Embed Size (px)
Citation preview

KHA-CARI Autosomal Dominant Polycystic Kidney Disease Guideline:
Screening for Polycystic Kidney DiseaseGopala K. Rangan, MB BS, PhD, FRACP,*,† Vincent W. Lee, MB BS, PhD, FRACP,*,†
Stephen I. Alexander, MB BS, MD, MPH, FRACP,‡ Chirag Patel, MB BS, MD, FRACP,§
David J. Tunnicliffe, MIPH,||,** and Philip Vladica, MB BS, FRANZR¶
*DS
†C
‡C
§G
||K
¶D
**S
Se
GUIDELINE RECOMMENDATIONS*
a. We recommend prior to screening at-risk individu-
als should receive appropriate counseling regarding
the potential benefits and risks of making the
diagnosis of autosomal dominant polycystic kidney
disease from their general practitioner in consulta-
tion with a clinical geneticist or nephrologist (2A).
b. We recommend that screening of individuals who
are at-risk (50% chance) be performed by renal
ultrasound and that the Pei-Ravine unified diagnos-
tic criteria for age-dependent cyst number (Tables 1
and 2) is used to make and exclude the diagnosis of
autosomal dominant polycystic kidney disease (1B).
epydenMeAuenTheAuental,HAdreepLocydAu
mi
artmneytre fdicastraltre f
CstraleticBri-CAn’sartmal Hneystral
nars
*Criteria used for recommendations and levels ofevidence (1,2;A-D) are described in more detail in Tables1 and 2 of Rangan G, Savige J. Introduction to the KHA-CARI Guidelines on ADPKD. Semin Nephrol.2015;35:521-3in this issue.
UNGRADED SUGGESTIONS FOR CLINICAL CARE
�
We suggest that physicians inform index cases tonotify first-degree relatives to see their generalpractitioner to discuss screening.�
Financial support: KHA-CARI Guidelines is supported by KidneyHealth Australia, the Australian and New Zealand Society ofSecond-degree and third relatives should bescreened on a case-by-case basis, due to the lowerprobability of autosomal dominant polycystic
0270-Crowreservhttp://
NepGui
ConflAdvticKDIADP
ent of Renal Medicine, Westmead Hospital, WesternLocal Health District, Sydney, Australia.or Transplant and Renal Research, Westmead Institute forl Research, University of Sydney, Westmead, Sydney,ia.or Kidney Research and the Department of Nephrology,hildren’s Hospital at Westmead, Westmead, NSW,ia.Health Queensland, Royal Brisbane and Women’s Hospi-sbane, Queensland, Australia.RI Guidelines, Centre for Kidney Research, The Chil-Hospital at Westmead, Westmead, Sydney, Australia.ent of Radiology, Westmead Hospital, Western Sydneyealth District, Westmead, Sydney, Australia.School of Public Health, University of Sydney, Sydney,ia.
AddreWesandmeaedu
in Nephrology, Vol 35, No 6, November 2015, pp 557–564
kidney disease (ADPKD) (25% and 12.5%,respectively), and lack of diagnostic criteria forrenal ultrasound.
�
In addition the screening assessment shouldinclude clinical evaluation for other featuressupporting a diagnosis of ADPKD, such askidney enlargement and extrarenal cysts.�
At-risk individuals ≤ 40 years of age and youngerwho have renal cysts detected on the ultrasoundbut who do not meet the Pei-Ravine criteria forcyst number could have repeat ultrasound scan-ning in 12 months with further follow-up in 3- to5-year intervals, depending on the clinical circum-stances and discussion with the patient.�
A normal renal ultrasound in at-risk individuals ≤ 40years of age does not exclude the diagnosis ofADPKD. Annual blood pressure measurement andrepeating the renal ultrasound at 5-year intervals(until the age of 40 years) may be considered. Incontrast, a cautious approach in assigning a diag-nosis of ADPKD should be undertaken in at-riskindividuals older than 40 years of age who haveequivocal ultrasound findings because of the increas-ing prevalence of simple age-related cysts.�
Presently, in the absence of a regulatory-approveddisease-specific therapy, screening at-risk pediatric9295/ - see front mattern Copyright & 2015 Published by Elsevier Inc. All rightsed.dx.doi.org/10.1016/j.semnephrol.2015.10.004
hrology, Amgen Australia, and Shire Australia Pty Ltd.deline members were not remunerated for their work.
ict of interest statement: Gopala Rangan is a member of theisory Committee on the Safety of Medical Devices, Therapeu-Goods Administration and received financial support fromGO to attend the KDIGO Controversies Conference onKD in January 2014.ss reprint requests to Gopala Rangan, MB BS, PhD, FRACP,tmead Institute for Medical Research, Centre for TransplantRenal Research, 176 Hawkesbury Rd, PO Box 412, West-d, Sydney, NSW, Australia 2145. E-mail: [email protected]
557
G.K. Rangan et al.558
subjects (o18 years of age) may not be justified.The decision to screen should take into accountclinical circumstances and parent/carer discussionregarding the potential benefits, risks, and limita-tions of ultrasound diagnosis in this population. Inchildren, a tailored approach for screening may beappropriate, and include blood pressure measure-ment with or without renal ultrasound imaging.
�
Screening of potential kidney donors who are atrisk of ADPKD requires comprehensive multi-disciplinary clinical and radiological assessment.Renal computed tomography (CT) is routinelyperformed during donor assessment but magneticresonance imaging (MRI) has greater sensitivityin detecting cysts than ultrasound and CT (0.3versus 0.5-1.0 versus 0.5 cm diameter, respec-tively). In at-risk individuals with a negativeultrasound, especially below 40 years of age, therisk benefit of kidney donation must be carefullyconsidered, as ADPKD is not excluded entirely.Under these circumstances, renal MRI and molec-ular genetic testing may assist in the decision-making.�
Ultrasound transducers, more sensitive than thatused in previous clinical studies of ADPKD (ie,45 MHz), increase the ability to detect renalcysts that are smaller than 1.0 cm in diameter.However, diagnostic criteria using these moresensitive transducers to differentiate ADPKDfrom age-related simple cysts are not defined.IMPLEMENTATION AND AUDIT
No suggestions.
BACKGROUND
Screening for ADPKD in at-risk individuals hasseveral benefits, including the early detection andtreatment of renal complications such as hypertensionand renal impairment. In this regard, recent clinicalstudies highlighted that conventional renoprotectivetherapies, such as angiotensin-converting enzymeinhibitors, angiotensin-receptor blockers,1 and statins2
may reduce the kidney enlargement and may poten-tially decrease the risk of end-stage kidney disease(ESKD). Other benefits of screening in early adulthoodinclude awareness for family planning as well as thedetection of serious extrarenal complications, particu-larly intracranial aneurysms. On the other hand, thepotential disadvantages of screening at-risk individualsrelates to the social and psychological impact ofmaking the diagnosis of ADPKD.
Almost all carriers of an ADPKD mutation willdevelop ultrasound-detectable multiple simple renal
cysts (Bosniak class 1) during their lifetime, but thepenetrance is progressive, insidious, and age-depend-ent, and cyst detection by imaging is difficult duringchildhood due to their microscopic size (and/orabsence) at that stage.3 Moreover, a significant pro-portion of ADPKD patients have mild renal diseaseand may remain clinically asymptomatic throughoutlife. Prior to the era of renal ultrasound, the mean ageof ADPKD diagnosis was 47.2 years of age, and usingclinical features alone, only 17% of subjects experi-enced abdominal pain and 2% had severe uremia bythe age of 35.4 In another cohort of more than 200patients followed up over 22 years, the median age atonset of hypertension, chronic kidney disease (CKD),and death was 46, 50, and 63 years of age, respec-tively, in PKD1 patients (in PKD2 patients 51, 68, and71 years, respectively).5 Thus, physical examinationand laboratory investigations alone are not suitabletools to screen for ADPKD in at-risk individuals, andrenal imaging is required.
Renal ultrasound has been used to screen forADPKD in at-risk individuals for more than 40 years.6
The key issues in the use of ultrasound as a screeningtool have been the false-positive and false-negativedetection rates of renal cysts. The false-positive rate isdue to the increasing prevalence of age-related simplebenign renal cysts that are common (410% prevalenceabove 50 years of age) in the general population,7,8
(associated with chronic renal pathology9 and hyper-tension),10 but do not confer a diagnosis of ADPKD. Incontrast, the false-negative rate is primarily a problemin young affected individuals (o40 years) who have amild renal phenotype (eg, PKD2 mutation) in whichcysts may be below the level of detection by ultra-sound. Therefore, age-related criteria using cyst num-ber to screen for ADPKD were developed, initiallyby Ravine et al11 in 1994 and subsequently revised byPei et al12 in 2009, to assist in reducing the false-positive and false-negative rates during the screeningof at-risk individuals. At present, the Pei-Ravinecriteria is the standard method used for making thediagnosis of ADPKD in at-risk individuals by renalultrasound.13
SEARCH STRATEGY
Databases Searched
Medical subject headings (MeSH) terms and textwords for ADPKD were combined with the MeSHterms and text words for screening. This was thencombined with further searches using the MeSH andtext words for diagnosis and imagining, and animalstudies were specifically excluded. The search wascarried out in Ovid MEDLINE (1946 to June 2014),Embase (1974 to May 23, 2014), PsycINFO (1806 to
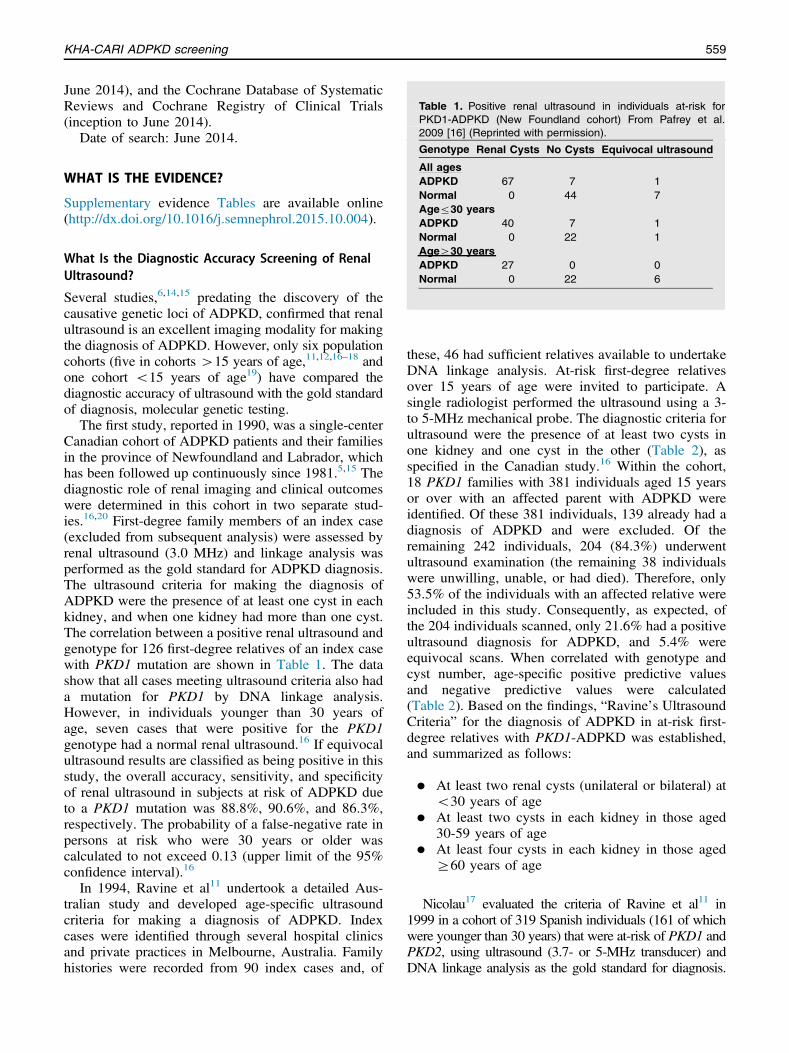
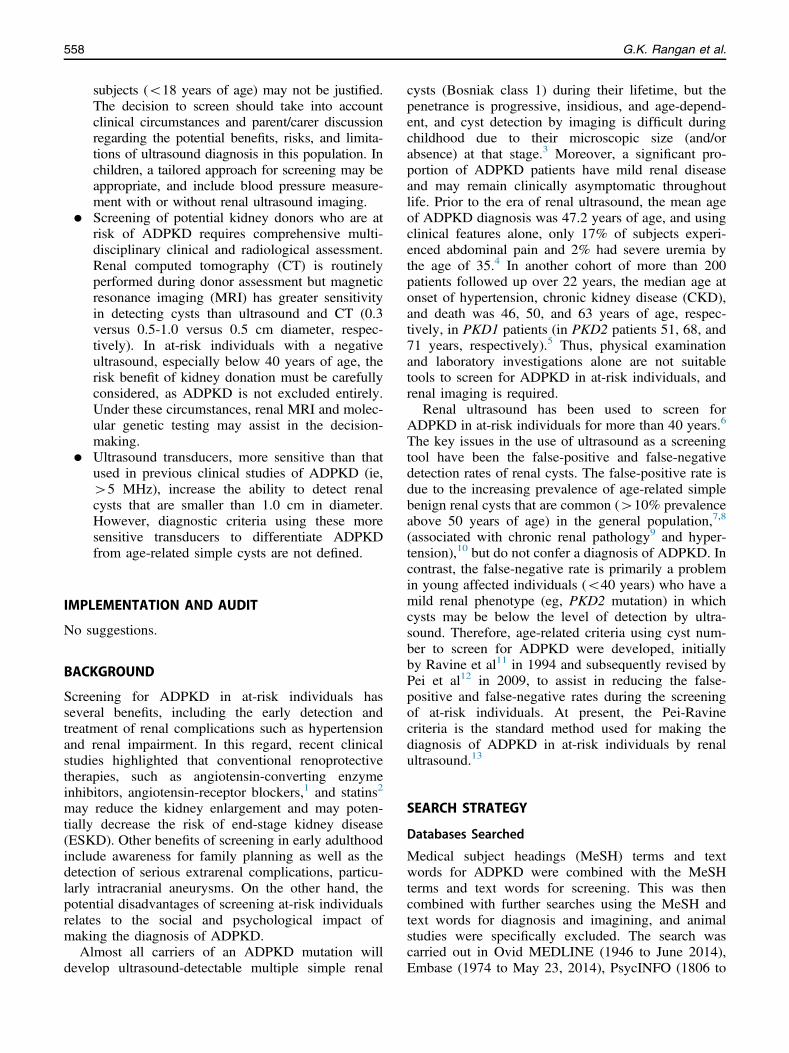
Table 1. Positive renal ultrasound in individuals at-risk forPKD1-ADPKD (New Foundland cohort) From Pafrey et al.2009 [16] (Reprinted with permission).
KHA-CARI ADPKD screening 559
June 2014), and the Cochrane Database of SystematicReviews and Cochrane Registry of Clinical Trials(inception to June 2014).
Date of search: June 2014.
Genotype Renal Cysts No Cysts Equivocal ultrasoundAll agesADPKD 67 7 1Normal 0 44 7Ager30 yearsADPKD 40 7 1Normal 0 22 1AgeZ30 yearsADPKD 27 0 0Normal 0 22 6
WHAT IS THE EVIDENCE?
Supplementary evidence Tables are available online(http://dx.doi.org/10.1016/j.semnephrol.2015.10.004).
What Is the Diagnostic Accuracy Screening of RenalUltrasound?
Several studies,6,14,15 predating the discovery of thecausative genetic loci of ADPKD, confirmed that renalultrasound is an excellent imaging modality for makingthe diagnosis of ADPKD. However, only six populationcohorts (five in cohorts 415 years of age,11,12,16–18 andone cohort o15 years of age19) have compared thediagnostic accuracy of ultrasound with the gold standardof diagnosis, molecular genetic testing.
The first study, reported in 1990, was a single-centerCanadian cohort of ADPKD patients and their familiesin the province of Newfoundland and Labrador, whichhas been followed up continuously since 1981.5,15 Thediagnostic role of renal imaging and clinical outcomeswere determined in this cohort in two separate stud-ies.16,20 First-degree family members of an index case(excluded from subsequent analysis) were assessed byrenal ultrasound (3.0 MHz) and linkage analysis wasperformed as the gold standard for ADPKD diagnosis.The ultrasound criteria for making the diagnosis ofADPKD were the presence of at least one cyst in eachkidney, and when one kidney had more than one cyst.The correlation between a positive renal ultrasound andgenotype for 126 first-degree relatives of an index casewith PKD1 mutation are shown in Table 1. The datashow that all cases meeting ultrasound criteria also hada mutation for PKD1 by DNA linkage analysis.However, in individuals younger than 30 years ofage, seven cases that were positive for the PKD1genotype had a normal renal ultrasound.16 If equivocalultrasound results are classified as being positive in thisstudy, the overall accuracy, sensitivity, and specificityof renal ultrasound in subjects at risk of ADPKD dueto a PKD1 mutation was 88.8%, 90.6%, and 86.3%,respectively. The probability of a false-negative rate inpersons at risk who were 30 years or older wascalculated to not exceed 0.13 (upper limit of the 95%confidence interval).16
In 1994, Ravine et al11 undertook a detailed Aus-tralian study and developed age-specific ultrasoundcriteria for making a diagnosis of ADPKD. Indexcases were identified through several hospital clinicsand private practices in Melbourne, Australia. Familyhistories were recorded from 90 index cases and, of
these, 46 had sufficient relatives available to undertakeDNA linkage analysis. At-risk first-degree relativesover 15 years of age were invited to participate. Asingle radiologist performed the ultrasound using a 3-to 5-MHz mechanical probe. The diagnostic criteria forultrasound were the presence of at least two cysts inone kidney and one cyst in the other (Table 2), asspecified in the Canadian study.16 Within the cohort,18 PKD1 families with 381 individuals aged 15 yearsor over with an affected parent with ADPKD wereidentified. Of these 381 individuals, 139 already had adiagnosis of ADPKD and were excluded. Of theremaining 242 individuals, 204 (84.3%) underwentultrasound examination (the remaining 38 individualswere unwilling, unable, or had died). Therefore, only53.5% of the individuals with an affected relative wereincluded in this study. Consequently, as expected, ofthe 204 individuals scanned, only 21.6% had a positiveultrasound diagnosis for ADPKD, and 5.4% wereequivocal scans. When correlated with genotype andcyst number, age-specific positive predictive valuesand negative predictive values were calculated(Table 2). Based on the findings, “Ravine’s UltrasoundCriteria” for the diagnosis of ADPKD in at-risk first-degree relatives with PKD1-ADPKD was established,and summarized as follows:
�
At least two renal cysts (unilateral or bilateral) ato30 years of age�
At least two cysts in each kidney in those aged30-59 years of age�
At least four cysts in each kidney in those agedZ60 years of ageNicolau17 evaluated the criteria of Ravine et al11 in1999 in a cohort of 319 Spanish individuals (161 of whichwere younger than 30 years) that were at-risk of PKD1 andPKD2, using ultrasound (3.7- or 5-MHz transducer) andDNA linkage analysis as the gold standard for diagnosis.
Table 2. Positive predictive value and negative predictive value of cyst number according to age at-risk for PKD1-ADPKD (Australiancohort) From Ravine et al. 1994 [11] (Reprinted with permission).
Cyst No. 20 yrs 30 yrs 40 yrs 50 yrs 60 yrs 70 yrs
Z1 cyst 100, 96.6 97.7, 100 96.9, 100 77.2, 100 73.8, 100 45.5, 100Z2 cysts* 100, 96.6 99.2, 100 98.9, 100 95.6, 100 94.7, 100 61.2, 100Z2 cysts in 1 kidney, Z1 cyst in the other 100, 90.5 99.2, 100 98.9, 100 98.2, 100 97.9, 100 85.2, 100Z2 cysts in each kidney 100, 87.7 100, 100 100, 100 100, 100 100, 100 90.7, 100Z4 cysts in each kidney 100, 85.1 100, 89.9 100, 100 100, 100 100, 100 95.9, 100
G.K. Rangan et al.560
The sensitivity of ultrasound for making the diagnosis was95% in individuals with a PKD1 mutation but only 67%for PKD2 in individuals younger than 30 years, whereas itwas 100% for both genotypes if the individual was overthe age of 30 years. In all patients (both PKD1 and PKD2),the overall sensitivity, specificity, and accuracy of ultra-sound was 97%, 100%, and 98%, respectively. Thus, thisstudy demonstrated that the criteria of Ravine et al11 couldnot be accurately applied in young at-risk individuals witha PKD2 mutation.
To address the issue of PKD2 mutations and alsobecause DNA linkage analysis is complex and notroutinely performed, in 2009 Pei et al12 revised theRavine’s Criteria11 criteria by establishing age-specificcriteria for individuals not only at risk for PKD1, butalso for PKD2, and those in which the genotype resultswere not known. This multicenter study recruitedparticipants from Australia, Europe, and North America,comprising individuals from 78 PKD1 families and 39PKD2 families, all born with a 50% risk for ADPKD.(Note: subjects included were, in part, derived fromprevious studies by Ravine et al11 and Parfrey et al.16)Renal ultrasound with a 3- or 5-MHz sector probe wasused in this study and the majority of “positive cysts”detected were greater than 1 cm in diameter. The resultsshowed that 52.3% of at-risk subjects had a mutationconfirmed by linkage analysis. The study tested theRavine11 criteria for PKD1 genotype and found that itcould not be applied to those with a PKD2 phenotype,who had milder disease. Consequently, new criteriawere developed. In addition, through simulation studiesusing statistical bootstrapping, diagnostic criteria for
Table 3. Pei-Ravine ultrasound criteria for making the diagnosispermission).
Age of first-degree relative at-risk of ADPKD PPV
15-30 years with Z 3 renal cysts (unilateral or bilateral) 100%30-39 years with Z 3 renal cysts (unilateral or bilateral) 100%40-59 years with Z 2 renal cysts in each kidney 100%Z 60 years with 44 renal cysts in each kidney -
at-risk individuals with an unknown genotype wasformulated and shown in Table 3. However, thesecriteria yielded a false-negative rate greater than 14%,and therefore cannot be used for disease exclusion. Inthese cases, the investigators suggested that a finding offewer than 2 renal cysts provides a negative predictivevalue of 100% and is sufficient for ruling out disease inat-risk individuals 40 years and older.
Finally, only one cohort has focused on the diag-nostic accuracy of ultrasound for screening at-riskpediatric subjects less than 15 years of age. In 1997,Gabow et al19 examined 106 children at 50% riskfor ADPKD from 40 families. The ultrasound wasconsidered positive if any cysts were present. Thediagnostic accuracy, sensitivity, and specificity ofultrasound was 84.9%, 77.4%, and 95.5%, respec-tively, with a 25% false-negative rate. The false-negative rate was highest (38%) if subjects were agedbetween 3 months and 5 years of age.19 This studyhighlights the difficulties in making a diagnosis ofADPKD in the pediatric population due to the insensi-tivity of ultrasound in this group.
What Other Features on Clinical Evaluation andUltrasound Are Useful in Screening At-Risk Individuals?
In clinical practice, the type of ADPKD mutation istypically unknown in affected individuals. Barua et al21
investigated whether clinical parameters may predictwhether a family carries a PKD1 or PKD2 mutation.The study examined 90 families with 484 affectedindividuals and all their first-degree relatives in a typical
of ADPKD Adapted from Pei et al. 2011 [22] (Reprinted with
ADPKD Mutation Type
PKD1 PKD2 Not known
Sensitivity PPV Sensitivity PPV Sensitivity
94.3% 100% 69.5% 100% 81.7%96.6% 100% 94.9% 100% 95.5%92.6% 100% 88.8% 100% 90%100% - 100% - 100%

Table 4. Pei-Ravine ultrasound criteria for the exclusion of ADPKD Adapted from Pei et al. 2011 [22] (Reprinted with permission).
ADPKD Mutation Type
PKD1 PKD2 Not known
Age of first-degree relative at-risk of ADPKD NPV Specificity NPV Specificity NPV Specificity
15-30 years with Z 1 renal cyst 99.1% 97.6% 83.5% 96.6% 90.8% 97.1%30-39 years with Z 1 renal cyst 100% 96% 96.8% 93.8% 98.3% 94.8%40-59 years with Z 1 renal cyst 100% 93.9% 100% 93.7% 100% 93.9%
KHA-CARI ADPKD screening 561
hospital clinic over an 8-year period. At least 60% ofparticipants were referred by primary care physicians.The results showed that having at least one familymember who developed ESKD at age 55 years oryounger predicted PKD1 mutation in approximatelythree quarters of families (sensitivity, 72%; positivepredictive value [PPV], 100%), whereas if the age was70 years and older, then this was more suggestive of aPKD2 mutation (sensitivity, 74%; PPV, 100%). Theinvestigators therefore suggested a family history of ageof onset of ESKD could be useful information duringthe clinical and ultrasonography assessment of at-riskindividuals.22
In ADPKD, the prevalence of other ultrasoundabnormalities, including nephromegaly and hepaticcysts, increase in an age-dependent manner. As shownin Table 4, these sonographic abnormalities are detectedat an earlier age than clinically detectable abnormalities,such as hypertension.23 Therefore, these additionalparameters may assist in making the diagnosis in at-risk individuals. However, no studies have evaluated theaccuracy of evaluating the composite of renal cysts,nephromegaly, and hepatic cysts as diagnostic criteria.
How Does the Diagnostic Accuracy of UltrasoundCompare With Other Imaging Modalities?
The Pei-Ravine ultrasound criteria are based on thedetection of renal cysts that are at least 1 cm indiameter. However, renal cyst detection by CT is betterthan ultrasound (0.5-cm cyst detectable), and evenbetter with MRI (0.3-cm cyst detectable).24 Untilrecently, no population cohort studies have specificallyestablished diagnostic criteria for screening at-riskindividuals using any of these imaging modalities,and their evaluation has been limited to case reports.For example, Zand et al24 reported a case of a 25-year-old at-risk individual who was found to have no cystsby ultrasound and proceeded as a kidney donor to hermother.24 However, at the time of surgery, cysts werenoted and the donation was abandoned. In the post-operative period a renal MRI was performed andconfirmed the presence of multiple renal cysts. Theinvestigators therefore suggested that MRI could be
used as an additional investigation to screen at-riskkidney donors under the age 30 years.24
In 2015, Pei et al25 compared the diagnosticperformance of high-resolution ultrasound with MRI.This was a single-center study conducted by theToronto Radiological Imaging Study of PKD Groupand consisted of 110 subjects with a 50% risk forADPKD aged between 16 to 40 years and 45 age-matched normal healthy control subjects. In the at-riskcohort, molecular genetic testing (long-range polymer-ase chain reaction) revealed that 66.4% (n ¼ 73) wereaffected by ADPKD, and, of these, at least half(54.8%) had PKD2 and nontruncating mutations(which are known to have less severe renal phenotype).Ultrasound scans were performed with 4- to 8-MHzprobes (more sensitive than previous studies), and MRIwas conducted on a 1.5-T scanner without gadolinium.Cysts were defined as having a diameter of at least 2 to3 mm by ultrasound and 2.6 mm in width on a single-image plane on MRI.25 In comparison to ultrasound,MRI correctly identified all affected cases (with 98.6%of subjects having 10 renal cysts and 100% of subjectshaving 20 renal cysts), but using the Pei-Ravinediagnostic ultrasound criteria yielded one false-negative and three false-positive cases. The false-negative case was a genetically affected subject witha body mass index of 35.6 kg/m2 who had more than20 renal cysts by MRI and no cyst detectable by asuboptimal ultrasound.
The diagnostic performance of a higher-sensitivityultrasound probe in this study was compared to aprevious cohort (Pei et al,12 2009) and the data areshown in Table 5 and Table 6. As expected, asignificant increase in diagnostic performance wasnoted with the more sensitive probe. Moreover, whilethe absence of renal cysts could be considered acriterion for disease exclusion in at-risk subjectsbetween 30 and 40 years of age, this cannot be appliedin younger patients.
The diagnostic performance and criteria from Peiet al25 using MRI are shown in Table 7. The results ofthe study25 showed that the presence of a total of 10cysts or more on renal MRI was considered sufficientto make the diagnosis of ADPKD (sensitivity and
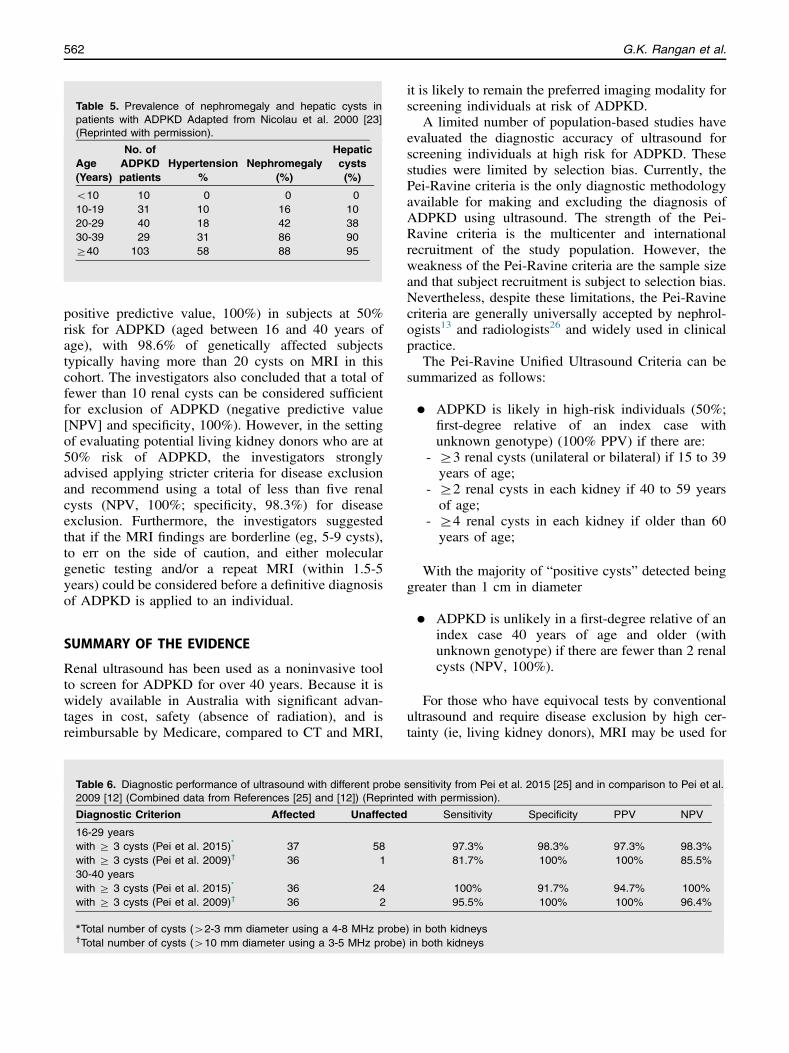
Table 5. Prevalence of nephromegaly and hepatic cysts inpatients with ADPKD Adapted from Nicolau et al. 2000 [23](Reprinted with permission).
Age(Years)
No. ofADPKDpatients
Hypertension%
Nephromegaly(%)
Hepaticcysts(%)
o10 10 0 0 010-19 31 10 16 1020-29 40 18 42 3830-39 29 31 86 90Z40 103 58 88 95
G.K. Rangan et al.562
positive predictive value, 100%) in subjects at 50%risk for ADPKD (aged between 16 and 40 years ofage), with 98.6% of genetically affected subjectstypically having more than 20 cysts on MRI in thiscohort. The investigators also concluded that a total offewer than 10 renal cysts can be considered sufficientfor exclusion of ADPKD (negative predictive value[NPV] and specificity, 100%). However, in the settingof evaluating potential living kidney donors who are at50% risk of ADPKD, the investigators stronglyadvised applying stricter criteria for disease exclusionand recommend using a total of less than five renalcysts (NPV, 100%; specificity, 98.3%) for diseaseexclusion. Furthermore, the investigators suggestedthat if the MRI findings are borderline (eg, 5-9 cysts),to err on the side of caution, and either moleculargenetic testing and/or a repeat MRI (within 1.5-5years) could be considered before a definitive diagnosisof ADPKD is applied to an individual.
SUMMARY OF THE EVIDENCE
Renal ultrasound has been used as a noninvasive toolto screen for ADPKD for over 40 years. Because it iswidely available in Australia with significant advan-tages in cost, safety (absence of radiation), and isreimbursable by Medicare, compared to CT and MRI,
Table 6. Diagnostic performance of ultrasound with different probe2009 [12] (Combined data from References [25] and [12]) (Reprinte
Diagnostic Criterion Affected Unaffected
16-29 yearswith Z 3 cysts (Pei et al. 2015)* 37 58with Z 3 cysts (Pei et al. 2009)† 36 130-40 yearswith Z 3 cysts (Pei et al. 2015)* 36 24with Z 3 cysts (Pei et al. 2009)† 36 2
*Total number of cysts (42-3 mm diameter using a 4-8 MHz probe†Total number of cysts (410 mm diameter using a 3-5 MHz probe)
it is likely to remain the preferred imaging modality forscreening individuals at risk of ADPKD.
A limited number of population-based studies haveevaluated the diagnostic accuracy of ultrasound forscreening individuals at high risk for ADPKD. Thesestudies were limited by selection bias. Currently, thePei-Ravine criteria is the only diagnostic methodologyavailable for making and excluding the diagnosis ofADPKD using ultrasound. The strength of the Pei-Ravine criteria is the multicenter and internationalrecruitment of the study population. However, theweakness of the Pei-Ravine criteria are the sample sizeand that subject recruitment is subject to selection bias.Nevertheless, despite these limitations, the Pei-Ravinecriteria are generally universally accepted by nephrol-ogists13 and radiologists26 and widely used in clinicalpractice.
The Pei-Ravine Unified Ultrasound Criteria can besummarized as follows:
sed
)i
�
nsitwith
in bon bo
ADPKD is likely in high-risk individuals (50%;first-degree relative of an index case withunknown genotype) (100% PPV) if there are:
-
i
t
Z3 renal cysts (unilateral or bilateral) if 15 to 39years of age;
-
Z2 renal cysts in each kidney if 40 to 59 yearsof age;-
Z4 renal cysts in each kidney if older than 60years of age;With the majority of “positive cysts” detected beinggreater than 1 cm in diameter
�
ADPKD is unlikely in a first-degree relative of anindex case 40 years of age and older (withunknown genotype) if there are fewer than 2 renalcysts (NPV, 100%).For those who have equivocal tests by conventionalultrasound and require disease exclusion by high cer-tainty (ie, living kidney donors), MRI may be used for
vity from Pei et al. 2015 [25] and in comparison to Pei et al.permission).
Sensitivity Specificity PPV NPV
97.3% 98.3% 97.3% 98.3%81.7% 100% 100% 85.5%
100% 91.7% 94.7% 100%95.5% 100% 100% 96.4%
th kidneysh kidneys
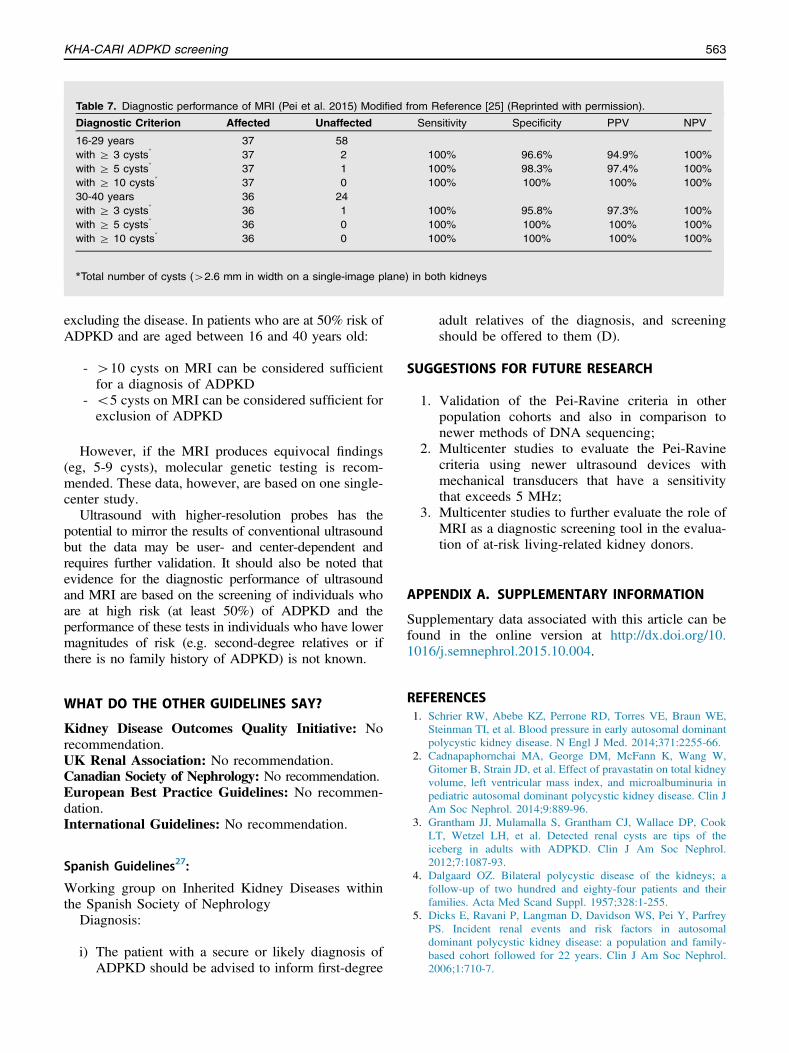
Table 7. Diagnostic performance of MRI (Pei et al. 2015) Modified from Reference [25] (Reprinted with permission).
Diagnostic Criterion Affected Unaffected Sensitivity Specificity PPV NPV
16-29 years 37 58with Z 3 cysts* 37 2 100% 96.6% 94.9% 100%with Z 5 cysts* 37 1 100% 98.3% 97.4% 100%with Z 10 cysts* 37 0 100% 100% 100% 100%30-40 years 36 24with Z 3 cysts* 36 1 100% 95.8% 97.3% 100%with Z 5 cysts* 36 0 100% 100% 100% 100%with Z 10 cysts* 36 0 100% 100% 100% 100%
*Total number of cysts (42.6 mm in width on a single-image plane) in both kidneys
KHA-CARI ADPKD screening 563
excluding the disease. In patients who are at 50% risk ofADPKD and are aged between 16 and 40 years old:
-
410 cysts on MRI can be considered sufficientfor a diagnosis of ADPKD-
o5 cysts on MRI can be considered sufficient forexclusion of ADPKDHowever, if the MRI produces equivocal findings(eg, 5-9 cysts), molecular genetic testing is recom-mended. These data, however, are based on one single-center study.
Ultrasound with higher-resolution probes has thepotential to mirror the results of conventional ultrasoundbut the data may be user- and center-dependent andrequires further validation. It should also be noted thatevidence for the diagnostic performance of ultrasoundand MRI are based on the screening of individuals whoare at high risk (at least 50%) of ADPKD and theperformance of these tests in individuals who have lowermagnitudes of risk (e.g. second-degree relatives or ifthere is no family history of ADPKD) is not known.
WHAT DO THE OTHER GUIDELINES SAY?
Kidney Disease Outcomes Quality Initiative: Norecommendation.UK Renal Association: No recommendation.Canadian Society of Nephrology: No recommendation.European Best Practice Guidelines: No recommen-dation.International Guidelines: No recommendation.
Spanish Guidelines27:
Working group on Inherited Kidney Diseases withinthe Spanish Society of Nephrology
Diagnosis:
i)
The patient with a secure or likely diagnosis ofADPKD should be advised to inform first-degreeadult relatives of the diagnosis, and screeningshould be offered to them (D).
SUGGESTIONS FOR FUTURE RESEARCH
1.
Validation of the Pei-Ravine criteria in otherpopulation cohorts and also in comparison tonewer methods of DNA sequencing;2.
Multicenter studies to evaluate the Pei-Ravinecriteria using newer ultrasound devices withmechanical transducers that have a sensitivitythat exceeds 5 MHz;3.
Multicenter studies to further evaluate the role ofMRI as a diagnostic screening tool in the evalua-tion of at-risk living-related kidney donors.APPENDIX A. SUPPLEMENTARY INFORMATION
Supplementary data associated with this article can befound in the online version at http://dx.doi.org/10.1016/j.semnephrol.2015.10.004.
REFERENCES1. Schrier RW, Abebe KZ, Perrone RD, Torres VE, Braun WE,
Steinman TI, et al. Blood pressure in early autosomal dominantpolycystic kidney disease. N Engl J Med. 2014;371:2255-66.
2. Cadnapaphornchai MA, George DM, McFann K, Wang W,Gitomer B, Strain JD, et al. Effect of pravastatin on total kidneyvolume, left ventricular mass index, and microalbuminuria inpediatric autosomal dominant polycystic kidney disease. Clin JAm Soc Nephrol. 2014;9:889-96.
3. Grantham JJ, Mulamalla S, Grantham CJ, Wallace DP, CookLT, Wetzel LH, et al. Detected renal cysts are tips of theiceberg in adults with ADPKD. Clin J Am Soc Nephrol.2012;7:1087-93.
4. Dalgaard OZ. Bilateral polycystic disease of the kidneys; afollow-up of two hundred and eighty-four patients and theirfamilies. Acta Med Scand Suppl. 1957;328:1-255.
5. Dicks E, Ravani P, Langman D, Davidson WS, Pei Y, ParfreyPS. Incident renal events and risk factors in autosomaldominant polycystic kidney disease: a population and family-based cohort followed for 22 years. Clin J Am Soc Nephrol.2006;1:710-7.
G.K. Rangan et al.564
6. Lufkin EG, Alfrey AC, Trucksess ME, Holmes JH. Polycystickidney disease: earlier diagnosis using ultrasound. Urology.1974;4:5-12.
7. Ravine D, Gibson RN, Donlan J, Sheffield LJ. An ultrasoundrenal cyst prevalence survey: specificity data for inherited renalcystic diseases. Am J Kidney Dis. 1993;22:803-7.
8. Chang CC, Kuo JY, Chan WL, Chen KK, Chang LS.Prevalence and clinical characteristics of simple renal cyst.J Chin Med Assoc. 2007;70:486-91.
9. Al-Said J, O’Neill WC. Reduced kidney size in patients withsimple renal cysts. Kidney Int. 2003;64:1059-64.
10. Hong S, Lim JH, Jeong IG, Choe J, Kim CS, Hong JH. Whatassociation exists between hypertension and simple renal cystin a screened population? J Hum Hypertens. 2013;27:539-44.
11. Ravine D, Gibson RN, Walker RG, Sheffield LJ, Kincaid-Smith P, Danks DM. Evaluation of ultrasonographic diagnosticcriteria for autosomal dominant polycystic kidney disease 1.Lancet. 1994;343:824-7.
12. Pei Y, Obaji J, Dupuis A, Paterson AD, Magistroni R, Dicks E,et al. Unified criteria for ultrasonographic diagnosis ofADPKD. J Am Soc Nephrol. 2009;20:205-12.
13. Rahbari-Oskoui F, Mittal A, Mittal P, Chapman A. Renalrelevant radiology: radiologic imaging in autosomal dominantpolycystic kidney disease. Clin J Am Soc Nephrol. 2014;9:406-15.
14. Milutinovic J, Fialkow PJ, Phillips LA, Agoda LY, Bryant JI,Denney JD, et al. Autosomal dominant polycystic kidneydisease: early diagnosis and data for genetic counselling.Lancet. 1980;1:1203-6.
15. Bear JC, McManamon P, Morgan J, Payne RH, Lewis H, GaultMH, et al. Age at clinical onset and at ultrasonographicdetection of adult polycystic kidney disease: data for geneticcounselling. Am J Med Genet. 1984;18:45-53.
16. Parfrey PS, Bear JC, Morgan J, Cramer BC, McManamon PJ, GaultMH, et al. The diagnosis and prognosis of autosomal dominantpolycystic kidney disease. N Engl J Med. 1990;323:1085-90.
17. Nicolau C, Torra R, Badenas C, Vilana R, Bianchi L, GilabertR, et al. Autosomal dominant polycystic kidney disease types
1 and 2: assessment of US sensitivity for diagnosis. Radiology.1999;213:273-6.
18. Papadopoulou D, Tsakiris D, Papadimitriou M. The use ofultrasonography and linkage studies for early diagnosis ofautosomal dominant polycystic kidney disease (ADPKD).Ren Fail. 1999;21:67-84.
19. Gabow PA, Kimberling WJ, Strain JD, Manco-Johnson ML,Johnson AM. Utility of ultrasonography in the diagnosis ofautosomal dominant polycystic kidney disease in children.J Am Soc Nephrol. 1997;8:105-10.
20. Bear JC, Parfrey PS, Morgan JM, Martin CJ, Cramer BC.Autosomal dominant polycystic kidney disease: new informa-tion for genetic counselling. Am J Med Genet. 1992;43:548-53.
21. Barua M, Cil O, Paterson AD, Wang K, He N, Dicks E, et al.Family history of renal disease severity predicts the mutatedgene in ADPKD. J Am Soc Nephrol. 2009;20:1833-8.
22. Pei Y. Practical genetics for autosomal dominant polycystickidney disease. Nephron. 2011;118:c19-30.
23. Nicolau C, Torra R, Bianchi L, Vilana R, Gilabert R, Darnell A,et al. Abdominal sonographic study of autosomal dominantpolycystic kidney disease. J Clin Ultrasound. 2000;28:277-82.
24. Zand MS, Strang J, Dumlao M, Rubens D, Erturk E, BronstherO. Screening a living kidney donor for polycystic kidneydisease using heavily T2-weighted MRI. Am J Kidney Dis.2001;37:612-9.
25. Pei Y, Hwang YH, Conklin J, Sundsbak JL, Heyer CM, ChanW, et al. Imaging-based diagnosis of autosomal dominantpolycystic kidney disease. J Am Soc Nephrol. 2015;26:746-53.
26. Wood CG 3rd, Stromberg LJ 3rd, Harmath CB, Horowitz JM,Feng C, Hammond NA, et al. CT and MR imaging forevaluation of cystic renal lesions and diseases. Radiographics.2015;35:125-41.
27. Ars E, Bernis C, Fraga G, Martinez V, Martins J, Ortiz A, et al.Spanish Working Group on Inherited Kidney Disease. Spanishguidelines for the management of autosomal dominant poly-cystic kidney disease. Nephrol Dial Transplant. 2014;29:(Suppl 4), 2014; iv95-105
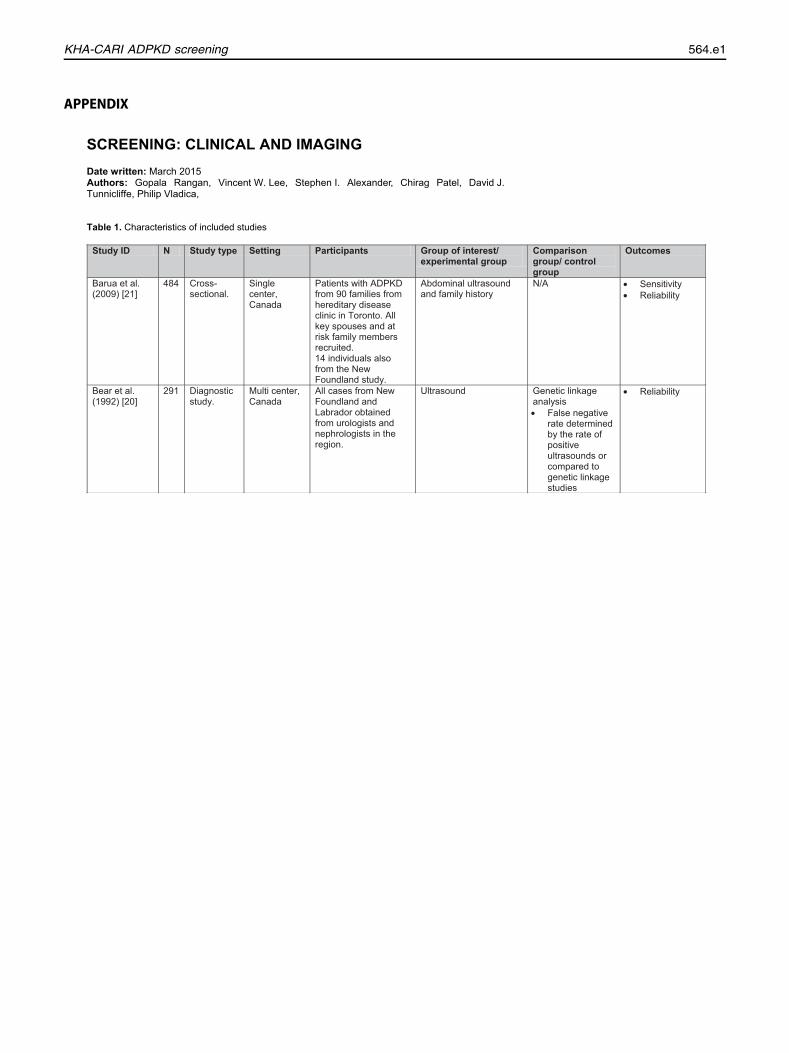
APPENDIX
Study ID N Study type Setting Participants Group of interest/ experimental group
Comparison group/ control group
Outcomes
Barua et al. (2009) [21]
484 Cross-sectional.
Single center, Canada
Patients with ADPKD from 90 families from hereditary disease clinic in Toronto. All key spouses and at risk family members recruited. 14 individuals also from the New Foundland study.
Abdominal ultrasound and family history
N/A • Sensitivity • Reliability
Bear et al. (1992) [20]
291 Diagnostic study.
Multi center, Canada
All cases from New Foundland and Labrador obtained from urologists and nephrologists in the region.
Ultrasound Genetic linkage analysis • False negative
rate determined by the rate of positive ultrasounds or compared to genetic linkage studies
• Reliability
SCREENING: CLINICAL AND IMAGING Date written: March 2015 Authors: Gopala Rangan, Vincent W. Lee, Stephen I. Alexander, Chirag Patel, David J. Tunnicliffe, Philip Vladica, Table 1. Characteristics of included studies
KHA-CARI ADPKD screening 564.e1
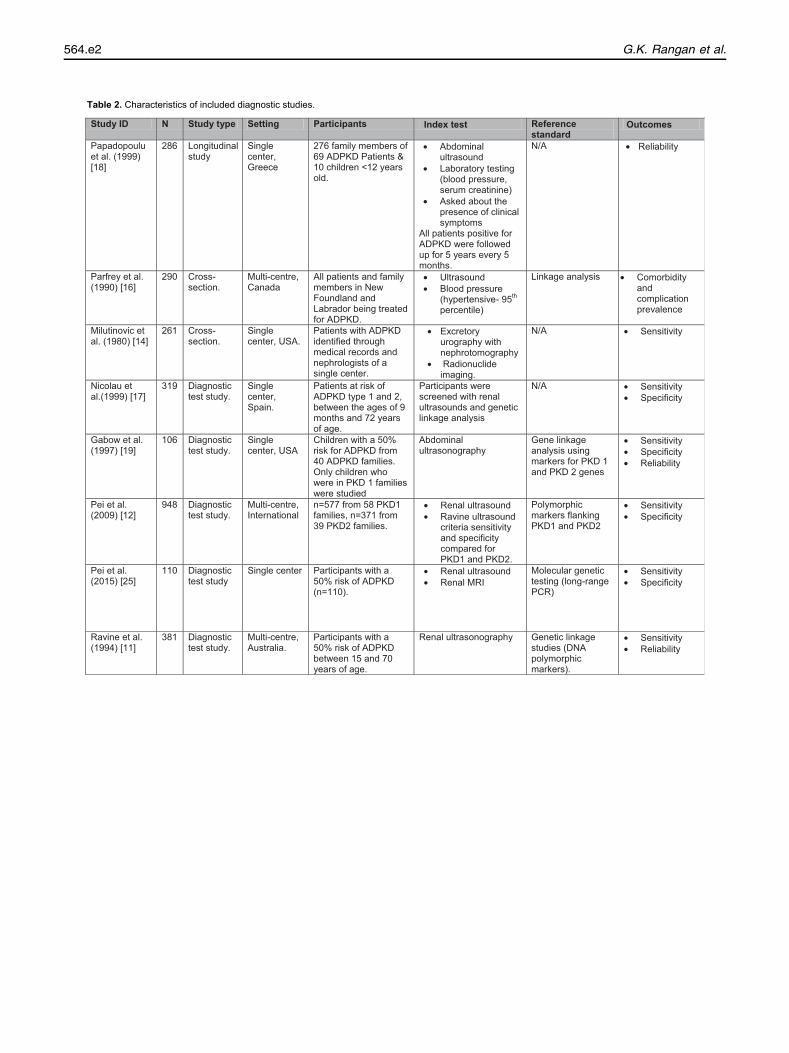
Study ID N Study type Setting Participants Index test Reference standard
Outcomes
Papadopoulu et al. (1999) [18]
286 Longitudinalstudy
Single center, Greece
276 family members of 69 ADPKD Patients & 10 children <12 years old.
• Abdominal ultrasound
• Laboratory testing (blood pressure, serum creatinine)
• Asked about the presence of clinical symptoms
All patients positive for ADPKD were followed up for 5 years every 5 months.
N/A • Reliability
Parfrey et al. (1990) [16]
290 Cross-section.
Multi-centre, Canada
All patients and family members in New Foundland and Labrador being treated for ADPKD.
• Ultrasound • Blood pressure
(hypertensive- 95th percentile)
Linkage analysis • Comorbidity and complication prevalence
Milutinovic et al. (1980) [14]
261 Cross-section.
Single center, USA.
Patients with ADPKD identified through medical records and nephrologists of a single center.
• Excretory urography with nephrotomography
• Radionuclide imaging.
N/A • Sensitivity
Nicolau et al.(1999) [17]
319 Diagnostic test study.
Single center, Spain.
Patients at risk of ADPKD type 1 and 2, between the ages of 9 months and 72 years of age.
Participants were screened with renal ultrasounds and genetic linkage analysis
N/A • Sensitivity • Specificity
Gabow et al. (1997) [19]
106 Diagnostic test study.
Single center, USA
Children with a 50% risk for ADPKD from 40 ADPKD families. Only children who were in PKD 1 families were studied
Abdominal ultrasonography
Gene linkage analysis using markers for PKD 1 and PKD 2 genes
• Sensitivity • Specificity • Reliability
Pei et al. (2009) [12]
948 Diagnostic test study.
Multi-centre, International
n=577 from 58 PKD1 families, n=371 from 39 PKD2 families.
• Renal ultrasound • Ravine ultrasound
criteria sensitivity and specificity compared for PKD1 and PKD2.
Polymorphic markers flanking PKD1 and PKD2
• Sensitivity • Specificity
Pei et al. (2015) [25]
110 Diagnostic test study
Single center Participants with a 50% risk of ADPKD (n=110).
• Renal ultrasound • Renal MRI
Molecular genetic testing (long-range PCR)
• Sensitivity • Specificity
Ravine et al. (1994) [11]
381 Diagnostic test study.
Multi-centre, Australia.
Participants with a 50% risk of ADPKD between 15 and 70 years of age.
Renal ultrasonography Genetic linkage studies (DNA polymorphic markers).
• Sensitivity • Reliability
Table 2. Characteristics of included diagnostic studies.
G.K. Rangan et al.564.e2
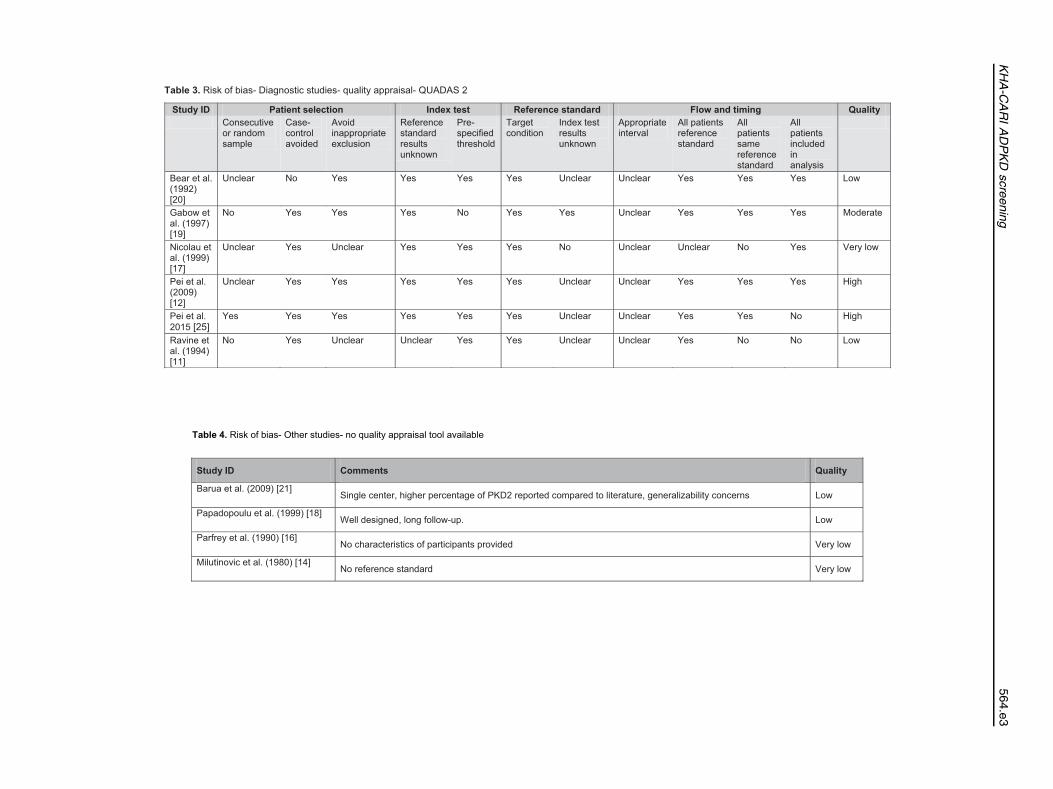
Study ID Patient selection Index test Reference standard Flow and timing Quality Consecutive
or random sample
Case-control avoided
Avoid inappropriate exclusion
Reference standard results unknown
Pre-specified threshold
Target condition
Index test results unknown
Appropriate interval
All patients reference standard
All patients same reference standard
All patients included in analysis
Bear et al. (1992) [20]
Unclear No Yes Yes Yes Yes Unclear Unclear Yes Yes Yes Low
Gabow et al. (1997) [19]
No Yes Yes Yes No Yes Yes Unclear Yes Yes Yes Moderate
Nicolau et al. (1999) [17]
Unclear Yes Unclear Yes Yes Yes No Unclear Unclear No Yes Very low
Pei et al. (2009) [12]
Unclear Yes Yes Yes Yes Yes Unclear Unclear Yes Yes Yes High
Pei et al. 2015 [25]
Yes Yes Yes Yes Yes Yes Unclear Unclear Yes Yes No High
Ravine et al. (1994) [11]
No Yes Unclear Unclear Yes Yes Unclear Unclear Yes No No Low
Table 3. Risk of bias- Diagnostic studies- quality appraisal- QUADAS 2
Study ID Comments Quality
Barua et al. (2009) [21] Single center, higher percentage of PKD2 reported compared to literature, generalizability concerns Low
Papadopoulu et al. (1999) [18] Well designed, long follow-up. Low
Parfrey et al. (1990) [16] No characteristics of participants provided Very low
Milutinovic et al. (1980) [14] No reference standard Very low
Table 4. Risk of bias- Other studies- no quality appraisal tool available
KHA-C
ARIADPKD
screening
564.e3
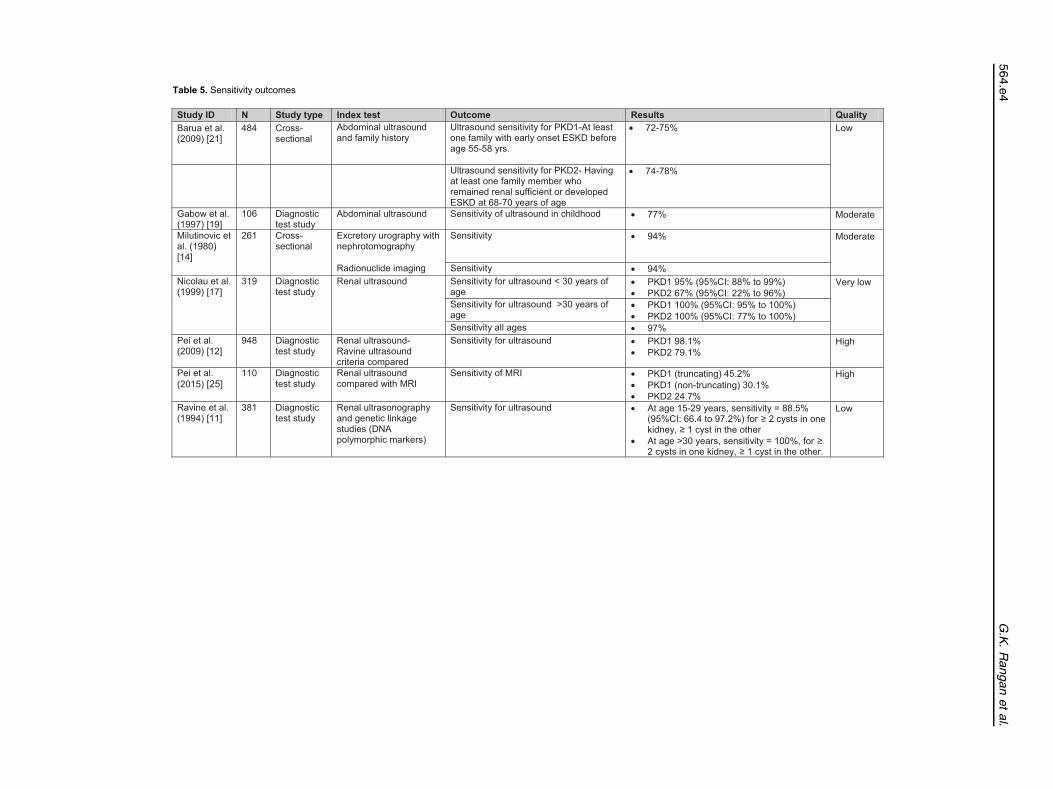
Study ID N Study type Index test Outcome Results Quality Barua et al. (2009) [21]
484 Cross-sectional
Abdominal ultrasound and family history
Ultrasound sensitivity for PKD1-At least one family with early onset ESKD before age 55-58 yrs.
• 72-75%
Low
Ultrasound sensitivity for PKD2- Having at least one family member who remained renal sufficient or developed ESKD at 68-70 years of age
• 74-78%
Gabow et al. (1997) [19]
106 Diagnostic test study
Abdominal ultrasound Sensitivity of ultrasound in childhood • 77% Moderate
Milutinovic et al. (1980) [14]
261 Cross-sectional
Excretory urography with nephrotomography
Sensitivity • 94% Moderate
Radionuclide imaging Sensitivity • 94% Nicolau et al. (1999) [17]
319 Diagnostic test study
Renal ultrasound Sensitivity for ultrasound < 30 years of age
• PKD1 95% (95%CI: 88% to 99%) • PKD2 67% (95%CI: 22% to 96%)
Very low
Sensitivity for ultrasound >30 years of age
• PKD1 100% (95%CI: 95% to 100%) • PKD2 100% (95%CI: 77% to 100%)
Sensitivity all ages • 97% Pei et al. (2009) [12]
948 Diagnostic test study
Renal ultrasound- Ravine ultrasound criteria compared
Sensitivity for ultrasound • PKD1 98.1% • PKD2 79.1%
High
Pei et al. (2015) [25]
110 Diagnostic test study
Renal ultrasound compared with MRI
Sensitivity of MRI • PKD1 (truncating) 45.2% • PKD1 (non-truncating) 30.1% • PKD2 24.7%
High
Ravine et al. (1994) [11]
381 Diagnostic test study
Renal ultrasonography and genetic linkage studies (DNA polymorphic markers)
Sensitivity for ultrasound • At age 15-29 years, sensitivity = 88.5% (95%CI: 66.4 to 97.2%) for ≥ 2 cysts in one kidney, ≥ 1 cyst in the other
• At age >30 years, sensitivity = 100%, for ≥ 2 cysts in one kidney, ≥ 1 cyst in the other.
Low
Table 5. Sensitivity outcomes
G.K.Ranganetal.
564.e4
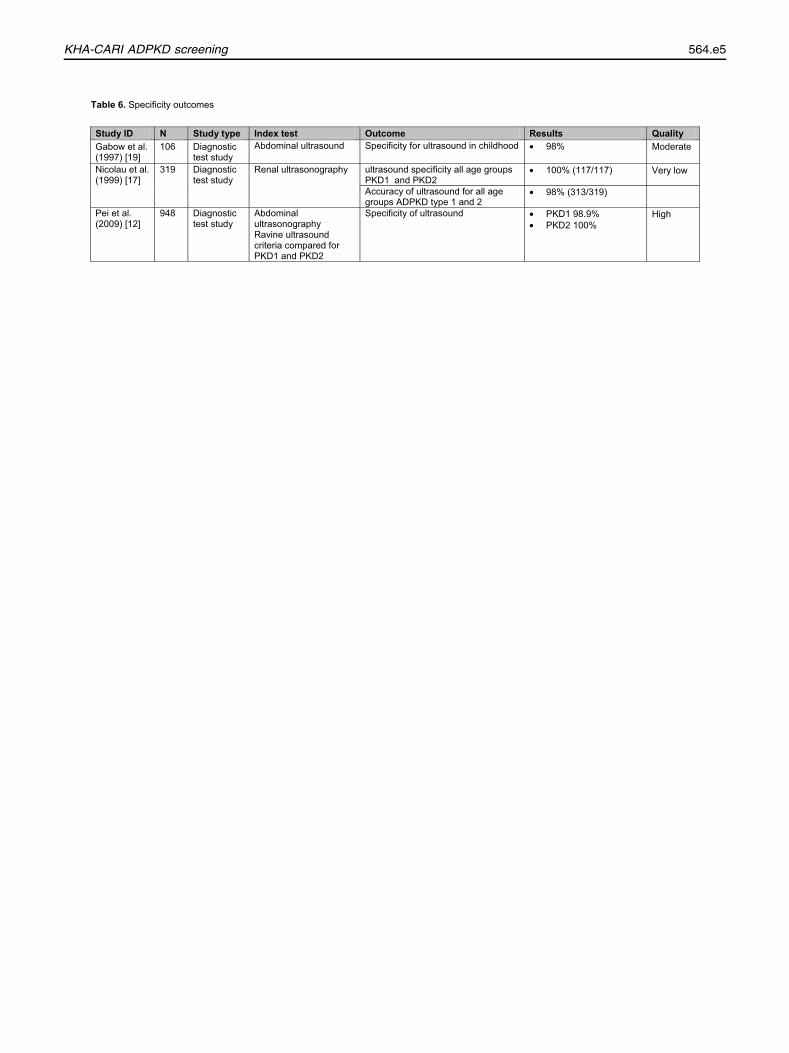
Study ID N Study type Index test Outcome Results Quality Gabow et al. (1997) [19]
106 Diagnostic test study
Abdominal ultrasound
Specificity for ultrasound in childhood • 98% Moderate
Nicolau et al. (1999) [17]
319 Diagnostic test study
Renal ultrasonography
ultrasound specificity all age groups PKD1 and PKD2
• 100% (117/117) Very low
Accuracy of ultrasound for all age groups ADPKD type 1 and 2
• 98% (313/319)
Pei et al. (2009) [12]
948 Diagnostic test study
Abdominal ultrasonography Ravine ultrasound criteria compared for PKD1 and PKD2
Specificity of ultrasound • PKD1 98.9% • PKD2 100%
High
Table 6. Specificity outcomes
KHA-CARI ADPKD screening 564.e5
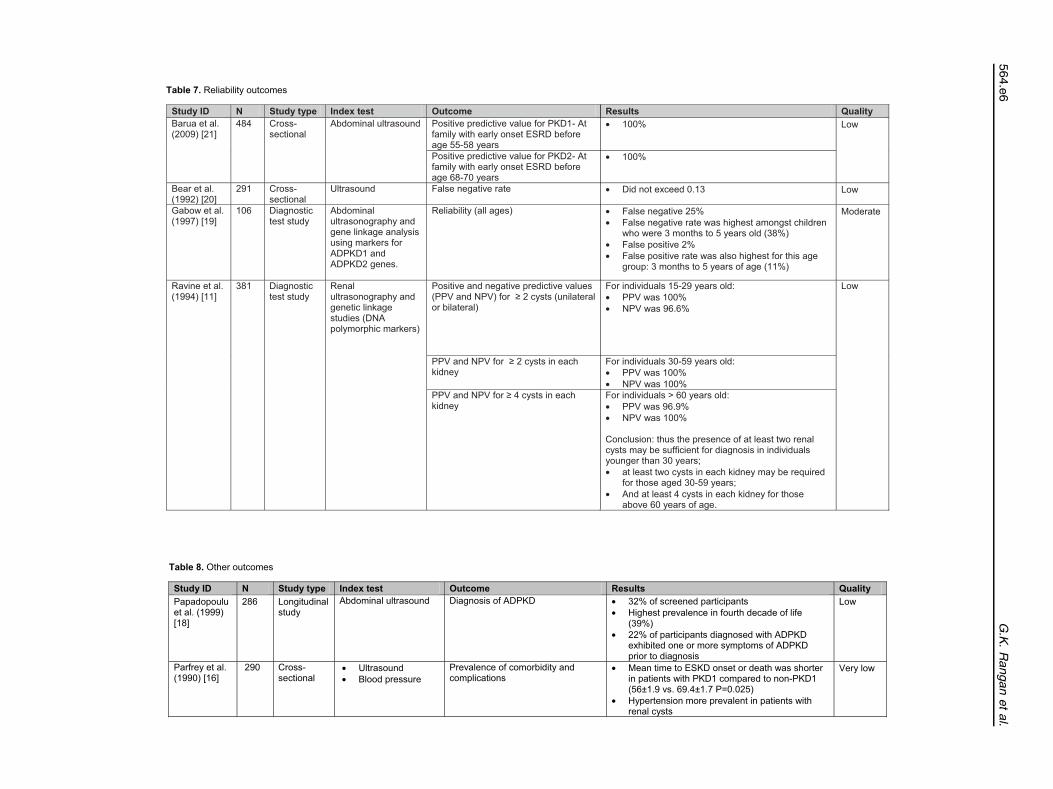
Study ID N Study type Index test Outcome Results Quality Barua et al. (2009) [21]
484 Cross-sectional
Abdominal ultrasound Positive predictive value for PKD1- At family with early onset ESRD before age 55-58 years
• 100% Low
Positive predictive value for PKD2- At family with early onset ESRD before age 68-70 years
• 100%
Bear et al. (1992) [20]
291 Cross-sectional
Ultrasound False negative rate • Did not exceed 0.13 Low
Gabow et al. (1997) [19]
106 Diagnostic test study
Abdominal ultrasonography and gene linkage analysis using markers for ADPKD1 and ADPKD2 genes.
Reliability (all ages) • False negative 25% • False negative rate was highest amongst children
who were 3 months to 5 years old (38%) • False positive 2% • False positive rate was also highest for this age
group: 3 months to 5 years of age (11%)
Moderate
Ravine et al. (1994) [11]
381 Diagnostic test study
Renal ultrasonography and genetic linkage studies (DNA polymorphic markers)
Positive and negative predictive values (PPV and NPV) for ≥ 2 cysts (unilateral or bilateral)
For individuals 15-29 years old: • PPV was 100% • NPV was 96.6%
Low
PPV and NPV for ≥ 2 cysts in each kidney
For individuals 30-59 years old: • PPV was 100% • NPV was 100%
PPV and NPV for ≥ 4 cysts in each kidney
For individuals > 60 years old: • PPV was 96.9% • NPV was 100%
Conclusion: thus the presence of at least two renal cysts may be sufficient for diagnosis in individuals younger than 30 years; • at least two cysts in each kidney may be required
for those aged 30-59 years; • And at least 4 cysts in each kidney for those
above 60 years of age.
Table 7. Reliability outcomes
Study ID N Study type Index test Outcome Results Quality Papadopoulu et al. (1999) [18]
286 Longitudinal study
Abdominal ultrasound
Diagnosis of ADPKD • 32% of screened participants • Highest prevalence in fourth decade of life
(39%) • 22% of participants diagnosed with ADPKD
exhibited one or more symptoms of ADPKD prior to diagnosis
Low
Parfrey et al. (1990) [16]
290 Cross-sectional
• Ultrasound • Blood pressure
Prevalence of comorbidity and complications
• Mean time to ESKD onset or death was shorter in patients with PKD1 compared to non-PKD1 (56±1.9 vs. 69.4±1.7 P=0.025)
• Hypertension more prevalent in patients with renal cysts
Very low
Table 8. Other outcomes
G.K.Ranganetal.
564.e6







![Clinical manifestations of autosomal recessive polycystic kidney ... · viduals to survive the perinatal period [ 8, 10]. Pulmonaryhypoplasia,aserio uscomplicationthatgenerally occurs](https://img.dokumen.tips/doc/110x75/5f09f6827e708231d4295907/clinical-manifestations-of-autosomal-recessive-polycystic-kidney-viduals-to.jpg)