Embed Size (px)
Citation preview

9/22/2020
1
Kathy Rock PT, MBA, CHCA, CRHC, CPC, CHC
Rock Consulting Inc.
150 Questions over case studies
5 hours and 40 minutes – Running time
Scoring breakdown
Anatomy
CPT
Evaluation and Management
HCPCS
ICD 10
Modifier
Practice Management
Scores released within 7-10 business days online and mailed

9/22/2020
2
Ensure coding resources are prepared for Exam
Confirm understanding of
Procedures and anatomy related to procedures
Medications to include reason for use, billable units and administration method
Common diagnostic services
Modifiers commonly used with E/M and procedures
Diagnoses coding guidelines
Explore Evaluation and Management coding guidelines
Book Preparation 12:00 pm – 1:30 pm
Break 1:30 pm – 1:45 pm
Case Studies 1:45 pm – 3:00 pm
Break 3:00 pm – 3:15 pm
Review of Knowledge 3:15 pm – 4:00 pm

9/22/2020
3
CPT
ICD-10
HCPCS
1995/1997 Guidelines

9/22/2020
4
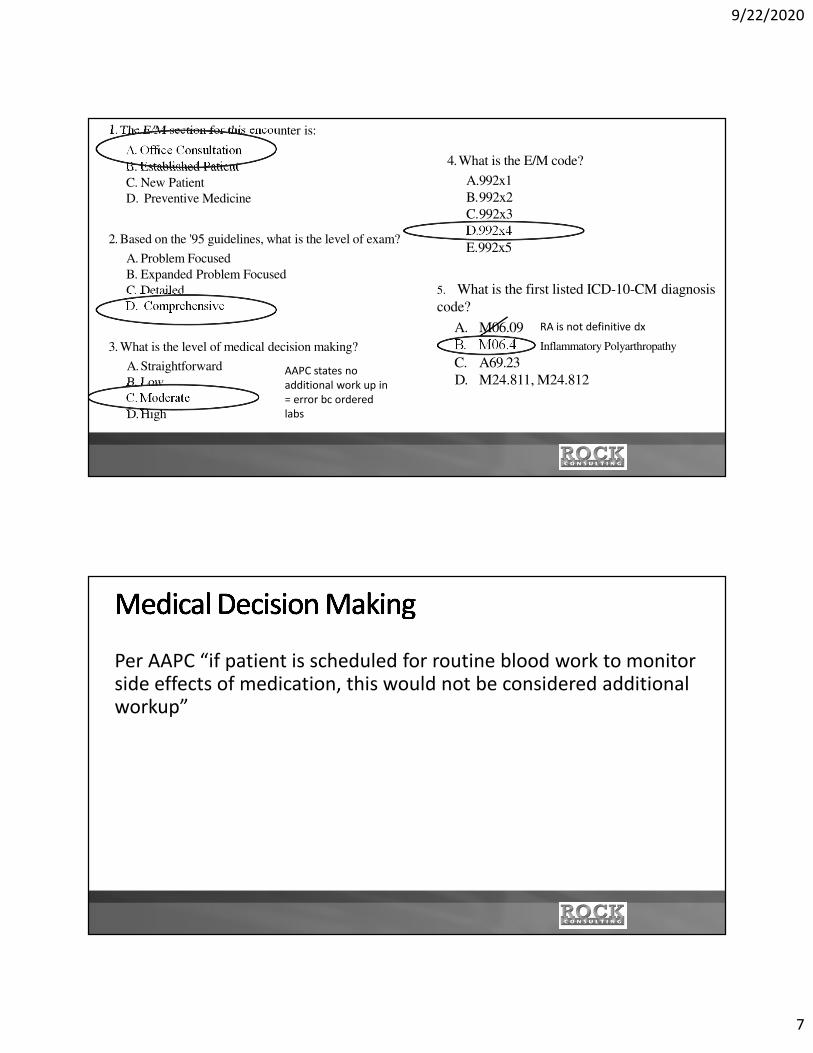
1.The E/M section for this encounter is:
A. Office Consultation
B. Established Patient
C. New Patient
D. Preventive Medicine
2. Based on the '95 guidelines, what is the level of exam?
A. Problem Focused
B. Expanded Problem Focused
C. Detailed
D. Comprehensive
3. What is the level of medical decision making?
A.Straightforward
B. Low
C. Moderate
D.High
4.What is the E/M code?
A.992x1
B.992x2
C.992x3
D.992x4
E.992x5
5. What is the first listed ICD-10-CM diagnosis
code?
A. M06.09
B. M06.4
C. A69.23
D. M24.811, M24.812

9/22/2020
5
Chief Complaint: Multiple joint pains.
History of Present Illness: Dr. X, the patient's PCP, requested I see the patient for further evaluation
of multiple joint pains. He states to me that his symptoms started about 4 weeks ago, affecting his
shoulders, knees and then both his wrists and hands. He professes to have 2 to 3 hours of
morning stiffness. He feels somewhat better when taking a hot shower and after he takes medi-
cations. He states that in May he had a motorcycle accident and had dislocated hip and broken ribs.
He gradually improved and started to exercise. After a few weeks his multiple joint pains started. He
was put on Celebrex for 3 weeks, which initially helped, and then it did not. He was given Naproxen
without any relief in his symptoms. He is currently taking aspirin, 325 mg, 2 tablets every 4 hours on
an as-needed basis, alternating with Tylenol, 2 tablets every 4 hours. He had multiple blood tests
done within the past few weeks, including herpes virus-6 antibody is negative; uric acid is normal;
CBC is within normal limits except slightly elevated WBC at 11.6, and platelet count 464. RPR was
nonreactive. Complete metabolic panel was normal except slightly elevated alkaline phosphatase. He
had Lyme tests done last week. The results are not available to us. He was put on Doxycycline for
presumable Lyme disease on September 28. He reports that he had multiple insect bites a week
before the pain started. He denies any tick bites or any rash.
13
4
2
ROS 1
Case Studies Page 1-3
Past Medical History:
1. Hypercholesterolemia.
2. History of colon cancer, status-post surgery in 1997.
3. GERD.
Medications:1. Doxycycline 100 mg. p.o. b.i.d.
2. Aspirin pm.
3. Tylenol pm.
4. Crestor 30 mg p.o. daily.
5. Prevacid 30 mg p.o. daily.
ALLERGIES: NKDA.
Social History: He is a retired military officer. He quit smoking in 1969. He drinks alcohol very
occasionally.
Family History: Father had prostate cancer. Mother had breast cancer. No siblings.
Review of Systems: He denies any constitutional symptoms except intentional weight, on military diet.
He denies any eye or ear symptoms, cardiovascular, respiratory, gastrointestinal, or genitourinary
symptoms. He has physical disability because of pain. He has joint pain and stiffness and difficulty with
making fists. He also has a numbness and tingling sensation in his right hand.
ROS 2
ROS 3 ROS 4
ROS 5
ROS 6 ROS 8ROS 7
ROS 9
ROS 10

9/22/2020
6
Physical Exam: He is an elderly male in no acute distress. Vital Signs: BP is 138/80, Temp: 98.0, Pulse: 80.
HEENT: Exam reveals no conjunctival injections or scleral icterus. There are oral mucosal ulcers. Chest:
Is clear bilaterally, without any crackles or wheezing. Equal air entry. Heart: Exam is unremarkable, with
SI, S2 regular. There is no murmur.
Abdomen: Benign. Soft, no masses or tenderness. Normal spleen. Neurological: Oriented and alert x 3.
Normal motor and sensory function.
Musculoskeletal Exam: No tenderness on both shoulders, with normal range of motion. There is no
swelling or tenderness on his elbows. He has tenderness on his right wrist with swelling. There is no
swelling on his left wrist. He has a slightly limited range of motion with flexion on both wrists, more on the
right side. He has synovitis across all MCP joints on his right hand, with no tenderness. There is a subtle
synovitis on his few PIP joints on both hands. There is a mild synovitis on his few MCP joints as well. He is
unable to make a fist on both his hands, more pronounced on the right one. He has a loss of the distal
portion of his 3rd and 4th finger at the PIP level on the left hand. He has full range of motion of hips,
without any pain. There is no effusion on his both knees. There is no increased warmth or swelling. There
is no tenderness on his ankles. Skin: Exam is unremarkable, without any nodules or rash. Warm/Dry, no
diaphoresis.
Assessment & Plan: This is a 64-year-old gentleman with inflammatory arthritis multiple sites, most
likely rheumatoid arthritis. I would like to obtain a rheumatoid factor, anti-CCP antibody, ESR and
CRP. I would like to put him on Prednisone, 10 mg in the morning, 5 mg at night for one week, then
decrease it to 5 mg p.o. b.i.d. until I see him. He will be seen in 2 weeks for further management.
He had Lyme tests done last week. The result is not available to me. He is on Doxycycline, I do not have
any clinical suspicion for Lyme disease, although I would rather wait for lab results before we make a
decision on Doxycycline at this point.
Please make sure Dr. X receives my written recommendations.
9/22/2020
7
1.The E/M section for this encounter is:
A. Office Consultation
B. Established Patient
C. New Patient
D. Preventive Medicine
2. Based on the '95 guidelines, what is the level of exam?
A. Problem Focused
B. Expanded Problem Focused
C. Detailed
D. Comprehensive
3. What is the level of medical decision making?
A.Straightforward
B. Low
C. Moderate
D.High
4.What is the E/M code?
A.992x1
B.992x2
C.992x3
D.992x4
E.992x5
5. What is the first listed ICD-10-CM diagnosis
code?
A. M06.09
B. M06.4
C. A69.23
D. M24.811, M24.812
RA is not definitive dx
AAPC states no
additional work up in
= error bc ordered
labs
Inflammatory Polyarthropathy
Per AAPC “if patient is scheduled for routine blood work to monitor side effects of medication, this would not be considered additional workup”
9/22/2020
8
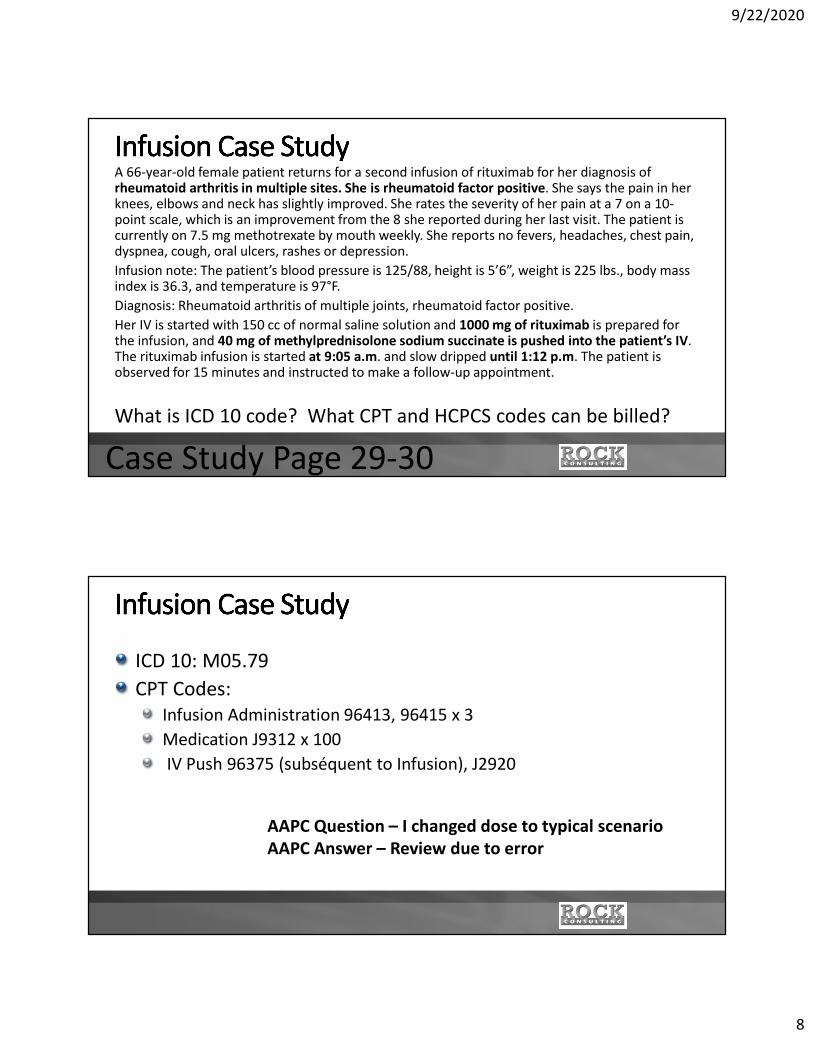
A 66-year-old female patient returns for a second infusion of rituximab for her diagnosis of rheumatoid arthritis in multiple sites. She is rheumatoid factor positive. She says the pain in her knees, elbows and neck has slightly improved. She rates the severity of her pain at a 7 on a 10-point scale, which is an improvement from the 8 she reported during her last visit. The patient is currently on 7.5 mg methotrexate by mouth weekly. She reports no fevers, headaches, chest pain, dyspnea, cough, oral ulcers, rashes or depression.
Infusion note: The patient’s blood pressure is 125/88, height is 5’6”, weight is 225 lbs., body mass index is 36.3, and temperature is 97°F.
Diagnosis: Rheumatoid arthritis of multiple joints, rheumatoid factor positive.
Her IV is started with 150 cc of normal saline solution and 1000 mg of rituximab is prepared for the infusion, and 40 mg of methylprednisolone sodium succinate is pushed into the patient’s IV. The rituximab infusion is started at 9:05 a.m. and slow dripped until 1:12 p.m. The patient is observed for 15 minutes and instructed to make a follow-up appointment.
What is ICD 10 code? What CPT and HCPCS codes can be billed?
Case Study Page 29-30
ICD 10: M05.79
CPT Codes:
Infusion Administration 96413, 96415 x 3
Medication J9312 x 100
IV Push 96375 (subséquent to Infusion), J2920
AAPC Question – I changed dose to typical scenario
AAPC Answer – Review due to error
9/22/2020
9
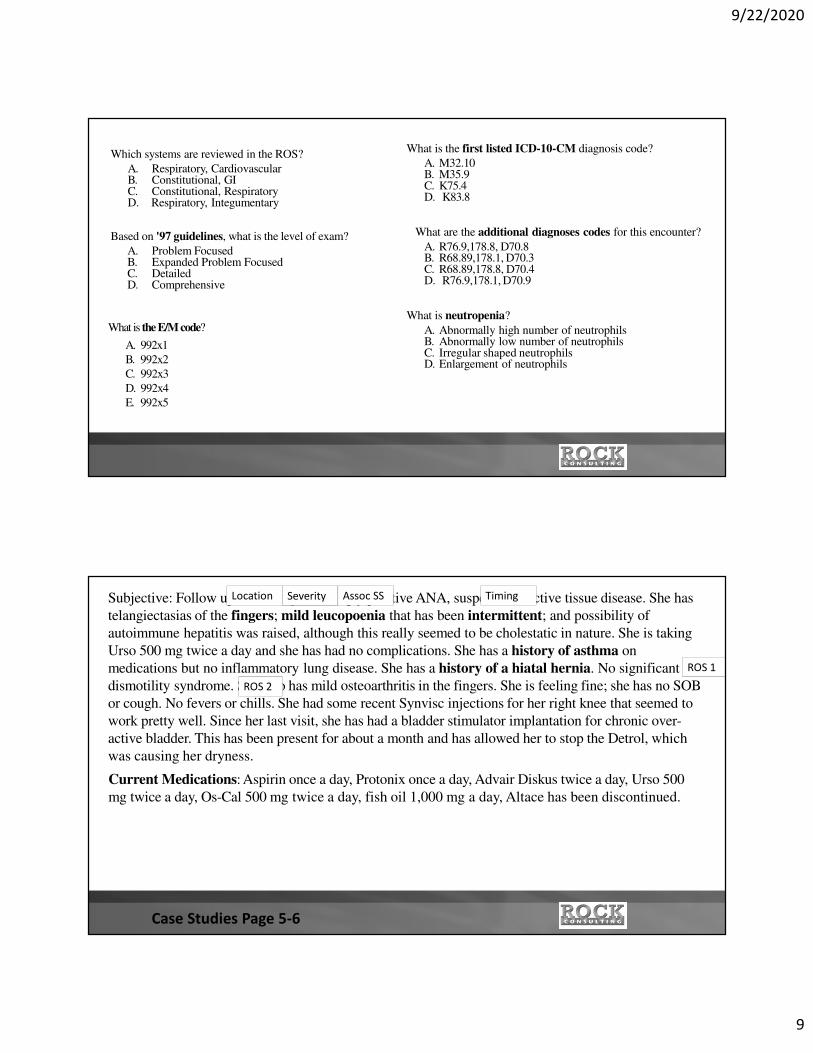
Which systems are reviewed in the ROS?
A. Respiratory, CardiovascularB. Constitutional, GIC. Constitutional, RespiratoryD. Respiratory, Integumentary
Based on '97 guidelines, what is the level of exam?
A. Problem FocusedB. Expanded Problem FocusedC. DetailedD. Comprehensive
What is the E/M code?
A. 992x1
B. 992x2
C. 992x3
D. 992x4
E. 992x5
What is the first listed ICD-10-CM diagnosis code?
A. M32.10B. M35.9C. K75.4D. K83.8
What are the additional diagnoses codes for this encounter?
A. R76.9,178.8, D70.8B. R68.89,178.1, D70.3C. R68.89,178.8, D70.4D. R76.9,178.1, D70.9
What is neutropenia?
A. Abnormally high number of neutrophilsB. Abnormally low number of neutrophilsC. Irregular shaped neutrophilsD. Enlargement of neutrophils
Subjective: Follow up for history of strongly positive ANA, suspect connective tissue disease. She has
telangiectasias of the fingers; mild leucopoenia that has been intermittent; and possibility of
autoimmune hepatitis was raised, although this really seemed to be cholestatic in nature. She is taking
Urso 500 mg twice a day and she has had no complications. She has a history of asthma on
medications but no inflammatory lung disease. She has a history of a hiatal hernia. No significant
dismotility syndrome. She also has mild osteoarthritis in the fingers. She is feeling fine; she has no SOB
or cough. No fevers or chills. She had some recent Synvisc injections for her right knee that seemed to
work pretty well. Since her last visit, she has had a bladder stimulator implantation for chronic over-
active bladder. This has been present for about a month and has allowed her to stop the Detrol, which
was causing her dryness.
Current Medications: Aspirin once a day, Protonix once a day, Advair Diskus twice a day, Urso 500
mg twice a day, Os-Cal 500 mg twice a day, fish oil 1,000 mg a day, Altace has been discontinued.
ROS 1
ROS 2
Location Severity Assoc SS Timing
Case Studies Page 5-6

9/22/2020
10
Physical Exam: She is alert and oriented, obese white female. BP: 126/80. Pulse: 70. Respirations: 12.
Lungs: Clear. Heart: Rate and rhythm are regular. Peripheral pulses: 2+ and equal bilaterally. Skin: No
suspicious lesions. There are small telangiectasias of the finger pads, actually unchanged. No sclerodactyly
or morphia or rashes on exam. There are a few scattered dilated capillary nail beds. These are unchanged as
well.
Musculoskeletal Exam: There is bony hypertrophy of the DIP and PIP joints. There is no synovitis.
There is medial joint line tenderness of the knees bilaterally without any effusion.
Review of Laboratory Data: (09/12/xx) Metabolic panel: Normal, GFR greater than 60; transaminases and
alk phos were normal. C-reactive protein .8, urine for micro-albumin is 66 mg/deciliter. But the micro-
albumin to creatinine ratio is 7, which is normal. CBC: WBC 3.9, otherwise normal, sed rate 1. Urinalysis:
No protein, WBCs, RBCs or casts. ANA was confirmed at a titer of 1:1280, which is essentially unchanged.
Assessment: The patient has connective tissue disease with a positive ANA, mild telangiectasias, possible
autoimmune hepatitis versus cholestasis, and mild chronic neutropenia.
Plan: Monitoring is indicated at this time. I would like to see her in six months or certainly sooner as needed.
Repeat labs at that time, which will include a metabolic panel, CBC, complements C3, C4, ANA, and a
urinalysis.
1997 Exam General System
Physical Exam: She is alert and oriented, obese white female. BP: 126/80. Pulse: 70. Respirations: 12.
Lungs: Clear. Heart: Rate and rhythm are regular. Peripheral pulses: 2+ and equal bilaterally. Skin: No
suspicious lesions. There are small telangiectasias of the finger pads, actually unchanged. No sclerodactyly
or morphia or rashes on exam. There are a few scattered dilated capillary nail beds. These are unchanged as
well.
Musculoskeletal Exam: There is bony hypertrophy of the DIP and PIP joints. There is no synovitis.
There is medial joint line tenderness of the knees bilaterally without any effusion.
Review of Laboratory Data: (09/12/xx) Metabolic panel: Normal, GFR greater than 60; transaminases and
alk phos were normal. C-reactive protein .8, urine for micro-albumin is 66 mg/deciliter. But the micro-
albumin to creatinine ratio is 7, which is normal. CBC: WBC 3.9, otherwise normal, sed rate 1. Urinalysis:
No protein, WBCs, RBCs or casts. ANA was confirmed at a titer of 1:1280, which is essentially unchanged.
Assessment: The patient has connective tissue disease with a positive ANA, mild telangiectasias,
possible autoimmune hepatitis versus cholestasis, and mild chronic neutropenia.
Plan: Monitoring is indicated at this time. I would like to see her in six months or certainly sooner as needed.
Repeat labs at that time, which will include a metabolic panel, CBC, complements C3, C4, ANA, and a
urinalysis.
1995 Exam - Extended
Table of Risk – Presenting problem
AAPC worsening?

9/22/2020
11
Which systems are reviewed in the ROS?
A. Respiratory, CardiovascularB. Constitutional, GIC. Constitutional, RespiratoryD. Respiratory, Integumentary
Based on '97 guidelines, what is the level of exam?
A. Problem FocusedB. Expanded Problem FocusedC. DetailedD. Comprehensive
What is the E/M code?
A. 992x1
B. 992x2
C. 992x3
D. 992x4
E. 992x5
What is the first listed ICD-10-CM diagnosis code?
A. M32.10B. M35.9C. K75.4 Digestive System PossibleD. K83.8 Digestive System Possible
What are the additional diagnoses codes for this encounter?
A. R76.9,178.8, D70.8B. R68.89,178.1, D70.3C. R68.89,178.8, D70.4D R76.9,178.1, D70.9
What is neutropenia?
A. bnormally high number of neutrophilsB. Abnormally low number of neutrophilsC. Irregular shaped neutrophilsD. Enlargement of neutrophils
Penia = deficiency
D70 Neutropenia Pg 506
What is the E/M code?
A. 992x1B. 992x2C. 992x3D. 992x4E. 992x5
What is the appropriate CPT" code for the DEXA
scan that was ordered?
A. 77086B. 77078C. 77081D. 77080
What are the ICD-10-CM diagnosis codes for the
encounter?
A. M15.0, M81.0B. M15.9, M81.6C. M06.09, M81.0D. M06.09, M81.8
9/22/2020
12
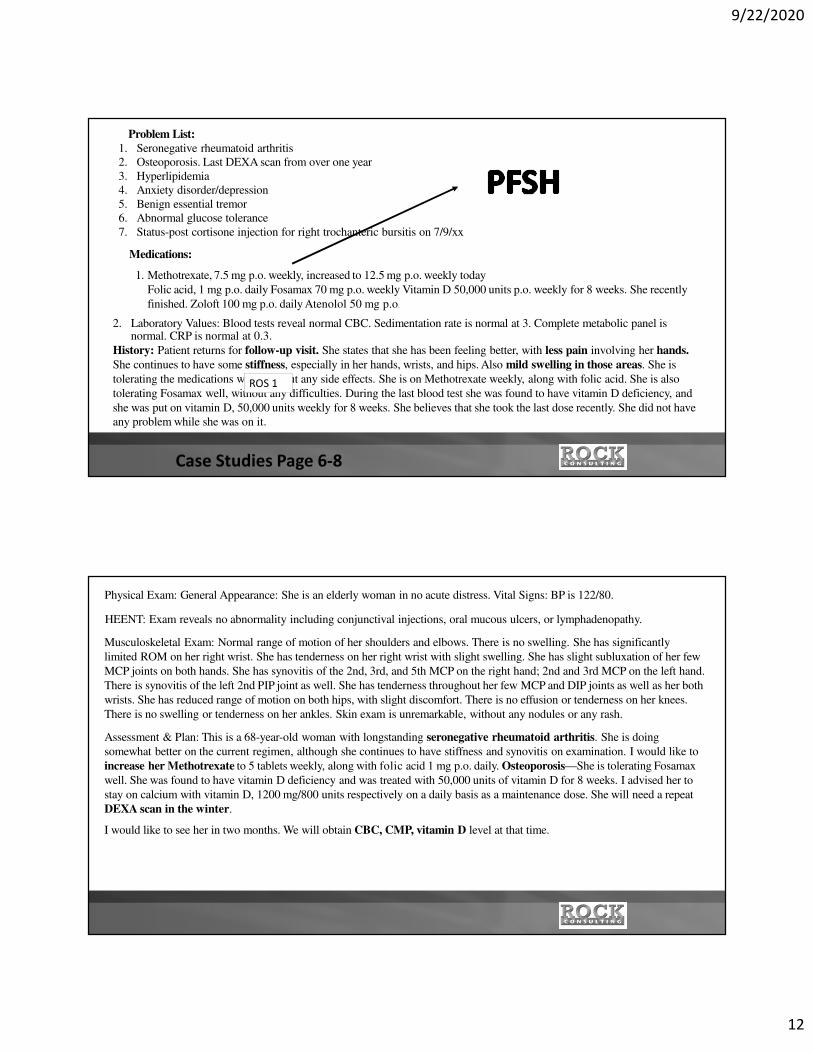
Problem List:
1. Seronegative rheumatoid arthritis
2. Osteoporosis. Last DEXA scan from over one year
3. Hyperlipidemia
4. Anxiety disorder/depression
5. Benign essential tremor
6. Abnormal glucose tolerance
7. Status-post cortisone injection for right trochanteric bursitis on 7/9/xx
Medications:
1. Methotrexate, 7.5 mg p.o. weekly, increased to 12.5 mg p.o. weekly today
Folic acid, 1 mg p.o. daily Fosamax 70 mg p.o. weekly Vitamin D 50,000 units p.o. weekly for 8 weeks. She recently
finished. Zoloft 100 mg p.o. daily Atenolol 50 mg p.o.
2. Laboratory Values: Blood tests reveal normal CBC. Sedimentation rate is normal at 3. Complete metabolic panel is normal. CRP is normal at 0.3.
History: Patient returns for follow-up visit. She states that she has been feeling better, with less pain involving her hands.
She continues to have some stiffness, especially in her hands, wrists, and hips. Also mild swelling in those areas. She is
tolerating the medications well, without any side effects. She is on Methotrexate weekly, along with folic acid. She is also
tolerating Fosamax well, without any difficulties. During the last blood test she was found to have vitamin D deficiency, and
she was put on vitamin D, 50,000 units weekly for 8 weeks. She believes that she took the last dose recently. She did not have
any problem while she was on it.
ROS 1
Case Studies Page 6-8
Physical Exam: General Appearance: She is an elderly woman in no acute distress. Vital Signs: BP is 122/80.
HEENT: Exam reveals no abnormality including conjunctival injections, oral mucous ulcers, or lymphadenopathy.
Musculoskeletal Exam: Normal range of motion of her shoulders and elbows. There is no swelling. She has significantly
limited ROM on her right wrist. She has tenderness on her right wrist with slight swelling. She has slight subluxation of her few
MCP joints on both hands. She has synovitis of the 2nd, 3rd, and 5th MCP on the right hand; 2nd and 3rd MCP on the left hand.
There is synovitis of the left 2nd PIP joint as well. She has tenderness throughout her few MCP and DIP joints as well as her both
wrists. She has reduced range of motion on both hips, with slight discomfort. There is no effusion or tenderness on her knees.
There is no swelling or tenderness on her ankles. Skin exam is unremarkable, without any nodules or any rash.
Assessment & Plan: This is a 68-year-old woman with longstanding seronegative rheumatoid arthritis. She is doing
somewhat better on the current regimen, although she continues to have stiffness and synovitis on examination. I would like to
increase her Methotrexate to 5 tablets weekly, along with folic acid 1 mg p.o. daily. Osteoporosis—She is tolerating Fosamax
well. She was found to have vitamin D deficiency and was treated with 50,000 units of vitamin D for 8 weeks. I advised her to
stay on calcium with vitamin D, 1200 mg/800 units respectively on a daily basis as a maintenance dose. She will need a repeat
DEXA scan in the winter.
I would like to see her in two months. We will obtain CBC, CMP, vitamin D level at that time.

9/22/2020
13
What is the E/M code?
A. 992x1B. 992x2C. 992x3D. 992x4E. 992x5
What is the appropriate CPT" code for the DEXA
scan that was ordered?
A. 77086B. 77078C. 77081D. 77080
What are the ICD-10-CM diagnosis codes for the
encounter?
A. M15.0, M81.0B. M15.9, M81.6C. M06.09, M81.0D. M06.09, M81.8
AAPC scoring varied – see audit tool; Their
answer was 99213 because they considered RA
diagnosis stable although MTX dose was
increased
How would you determine the appropriate E/M level for
this encounter?
A. Based on history, exam, and medical decision making
B. Based on the amount of time for the visit
C. Based on the MDM and time
D. Based on the exam, MDM, and time
In addition to the E/M service, what additional procedures were performed during the encounter?
A. 36415,86140B. 85025C. 36415, 86140, 85025D. None of the above
What are the appropriate ICD-10-CM diagnosis codes?
A. M35.3, M15.9B. M35.3, M25.50C. M35.3, M15.0, M25.51D. M35.3, M15.3, M25.50
9/22/2020
14
Current Medications:
Folic acid 400 meg, Tab, 1 tablet daily
Imitrex 50 mg, Tab, prn
Nutritional Supplements, Tab, 760/600, qd
Omega-3 Fatty Acids 1000 mg, Caps, qd
Tylenol Arthritis Pain 650 mg, Taken As Directed, 2 bid
Rheumatology Visit:
The patient presents for follow-up of polymyalgia rheumatica and osteoarthritis. The Dr. reports that she
has been doing fairly well overall. She has multiple areas that are bothering her. Her knees continue to
bother her some. She did quit her leg presses. She has a couple of toes on her right foot that are sore. Her
right fourth PIP is achy and slightly swollen. Her shoulders bother her a bit. She has trouble getting into a
comfortable position in bed at night. None of these are terrible with regard to the amount of pain they
cause. She relates that her low back pain is significantly worse and is there all the time. She finds it to be
puzzling. She isn't certain whether these relate to her polymyalgia or just what is happening. She hasn't
really had symptoms that are like what she had when her polymyalgia was active. She is able to exercise
regularly. She is taking Tylenol Arthritis 2 tablets twice a day. She isn't certain that it is helping all that much
although she has not stopped the Tylenol to see if she is worse without it. Her general health has otherwise
been good.
Case Studies Page 9-11
Vital Signs: Vitals (Adults) -Weight (lbs): 123 Blood Pressure (R) initial: 132/74
GENERAL APPEARANCE:
The patient appears healthy, and thin. She appears to be in no acute distress. The patient's affect is pleasant. The patient is alert
and oriented times three.
Major Joint Exam:
All joints indicated were examined for tenderness, swelling, range of motion, stability, crepitance, warmth, and erythema:
shoulders, elbows, wrists, MCPs, ankles, MTP joints, toes. These joints were found to be without abnormality unless otherwise
indicated. She does have mild bony hypertrophy suggestive of osteoarthritis scattered through the PIPs and DIPs but these do
not limit her mobility. The R 4th PIP has some mild synovial thickening with tenderness today. The other PIPs and DIPs are
nontender. The knees are cool and have no effusions. There is no joint line tenderness. There is some patellofemoral crepitance.
The patient has some clicking in the acromioclavicular joint on the left side with motion of her shoulders. Her range of motion is
full. There is no subacromial tenderness today.
Skin Exam:
There is no rash, swelling, redness, or other lesions involving the skin on the upper or lower extremities.
Extremities Exam:
There is no clubbing, cyanosis, or edema.
Joint Exam Cont'd:
There are degenerative changes in both great toes, right greater than left. There are degenerative changes scattered through the
right toes; the left toes look better. There is no evidence of synovitis through the MTP joints today.

9/22/2020
15
Conclusion:
Problem #1 Polymyalgia Rheumatica: I don't think her symptoms are consistent with polymyalgia. I can't rule out that the
shoulder symptoms might be consistent but these symptoms are not like what she has had in the past and her symptoms are
not really consistent like I would expect to see if this were due to ongoing inflammation from PMR. We will check her CRP
today.
Problem ?2 Arthralgias: I think most of what she is experiencing relates to degenerative change. I am not finding changes
consistent with an inflammatory process. She understands that polymyalgia can sometimes lead into rheumatoid disease but
at this point I can't make that diagnosis.
Problem #3 Osteoarthritis: The patient has changes of osteoarthritis in scattered joints. She may be having more symptoms
from this as her disease progresses a bit. We talked about having her stop the Tylenol Arthritis to see if her achiness is worse
without the medication. If not there is no sense having her take it. If her achiness is worse, she will restart it as it is the safest
medication she can take. The patient's current pain level is mild. Her functional level is: minimal limitation of activities of
daily living.
Encounter Time:
At least 50% of this visit was spent on counseling and/or coordination of care. Total visit time was: 25
minutes.
Follow-Up Orders:
Follow up: 2 months. The patient will call if there are any problems.
Charge Ticket:
Blood Drawing, C-Reactive Protein
How would you determine the appropriate E/M level for this
encounter?
A. Based on history, exam, and medical decision makingB. Based on the amount of time for the visitC. Based on the MDM and time
D. Based on the exam, MDM, and time
In addition to the E/M service, what additional procedures were performed during the encounter?
A. 36415,86140B. 85025C. 36415,86140,85025D. None of the above
What are the appropriate ICD-10-CM diagnosis codes?
A. M35.3.M15.9B. M35.3.M25.50C. M35.3,M15.0,M25.51D. M35.3.M15.3.M25.50
9/22/2020
16
What is the ICD 10 Code(s)?
What is the CPT Code(s)?
A 67-year-old female patient with Medicare returns to the office for a follow-up of her age-related
osteoporosis. She states she has an achy pain in her left hip that lasts for 30-40 minutes in the morning.
Currently, she has taken ibandronate sodium and alendronate sodium for the past year, and her pain level
is a 7 out of 10. The patient indicates that she has general fatigue and pain in the left hip. All other systems
are negative. She does not smoke or drink. The rheumatologist performs an expanded problem-
focused examination.
Her last dual-energy X-ray absorptiometry (DEXA) was one year ago. After a treatment course is
discussed with the patient, the physician concludes that a DEXA scan is needed, because the patient is on
a current regimen of glucocorticoids. The physician sends her to the imaging room for a dual-energy X-ray
of the axial skeleton and a vertebral fracture assessment, and schedules her for a follow-up visit in
one month.
12 3
4 ROS Complete
Case Studies Page 19-20
9/22/2020
17
CPT: 99213-25, 77085
ICD-10: Diagnosis M81.0, Z79.52
The encounter is coded as 99213 as follows:
* History—The history of the present illness was extended. The review of systems was complete, and the past
medical history and Social was documented. This makes the history detailed. Comprehensive
* Examination—The examination was expanded problem focused.
* Medical decision making—The diagnosis was an established problem worsening; an X-ray was ordered and
her prescription drugs were managed.
77085: Dual-energy X-ray absorptiometry (DEXA), bone density study, one or more sites; axial skeleton (e.g., hips,
pelvis, spine), including vertebral fracture assessment. Do NOT REPORT with 77080
M81.0 is age-related osteoporosis without current pathological fracture. Z79.52 is long-term (current) use of
systemic steroids.
What is the ICD 10 Code(s)?
What is CPT Code(s)?
9/22/2020
18
A 70-year-old female patient comes in for a follow-up visit for pain and stiffness in her left hip. She
injured her hip in a skiing accident three years before and reports the X-rays at that time showed no
fractures. Due to no obvious fracture at the time, she was given ibuprofen and advised to put ice on the
affected area. She is now experiencing increased pain and stiffness in her right hip, usually in the morning,
which has been happening for the past four weeks. She is taking over-the-counter non-steroidal anti-
inflammatory drugs to relieve the pain. The patient does not show any weight loss or gain and has no
complaint of fatigue.
The patient is a fit adult, with a generally good appearance. Her gait is normal. Her muscle strength is
normal in her lower extremities. There is tenderness on palpation of the right hip. There is no swelling or
crepitus. A single-view X-ray of the bilateral hips was done for a comparison. The right hip is normal, but
the left hip shows sclerosis of the superior aspect of the acetabulum, including a single Egger cyst.
The patient is assessed with post-traumatic osteoarthritis of the right hip. Physical therapy is ordered three
times a week for four weeks, and she is prescribed 300 mg ibuprofen twice a day. She is to return for
follow-up in six weeks.
CPT: 99213, 73500-RT, 73500-LT ICD-10: M16.52
This E/M service entailed:
* The history is detailed;
* The examination is expanded problem focused; and
* The medical decision making is of low complexity.
The X-ray reviewed was for radiologic examination, hip, unilateral: one view for the left hip and for the right hip.
M16.52—The diagnosis identifies unilateral post-traumatic osteoarthritis of the left hip.
9/22/2020
19
1997 Musculoskeletal Exam – Case Studies Page 25-28
Year End Questions - Case Studies Page 43 - 46

9/22/2020
20
What is the ICD 10 Code(s)?
What is Evaluation and Management Code?
A 43-year-old patient is seen in the office for a follow-up visit of her RF-positive rheumatoid arthritis and primary osteoarthritis of
the left knee. The patient is on sulindac, methotrexate and folic acid. At her last visit, the patient's methotrexate dose was
increased, which has greatly reduced her pain. Her pain is at Level 2 for her knees. The osteoarthritis is stable. The patient
denies any chest pain; her dyspnea and all other systems are negative.
On examination, the patient is alert and oriented. Her weight is 155 lbs., height 5 feet and 6 inches with a temperature of 98°F.
There is no lymphadenopathy. Her lungs are clear. She has a regular heart rate and rhythm with no murmurs or friction rubs. Her
skin shows no lesions or rashes, and her abdomen is soft with no masses or HSM. Intact Sensation in UE.
Musculoskeletal exam: Bony proliferation and slight ulnar deviation in the bilateral wrists, bony proliferation and slightly
decreased flexion in the bilateral second and fifth PIP joints, and bony proliferation of the bilateral knees. All other joints are
unremarkable with FROM.
Diagnoses:
1. Rheumatoid arthritis with rheumatoid factor;
2. Osteoarthritis of the left knee;
3. Long-term nonsteroidal anti-inflammatory drug (NSAID); and
4. Long-term disease-modifying anti-rheumatic drug (DMARD).
Plan: Complete blood count and liver function tests are ordered to monitor drug toxicity. The patient is to continue on her current
medication regimen. The patient is told to schedule a follow-up visit in two months.
Not in Case Study Packet

9/22/2020
21
CPT: 99214Diagnosis Codes: M05.79, M17.12, Z79.1, Z79.899
Rationale to code this encounter as 99214:
History—The history of present illness was extended. The review of systems was comprehensive, and one of the three past, family and social history were documented. This makes the history level Expanded Problem Focused.
Eight systems were examined. This makes the exam level comprehensive.
Medical decision making—The diagnoses are four established problems stable. Labs were ordered, and the labs were done to monitor toxicity of medication. Prescription Management occurred. This makes the MDM Moderate.
9/22/2020
22
L40.0 Psoriasis Vulgaris
Plaque psoriasis
R21 Rash NOS
86480 Tuberculosis test, cell mediated immunity antigen response measurement; gamma interferon
9/22/2020
23
History
Exam
Medical Decision Making
The ANA test is a test helping to diagnose a suspected autoimmune discorder or rule out other conditions with similar signs and symptoms.
ANA = Antinuclear antibodies
Titer = the concentration of an antibody, as determined by finding the highest dilution at which it is still able to cause agglutination of the antigen.
CPT 86039
9/22/2020
24
95908 - as 4 NCSs were performed. Each motor nerve with F-wave study is considered a single NCS
72114 Radiologic examination, spine, lumbosacral; complete including bending views, minimum of 6 views
9/22/2020
25
20611
20611 59
Modifier 59 indicates the second service was a distinct procedure
72146 Magnetic resonance imaging, spinal canal and contents, thoracic; without contrast
**Assume no contrast unless mentioned**
9/22/2020
26
M32.9 Systemic lupus erythematosus unspecified
SLE NOS
Systemic lupus erythematosus NOS
Systemic lupus erythematosus without organ involvement
unilateral sural sensory nerve,- unilateral peroneal motor nerve recording from extensor digitorum brevis (EDB) with F-wave
- unitateral tibial motor nerve with F-wave?
95908 - three NCSs were performed
9/22/2020
27
Ulna
Radius
Carpals
Metacarpals
Phalanges
E/M level 99213
No it will NOT be billed “Incident to” because the case study does not indicate the physician is providing “direct” supervision. The NP NPI will be listed as the rendering provider on the claim to Medicare
9/22/2020
28
Modifier 26
Radiology Services
Professional component: 26 modifier
Technical component: TC modifier
Place of Service 21 indicates the service was performed in an Inpatient Hospital setting

9/22/2020
29
Report code 95908 in addition to the EMG studies, as four NCSs were performed. For the EMG studies, there were three muscles tested, therefore, report add-on code 95885 for limited EMG studies less than five muscles. If five or more muscles were tested, report code 95886 for complete limb
Extended
9/22/2020
30
M07.661 enteropathic arthropathies right knee
M07 Notes
“Code also associated enteropathy such as regional enteritis “
Excludes 1 PSA (L40.5X)
K50.00 Crohn’s disease of the small intestine without complications
Modifier 24
Apply ONLY to E/M code
The procedure billed previously may have 10 or 90 day global period
9/22/2020
31
Written or verbal request for consult documented in medical record
Consult is documented with provider’s opinion
Written report is sent to the requesting physician
No, Modifier 25 can only be added to an Evaluation and Management service
9/22/2020
32
R68.2 Dry Mouth
Alpha Index: Dry/Mouth R68.2
Tabular: Dry Mouth Unspecified R68.2
Excludes dry mouth due to Sicca Syndrome (Sjogren) (M35.0X)
R70.0 Elevated erythrocyte sedimentation rate (ESR)
M25.541 Pain in joints of right hand
Alpha Index: Pain/Joint/Hand M25.54X
Tabular: Pain in joints of hand right M25.541
72100 Radiologic examination, spine, lumbosacral; 2-3 views
9/22/2020
33
Modifier 25 would be reported with the Evaluation and Management service
Hydration, Therapeutic, Prophylactic, Diagnostic Injections and Infusions, and Chemotherapy and Other Highly Complex Drug or Highly Complex Biologic Agent Administration Guidelines
“For same day E/M service, a different diagnosis is not required”
Pg 717
9/22/2020
34
Advanced Beneficiary Notice required by Medicare when provider determines services may not be covered and the provider plans to collect from the patient for services
Alpha Index: Fibromyalgia M79.7
Tabular:
M79.7 Fibromyalgia
Fibromyositis
Fibrositis
Myofibrositis

9/22/2020
35
80053 Comprehensive Metabolic Panel
36415 Collection of venous blood by venipuncture
72200 Radiologic examination, sacroiliac joint; less than 3 views
9/22/2020
36
CPT Index
Hepatitis/Hepatitis Antibody/Panel/Acute vs Obstetric
80074 Acute hepatitis panel
Page 539
20600 F7 Small joint injection 3rd Right finger
20600 F1 Small joint injection 2nd Left finger
9/22/2020
37
71046 Radiological examination, chest, 2 views,
Old Code maybe on test - 71020
History of Present Illness (HPI)
Review of Systems (ROS)
Past, Family, Social History (PFSH)
9/22/2020
38
20611 RT – 1 unit
20611 LT – 1 unit
OR
20611 50 – 1 unit
Under column “Presenting Problem”, you will see One or more chronic illnesses with mild exacerbation, progression or side effect of treatment which indicates Moderate Risk
9/22/2020
39
Femoral Head
Acetabulum
sheath
DX: M77.11 Right Lateral Epicondylitis
20550 Tendon sheath injection
J1020 Methylpredisolone Acetate (Depomedrol) 20mg

9/22/2020
40
72202 Radiologic examination, sacroiliac joint; 3 or more views
Place of Service
9/22/2020
41
76881 US Complete Examination to include real time scan of muscle, bone, tendon, joint and soft tissue within a specific musculoskeletal area
76882 US Limited Examination – specific anatomical structure examined
POS 11 indicates the service was performed at an office
9/22/2020
42
27096 RT
E/M level 99214
It will be billed “Incident to” because the physician is providing “direct” supervision; the physician’s NPI will be listed as the rendering provider on the claim to Medicare
9/22/2020
43
Add the GA modifier to the procedure
Three
9/22/2020
44
Alpha Index:
Back (see condition)
Pain/low back M54.5
OR
Sciatic (see condition)
Sciatica with lumbago M54.4X
Tabular: M54.41 Lumbago with sciatica, Right side
Tibia
Fibula (Not weight bearing)
Tarsals
Metatarsals
Phalanges
9/22/2020
45
Three
Head
Eyes
Ears, Nose, Mouth, Throat
Remember each would need to be documented
Past history
9/22/2020
46
Under Management Option – Est problem worsening
Table of Risk – Moderate due to pharmacological management
Add the GC modifier
9/22/2020
47
85025 Complete CBC, automated and automated differential WBC count.
20526 Carpal Tunnel Injection
76942 Ultrasound Guidance
J3301 x 1 unit Kenalog
9/22/2020
48
20552 Trigger Point injection because no fluoroscopy was used
J1020 Depomedrol x 1 unit
20611 Aspiration of Baker’s cyst with USG
Alpha index:
Baker’s Cyst – see Cyst, Bakers
Cyst, Bakers M71.2X
M71.21 Synovial cyst of popliteal space (Baker’s) right knee
9/22/2020
49
1997 because I can count an update of 3 chronic conditions as an extended HPI
72074 Radiologic examination, spine, thoracic, minimum 4 views
9/22/2020
50
Alpha index:
Scleroderma, sclerodermia/Systemic M34.9
Tabular: M34.9 Systemic sclerosis unspecified – look above to M34 Systemic Sclerosis (scleroderma)
Alpha index: Long-Term/Steroids/Systemic Z79.52
Tabular: Z79.52 Long term (current) use of Systemic Steroids
You would look under the column “Presenting Problem” and view One stable chronic illness to conclude Low Risk
9/22/2020
51
ROS - Eyes
ROS - Respiratory
9/22/2020
52
86580 Tuberculosis test, intradermal
20606 AC joint injection (medium joint) with USG
J1020 Methylpredisolone Acetate 20mg
9/22/2020
53
ROS – Allergic/Immunologic or Eyes
Under General Multi-System Exam 12 elements in at least 2 organ systems or body areas
Under Single Organ System Exam 12 elements identified by a bullet
9/22/2020
54
ROS - Gastrointestinal
Timing

9/22/2020
55
20553 Trigger point injections 3 or more muscles
J3301 X 4 four muscles injected with 10mg each= 40 mg total
ROS – Psychiatric OR Constitutional
9/22/2020
56
Unable to code RA because it has not been confirmed
We may code the symptoms if documented
ENA = Extractable Nuclear Antigen CPT 86235
Detection of antibodies to the extractable nuclear antigens Sm (Smith), RNP, SS-A (Ro), SS-B (La), Scl-70, and Jo-1 in serum. The results will be reported in ENA Units with corresponding interpretations of negative, borderline or positive.
Report each antibody
9/22/2020
57
CREST
Alpha Index CREST syndrome M34.1
Tabular: CREST syndrome M34.1
OR look at your tabs
Erythrocyte sedimentation rate
ESR
Sed Rate
CPT Sedimentation Rate, Erythrocyte; non automated 85651
VS Automated 85652

9/22/2020
58
If bone density (DEXA or DXA) is performed under 2 years and patient is not taking steroids.
ABN also would not be needed for first bone density
J3420 Injection, vitamin b-12 cyanocobalamin, up to 1000 mc

9/22/2020
59
CPT 80305 Drug Test(s), presumptive, any number of drug classes, any number of devices or procedures; capable of being read by direct optical observation only
Review Page 546 Drug Testing codes
In the HPI, patient will show complaints in a specific anatomical area or disease process
During the exam, the provider may note abnormal findings
The provider changes the medication or increases the dose
The provider orders additional diagnostic tests
9/22/2020
60
72148 Magnetic resonance imaging, spinal canal and contents, lumbar, without contrast material
**Assume no contrast unless mentioned**
ROS - Neurological
9/22/2020
61
J1745 Remicade/Infliximab per 10mg X 50 units
96413 First hour X 1
96415 Additional hours X 2
80048 Basic Metabolic Panel (Calcium Total)
9/22/2020
62
ROS – Endocrine or Integumentary
DX: M17.11 Unilateral primary osteoarthritis of the knee
J7321 X 1 unit EJ modifier
20611 X 1 unit
9/22/2020
63
ROS - Integumentary
You must meet 2 out of 3 to achieve the MDM level (Straightforward, Low Complexity, Moderate Complexity, High Complexity)
9/22/2020
64
95910 - eight NCSs performed + 95886 for complete limb EMG.
No – for a comprehensive level, you can only use organ systems
9/22/2020
65
ROS - Hematologic
Context
9/22/2020
66
1997 Evaluation and Management Guidelines because “using only the Musculoskeletal system”
Perform all elements identified by a bullet; document every element in each box with a shaded border and at least one element in each box with an unshaded border
96413 Chemotherapy administration, intravenous infusion; up to 1 hour
J0129 Orencia, Abatacept per 10mg X 100 units

9/22/2020
67
DX M81.0 Age-related osteoporosis
J1740 Boniva x 3 mg (dose is always 3mg)
96374 Boniva is administered through an IV push
Select the BEST answer - 59
9/22/2020
68
Radiology (7000s series)
Iodine and Barium
50 for bilateral

9/22/2020
69
Alpha Index: Raynaud;s disease (secondary) I73.0
Tabular: I73.00 Raynaud’s syndrome without gangrene
“NOT coded here”
An Excludes1 note indicates that the code excluded should never be used at the same time as the code above the Excludes1 note. An Excludes1 is used when two conditions cannot occur together.
Example:
M30 Polyarteritis nodosa
Excludes1 microscopic polyarteritis (M31.7)
9/22/2020
70




![Moselele Book6 Extraction · [Em][G*]!Iwannarock![Am*]!(ROCK)!rock![Am*]!(ROCK)!rock![Am]!(ROCK)! [Em][G*]!Iwannarock![Am*]!(ROCK)!rock![Am*]!(ROCK)!rock![Am]!(ROCK)! I[Em]!want[C*]!to!rock
























