Embed Size (px)
Citation preview

Key Issues in Drug Interac0ons in the DAA Era.
David Back -‐ Liverpool, UK

Disclosures • Honoraria received from Gilead, Janssen, Merck, Abbvie, BMS, Boehringer-‐Ingelheim, Viiv.
• Research or EducaConal Grant support from Gilead, Janssen, Merck, Abbvie, Roche, Vertex, BMS, Boehringer-‐Ingelheim, Viiv.
• PresentaCon refers to the following unlabelled/unapproved drugs: faldaprevir, daclatasvir, asunaprevir, ledipasvir, ABT-‐450/r, ABT-‐267, ABT-‐333; MK-‐5172, MK-‐8742.

HCV DAAs: a success story of multiple disciplines.
Ø Molecular Virology Deciphered the viral replication cycle and identified druggable targets.
Ø Structural Biology Provided high-resolution structures of viral targets such as NS3, NS5A and NS5B – allowing modelling of drug-target interactions
Ø Molecular & Clinical Pharmacology Shown the disposition profiles of the compounds and helped develop strategies to optimise therapies – in particular in relation to drug-drug interactions.

Anti-HCV drugs approved and in advanced development
Manns M & van Hahn Nature Rev Drug Discovery, 2013; 12: 595-610

Direct Acting Antivirals against HCV

DAA Co-med*
Reduced Efficacy
Toxicity
Concentration of DAA
Concentration of Co-med
Drug- Drug Interactions
* The Co-med may be an antiretroviral

DAA Co-med
Perpetrator
Victim

1st Generation DAAs Telaprevir and Boceprevir
Statement from Page 20 of www.hcvguidelines.org

Drug CYP 3A4 Transporters Non-CYP
metabolism
Telaprevir § Metabolised by § Inhibits
§ Transported by P-gp § Inhibits P-gp;
OATP1B1/2 –
Boceprevir § Metabolised by § Inhibits
§ Transported by P-gp; BCRP
§ Inhibits P-gp; OCT1/2
AKR § Metabolised
by
Telaprevir and Boceprevir Interactions: What have we learned?
P-gp: P-glycoprotein; AKR: aldo-keto reductase
CYP 3A isozymes are § The most abundant CYP enzymes in the liver § Involved in the metabolism of many drugs
Kessara C et al 18th CROI, Abs 118; Garg V et al 18th CROI, Abs 629; Telaprevir SmPC, 2013; Boceprevir SmPC, 2013; Kiser JJ et al Hepatology 2012; 55: 1620-1628; Kunze A et al Biochem Pharmacol 2012; 84: 1096-1102.

Slide 10 Importance of metabolism and transport in relation to systemic drug levels
Adapted from: Bailey DG, et al. CMAJ 2013;185:1066
Enterocytes
Hepatocytes drug
100%
1
2
CYP3A4
P-‐gp BCRP MRP2
OATP1A2 OATP2B1
CYP3A4
UGTs
OATP1B1 OATP1B3 OCT1
Ø Dissolution Ø Food effects
Ø Enzyme induction/inhibition Ø Transporter induction/
inhibition
CYP 1A2 CYP 2A6 CYP 2B6
CYP 2C8 CYP 2C9
CYP 2C19 CYP 2D6
CYP 2E1 CYP 3A

Slide 11
q If clearance of co-med involves just CYP3A4 – co-med levels increase.
q But if other or additional metabolic pathways – co-med levels could decrease.
q There may be other interaction mechanisms (eg protein binding)
Telaprevir and Boceprevir Interactions: What have we learned?

Co-meds cleared by CYP3A4: TVR and BOC are Perpetrators of marked interactions
Drug TVR effect on the AUC (exposure)
BOC effect on the AUC (exposure)
Cyclosporine A
4.6-fold increase 2.7-fold increase
Tacrolimus
70-fold increase 17-fold increase
Midazolam 9-fold increase (oral) 6.3-fold increase (oral)
Atorvastatin 7.9-fold increase 2.3-fold increase
Amlodipine
2.8-fold increase
May be increased
Garg V, et al. Heptatology 2011:54:20–27; Garg V, et al. J Clin Pharmacol 2012 ; Lee JE, et al. Antimicrob Agents Chemother 2011;55:4569–74; Telaprevir SmPC; Hulskotte EGJ et al HEPDart 2011; Abs 122 and Abs 123; Kessara C et al, CROI 2011, Abs 118; Boceprevir SmPC

ARVs cleared by CYP3A4: Maraviroc (major), Rilpivirine (major), Raltegravir
(minor; UGT1A1 is major) - Predictable
§ Finding consistent with CYP3A
inhibition § Is increase in RPV exposure clinically significant? Note: No dose adjustment recommended.
De Kanter C et al CID 2013; 56: 300-306 van Heeswijk R et al; ICAAC 2011; Vourvahis M et al IWCPHT, 2013; Abs O-17
ARV exposure (AUC) Effect of TVR Effect of BOC
Maraviroc ↑ 9-fold ↑ 3-fold
Rilpivirine ↑ 78% ↑ 39%
Raltegravir ↑ 31% ↑ 4%
Clin Pharm Review FDA Sept 2011 Eviplera SmPC 31/10/13

Why is exposure of boosted HIV PIs mainly decreased in healthy volunteer studies?
Effect of TVR & BOC on HIV Boosted PI concentrations
NOTE: RTV inhibits ~95% of CYP3A activity so TVR & BOC exert other effects.
Effect of HIV Boosted on TVR & BOC concentrations
Complex enzyme – transporter interplay between the 3 components ie DAA, HIV PI, RTV; Also protein binding displacement or even absorption
effects.
Are drug interactions different in HCV patients compared to healthy subjects?
Ø Evidence that drug exposure in plasma of some DAAs is altered (note: hepatic impairment)
Ø Changes in protein binding in liver disease. Ø Evidence that enzyme activity is altered in liver
disease
Ø Some evidence from co-infection that the magnitude of an interaction may be different.

Effect of Mild or Moderate Hepatic Impairment on DAA PK
Drug Mild Moderate
Telaprevir AUC decreased 15% AUC decreased 46%A
Boceprevir No change No change
Simeprevir AUC increased 2.4-fold
Sofosbuvir AUC increased 2.3-fold
Daclatasvir AUC decreased 43% AUC decreased 40%
Asunaprevir AUC decreased 21% AUC increased 9.8-fold
Faldaprevir No change in cirrhotics
www.hep-druginteractions.org
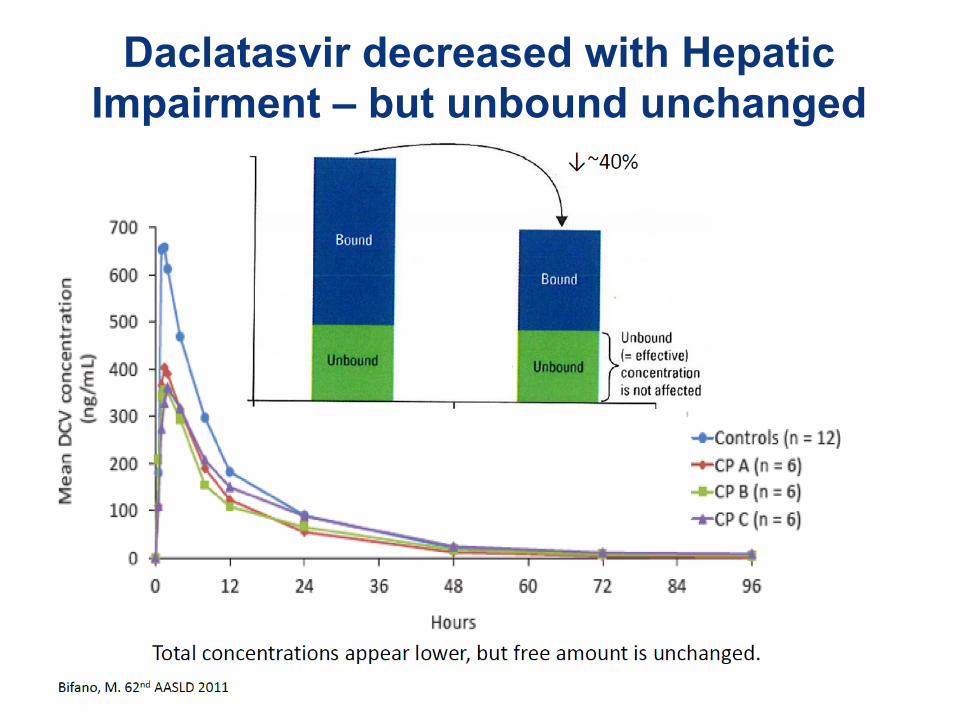
Daclatasvir decreased with Hepatic Impairment – but unbound unchanged
Are drug interactions different in HCV patients compared to healthy subjects?
Ø Evidence that drug exposure in plasma of some DAAs is altered (note: hepatic impairment)
Ø Changes in protein binding in liver disease
Ø Evidence that enzyme activity is altered in liver disease
Ø Some evidence from co-infection that the magnitude of an interaction may be different.

Sofosbuvir
Not metabolised by CYP No inhibition of CYP
Interaction with intestinal P-gp & BCRP (Victim)

Sofosbuvir Intracellular Activation
SOF is activated in hepatocyte § Hydrolases – CES1, cathepsin A; HNT1
§ Phosphorylation to active GS-4612003
§ Predominant circulating metabolite is GS-331007
Gilead – with permission

Effect of ARVs on Sofosbuvir: Victim Drug Effect on Sofosbuvir and
GS-331007 AUC (exposure) Recommendation
Darunavir/r
SOF increased 34%; GS-331007 – no effect
No dose adjustment
Rilpivirine
No effect on SOF or GS-331007 No dose adjustment
Efavirenz No effect on SOF or GS-331007 No dose adjustment
Raltegravir No effect on SOF or
GS-331007: RAL decreased 27%
No dose adjustment
Tenofovir No effect on SOF or GS-331007
No dose adjustment
Mathias A 14th Int Workshop on Clin Pharm of HIV Ther Session 5; Kirby B et al 63rd AASLD 2012; Abs 1877. ; Sofosbuvir USPI 2013
No known or anticipated interactions with antiretrovirals

Effect of Other Co-administered Drugs on Sofosbuvir: Victim
Drug Effect on Sofosbuvir and GS-331007 AUC (exposure) Recommendation
Methadone (multiple dose)
SOF increased 30%; no effect on GS-331007
No dose adjustment
Cyclosporine
SOF increased 4-fold but no effect on GS-331007 No dose adjustment
Tacrolimus No effect on SOF or GS-331007 No dose adjustment
Rifampicin Rifampicin is a potent P-gp inducer* Not recommended
Mathias A 14th Int Workshop on Clin Pharm of HIV Ther Session 5; Kirby B et al 63rd AASLD 2012; Abs 1877. ; Sofosbuvir USPI 2013

Sofosbuvir and P-gp Induction
• Potent P-gp inducers in the intestine (rifampicin, St. John's wort, carbamazepine and phenytoin) may significantly decrease sofosbuvir plasma concentration leading to reduced therapeutic effect. Sofosbuvir should not be co-administered with known inducers of P-gp.
• Other P-gp inducers eg modafanil?
Sovaldi SPc – accessed March 10th 2014

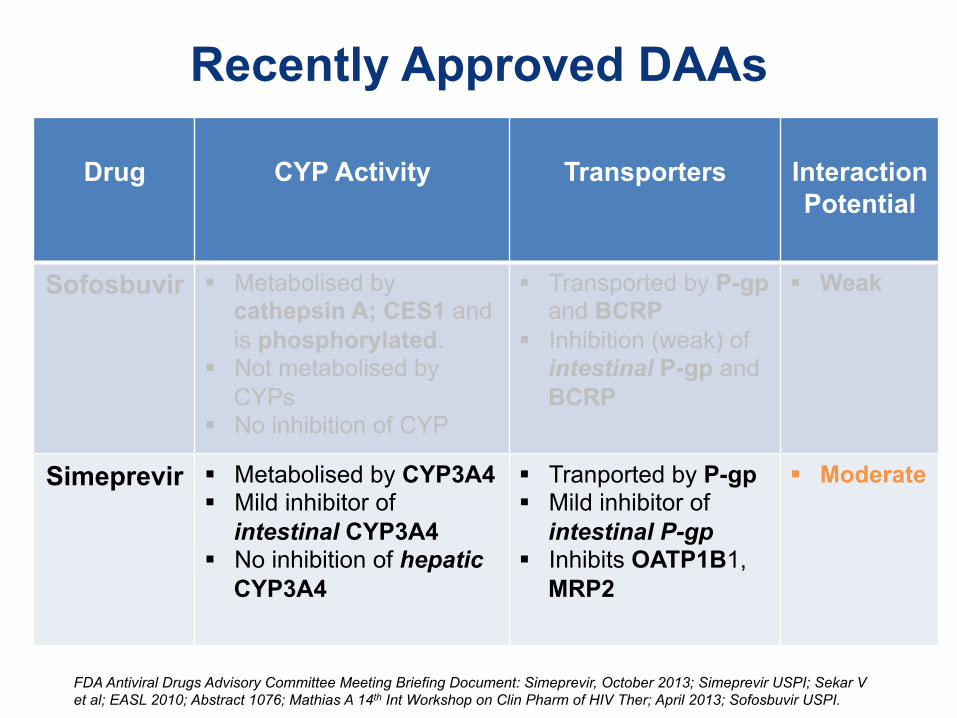
Recently Approved DAAs
Drug
CYP Activity
Transporters
Interaction Potential
Sofosbuvir § Metabolised by cathepsin A; CES1 and is phosphorylated.
§ Not metabolised by CYPs
§ No inhibition of CYP
§ Transported by P-gp and BCRP
§ Inhibition (weak) of intestinal P-gp and BCRP
§ Weak
Simeprevir § Metabolised by CYP3A4 § Mild inhibitor of
intestinal CYP3A4 § No inhibition of hepatic
CYP3A4
§ Tranported by P-gp § Mild inhibitor of
intestinal P-gp § Inhibits OATP1B1,
MRP2
§ Moderate
FDA Antiviral Drugs Advisory Committee Meeting Briefing Document: Simeprevir, October 2013; Simeprevir USPI; Sekar V et al; EASL 2010; Abstract 1076; Mathias A 14th Int Workshop on Clin Pharm of HIV Ther; April 2013; Sofosbuvir USPI.

Simeprevir
Metabolised by CYP3A4 (Victim) Mild inhibitor of CYP3A4 in intestine
Inhibits OATP1B1 (Perpetrator) Small Intes0nes
Efflux
Influx
Influx
Liver
Efflux
OATP
CYP3A CYP3A UGT

Effect of ARVs on Simeprevir: Victim Drug Effect on Simeprevir AUC
(exposure) Mechanism/
Recommendation
Darunavir/r
2.6-fold increase (DRV increased 18%)
RTV Inhibits CYP3A4
Not recommended
Rilpivirine
No effect No dose adjustment
Efavirenz 70% decrease EFV induces CYP3A4 Not recommended
Raltegravir 11% decrease
No dose adjustment
Tenofovir 14% decrease (TFV increase 18%)
Intestine or renal transport No dose adjustment
Ouwerkerk-Mahadevan S et al, IDSA 2012; Abs 1618; Ouwerkerk-Mahadevan S et al, CROI 2012; Abs 49 ; Simeprevir (Olysio) USPI

Permitted Antiretrovirals with Simeprevir
1st Agent NRTIs
Raltegravir Tenofovir Maraviroc Emtricitabine Rilpivirine Lamivudine
Abacavir
www.hcvguidelines.org.

Effect of Simeprevir on Statins: Perpetrator
Drug Effect of Simeprevir on Sta0n AUC
Mechanism/ Recommenda)on
AtorvastaCn
2.1-‐fold increase
CYP3A & OATP1B1 inhibiCon
Use lowest dose
RosuvastaCn
3.2-fold increase OATP1B1 inhibition Initiate with 5mg
Simvastatin 40% increase CYP3A inhibition Titrate dose carefully
Simprevir (Olysio) USPi 2013
Recently Approved DAAs
Drug
CYP Activity
Transporters
Interaction Potential
Sofosbuvir § Metabolised by cathepsin A; CES1 and is phosphorylated.
§ Not metabolised by CYPs
§ No inhibition of CYP
§ Transported by P-gp and BCRP
§ Inhibition (weak) of intestinal P-gp and BCRP
§ Weak
Simeprevir § Metabolised by CYP3A4 § Mild inhibitor of
intestinal CYP3A4 § No inhibition of hepatic
CYP3A4
§ Tranported by P-gp § Mild inhibitor of
intestinal P-gp § Inhibits OATP1B1,
MRP2
§ Moderate
FDA Antiviral Drugs Advisory Committee Meeting Briefing Document: Simeprevir, October 2013; Simeprevir USPI; Sekar V et al; EASL 2010; Abstract 1076; Mathias A 14th Int Workshop on Clin Pharm of HIV Ther; April 2013; Sofosbuvir USPI.

Faldaprevir
Metabolised by CYP3A4 Transported by P-gp, OATP1B1, MRP2
(Victim) Inhibition of CYP3A4 (at high dose)
Inhibition of UGT1A1 Probable inhibition of OATP1B1, MRP2
(Perpetrator)

Faldaprevir and Bilirubin Disposition
Ø Faldaprevir is associated with hyperbilirubinemia largely due to unconjugated BIL
Sane R et al J Hepatology 2011; 54 (Suppl 1) S488

Drug Effect of ARV on FDV AUC
Victim
Effect of FDV on ARV AUC Perpetrator
Mechanism/ Recommendation
Darunavir/r
2.29-fold increase
15% increase (Healthy) but
50% decrease (HIV-HCV)
RTV Inhibits CYP3A4 Use FDV at 120 mg/day
Atazanavir/r 2.19-fold increase
No effect (HIV-HCV)
RTV Inhibits CYP3A4 Use FDV at 120 mg/day
Efavirenz 35% decrease 16% increase (Healthy)
EFV induces CYP3A4 Use FDV at 240 mg/day
Raltegravir No effect 2.7-fold increase (Healthy) FDV likely inhibits P-gp
Tenofovir 22% decrease 22% increase (Healthy)
Intestinal/renal transport
No dose adjustment Sabo J et al ICCA 2012; Sabo J et al CROI 2013; Nelson M et al CROI 2014; Abs 499; Rockstroh J et al CROI 2014; Abs 497;
Joseph D et al; CROI 2014; Abs 501
Interaction of Faldaprevir (FDV) and ARVs

Faldaprevir Drug Interactions: Perpetrator
Ø Faldaprevir showed moderate inhibition of CYP3A4 and weak inhibition of CYP2C9 and 2C19.
Sabo J et al ICAAC 2012; A-1248

Daclatasvir
Metabolised by CYP3A4 Transported by P-gp
(Victim) Inhibits P-gp and OATP1B1
(Perpetrator)

Effect of Co-adminstered drugs on Daclatasvir: Victim
Drug Effect on Daclatasvir Recommendation
Atazanavir/r
DCV AUC increased 2.1-fold DCV Cmin increased 3.6-fold
Decrease dose to 30mg
Efavirenz
DCV AUC decreased 32% DCV Cmin decreased 59% Increase dose to 90 mg
Tenofovir No effect No dose adjustment
Omeprazole DCV AUC decreased 18% No dose adjustment
Bifano M et al 2013; 18: 931-941; Bifano M et al; 2013;EASL Abs 794.;

Effect of Daclatasvir on Co-meds: Perpetrator
Drug Effect of Daclatasvir on co-med Recommendation
Sofosbuvir
SOF AUC increased 35%; GS-331007 – no effect
No dose adjustment
Midazolam
MDZ AUC decreased 13% No dose adjustment
Cyclosporine No effect on CsA No dose adjustment
Tacrolimus No effect on TAC No dose adjustment
Oral Contraceptive
No effect on EE; Norgestrel AUC increased 12%
No dose adjustment
Eley T et al. 2013. 8th IWCPHepTHer Abs O-14; Eley T et al. 2013. 8th IWCPHepTHer Abs O-15; Bifano M et al, CROI 2014; Abs 502; Bifano M et al 2011; 62nd AASLD; ABS 1340.

DAAs in Development
Drug
CYP/enzyme Activity
Transporters
Interaction Potential
Faldaprevir § Metabolised by
CYP3A4 § Inhibits CYP3A4 (240
mg dose) § Inhibits CYP2C9 (240
mg dose) § Inhibits UGT1A1
§ Transported by P-gp, MRP2, OATP1B1
§ Probable inhibitor of OATP1B1/3; MRP2
§ Moderate
Daclatasvir § Metabolised by CYP3A4
§ Does not inhibit major CYPs
§ Transported by P-gp
§ Inhibits OATP1B1; P-gp
§ Moderate
Kort J 2013; 14th Int Workshop on Clin Pharm of HIV Ther, Session 5; Sane R et al 2011, 46th EASL, Abs 1236; Sabo JP et al, 52nd ICAAC, Abs A-1248; Bertz R 2013; 14th Int Workshop on Clin Pharm of HIV Ther, Session 5; Bifano M et al, 2013, 8th Int Workshop on Clin Pharm of Hep Ther, Abs O-15; Amblard F et al; Bioorg Med Chem Lett 23; 2031-2034.

DAAs in Development
Drug
CYP Ac0vity
Transporters
Interac0on Poten0al
Ledipasvir § Little metabolism § Not Inhibitor of CYP
or UGT § Not Inducer of CYP
or UGT
§ Transported by P-gp (likely)
§ Inhibits intestinal P-gp (weak)
§ Inhibits OATP1B1/3 (weak)
§ Weak
Asunaprevir § Metabolised by CYP3A4
§ Induces CYP3A4 (weak)
§ Inhibits CYP2D6 (weak)
§ Transported by P-gp, OATP1B1/3
§ Inhibits P-gp (weak), OATP1B1/3
§ Moderate
Eley T et al, 2013, 8th Int Workshop on Clin Pharm of Hep Ther; Abs O-13; Eley T et al, 2011, 62nd AASLD Abs 381; Eley T et al 2012, 7th Int Workshop on Clin Pharm of Hep Ther; Abs O-4; Kirby B et al 2013, 8th Int Workshop on Clin Pharm of Hep Ther; Abs O-20; Mathias A, 14th Int Workshop on Clin Pharm of HIV Ther, Session 5

Abbvie 3D (ABT-‐450/r; ABT-‐267; ABT-‐333)
Drug
CYP/enzyme Activity
Transporters
Interaction Potential
ABT-450 § Metabolised by
CYP3A4 § Inhibits CYP2C8 § Inhibits UGT1A1
§ Transported by P-gp, OATP1B1
§ Inhibits OATP1B1 and OATP1B3
§ High
ABT-267 § Metabolised by CYP3A4
§ Inhibits CYP2C8 § Inhibits UGT1A1
§ Transported by P-gp
§ Moderate
ABT-333 § Metabolised by CYP2C8 > CYP3A4 > CYP2D6
§ Inhibits UGT1A1
§ Transported by P-gp
§ Inhibits OATP1B1
§ Moderate
Abbvie – Personal Communication

Note
Ø Ritonavir has effects on multiple enzymes and transporters.
Ø Formal drug interaction studies performed with either the 3-DAA regimen or the 2-DAA combination of ABT-450/r + ABT-333

Merck drugs (MK-‐5172 and MK-‐8742)
Drug
CYP/enzyme Activity
Transporters
Interaction Potential
MK-5172 § Metabolised by CYP3A4
§ Inhibits (weak) CYP3A4 § Inhibits CYP2C8 § Inhibits UGT1A1 (weak)
§ Transported by P-gp & OATP1B1 § Inhibits BCRP?
§ Moderate
MK-8742 § Metabolised by CYP3A4 § Does not Inhibit CYP3A4 § Inhibits UGT1A1 (weak)
§ Transported by P-gp
§ Transported by OATP1B1 (?)
§ Moderate
Yeh WW, HEP Dart 2013; Abs 52; Yeh WW et al CROI 2014, Abs 498 & Abs 638.

HCV DDIs

Web resources § Drug interactions
– http://www.drugs.com/drug_interactions.html
– http://www.medscape.com/druginfo/druginterchecker – http://www.drugstore.com/pharmacy/drugchecker/
– http://drugchecker.aol.com
§ List of CYP substrates, inhibitors, inducers – http://medicine.iupui.edu/clinpharm/ddIs
§ HIV drug interactions – http://www.hiv-druginteractions.org
§ Hepatitis interactions – http://www.hep-druginteractions.org

OATP1A2
DDIs: Always be aware of unexpected!

A stepwise approach to DDI management
OTC: over the counter
Note all co-medications (prescribed, OTC and herbal products)
Consult pharmacist and online resources
Consider temporary interruption of co-medication if interaction is anticipated OR seek alternative drug
Many interactions can be managed by dose adjustment. However, monitoring is required
1
2
3
4
Acknowledgements
Grateful thanks to the Liverpool Website team: Saye Khoo Sara Gibbons Fiona Marra Catia Marzolini Justin Chiong
Back Ups

Alimentary Pharmacology Theraputics 2013: 38: 1365-1372
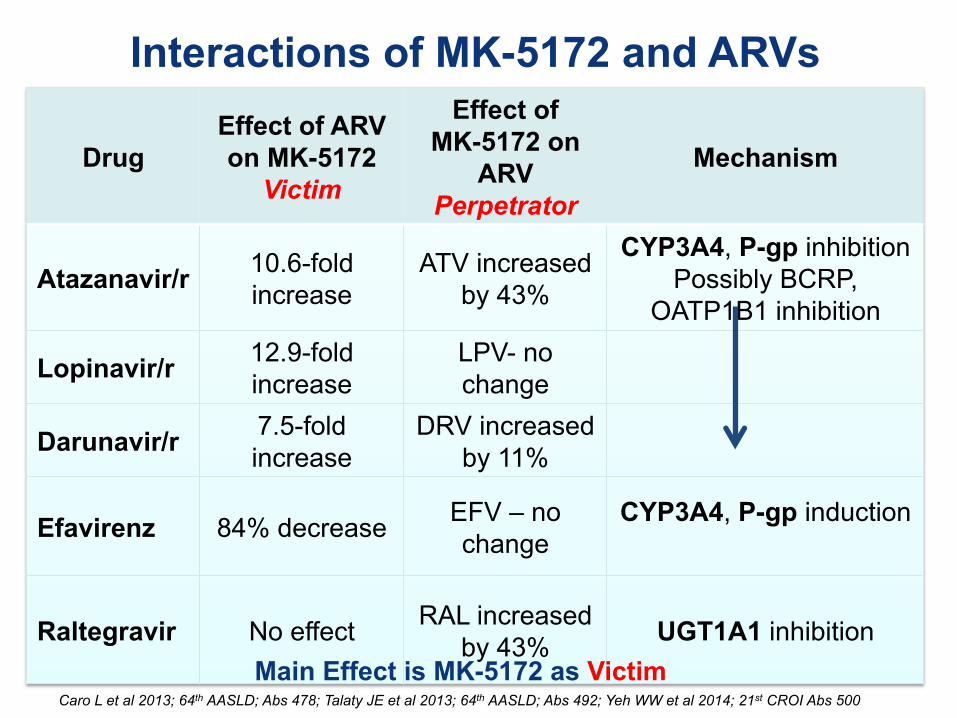
Drug Effect of ARV on MK-5172
Victim
Effect of MK-5172 on
ARV Perpetrator
Mechanism
Atazanavir/r 10.6-fold increase
ATV increased by 43%
CYP3A4, P-gp inhibition Possibly BCRP,
OATP1B1 inhibition
Lopinavir/r 12.9-fold increase
LPV- no change
Darunavir/r 7.5-fold increase
DRV increased by 11%
Efavirenz 84% decrease EFV – no change
CYP3A4, P-gp induction
Raltegravir No effect RAL increased by 43% UGT1A1 inhibition
Caro L et al 2013; 64th AASLD; Abs 478; Talaty JE et al 2013; 64th AASLD; Abs 492; Yeh WW et al 2014; 21st CROI Abs 500
Interactions of MK-5172 and ARVs
Main Effect is MK-5172 as Victim

Effect of MK-5172 on Co-meds: Perpetrator
Drug Effect of MK-5172 on co-med Recommendation
Midazolam
MDZ AUC decreased 34% Monitor
Pitavastatin PIT AUC increased 11% No dose adjustment
Atorvastatin ATOR AUC increased 3-fold Start with lowest dose
Oral Contraceptive
EE AUC increased 10% LNG AUC increased 23%
Not considered clinically relevant
Daclatasvir DAC Ctrough increased 23% No dose adjustment
Yeh WW et al 2013; 64th AASLD; Abs 464; Caro L et al 2013; 64th AASLD; Abs 477; Yeh WW, 2013; HEPDART Abs 53.

Drug Effect of ARV on MK-8742
Victim
Effect of MK-8742 on
ARV Perpetrator
Mechanism
Atazanavir/r 4.8-fold increase ATV- no change CYP3A4, P-gp inhibition
Possibly OATP1B1 inhibition
Lopinavir/r 3.7-fold increase LPV- no change
Darunavir/r 1.7-fold increase DRV- no change
Efavirenz 54% decrease 18% decrease
CYP3A4, P-gp induction
Raltegravir 19% decrease RAL- no change -
Yeh WW et al 2014; 21st CROI Abs 498 and 638
Interactions of MK-8742 and ARVs
Main Effect is MK-8742 as Victim
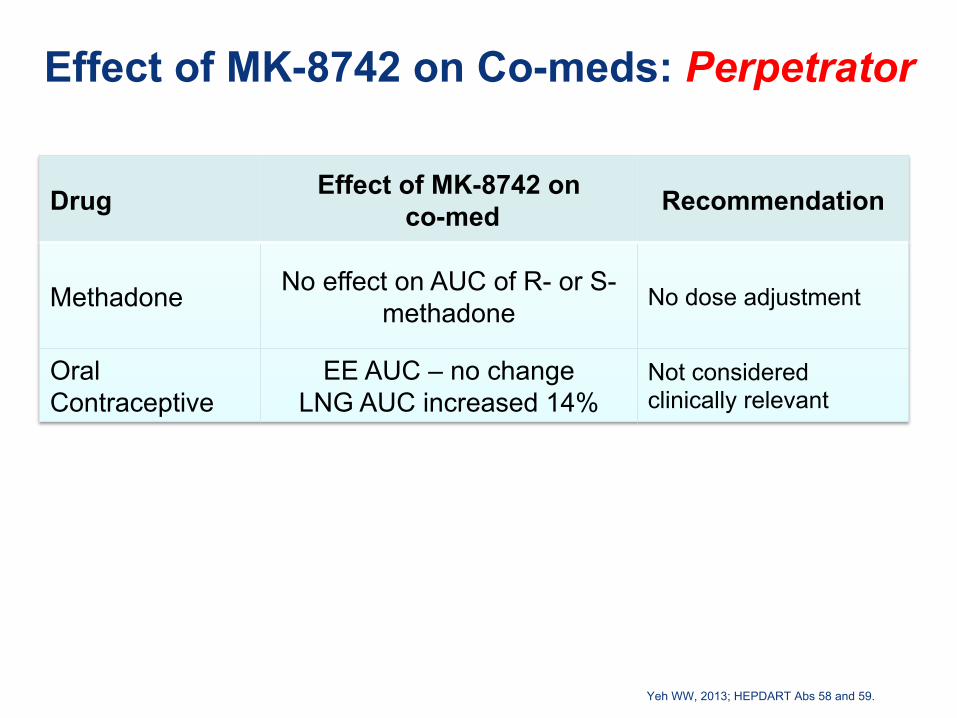
Effect of MK-8742 on Co-meds: Perpetrator
Drug Effect of MK-8742 on co-med Recommendation
Methadone
No effect on AUC of R- or S- methadone No dose adjustment
Oral Contraceptive
EE AUC – no change LNG AUC increased 14%
Not considered clinically relevant
Yeh WW, 2013; HEPDART Abs 58 and 59.

Effect of Co-adminstered drugs on Asunaprevir: Victim
Drug Effect on Asunaprevir Recommendation
Rifampicin
AUC decreased 21%
Ketoconazole
AUC increased 9.6-fold
Daclatasvir No change
Eley T et al 2013; 8th IWCPHepTher Abs O-13; Bifano M et al 2010; AASLD Abs 827.

Effect of Asunaprevir on Co-meds: Perpetrator
Drug Effect of Asunaprevir on co-med Recommendation
Caffeine No effect
Midazolam
MDZ AUC decreased 29%
Dextromethorphan DEX AUC increased 3.9-fold
Omeprazole OMP AUC decreased 20%
Rosuvastatin ROS AUC increased 41%
Daclatasvir DAC AUC increased 20%
Eley T et al. 2012. 7th IWCPHepTHer Abs O-4; Eley T et al. 2011; 62nd AASLD; ABS 381; Bifano M et al 2010; 61st AASLD Abs 827.

Slide 55
Co-medication
TVR effect BOC effect
AUC AUC Escitalopram (SSRI)
Metabolised by CYP2C19 & CYP3A4
↓ 35% ↓ 21%
van Heeswijk R, et al. IWCPHT 2010. Abstract 12; Telaprevir SmPC; Hulskotte EGJ et al HEP Dart 2011; Abs 121; Boceprevir SmPC.
§ Mechanism: Not clearly determined but INDUCTION of CYP2C19? § Doses may need to be increased when combined with telaprevir § Dose adjustment not anticipated with boceprevir.
Telaprevir & Boceprevir decrease exposure of other CYP-metabolised drugs:
Perpetrator

56
CYP Enzyme Expression & Function with Progressive Hepatic Impairment

PK of Simeprevir in volunteers with moderate or severe hepatic impairment
Ouwerkerk-‐Mahadevan S et al EASL 2013. Abs 762.
SMV exposure higher in volunteers with moderate hepatic impairment (CP-B) compared to matched healthy controls. SMV exposure in volunteers with moderate hepatic impairment similar to HCV-infected subjects with no cirrhosis and up to CP-A.





























