Embed Size (px)
Citation preview
Kingston Exam ReviewOrthopedics
Tom Green MD. MSc. FRCPC, Dip Sports Med
(CASEM)
Emergency Medicine and Sports Medicine
Royal Columbian HospitalAllan McGavin Sports Medicine Clinic
University of British Columbia
What will we cover
• Not a comprehensive review of everything!!!
• Prioritizing your biggest resource: TIME!!!
• Some General exam tips from someone not too too far out.
• What ortho to expect on exam day.
• The Ortho Chapters
• Representative written questions and Visual Stim
2
My General Exam Tips:
There is a lot to cover– Don’t get bogged down in the details– Don’t over think it.
High vs. Low Yield– Discuss in study group
Where are the lists??– Each page of Rosen’s– review till your eyes hurt
On exam day– Don’t get hung up on low yield effort.– Taking a hit on a few questions is ok.– Questions have multiple parts.
Orthopedics in the study year
• 239 pages out of 2511 pages of Rosen’s• Thats 9.5%
• 2 weeks in our study schedule • early in the year!!!
• Strategies to re-review• X-ray visual stim• Quick snappers
Resources = Rosen’s• Rosen’s and Tint are where the money is.
• Ortho is well covered.–Good for fractures and major complications–So so for soft tissue, rehab, common complications of minor
injury
• Not the most realistic in the real “Canadian” world.–Lots of consults and MRIs.
• Lags behind evidence.–Not much new in ortho, but things evolve–Open Fractures, Clavicle, Achilles, Scaphoid, AC separation
• Other Texts which are pretty good–Harris and Harris: Radiology of Emergency
Medicine–Simon and Sherman: Emergency Orthopedics
Orthopedics on Exam Day
• On the exam: 4-6 Questions??
• Where are you going to see ortho:
–Visual Stim / Written / Parts of oral
• Anatomy: common injuries in commonly injured bones– ie: Label the x-ray or Rosen’s diagram
• Indications for surgical consult• Complications of common injuries• Associated injuries: ie: ongoing pain in ankle sprain
LOOK CAREFULLY
• Is this a non accidental pattern.• Is this a pathologic injury.• Patterns associated with significant injury
• Potential big miss.• Ortho question on an oral exam!!!• Don’t trip over the lifeline
Exam Day StrategyAm I Missing Something??
• Each section has potential subtle findings• lipohemarthrosis / talar dome / hand and foot
bones......
• Highest Yield chapter• Questions likely to have portion from this chapter• Lots of lists in boxes and text.
• Fracture descriptions and Eponyms (CAREFUL HERE)
• Complications
• Associated Injuries
• Salter Harris
• Open Fractures
• Splinting Basics
Chapter 49: General Principles
General Principles
The HandChapter 50: hand
• Information overload.–Acceptable angles etc.....–+++ text
Higher Yield• Flexor and extensor tendon anatomy• Zones of extensor tendons• Ligamentous injuries: ie: Skiers thumb• Tenosynovitis (Kanavel’s signs)
Also High Yield• Amputations and Avulsions
Wrist and ForearmChapter 51: Wrist and Forearm
• Common on exams (and in practice)
• Types of fractures• Normal Anatomy and Acceptable
reductions• Criteria for distal radius reduction• Pediatric radius fractures• Carpal ligamentous instability
• DISI / VISI
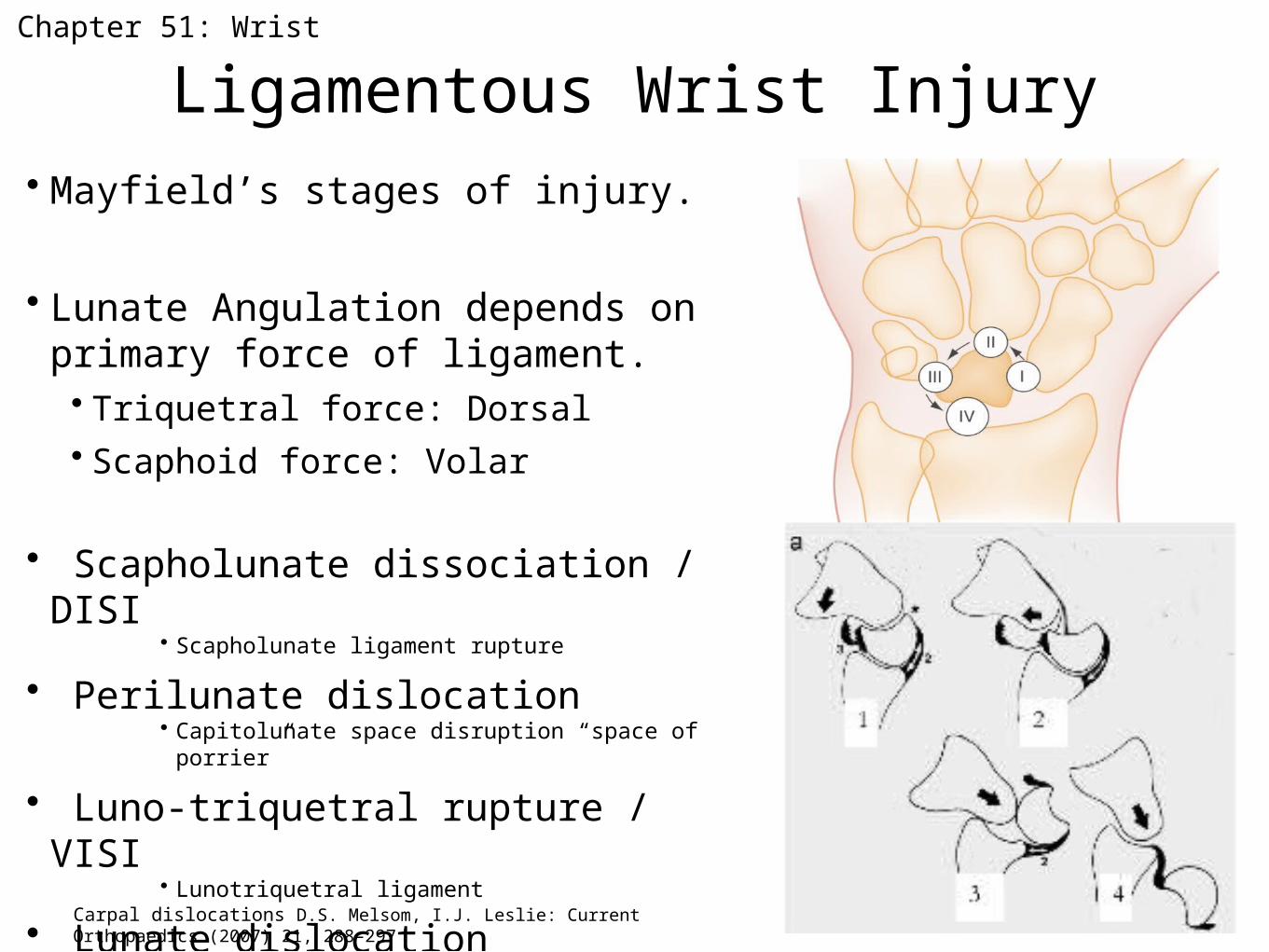
Ligamentous Wrist Injury• Mayfield’s stages of injury.
• Lunate Angulation depends on primary force of ligament.• Triquetral force: Dorsal• Scaphoid force: Volar
• Scapholunate dissociation / DISI• Scapholunate ligament rupture
• Perilunate dislocation• Capitolunate space disruption “space of porrier”
• Luno-triquetral rupture / VISI• Lunotriquetral ligament
• Lunate dislocation• Dorsal Radiolunate ligament
Chapter 51: Wrist
Carpal dislocations D.S. Melsom, I.J. Leslie: Current Orthopaedics (2007) 21, 288–297
When the wrist x-ray looks normalCommon missed or subtle injuries
• Scaphoid fracture
• Dorsal Triquetral• Ligamentous injury–Ligamentous carpal instability: stages 1-4–VISI, DISI
• In real life and maybe on the exam:–Can always splint and get follow-up............
or CT.
Chapter 51: Wrist
Elbow
• Neurovascular anatomy and risk with fractures and dislocations.
• Supracondylar fractures: highest yield
• Midshaft Humerus fractures
• Radial Head fractures
• Pulled Elbow
• Most other elbow fractures require ortho consult
–Less you can ask about on exam.
Chapter 52: Humerus and Elbow
ShoulderChapter 53: Shoulder
• Dislocation–Types
–Reduction method (tough question to ask)
• AC separation grades and management.
• Clavicle fractures.–Surgical indications
• Good practical info on soft tissue injuries.–Lower yield on exam, but high yield at work
• Rehab!!!!
Back Pain• Low Yield Chapter for Exam Prep
• This edition is well written • decent summary of approach.
Chapter 54: MSK Back Pain
Key Points
• Indications for plain films in low back pain• Plain films vs. Advanced imaging?
• RED FLAGS
Pelvis• High Yield• Lots of lists in this chapter
• Oral Exam!!!–More likely ortho for oral exam??–Decisions in trauma management.• ie: angio vs OR
• Label the Anatomy!!!
• Classification of Pelvic Fractures–Tile / Young & Burgess
• Trauma management
Chapter 55: Pelvis
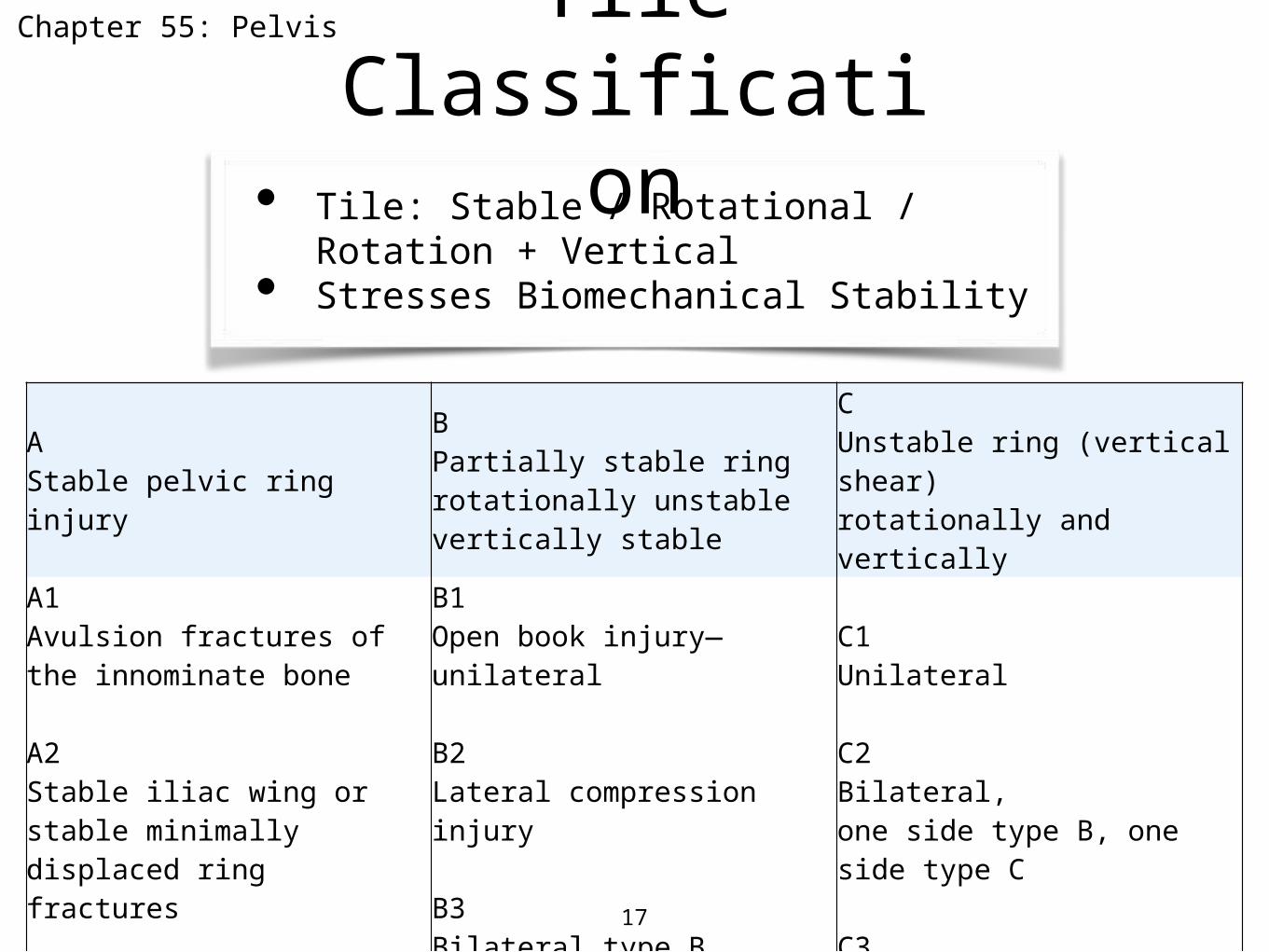
Tile Classification
17
AStable pelvic ring injury
BPartially stable ringrotationally unstablevertically stable
CUnstable ring (vertical shear) rotationally and vertically
A1Avulsion fractures of the innominate bone A2Stable iliac wing or stable minimally displaced ring fractures
A3Transverse fractures of the coccyx and sacrum
B1Open book injury—unilateral B2Lateral compression injury B3Bilateral type B injuries
C1Unilateral C2Bilateral, one side type B, one side type C C3Bilateral type C lesions
• Tile: Stable / Rotational / Rotation + Vertical
• Stresses Biomechanical Stability
Chapter 55: Pelvis
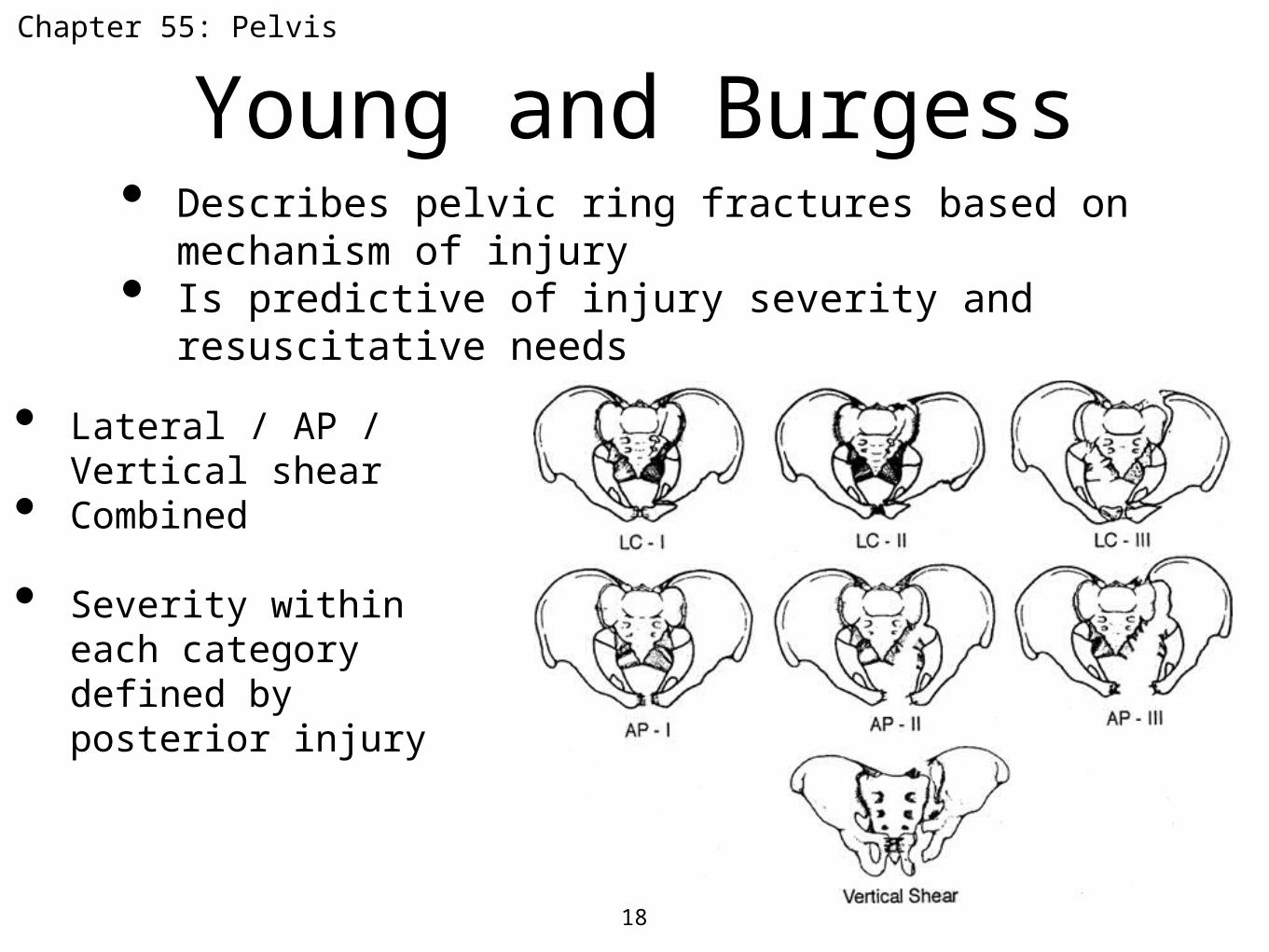
Young and Burgess
18
• Lateral / AP / Vertical shear
• Combined
• Severity within each category defined by posterior injury
• Describes pelvic ring fractures based on mechanism of injury
• Is predictive of injury severity and resuscitative needs
Chapter 55: Pelvis
When the x-ray looks normal
Hard to see
–Acetabular fractures.
Chapter 55: Pelvis
• Displaced ramus fractures.
• Sacral foramina asymmetry.
• Sacral lateral lip avulsion.
• Ischial spine avulsions.
• L5 transverse process.
Markers of posterior arch fractures
Femur and Hip High Yield
• Child with a limp!!!!!
• Hip fracture–Anatomy and blood supply–Femoral nerve block
• Femur Fractures
• Differential Diagnosis of Hip Pain without fracture.–Big and common sense list–Low Yield
• Dislocation –Techniques–management and complications.
Chapter 56: Femur and Hip
Knee and Lower Leg• Knee dislocation–Management–Risks / Investigations
• Soft Tissue Injuries and sports medicine injuries.
• When the x-ray looks normal–Effusion–Lipohemarthrosis–Tibial spine avulsion–Osteochondral lesion–Segond fracture–Arcuate sign
Chapter 57: Knee and Lower Leg
Ankle and FootLots of Good Questions
Chapter 58: Ankle and Foot
• Classification and mechanism of ankle fractures
• Management of ankle fractures (ie: surgery / cast)
• Ankle sprain and Differential diagnosis of sprain
• Foot: Lisfranc• Calcaneus fractures: x-ray visual stim
Ankle and FootWhen the x-ray looks normal
Chapter 55: Ankle and Foot
• Talar Dome• 5th MT
avulsion• Joint spaces • Mortise• Syndesmosis• Talar tilt• Calcaneus• Lisfranc
Summary
• Lists, lists, lists, lists, lists.......
• Don’t over think and over resource.
• Questions are multipart and there are lots of them
• Visual stim: keep your good x-rays.
• Anatomy of commonly injured joints
• Common soft tissue complications
• Is this a non accidental injury pattern
• When the x-ray looks normal
Thank You
If you have any questions.......about ortho
Tom Green





























