Embed Size (px)
Citation preview

Kidney International, Vol. 68 (2005), pp. 330–337
Kidney transplantation and wait-listing rates from theinternational Dialysis Outcomes and Practice PatternsStudy (DOPPS)
SUDITIDA SATAYATHUM, RONALD L. PISONI, KEITH P. MCCULLOUGH, ROBERT M. MERION,BJORN WIKSTROM, NATHAN LEVIN, KENNETH CHEN, ROBERT A. WOLFE, DAVID A. GOODKIN1,LUIS PIERA, YASUSHI ASANO, KIYOSHI KUROKAWA, SHUNICHI FUKUHARA, PHILIP J. HELD, andFRIEDRICH K. PORT
University Renal Research and Education Association, Ann Arbor, Michigan; Department of Surgery, University of Michigan, AnnArbor, Michigan; Nephrology, Uppsala Universitet, Uppsala, Sweden; Renal Research Institute, New York, New York; Amgen, Inc.,Thousand Oaks, California; Department of Biostatistics, School of Public Health, University of Michigan, Ann Arbor, Michigan;Hospital General, Vall d’Hebron, Barcelona, Spain; Jichi Medical School and Sashima Red Cross Hospital, Ibaraki, Japan; TheInstitute of Medical Sciences, Tokai University, Isehara, Kanagawa, Japan; and School of Medicine, Kyoto University, Kyoto, Japan
Kidney transplantation and wait-listing rates from the in-ternational Dialysis Outcomes and Practice Patterns Study(DOPPS).
Background. The international Dialysis Outcomes and Prac-tice Patterns Study (DOPPS I and II) allows description of vari-ations in kidney transplantation and wait-listing from nationallyrepresentative samples of 18- to 65-year-old hemodialysis pa-tients. The present study examines the health status and socioe-conomic characteristics of United States patients, the role offor-profit versus not-for-profit status of dialysis facilities, and thelikelihood of transplant wait-listing and transplantation rates.
Methods. Analyses of transplantation rates were based on5267 randomly selected DOPPS I patients in dialysis units inthe United States, Europe, and Japan who received chronichemodialysis therapy for at least 90 days in 2000. Left-truncatedCox regression was used to assess time to kidney trans-plantation. Logistic regression determined the odds of beingtransplant wait-listed for a cross-section of 1323 hemodialysispatients in the United States in 2000. Furthermore, kidney trans-plant wait-listing was determined in 12 countries from cross-sectional samples of DOPPS II hemodialysis patients in 2002 to2003 (N = 4274).
Results. Transplantation rates varied widely, from very lowin Japan to 25-fold higher in the United States and 75-foldhigher in Spain (both P values <0.0001). Factors associated withhigher rates of transplantation included younger age, nonblackrace, less comorbidity, fewer years on dialysis, higher income,
1Dr. Goodkin is currently working at ICOS Corporation, Bothell,Washington.
Key words: cadaveric kidney transplantation, end-stage renal disease,socioeconomic status, transplantation access, transplant wait-listing.
Received for publication February 4, 2004And in revised form August 18, 2004Accepted for publication January 27, 2005
C© 2005 by the International Society of Nephrology
and higher education levels. The likelihood of being wait-listedshowed wide variation internationally and by United States re-gion but not by for-profit dialysis unit status within the UnitedStates.
Conclusion. DOPPS I and II confirmed large variations inkidney transplantation rates by country, even after adjusting fordifferences in case mix. Facility size and, in the United States,profit status, were not associated with varying transplantationrates. International results consistently showed higher trans-plantation rates for younger, healthier, better-educated, andhigher income patients.
Patients who undergo kidney transplantation havelonger survival and better quality of life than patientson either hemodialysis or peritoneal dialysis [1–5]. Fur-thermore, the long-term cost of transplantation is lowerthan remaining on either dialysis modality [6].
The number of persons treated for end-stage renaldisease (ESRD) doubled during the last decade in theUnited States [7] and in Europe [8]. During that time,the number of patients on the United States transplantwaiting list increased 2.8-fold. At the end of 2001, the Sci-entific Registry of Transplant Recipients (SRTR) reportsthat 48,405 patients were on a kidney transplant waitinglist in the United States, while only 14,343 patients re-ceived a deceased donor kidney [9]. Similar discrepanciesbetween demand for and supply of organs are observedin other countries, too [8].
Despite a 30% increase in the number of transplantsperformed in the United States during the last 10 years,a strong need continues for greater organ availability, asindicated by the doubling from 1992 to 2001 in the annualnumber of patients who died while on transplant waitinglists. The demand for organs has outpaced supply [10].
330

Satayathum et al: International transplantation and wait-listing rates 331
Previous studies from the United States have evaluatedtransplantation rates by patient characteristics. Thesestudies have shown that blacks, women, and persons oflow socioeconomic status are less likely to receive kid-ney transplants [2, 11]. To better understand interna-tional trends in transplantation, the present analyses useddata from the Dialysis Outcomes and Practice PatternsStudy (DOPPS I and II) to describe patient characteris-tics and country variations in kidney transplantation ratesfrom representative samples of hemodialysis facilities inFrance, Germany, Italy, Japan, Spain, the United King-dom, and the United States. The present study also exam-ines the health status and socioeconomic characteristicsof patients in United States for-profit and not-for-profitdialysis facilities to explore access-to-care issues.
METHODS
The DOPPS is an international, prospective, observa-tional study of hemodialysis practice patterns and theirassociated outcomes. Data for the DOPPS I were col-lected from nationally representative samples of ran-domly selected dialysis facilities from Europe [101 facil-ities, 2320 adult patients (ages ≥18 years) from France,Germany, Italy, Spain, and the United Kingdom], Japan(65 facilities, 1651 patients), and the United States (145facilities, 4831 patients). Further details of the DOPPSdata collection protocol and study design have been de-scribed [12]. DOPPS II, which was initiated in 2002,includes the addition of Australia, Belgium, Canada,New Zealand, and Sweden to the study, bringing thenumber of facilities participating up to 340, from 308 inDOPPS I.
Excluded from most analyses here were patients witha previous transplant and patients who were older than65 years of age, since transplantation rates are very lowabove this age [4]. Laboratory measurements, demo-graphic factors, comorbidities, and treatment factors werecollected at patient entry into the study. Data collectionbegan in 1996 in the United States, 1998 in Europe, and1999 in Japan. Patients were replaced on an ongoing basisdue to death, transplantation, change in treatment modal-ity, withdrawal from dialysis, recovery of renal function,or transfer to another facility.
The kidney transplant wait-listing information wasavailable only for randomly selected United StatesDOPPS patients (N = 1323), 18 to 65 years of age, whowere receiving hemodialysis therapy for ESRD on June1, 2000, and who had been receiving maintenance dial-ysis for 90 days or more. The present study analyzedthe hemodialysis patient population because its data arereadily available from the DOPPS and because this pa-tient population represents approximately 90% of all pa-tients on the kidney transplant waiting list.
Statistical methods
Unadjusted transplant rates are reported here per 100patient years, for ages 18 to 65 and as a contrast for ages.A Cox proportional hazards regression, left-truncatedfor time since start of dialysis, was used to assess timeto kidney transplantation, with either a living or ca-daveric kidney donor. Patient-level characteristics andfacility-level practice patterns were examined in sepa-rate models. Models accounted for facility clustering ef-fects and were adjusted for age, race, sex, years withESRD, predialysis serum albumin, creatinine, phospho-rus, hematocrit, nursing home status, smoking status,hospital or nonhospital-based facility, education level,country, body mass index (BMI), 14 summary comor-bid conditions [coronary artery disease, congestive heartfailure, other cardiac disease, hypertension, cerebrovas-cular disease, peripheral vasculopathy disease, diabetesmellitus, lung disease, cancer (excluding skin cancer),gastrointestinal bleeding, neurologic disease, psychiatricdisease, recurrent cellulitis/skin disease, and human im-munodeficiency virus (HIV)/acquired immunodeficiencysyndrome (AIDS)], and yearly household income. Equiv-alent income categories were provided on the Euro-pean and Japanese questionnaires, based on UnitedStates monetary exchange rates in 1998 for Europe andexchange rates in 1999 for Japan. Facility-level analy-ses excluded patients with fewer than 90 days of expo-sure to facility practice patterns. Facility practice pat-terns that were examined included facility type (hos-pital vs. nonhospital-based) and size, and patient timewith a social worker. All models, except those pertainingto country rates, were stratified by country. Clusteringeffects were addressed with robust standard-error esti-mates based on the sandwich estimator [13].
Wait-listing results were restricted to patients receiv-ing hemodialysis for at least 90 days. This allowed suffi-cient time for health care providers to place patients on atransplant waiting list for a deceased donor kidney. All ofthe results were limited to hemodialysis patients 18 to 65years old, since over 85% of all kidney transplants are per-formed on people in this age group. Logistic regression—accounting for facility-clustering effects and adjusted fordemographics, unit type, United States geographic re-gion, years with ESRD, and 14 comorbid conditions—wasused to determine the odds of United States hemodialy-sis patients being on a kidney transplant waiting list. Allstatistical analyses were performed with SAS software,version 8.2 (SAS Institute, Cary, NC, USA).
RESULTS
Kidney transplantation rates
Differences by demographics. Table 1 shows the dis-tribution of hemodialysis patient baseline characteristics.The mean age among the 18- to 65-year-old patients was

332 Satayathum et al: International transplantation and wait-listing rates
Table 1. Relative rate (RR) of kidney transplantation by patient characteristics among patients 18 to 65 years of agea
Measure Patients% RR transplant P value
Age years18–34 11.8 2.44 <0.000135–49 31.5 2.02 <0.000150–65 56.7 1.00 Ref
RaceWhite 51.7 1.00 RefBlack 23.3 0.35 <0.0001Asian 20.9 0.65 0.05Other 4.12 0.57 0.001
GenderMale (vs. female) 59.6 1.15 0.07
Years with end-stage renal disease (per 1 year) — 0.94 <0.0001Comorbid conditions (present vs. not)
Coronary artery disease 28.7 0.79 0.03Congestive heart failure 27.0 0.73 0.005Hypertension 76.0 1.23 0.05Peripheral vasculopathy 16.9 0.61 0.001Diabetes mellitus 35.9 0.93 0.52Cancer (excluding skin) 6.1 0.57 0.003Psychiatric disease 23.0 0.68 0.0002Recurrent cellulitis/skin disease 7.2 0.48 0.003
Smoker 21.4 0.79 0.03Income in United States dollars (missing for 54%)
>$5000 15.3 0.98 0.91$5001–$10,000 25.8 1.00 0.98$10,001–$20,000 25.0 1.00 Ref$20,001–$40,000 21.6 1.40 0.01$40,001–$75,000 9.0 1.36 0.08>$75,000 3.4 2.62 <0.0001
Education levelLess than high school 30.6 0.81 0.06High school or some college 39.8 1.04 0.66College graduate 29.6 1.00 Ref
In Nursing Home (vs. not) 2.8 0.21 0.03
aRelative rate adjusted for all factors, years on hemodialysis (see Fig. 1), and for country. Total number of patients from all seven Dialysis Outcomes and PracticePatterns Study (DOPPS) I countries = 5267.
49.5 years (not shown). Men made up 60% of the sample,52% were white, 23% black (mostly in the United States),and 21% Asian (19% living in Japan, 2% in the UnitedStates). Of the patients in the sample, 36% had diabetesmellitus and 76% had hypertension. In the sample, 21%of the patients were smokers, and 3% lived in a nursinghome.
Table 1 also provides relative rates of transplantation.Transplantation was inversely associated with age, withpatients 18 to 34 years old having a 2.4-fold higher rateof transplantation than patients 50 to 65 years old. Blackand Asian patients received kidney transplants at sub-stantially lower rates than white patients. Kidney trans-plantation rates tended to be higher for men (RR = 1.15,P = 0.07) than women, although this result was not signifi-cant. Patients with a comorbid condition [coronary arterydisease, congestive heart failure, peripheral vasculopa-thy, cancer (excluding skin), psychiatric disease, or recur-rent cellulitis/skin disease] had significantly lower rates oftransplantation than patients without one of the comor-bid conditions. Patients with diabetes mellitus also had alower rate of transplantation, although the result was notsignificant. Patients with hypertension had a significantlyhigher rate of transplantation (RR = 1.23, P = 0.05)
than those without hypertension. However, this associa-tion with hypertension is largely explained by the adjust-ment for cardiovascular disease, diabetes mellitus, and/orperipheral vasculopathy, since removing the adjustmentsubstantially reduces the RR. The relative rate of kid-ney transplantation was significantly higher for groupswith higher income and education levels. For instance,patients whose incomes exceeded $75,000 (USD) had a2.6-fold higher rate (P < 0.0001) of receiving a transplantthan patients with incomes between $10,001 and $20,000(USD). Patients with less than a high school–level educa-tion had less of a chance of transplantation (RR = 0.81, P= 0.06) than those with a college degree or higher. Therewas no significant difference in the chance of transplan-tation for those with a high school degree or some collegeversus those with a college degree or higher. Smokers hada 21% lower chance of transplantation (RR = 0.79, P =0.03) than nonsmokers. Nursing home patients displayeda nearly fivefold lower rate of kidney transplantation (RR= 0.21, P = 0.03) than those who did not live in nursinghomes. Patients with fewer than 3 years of ESRD therapyhad approximately a twofold higher rate of transplanta-tion than did patients with 6 or more years of dialysis(Fig. 1).

Satayathum et al: International transplantation and wait-listing rates 333
9.08.07.06.05.04.03.02.01.00.0U
nadj
uste
d tr
ansp
lant
rat
e,pe
r 10
0 pa
tient
yea
rs
0-0.9 1-2.9 3-5 6-8 9-11 12-14 15-17 18-20 21-23 >23Years on hemodialysis
8.5
6.9
5.4
3.5 3.6 4.0
2.83.5
2.5 2.7
Fig. 1. Unadjusted transplantation rate byyears on hemodialysis for ages 18 to 65 years.
25
20
15
10
5
0SP UK FR GE IT US JA SP UK FR GE IT US JA
Country
22
1311
6 6 6
0.4
32
0.2 1.0 .2 10.0
Age >65 years
N = 6290
Age 18-65 years
N = 9123
Cru
de k
idne
y tr
ansp
lant
rat
epe
r 10
0 pa
tient
-yea
rs
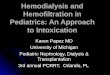
Fig. 2. Crude kidney transplant rates forhemodialysis patients in the Dialysis Out-comes and Practice Patterns Study (DOPPSI), 1997 to 2001, by age group. Abbreviationsare: SP, Spain; UK, United Kingdom; FR,France; GE, Germany; IT, Italy; US, UnitedStates; JA, Japan.
Table 2. Adjusted relative rate of kidney transplantation by country
Country RR Transplant P value 95% CI
France 1.52 0.004 (1.15, 2.01)Germany 0.79 0.23 (0.54, 1.16)Italy 0.84 0.39 (0.57, 1.24)Japan 0.04 <0.0001 (0.02, 0.09)Spain 3.04 <0.0001 (2.22, 4.16)United Kingdom 1.45 0.04 (1.02, 2.05)United States 1.00 Ref Ref
Restricted to patients aged 18 to 65 years (N = 5267). Relative rates fortransplantation were estimated by Cox proportional hazards regression, left-truncated for time since start of dialysis and adjusted for age, race, sex, years withend-stage renal disease (ESRD), predialysis serum albumin, serum creatinine,serum phosphorus, hematocrit, nursing home status, yearly household income,smoking status, hospital or nonhospital-based facility, education level, country,body mass index (BMI), and 14 summary comorbidities. Analyses accountedfor facility clustering effects.
Differences by country. Figure 2 illustrates the crudekidney transplantation rates by two age groups and bycountry. Overall, those who were over 65 years oldhad substantially fewer transplants than those 65 andyounger. Table 2 provides the adjusted relative rateof kidney transplantation by country for those whowere 18 to 65 years old. France, Spain, and the UnitedKingdom had higher rates of transplantation than the
United States, whereas Japan was found to have the low-est rate of transplantation among the seven countriesstudied.
Differences by facility characteristics. Transplantationrates varied widely by dialysis facility. Excluding agesabove 65 years, the majority of dialysis facilities (51.8%)had crude transplantation rates of fewer than 5 per 100patient-years, 25.4% had rates of 5 to 10 per 100 patient-years, and 23.8% had transplantation rates of 10 to over40 per 100 patient-years. No pattern of association withtransplantation rates could be observed by facility size.Furthermore, the facility practice of more frequent rou-tine assessments by social workers was not associatedwith significantly increased rates of transplantation. Apattern of large United States geographic regional vari-ation in kidney transplantation was seen after the analy-ses were adjusted for regional differences in patient age,sex, race, 14 summary comorbid conditions, incident (i.e.,new to dialysis) patients, facility clustering, and unit type(Fig. 3). These adjusted analyses indicated 2.4-fold higherodds of hemodialysis patients receiving a transplant inthe Mountain region than patients in the Western SouthCentral region (P ≤ 0.01).

334 Satayathum et al: International transplantation and wait-listing rates
2.0RR
1.5
1.0
0.5
0.0
Mou
n
N = 16
5
W N
Centra
l
N = 20
4 New E
ng
N = 95
E NCen
tral
N = 38
3 Mid
Atl
N = 58
3
E SCen
tral
N = 28
7PA
C
N = 55
2
S Atl
N = 12
26
W S
Centra
l
N = 56
1
1.60 1.551.36
1.23 1.17 1.07 1.000.73 0.66
P = 0.
09
P = 0.
24Ref
P = 0.
77
P = 0.
41
P = 0.
31
P = 0.
27P =
0.05
P = 0.
03Fig. 3. Effects of United States geographicregion on relative rate (RR) of kidney trans-plantation. Analysis included only UnitedStates Dialysis Outcomes and Practice Pat-terns Study (US-DOPPS) point-prevalentsample (June 1, 2000) and only patients whowere <65 old (N = 1323). RR is relative rateof transplantation from Cox model, adjustedfor patient age, sex, race, 14 summary comor-bid conditions, incident (i.e., new to dialysis)patients, facility clustering, and unit type. SeeAppendix for which states fall under each ge-ographic region shown.
Table 3. Percentage of hemodialysis patients on kidney transplantwaiting lists (2002 and 2003)
DOPPS Sample number Kidney transplantCountry (N) waiting list%
Japan 884 10United States 1129 24Sweden 258 28France 182 34Belgium 201 35Australia/New Zealand 274 36Canada 290 39Italy 253 39Germany 300 40Spain 254 48United Kingdom 249 55
Dialysis Outcomes and Practice Patterns Study II prevalent cross-section,hemodialysis patients ages 18 to 65 years.
Kidney transplant wait-listing
Differences by country and United States geographic re-gion. The DOPPS studied 12 countries in 2002 and 2003,with nationally representative hemodialysis facilities andpopulations by country. Table 3 shows the percentage ofpatients aged 18 to 65 years on kidney transplant waitinglists. There was large variation in the percentages of pa-tients on waiting lists, ranging from 10% in Japan to 55%in the United Kingdom.
The United States data indicated that, for hemodial-ysis patients aged 18 to 65 years, the percentage of pa-tients placed on kidney transplant waiting lists variedmore than 2.5-fold across nine geographic regions, rang-ing from 13% in the Eastern South Central region to 33%in New England (Fig. 4).
Differences by age and race in the United States. TheDOPPS examined the likelihood of hemodialysis patientsbeing placed on a kidney transplant waiting list, based ontheir age (18 to 65 years old) and race. Kidney transplantwait-listing was found to decline significantly with age(adjusted OR = 0.66 for every 10 years older, P < 0.001).Furthermore, wait-listing was significantly lower for black
hemodialysis patients (adjusted OR = 0.59, P = 0.007)than white. A significantly lower odds (P < 0.05) of wait-listing was also seen for patients with congestive heartfailure, lung disease, or cancer (other than skin cancer).These analyses were adjusted for gender, United Statesregion, 14 comorbid conditions, unit type, and years withESRD.
Hospital units and for-profit versus not-for-profit dial-ysis units in the united States. National data from theCenters for Medicare and Medicaid Services (CMS) in-dicated that, for year 2000, 80% of United States dialysisunits were freestanding and 20% were hospital-based.Furthermore, 85% of the freestanding units were cate-gorized as for-profit units and 15% as not-for-profit. TheDOPPS used data from the CMS Provider files along withdata collected from each participating DOPPS dialysisunit to evaluate the variation in kidney transplant wait-listing according to dialysis unit type. As shown in Table4, the percentage of patients on a kidney transplant wait-ing list was 16% in not-for-profit units, 23% in for-profitunits, and 26% in all other units, including hospital-basedunits. After detailed adjustment for differences in facilityclustering, United States region, age, sex, race, incident(i.e., new to dialysis) patients, and 14 summary comorbidconditions, the likelihood of patients being placed on akidney transplant waiting list did not significantly differamong those treated in the three types of dialysis units.
DISCUSSION
The observed lower likelihood of black hemodialysispatients than white hemodialysis patients being placedon a kidney transplant waiting list is corroborated bydata from the SRTR. In year 2000, for approximately116,000 ESRD patients aged 18 to 65 years, the SRTRshowed that the fraction of black patients placed on a kid-ney transplant waiting list was 31% lower than for whitehemodialysis patients. The DOPPS analyses expandedon this observation by adjusting for a large number of

Satayathum et al: International transplantation and wait-listing rates 335
AOR*2.0
1.5
1.0
0.5
0.0
New E
nglan
d
N = 39 E N
Centra
l
N = 15
2 Pacific
N = 15
9
W N
Centra
l
N = 41 M
id Atla
ntic
N = 16
8 Mou
ntain
N = 56
W S
Centra
l
N = 19
1 S Atla
ntic
N = 43
6
E SCen
tral
N = 81
33 31 28 28 24 22 19 17 13
1.56* 1.53*1.34 1.22
1.06 0.970.77
0.59* 0.56
*P≤0.05
Fig. 4. Adjusted odds ratio (AOR) of beingon a kidney transplant waiting list, by UnitedStates census region, ages 18 to 65 years. Point-prevalent sample (June 1, 2000) (N = 1,323).Adjusted OR compared to United States na-tional average, adjusted for facility clustering,unit type, United States regional demograph-ics, years on hemodialysis, and 14 summarycomorbid conditions, compared with nationalaverage. Numbers in bars indicate percentageof patients on waiting list. See Appendix forwhich states fall under each geographic regionshown.
Table 4. Odds of being on a kidney transplant waiting list by unit type
% Patients on kidney Adjusted ORa of beingUnit type Patient number (N) waiting-list (unadjusted) on kidney waiting list (95% CI) P value
For-profitFreestanding 842 23 1.00 Ref
Not-for-profitFreestanding 125 16 1.11 (0.54, 2.24) 0.78
All others 356 26 1.10 (0.64, 1.95) 0.69
Analysis included United States-Dialysis Outcomes and Practice Patterns Study (US-DOPPS) point-prevalent sample (June 1, 2000) of hemodialysis patients, aged18 to 65 years, receiving chronic maintenance dialysis for 90 days or more.
aAdjusted odds ratio model was adjusted for differences in facility clustering, United States region, age, sex, race, incident (i.e., new to dialysis) patients, and 14summary comorbid conditions (N = 1323).
comorbid conditions. The DOPPS results pertaining tokidney transplantation and associated sociodemographicfactors showed that, independent of income and educa-tion, blacks again were less likely than whites to receivetransplants. Prior studies have shown that black patientshave disproportionately lower transplantation and wait-listing rates than whites [14–18]. Potential factors thatmay account for lower transplant rates among blacks in-clude attitudinal and interpersonal issues (e.g., less par-ticipation in medical decision making and less trust inphysicians and the medical establishment [6, 11, 15]). Ad-ditionally, there is the possibility that medical teams donot communicate transplant benefits to minorities, thepoor, or uneducated as well as they do to others. Wolfe etal [14] have shown that significantly lower rates of trans-plantation in wait-listed blacks and Asians compared withwhites are explained in part by physiologic factors of dis-tributions of human leukocyte antigen (HLA) B typesand blood groups. Roberts et al [19] found that HLAtypes explain 7% of the 33% difference in transplanta-tion rates between black and white patients. This level ofadjustment does not come close to explaining either thedifferences Wolfe et al found or the differences foundin this paper. Blood type, rare HLA types, and early ormultiple wait-listing also do not explain the differencebetween black and white patient transplantation rates[2].
Results from the DOPPS indicate that after adjustmentfor numerous patient characteristics, Spain had the high-est relative rate of kidney transplantation while Japan hadthe lowest. A comparison of transplant rates reportedby country registries indicates a similar pattern: Spain(11.2 transplants per 100 dialysis patients [20]), UnitedKingdom (9.3 transplants per 100 dialysis patients [21]),United States (5.2 transplants per 100 dialysis patients[22]), Germany (4.1 transplants per 100 dialysis patients[23]), Italy (4.0 transplants per 100 dialysis patients [24]),and Japan (0.3 transplants per 100 dialysis patients [25]).
Many factors could account for the international dif-ferences seen among kidney transplantation rates. Thesocioeconomic, religious, cultural, and political nature ofa country may play a large role in influencing the num-ber of donors from a population and the patient view oftransplantation itself [26]. For instance, it may be thatJapan’s relatively low transplantation rate potentially re-flects medical ethics rooted in tradition, which affectsoutlooks on life, death, and the concept of brain death[27]. Spain’s relatively high transplantation rate, on theother hand, could owe to its national policy of presumedconsent for organ donation and its higher use of organsfrom older donors with adequate histology, among otherfactors [28]. Overall, the DOPPS results confirmed largevariations in terms of kidney transplantation rates bycountry, even after adjusting for differences in case mix.

336 Satayathum et al: International transplantation and wait-listing rates
Previous studies have reported that, on average,younger, healthier patients, and those with higher socioe-conomic status, had higher transplantation rates than oth-ers [16–18]. The DOPPS showed similar results and pro-vides detail by specific comorbid conditions. Althoughthe association of certain medical conditions—such asheart disease, vascular disease, cellulitis, cancer, and psy-chiatric disease—with significantly lower transplantationrates may not be unexpected, it is of interest to observethe magnitude of the reduction in transplantation rates.
The present results confirm prior findings indicatingthat women have significantly lower rates of transplan-tation than men. Garg et al [29] and Bloembergen et al[30] speculate that women may less aggressively negoti-ate the multiple steps needed for activation on the wait-ing list and that attitudinal and interpersonal factors—patient preferences, provider biases, and patient-providerinteractions—may play a role. Wolfe et al [14] confirmedthis gender gap toward wait-listing but explained muchof the lower transplantation rate for wait-listed femalecandidates by their higher panel reactive antibody levels,presumably due to prior pregnancies.
In the United States, Garg et al [29] suggested that for-profit dialysis units had substantially lower wait-listingrates than not-for-profit units, based on 1990 and 1993samples of dialysis patients. The present results from theDOPPS, based on a sample of year 2000 United Stateshemodialysis patients, indicated that the percentage ofpatients on the waiting list in for-profit facilities did notsignificantly differ from those in not-for-profit units. Al-though the sample rise was relatively small for not-for-profit units, these results agree both in direction and instatistical significance with the recent results of Ashbyet al [abstract; Ashby VB, et al, J Am Soc Nephrol14:253A, 2003], who did not see a significant difference(−0.5%) in kidney transplant wait-listing between for-profit versus not-for-profit United States dialysis units,based on over 3400 United States dialysis units in 2002.The present analysis found no significant associations be-tween facility size and transplantation rates, in agreementwith Alexander and Sehgal [31]. Nor could the presentanalysis find a relationship between transplantation ratesand frequency of visits with social workers.
In the United States, regional factors were importantin the chance of receiving a transplant, as Port [9] andAshby et al [abstract; Ashby VB, et al, J Am Soc Nephrol10:719A, 1999] have shown. Substantial regional varia-tion in the United States in kidney transplant wait-listinghad also been observed in a study of patients startingdialysis in 1991 to 1996 [abstract; Ashby et al, J Am SocNephrol 10:719A, 1999]. The same study also indicatedlarge differences in kidney transplant wait-listing by in-dividual states. The present DOPPS investigation indi-cates that large regional differences in kidney transplantwait-listing still exist in the United States. We did not ex-
amine to what extent United States regional differencesin kidney transplant wait-listing were related to regionaldifferences in organ donation or organ availability.
CONCLUSION
The DOPPS, using uniform data collection in nation-ally representative dialysis units, shows that there is largevariation in transplantation rates by country and alsowithin regions of the United States. Furthermore, thepresent international results consistently show that pa-tients who are younger, healthier, with higher educationand income, have higher rates of transplantation. Finally,transplantation rates did not significantly differ in theUnited States between for-profit and not-for-profit dial-ysis units.
The results from the waiting list investigation also showlarge differences between countries and between regionsof the United States in placing hemodialysis patients onkidney transplant waiting lists, even after adjusting fordifferences in patient demographics and comorbidity.
These findings from the DOPPS suggest opportunitiesto study factors in greater detail that allow certain coun-tries, regions, and dialysis units to have high wait-listingand transplantation rates. Greater access to transplan-tation may be achieved by improvements at the dialy-sis facility level by seeking living donors and increasingplacement on the waiting list for deceased donors.
APPENDIXStates in United States geographic regions (based onUnited States census divisions)
New England (New Eng): Connecticut, Maine, Massachusetts, NewHampshire, Rhode Island, VermontMiddle Atlantic (Mid Atl): New Jersey, New York, PennsylvaniaEast North Central (E N Central): Indiana, Illinois, Michigan, Ohio,WisconsinWest North Central (W N Central): Iowa, Kansas, Minnesota, Missouri,Nebraska, North Dakota, South DakotaSouth Atlantic (S Atl): Delaware, District of Columbia, Florida, Geor-gia, Maryland, North Carolina, South Carolina, Virginia, West VirginiaEast South Central (E S Central): Alabama, Kentucky, Mississippi, Ten-nesseeWest South Central (W S Central): Arkansas, Louisiana, Oklahoma,TexasMountain (Moun): Arizona, Colorado, Idaho, New Mexico, Montana,Utah, Nevada, WyomingPacific (PAC): Alaska, California, Hawaii, Oregon, Washington
ACKNOWLEDGMENTS
The DOPPS is supported by research grants from Amgen, Inc. andKirin Brewery, Ltd. without restrictions on publications. The authorsexpress appreciation to members of the DOPPS Committee for con-tributions during the design and implementation of the DOPPS. For afull listing of committee members, please see [12]. This paper was pre-sented in part at the 2002 International Congress on Transplantationand at the American Society of Nephrology (2003). The authors wishto thank Miles P. Finley for his editorial assistance in the preparation ofthis manuscript.

Satayathum et al: International transplantation and wait-listing rates 337
Reprint requests to Friedrich K. Port, M.D., M.S., University RenalResearch and Education Association, 315 W. Huron, Suite 260, AnnArbor, MI 48103.E-mail: [email protected].
REFERENCES
1. PORT FK, WOLFE RA, MAUGER EA, et al: Comparison of survivalprobabilities for dialysis patients vs cadaveric renal transplant re-cipients. JAMA 270:1339–1343, 1993
2. WOLFE RA, ASHBY VB, MILFORD EL, et al: Comparison of mortalityin all patients on dialysis, patients on dialysis awaiting transplanta-tion, and recipients of a first cadaveric transplant. N Engl J Med341:1725–1730, 1999
3. OJO AO, HANSON JA, MEIER-KRIESCHE H, et al: Survival in recipientsof marginal cadaveric donor kidneys compared with other recipientsand wait-listed transplant candidates. J Am Soc Nephrol 12:589–597,2001
4. WYNN JJ, DISTANT DA, PIRSCH JD, et al: Kidney and pancreas trans-plantation. Am J Transplant 4(Suppl 9):72–80, 2004
5. EVANS RW, MANNINEN DL, GARRISON LP JR., et al: The quality of lifeof patients with end-stage renal disease. N Engl J Med 312:553–559,1985
6. CHERTOW GM, LEE J, KUPERMAN GJ, et al: Guided medication dosingfor inpatients with renal insufficiency. JAMA 286:2839–2844, 2001
7. U.S. RENAL DATA SYSTEM: USRDS 2003 Annual Data Report: Atlasof End-Stage Renal Disease in the United States, Bethesda, MD,National Institutes of Health, National Institute of Diabetes andDigestive and Kidney Diseases, 2003
8. JAGER K, VAN DIJK P: 2003 Annual Report, 40th ERA-EDTACongress, Berlin, 2003 (available at http://www.era-edta-reg.org/files/presentations/pdf/berlin-Jager-AnnualReport03.pdf , accessedAugust 17, 2004)
9. PORT FK: Organ donation and transplantation trends in the UnitedStates, 2001. Am J Transplant 3(Suppl 4):7–12, 2003
10. NATHAN HM, CONRAD SL, HELD PJ, et al: Organ donation in theUnited States. Am J Transplant 3(Suppl 4):29–40, 2003
11. EPSTEIN AM, AYANIAN JZ, KEOGH JH, et al: Racial disparities inaccess to renal transplantation—Clinically appropriate or due tounderuse or overuse? N Engl J Med 343:1537–1544, 2000
12. YOUNG EW, GOODKIN DA, MAPES DL, et al: The Dialysis Outcomesand Practice Patterns Study: An international hemodialysis study.Kidney Int 57(Suppl 74):S74–S81, 2000
13. KLEIN JP, MOESCHBERGER ML: Survival Analysis Techniques forCensored and Truncated Data, New York, Springer, 1997, pp 417
14. WOLFE RA, ASHBY VB, MILFORD EL, et al: Differences in access tocadaveric renal transplantation in the United States. Am J KidneyDis 36:1025–1033, 2000
15. AYANIAN JZ, CLEARY PD, WEISSMAN JS, et al: The effect of patients’preferences on racial differences in access to renal transplantation.N Engl J Med 341:1661–1669, 1999
16. GAYLIN DS, HELD PJ, PORT FK, et al: The impact of comorbid andsociodemographic factors on access to renal transplantation. JAMA269:603–608, 1993
17. HELD PJ, PAULY MV, BOVBJERG RR, et al: Access to kidney trans-plantation. Has the United States eliminated income and racial dif-ferences? Arch Intern Med 148:2594–2600, 1988
18. KASISKE BL, LONDON W, ELLISON MD: Race and socioeconomicfactors influencing early placement on the kidney transplant waitinglist. J Am Soc Nephrol 9:2142–2147, 1998
19. ROBERTS JP, WOLFE RA, BRAGG-GRESHAM JL, et al: The effect ofchanging the priority for human leukocyte antigen (HLA) matchingon kidney transplantation rates and outcomes in minority groups.N Engl J Med 350:545–551, 2004
20. SOCIEDAD ESPANOLA DE NEFROLOGIA: (available at http://www.senefro.org/modules.php?name = subsection&idsection = 7&idsub-section = 128, accessed August 17, 2004)
21. PETERS J, IN ASSOCIATION WITH THE PROJECT ADVISORY GROUP: Renalservices for dialysis: Commissioner & provider perspectives—Aposition paper by The National Kidney Research Fund (availableat http://www.nkrf.org.uk/pdfs/news/scharr report april2003.pdf ,accessed August 17, 2004)
22. U.S. RENAL DATA SYSTEM: USRDS 2002 Annual Data Report: Atlasof End-Stage Renal Disease in the United States, Bethesda, MD,National Institutes of Health, National Institute of Diabetes andDigestive and Kidney Diseases, 2002
23. FREI U, SCHOBER-HALSTENBERG H-J: Annual Report on DialysisTreatment and Renal Transplantation in Germany for 2001/2002[Web site of QuaSi-Niere gGmbH] (available at http://www.quasi-niere.de/english/report/01/world.html, accessed August 17, 2004)
24. CONTE F, SALOMONE M: Italian Registry of Dialysis and Transplanta-tion Report 2001 [Web site of the Societa Italiana di Nefrologia (Ital-ian Society of Nephrology)] (available at http://www.sin-ridt.org/sin-ridt/sin-ridt.org.htm, accessed August 17, 2004)
25. THE JAPAN SOCIETY FOR TRANSPLANTATION: (available at http://www.medi-net.or.jp/tcnet/JST/fact 03/fact03 01.html, accessed August 17,2004)
26. TAKAGI H: Organ transplants still too few in Japan and Asian coun-tries. Transplant Proceedings 29:1580–1583, 1997
27. TAKAHASHI K: Current status of treatment for chronic renal fail-ure and factors behind increasing use of ABO-incompatible kid-ney transplantation, in ABO-Incompatible Kidney Transplantation(chapter 2), edited by Takahashi K, Amsterdam, Elsevier Science,2001, pp 5–8
28. MIRANDA B, GONZALEZ ALVAREZ I, CUENDE N, et al: Update on or-gan donation and retrieval in Spain. Nephrol Dial Transplant 14:842,1999
29. GARG PP, FRICK DD, DIENER-WEST M, et al: Effect of the ownershipof dialysis facilities on patients’ survival and referral for transplan-tation. N Engl J Med 341:1654–1660, 1999
30. BLOEMBERGEN WE, MAUGER EA, WOLFE RA, et al: Association ofgender and access to cadaveric renal transplantation. Am J KidneyDis 30:733–738, 1997
31. ALEXANDER GC, SEHGAL AR: Transplant Task Force of TheRenal Network, Inc: Variation in access to kidney transplan-tation across dialysis facilities: Using process of care mea-sures for quality improvement. Am J Kidney Dis 40:824–831,2002