Embed Size (px)
Citation preview

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 1/56
KhanNUHS.
8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 2/56
Hypersensitivity Reactions Outline
Introduction
Type I Hypersensitivity Type II Hypersensitivity
Type III Hypersensitivity
Type IV Hypersensitivity

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 3/56
Introduction
Normal immune reactions do their job withouthurting the host.
Sometimes, immune reactions can beexcessive, resulting in disease.
People who mount normal immune responsesare sensitized to that antigen.
People who have excessive responses arehypersensitive.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 4/56
Introduction
Bugs
Environmental antigens
Self antigens
What antigens initiate these “hypersensitivity reactions”?

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 5/56
Introduction
The immune response is triggered andmaintained inappropriately.
Hard to eliminate stimulus!
Hard to stop response once it starts!
So hypersensitivity diseases are often chronic,
debilitating, hard to treat.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 6/56
Mechanisms of HypersensitivityReactions
These reactions give rise to immunologic injury in variety ofdiseases and causing damage to tissues due to :
A. Exogenous antigens (Dust, pollens, foods, drugs,
microbiologic agents, chemicals, and many blood products.) .
B. Endogenous tissue Antigens. Against Self antigens (causeAutoimmune diseases)
C. Often associated with the Inheritance of Susceptible Genes
(HLA Genes).

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 7/56
Mechanisms of HypersensitivityReactions
Tissue injury may be caused by Humoral or Cellmediated.
Reactions takes “ VARIETY OF FORMS”:
Such as itching of skin . Swelling ,spasm, narrowing of lumen leading to
fatal diseases (like bronchial asthma ,anaphylaxis.)

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 8/56
Classification
They are classified as: Based on immunologic mechanism thatmediates :
Type I ( Immediate ) hypersensitivity reactions. The immune response is mediated by TH2 cells, IgE antibodies and
mast cells . Mast cells release vasoactive and spasmogenic substances(LIKE
histamine or like substances) Which are acting on vessels and smooth muscle and with
inflammatory cells. Type II (Antibody Mediated ) hypersensitivity reactions.
Antibodies(IgG and IgM) directly causing injury to the cells byphagocytosis or lysis and inflammation.
Antibodies may also interfere with cellular function and causedisease.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 9/56
Continue- Hypersensitivity reactions
Type III (Immune complex mediated) . Antibody ( IgG, IgM) binds to antigen,induce
inflammation directly or with complements. Neutrophils and Macrophages cause tissue damage.
Type IV ( Cells (T) mediated ) hypersensitivity reactions, cause tissue injury.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 10/56
Type I Hypersensitivity
ALLERGY: Is an example of “Immediate” hypersensitivity. Antigen (allergen) binds to IgE antibodies on
surface of mast cell Mast cell releases nasty mediators. End result: dilation of vessels, contraction of
smooth muscles.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 11/56
Type I Hypersensitivity
Allergen isinhaled/eaten/injected
Allergen stimulates TH2production
TH2 cell secretes cytokines:• IL-4 stimulates B cells to
make IgE.• IL-5 recruits eosinophils• IL-13 stimulates mucous
secretion.
Mast cell binds IgE. Allergen bridges IgE on mast
cell.
Mast cell degranulates.
Release of mediators.
Sequence of events

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 12/56

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 13/56
Type I Hypersensitivity
What nasty stuff does the mast cellrelease?
Granule contents• histamine
• some chemotactic factors
Membrane phospholipid metabolites• prostaglandin D2 • leukotrienes
Cytokines• TNF
• interleukins• IL-13

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 14/56
Type I Hypersensitivity
What do these nasty substances do? Act on blood vessels, smooth muscle, and WBCs.
Immediate response (minutes)
• vasodilation, vascular leakage, smooth muscle spasm• granule contents, prostaglandin, leukotrienes
Late phase reaction (hours)
• inflammation, tissue destruction
• cytokines

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 15/56
Type I Hypersensitivity
Act on blood vessels, smooth muscle, andWBCs.
Immediate response (minutes)
• vasodilation, vascular leakage, smooth musclespasm
• granule contents, prostaglandin, leukotrienes
Late phase reaction (hours)• inflammation, tissue destruction
• cytokines
What do these nasty substances do?

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 16/56
Mast cells intact (left) and degranulated (right) Mast cell. Type I hypersensitivity. In a type Ihypersenstivity reaction, the mast cell has IgE on its surface. When an allergen comes along, itbinds to the IgE, and the mast cell busts open, releasing its contents, mostly histamine

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 17/56
Type I Hypersensitivity Reaction (Allergy)
Immediate Reaction. within minutes,after
combination ofantigen with antibodybound to mast cells(also Basophils).
In individuals
previously sensitizedto an antigens ,Systemic or localreactions can occur.
Begin within 30minutes and subsidewithin 60 min.
Infiltration of tissues
with eosinophils,neutrophils,basophils, monocytescells(CD4+T)

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 18/56
Type I Hypersensitivity Reaction (Allergy)
What happens to the patient? Local reactions
• skin: itching, hives
• GI: diarrhea
• lung: bronchoconstriction Anaphylaxis
• itching, hives, erythema• constriction of bronchioles, wheezing
• laryngeal edema, hoarseness
• vomiting, cramps, diarrhea• laryngeal obstruction
• shock
• DEATH

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 19/56
Type I Hypersensitivity
“Atopy” – predisposition to react toallergens.
Atopy refers to predisposition to developlocalized immediate hypersensitivityreactions.
Family history of allergy is found in 50%of atopic individuals
Atopic patientshave higher IgE levels, moreTH2 cells
Candidate genes:• 5q31 (bunch of cytokine genes here)• 6p (close to HLA complex)
Why do some people have allergies, whileothers don’t?
8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 20/56
Type II Hypersensitivity
ANTIBODIES.
“Antibody-mediated” hypersensitivity.
Antibodies bind to antigens on cell surface.
Macrophages eat up cells, complement getsactivated, inflammation comes in.
End result: cells die, inflammation har.ms tissue

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 21/56
Type II Hypersensitivity
Disease Antigen Symptoms
Autoimmune
hemolytic anemiaRBC antigens, drugs Hemolysis
Pemphigus vulgarisProteins between
epithelial cellsBullae
Goodpasture syndrome Proteins in glomeruliand alveoli
Nephritis, lunghemorrhage
Myasthenia gravis Acetylcholine receptor Muscle weakness
Graves disease TSH receptor Hyperthyroidism
What kinds of diseases involve type IIhypersensitivity?

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 22/56
Type II Hypersensitivity
Antibodies bind tocell-surfaceantigens
One of three thingshappens:
• 1.Opsonizationand phagocytosis
• 2.Inflammation
• 3.Cellulardysfunction
Sequence of events
Type II hypersensitivity. Antibodies bind to fixed antigens on cell surfaces.
One of three things happens: 1) opsonization and phagocytosis, 2) inflammation(shown here), 3) cellular dysfunction.
Diseases that have type II hypersensitivity include autoimmune hemolytic anemia,myasthenia gravis, and Graves disease.( important for exam.)

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 23/56
Type II Hypersensitivity Reaction There are Three types of antibody dependant
mechanisms.
1. Detection and removal of cells : By Opsonizatio and Phagocytosis: Cells are Targeted by Antibodies ,This is
called opsonized that make them attractive
for phagocytes( Phagocytosis). This may be due to complement activation,
which tags antigens with its byproducts andmakes them recognizable by phagocytes.
2. Antibody mediated destruction of
cells : A process-Antibody dependant cellularcytotoxicity(ADCC) may lead to destruction of cells .
Does not involve complement but requiresleukocytes.
Cells are coated with IgG antibody.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 24/56
Type II Hypersensitivity Reaction
3.Antibody Mediated CellularDysfunction.
Antibody is directed against cell surfacereceptors, impair or dysregulate function“without causing cell injury or
inflammation.” Example: Myashthenia Gravis and Grave’s
disease. Antibodies in MG are directed against
Post-synaptic Ach receptors. Antibodies in Grave’s disease are directed
against TSH receptors on Thyroid Follicles.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 25/56
Summary . Draw this picture twice

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 26/56
Type III Hypersensitivity
IMMUNE COMPLEXES
“Immune complex-mediated” hypersensitivity
Antibodies bind to antigens, forming complexes
Complexes circulate, get stuck in vessels,stimulate inflammation
End result: bad inflammation, necrotizingvasculitis

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 27/56
Type III Hypersensitivity
Disease Antigen Symptoms
Systemic lupuserythematosus
Nuclear antigens Nephritis, skin lesions,arthritis…
Post-streptococcal
glomerulonephritisStreptococcal antigen Nephritis
Polyarteritis nodosa Hepatitis B antigen Systemic vasculitis
Serum sickness Foreign proteinsArthritis, vasculitis,
nephritis
Arthus reaction Foreign proteins Cutaneous vasculitis
What kinds of diseases involve type IIIhypersensitivity?

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 28/56
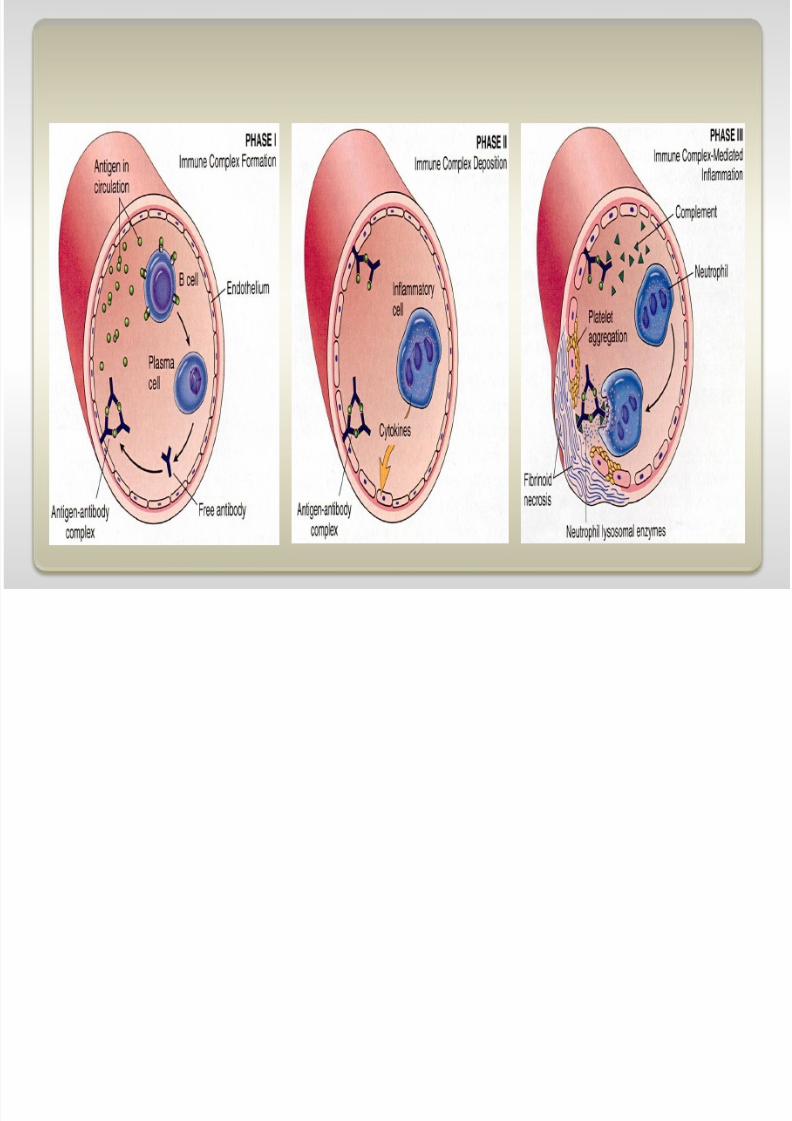
Type III Hypersensitivity
Two kinds of type III hypersensitivity reactions.
Systemic immune complex disease Complexes formed in circulation
Deposited in several organs Example: serum sickness Local immune complex disease
To specific organs such as Kidney- Glomerulonephritis,Joints-Arthritis
Complexes formed at site of antigen injection. Precipitated at injection site.
Example: Arthus reaction.
8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 29/56

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 30/56
Type III Hypersensitivity
How do the complexes causeinflammation?
Immune complexes activatecomplement, which:
attracts and activates neutrophils and
monocytes. Neutrophils and monocytes release
bad stuff (PG, tissue-dissolvingenzymes, etc.)
makes vessels leaky. Immune complexes also activate
clotting, causing microthrombi. Outcomes: vasculitis, glomerulonephritis,
arthritis,other –itises.Immune-complex-mediated vasculitis

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 31/56
Type III Hypersensitivity
C3b: promotes phagocytosis of complexes (and bugs!) C3a, C5a (anaphylatoxins): increase permeability
C5a: chemotactic for neutrophils, monocytes
C5-9: membrane damage or cytolysis
What are the important complementfractions to know?

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 32/56
Type III Hypersensitivity
Serum sickness Due to large amounts of foreign serum for passive
immunization (Antidiphtherial Toxin).
In olden days: used horse serum for immunization
Inject foreign protein (antigen).
Antibodies are made; they form complexes withantigens.
Complexes lodge in kidney, joints, small vessels.
Inflammation causes fever, joint pain, proteinuria.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 33/56
Type III Hypersensitivity
Arthus reaction
“Arthus reaction” = localized area of skin necrosisresulting from immune complex vasculitis
Inject antigen into skin of previously-immunizedperson
Pre-existing antibodies form complexes with antigen
Complexes precipitate at site of infection Inflammation causes edema, hemorrhage,
ulceration

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 34/56
8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 35/56
Type IV Hypersensitivity
“T-cell-mediated” hypersensitivity
Activated T cells do one of two things:• release cytokines that activate macrophages, or
• kill cells directly This process is normally useful against intracellular
organisms (viruses, fungi, parasites)
Here, it causes bad stuff: inflammation, cell destruction,
granuloma formation

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 36/56
Type IV Hypersensitivity
Two kinds of type IV hypersensitivity
Delayed-type hypersensitivity (DTH):• CD4+ T cells secrete cytokines
• macrophages come and kill cells Direct cell cytotoxicity:
• CD8+ T cells kill targeted cells

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 37/56
Type IV Hypersensitivity
Delayed-typehypersensitivity (DTH)
Patient exposed to antigen• Antigen presenting cells (APC)
presents antigen to CD4+ T cell
•T cells differentiate into effector andmemory TH1 cells
Patient exposed to antigen again• TH1 cells come to site of antigen
exposure• Release cytokines that activate
macrophages, increase inflammation
Results• Macrophages eat antigen (good)• Lots of inflammation and tissue
damage (bad)

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 38/56
Perivascular cuffing by CD4+ cells

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 39/56
Type IV Hypersensitivity
Prolonged DTH can lead togranulomatous inflammation
Perivascular CD4+ T cells
replaced by macrophages• Macrophages are activated,look “epithelioid”
• Macrophages sometimesfuse into “giant cells”
Granuloma = collection ofepithelioid macrophages

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 40/56
Type IV Hypersensitivity
Good example of DTH: positive Mantoux test
Patient previously exposed to TB
Inject (inactive) TB antigen into skinSee reddening, induration. Peaks in 1-3 days

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 41/56
Type IV Hypersensitivity
Why, yes it does. The same mechanisms underlie
both. Cell-mediated immunity is the major defense we have
against intracellular bugs (like TB and fungi).
Cell-mediated immunity (good) can coexist with DTH(bad)!
Patients with AIDS:• Lack CD4+ cells• So have poor cell-mediated immune response!• Macrophages sit there unactivated; can’t kill bugs.
DTH sounds a lot like cell-mediatedimmunity!

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 42/56
Type IV Hypersensitivity
CD8+ T cell recognize antigens onthe surface of cells
T cells differentiate into cytotoxic Tlymphocytes (CTLs) which killantigen-bearing cells
CTLs normally kill viruses and tumorcells
In T-cell mediated cytotoxicity, CTLskill other things:
• Transplanted organ cells• Pancreatic islet cells (Type I
diabetes)
T-cell-mediated cytotoxicity

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 43/56
Summary
Type I• Allergy• TH2 cells, IgE on mast cells, nasty mediators
Type II
• Antibodies• Opsonization, complement activation, or cell dysfunction
Type III• Immune complexes
• Lodge, cause inflammation, tissue injury
Type IV• CD4+ or CD8+ T cells• DTH or T-cell-mediated cytotoxicity

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 44/56
Clinical
Type II reactions occur in the following situations:
Transfusion reactions. Erythroblastosis fetalis (blood-type mismatch)
Autoimmune hemolytic anemia, thrombocytopenia,
agranulocytosis Certain drug reactions.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 45/56
Tuberculin skin reaction-
Delayed type hypersensitivity- classic example is tuberculin skinreaction-
injection of tuberculin ( protein-lipopollysaccharide component oftuberculous bacillus) in a previously sensitized person-redness+edema occurs 8-12 hours after injection due to
accumulation of T cells around small veins and venules. Eventually in Lungs replaced by macrophages in 2-3 weeks
Epitheloid cells and Giant cells which accumulate and aresurrounded by lymphocytes(Granulomatous inflammation).
1st exposure to protein antigen of Tuberculous bacilli -
Recognition by CD4+T cells+ class II molecules- CD4+T cells to TH1 cells- cytokines, also IL-12 lead to delayed hypersensitivity.
8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 46/56
Immunologic Deficiency Syndromes
Divided into Primary and Secondary. Primary are genetically determined
Primary most commonly in children( 6 months a --2yrs.) withrecurrent infections.
Adaptive (Both Humoral-B) and Cellular immunity-T)
Secondary-as a complications of: Malnutrition. Aging. effects of immunosuppression,irradiation, chemotherapy, and
other autoimmune diseases

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 47/56
X-linked Agammaglobulinemia of Burton
One of the more common of Primary immunodeficiency disorders Almost most commonly seen in males.
Seen at age 6 months . It is characterized by failure of B-cell precursors(Immature) to
mature B-cells,Plasma cells.
Genes of light chains immunoglobulins are absent (because ofMutations)
Recurrent bacterial and viral infections(Staph.aureus, Hemophilusinfluenza,Strep.
B-cells are decreased in circulation.
Immunogloulin level is depressed. Germinal centers in lymphoid tissues is underdeveloped. Plasma cells are absent.
T-cell mediated reactions are normal.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 48/56
Isolated IgA deficiency
A common immunodeficiency disorder.
It is far less in Blacks and Asians.
IgA deficiency- 1:600 European individuals.
Low levels of both serum and secretory IgA present. Familial or aquired ( with Measles, toxoplasmosis and
other viral inf.) Mucosal defenses are weakened . infection occurs in respiratory, GI and urogenital tracts. Antibodies against IgA are present in 40%. If transfused with IgA containing blood .
the immune system will attack the IgA as foreign and killthe person.
Autoimmune diseases.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 49/56
Immunologic deficiency syndromes
DiGeorge Syndrome (thymic hypoplasia)
T cell deficiency resulting from failure of development ofthird and fourth pharyngeal pouches- thymus, parathyroid,parts of thyroid, parts of CV system.
Result is loss of T cell immunity. Tetany, congenital CV(Defects in heart and great vessels
defects)

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 50/56
Severe combined immunodeficiencydisease
(SCID)- defects in both humoral and cell mediated immunity.
Infants present with Extensive thrush(Oral Candidiasis), diaperrash, failure to thrive.
Death within 1st year occurs if BM transplant is not done.
Most are X-linked. All lymphoid tissue is hypoplastic

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 51/56
Immunodeficiency with thrombocytopenia andEczema(Wiskott-Aldrich Syndrome)
X-linked recessive with Thrombocytopenia, eczema, recurrent infection , ending in early
death Thymus normal, but progressive depletion of T Lymphs Prone to malignant lymphoma .

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 52/56
Summary : Reading assignment

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 53/56
What type of cell is this? In what hypersensitivity reaction does it play a role?What does it have on its surface, and what does it have inside?

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 54/56
This person was frolicking in the bushes (having frolicked in same bushesmonths earlier). He got these lesions on his hands, and perhaps elsewhere.What type of hypersensitivity reaction does this represent?
Reminder: Where do inflammatory

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 55/56
Reminder: Where do inflammatorymediators come from?
Complementproteins
Coagulationfactors
Factors XII, XI, X, etc.

8/3/2019 Khan Hypersensitivity Reactions Final 2011
http://slidepdf.com/reader/full/khan-hypersensitivity-reactions-final-2011 56/56