Embed Size (px)
Citation preview

Why Does CAR T-Cell Therapy Fail?Sattva Neelapu, MD

Why does CAR T-cell therapy fail?
Sattva S. Neelapu, M.D.
Professor and Deputy Chair ad interim
Department of Lymphoma and Myeloma
The University of Texas MD Anderson Cancer Center
Houston, TX

Disclosures
• Research support from Kite/Gilead, Merck, BMS, Cellectis, Poseida,
Karus, Acerta, and Unum Therapeutics
• Advisory Board Member / Consultant for Kite/Gilead, Merck, Celgene,
Novartis, Unum Therapeutics, Pfizer, Precision Biosciences, CellMedica,
and Incyte.
• I will discuss investigational use of CAR T-cell therapy

Axicabtagene ciloleucel and tisagenlecleucel:
Current indications
• Axicabtagene ciloleucel (CD19/CD3z/CD28)
✓ Adult patients with relapsed or refractory large B cell lymphoma after two
or more lines of systemic therapy, including DLBCL, high-grade B cell
lymphoma, PMBCL, and transformed follicular lymphoma
• Tisagenlecleucel (CD19/CD3z/4-1BB)
✓ Adult patients with relapsed/refractory large B cell lymphoma after two or
more lines of systemic therapy including DLBCL, high-grade B cell
lymphoma and transformed follicular lymphoma

Durable responses with CAR T-cell therapy in
r/r large B-cell lymphoma
Schuster et al. N Eng J Med 2019Neelapu, Locke et al. N Eng J Med 2017
Locke, Neelapu et al. Lancet Oncol 2019
ZUMA-1: PFS with axi-cel
39% progression-free at 27.1 mo
JULIET: PFS with tisagenlecleucel
34% progression-free at 14 mo#
Median f/u: 27.1 mo
Median PFS: 5.9 mo
Patients at Risk
Median f/u: 14 mo
Median PFS: 2.9 mo
#Calculated value from publication

Major improvement compared with historical data
Overall survival: SCHOLAR-1
Crump, Neelapu et al. Blood 2017
Overall survival: ZUMA1
• N = 636
• ORR = 26%; CR rate = 7%
• Median OS = 6.3 months
• N = 108
• ORR = 83%; CR rate = 58%
• Median OS = >24 monthsNeelapu, Locke et al. N Eng J Med 2017
Locke, Neelapu et al. Lancet Oncol 2019

Patterns of failure in DLBCL after axi-cel
CRs PRs
~60% ~20%
Durable
CRs
Late
relapse
Early
relapse
~40% ~10%
> 6 mo
~10%
2-6 mo
Early
relapse
~20%
1-2 mo
Axi-cel CD19 CAR T therapy
Primary resistance Responders
~20% ~80%
• All numbers are rounded off
1 mo
Neelapu et al. N Eng J Med 2017
~60% failure

ZUMA1: Biomarkers of response and durability
Covariate Impact on efficacy
Clinical prognostic markers
Age, stage, IPI, bulky, extranodal, refractory
subgroup, primary refractory, prior ASCT
No
Product characteristics
CD4:CD8 ratio No
Phenotype No
T-cell doubling time No
Tumor characteristics
Cell of origin (ABC vs. GCB) No
DLBCL vs. PMBCL vs. TFL No
CD19 H score No
Pre-infusion

ZUMA1: Biomarkers of response and durability
Covariate Impact on efficacy
Clinical prognostic markers
Age, stage, IPI, bulky, extranodal, refractory
subgroup, primary refractory, prior ASCT
No
Product characteristics
CD4:CD8 ratio No
Phenotype No
T-cell doubling time No
Tumor characteristics
Cell of origin (ABC vs. GCB) No
DLBCL vs. PMBCL vs. TFL No
CD19 H score No
Post-infusion
Peak CAR and CAR-AUC Yes
CAR T persistence No
Tocilizumab and steroid use No
Pre-infusion

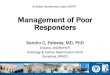
ZUMA1: CAR T-cell expansion after axi-cel infusion is
associated with response
Neelapu et al. N Eng J Med 2017

Is long-term persistence of CAR T cells needed?
• R-CHOP chemotherapy does not persist long-term but cures
~60% of DLBCL patients
• If every cancer cell in the body is eliminated within the first 1-3
months, long-term persistence of CAR T cells is not needed!
• Need to cure the cancer only once!
• Short- to intermediate-term persistence is likely sufficient

ZUMA1: ~30% of patients in remission at 1 year
did not have detectable CAR T cells
BL, baseline; LLOQ, lower level of quantification.
Solid line indicates median. Dashed lines indicate Q1 and Q3.
106 99 86 58 52 22 6 3
No. of Patients
1 2 3
2 0
4 0
6 0
8 0
6 1 2 1 8 2 4
T i m e P o s t - A x i - c e l I n f u s i o n , m o n t h s
CA
R
T
Ce
ll
s/
L
Bl
oo
d
L L O Q
B L
4598 99
• Persisting CAR T cells were observed
in 71% (32/45) of patients remaining in
response at 1 year
• Durable responses were present in
patients with and without detectable
persisting CAR T cells
Neelapu et al. ASH 2017

ZUMA1: 75% of patients in remission at 2 years
had detectable B cells
• 75% of patients (24/32) with
ongoing responses had
detectable B cells 2 years after
axi-cel infusion
• Throughout the course of the
study, 31% of patients received
intravenous immunoglobulins
Locke et al Neelapu, Lancet Oncol 2019

Mechanisms of resistance after CD19 CAR T cell therapy
• If the CAR T therapy does what it is supposed to do (i.e.
eliminate every CD19 expressing tumor cell in the body),
most relapse tumors should be CD19-ve
• In contrast, if the CAR T therapy therapy is not very
effective, most relapse tumors should be CD19+

ZUMA1: Case 1
Pre 1 month (PR) 3 months (PD)
CD19+
DLBCL
H&E PAX5
CD19Ki67
Pre-axi-cel
CD19-
DLBCL
H&E PAX5
CD19Ki67
Post-axi-cel
68/M/DLBCL
•R-CHOP - PD
•R-GDP - PD
•R-ICE - PD
•ACP-196+Pembro - PD
Pre 1 month
Heterogeneity in
CD19 expression

ZUMA1: Case 2
Baseline 1 month (CR)
72 yo M with DLBCL
Prior therapies
• R-CHOP x 6 - PD
• Radiation - PD
3 months (RD)
CD19-
DLBCL
CD19+
DLBCL
Very low frequency
of CD19-ve clones
at baseline?

ZUMA1: Case 3
Baseline 1 month (CR)
75 yo M with DHL
Prior therapies
• R-EPOCH - PD
• R-Gem-Ox - PDCD19+
DHL
14 months (RD)
CD19-
DHL
Very low frequency
of CD19-ve clones
at baseline?

Alternatively spliced variants of CD19 after CAR T therapy
• At relapse, 15/16 (94%) patients
assessed had CD19 loss on ELIANA trial
Maude et al, N Eng J Med 2018
Loss of exon 2 or exons 5-6
Cancer Discov 2015

Canonical and novel splice junctions
of CD19 in DLBCL after axi-cel

Mechanisms of anti-CD19 CAR T resistance
DLBCL after axi-cel
CD19 negative CD19 positive
• Impaired T-cell fitnesso Apheresis product
o CAR T product
o Host environment
o Tumor microenvironment
• Antigen escape
o CD19 alternative splicing
o CD19 mutation
1/2 1/2

ZUMA-1: CAR T-cell fitness by prior lines of therapy
• Early referral may improve the efficacy of CAR T-cell therapy

Quantification of 32-plex CAR T cell polyfunctionality using
IsoPlexis Platform and Polyfunctional Strength Index (PSI)
Polyfunctional strength index
(PSI)
% Polyfunctional T cells
Cytokine intensities
IL-1βIL-6
IL-17AIL-17F
MCP-1MCP-4
Inflammatoryelicit systematic inflammation and autoimmunity
IL-4IL-10IL-13IL-22
TGF-β1sCD137sCD40L
Regulatorydampen anti-tumor immune response
Granzyme BIFN-γMIP-1αPerforinTNF-αTNF-β
Effectoranti-tumor
immunity or cytotoxic functions
Stimulatorystimulation/
proliferation of immune cells
GM-CSFIL-2IL-5IL-7IL-8IL-9IL-12IL-15IL-21
CCl-11IP-10MIP-1βRANTES
Chemoattractiverecruit immune cells to
tumor site
IsoPlexis IsoCode Technology and Ma et al 2013Rossi et al. Blood 2018;132:804-814

Analysis of pre-Infusion CAR T cell polyfunctionality on the
IsoPlexis Single-Cell, High-Multiplexing ELISA System
Antibodies “barcode” each
single-cell chamber
32 cytokines captured,
per CAR T cell
CAR T cells,
versus CD19
ELISA steps allow
cytokine monitoringcell
cytokine / protein
Each “barcoded cytokine readout”
per cell x 1000s of patient cells
Single-cell antibody
barcode cytokine panel
Rossi et al. Blood 2018;132:804-814

Pre-Infusion single-cell CAR Polyfunctional Strength Index (PSI)
associated with objective response (axi-cel)
KD19 KD24 KD06 KD16 KD20 KD25 KD18 KD23 KD08 KD09 KD07 KD21 KD22 KD12 KD17 KD11 KD13 KD10 KD15 KD14
Non-RespondersResponders
Single-Cell CAR PSI ( n = 20)
p = 0.0119**
Effector Stimulatory Regulatory InflammatoryChemoattractive
22
%
% polyfunctional
cells in sample
Product CD4 subpopulation
25%
% polyfunctional
cells in sample
Product CD8 subpopulation
Clinical outcome – NCI study (N = 22)
• ORR/ CR = 73% / 55%
• 11/12 CRs are ongoing (7-24 mo+)
Rossi et al. Blood 2018;132:804-814

T-cell intrinsic fitness in apheresis product may affect CAR T efficacy
Fraietta et al, Nat Med Apr 2018
• Increased frequency of CD27+CD45RO-
CD8+ T cells before CAR T generation
associated with durable remission in CLL
• CD27+PD-1-CD8+ CAR T cells associated
with response
• Rationale for allogeneic CAR or
banking T cells when healthy

Improving T-cell fitness: Allogeneic CAR T-cell therapy
Disrupt TRAC (loss of TCRab) to prevent GVHD
Qasim et al. Sci Transl Med 2017
PALL / CALM studies with UCART19:
Pediatric and adult ALL
• CR/CRi: 14/17 (82%) in Cy/Flu/Alemtuzumab conditioned pts
• MRD-: 10/14pts (71%)
• Grade 1 skin GVHD in 2 (9.5%)
Benjamin et al. ASH 2018

CAR T-cell fitness in vivo may be affected by
host conditioning
Turtle et al. Sci Transl Med 2016
Subgroup N ORR CR
Cy or Cy/E 12 50% 8%
Cy/Flu 18 72% 50%
DLBCL, transformed LBCL, FL, MCL (CD19/CD3z/4-1BB)
• CAR T cells reached higher peaks and persisted longer with Cy/Flu conditioning regimen compared with Cy regimen
CD4 CD8 Total CAR T

Effects of conditioning therapy
Neelapu SS. Blood, In Press (Commentary)

ZUMA1: Case 4
Baseline 1 month (PR) 28 yo M with HGBCL
Prior therapies
• R-CHOP - PR
• R-ICE - PD
• R-Hypercytoxan - PD
• TTR - PD
• Radiation - PD
3 months (PD)
CD19+
HGBCL
1 month (PR)
• Immune checkpoints?

Post-infusion conditioning with PD-1/PD-L1 blockade
CD19 at Baseline CD19 at PD PD-L1 at PD
Post-axi-cel in DLBCL: ~2/3 of tumors at progression were PD-L1 positive
ZUMA-6: Axi-cel in combination with PD-L1 blockade ongoing
Neelapu et al. ASH 2017

Post-infusion conditioning with lenalidomide
Oncoimmunology 2016

Outcomes with lenalidomide after CAR T failure
Age/
SexDiagnosis Pre-CAR T therapies CAR T therapy
Response / PD
post-CAR T
Post-CAR T
therapy
Response to Len /
Duration
54/MNon-GCB
DLBCL
DA-EPOCH-R +
HD MtxAxi-cel PD 1 mo Rit + Len 15 mg CR / 26+ mo
54/M PMBCLR-CHOP / R-ICE /
Nivo+4-1BB AbAx-cel CR → PD 10 mo Rit + Len 20 mg CR / 15+ mo
60/MNon-GCB
DLBCLR-CHOP / R-ICE Ax-cel CR → PD 5 mo
Acala + Pembro /
Rit + Len 20 mgPD
68/F TFL / DHL
BR / Obi-Len /
Ibr+R-CHOP /
R-Gem-Ox
CD19/CD28/CD3z
CD19/CD28/
4-1BB/CD3z
PR → PD 3 mo Rit + Len 15 mg CR / 15+ mo
76/M DHLDA-EPOCH-R /
R-Gem-OxAx-cel CR → PD 14 mo Obi + Len 20 mg PD
55/F FL Gr 3a
R-CHOP / Rit / BR / R-
EPOCH / Rit-Len /
Idelalisib / R-Hyper
Cytoxan
Axi-cel (NCI) PR → PD 4 mo Obi + Len 15 mg
CR / 6+ mo
Allo-SCT at 6 mo
Died in CR at
14 mo
49/F FL Gr 3aR-CHOP / BR /
R-ICE / Rit-LenAxi-cel PR → PD 3 mo Obi + Len 20 mg PR / 4 mo
58/M TMZLR-CVP, R-CHOP, R-ICE,
Ofa-GDP, ASCT, RHCVDAxi-cel SD at 1 mo Len 20 mg PR / 2+ mo

Lenalidomide for SD after SOC axi-cel
Baseline 1 mo (SD)
58 yo M with MZL (2011)
→ DLBCL (2012)
• R-CVP
• R-CHOP
• R-ICE
• Ofatumumab-GDP
• RIE → ASCT (2015)
• RHCVD
3 mo (PR)
Axi-cel Len 20 mg

Pre- and post-infusion conditioning with ibrutinib
Jun 2016
ASCO 2017, Abstract 7509 10 patients: 9 MRD-ve marrow CR

Improving efficacy of CAR T therapy in B-cell malignancies
B-cell malignancies
CD19 negative CD19 positive
• Improve T-cell fitnesso Apheresis product
➢ Allogeneic source
➢ Specific T cell subsets
➢ Ibrutinib
o CAR T product
➢ Design
➢ Phenotype / Function
o Pre-infusion conditioning therapy
➢ Fludarabine-based
➢ TKIs
o Post-infusion conditioning therapy
➢ PD-1/PD-L1
➢ IMIDs
➢ TKIs
• Target multiple antigens
o CD19-CD22 CAR T
o CD19-CD20 CAR T
o CD79b CAR T

Summary
• CD19 CAR-T induces durable remissions in ~40% of r/r
large B-cell lymphoma
• CD19 loss and impaired T-cell fitness may be major
mechanisms of resistance
• Targeting multiple antigens and strategies for improving
T-cell fitness may improve efficacy of CAR T-cell
therapy

Thank you!