Embed Size (px)
Citation preview

Kidney and Urinalysis
Prepared by: Sr. Siti Norhaiza Hadzir

Functions of the kidney Elimination of excess body water Elimination of waste products of
metabolism e.g urea & creatinine Elimination of foreign substances e.g
drugs Retention of substances necessary for
normal body function e.g protein, amino acids & glucose
Regulation of electrolytes balance & osmotic pressure of the body fluids.

The Nephron
The functional unit of the kidney. Consists of renal corpuscle
(glomerulus) & renal tubule. Structure of glomerulus Structure of tubule

Kidney blood supply
Renal artery from aorta → afferent arterioles → efferent arterioles → renal vein → heart

Glomerular Filtration Rate
Normally this amounts to about 130mL per minute (180 liters per 24 hours).

Renal Function Test Falls into 2 major group:
i) Detect the presence of disease- not give indication as to the degree of functional impairment e.g proteinuria, cast, hematuria, WBC
ii) Evaluate the degree of impairment e.g BUN, creatinine

Test of Urinary tract involvement Proteinuria
• Healthy glomerular permeable membrane passes only substances with MW of less than 70 000.
• Excess small proteins are reabsorbed completely by proximal tubule
• Albumin is very close to cut off value (70000MW) can get access to the urine in glomerular disease.
• Proteinuria are classified into 3:
Pre-renal- The glomerular membrane damage and tubular reabsorption inefficiency e.g Bence Jones protein in multiple myeloma.
Renal- renal parenchyma disease e.g amyloidosis.
Postrenal- Urinary tract problem e.g inflammation

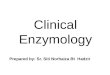
Figure 1:
Normal urine is compared with proteinuria sample.
Note increase in turbidity in proteinuria sample

Cast Cast are precipitates of protein
formed in the distal convoluted and collecting tubules of the kidney, where conditions of filtrate flow and pH are optimal for protein precipitation.
Normal condition-hyaline cast in small number
Large number indicates active renal disease.

Nature of cast It is a muco-protein formed normally by the
tubule; it is not formed in plasma.
It is long, rod like, flexible molecule.
As the glomerular filtrate travels down the nephron tubule, the concentrations of salts & H+ ↑.
At pH about 4.5, albumin and myoglobin change from negatively to positively charge molecules, the muco-protein is still negatively charge.
Opposite electric charge leads to precipitation and the formation of casts.

Hematuria & hemoglobinuria Presence indicate bleeding within the
urinary tract. In acute glomerulonephritis there is
hemorrhage from the glomeruli, Hb is convreted to hematin and methemoglobin.
These factors combine to give the “smoky” red brown urine characteristic of the disease.

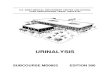
Figure 2:
The presence of blood in the urine

White Blood Cells
An increased number of white blood cells in a correctly collected specimen indicates inflammation in the urinary tract.

Test for Degree of Renal Impairment
Test based on water elimination and reabsorption
Blood Urea Nitrogen (BUN) Creatinine BUN: Creatinine

Test based on water elimination and reabsorption
Normally, conservation of water is reflected by concentrated urine with a high specific gravity
Excretion of an excess of water is illustrated by urine of low specific gravity

Impaired concentrating power
Tubular damage e.g chronic glomerulonephritis, polycystic disease
Severe potassium depletion Hypercalcemia e.g due to vitamin D
intoxication, hyperPTH Inborn defects of tubular function Diabetes insipidus

Non-protein nitrogen in blood
It is heterogenous collection of substances including urea, creatinine, uric acid, nucleotides, glutathione.
Estimation of NPN was replaced by determination of urea and creatinine, more specific indicators of renal condition, easily automated.

Blood Urea/BUN
Urea is the major excretion product of protein catabolism.
After elaboration, urea is passed to the blood and is excreted through the glomeruli and partly reabsorbed in the tubules.

Causes of ↑ BUN Pre-renal: Circulation in the kidney is
less efficient e.g CCF Renal: Renal parenchyma damage,
phylonephritis Post-renal: Obstruction to the urinary
tract Presence of high level of urea is called
uremia. Very high level of urea leads to
azotemia with kidney failure.

Creatinine
Nitrogenous substances found in muscle.
Since creatinine is derived entirely from endogenous metabolism (not form dietary protein) and is not reabsorbed by the renal tubules, its blood level; is a reliable index to renal function.

BUN/creatinine ratio
Normal ratio is 10:1. Ratio more than 10:1 occur in:
Ration less than 10:1 occur in:
-Excessive turnover of protein (hemorrhage, burns and infection)
- Reduced glomerular perfusion
- Repeated dialysis
- Severe vomiting or diarrhea
- Liver failure

Routine urinalysis
The procedure1. Urine collection and storage
2. Macroscopic examination
- Color
- turbidity and clarity (smoky. milky, cloudy)
- smell
- SG and osmolality

Color Possible cause
Straw to amber Normal
Orange Concentrated urine
Greenish orange bilirubin
Smoky Red blood cells
Brown to black on standing
Melanin or homogentisic acid
Almost colorless Dilute urine

Urine container Centrifuge tube
Pipetting the supernatant

The procedure: cont; Urine processing- Centrifuge
- Separate debris and supernatant
- Microscopic examination [cells (epithelium, RBC,
WBC, cast, mucus tread, ova and parasites,
crystals]
- Biochemical analysis (pH, protein, glucose, ketones, bilirubin, blood, nitrite, urobinogen, ascorbic acid)






Urine dipstick