cytokines• Deliver immunomodulating molecules specifically to the tumor.
• Initiate tumor cell lysis (e.g. by ADCC or CDC).
• Liberate additional tumor-associated antigens (TAA).
• Induce specific T-cell response against the target antigen and additional TAAs (antigen spreading and immunological memory).

Preclinical Experience for IC Therapy: Combination IC &
Chemotherapy• Cyclophosphamide and huKS-IL-2 in a 4T1/KSA
murine mammary tumor lung metastases assay.
0
0,1
0,2
0,3
0,4
0 mg/kg 15 mg/kg 40 mg/kg
Cyclophosphamide
Ave
rage
Tum
or B
urde
n (g
)
- huKS-IL-2+ huKS-IL-2
Holden SA et al. Clin Can Res 2001; 7: 2862-2869.

Monoclonal Antibodies: Mechanisms of MoAbs
Immune Mobilization: Effector cells (ADCC) & Complement (CDC)
Induction ofApoptosis
Radiation/Radionuclide
Toxin/Drug
Target cell
Synergy of cytokine-MoAb
with Chemotherapy

Prinzip der Toxizität von Strahlentherapie/RadionuklidtherapRadio-Immuntherapie

Monoclonal Antibodies: Mechanisms of MoAbs
Immune Mobilization: Effector cells (ADCC) & Complement (CDC)
Induction ofApoptosis
Radiation/Radionuclide
Toxin/Drug
Target cell
Synergy of cytokine-MoAb
with Chemotherapy

CD
33 P
E
FSC
SSC
CD34 FITC
AML mit hoher CD33 Expression

Gemtuzumab Ozogamicin (GO): Putative Mechanism of Action
C CD33 Antigen
hP67.6=α-CD33
C
C C
C C
CC
C CCell
DeathC=calicheamicin:anthracyclin, binding to minor groove Dand inducing double strand breaks
Hydrolysis of Cintracellularly

Antitumorale Immuntherapie –Suche nach dem idealen
Zielantigen
• Expression auf Tumorzellen - nicht auf normalen Zellen
• Relevanz für Zellfunktion und Zellüberleben
• Tumor spezifisches Antigen vs. Antigen-Überexpression

Epidermal Growth Factor Receptor (EGFR) Expression in
KarzinomenÜberexpression assoziiert mit:
• Invasion und Metastasierung
• Fortgeschrittenem Stadium
• Schlechter Prognose
• Resistenz gegen Radio- / Chemo- / Hormontherapie
70-100Kopf-Hals
50-90Lunge14-91Mamma40-70Prostata35-60Ovar
80-100Niere30-80GIT
Überexpr. (%)
Tumor

Die EGFR (erbB) FamilieEGF
TGFα
Cystein-reicheDomänen (EZD)
Tyrosin KinaseDomäne
HER1ErbB-1EGFR
HER2/neuErbB-2
HER3ErbB-3
HER4ErbB-4
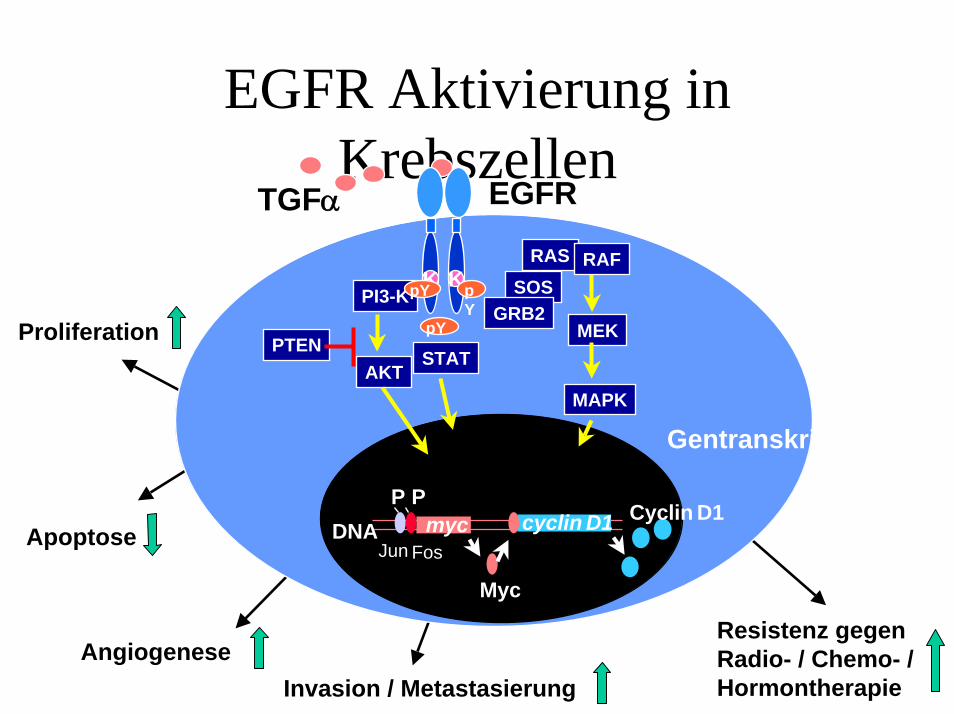
EGFR Aktivierung inKrebszellen
Apoptose
Angiogenese
TGFα
Proliferation
Invasion / Metastasierung
MAPK
MEK
Gentranskription
PI3-K
RAS RAFSOS
GRB2
AKTSTAT
KpY
pY
K
DNA myc
Myc
cyclin D1 Cyclin D1
Jun Fos
P P
PTEN
EGFR
pY
Resistenz gegenRadio- / Chemo- /Hormontherapie

Kombination mit Radio- / Chemotherapie
• Radio- / Chemotherapie aktiviert EGFR in Krebszellen (Apoptoseprotektion)
• Blockade von EGFR – Unterstützung konventioneller Behandlung durch z.B. Apoptoseinduktion
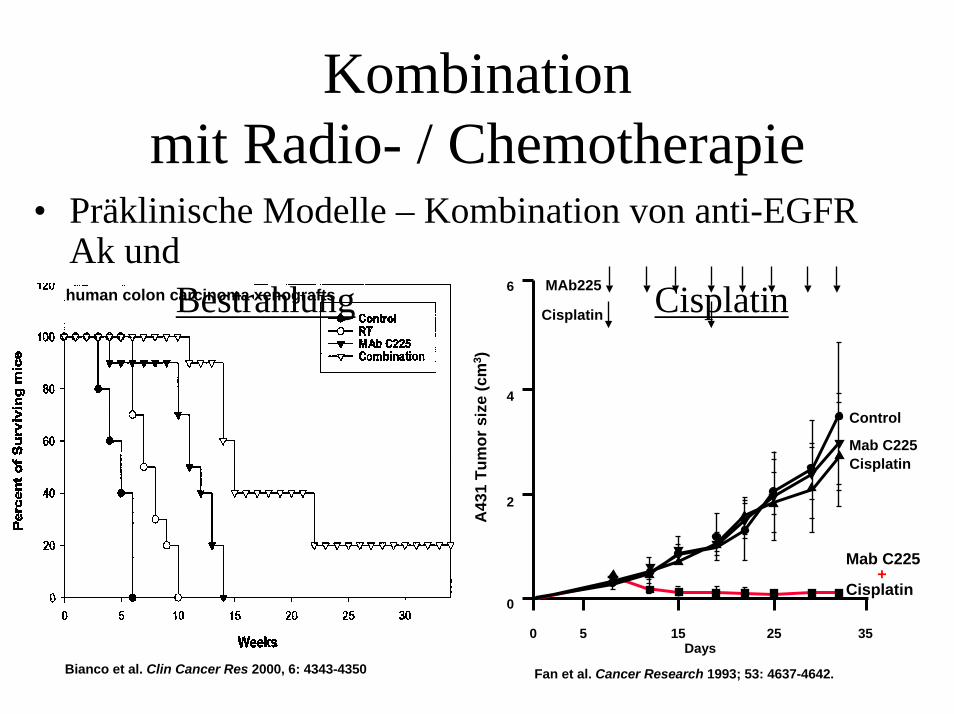
Kombination mit Radio- / Chemotherapie
• Präklinische Modelle – Kombination von anti-EGFR Ak und
Bestrahlung Cisplatin
Mab C225+
Cisplatin
6
4
2
0
0 5 15 25 35Days
A43
1 Tu
mor
siz
e (c
m3 )
MAb225
Cisplatin
Control
Mab C225Cisplatin
Fan et al. Cancer Research 1993; 53: 4637-4642.Bianco et al. Clin Cancer Res 2000, 6: 4343-4350
human colon carcinoma xenografts





























