Embed Size (px)
Citation preview
546
A MirrorOF THE PRACTICE OF
MEDICINE AND SURGERYIN THE
HOSPITALS OF LONDON.
Nulla est alia pro certo noscendi via, nisi quam plurimas et morborum etdissectionum historias, tam aliorum proprias, collectas habere et inter se com-parare.—MORGAGNI. De Sed. et Cuus. Morb. lib. 14. Proœmium.
KING’S COLLEGE HOSPITAL.
THREE CASES OF EXCISION OF THE ELBOW-JOINT FOR DISEASIOF THE BONES, BY THE LONGITUDINAL INCISION; GOOD RE-COVERY IN EACH, WITH MOTION BY MEANS OF A NEW SPLINT.
(Under the care of Mr. FERGUSSON.)THE operation of excision of the elbow is one of constant oc-
currence, and with results almost invariably satisfactory, in sofar as saving the life of the patient and,the possession of use-ful arm, with good motion. This last condition cannot alwaysbe obtained, unless the joint is freely removed : we mean bythis expression, that the surgeon need not fear taking awayfrom the elbow more than mere slices of the ends of the bones,because anchylosis is not sought for; it is motion and flexibilitythat are required. There have been several cases of excisionof the elbow-joint, of recent occurrence, all of which have
turned out well. We saw Mr. Henry Thompson perform ex-cision upon an elderly man, on the 14th of October, at Univer-sity College Hospital, and Mr. Birkett, at Guy’s, on the 20thof October. The subject of Mr. Birkett’s case was a boy whohad an attack of pleuro-pneumonia fourteen months ago, witheffusion into the chest, and disease of the elbow of four months’duration. Three weeks after the operation the wound hadalmost entirely healed up. We saw Mr. Thompson’s patient onthe llth instant, and found the wound nearly healed, not asinus remaining. The injury to this man’s arm was inflictedby a lunatic, and was associated afterwards with constant pain.The result in Mr. Ure’s patient, a notice of whose elbow beingexcised has already appearedinour "Clinical Records, wasverysatisfactory, Mr. Ure remarking upon the rapidity with whichthe wound had healed up. This case we give on the presentoccasion. The single longitudinal incision employed, althoughpractised by Parke upwards of fifty years ago, is especiallysuitable in these cases, the edges of the wound often healing byadhesion, without the great collections of pus which we are inthe habit of seeing sometimes when the H incision is employed.The elbow of a Lascar, aged thirty, was excised for disease
on board of the Dreadaoug7at, by Mr. Tudor, with good results.Mr. Le Gros Clarke performed the same operation upon a boy,aged fifteen years, at St. Thomas’s Hospital, on the 23rd ofMay, for disease of a year’s standing. The little fellow didwell. At St. Bartholomew’s Hospital, Mr. Coote excised theelbow of a soldier, aged twenty-eight, for disease of eightyears’ standing. A single long incision was made; the re-
covery was good. And, lastly, Mr. Hillman, at the West-minster Hospital, submitted a little boy, three years old, toexcision, on the 7th of July last, and a good recovery has beenmade.The limits of our space prevent us giving all these and some
other valuable cases in detail. We are contented, for the pre-sent, to refer to them; but we record three instances of ex-cision of the elbow, in King’s College Hospital, in which a newform of splint, invented by Mr. Christopher Heath, has beenused with marked benefit, in effecting motion after the processof healing was nearly completed. After all, this is really theimportant desideratum of the operation; for a stiff arm is auseless appendage, and to obtain a flexible elbow, containingno joint, great attention must be paid to ea1’ly passive motion.Mr. Heath’s instrument seems to prevent the bones cominginto close contact, and yet permits of flexion and extension,and is now in general use in this hospital.The notes of the three following cases were kindly furnished
to us by Mr. W. P. Swain, house-surgeon to the hospital :-CASE 1.—Margaret W—, aged twenty-one, admitted into
No. 3 Ward, May 9th, 1857, with disease of the right elbow- Ijoint. The patient is a native of Maidstone, where she had I
been in service; has never been very strong; and about twelvemonths ago had a glandular abscess in the neck, which is stillopen. About six months ago, without any previous injury,the right elbow began to swell, and became so painful that shewas unable to move the joint. Fomentations and linimentswere used without any relief. The joint became more tender;and, in the month of April, an abscess burst a little below theexternal condyle of the humerus, where an ulcer still remains.The arm continuing swollen and immovable, she was advisedto come to King’s College Hospital. On admission: she is a
pale, delicate-looking young woman. On the neck are thescars of some scrofulous ulcers; there is considerable enlarge-
’
ment of the right elbow; the arm is bent at a very obliqueangle, and requires to be supported; there is some slight move-ment in the joint; the ulna can be pushed up against thehumerus, and slightly moved from side to side. About two
inches below the outer condyle of the humerus is a small ulcer,the size of a fourpenny-piece, which discharges a serous-lookingfluid; the skin covering the joint is red and shining. She com-plains of considerable pain in the joint, aggravated by move-ment.
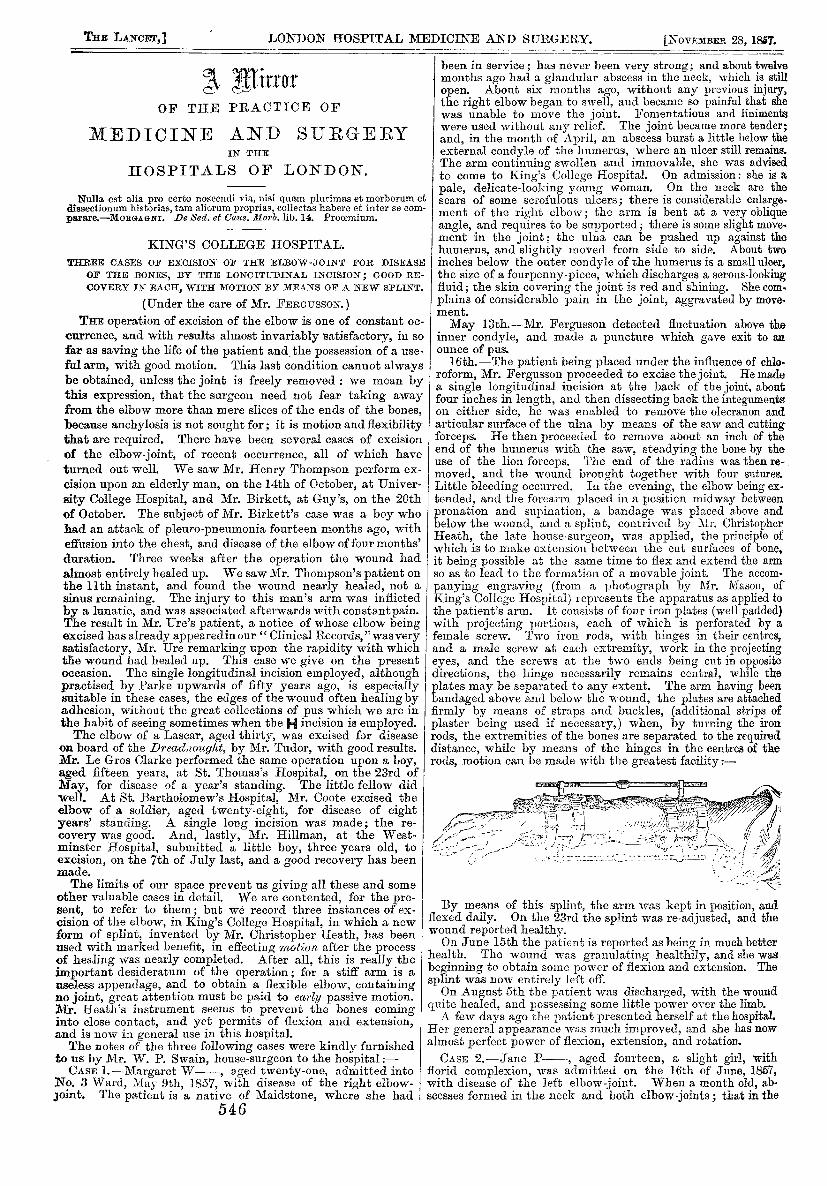
May 13th.--Mr. Fergusson detected fluctuation above theinner condyle, and made a puncture which gave exit to anounce of pus.16th.-The patient being placed under the influence of chlo-roform, Mr. Fergusson proceeded to excise the joint. He madea single longitudinal incision at the back of the joint, aboutfour inches in length, and then dissecting back the integumentson either side, he was enabled to remove the olecranon andarticular surface of the ulna by means of the saw and cuttingforceps. He then proceeded to remove about an inch of theend of the humerus with the saw, steadying the bone by theuse of the lion forceps. The end of the radius was then re-moved, and the wound brought together with four sutures.Little bleeding occurred. In the evening, the elbow being ex-tended, and the forearm placed in a position midway betweenpronation and supination, a bandage was placed above andbelow the wound, and a splint, contrived by Mr. ChristopherHeath, the late house-surgeon, was applied, the principle ofwhich is to make extension between the cut surfaces of bone,it being possible at the same time to flex and extend the armso as to lead to the formation of a movable joint. The accom-
panying engraving (from a photograph by Mr. Mason, of
King’s College Hospital) represents the apparatus as applied tothe patient’s arm. It consists of four iron plates (well padded)with projecting portions, each of which is perforated by afemale screw. Two iron rods, with hinges in their centres,and a male screw at each extremity, work in the projectingeyes, and the screws at the two ends being cut in oppositedirections, the hinge necessarily remains central, while theplates may be separated to any extent. The arm having beenbandaged above and below the wound, the plates are attachedfirmly by means of straps and buckles, (additional strips ofplaster being used if necessary,) when, by turning the ironrods, the extremities of the bones are separated to the requireddistance, while by means of the hinges in the centres of therods, motion can be made with the greatest facility.-
By means of this splint, the arm was kept in position, andflexed daily. On the 23rd the splint was re-adjusted, and thewound reported healthy.On June 15th the patient is reported as being in much better
health. The wound was granulating healthily, and she wasbeginning to obtain some power of flexion and extension. Thesplint was now entirely left off.On August 5th the patient was discharged, with the wound
quite healed, and possessing some little power over the limb.A few days ago the patient presented herself at the hospital.
Her general appearance was much improved, and she has nowalmost perfect power of flexion, extension, and rotation.CASE 2.-Jane P-, aged fourteen, a slight girl, with
florid complexion, was admitted on the 16th of June, 1857,with disease of the left elbow-joint. When a month old, ab-scesses formed in the neck and both elbow-joints ; that in the

547
right subsided, and perfect motion was obtained after a shortperiod; but the abscess in the left joint led to complete anchy-losis. The joint remained in a quiescent state up to five yearsago, when an abscess formed in its neighbourhood; this,however, subsided, and she experienced no inconvenience untila month before admission, when another abscess formed onthe inner side of the joint, which burst, and has continued todischarge ever since. The forearm is slightly flexed on thehumerus; the elbow is perfectly locked, very tender, andslightly enlarged. Just over the internal condyle there is anulcer about the size of a sixpence; through which a probe canbe-passed down to the bare bone. On the posterior surface ofthe joint, and on the outer side of the forearm, there are oldcicatrices.June 27th.-Dr. Snow having administered amylene, Mr.
Fergusson proceeded to excise the joint. Having made a ver-tical incision about six inches long at the back of the joint, hedissected back the integuments on either side, until the jointwas fully exposed. During this dissection no ulnar nervecould be discovered. He then applied the saw to the olecranonat its junction with the shaft of the ulna, and having sawnthrough the bone in that position, the saw was again appliedto. the humerus just above the condyles, and the piece of boneintervening between the two cuts removed. At this stage ofthe proceedings a large quantity of pus spirted out with greatforce from the neighbourhood of the joint. Some diseasedtissues, implicated in the abscess, were then dissected off. No
ligatures were required, and the edges of the wound werebrought together by two stitches.30th.-The patient having gone on very well during the
intervening days, the arm was placed in Mr. Heath’s splint(before described), and flexed once or twice upon the humerus.The bones were kept well apart from one another; but after atime the arm and hand became rather swollen, andOn July 3rd the splint was taken off, and the arm placed on
a straight splint.On the 7th, Heath’s splint was again applied and the arm
now and then flexed, the extension caused by the splint muchlessening the pain of that operation. The wound assumed a
healthy appearance, and the patient was in a very satisfactorystate.On the 20th, the wound was reported as "looking very
healthy," and at each dressing the arm was flexed and ex-tended, not much pain being inflicted.At the beginning of August the side splints were taken off,
and a straight splint in front of the joint was substituted. Thewound now scarcely discharged at all. The arm was flexed,extended, and rotated at each dressing. By the middle of themouth the patient had regained some power of motion in thefingers and wrist.On the 25th August the splint was left off, and the arm was
supported in a sling.About the second week in September, when she left the
hospital, the wound had almost closed. There was plenty ofmotion in the joint, and she could raise the hand to the head.CASE 3.-Wm. R—, aged twenty-six, a florid, robust-look-
ing man, was admitted on August 19th, 1857, with disease ofthe right elbow-joint. The patient states that up to about sixyears ago he has always enjoyed good health. About thattime he contracted syphilis, for which he was mercurialized.This was followed by an eruption, accompanied by pain in thelimbs and joints, more especially the right elbow and knee.Shortly after he found that his right elbow was swollen and
painful. This in about three months yielded to treatment,but he was never after able to place the limb in a perfectlystraight position, nor could he flex it sufficiently to touch theshoulder without great pain. In May last he had a return ofthe pain and swelling in the joint. This continued unabatedup to about five weeks ago, when an abscess formed in thejoint.On admission, the swelling was considerable about the elbow,
and the contour of the joint entirely lost. The forearm wasslightly flexed on the upper arm, and on pressing the forearmupwards a peculiar elastic feeling was given.Aug. 20th.--An incision was made midway between the
condyles of the humerus, and a considerable amount of offensivematter discharged itself. A probe introduced through thewound passes readily into the joint.30th.---The patient being placed under the influence of chlo-
roform, Mr. Fergusson proceeded to excise the joint. As inthe other cases, this was accomplished by making the verticalincision at the back of the joint. The ulnar nerve being care-fully hooked back and secured from injury, the humerua wassawn through just above the condyles, and the olecranon and
the head of the radius were also removed. Much bleedingoccurred during the operation.
Sept. 1st.—Heath’s splint was put on, and sufficient exten-sion made with it to separate the ends of the bones. Thewound looks healthy, and the patient suffers little pain.7th.-The arm was bent for the first time, and caused very
little pain.l0th.-The splint was removed to allow the swelling to de-
crease.
20th.-The splint was left off entirely, as it was thoughtthat the effect it had had in keeping the bones asunder wassufficient to secure perfect motion in the joint. The patientcan flex the arm a little himself, and with slight assistance canraise his hand to his mouth. The wound is looking veryhealthy, having closed up to a great extent in a surprisinglyshort period of time. The patient’s health is much improved,and a most favourable result is expected.
ST. MARY’S HOSPITAL.
EXCISION OF THE ELBOW-JOINT IN A BOY, FOR GENERAL DISEASEOF THE ARIICULATION; SPEEDY RECOVERY WITH A GOOD
ARM.
(Under the care of Mr. URE.)G. W-, aged thirteen, a boy with a fine, intelligent
countenance, good complexion, fair hair, and grey irides, wasadmitted on the 1st of August, 1857. About fourteen months
preceding, while playing with some lads, and jumping overone of their backs, he fell to the ground upon his left elbow;this was followed by swelling of the part. About a monthafterwards, he again fell upon the same elbow, whereupon anabscess formed at the seat of injury, and was laid open by asurgeon. The inflammatory swelling did not subside, and amonth or so before the date of his admission another abscessmade its appearance, which was also laid open; a third de-veloped itself the day after he entered the hospital. At thisperiod, the elbow was swollen, measuring nine inches and aquarter in circumference, while that of the other arm measuredseven inches and three-eighths; it was stiff and semi-flexed.Pain was experienced on pressing the olecranon. He also feltfrequent darting pain in the course of the arm. The surround-ing integument presented a reddish blush; there were threefistulous openings, evidently communicating with the joint,situate on the ulnar side of the elbow, each about an inch.apart, and from which a little sero-purulent fluid issued.
Before resorting to,excision, it was recommended, in consulta-tion, that a trial should be given to perfect rest of the affectedjoint. The arm was accordingly placed in an interruptedangular splint, which was well padded, and adjusted so as t()callow free egress to the secretion from the sinuous openings.The result of this plan of treatment, which was persevered infor a month, was some diminution of the swelling, but no de·cided improvement in other respects; and as the lad wassolicitous to be relieved of his painful infirmity, Mr. Ure per-formed the operation on the 2nd of September, the patienthaving been previously rendered insensible by chloroform.The edge of the knife was entered close to the outer margin
of the olecranon, and the linear incision prolonged directlyupwards and downwards, to an extent of about three inchesand a half. The integuments were dissected back, the in.sertion of the triceps muscle was divided, and the olecranonremoved with bone-nippers. The lateral ligaments were nextsevered, and the extremity of the humerus, being made to pro-trude from the wound, was cut off through the tuberositieswith bone-nippers. The head of the radius was then takenaway, and finally the remaining portion of the sigmoid cavityof the ulna. The operation was attended with very littlebleeding, and no vessels required to be tied. The edges of thewound were kept in apposition by five points of suture; a.
pledget of moist lint, and a bandage applied round the arm,which was bent at a right angle, completed the dressing. Asthe patient complained considerably of pain on awakeningfrom the effects of the chloroform, an opiate draught was ex-hibited.
It was ascertained on examination that the joint had con-tained pus, that there was pulpy degeneration of the synovialmembrane, erosion of the cartilages, a softened condition of theligamentous tissues, and what was most important, that thewhole of the morbid cartilaginous surface had been removed inthe operation.
Sept. 3rd.-Slept well; countenance cheerful; skin moistand cool; tongue clean; pulse 120; hand of the natural tempera-tnw hf makes no complaint excent when the limh happens tft