Embed Size (px)
Citation preview
June 24, 2014 Dr. Bernice Hecker, MD, MHA, FACC Contractor Medical Director Noridian Healthcare Solutions, LLC 900 42nd Street S. P.O. Box 6740 Fargo, ND 58108-6740 Re: LCD DL35236- Draft LCD for Stereotactic Radiation Therapy: Stereotactic Radiosurgery (SRS) and Stereotactic Body Radiation Therapy (SBRT) Dear Dr. Hecker: The American Society for Radiation Oncology* (ASTRO) appreciates the opportunity to review and provide comments on the Noridian Healthcare Solutions, LLC Jurisdiction E, draft LCD DL35236 on Stereotactic Radiosurgery (SRS) and Stereotactic Body Radiation Therapy (SBRT). Noridian accepted some of ASTRO’s previous recommendations sent on April 17, 2012, but in light of recently published data, ASTRO respectfully submits the following comments. Stereotactic Radiosurgery (SRS) Indications The draft LCD states that patients with more than three primary or metastatic brain lesions must be enrolled in an IRB-approved clinical trial or appropriate clinical registry for coverage. ASTRO recommends the removal of the limit on the number of primary or metastatic lesions to determine medical necessity. We recommend a more nuanced approach in which the number of intracranial lesions is not the essential consideration in making a determination to use SRS. A large body of published literature shows that patients presenting with greater than three lesions and excellent performance status also benefit from SRS1-5. Recent studies found Karnofsky Performance Status (KPS) score, not the number of brain metastases, significantly correlated with overall survival2-4. The total intracranial volume rather than the number of metastases has been demonstrated to be an important predictor of survival in two major series4,5. While ASTRO supports the accrual of additional data and research, including the creation of a national SRS * ASTRO is the premier radiation oncology society in the world, with more than 10,000 members who are physicians, nurses, biologist, physicists, radiation therapists, dosimetrists and other health care professionals that specialize in treating patients with radiation therapies. As the leading organization in radiation oncology, the Society is dedicated to improving patient care through professional education and training, support for clinical practice and health policy standards, advancement of science and research, and advocacy. ASTRO publishes two medical journals, International Journal of Radiation Oncology, Biology, Physics (www.redjournal.org) and Practical Radiation Oncology (www.practicalradonc.org); developed and maintains an extensive patient website, www.rtanswers.org; and created the Radiation Oncology Institute (www.roinstitute.com), a non-profit foundation to support research and education efforts around the world that enhance and confirm the critical role of radiation therapy in improving cancer treatment. To learn more about ASTRO, visit www.astro.org.

ASTRO Comments – Noridian Draft LCD (DL35236) for SRS and SBRT Page 2 registry, which we anticipate joining with another professional society, we believe that the limiting criteria listed in items 7,8,and 9 under “Indications for SRS/SBRT (for Cranial Lesions only)” to be unnecessary and overly restrictive. Likewise, item #3 should be deleted. Additionally, the draft policy declares cobalt-60 pallidotomy a non-covered service. In Chapter 13 of the “ASTRO/ACR Guide to Radiation Oncology Coding 2010” under Common Clinical Indications, ASTRO states that SRS may be used as a course of treatment in movement disorders such as Parkinson’s disease, essential tremor, and other disabling tremors when open neurosurgical thalamotomy cannot be performed and medical therapy is unsatisfactory. Several studies support this approach6-8. The draft policy also does not include ICD-9-CM code 333.1 (Essential and Other Specified Forms of Tremor) in the list of codes that support medical necessity. ASTRO’s SRS Model Policy recommends coverage for ICD-9-CM code 333.1 “be limited to the patient who cannot be controlled with medications, has major systemic disease or coagulopathy, and who is unwilling or unsuited for open surgery. Coverage should further be limited to unilateral thalamotomy.” While ASTRO agrees that SRS is not the primary treatment for all patients suffering from functional disorders, stereotactic radiotherapy offers an appropriate alternative for select cases. Thus, we recommend removing the cobalt-60 pallidotomy non-coverage statement and adding ICD-9-CM code 333.1 to the final policy. Stereotactic Body Radiation Therapy (SBRT) Indications ASTRO proposes Noridian remove the requirement that prostate cancer patients be enrolled in an IRB-approved clinical trial or registry. ASTRO updated its SBRT Model Policy in April 2013 to reflect the many clinical studies now supporting SBRT in the treatment of prostate cancer. The clinical data has matured to a point where SBRT represents an appropriate alternative for select patients with low to intermediate risk prostate cancer. A recently published pooled analysis of 1100 patients enrolled on prospective trials of SBRT for prostate cancer demonstrates biochemical relapse-free survival rates and quality of life outcomes that compare favorably with other definitive treatments for prostate cancer 9,10. After a median dose of 36.25 Gy in 4-5 fractions, the 5-year biochemical relapse free survival rate was 93% for all patients; 95%, 83% and 78% for GS ⩽6, 7 and ⩾8, respectively; and 95%, 84% and 81% for low-, intermediate- and high-risk patients, respectively. A transient decline in the urinary and bowel domains was observed within the first 3 months after SBRT which returned to baseline status or better within 6 months and remained so beyond 5 years. In addition, SBRT’s cost effectiveness relative to other forms of radiation therapy of prostate cancer11,12 in this is appealing in this setting. Additionally, the draft policy lacks crucial ICD-9-CM codes indicated for SBRT including those for “recurrent pelvic and head and neck tumors that have recurred after primary irradiation”, listed on page seven of the LCD. SBRT may also treat patients with recurrent nodal metastasis who have already undergone prior conventionally fractionated radiotherapy and thus the corresponding diagnosis codes should be included in the policy. ASTRO recommends the following ICD-9-CM codes be added to the final LCD:
• 147.0-149.9 Malignant neoplasms of the pharynx
ASTRO Comments – Noridian Draft LCD (DL35236) for SRS and SBRT Page 3
• 160.0-161.9 Malignant neoplasms of the nasal cavities, accessory sinuses, and larynx
• 154.0-154.8 Malignant neoplasms of the rectum and anus • 179-184.9 Malignant neoplasms of the female reproductive system • 195.2 Malignant neoplasm of abdomen • 195.3 Malignant neoplasm of pelvis • 196.0-196.9 Secondary and unspecified malignant nodal neoplasms
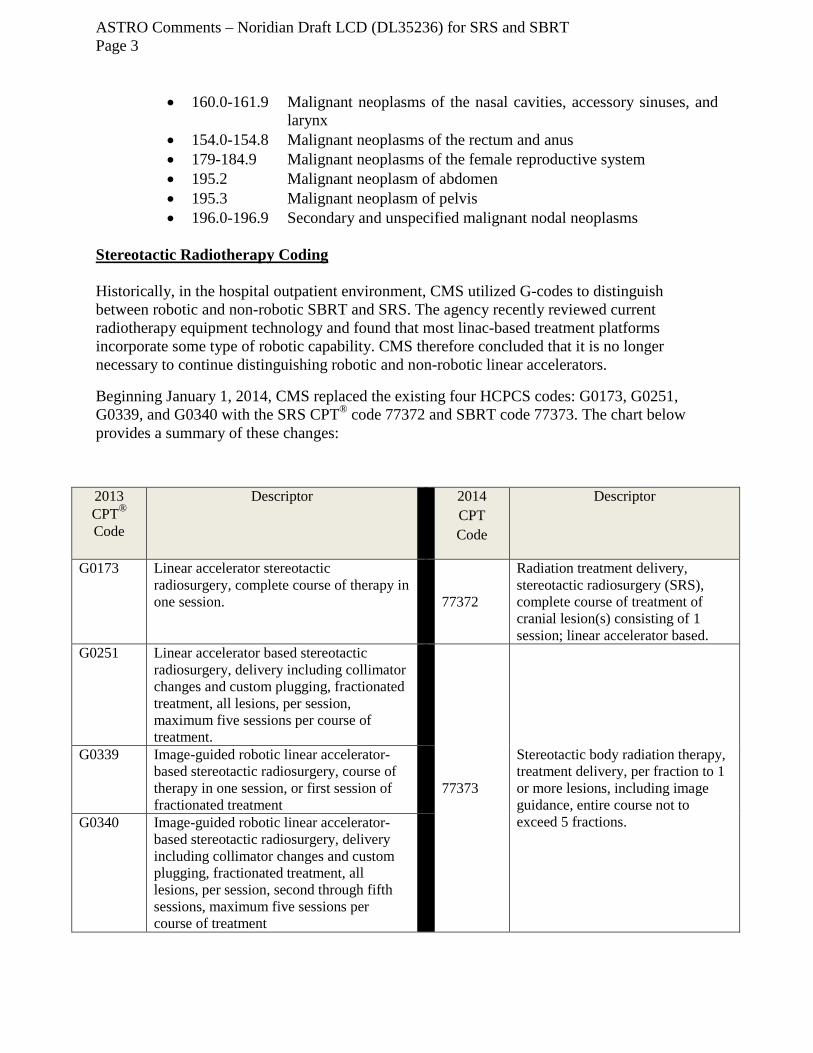
Stereotactic Radiotherapy Coding Historically, in the hospital outpatient environment, CMS utilized G-codes to distinguish between robotic and non-robotic SBRT and SRS. The agency recently reviewed current radiotherapy equipment technology and found that most linac-based treatment platforms incorporate some type of robotic capability. CMS therefore concluded that it is no longer necessary to continue distinguishing robotic and non-robotic linear accelerators.
Beginning January 1, 2014, CMS replaced the existing four HCPCS codes: G0173, G0251, G0339, and G0340 with the SRS CPT® code 77372 and SBRT code 77373. The chart below provides a summary of these changes:
2013 CPT® Code
Descriptor 2014 CPT Code
Descriptor
G0173 Linear accelerator stereotactic radiosurgery, complete course of therapy in one session.
77372
Radiation treatment delivery, stereotactic radiosurgery (SRS), complete course of treatment of cranial lesion(s) consisting of 1 session; linear accelerator based.
G0251 Linear accelerator based stereotactic radiosurgery, delivery including collimator changes and custom plugging, fractionated treatment, all lesions, per session, maximum five sessions per course of treatment.
77373
Stereotactic body radiation therapy, treatment delivery, per fraction to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions.
G0339 Image-guided robotic linear accelerator-based stereotactic radiosurgery, course of therapy in one session, or first session of fractionated treatment
G0340 Image-guided robotic linear accelerator-based stereotactic radiosurgery, delivery including collimator changes and custom plugging, fractionated treatment, all lesions, per session, second through fifth sessions, maximum five sessions per course of treatment
ASTRO Comments – Noridian Draft LCD (DL35236) for SRS and SBRT Page 4 The draft coverage policy lists G-codes in the “CPT/HCPCS Code” section. In order to avoid any confusion, ASTRO recommends Noridian remove all G-codes from the final LCD.
Enclosed for your reference are the current version of ASTRO’s SRS and SBRT Model Coverage Policies. ASTRO recently mailed Noridian complimentary copies of the ASTRO/ACR Guide to Radiation Oncology Coding 2010: 2014 Supplement. Chapters 13 and 14 provide extensive coding information for these technologies including the codes integral to the process of care. Since no specific codes for SRS planning or for the professional component of SBRT planning exist, other codes such as CPT code 77295 (3-dimensional radiotherapy plan, including dose-volume histograms) or IMRT CPT code 77301 (Intensity modulated radiotherapy plan, including dose-volume histograms for target and critical structure partial tolerance specifications) are appropriate. Thank you for your consideration of our comments. Should you have any questions or wish to discuss SRS/SBRT and our recommendations further, please contact ASTRO’s Assistant Director of Health Policy, Anne Hubbard, at (703) 839-7394 or via email at [email protected]. Sincerely, Laura I Thevenot Chief Executive Officer cc: Arthur Lurvey, MD Richard Whitten, MD, MBA, FACP Enclosures: ASTRO SRS Model Policy ASTRO SBRT Model Policy ASTRO/ACR Guide to Radiation Oncology Coding – Chapter 13 and 14
Radiotherpetuic and surgical management for newly diagnosed brain metastasis(es): an American Society for Radiaion Oncology evidence based guideline
References:
1. Serizawa T, Hirai T, Nagano O, et al. Gamma knife surgery for 1–10 brain metastases without prophylactic whole-brain radiation therapy: analysis of cases meeting the Japanese prospective multi-institute study (JLGK0901) inclusion criteria. J Neurooncol. 2010; 98(2): 163-167.
2. Hunter GK, Suh JH, Reuther AM, et al. Treatment of five or more brain metastases with stereotactic radiosurgery. Int J Radiat Oncol Biol Phys. 2012; 83(5): 1394-1398.
3. Raldow AC, Chiang VL, Knisely JP, et al. Survival and intracranial control of patients with 5 or more brain metastases treated with gamma knife stereotactic radiosurgery. Am J Clin Oncol. 2013; 36(5): 486-490.
4. Bhatnagar AK, Flickinger JC, Kondziolka D, Lunsford LD. Stereotactic radiosurgery for four or more intracranial metastases. Int J Radiat Oncol Biol Phys. 2006; 64(3):898-903.
5. Likhacheva A, Pinnix CC, Parikh NR, et al. Predictors of survival in contemporary practice after initial radiosurgery for brain metastases, Int J Radiat Oncol Biol Phys. 2013; 85(3): 656-661.

ASTRO Comments – Noridian Draft LCD (DL35236) for SRS and SBRT Page 5
6. Kooshkabadi A, Lunsford LD, Tonetti D, et al. Gamma Knife thalamotomy for tremor in the magnetic resonance imaging era. J Neurosurg. 2013; 118(4):713-8.
7. Ohye C1, Higuchi Y, Shibazaki T, et al. Gamma knife thalamotomy for Parkinson disease and essential tremor: a prospective multicenter study. Neurosurgery. 2012; 70(3):526-535.
8. Young RF, Li F, Vermeulen S, Meier R. Gamma Knife thalamotomy for treatment of essential tremor: long-term results. J Neurosurg. 2010; 112(6):1311-1317.
9. King CR, Freeman D, Kaplan I, et al. Stereotactic body radiotherapy for localized prostate cancer: pooled analysis from a multi-institutional consortium of prospective phase II trials. Radiother and Oncol. 2013; 109(2): 217-221.
10. King CR, Collins S, Fuller D, et al. Health-related quality of life after stereotactic body radiation therapy for localized prostate cancer: results from a multi-institutional consortium of prospective trials. Int J Radiat Oncol Biol Phys. 2013; 87(5): 939-945.
11. Hodges JC, Lotan Y, Boike TP, et al. Cost-effectiveness analysis of stereotactic body radiation therapy versus intensity-modulated radiation therapy: an emerging initial radiation treatment option for organ-confined prostate cancer. J Oncol Practice. 2012; 8(3 Suppl):e31s-37s.
12. Parthan A, Pruttivarasin N, Davies D, et al. Comparative cost-effectiveness of stereotactic body radiation therapy versus intensity-modulated and proton radiation therapy for localized prostate cancer. Front Oncol. 2012; 2:81.

American Society for Radiation Oncology (ASTRO) Stereotactic Radiosurgery (SRS) Model Coverage Policy
AMA CPT / Copyright Statement CPT® codes, descriptions and other data only are copyright 2010 American Medical Association (or such other date of publication of CPT). CPT is a registered trademark of the American Medical Association. All Rights Reserved. Indications and Limitations of Coverage and/or Medical Necessity This Model Policy1 addresses coverage for Stereotactic Radiosurgery (SRS). Stereotactic Radiosurgery (SRS) is a distinct discipline that utilizes externally generated ionizing radiation in certain cases to inactivate or eradicate a defined target(s) in the head or spine without the need to make an incision. The target is defined by high-resolution stereotactic imaging. To assure quality of patient care, the procedure involves a multidisciplinary team consisting of a neurosurgeon, radiation oncologist, and medical physicist. (For a subset of tumors involving the skull base, the multidisciplinary team may also include a head and neck surgeon with training in stereotactic radiosurgery). The adjective “Stereotactic” describes a procedure during which a target lesion is localized relative to a fixed three dimensional reference system, such as a rigid head frame affixed to a patient, fixed bony landmarks, a system of implanted fiducial markers, or other similar system. This type of localization procedure allows physicians to perform image-guided procedures with a high degree of anatomic accuracy and precision. Stereotactic radiosurgery (SRS) couples this anatomic accuracy and reproducibility with very high doses of highly precise, externally generated, ionizing radiation, thereby maximizing the ablative effect on the target(s) while minimizing collateral damage to adjacent tissues. SRS requires computer-assisted, three-dimensional planning and delivery with stereotactic and convergent-beam technologies, including, but not limited to: multiple convergent cobalt sources (e.g. Gamma Knife®); protons; multiple, coplanar or non-coplanar photon arcs or angles (e.g. XKnife®); fixed photon arcs; or image-directed robotic devices (e.g. CyberKnife®) that meet the criteria. SRS typically is performed in a single session, using a rigidly attached stereotactic guiding device, other immobilization technology and/or a stereotactic-guidance system, but can be performed in a limited number of sessions, up to a maximum of five. Regardless of the number of sessions, all SRS procedures include the following components:
1. Position stabilization (attachment of a frame or frameless) 2. Imaging for localization (CT, MRI, angiography, PET, etc.) 3. Computer assisted tumor localization (i.e. “Image Guidance”)
1 ASTRO model policies were developed as a means to efficiently communicate what ASTRO believes to be correct coverage policies for radiation oncology services. The ASTRO Model Policies do not serve as clinical guidelines and they are subject to periodic review and revision without notice. The ASTRO Model Policies may be reproduced and distributed, without modification, for noncommercial purposes.

4. Treatment planning - number of isocenters, number, placement and length of arcs or angles, number of beams, beam size and weight, etc.
5. Isodose distributions, dosage prescription and calculation 6. Setup and accuracy verification testing 7. Simulation of prescribed arcs or fixed portals
Radiation oncologists and neurosurgeons have separate CPT billing codes for SRS. CPT Codes 61781–61783, 61796-61800 and 63620 and 63621 are reported for the work attributed to the neurosurgeon. These codes are mutually exclusive with the radiation oncology CPT codes 77432 and 77435; therefore the same physician should not bill for both of these codes. A radiation oncologist may bill the SRS management code 77432 (stereotactic radiation treatment management of cranial lesion(s) (complete course of treatment consisting of one session) for single fraction intracranial SRS (and only once per treatment course) when and only when fully participating in the management of the procedure. CPT 77432 will be paid only once per course of treatment for cranial lesions regardless of the number of lesions. When SRS is administered in more than one but not more than five fractions to the brain or in one through five fractions to the spine, the radiation oncologist should instead bill the Stereotactic Body Radiation Therapy (SBRT) code 77435 to cover patient management during that course of therapy. CPT 77435 will be paid only once per course of therapy regardless of the number of sessions, lesions or days of treatment. The radiation oncologist may not bill 77432 and 77435 for the same course of therapy. In addition to the management codes, a radiation oncologist may bill other appropriate radiation oncology (77xxx) codes for services performed prior to the delivery of SRS as indicated by the pattern of care and other Medicare policies. No one physician may bill both the neurosurgical codes 61781-83, 61796–61800, 63620 or 63621 and the radiation oncology 77XXX codes. If either the radiation oncologist or the neurosurgeon does not fully participate in the patient’s care, that physician must take care to indicate this change by use of the appropriate -54 modifier (followed by any appropriate -55 modifier) on the global procedure(s) submitted. As the services are collegial in nature with different specialties providing individual components of the treatment, surgical assistants will not be reimbursed. The technical charges used by hospital-based and outpatient facilities for SRS delivery are described by the CPT codes listed below. It is not appropriate to bill more than one treatment delivery code on the same day of service, even though some types of delivery may have elements of several modalities (for example, a stereotactic approach with IMRT). Only one delivery code is to be billed. Other radiation oncology professional and technical services required prior to the delivery of SRS are coded separately and may be appropriately billed by the radiation oncologist, when necessary.
ASTRO SRS Model Coverage Policy Page 2 Final Approval 1-14-11 Updated 7-25-11

Indications for SRS: 1. Primary central nervous system malignancies, generally used as a boost or salvage
therapy for lesions <5cm. 2. Primary and secondary tumors involving the brain or spine parenchyma, meninges/dura,
or immediately adjacent bony structures. 3. Benign brain tumors and spinal tumors such as meningiomas, acoustic neuromas, other
schwannomas, pituitary adenomas, pineocytomas, craniopharyngiomas, glomus tumors, hemangioblastomas
4. Arteriovenous malformations and cavernous malformations. 5. Other cranial non-neoplastic conditions such as trigeminal neuralgia and select cases of
medically refractory epilepsy. As a boost treatment for larger cranial or spinal lesions that have been treated initially with external beam radiation therapy or surgery (e.g. sarcomas, chondrosarcomas, chordomas, and nasopharyngeal or paranasal sinus malignancies).
6. Metastatic brain or spine lesions, with stable systemic disease, Karnofsky Performance Status 40 or greater (and expected to return to 70 or greater with treatment), and otherwise reasonable survival expectations, OR an Eastern Cooperative Oncology Group (ECOG) Performance Status of 3 or less (or expected to return to 2 or less with treatment).
7. Relapse in a previously irradiated cranial or spinal field where the additional stereotactic precision is required to avoid unacceptable vital tissue radiation.
Limitations: SRS is not considered medically necessary under the following circumstances:
1. Treatment for anything other than a severe symptom or serious threat to life or critical functions.
2. Treatment unlikely to result in functional improvement or clinically meaningful disease stabilization, not otherwise achievable.
3. Patients with wide-spread cerebral or extra-cranial metastases with limited life expectancy unlikely to gain clinical benefit within their remaining life.
4. Patients with poor performance status (Karnofsky Performance Status less than 40 or ECOG Performance greater than 3) - see Karnofsky and ECOG Performance Status scales below.
5. For ICD-9-CM code 333.1, essential tremor, coverage should be limited to the patient who cannot be controlled with medication, has major systemic disease or coagulopathy, and who is unwilling or unsuited for open surgery. Coverage should further be limited to unilateral thalamotomy.
ASTRO SRS Model Coverage Policy Page 3 Final Approval 1-14-11 Updated 7-25-11

Karnofsky Performance Status Scale 100 Normal; no complaints, no evidence of disease 90 Able to carry on normal activity; minor signs or symptoms of disease 80 Normal activity with effort; some signs or symptoms of disease 70 Cares for self; unable to carry on normal activity or to do active work 60 Requires occasional assistance but is able to care for most needs 50 Requires considerable assistance and frequent medical care 40 Disabled; requires special care and assistance 30 Severely disabled; hospitalization is indicated although death not imminent 20 Very sick; hospitalization necessary; active supportive treatment is necessary 10 Moribund, fatal processes progressing rapidly 0 Dead Karnofsky DA, Burchenal JH. (1949). "The Clinical Evaluation of Chemotherapeutic Agents in Cancer." In: MacLeod CM (Ed), Evaluation of Chemotherapeutic Agents. Columbia Univ Press. Page 196. ECOG Performance Status Scale Grade 0: Fully active, able to carry on all pre-disease performance without
restriction. Grade 1: Restricted in physically strenuous activity but ambulatory and able to
carry out work of a light or sedentary nature, e.g. light house work, office work.
Grade 2: Ambulatory and capable of all self-care but unable to carry out and work activities. Up and about more than 50% of waking hours.
Grade 3: Capable of only limited self-care, confined to bed or chair more than 50% of waking hours.
Grade 4: Completely disabled. Cannot carry on any self-care. Totally confined to bed or chair.
Grade 5: Dead
Eastern Cooperative Oncology Group, Robert Comis M.D., Group Chair.
* As published in Am. J. Clin. Oncol.:Oken, M.M., Creech, R.H., Tormey, D.C., Horton, J., Davis, T.E., McFadden, E.T., Carbone, P.P.: Toxicity And Response Criteria Of The Eastern Cooperative Oncology Group. Am J Clin Oncol 5:649-655, 1982. CPT/HCPCS Codes Note: Uses of 77435 and 77373 are addressed in both this Model Policy and in the Stereotactic Body Radiation Therapy Model Policy. 77371 Radiation treatment delivery, stereotactic radiosurgery (SRS), complete course of treatment of cranial lesion(s) consisting of 1 session; multi-source Cobalt 60 based
ASTRO SRS Model Coverage Policy Page 4 Final Approval 1-14-11 Updated 7-25-11
77372 Radiation treatment delivery, stereotactic radiosurgery (SRS), complete course of treatment of cranial lesion(s) consisting of 1 session; linear accelerator based 77373 Stereotactic body radiation therapy, treatment delivery, per fraction to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions. (Do not report 77373 in conjunction with 77401-77416, 77418). (For single fraction cranial lesion, see 77371, 77372) 77432 Stereotactic radiation treatment management of cranial lesion(s) (complete course of treatment consisting of 1 session)
(The same physician should not report both stereotactic radiosurgery services [61796-61800] and radiation treatment management [77432 or 77435] for cranial lesions)
(For stereotactic body radiation therapy treatment, use 77435)
77435 Stereotactic body radiation therapy, treatment management, per treatment course, to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions (Do not report 77435 in conjunction with 77427-77432) (The same physician should not report both stereotactic radiosurgery services [63620, 63621] and radiation treatment management [77435] for extracranial lesions) G0173 Linear accelerator based stereotactic radiosurgery, complete course of therapy in one session G0251 Linear accelerator based stereotactic radiosurgery, delivery including collimator changes and custom plugging, fractionated treatment, all lesions, per session, maximum five sessions per course of treatment G0339 Image-guided robotic linear accelerator-based stereotactic radiosurgery, complete course of therapy in one session or first session of fractionated treatment G0340 Image-guided robotic linear accelerator-based stereotactic radiosurgery, delivery including collimator changes and custom plugging, fractionated treatment, all lesions, per session, second through fifth sessions, maximum five sessions per course of treatment ICD-9 Codes that Support Medical Necessity Note: Diagnosis codes are based on the current ICD-9-CM codes that are effective at the time of Model Policy publication. Any updates to ICD-9-CM codes will be reviewed by ASTRO, and coverage should not be presumed until the results of such review have been published/posted. These ICD-9-CM codes support medical necessity under this Model Policy: 147.0 MALIGNANT NEOPLASM OF SUPERIOR WALL OF NASOPHARYNX 147.1 MALIGNANT NEOPLASM OF POSTERIOR WALL OF NASOPHARYNX 147.2 MALIGNANT NEOPLASM OF LATERAL WALL OF NASOPHARYNX 147.3 MALIGNANT NEOPLASM OF ANTERIOR WALL OF NASOPHARYNX
ASTRO SRS Model Coverage Policy Page 5 Final Approval 1-14-11 Updated 7-25-11

147.8 MALIGNANT NEOPLASM OF OTHER SPECIFIED SITES OF NASOPHARYNX 147.9 MALIGNANT NEOPLASM OF NASOPHARYNX UNSPECIFIED SITE 160.0 MALIGNANT NEOPLASM OF NASAL CAVITIES 160.1 MALIGNANT NEOPLASM OF AUDITORY TUBE MIDDLE EAR AND MASTOID
AIR CELLS 160.2 MALIGNANT NEOPLASM OF MAXILLARY SINUS 160.3 MALIGNANT NEOPLASM OF ETHMOIDAL SINUS 160.4 MALIGNANT NEOPLASM OF FRONTAL SINUS 160.5 MALIGNANT NEOPLASM OF SPHENOIDAL SINUS 160.8 MALIGNANT NEOPLASM OF OTHER ACCESSORY SINUSES 160.9 MALIGNANT NEOPLASM OF ACCESSORY SINUS UNSPECIFIED 191.0 MALIGNANT NEOPLASM OF CEREBRUM EXCEPT LOBES AND VENTRICLES 191.1 MALIGNANT NEOPLASM OF FRONTAL LOBE 191.2 MALIGNANT NEOPLASM OF TEMPORAL LOBE 191.3 MALIGNANT NEOPLASM OF PARIETAL LOBE 191.4 MALIGNANT NEOPLASM OF OCCIPITAL LOBE 191.5 MALIGNANT NEOPLASM OF VENTRICLES 191.6 MALIGNANT NEOPLASM OF CEREBELLUM NOS 191.7 MALIGNANT NEOPLASM OF BRAIN STEM 191.8 MALIGNANT NEOPLASM OF OTHER PARTS OF BRAIN 191.9 MALIGNANT NEOPLASM OF BRAIN UNSPECIFIED SITE 192.0 MALIGNANT NEOPLASM OF CRANIAL NERVES 192.1 MALIGNANT NEOPLASM OF CEREBRAL MENINGES 194.3 MALIGNANT NEOPLASM OF PITUITARY GLAND AND CRANIOPHARYNGEAL
DUCT 194.4 MALIGNANT NEOPLASM OF PINEAL GLAND 194.6 MALIGNANT NEOPLASM OF AORTIC BODY AND OTHER PARAGANGLIA 198.3 SECONDARY MALIGNANT NEOPLASM OF BRAIN AND SPINAL CORD 198.4* SECONDARY MALIGNANT NEOPLASM OF OTHER PARTS OF NERVOUS
SYSTEM 198.5* SECONDARY MALIGNANT NEOPLASM OF BONE AND BONE MARROW 198.89* SECONDARY MALIGNANT NEOPLASM OF OTHER SPECIFIED SITES 225.0 BENIGN NEOPLASM OF BRAIN 225.1 BENIGN NEOPLASM OF CRANIAL NERVES 225.2 BENIGN NEOPLASM OF CEREBRAL MENINGES 227.3 BENIGN NEOPLASM OF PITUITARY GLAND AND CRANIOPHARYNGEAL DUCT 227.4 BENIGN NEOPLASM OF PINEAL GLAND 227.5 BENIGN NEOPLASM OF CAROTID BODY 227.6 *BENIGN NEOPLASM OF AORTIC BODY AND OTHER PARAGANGLIA 228.02 HEMANGIOMA OF INTRACRANIAL STRUCTURES 237.0 NEOPLASM OF UNCERTAIN BEHAVIOR OF PITUITARY GLAND AND
CRANIOPHARYNGEAL DUCT 237.1 NEOPLASM OF UNCERTAIN BEHAVIOR OF PINEAL GLAND 237.3* NEOPLASM OF UNCERTAIN BEHAVIOR OF PARAGANGLIA 237.5* NEOPLASM OF UNCERTAIN BEHAVIOR OF BRAIN AND SPINAL CORD 237.6* NEOPLASM OF UNCERTAIN BEHAVIOR OF MENINGES
ASTRO SRS Model Coverage Policy Page 6 Final Approval 1-14-11 Updated 7-25-11
239.6* NEOPLASM OF UNSPECIFIED NATURE OF BRAIN 239.7* NEOPLASM OF UNSPECIFIED NATURE OF ENDOCRINE GLANDS AND OTHER
PARTS OF NERVOUS SYSTEM 332.0 PARALYSIS AGITANS 333.1** ESSENTIAL AND OTHER SPECIFIED FORMS OF TREMOR 345.11 GENERALIZED CONVULSIVE EPILEPSY WITH INTRACTABLE EPILEPSY 345.3 GRAND MAL STATUS EPILEPTIC 345.91 EPILEPSY UNSPECIFIED WITH INTRACTABLE EPILEPSY 350.1 TRIGEMINAL NEURALGIA 350.8 OTHER SPECIFIED TRIGEMINAL NERVE DISORDERS 350.9 TRIGEMINAL NERVE DISORDER UNSPECIFIED 351.0 BELL'S PALSY 351.1 GENICULATE GANGLIONITIS 351.8 OTHER FACIAL NERVE DISORDERS 351.9 FACIAL NERVE DISORDER UNSPECIFIED 352.0* DISORDERS OF OLFACTORY (1ST) NERVE 352.1* GLOSSOPHARYNGEAL NEURALGIA 352.2* OTHER DISORDERS OF GLOSSOPHARYNGEAL (9TH) NERVE 352.3* DISORDERS OF PNEUMOGASTRIC (10TH) NERVE 352.4* DISORDERS OF ACCESSORY (11TH) NERVE 352.5* DISORDERS OF HYPOGLOSSAL (12TH) NERVE 352.6* MULTIPLE CRANIAL NERVE PALSIES 352.9* UNSPECIFIED DISORDER OF CRANIAL NERVES 747.81* CONGENITAL ANOMALIES OF CEREBROVASCULAR SYSTEM 990*** EFFECTS OF RADIATION UNSPECIFIED * ICD-9-CM codes 198.4, 198.5, 198.89, 234.8, 237.5, 237.6, 239.6, 239.7, 333.1, 352.0, 352.1, 352.2, 352.3, 352.4, 352.5, 352.6, 352.9 and 747.81 are all limited to use for lesions occurring either above the neck or in the spine. ** ICD-9-CM 333.1 code is limited to the patient who cannot be controlled with medication, has major systemic disease or coagulopathy, and who is unwilling or unsuited for open surgery. *** ICD-9-CM 990 may only be used where prior radiation therapy to the site is the governing factor necessitating SRS in lieu of other radiotherapy. An ICD-9-CM code for the anatomic diagnosis must also be used. General Information Documentation Requirements The patient's record must support the necessity and frequency of treatment. Medical records should include not only the standard history and physical but also the patient's functional status and a description of current performance status (Karnofsky Performance Status or ECOG Performance Status). See Karnofsky Performance Status or ECOG Performance Status listed under Indications and Limitation of Coverage above.
ASTRO SRS Model Coverage Policy Page 7 Final Approval 1-14-11 Updated 7-25-11

Documentation should include the date and the current treatment dose. A radiation oncologist and a neurosurgeon must evaluate the clinical aspects of the treatment, and document and sign this evaluation as well as the resulting management decisions. A radiation oncologist and medical physicist must evaluate the technical aspects of the treatment and document and sign this evaluation as well as the resulting treatment management decisions. For Medicare claims, the HCPCS/CPT code(s) may be subject to Correct Coding Initiative (CCI) edits. This policy does not take precedence over CCI edits. Please refer to the CCI for correct coding guidelines and specific applicable code combinations prior to billing Medicare.
ASTRO SRS Model Coverage Policy Page 8 Final Approval 1-14-11 Updated 7-25-11
SRS References
1. Adler JR Jr, Gibbs IC, Puataweepong P, Chang SD. Visual field preservation after multisession cyberknife radiosurgery for perioptic lesions. Neurosurgery. 2006 Aug; 59(2):244-54; discussion 244-54. 2. American College of Radiology ACR Appropriateness Criteria Brain Metastasis. 2006. Accessed April 2009. Available at: http://www.acr.org/SecondaryMainMenuCategories/quality_safety/app_criteria/pdf/Expert
3. American College of Radiology Practice Guideline for the performance of Stereotactic Radiosurgery. Effective 10/01/2006. Accessed April 2009. Available at URL address: http://www.acr.org/ SecondaryMainMenuCategories/ quality_safety/guidelines/ro/ stereotactic_radiosurgery.aspx 4. American College of Radiology Practice Guideline for the Performance of Stereotactic Body Radiation Therapy. Amended 2006 Accessed April 2009. Available at: http://www.acr.org /Secondary MainMenuCategories /quality_safety/ guidelines /ro/stereo_body_radiation.aspx 5. American Society for Radiation Oncology (ASTRO). Report of the ASTRO Emerging Technology Committee (ETC) September 19, 2008 Stereotactic Body Radiotherapy (SBRT) For Primary Management of Early-Stage, Low-Intermediate Risk Prostate Cancer Available at: http://www.astro.org/HealthPolicy/EmergingTechnology/EvaluationProjects/documents/SBRTpros.pdf. Accessed April 2009. 6. American Society for Therapeutic Radiation and Oncology (ASTRO). The ASTRO/ACR Guide to Radiation Oncology Coding 2007. Fairfax, VA: ASTRO; 2007. 7. Andrews DW, Scott CB, Sperduto PW, Flanders AE, Gaspar LE, Schell MC, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet. 2004 May 22; 363(9422):1665-72. 8. Aoyama H, Shirato H, Tago M, Nakagawa K, Toyoda T, Hatano K, et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. JAMA. 2006 Jun 7; 295(21):2483-91. 9. Barajas MA, Ramirez-Guzman MG, Rodriguez-Vazquez C, Toledo-Buenrostro V, Cuevas-Solorzano A, Rodriguez-Hernandez G. Gamma Knife surgery for hypothalamic hamartomas accompanied by medically intractable epilepsy and precocious puberty: experience in Mexico. J Neurosurg. 2005 Jan; 102 Suppl: 53-5. 10. Barbaro NM, Quigg M, Broshek DK, et al. A multicenter, prospective pilot study of gamma knife radiosurgery for mesial temporal lobe epilepsy: seizure response, adverse
ASTRO SRS Model Coverage Policy Page 9 Final Approval 1-14-11 Updated 7-25-11
events, and verbal memory. Ann Neurol. 2009 Feb;65(2):167-75. 11. Barcia-Salorio JL, Barcia JA, Hernandez G, Lopez-Gomez L. Radiosurgery of epilepsy. Long-term results. Acta Neurochir Suppl (Wien). 1994; 62:111-113. 12. Barnett GH, Linskey ME, Adler JR, Cozzens JW, Friedman WA, Heilbrun MP, Lunsford LD, Schulder M, Sloan AE; American Association of Neurological Surgeons; Congress of Neurolofical Surgeons Washington Committee Stereotactic Radiosurgery Task Force. Stereotactic radiosurgery--an organized neurosurgery-sanctioned definition. J Neurosurg. 2007 Jan; 106(1):1-5. 13. Bhatnagar AK, Flickinger JC, Kondziolka D, Lunsford LD. Stereotactic radiosurgery for four or more intracranial metastases. Int J Radiat Oncol Biol Phys. 2006 Mar 1; 64(3):898-903. 14. Brisman R. Microvascular decompression vs. Gamma Knife radiosurgery for typical trigeminal neuralgia: preliminary findings. Stereotact Funct Neurosurg. 2007; 85(2-3):94-8. 15. Chang SD, Gibbs IC, Sakamoto GT, Lee E, Oyelese A, Adler JR Jr. Staged stereotactic irradiation for acoustic neuroma. Neurosurgery. 2005 Jun; 56(6):1254-61; discussion 1261-3. 16. Chougule PB, Burton-WilliamsM, Saris S, Zheng Z, Ponte B, Noren G, et al. Randomized treatment of brain metastases with Gamma Knife radiosurgery, whole brain radiotherapy or both (abstract). International Journal of Radiation Oncology, Biology, Physics 2000; 48: 114. 17. Chua DT, Sham JS, Hung KN, Leung LH, Au GK. Predictive factors of tumor control and survival after radiosurgery for local failures of nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2006 Dec 1; 66(5):1415-21. 18. Cohen VM, Carter MJ, Kemeny A, Radatz M, Rennie IG. Metastasis-free survival following treatment for uveal melanoma with either stereotactic radiosurgery or enucleation. Acta Ophthalmol Scand. 2003 Aug; 81(4):383-8. 19. Dieckmann K, Georg D, Bogner J, Zehetmayer M, Petersch B, Chorvat M, et al. Optimizing LINAC based stereotactic radiotherapy of uveal melanomas: 7 years' clinical experience. Int J Radiat Oncol Biol Phys. 2006 Nov 15; 66(4 Suppl):S47-52. 20. Donnet A, Tamura M, Valade D, RJ. Trigeminal nerve radiosurgical treatment in intractable chronic cluster headache: unexpected high toxicity. Neurosurgery. 2006 Dec; 59(6):1252-7; discussion 1257. 21. Dodd RL, Ryu MR, Kamnerdsupaphon P, Gibbs IC, Chang SD Jr, Adler JR Jr. CyberKnife radiosurgery for benign intradural extramedullary spinal tumors. Neurosurgery. 2006 Apr; 58(4):674-85; discussion 674-85.
ASTRO SRS Model Coverage Policy Page 10 Final Approval 1-14-11 Updated 7-25-11
22. Duma CM. Movement disorder radiosurgery--planning, physics and complication avoidance. Prog Neurol Surg. 2007; 20:249-66. 23. ECRI Institute Health Technology Assessment Information Service (HTAIS). CyberKnife and Gamma Knife Radiosurgery for Trigeminal Neuralgia. Hotline Response. May 2007. Archived 24. Elia AE, Shih HA, Loeffler JS. Stereotactic radiation treatment for benign meningiomas. Neurosurg Focus. 2007; 23(4):E5. 25. Friehs GM, Park MC, Goldman MA, Zerris VA, NorG, Sampath P. Stereotactic radiosurgery for functional disorders. Neurosurg Focus. 2007; 23(6):E3. 26. Gagnon GJ, Henderson FC, Gehan EA, Sanford D, Collins BT, Moulds JC, Dritschilo A. Cyberknife radiosurgery for breast cancer spine metastases: a matched-pair analysis. Cancer. 2007 Oct 15; 110(8):1796-802. 27. Gerszten PC, Burton SA, Ozhasoglu C, Welch WC. Radiosurgery for spinal metastases: clinical experience in 500 cases from a single institution. Spine. 2007 Jan 15; 32(2):193-9. 28. Gerszten PC, Burton SA. Clinical Assessment of Stereotactic IGRT: Spinal Radiosurgery. Med Dosim. 2008 summer; 33(2):107-16. 29. Gerszten PC, Burton SA, Ozhasoglu C, McCue KJ, Quinn AE. Radiosurgery for benign intradural spinal tumors. Neurosurgery. 2008 Apr; 62(4):887-95; discussion 895-6. 30. Gerszten PC, Ozhasoglu C, Burton SA, Vogel WJ, Atkins BA, Kalnicki S, Welch WC. CyberKnife frameless stereotactic radiosurgery for spinal lesions: clinical experience in 125 cases. Neurosurgery. 2004 Jul; 55(1):89-98; discussion 98-9. 31. Gerszten PC, Ozhasoglu C, Burton SA, Vogel WJ, Atkins BA, Kalnicki S, Welch WC. CyberKnife frameless single-fraction stereotactic radiosurgery for benign tumors of the spine. Neurosurg Focus. 2003 May 15; 14(5):e16. 32. Gerszten PC, Burton SA, Welch WC, Brufsky AM, Lembersky BC, Ozhasoglu C, Vogel WJ. Single-fraction radiosurgery for the treatment of spinal breast metastases. Cancer. 2005a Nov 15; 104(10):2244-54. 33. Gerszten PC, Burton SA, Ozhasoglu C, Vogel WJ, Welch WC, Baar J, Friedland DM. Stereotactic radiosurgery for spinal metastases from renal cell carcinoma. J Neurosurg Spine. 2005b Oct; 3(4):288-95. 34. Gerszten PC, Burton SA, Quinn AE, Agarwala SS, Kirkwood JM Radiosurgery for the treatment of spinal melanoma metastases. Stereotact Funct Neurosurg. 2005c; 83(5-6):213-21.
ASTRO SRS Model Coverage Policy Page 11 Final Approval 1-14-11 Updated 7-25-11

35. Gerszten PC, Germanwala A, Burton SA, Welch WC, Ozhasoglu C, Vogel WJ. Combination kyphoplasty and spinal radiosurgery: a new treatment paradigm for pathological fractures. J Neurosurg Spine. 2005d Oct; 3(4):296-301. 36. Gerszten PC, Burton SA, Belani CP, Ramalingam S, Friedland DM, Ozhasoglu C, Quinn AE, McCue KJ, Welch WC. Radiosurgery for the treatment of spinal lung metastases. Cancer. 2006 Dec 1; 107(11):2653-61. 37. Gibbs IC, Kamnerdsupaphon P, Ryu MR, Dodd R, Kiernan M, Chang SD, Adler JR Jr. Image-guided robotic radiosurgery for spinal metastases. Radiother Oncol. 2007 Feb; 82(2):185-90. 38. Giller CA, Berger BD, Fink K, Bastian E. A volumetric study of CyberKnife hypofractionated stereotactic radiotherapy as salvage for progressive malignant brain tumors: initial experience. Neurol Res. 2007 Sep; 29(6):563-8. 39. Gopalan R, Dassoulas K, Rainey J, Sherman JH, Sheehan JP. Evaluation of the role of Gamma Knife surgery in the treatment of craniopharyngiomas. Neurosurg Focus. 2008; 24(5):E5. 40. Gottfried ON, Liu JK, Couldwell WT. Comparison of radiosurgery and conventional surgery for the treatment of glomus jugulare tumors. Neurosurg Focus. 2004 Aug 15; 17(2):E4. 41. Grabenbauer GG, Reinhold Ch, Kerling F, et al. Fractionated stereotactically guided radiotherapy of pharmacoresistant temporal lobe epilepsy. Acta Neurochir Suppl. 2002; 84: 65-70. 42. Gronseth G, Cruccu G, Alksne J, Argoff C, Brainin M, Burchiel K, Nurmikko T, Zakrzewska JM. Practice parameter: the diagnostic evaluation and treatment of trigeminal neuralgia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the European Federation of Neurological Societies. Neurology. 2008 Oct 7; 71(15):1183-90. 43. Han JH, Kim DG, Chung HT, et al. Clinical and neuroimaging outcome of cerebral arteriovenous malformations after Gamma Knife surgery: analysis of the radiation injury rate depending on the arteriovenous malformation volume. J Neurosurg. 2008; 109(2):191-198. 44. Hara W, Loo BW Jr, Goffinet DR, Chang SD, Adler JR, Pinto HA, et al. Excellent Local Control with Stereotactic Radiotherapy Boost After External Beam Radiotherapy in Patients with Nasopharyngeal Carcinoma. Int J Radiat Oncol Biol Phys. 2007 Dec 28. 45. Hayes, Inc. HAYES Medical Technology Directory. Stereotactic Radiosurgery for Arteriovenous Malformations and Intracranial Tumors. Lansdale, PA: Hayes, Inc. January 2009.
ASTRO SRS Model Coverage Policy Page 12 Final Approval 1-14-11 Updated 7-25-11

46. Ikeda H, Jokura H, Yoshimoto T. Transsphenoidal surgery and adjuvant Gamma Knife treatment for growth hormone-secreting pituitary adenoma. J Neurosurg. 2001 Aug; 95(2):285-91. 47. International RadioSurgery Association. Radiosurgery practice guideline initiative: stereotactic radiosurgery for patients with vestibular schwannomas. Issued May 2006. Accessed April 2009. Available at: http://www.irsa.org/AN%20Guideline.pdf. 48. International RadioSurgery Association. Radiosurgery practice guideline initiative: stereotactic radiosurgery for patients with intractable typical trigeminal neuralgia who have failed medical management. Issued: September 2003. Accessed April 2009. Available at: http://www.irsa.org/ TN%20Guideline.pdf. 49. International RadioSurgery Association. Radiosurgery practice guideline initiative: stereotactic radiosurgery for patients with pituitary adenomas. Issued: April 2004. Accessed April 2009. Available at: http://www.irsa.org /Pituitary%20 Guideline.pdf 50. International RadioSurgery Association, The. Radiosurgery practice guideline initiative: stereotactic radiosurgery for patients with intracranial arteriovenous malformations. Issued September 2003. Accessed April 2009. Available at: http://www.irsa.org/AVM%20Guideline.pdf 51. Ishihara H, Saito K, Nishizaki T, Kajiwara K, Nomura S, Yoshikawa K, Harada K, Suzuki M. CyberKnife radiosurgery for vestibular schwannoma. Minim Invasive Neurosurg. 2004 Oct; 47(5):290-3. 52. Kajiwara K, Saito K, Yoshikawa K, Kato S, Akimura T, Nomura S, Ishihara H, Suzuki M. Image-guided stereotactic radiosurgery with the CyberKnife for pituitary adenomas. Minim Invasive Neurosurg. 2005 Apr; 48(2):91-6. 53. Karpinos M, Teh BS, Zeck O, Carpenter LS, Phan C, Mai WY, Lu HH, Chiu JK, Butler EB, Gormley WB, Woo SY. Treatment of acoustic neuroma: stereotactic radiosurgery vs. microsurgery. Int J Radiat Oncol Biol Phys. 2002 Dec 1; 54(5):1410-21. Stereotactic radiotherapy. Front Radiat Ther Oncol. 2007; 40:415-26. 54. Kim SH, Weil RJ, Chao ST, Toms SA, Angelov L, Vogelbaum MA, Suh JH, Barnett GH. Stereotactic radiosurgical treatment of brain metastases in older patients. Cancer. 2008 Aug 15; 113(4):834-40. 55. Kondziolka D, Ong JG, Lee JY, Moore RY, Flickinger JC, Lunsford LD. Gamma Knife thalamotomy for essential tremor. J Neurosurg. 2008 Jan; 108(1):111-7. 56. Kondziolka D, Patel A, Lunsford LD, Kassam A, Flickinger JC. Stereotactic radiosurgery plus whole brain radiotherapy versus radiotherapy alone for patients with multiple brain metastases. Int J Radiat Oncol Biol Phys. 1999 Sep 1; 45(2):427-34.
ASTRO SRS Model Coverage Policy Page 13 Final Approval 1-14-11 Updated 7-25-11

57. Kong DS, Lee JI, Lim do H, Kim KW, Shin HJ, Nam DH, et al. The efficacy of fractionated radiotherapy and stereotactic radiosurgery for pituitary adenomas: long-term results of 125 consecutive patients treated in a single institution. Cancer. 2007 Aug 15; 110(4):854-60. 58. Lee M, Kalani MY, Cheshier S, Gibbs IC, Adler JR, Chang SD. Radiation therapy and CyberKnife radiosurgery in the management of craniopharyngiomas. Neurosurg Focus. 2008; 24(5):E4. 59. Lee JY, Kondziolka D, Flickinger JC, Lunsford LD. Radiosurgery for intracranial meningiomas. Prog Neurol Surg. 2007; 20:142-9. 60. Lim M, Bower R, Nangiana JS, Adler JR, Chang SD. Radiosurgery for glomus jugulare tumors. Technol Cancer Res Treat. 2007 Oct; 6(5):419-23. 61. Lim M, Cotrutz C, Romanelli P, Schaal D, Gibbs I, Chang SD, Adler JR. Stereotactic radiosurgery using CT cisternography and non-isocentric planning for the treatment of trigeminal neuralgia. Comput Aided Surg. 2006 Jan; 11(1):11-20. 62. Lim M, Villavicencio AT, Burneikiene S, Chang SD, Romanelli P, McNeely L,McIntyre M, Thramann JJ, Adler JR. CyberKnife radiosurgery for idiopathic trigeminal neuralgia. Neurosurg Focus. 2005 May 15; 18(5):E9. 63. Linskey ME, Davis SA, Ratanatharathorn V. Relative roles of microsurgery and stereotactic radiosurgery for the treatment of patients with cranial meningiomas: a single-surgeon 4-year integrated experience with both modalities. J Neurosurg. 2005 Jan; 102 Suppl: 59-70. 64. Lipani JD, Jackson PS, Soltys SG, Sato K, Adler JR. Survival Following CyberKnife Radiosurgery and Hypofractionated Radiotherapy for Newly Diagnosed Glioblastoma Multiforme. Technol Cancer Res Treat. 2008 Jun; 7(3):249-56. 65. Madsen BL, Hsi RA, Pham HT, Fowler JF, Esagui L, Corman J. Stereotactic hypofractionated accurate radiotherapy of the prostate (SHARP), 33.5 Gy in five fractions for localized disease: first clinical trial results. Int J Radiat Oncol Biol Phys. 2007 Mar 15; 67(4):1099-105. 66. Mathieu D, Kondziolka D, Niranjan A, Flickinger J, Lunsford LD. Gamma knife radiosurgery for refractory epilepsy caused by hypothalamic hamartomas. Stereotact Funct Neurosurg. 2006; 84(2-3):82-7. 67. McClelland S 3rd, Gerbi BJ, Higgins PD, Orner JB, Hall WA. Safety and efficacy of fractionated stereotactic radiotherapy for acoustic neuromas. J Neurooncol. 2008 Jan; 86(2):191-4. 68. Meijer OW, Vandertop WP, Baayen JC, Slotman BJ. Single-fraction vs. fractionated
ASTRO SRS Model Coverage Policy Page 14 Final Approval 1-14-11 Updated 7-25-11

linac-based stereotactic radiosurgery for vestibular schwannoma: a single-institution study. Int J Radiat Oncol Biol Phys. 2003 Aug 1; 56(5):1390-6. 69. Muacevic A, Wowra B, Siefert A, Tonn JC, Steiger HJ, Kreth FW. Microsurgery plus whole brain irradiation versus Gamma Knife surgery alone for treatment of single metastases to the brain: a randomized controlled multicentre phase III trial. J Neurooncol. 2008 May; 87(3):299-307. 70. Muragaki Y, Nakamura R, Iseki H, Hori T, Takakura K. Outcome after pituitary radiosurgery for thalamic pain syndrome. Int J Radiat Oncol Biol Phys. 2007 Nov 1; 69(3):852-7. 71. Myrseth E, MP, Pedersen PH, Vassbotn FS, Wentzel-Larsen T, Lund-Johansen M. Vestibular schwannomas: clinical results and quality of life after microsurgery or Gamma Knife radiosurgery. Neurosurgery. 2005 May; 56(5):927-35; discussion 927-35. 72. National Comprehensive Cancer Network (NCCN).Web site. Clinical Practice Guidelines in Oncology. Central Nervous System Cancers V.1.2008. Accessed April 2009. Available at http://www.nccn.org/professionals/physician_gls/PDF/cns.pdf.
73. National Comprehensive Cancer Network (NCCN).Web site. Clinical Practice Guidelines in Oncology. Soft Tissue Sarcoma. V.1.2009. Accessed April 2009. Available at: http://www.nccn.org/professionals/physician_gls/PDF/sarcoma.pdf. 74. National Institute for Clinical Excellence. Stereotactic radiosurgery for trigeminal neuralgia using the Gamma Knife. August 2004. 75. National Institute for Health and Clinical Excellence. Interventional procedure Guidance IPG085 Stereotactic radiosurgery for trigeminal neuralgia using the Gamma Knife - guidance. August 2004. Accessed April 2009. Available at: http://www.nice.org.uk/nicemedia/pdf/ip/IPG085guidance .pdf. 76. National Institute for Health and Clinical Excellence. Systematic review of the clinical efficacy and safety of stereotactic radiosurgery (Gamma Knife) in the treatment of trigeminal neuralgia. 27 April 2004. Accessed April 2009. Available at: http://www.nice.org.uk /nicemedia /pdf/ip/173 systematic review.pdf. 77. Niranjan A, Jawahar A, Kondziolka D, Lunsford LD. A comparison of surgical approaches for the management of tremor: radiofrequency thalamotomy, Gamma Knife thalamotomy and thalamic stimulation. Stereotact Funct Neurosurg. 1999; 72(2-4):178-84. 78. Nishizaki T, Saito K, Jimi Y, Harada N, Kajiwara K, Nomura S, Ishihara H, Yoshikawa K, Yoneda H, Suzuki M, Gibbs IC. The role of cyberknife radiosurgery/radiotherapy for brain metastases of multiple or large-size tumors. Minim Invasive Neurosurg. 2006 Aug; 49(4):203-9.
ASTRO SRS Model Coverage Policy Page 15 Final Approval 1-14-11 Updated 7-25-11

79. Ogilvy CS, Stieg PE, Awad I, Brown RD Jr, Kondziolka D, Special Writing Group of the Stroke Council, American Stroke Association, et al. AHA Scientific Statement: Recommendations for the management of intracranial arteriovenous malformations: a statement for healthcare professionals from a special writing group of the Stroke Council, American Stroke Association. Stroke. 2001 Jun; 32(6):1458-71. 80. Okun MS, Stover NP, Subramanian T, Gearing M, Wainer BH, Holder CA, Watts RL, Juncos JL, Freeman A, Evatt ML, Schuele SU, Vitek JL, DeLong MR. Complications of Gamma Knife surgery for Parkinson disease. Arch Neurol. 2001 Dec; 58(12):1995-2002. 81. Pan DH, Guo WY, Chung WY, et al. Gamma knife radiosurgery as a single treatment modality for large cerebral arteriovenous malformations. J Neurosurg. 2000; 93(suppl 3):113-119. 82. Patil CG, Veeravagu A, Bower RS, Li G, Chang SD, Lim M, Adler JR Jr. CyberKnife radiosurgical rhizotomy for the treatment of atypical trigeminal nerve pain. Neurosurg Focus. 2007; 23(6):E9. 83. Picozzi P, Losa M, Mortini P, Valle MA, Franzin A, Attuati L, Ferrari da Passano C, Giovanelli M. Radiosurgery and the prevention of regrowth of incompletely removed nonfunctioning pituitary adenomas. J Neurosurg. 2005 Jan; 102 Suppl: 71-4. 84. Pollock BE, Stafford SL, Utter A, Giannini C, Schreiner SA. Stereotactic radiosurgery provides equivalent tumor control to Simpson Grade 1 resection for patients with small- to medium-size meningiomas. Int J Radiat Oncol Biol Phys. 2003 Mar 15; 55(4):1000-5. 85. Pollock BE. Stereotactic radiosurgery in patients with glomus jugulare tumors. Neurosurg Focus. 2004 Aug 15; 17(2):E10. 86. Pollock, BE. An evidence-based medicine review of stereotactic radiosurgery. Prog Neurol Surg. 2006; 19152-170. 87. Pollock BE, Lunsford LD, Flickinger JC, Clyde BL, Kondziolka D. Vestibular schwannoma management. Part I. Failed microsurgery and the role of delayed stereotactic radiosurgery. J Neurosurg. 1998 Dec; 89(6):944-8. 88. Quigg M, Barbaro NM. Stereotactic radiosurgery for treatment of epilepsy. Arch Neurol. 2008 Feb; 65(2):177-83. 89. Rades D, Bohlen G, Pluemer A, Veninga T, Hanssens P, Dunst J, Schild SE. Stereotactic radiosurgery alone versus resection plus whole-brain radiotherapy for 1 or 2 brain metastases in recursive partitioning analysis class 1 and 2 patients. Cancer. 2007 Jun 15; 109(12):2515-21. 90. Regis J, Arkha Y, Yomo S, Bartolomei F, Peragut JC, Chauvel P. Radiosurgery for drug-resistant epilepsies: state of the art, results and perspectives. Neurochirurgie. 2008 May;
ASTRO SRS Model Coverage Policy Page 16 Final Approval 1-14-11 Updated 7-25-11
54(3):320-31. 91. Regis J, Bartolomei F, Rey M, et al. Gamma knife surgery for mesial temporal lobe epilepsy. J Neurosurg. 2000; 93(Suppl 3):141-146. 92. Regis J, Pellet W, Delsanti C, Dufour H, Roche PH, Thomassin JM, Zanaret M, Peragut JC. Functional outcome after Gamma Knife surgery or microsurgery for vestibular schwannomas. J Neurosurg. 2002 Nov; 97(5):1091-100. 93. Regis J, Rey M, Bartolomei F, Vladyka V, Liscak R, Schrottner O, Pendl G. Gamma knife surgery in mesial temporal lobe epilepsy: a prospective multicenter study. Epilepsia. 2004 May;45(5):504-15. 94. Regis J, Scavarda D, Tamura M, et al. Epilepsy related to hypothalamic hamartomas: Surgical management with special reference to Gamma Knife surgery. Childs Nerv Syst. 2006; 22(8):881-895. 95. Regis J, Bartolomei F, de Toffol B, Genton P, Kobayashi T, Mori Y, et al. Gamma knife surgery for epilepsy related to hypothalamic hamartomas. Neurosurgery. 2000 Dec; 47(6):1343-51; discussion 1351-2. 96. Regis J, Rey M, Bartolomei F, Vladyka V, Liscak R, Schrottner O, Pendl G. Gamma knife surgery in mesial temporal lobe epilepsy: a prospective multicenter study. Epilepsia. 2004 May; 45(5):504-15. 97. Roche PH, Robitail S, Delsanti C, Marouf R, Pellet W, RJ. Radiosurgery of vestibular schwannomas after microsurgery and combined radio-microsurgery Neurochirurgie. 2004 Jun; 50(2-3 Pt 2):394-400. 98. Romanelli P, Anschel DJ. Radiosurgery for epilepsy. Lancet Neurol. 2006 Jul; 5(7):613-20. 99. Romanelli P, Heit G, Chang SD, Martin D, Pham C, Adler J. Cyberknife radiosurgery for trigeminal neuralgia. Stereotact Funct Neurosurg. 2003; 81(1-4):105-9. 100. Ryu S, Jin R, Jin JY, Chen Q, Rock J, Anderson J, Movsas B. Pain control by image-guided radiosurgery for solitary spinal metastasis. J Pain Symptom Manage. 2008 Mar; 35(3):292-8. 101. Sahgal A, Chou D, Ames C, Ma L, Lamborn K, Huang K, Chuang C, Aiken A, Pett P, Weinstein P, Larson D .Image-guided robotic stereotactic body radiotherapy for benign spinal tumors: the University of California San Francisco preliminary experience. Technol Cancer Res Treat. 2007 Dec; 6(6):595-604. 102. Schaeuble B, Cascino GD, Pollock BE, Gorman DA, Weigand S, Cohen-Gadol AA, McClelland RL. Seizure outcomes after stereotactic radiosurgery for cerebral arteriovenous
ASTRO SRS Model Coverage Policy Page 17 Final Approval 1-14-11 Updated 7-25-11

malformations. Neurology. 2004 Aug 24; 63(4):683-7. 103. Selch MT, Gorgulho A, Mattozo C, Solberg TD, Cabatan-Awang C, DeSalles AA. Linear accelerator stereotactic radiosurgery for the treatment of gelastic seizures due to hypothalamic hamartoma. Minim Invasive Neurosurg. 2005 Oct; 48(5):310-4.
104. Serizawa, Toru; Hirai, Tatsuo; Nagano, Osamu; Higuchi, Yoshinori; Matsuda, Shinji; Ono, Junichi; Saeki, Naokatsu. Gamma knife surgery for 1–10 brain metastases without prophylactic whole-brain radiation therapy: analysis of cases meeting the Japanese prospective multi-institute study (JLGK0901) inclusion criteria. Journal of Neuro-Oncology (2010) 98: 163-167, June 10, 2010 105. Sinclair J, Chang SD, Gibbs IC, Adler JR Jr. Multisession CyberKnife radiosurgery for intramedullary spinal cord arteriovenous malformations. Neurosurgery. 2006 Jun; 58(6):1081-9; discussion 1081-9. 106. Souhami L, Seiferheld W, Brachman D, Podgorsak EB, Werner-Wasik M, Lustig R, Schultz CJ, Sause W, Okunieff P, Buckner J, Zamorano L, Mehta MP, Curran WJ Jr. Randomized comparison of stereotactic radiosurgery followed by conventional radiotherapy with carmustine to conventional radiotherapy with carmustine for patients with glioblastoma multiforme: report of Radiation Therapy Oncology Group 93-05 protocol. Int J Radiat Oncol Biol Phys. 2004 Nov 1; 60(3):853-60. 107. Steinvorth S, Wenz F, Wildermuth S, et al. Cognitive function in patients with cerebral arteriovenous malformations after radiosurgery: prospective long-term follow-up. Int J Radiat Oncol Biol Phys. 2002; 54(5):1430-7. 108. Tsao MN, Lloyd N, Wong R, Chow E, Rakovitch E, Laperriere N. Whole brain radiotherapy for the treatment of multiple brain metastases. Cochrane Database of Systematic Reviews 2006, Issue 3. Art. No.: CD003869. 109. Tsao MN, Mehta MP, Whelan TJ, Morris DE, Hayman JA, Flickinger JC, Mills M, Rogers CL, Souhami L. The American Society for Therapeutic Radiology and Oncology (ASTRO) evidence-based review of the role of radiosurgery for malignant glioma. Int J Radiat Oncol Biol Phys. 2005 Sep 1; 63(1):47-55. 110. Villavicencio AT, Lim M, Burneikiene S, Romanelli P, Adler JR, McNeely L, Chang SD, Fariselli L, McIntyre M, Bower R, Broggi G, Thramann JJ. Cyberknife radiosurgery for trigeminal neuralgia treatment: a preliminary multicenter experience. Neurosurgery. 2008 Mar; 62(3):647-55; discussion 647-55. 111. Whang CJ, Kwon Y. Long-term follow-up of stereotactic Gamma Knife radiosurgery in epilepsy. Stereotact Funct Neurosurg. 1996; 66(Suppl 1):349-356. 112. Weil M. Stereotactic Radiosurgery for Brain Tumors. Hematology/Oncology Clinics of North America. 2001; 15(6).
ASTRO SRS Model Coverage Policy Page 18 Final Approval 1-14-11 Updated 7-25-11

113. Wu SX, Chua DT, Deng ML, Zhao C, Li FY, Sham JS, Wang HY, Bao Y, Gao YH, Zeng ZF. Outcome of fractionated stereotactic radiotherapy for 90 patients with locally persistent and recurrent nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2007 Nov 1; 69(3):761-9. 114. Yang KJ, Wang KW, Wu HP, Qi ST. Radiosurgical treatment of intractable epilepsy with low radiation dose. Di Yi Jun Yi Da Xue Xue Bao. 2002; 22(7):645-647. 115. Yoshikawa K, Saito K, Kajiwara K, Nomura S, Ishihara H, Suzuki M. CyberKnife stereotactic radiotherapy for patients with malignant glioma. Minim Invasive Neurosurg. 2006 Apr; 49(2):110-5. 116. Young RF, Jacques S, Mark R, Kopyov O, Copcutt B, Posewitz A, Li F. Gamma knife thalamotomy for treatment of tremor: long-term results. J Neurosurg. 2000 Dec; 93 Suppl 3:128-35. 117. Young RF, Vermeulen S, Posewitz A, Shumway-Cook A. Pallidotomy with the Gamma Knife: a positive experience. Stereotact Funct Neurosurg. 1998 Oct; 70 Suppl 1:218-28. 118. Young RF, Vermeulen SS, Grimm P, Posewitz AE, Jacques DB, Rand RW, Copcutt BG. Gamma Knife thalamotomy for the treatment of persistent pain. Stereotact Funct Neurosurg. 1995; 64 Suppl 1:172-81. 119. Zesiewicz TA, Elble R, Louis ED, Hauser RA, Sullivan KL, Quality Standards Subcommittee of the American Academy of Neurology, et al. Practice parameter: therapies for essential tremor: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2005 Jun 28; 64(12):2008-20.
ASTRO SRS Model Coverage Policy Page 19 Final Approval 1-14-11 Updated 7-25-11
STEREOTACTIC BODY RADIATION THERAPY (SBRT)
Model Policies
This Model Policy1 addresses coverage for Stereotactic Body Radiation Therapy (SBRT).
Description
SBRT is a treatment that couples a high degree of anatomic targeting accuracy and reproducibility with very high doses of extremely precise, externally generated, ionizing radiation, thereby maximizing the cell-killing eff ect on the target(s) while minimizing radiation-related injury in adjacent normal tissues. SBRT is used to treat extra-cranial sites as opposed to stereotactic radiosurgery (SRS) which is used to treat intra-cranial and spinal targets. However, some of the CPT® codes discussed here are also utilized in the billing process for SRS and are discussed accordingly in the SRS model policy.
The adjective “stereotactic” describes a procedure during which a target lesion is localized relative to a known three- dimensional reference system that allows for a high degree of anatomic accuracy and precision. Examples of devices used in SBRT for stereotactic guidance may include a body frame with external reference markers in which a patient is positioned securely, a system of implanted fi ducial markers that can be visualized with low-energy (kV)X-rays and CT-imaging-based systems used to confi rm the location of a tumor immediately prior to treatment.
Treatment of extra-cranial sites requires accounting for internal organ motion as well as for patient motion. Thus, reliable immobilization or repositioning systems must often be combined with devices capable of decreasing organ motion or accounting for organ motion e.g. respiratory gating. Additionally, all SBRT is performed with at least one form of image guidance to confi rm proper patient positioning and tumor localization prior to delivery of each fraction. The ASTRO/ACR Practice Guidelines for SBRT outline the responsibilities and training requirements for personnel involved in the administration of SBRT.
SBRT may be delivered in one to fi ve sessions (fractions). Each fraction requires an identical degree of precision, localization and image guidance. Since the goal of SBRT is to maximize the potency of the radiotherapy by completing an entire course of treatment within an extremely accelerated time frame, any course of radiation treatment extending beyond fi ve fractions is not considered SBRT and is not to be billed using these codes. SBRT is meant to represent a complete course of treatment and not be used as a boost following a conventionally fractionated course of treatment.
1 ASTRO model policies were developed as a means to effi ciently communicate what ASTRO believes to be correct coverage policies for radiation oncology services. The ASTRO model policies do not serve as clinical guidelines and they are subject to periodic review and revision without notice. The ASTRO Model Policies may be reproduced and distributed, without modifi cation, for noncommercial purposes.
Approved 8-2-10Updated 4-17-13
CPT copyright 2012 American Medical Association. All rights reserved.
Page 2STEREOTACTIC BODY RADIATION THERAPY (SBRT) MODEL POLICY
Indications and Limitations of Coverage and/or Medical Necessity
This Model Policy addresses only the CPT® codes for SBRT treatment management - 77435, and SBRT treatment delivery -77373, G0251, G0339 and G0340.
When billing for SBRT delivery, it is not appropriate to bill more than one treatment delivery code on the same day of service, even though some types of delivery may have elements of several modalities (for example, a stereotactic approach with intensity-modulated static beams or arcs). Also, only one delivery code is to be billed even if multiple lesions are treated on the same day.
Indications for SBRT:
SBRT is indicated for primary tumors of and tumors metastatic to the lung, liver, kidney, adrenal gland or pancreas as well as for pelvic and head and neck tumors that have recurred after primary irradiation when and only when each of the following criteria are met, and each specifi cally documented in the medical record. Multiple ICD diagnosis codes(ICD-9 or ICD-10) fi t this description and are listed in this coverage policy.
1. The patient’s general medical condition (notably, the performance status) justifi es aggressive treatment to a primary cancer or, for the case of metastatic disease, justifi es aggressive local therapy to one or
more discrete deposits of cancer within the context of eff orts to achieve total clearance or clinically benefi cial reduction in the patient’s overall burden of systemic disease.
2. The tumor burden can be completely targeted with acceptable risk to critical normal structures. Other Neoplasms
Prostate Cancer:
Many clinical studies supporting the effi cacy and safety of SBRT in the treatment of prostate cancer have been published. At least one study has shown excellent fi ve year biochemical control rates with very low rates of serious toxicity. Additionally, numerous studies have demonstrated the safety of SBRT for prostate cancer after a follow-up interval long enough (two to three years) to provide an opportunity to observe the incidence of late GU or GI toxicity. While it is necessary to observe patients treated for prostate cancer for extended intervals to gauge the rate of long term (beyond 10 years) biochemical control and overall survival, the interim results reported appear at least as good as other forms of radiotherapy administered to patients with equivalent risk levels followed for the same duration post-treatment.
It is ASTRO’s opinion that data supporting the use of SBRT for prostate cancer have matured to a point where SBRT could be considered an appropriate alternative for select patients with low to intermediate risk disease.
Bone Metastases:
SBRT has been demonstrated to achieve durable tumor control when treating lesions in vertebral bodies or the paraspinous region, where extra care must be taken to avoid excess irradiation of the spinal cord when tumor-ablative doses are administered. There is an important clinical distinction between the status of patients described above and a patient with widely metastatic disease for whom palliation is the major objective. In one setting, a patient with limited metastatic disease and good performance status is treated with the intention of eradicating all known active disease or greatly reducing the total disease burden in a manner that can extend progression-free survival. For such a patient, SBRT can be a reasonable therapeutic intervention. However, for uncomplicated, previously untreated bone metastases in a patient with widespread progressive disease in the spine or elsewhere, where the prognosis is unfavorable, it is generally appropriate to use a less technically complex form of palliative radiotherapy rather than SBRT.
CPT copyright 2012 American Medical Association. All rights reserved.
Page 3
Other Indications for SBRT:
For patients with tumors of any type arising in or near previously irradiated regions, SBRT may be appropriate when a high level of precision and accuracy is needed to minimize the risk of injury to surrounding normal tissues. Also, in other cases where a high dose per fraction treatment is indicated SBRT may be appropriate. The necessity should be documented in the medical record.
Limitations:
SBRT is not considered medically necessary under the following circumstances:
1. Treatment unlikely to result in clinical cancer control and/or functional improvement. 2. The tumor burden cannot be completely targeted with acceptable risk to critical normal structures. 3. Patients with poor performance status (Karnofsky Performance Status less than 40 or Eastern Cooperative Oncology Group (ECOG) Status of 3 or worse) - see Karnofsky Performance Status and ECOG Status below.
Karnofsky Performance Status Scale
100 Normal; no complaints, no evidence of disease90 Able to carry on normal activity; minor signs or symptoms of disease
80 Normal activity with eff ort; some signs or symptoms of disease70 Cares for self; unable to carry on normal activity or to do active work60 Requires occasional assistance but is able to care for most needs50 Requires considerable assistance and frequent medical care40 Disabled; requires special care and assistance30 Severely disabled; hospitalization is indicated although death not imminent20 Very sick; hospitalization necessary; active supportive treatment is necessary10 Moribund, fatal processes progressing rapidly0 Dead
Karnofsky DA, Burchenal JH. (1949). “The Clinical Evaluation of Chemotherapeutic Agents in Cancer.” In: MacLeod CM (Ed), Evaluation of Chemotherapeutic Agents. Columbia Univ Press. Page 196.
STEREOTACTIC BODY RADIATION THERAPY (SBRT) MODEL POLICY

Page 4
Grade 0: Fully active, able to carry on all pre-disease performance without restriction.Grade 1: Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary
nature, e.g. light house work, offi ce work.Grade 2: Ambulatory and capable of all self-care but unable to carry out and work activities. Up and about more
than 50% of waking hours.Grade 3: Capable of only limited self-care, confi ned to bed or chair more than 50% of waking hours.
Grade 4: Completely disabled. Cannot carry on any self-care. Totally confi ned to bed or chair.Grade 5: Dead
Eastern Cooperative Oncology Group, Robert Comis MD, Group Chair.
* As published in Am. J. Clin. Oncol.:Oken, M.M., Creech, R.H., Tormey, D.C., Horton, J., Davis, T.E., McFadden, E.T., Carbone, P.P.: Toxicity And Response Criteria Of The Eastern Cooperative Oncology Group. Am J Clin Oncol 5:649-655, 1982.
PHYSICIANS’ CURRENT PROCEDURAL TERMINOLOGY (CPT®)/HCPCS SECTION
[(Note – CPT is a trademark of the American Medical Association (AMA)]
77435 Stereotactic body radiation therapy, treatment management, per treatment course, to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions (The same physician should not report both the stereotactic radiosurgery services [32701, 63620, 63621] and radiation treatment management [77435])
77373 Stereotactic body radiation therapy, treatment delivery, per fraction to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions (For single fraction cranial lesions, see 77371, 77372)
G0339 Image-guided robotic linear accelerator-based stereotactic radiosurgery, complete course of therapy in one session, or fi rst session of fractionated treatment
CPT copyright 2012 American Medical Association. All rights reserved.
STEREOTACTIC BODY RADIATION THERAPY (SBRT) MODEL POLICY
This code should not be reported in conjunction with any other treatment delivery codes e.g. 77401-77416, 77418. This code will be paid only once per day of treatment regardless
of the number of sessions or lesions.
This code includes all image guidance on the days of treatment delivery, so do not report G0339 in conjunction with 77421 or 77014 on the days of treatment delivery. This code will be paid only once per day of treatment regardless of the number of sessions or lesions.
This code will be paid only once per course of treatment and should not be reported in conjunction with any other treatment management codes (77427-77432).
CPT/HCPCS Codes:
ECOG Performance Status Scale

G0340 Image-guided robotic linear accelerator-based stereotactic radiosurgery, delivery including collimator changes and custom plugging, fractionated treatment, all lesions, per session, second through fi fth sessions, maximum fi ve sessions per course of treatment
G0251 Linear accelerator based stereotactic radiosurgery, delivery including collimator changes and custom plugging, fractionated treatment, all lesions, per session, maximum fi ve sessions per course of treatment
For reporting fractions 2 through 5 after reporting G0339 for the fi rst fraction. This code includes all image guidance on the days of treatment delivery, so do not report G0340 in conjunction with 77421 or 77014 on the days of treatment delivery. This code will be paid only once per day of treatment regardless of the number of sessions or lesions.
This code should be utilized only by hospital outpatient departments to report non-robotic Linac based treatments for fractions two through fi ve. This code is excluded from MPFS by regulation.
Page 5STEREOTACTIC BODY RADIATION THERAPY (SBRT) MODEL POLICY
ICD Diagnosis Codes that Support Medical NecessityNote: Diagnosis codes are based on the current ICD-9-CM codes that are eff ective at the time of Model Policy publication. Any updates to ICD-9-CM or ICD-10-CM codes will be reviewed by ASTRO, and coverage should not be presumed until the results of such review have been published/posted. These ICD diagnosis codes support medical necessity under this Model Policy:
Diagnosis ICD-9 Code(s) ICD-10 Code(s) Comment
Primary lung cancer 162.2 – 162.9 C34.00 – C34.92Thoracic lymph nodes 196.1 C77.1Lung metastasis 197.0 C78.00 – C78.02Primary liver or bile duct cancer
155.0, 155.1, 155.2 C22.0 – C22.9
Liver metastasis 197.7 C78.7Primary Pancreas cancer 157.0 – 157.9 C25.0 – C25.9Kidney cancer or metastasis
189.0, 189.1, 198.0
C64.1 – C65.9,C79.00 – C79.02
Adrenal Gland primary or metastasis
194.0, 194.6, 198.7
C74.00 – C74.92,C75.5, C79.70 – C79.72
Prostate cancer 185 C61Pelvic cancer Abdomen and Pelvis Gynecological Rectum and Anus Eff ects of Radiation
195.2, 195.3 179 – 184.9 154.0 – 154.8 990*
C76.2, C76.3 C51.0 – C58 C19 – C21.8 T66.XXXA*
recurrent after prior conventionally fractionated RT
Head & Neck cancer, multiple primary sites
140.0 – 146.8, 990*
C00.0 – C10.8,T66.XXXA*
recurrent after prior conventionally fractionated RT
Nodal metastasis 196.0 – 196.9 C77.0 – C77.9 recurrent after prior conventionally fractionated RT
*ICD-9-CM 990 or ICD-10-CM T66.XXXA (Eff ects of Radiation, Unspecifi ed) may only be used where prior radiation therapy to the site is the governing factor necessitating SBRT in lieu of other radiotherapy. An ICD diagnosis code for the anatomic diagnosis must also be used.
CPT copyright 2012 American Medical Association. All rights reserved.
The CPT® codes discussed in this Model Policy are applicable to all diagnoses listed in the ASTRO SRS Model Policy, a companion document to the SBRT model policy.

Page 6STEREOTACTIC BODY RADIATION THERAPY (SBRT) MODEL POLICY
General Information
Documentation Requirements
The patient’s record must support the necessity and frequency of treatment. Medical records should include not only the standard history and physical but also the patient’s functional status and a description of current performance status (Karnofsky Performance Status or ECOG Performance Status). See Karnofsky Performance Status or ECOG Performance Status listed under Limitations above. A radiation oncologist must evaluate the clinical and technical aspects of the treatment, and document this evaluation as well as the resulting management decisions. Documentation of the technical aspects of treatment planning and delivery should include details of target dose and relevant dose-limiting normal structures. Documentation should include the date and the current treatment dose. All documentation must be available upon request of the insurer. For Medicare claims, the HCPCS/CPT® code(s) may be subject to Correct Coding Initiative (CCI) edits. This policy does not take precedence over CCI edits. Please refer to the CCI for correct coding guidelines and specifi c applicable code combinations prior to billing Medicare.
CPT copyright 2012 American Medical Association. All rights reserved.
Page 7
General
1. Benedict SH, Yenice KM, Followill D, et al. Stereotactic body radiation therapy: The report of AAPM Task Group 101. Med Phys. 2010; 37(8): 4078-4101.
2. Chang R, Timmerman R. Stereotactic Body Radiation Therapy : A Comprehensive Review. Am J Clin Oncol. 2007; 30(6): 637-644.
3. Corbin KS, Hellman S, Weichselbaum RR. Extracranial oligometastases: a subset of metastases curable with stereotactic radiotherapy. J Clin Oncol. 2013; 31(11):1384-1390.
4. Halperin EC, Perez, CA, Brady LW. Principles and Practice of Radiation Therapy, 5th edition. Philadelphia, PA: Lippincott Williams & Wilkins; 2008.
5. Kavanagh BD and Timmerman RD (Eds.) Stereotactic Body Radiation Therapy, Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
6. Lo S, Fakiris A, Chang E, et al. Stereotactic body radiation therapy: a novel treatment modality. Nat Rev Clin Oncol. 2010; 7(1): 44-54.
7. Martin A, Gaya A, Stereotactic Body Radiotherapy: A Review. Clin Oncol (R Coll Radiol). 2010; 22(3): 157-172.
8. Milano MT, Katz A, Muhs, AG et al. A prospective pilot study of curative-intent stereotactic body radiation therapy in patients with 5 or fewer oligometastatic lesions. Cancer. 2008; 112(3): 650-658.
9. Potters L, Kavanagh B, Galvin JM, et al. American Society for Therapeutic Radiology and Oncology (ASTRO) and American College of Radiology (ACR) practice guideline for the performance of stereotactic body radiation therapy. Int J Radiat Oncol Biol Phys. 2010; 76(2): 326-332.
10. Timmerman RD, Kavanagh BD, Cho LC, et al. Stereotactic Body Radiation Therapy in Multiple Organ Sites. J Clin Oncol. 2007; 25(8): 947-952.
Bone Metastasis
11. Chang EL, Shiu AS, Lii MF, et al. Phase I clinical evaluation of near- simultaneous computed tomographic image-guided stereotactic body radiotherapy for spinal metastases. Int J Radiat Oncol Biol Phys. 2004; 5 9(5): 1288-1294.
12. Chang EL, Shiu AS, Mendel E, et al. Phase I/II study of stereotactic body radiotherapy for spinal metastasis and its pattern of failure. J Neurosurg Spine. 2007; 7(2): 151-160.
13. Choi CY, Adler JR, Gibbs IC, et al. Stereotactic Radiosurgery for Treatment of Spinal Metastases Recurring in Close Proximity to Previously Irradiated Spinal Cord. Int J Radiat Oncol Biol Phys. 2010; 78(2): 499-506.
14. Gagnon GJ, Nasr NM, Liao JJ, et al. Treatment of spinal tumors using CyberKnife fractionated stereotactic radiosurgery: pain and quality of life assessment after treatment in 200 patients. Neurosurgery. 2009; 64(2): 297–306.
15. Haley M, Gerszten P. Stereotactic Radiosurgery in the Management of Cancer Pain. Curr Pain Headache Rep. 2009; 13(4): 277–281.
16. Janjan N, Lutz S, Bedwinek J, et al. Therapeutic Guidelines for the Treatment of Bone Metastasis: A Report from the American College of Radiology Appropriateness Criteria Expert Panel on Radiation Oncology. J Palliat Med. 2009; 12(5): 417-426.
17. Nelson JW, Yoo DS, Sampson JH, et al. Stereotactic body radiotherapy for lesions of the spine and paraspinal regions. Int J Radiat Oncol Biol Phys. 2009; 73(5): 1369–1375.
18. Papatheofanis F, Williams E, Chang S. Cost-utility analysis of the cyberknife system For metastatic spinal tumors. Neurosurgery. 2009; 64(2 Suppl): A73-A82.
19. Parikh S, Heron D. Fractionated radiosurgical management of intramedullary spinal cord metastasis: A case report and review of the literature. Clin Neurol Neurosurg. 2009; 111(10): 858-861.
20. Sahgal A, Ames C, Chou D, et al. Stereotactic Body Radiotherapy Is Eff ective Salvage Therapy for Patients with Prior Radiation of Spinal Metastases. Int J Radiat Oncol Biol Phys. 2008; 71: 652–665.
Breast
21. Milano MT, Zhang H, Metcalfe SK, et al. Oligometastatic breast cancer treated with curative-intent stereotactic body radiation therapy. Breast Cancer Res Treat. 2009; 115(3): 601-608.
Head and Neck
22. Chen HH, Tsai ST, Wang MS, et al. Experience in fractionated stereotactic body radiation therapy boost for newly diagnosed nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2006; 66(5): 1408-1414.
23. Kawaguchi K, Sato K, Horie A, et al. Stereotactic radiosurgery may contribute to overall survival for patients with recurrent head and neck carcinoma. Radiat Oncol. 2010; 5:51.
24. Rwiegema J, Heron D, Ferris R, et al. Fraactionated stereotactic body radiation therapy in the treatment of previously-irradiated recurrent head and neck carcinoma. Updated report of the University of Pittsburgh experience. Am J Clin Oncol. 2009; 33(3): 286-293.
25. Unger KR, Lominska CE, Deeken JF, et al. Fractionated Stereotactic Radiosurgery for Reirradiation of Head-and-Neck Cancer. Int J Radiat Oncol Biol Phys. 2010; 77(5): 1411-1419.
Kidney
26. Svedman C, Karlsson K, Rutkowska E, et al. Stereotactic body radiotherapy of primary and metastatic renal lesions for patients with only one functioning kidney. Acta Oncol. 2008; 47(8): 1578-1583.
Liver
27. Choi BO, Choi IB, Jang HS, et al. Stereotactic body radiation therapy with or without transarterial chemoembolization for patients with primary hepatocellular carcinoma: preliminary analysis. BMC Cancer. 2008; 8: 351.
28. Katz AW, Carey-Sampson M, Muhs AG, et al. Hypofractionated stereotactic body radiation therapy (SBRT) for limited hepatic metastases. Int J Radiat Oncol Biol Phys. 2007; 67(3): 793-798.
29. Kavanagh BD, Schefter TE, Cardenes HR, et al. Interim analysis of a prospective phase I/II trial of SBRT for liver metastases. Acta Oncol. 2006; 45(7): 848-855.
References
STEREOTACTIC BODY RADIATION THERAPY (SBRT) MODEL POLICY

Page 8
30. Lee MT, Kim JJ, Dinniwell R, et al. Phase I study of individualized stereotactic body radiotherapy for liver metastases. J Clin Oncol. 2009; 27: 1585–1591.
31. McCammon R, Schefter TE, Gaspar LE, et al. Observation of a dose-control relationship for lung and liver tumors after stereotactic body radiation therapy. Int J Radiat Oncol Biol Phys. 2009; 73(1): 112-118.
32. Méndez Romero A, Wunderink W, Hussain SM, et al. Stereotactic body radiation therapy for primary and metastatic liver tumors: A single institution phase i-ii study. Acta Oncol. 2006; 45(7): 831-837.
33. Méndez Romero A, Wunderink W, van Os RM, et al. Quality of life after stereotactic body radiation therapy for primary and metastatic liver tumors. Int J Radiat Oncol Biol Phys. 2008; 70(5): 1447-1452.
34. Rusthoven KE, Kavanagh BD, Cardenes H, et al. Multi-institutional phase I/II trial of stereotactic body radiation therapy for liver metastases. J Clin Oncol. 2009; 27: 1579–1584.
35. Rusthoven KE, Kavanagh BD, Cardenes H, et al. Multi-institutional phase I/ II trial of stereotactic body radiation therapy for liver metastases. J Clin Oncol. 2009; 27(10): 1572-1578.
36. Schefter TE, Kavanagh BD, Timmerman RD, Cardenes HR, Baron A, Gaspar LE. A phase I trial of stereotactic body radiation therapy (SBRT) for liver metastases. Int J Radiat Oncol Biol Phys. 2005; 62(5): 1371-1378.
37. Tse RV, Hawkins M, Lockwood G, Kim JJ, Cummings B, Knox J, Sherman M, Dawson LA. Phase I study of individualized stereotactic body radiotherapy for hepatocellular carcinoma and intrahepatic cholangiocarcinoma. J Clin Oncol. 2008; 26(4):657-664.
Lung
38. Collins BT, Vahdat S, Erickson K, et al. Radical cyberknife radiosurgery with tumor tracking: an eff ective treatment for inoperable small peripheral stage I non-small cell lung cancer. J Hematol Oncol. 2009; 2: 1.
39. Banki F, Luketich JD, Chen H, et al. Stereotactic radiosurgery for lung cancer. Minerva Chir. 2009; 64(6): 589-598.
40. Baumann P, Nyman J, Hoyer M, et al. Outcome in a prospective phase II trial of medically inoperable stage I non-small-cell lung cancer patients treated with stereotactic body radiotherapy. J Clin Oncol. 2009; 27(20): 3290–3296.
41. Baumann P, Nyman J, Hoyer M, et al. Stereotactic body radiotherapy for medically inoperable patients with stage I non-small cell lung cancer - a fi rst report of toxicity related to COPD/CVD in a non-randomized prospective phase II study. Radiother Oncol. 2008; 88(3): 359-367.
42. Baumann P, Nyman J, Lax I, et al. Factors important for effi cacy of stereotactic body radiotherapy of medically inoperable stage I lung cancer. A retrospective analysis of patients treated in the Nordic countries. Acta Oncol. 2006; 45(7): 787-795.
43. Chang JY, Balter PA, Dong L, et al. Stereotactic body radiation therapy in centrally and superiorly located stage I or isolated recurrent non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2008; 72(4): 967–971.
44. Chang JY, Balter PA, Dong L, et al. Stereotactic body radiation therapy in centrally and superiorly located stage I or isolated recurrent non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2008; 72(4): 967-971.
45. Chen Y, Guo W, Lu Y,et al. . Dose-individualized stereotactic body radiotherapy for T1-3N0 non-small cell lung cancer: long-term results and effi cacy of adjuvant chemotherapy. Radiother Oncol. 2008; 88(3): 351-358.
46. Coons D, Gokale A, Burton A, et al. Fractionated stereotactic body radiation therapy in the treatment of primary, recurrent, and metastatic lung tumors: the role of positron emission tomography/computed tomography-based treatment planning. Clin Lung Cancer. 2008; 9(4): 217-221.
47. Fakiris, AJ, McGarry RC, Yiannoutsos CT, et al. Stereotactic body radiation therapy for early-stage non-small-cell lung carcinoma: four-year results of a prospective phase II study. Int J Radiat Oncol Biol Phys. 2009; 75(3): 677–682.
48. Fritz P, Kraus HJ, Blaschke T, et al. Stereotactic, high single-dose irradiation of stage I non-small cell lung cancer (NSCLC) using four- dimensional CT scans for treatment planning. Lung Cancer. 2008; 60(2): 193-199.
49. Guckenberger M, Wulf J, Mueller G, et al. Response Relationship for Image-Guided Stereotactic Body Radiotherapy of Pulmonary Tumors: Relevance of 4d Dose Calculation. Int J Radiat Oncol Biol Phys. 2009; 73(2): 442-448.
50. Henderson M, McGarry R, Yiannoutsos C, et al. Baseline pulmonary function as a predictor for survival and decline in pulmonary function over time in patients undergoing stereotactic body radiotherapy for the treatment of stage I non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2008; 72(2): 404-409.
51. Hiraoka M, Matsuo Y, Nagata Y. Stereotactic body radiation therapy (SBRT) for early-stage lung cancer. Cancer Radiother. 2007; 11(1-2): 32-35.
52. Joyner M, Salter BJ, Papanikolaou N, et al. Stereotactic body radiation therapy for centrally located lung lesions. Acta Oncol. 2006; 45(7): 802- 807.
53. Koto M, Takai Y, Ogawa Y, et al. A phase II study on stereotactic body radiotherapy for stage I non-small cell lung cancer. Radiother Oncol. 2007; 85(3): 429-434.
54. McCammon R, Schefter TE, Gaspar LE, et al. Observation of a dose-control relationship for lung and liver tumors after stereotactic body radiation therapy. Int J Radiat Oncol Biol Phys. 2009; 73(1): 112- 118.
55. McGarry RC, Papiez L, Williams M, et al. Stereotactic body radiation therapy of early-stage non-small-cell lung carcinoma: phase I study. Int J Radiat Oncol Biol Phys. 2005; 63(4): 1010-1015.
56. Norihisa Y, Nagata Y, Takayama K, et al. Stereotactic body radiotherapy for oligometastatic lung tumors. Int J Radiat Oncol Biol Phys. 2008; 72(2): 398-403.
57. Okunieff P, Petersen AL, Philip A, et al. Stereotactic Body Radiation Therapy (SBRT) for lung metastases. Acta Oncol. 2006; 45(7): 808-817.
58. Pennathur A, Luketick J, Heron D, et. al. Stereotactic radiosurgery for the treatment of lung neoplasm: experience in 100 consecutive patients. Ann Thorac Surg. 2009; 88: 1594-1600.
59. Rusthoven KE, Kavanagh BD, Burri SH, et al. Multi-institutional phase I/II trial of stereotactic body radiation therapy for lung metastases. J Clin Oncol. 2009; 27(10): 1579-1584.
60. Salazar OM, Sandhu TS, Lattin PB, et al. Once-weekly, high-dose stereotactic body radiotherapy for lung cancer: 6-year analysis of 60 early-stage, 42 locally advanced, and 7 metastatic lung cancers. Int J Radiat Oncol Biol Phys. 2008; 72(3): 707-715.
61. Schefter TE, Kavanagh BD, Raben D, et al. A Phase I/II trial of Stereotactic Body Radiation Therapy (SBRT) for Lung Metastases: Initial report of dose escalation and early toxicity. Int J Radiat Oncol Biol Phys. 2006; 66(4 Suppl): S120-S127.
STEREOTACTIC BODY RADIATION THERAPY (SBRT) MODEL POLICY
Page 9
62. Scorsetti M, Navarria P, Facoetti A, et al. Eff ectiveness of stereotactic body radiotherapy in the treatment of inoperable early-stage lung cancer. Anticancer Res. 2007; 27(5B): 3615-3619.
63. Senan S, Lagerwaard F. Stereotactic radiotherapy for stage I lung cancer: Current results and new developments. Cancer Radiother. 2010; 14(2): 115-118.
64. Sonke JJ, Rossi M, Wolthaus J,. et al. Frameless stereotactic body radiotherapy for lung cancer using four dimensional cone beam CT guidance. Int J Radiat Oncol Biol Phys. 2009; 74(2): 567–574.
65. Takeda A, Sanuki N, Kunieda E, et al. Stereotactic Body Radiotherapy for Primary Lung Cancer at a Dose of 50 Gy Total in Five Fractions to the Periphery of the Planning Target Volume Calculated Using a Superposition Algorithm. Int J Radiat Oncol Biol Phys. 2009; 73(2): 442-448.
66. van der Voort van Zyp NC, Prevost J-B, Hoogeman MS, et al. Stereotactic radiotherapy with real-time tumor tracking for non-small cell lung cancer: clinical outcome. Radiother Oncol. 2009; 91(3): 296–300.
67. van der Voort van Zyp NC, van der Holt B, van Klaveren RJ, et al. Stereotactic body radiotherapy using real-time tumor tracking in octogenarians with non-small cell lung cancer. Lung Cancer. 2010; 69(3): 296-301.
68. Zimmermann F, Wulf J, Lax I, et al. Stereotactic Body Radiation Therapy for Early Non-Small Cell Lung Cancer. Front Radiat Ther Oncol. 2010; 42: 94-114.
Pancreas
69 . Chang DT, Schellenberg D, Shen J, et al. Stereotactic radiotherapy for unresectable adenocarcinoma of the pancreas. Cancer. 2009; 115(3): 665-672.
70. Mahadevan A, Jain S, Goldstein M, et al. Stereotactic Body Radiotherapy and Gemcitabine for Locally Advanced Pancreatic Cancer. Int J Radiat Oncol Biol Phys. 2010; 78(3): 735-742.
71. Rwigema J, Parihk S, Heron D, et al. Stereotactic body radiotherapy in the treatment of advanced adenocarcinoma of the pancreas. Am J Clin Oncol. 2011; 34(1): 63-69.
72. Schellenberg D, Goodman KA, Lee F, et al. Gemcitabine chemotherapy and single-fraction stereotactic body radiotherapy for locally advanced pancreatic cancer. Int J Radiat Oncol Biol Phys. 2008; 72: 678–686.
73. Schellenberg D, Quon A, Yuriko Minn A et al. 18 Fluorodeoxyglucose PET is prognostic of progression-free and overall survival in locally advanced pancreas cancer treated with stereotactic radiotherapy. Int J Radiat Oncol Biol Phys. 2010; 77(5): 1420- 1425.
Pelvic
74. Choi C, Cho C, Yoo S, et al. Image-guided Stereotactic Body Radiation Therapy in Patients with Isolated Para-aortic Lymph Node Metastases from Uterine Cervical and Corpus Cancer. Int J Radiat Oncol Biol Phys. 2009; 74(1): 147-153.
75. Kim MS, Choi C, Yoo S, et al. Stereotactic body radiation therapy in patients with pelvic recurrence from rectal carcinoma. Jpn J Clin Oncol. 2008; 38(10): 695-700.
Prostate
76. Buyyounouski MK, Price RA, Harris EER, et al. Stereotactic body radiotherapy for primary management of early-stage, low-to intermediate-ris prostate cancer: Report of the American Society for Therapeutic Radiology and Oncology Emerging Technology Committee. Int J Radiat Oncol Biol Phys. 2010; 76(5): 1297-1304.
77. Freeman DF, King CR. Stereotactic body radiation for low-risk prostate cancer: fi ve year outcomes. Radiat Oncol. 2011; 6:3.
78. Ishiyama H, Teh BS, Lo SS, et al. Stereotactic body radiation therapy for prostate cancer. Future Oncol. 2011; 7(9): 1077-1086. 79. King CR, Brooks JD, Gill H, et al. Long-term outcomes from a prospective trial of stereotactic body radiotherapy for low-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2012; 82(2); 877-882.
80. King CR, Brooks JD, Gill H, et al. Stereotactic body radiotherapy for localized prostate cancer: interim results of a prospective phase II ` clinical trial. Int J Radiat Oncol Biol Phys. 2009; 73(4): 1043–1048.
81. Katz AJ, Santoro M, Ashley R, et al. Stereotactic body radiotherapy for organ-confi ned prostate cancer. BMC Urol. 2010; 10(1) (doi:10.1186/1471-2490-10-1).
82. Madsen BL, Hsi RA, Pham HT, et al. Stereotactic hypofractionated accurate radiotherapy of the prostate (SHARP), 33.5 Gy in fi ve fractions for localized disease: fi rst clinical trial results. Int J Radiat Oncol Biol Phys. 2007; 67(4): 1099-1105.
83. Parthan A, Pruttivarasin N, Davies D, et al. Comparative cost-eff ectiveness of stereotactic body radiation therapy versus intensity-modulated and proton radiation therapy for localized prostate cancer. Front Oncol. 2012; 2:81.
STEREOTACTIC BODY RADIATION THERAPY (SBRT) MODEL POLICY
www.practicalradonc.org
C M EPractical Radiation Oncology (2012) 2, 210–225
Special Article
Radiotherapeutic and surgical management for newlydiagnosed brain metastasis(es): An American Societyfor Radiation Oncology evidence-based guidelineMay N. Tsao MDa,⁎, Dirk Rades MDb, Andrew Wirth MDc, Simon S. Lo MDd,Brita L. Danielson MDe, Laurie E. Gaspar MD, MBAf, Paul W. Sperduto MD, MPPg,Michael A. Vogelbaum MD, PhDh, Jeffrey D. Radawski MDi,Jian Z. Wang PhDn, Michael T. Gillin PhD j, Najeeb Mohideen MDk,Carol A. Hahn MDl, Eric L. Chang MDm
aDepartment of Radiation Oncology, University of Toronto, Odette Cancer Centre, Toronto, Ontario, CanadabDepartment of Radiation Oncology, University Hospital Schleswig-Holstein, Luebeck, Germany (ESTRO representative)cPeter MacCallum Cancer Center, Trans Tasman Radiation Oncology Group (TROG), East Melbourne, AustraliadDepartment of Radiation Oncology, Case Western Reserve University,University Hospitals Case Medical Center, Cleveland, OhioeDepartment of Radiation Oncology, Cross Cancer Institute, University of Alberta, Edmonton, Canada (CARO representative)fDepartment of Radiation Oncology, University of Colorado, Aurora, ColoradogUniversity of Minnesota Gamma Knife Center and Minneapolis Radiation Oncology, Minneapolis, MinnesotahDepartment of Neurological Surgery, Cleveland Clinic, Cleveland, OhioiDepartment of Radiation Oncology, Ohio State University, Columbus, OhiojDepartment of Radiation Oncology, M.D. Anderson Cancer Center, Houston, TexaskDepartment of Radiation Oncology, Northwest Community Hospital, Arlington Heights, IllinoislDepartment of Radiation Oncology, Duke University Medical School, Durham, North CarolinamDepartment of Radiation Oncology, University of Southern California Keck School of Medicine, Los Angeles, CalifornianDepartment of Radiation Oncology, Ohio State University, Columbus, Ohio (deceased)
Received 27 October 2011; revised 9 December 2011; accepted 15 December 2011
Note: An online CME test for this article can be taken at http://astro.org/MOC.Conflicts of interest: Before initiation of this Guideline, all members of the Guidelines Task Group were required to complete disclosure statements.
These statements are maintained at the American Society for Radiation Oncology (ASTRO) headquarters in Fairfax, Virginia and pertinent disclosures arepublished with the report. The ASTRO Conflict of Interest Disclosure Statement seeks to provide a broad disclosure of outside interests. Where a potentialconflict is detected, remedial measures to address any potential conflict are taken and will be noted in the disclosure statement. Dirk Rades has receivedresearch grants from Merck Serono and Novartis, and serves as a consultant for Amgen and Astra Zeneca. Michael Vogelbaum has received researchfunding from Schering-Plough, Genentech, Brainlab, and Astra Zeneca; he owns stock in Johnson and Johnson. Jian Wang has received a prostate cancerresearch grant from the Ohio Cancer Research Associates. Expert reviewers were also required to complete disclosure statements, which are maintained atASTRO Headquarters. The Task Group Chairs reviewed all disclosures and determined that they were not relevant to the subject matter of the Guideline.
⁎ Corresponding author. Odette Cancer Centre, 2075 Bayview Ave, Toronto, ON M4N 3M5.E-mail address: [email protected] (M.N. Tsao).
1879-8500/$ – see front matter © 2012 American Society for Radiation Oncology. Published by Elsevier Inc. All rights reserved.doi:10.1016/j.prro.2011.12.004

Brain metastases: An ASTRO guideline 211Practical Radiation Oncology: July-September 2012
AbstractPurpose: To systematically review the evidence for the radiotherapeutic and surgical managementof patients newly diagnosed with intraparenchymal brain metastases.Methods and Materials: Key clinical questions to be addressed in this evidence-based Guidelinewere identified. Fully published randomized controlled trials dealing with the management ofnewly diagnosed intraparenchymal brain metastases were searched systematically and reviewed.The U.S. Preventative Services Task Force levels of evidence were used to classify various optionsof management.Results: The choice of management in patients with newly diagnosed single or multiple brainmetastases depends on estimated prognosis and the aims of treatment (survival, local treated lesioncontrol, distant brain control, neurocognitive preservation).
Single brainmetastasis and good prognosis (expected survival 3months ormore): For a single brainmetastasis larger than 3 to 4 cm and amenable to safe complete resection, whole brain radiotherapy(WBRT) and surgery (level 1) should be considered. Another alternative is surgery and radiosurgery/radiation boost to the resection cavity (level 3). For single metastasis less than 3 to 4 cm, radiosurgeryalone or WBRT and radiosurgery or WBRT and surgery (all based on level 1 evidence) should beconsidered. Another alternative is surgery and radiosurgery or radiation boost to the resection cavity(level 3). For single brain metastasis (less than 3 to 4 cm) that is not resectable or incompletely resected,WBRTand radiosurgery, or radiosurgery alone should be considered (level 1). For nonresectable singlebrain metastasis (larger than 3 to 4 cm), WBRT should be considered (level 3).
Multiple brain metastases and good prognosis (expected survival 3 months or more): For selectedpatients with multiple brain metastases (all less than 3 to 4 cm), radiosurgery alone, WBRT andradiosurgery, orWBRTalone should be considered, based on level 1 evidence. Safe resection of a brainmetastasis or metastases causing significant mass effect and postoperative WBRT may also beconsidered (level 3).
Patients with poor prognosis (expected survival less than 3 months): Patients with either single ormultiple brain metastases with poor prognosis should be considered for palliative care with or withoutWBRT (level 3).
It should be recognized, however, that there are limitations in the ability of physicians to accuratelypredict patient survival. Prognostic systems such as recursive partitioning analysis, and diagnosis-specific graded prognostic assessment may be helpful.Conclusions:Radiotherapeutic intervention (WBRTor radiosurgery) is associatedwith improved braincontrol. In selected patients with single brain metastasis, radiosurgery or surgery has been found toimprove survival and locally treated metastasis control (compared with WBRT alone).© 2012 American Society for Radiation Oncology. Published by Elsevier Inc. All rights reserved.
Introduction
Brain metastases represent a significant health careproblem. It is estimated that 20% to 40% of cancerpatients will develop brain metastases during the courseof their illness.1
Systematic reviews based on randomized phase IIIcontrolled trials for the management of single ormultiple brain metastases in adult patients have beenpublished.1-8 Various treatment modalities exist, includ-ing whole brain radiotherapy (WBRT), resection, stereo-tactic radiosurgery, and best supportive care with the useof dexamethasone. A series of articles performing asystematic review and evidence-based clinical practiceguidelines have been published from the perspective ofthe modalities listed above under the auspices of theAmerican Association of Neurological Surgeons/Congressof Neurosurgeons (AANS/CNS).4-8 The conclusions fromthis American Society for Radiation Oncology (ASTRO)Guideline are congruent with the conclusions put forthby the AANS/CNS. While these articles are important in
that they are modality-based, it was also felt importantto develop guidelines from an international perspectivewith international representation on the Brain MetastasesTask Group. Additional key questions are posed (notnecessarily previously addressed) such as prognosticclassification systems, radiotherapy fractionation schemes,comparison of surgery and radiosurgery, neurocognitionas an outcome variable in decision-making, palliativesupportive care, and radiation sensitizers.
Treatment recommendations are based on patientfactors (such as age, performance status), tumor factors(such as number and size of brain metastases, tumortype, extracranial disease activity), and available treat-ment options (such as access to neurosurgery orstereotactic radiosurgery).
This Guideline builds on the previous ASTRO HealthServices Research Committee publication, “The AmericanSociety for Therapeutic Radiology and Oncology(ASTRO) evidence-based review of the role of radiosur-gery for brain metastases.”1 This present guideline hasbeen endorsed by the CNS.

212 M.N. Tsao et al Practical Radiation Oncology: July-September 2012
Methods and materials
Process
The Guidelines Subcommittee of the Clinical Affairsand Quality Committee, in accordance with establishedASTRO policy, recruited a Task Group composed ofrecognized experts in the fields of radiotherapy, surgery,and radiosurgery for brain metastases. These expertsrepresent radiation oncology, neurosurgery, physics, out-comes, and health services research. The Task Group wasasked to systematically review the literature on theradiotherapeutic and surgical management for patientswith newly diagnosed metastatic disease to the brain.
In June 2009, the ASTRO Board of Directors approveda proposal to develop a Guideline on radiotherapeutic andsurgical management for newly diagnosed brain metasta-ses. In January 2010, the Board authorized the Task Groupmembership. The Task Group participated in a series ofcommunications by e-mail and conference calls to reviewthe relevant publications, to discuss controversial issues,and formulate the Guidelines contained herein. The TaskGroup agreed by consensus on the various recommenda-tions based on the randomized trials and relevantpublications. The initial draft of the manuscript wasreviewed by 3 expert reviewers and was placed on theASTRO website during the month of April 2011 for publiccomment. Upon integration of the feedback, the documentwas then submitted to the ASTRO Board of Directors fortheir final review and approval in October 2011.
Literature search
MEDLINE (1966-Nov. 3, 2010), EMBASE (1980-2010 week 46), and the CENTRAL databases (issue 4,2010) were searched (Appendix 1). The search strategiesresulted in 1826 publications, 597 publications, and 425publications fromMEDLINE, EMBASE, and CENTRAL,respectively (search strategy courtesy of the CochraneLibrary). Only randomized phase III trials pertinent to themanagement of newly diagnosed brain metastases wereincluded. Trials dealing with the use of WBRT, surgery,radiosurgery, chemotherapy, radiosensitizers, and pallia-tive care alone were considered. Trials that examined theuse of prophylactic cranial irradiation were excluded. Atotal of 36 randomized controlled trials were retrieved.One trial was excluded as it was published in abstract formin the year 2000 but never fully reported.9 Two duplicatepublications of the same trial10,11 were included.
Lead representatives from international radiation on-cology groups, ASTRO, Canadian Association of Radia-tion Oncology (CARO), European Society for TherapeuticRadiology and Oncology (ESTRO), and Trans-TasmanRadiation Oncology Group (TROG), reviewed the 36retrieved trials.
As a result of feedback received from public comments,the literature search was further expanded to includenonrandomized studies (prospective or retrospective)dealing with the use of either radiosurgery or fractionatedradiation to the postoperative surgical cavity. The MED-LINE (1947 to May week 2, 2011) search resulted in 1549nonrandomized publications and EMBASE (1980-2011week 20) gave 3721 nonrandomized publications. TheCENTRAL search resulted in 0 randomized controlledtrials. Titles and abstracts were screened and a final total of15 relevant publications were retrieved.
Of note, all the radiosurgery trials used frame-basedsingle fraction radiosurgery techniques with either a linearaccelerator or gamma knife unit.
Management options were graded by the level ofevidence available using the U.S. Preventative ServicesTask Force levels.12 Due to the lack of high-qualitystudies, management of patients with recurrent metastaticdisease to the brain is not included in this report.
The U.S. Preventative Services Task Force levels ofevidence12 are as follows.
Level I: Evidence obtained from at least 1 properly designedrandomized controlled trial.Level II-1: Evidence obtained from well-designed controlledtrials without randomization.Level II-2: Evidence obtained from well-designed cohort orcase-controlled analytic studies, preferably from more than 1center or research group.Level II-3: Evidence obtained from multiple time series withor without the intervention.
Dramatic results from uncontrolled trials might also beregarded as this type of evidence.
Level III: Opinions of respected authorities, based on clinicalexperience, descriptive studies or reports of expert committees.
The medical management issues associated with brainmetastases will not be addressed by this Guideline as theyare outside the scope of this review. Optimal follow-upbrain imaging for patients with brain metastases has notbeen evaluated using high-quality trials. Based on expertopinion, in patients with good prognostic features andwhere there is potential for future salvage brain metastasestreatment, enhanced magnetic resonance imaging follow-up every 2 to 4 months should be considered.
Results
Table 1 and Table 2 summarize common scenariosrelated to patients presenting initially with either single ormultiple brain metastasis(es). These tables include notonly the level 1 evidence but also other treatment optionsbased on panel opinion and supported by literature oflower quality evidence.

Table 1 Single brain metastasis—initial management
Prognosticcategory ( a)
Otherfeatures
Treatment options (evidence grade)references
Clinical benefit
S LC WB control Neurocognition
Good prognosis Completeresectionpossible
If brain metastasis ≤3-4 cm:
Expected survival3 mo or more
• Surgery and WBRT (level 1)10,11,22,23,42,43,b ✓ ✓ ✓• Radiosurgery and WBRT (level 1)51,53 ✓ ✓ ✓• Radiosurgery alone (Level 1)23,54 ✓ ✓• Surgery with radiosurgery/radiation boostto the resection cavity with or withoutWBRT (level 3)26-41,b
✓ ✓ (with WBRT)
If brain metastasis N3-4 cm:• Surgery and WBRT (level 1)10,11,22,23,42,43,b ✓ ✓ ✓• Surgery with radiosurgery/radiationboost to the resection cavity with or withoutWBRT (level 3)26-41,b
✓ ✓ (with WBRT)
Good prognosis Notresectable
If brain metastasis ≤3-4 cm:
Expected survival3 mo or more
• Radiosurgery and WBRT (level 1)51,53 ✓ ✓ ✓• Radiosurgery alone (level 1)23,54 ✓ ✓
If brain metastasis N3-4 cm:• WBRT (level 3), with consideration ofbiopsy, if primary unknown59,85,86
✓ ✓ ✓
Poor prognosis • WBRT (level 3)59,85 ✓ ✓Expected survivalless than 3 mo
• Palliative care without WBRT (level 3)59,85
KPS, Karnofsky performance status; LC, local control; S, survival; WB, whole brain; WBRT, whole brain radiotherapy.Surgery may be favored if the diagnosis is uncertain (eg, no known primary cancer or remote history of cancer and no known extracranial metastasesor metastasis).
a Prognostic category based on known prognostic factors (see clinical question 1, references 13-21).b Excluding radiosensitive histologies (eg, small cell lung cancer, leukemia, lymphoma, germ cell tumor). A 6%-9% minority of patients in
Radiation Therapy Oncology Group (RTOG) 9508 trial had small cell lung cancer.
Brain metastases: An ASTRO guideline 213Practical Radiation Oncology: July-September 2012
The questions and guideline statements regarding theradiotherapeutic and surgical management for newlydiagnosed brain metastases are listed below.
1. What prognostic factors are important forassessing and managing patients with newlydiagnosed brain metastases?
Interpretative summary
Several prognostic indices have been reported in theliterature13-21 for survival duration among patients withnewly diagnosed brain metastases. These are useful incategorizing patients into survival time strata for treatmentdecisions, for predicting the results of therapeutic in-terventions, and for comparing treatment results.
The Radiation Therapy Oncology Group (RTOG)devised 3 prognostic groups using recursive partitioninganalysis13,14 based on 1200 patients treated on prospec-tive clinical trials with WBRT alone or additionally with
radiosensitizers: class I, patients with Karnofsky perfor-mance status (KPS) ≥70 years, less than 65 years of agewith controlled primary (3-month stability on imaging ornewly diagnosed), and no extracranial metastases; classIII, KPS b70; class II, All others. Median survival was 7.1months, 4.2 months, and 2.3 months for class I, II, and III,respectively.
Brain metastases are a heterogeneous population.The purpose of the graded prognostic assessment(GPA) was to identify significant diagnosis-specificprognostic factors in an updated era (1985-2007) ascompared with the RTOG recursive partitioninganalysis (RPA) (1979-1993). The original GPA wasbased on 4 criteria15: age, KPS, number of brainmetastases, and presence or absence of extracranialmetastases. Each of the 4 criteria is given a score of 0,0.5, or 1.0 and these 4 scores are summed to determine theGPA score. Patients with the best prognosis have a GPAscore of 4.0. The authors established this prognostic indexbased on 1960 patients treated with WBRT alone, WBRTand radiosensitizers, or WBRT and radiosurgery in the
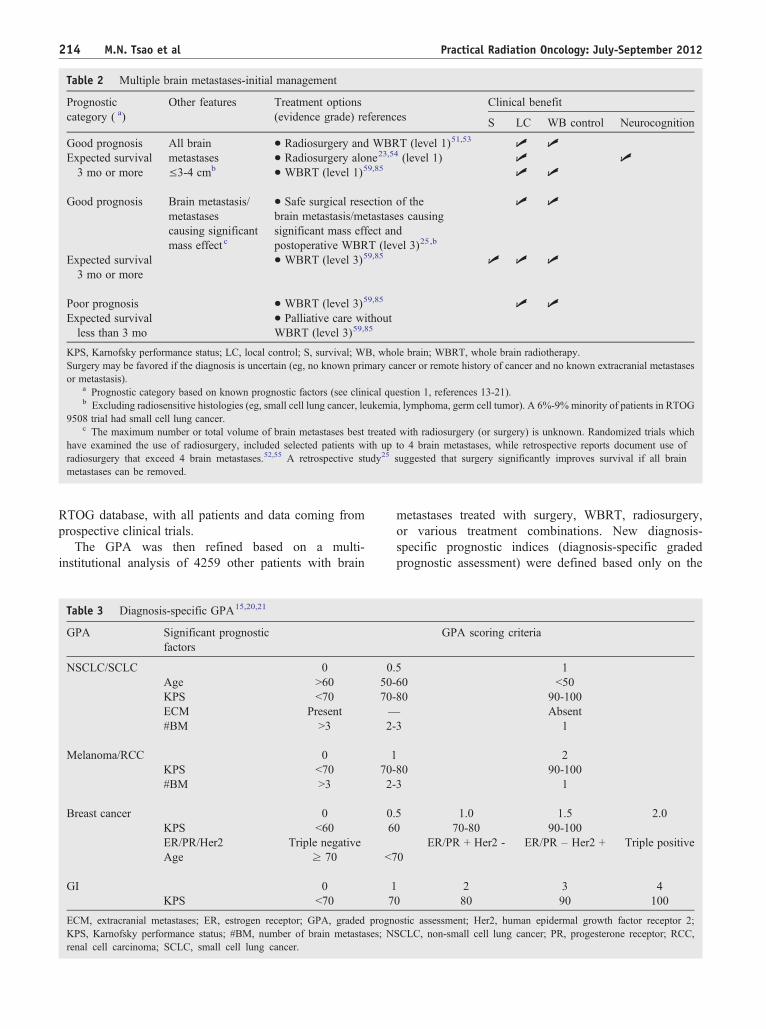
Table 2 Multiple brain metastases-initial management
Prognosticcategory ( a)
Other features Treatment options(evidence grade) references
Clinical benefit
S LC WB control Neurocognition
Good prognosis All brainmetastases≤3-4 cmb
• Radiosurgery and WBRT (level 1)51,53 ✓ ✓Expected survival3 mo or more
• Radiosurgery alone23,54 (level 1) ✓ ✓• WBRT (level 1)59,85 ✓ ✓
Good prognosis Brain metastasis/metastasescausing significantmass effect c
• Safe surgical resection of thebrain metastasis/metastases causingsignificant mass effect andpostoperative WBRT (level 3)25,b
✓ ✓
Expected survival3 mo or more
• WBRT (level 3)59,85 ✓ ✓ ✓
Poor prognosis • WBRT (level 3)59,85 ✓ ✓Expected survivalless than 3 mo
• Palliative care withoutWBRT (level 3)59,85
KPS, Karnofsky performance status; LC, local control; S, survival; WB, whole brain; WBRT, whole brain radiotherapy.Surgery may be favored if the diagnosis is uncertain (eg, no known primary cancer or remote history of cancer and no known extracranial metastasesor metastasis).
a Prognostic category based on known prognostic factors (see clinical question 1, references 13-21).b Excluding radiosensitive histologies (eg, small cell lung cancer, leukemia, lymphoma, germ cell tumor). A 6%-9% minority of patients in RTOG
9508 trial had small cell lung cancer.c The maximum number or total volume of brain metastases best treated with radiosurgery (or surgery) is unknown. Randomized trials which
have examined the use of radiosurgery, included selected patients with up to 4 brain metastases, while retrospective reports document use ofradiosurgery that exceed 4 brain metastases.52,55 A retrospective study25 suggested that surgery significantly improves survival if all brainmetastases can be removed.
214 M.N. Tsao et al Practical Radiation Oncology: July-September 2012
RTOG database, with all patients and data coming fromprospective clinical trials.
The GPA was then refined based on a multi-institutional analysis of 4259 other patients with brain
Table 3 Diagnosis-specific GPA15,20,21
GPA Significant prognosticfactors
NSCLC/SCLC 0 0Age N60 50-KPS b70 70-ECM Present —#BM N3 2-
Melanoma/RCC 0 1KPS b70 70-#BM N3 2-
Breast cancer 0 0KPS b60 6ER/PR/Her2 Triple negativeAge ≥ 70 b7
GI 0 1KPS b70 7
ECM, extracranial metastases; ER, estrogen receptor; GPA, graded prognKPS, Karnofsky performance status; #BM, number of brain metastases; Nrenal cell carcinoma; SCLC, small cell lung cancer.
metastases treated with surgery, WBRT, radiosurgery,or various treatment combinations. New diagnosis-specific prognostic indices (diagnosis-specific gradedprognostic assessment) were defined based only on the
GPA scoring criteria
.5 160 b5080 90-100
Absent3 1
280 90-1003 1
.5 1.0 1.5 2.00 70-80 90-100
ER/PR + Her2 - ER/PR – Her2 + Triple positive0
2 3 40 80 90 100
ostic assessment; Her2, human epidermal growth factor receptor 2;SCLC, non-small cell lung cancer; PR, progesterone receptor; RCC,
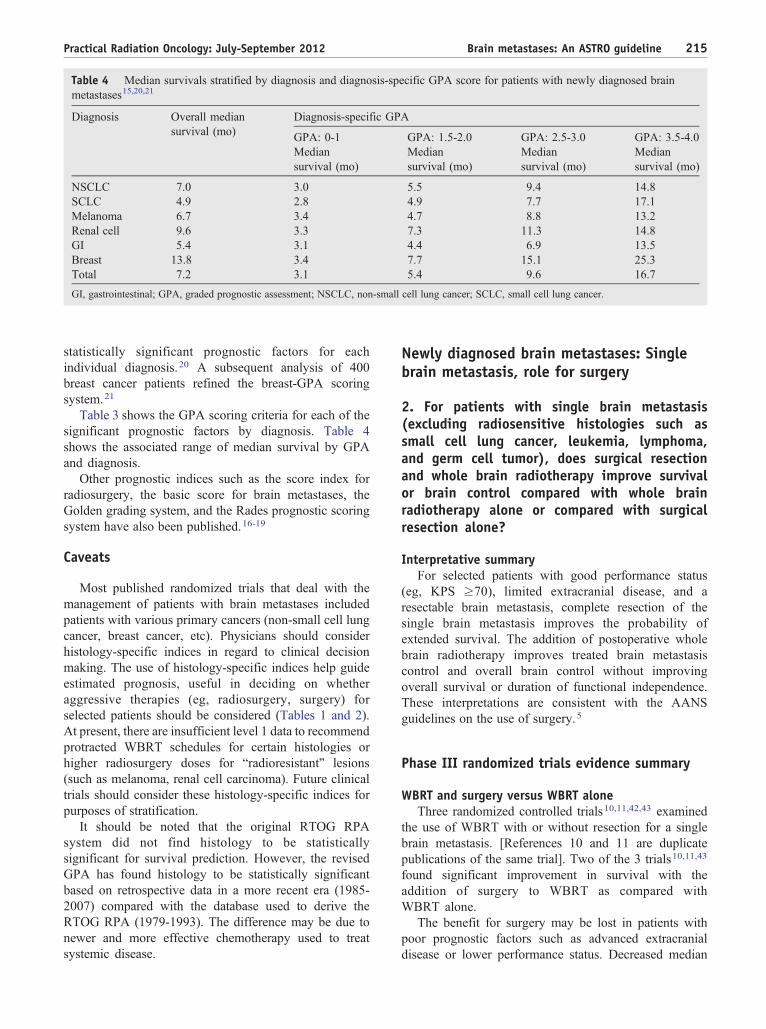
Table 4 Median survivals stratified by diagnosis and diagnosis-specific GPA score for patients with newly diagnosed brainmetastases15,20,21
Diagnosis Diagnosis-specific GPA
GPA: 0-1 GPA: 1.5-2.0 GPA: 2.5-3.0 GPA: 3.5-4.0
Overall mediansurvival (mo)
Mediansurvival (mo)
Mediansurvival (mo)
Mediansurvival (mo)
Mediansurvival (mo)
NSCLC 7.0 3.0 5.5 9.4 14.8SCLC 4.9 2.8 4.9 7.7 17.1Melanoma 6.7 3.4 4.7 8.8 13.2Renal cell 9.6 3.3 7.3 11.3 14.8GI 5.4 3.1 4.4 6.9 13.5Breast 13.8 3.4 7.7 15.1 25.3Total 7.2 3.1 5.4 9.6 16.7
GI, gastrointestinal; GPA, graded prognostic assessment; NSCLC, non-small cell lung cancer; SCLC, small cell lung cancer.
Brain metastases: An ASTRO guideline 215Practical Radiation Oncology: July-September 2012
statistically significant prognostic factors for eachindividual diagnosis.20 A subsequent analysis of 400breast cancer patients refined the breast-GPA scoringsystem.21
Table 3 shows the GPA scoring criteria for each of thesignificant prognostic factors by diagnosis. Table 4shows the associated range of median survival by GPAand diagnosis.
Other prognostic indices such as the score index forradiosurgery, the basic score for brain metastases, theGolden grading system, and the Rades prognostic scoringsystem have also been published.16-19
Caveats
Most published randomized trials that deal with themanagement of patients with brain metastases includedpatients with various primary cancers (non-small cell lungcancer, breast cancer, etc). Physicians should considerhistology-specific indices in regard to clinical decisionmaking. The use of histology-specific indices help guideestimated prognosis, useful in deciding on whetheraggressive therapies (eg, radiosurgery, surgery) forselected patients should be considered (Tables 1 and 2).At present, there are insufficient level 1 data to recommendprotracted WBRT schedules for certain histologies orhigher radiosurgery doses for “radioresistant” lesions(such as melanoma, renal cell carcinoma). Future clinicaltrials should consider these histology-specific indices forpurposes of stratification.
It should be noted that the original RTOG RPAsystem did not find histology to be statisticallysignificant for survival prediction. However, the revisedGPA has found histology to be statistically significantbased on retrospective data in a more recent era (1985-2007) compared with the database used to derive theRTOG RPA (1979-1993). The difference may be due tonewer and more effective chemotherapy used to treatsystemic disease.
Newly diagnosed brain metastases: Singlebrain metastasis, role for surgery
2. For patients with single brain metastasis(excluding radiosensitive histologies such assmall cell lung cancer, leukemia, lymphoma,and germ cell tumor), does surgical resectionand whole brain radiotherapy improve survivalor brain control compared with whole brainradiotherapy alone or compared with surgicalresection alone?
Interpretative summaryFor selected patients with good performance status
(eg, KPS ≥70), limited extracranial disease, and aresectable brain metastasis, complete resection of thesingle brain metastasis improves the probability ofextended survival. The addition of postoperative wholebrain radiotherapy improves treated brain metastasiscontrol and overall brain control without improvingoverall survival or duration of functional independence.These interpretations are consistent with the AANSguidelines on the use of surgery.5
Phase III randomized trials evidence summary
WBRT and surgery versus WBRT aloneThree randomized controlled trials10,11,42,43 examined
the use of WBRT with or without resection for a singlebrain metastasis. [References 10 and 11 are duplicatepublications of the same trial]. Two of the 3 trials10,11,43
found significant improvement in survival with theaddition of surgery to WBRT as compared withWBRT alone.
The benefit for surgery may be lost in patients withpoor prognostic factors such as advanced extracranialdisease or lower performance status. Decreased median

216 M.N. Tsao et al Practical Radiation Oncology: July-September 2012
survival was reported in 2 randomized trials10,11,42 inpatients with a greater systemic involvement of theirprimary malignancy. Noordijk et al10 reported a 5-monthmedian survival in patients with progressive systemicdisease in both the WBRT plus surgery versus WBRTalone arms. Patients with stable systemic disease had a12-month survival with WBRT and surgery versus 7months with WBRT alone. Mintz et al42 reported asignificant difference (P = .009) in the Cox regressionanalysis for mortality in patients having extracranialmetastases versus no evidence of primary tumor (riskratio 2.3). Forty-five percent of the patients in the studyby Mintz et al42 had extracranial metastases comparedwith only 37.5% in the trial by Patchell et al43 and31.7% in the trial by Vecht et al.11
WBRT and surgery versus surgery aloneTwo randomized trials22,23 have been completed that
found a significant improvement in brain control (primaryendpoint) in patients treated with WBRT and surgery ascompared with surgery alone. The first trial22 showed thatpostoperative WBRT significantly prevented brain recur-rence at the site of the original metastasis (10% vs 46%,P b .001) and at other sites in the brain (14% vs 37%, P b.01). The authors found no difference in survival with theuse of WBRT and surgery versus surgery alone, althoughthe study was not powered for survival (a secondaryendpoint of this trial).22
The second trial,23 the European Organization forResearch and Treatment of Cancer (EORTC) 22952-26001 study, found that WBRT reduced the 2-year relapseat the initial site of surgery from 59% to 27% (P b .001),and at new sites from 42% to 23% (P = .008). In addition,salvage therapies were used more frequently afterobservation, compared with after WBRT.23
Caveats
There are 2 completed randomized trials that examineWBRT and surgery versus surgery alone.22,23 The firsttrial22 was small and not powered for survival. The secondtrial by the EORTC23 included patients randomized toreceive postoperative WBRT. A total dose of 30 Gy in 10fractions at 3 Gy per fraction within 6 weeks of surgerywas administered.
The Trans-Tasman Radiation Oncology Group trial(TROG 98.05) was closed early due to poor accrual.24 Theaccrual target was a total of 130 patients. The authorsreported on the 9 patients randomized to observation aftersurgery or radiosurgery and 10 patients randomized toWBRT after surgery or radiosurgery for single brainmetastasis. However, no conclusions could be made fromthis severely underpowered study.
No prospective studies have evaluated whether resec-tion of more than one metastasis conveys meaningfulclinical benefit. A retrospective case control series
suggests the hypothesis that resection of multiple metas-tases may convey a similar benefit as conferred byresection of a single brain metastasis.25 Furthermore, thebenefit of excising multiple brain metastases causing masseffect has not been definitively proven with level 1evidence. However, it was felt by the guideline authorsthat safe resection of multiple brain metastases causingmass effect should be included as an option for goodprognosis patients.
There is a lack of level 1 evidence relating to the useof surgery and radiation boost to the surgical cavity withor without WBRT, although there are publications (withlower level of evidence) supporting its use.26-41 Fourteenpublications27-40 reported on the use of surgery and localradiation (radiosurgery in 10 series and conformalfractionated radiation therapy in 4 series), with therationale to defer or avoid WBRT, without compromis-ing survival. One publication reported on the use ofsurgery, WBRT, and radiosurgery to the surgical cavity,with the rationale to maximize whole brain and localtumor bed control.26
However, due to the paucity of randomized data, it isunknown whether the omission of postoperative WBRT(with a strategy of close radiographic and clinicalfollow-up and the use of salvage radiosurgery orWBRT at relapse) reduces neurocognitive declinecompared with patients undergoing immediate postoper-ative WBRT. On the other hand, in a post hoc analysisof a randomized trial, distant brain metastases recurrence(a higher risk with radiosurgery alone) may have abigger impact on neurocognitive decline.57
Newly diagnosed brain metastases: Singlebrain metastasis, surgery versus radiosurgery
3. Is survival or brain control different in selectedpatients with single brain metastasis (excludingradiosensitive histologies such as small cell lungcancer, leukemia, lymphoma, and germ celltumor) treated with surgery or radiosurgery?
Interpretative summaryThere have been no high quality randomized trials that
have assessed whether selected patients with a small singlebrain metastasis, in surgically accessible sites, shouldundergo radiosurgery or resection. Adding WBRT did notimprove overall survival or functional independence.
Evidence summary
WBRT and surgery versus radiosurgery aloneOne trial44 randomized patients with single (less than
3 cm) resectable brain metastasis to resection plus WBRTversus radiosurgery alone. Due to poor patient accrual, the
Brain metastases: An ASTRO guideline 217Practical Radiation Oncology: July-September 2012
trial was stopped early and reported 33 patients in thesurgery and WBRT arm and 31 patients in the radiosur-gery alone arm. This trial was too underpowered for anyconclusions to be made.
WBRT and radiosurgery versus WBRT and surgeryOne randomized trial examined the use of radiosur-
gery and WBRT versus surgery and WBRT.45 This trialwas closed due to slow accrual. Results were reportedfor 11 patients randomized to radiosurgery and WBRTand 10 patients randomized to surgery and WBRT.Unfortunately, the trial was too underpowered to makeany conclusions.
There have been 2 retrospective series46,47 and 2retrospective matched pair analyses48,49 that examinedthe use of WBRT and radiosurgery versus WBRT andsurgery for a single brain metastasis. These publicationssuggested no difference in overall survival between the2 study groups.
Radiosurgery for “radioresistant” histologiesA phase II trial of radiosurgery for 1 to 3 newly
diagnosed brain metastases (4 cm or less in maximumdimension) from histologies (renal cell carcinoma, mela-noma, and sarcoma) that historically have been deemedradioresistant to fractioned external beam radiotherapy,was reported by the Eastern Cooperative OncologyGroup.50 Thirty-one eligible patients were treated withradiosurgery alone. Three-month intracranial failure withradiosurgery alone was 25.8%; in-field failure rate at 3months was 19.3%.
Distant intracranial failure rate at 3 months was32.2%. Survival was consistent with other publishedseries of similar patients treated with surgery, radiosur-gery, WBRT, or a combination of these therapies. Theintracranial relapse rate was moderately high in this studyof patients treated with radiosurgery alone. Whethersurgery has better local control or survival as comparedwith radiosurgery for “radioresistant” single brainmetastasis could not be answered by this study due tolack of direct comparisons with a surgical group.
Caveats
In good prognosis patients with single brainmetastasis (less than 3 to 4 cm in maximum dimensionand amenable to gross total resection), either surgery orradiosurgery may be considered. Surgery may befavored in patients with unknown primary, or inpatients with single brain metastasis causing significantmass effect. In good prognosis patients with single brainmetastasis less than 3 to 4 cm in maximum dimension(in eloquent brain areas not amenable to safe totalresection or in patients who are unfit for surgery),radiosurgery may be considered.
Newly diagnosed brain metastases: Single ormultiple brain metastasis(es), WBRT with orwithout radiosurgery boost
4. Is there a survival or brain control difference inpatients treated with WBRT and radiosurgeryboost versus WBRT alone?
Interpretative summaryFor good prognosis patients with single brain metasta-
ses (less than 4 cm in size, in patients with goodperformance status and controlled extracranial disease),the use of radiosurgery added to WBRT improvessurvival, treated brain lesion control, and overall braincontrol as compared with WBRT alone.
In good prognosis patients with multiple brainmetastases (all less than 4 cm in size and up to 4 brainmetastases in number), radiosurgery boost when added toWBRT improves treated brain lesion and overall braincontrol as compared with WBRT alone. As there is nosurvival advantage with radiosurgery added to WBRT inpatients with multiple brain metastases, WBRT alonemay be considered.
One randomized trial51 (RTOG 9508) that includedpatients with up to 3 brain metastases found animprovement in KPS and decreased steroid use at 6months with the use of radiosurgery boost added toWBRT. These interpretations are consistent with theAANS guidelines on the use of radiosurgery boost.7
Phase III randomized trials evidence summary
WBRT alone versus WBRT and radiosurgery boostThe multi-institutional, cooperative RTOG 9508 trial51
examined the use of WBRT and radiosurgery boost (n =167) versus WBRT alone (n = 164). This trial includedselected patients with 1 to 3 newly diagnosed brainmetastases with a maximum diameter of 4 cm (for thelargest lesion) and additional lesions not exceeding 3 cm indiameter. Median survival was significantly improved inpatients with single brain metastasis treated with radio-surgery boost (6.5 months) as compared with 4.9 monthsin patients treated with WBRT alone. Higher responserates at 3 months and better control of treated lesions at 1year were observed in the WBRT and radiosurgery groupversus WBRT alone (82% vs 71%, P = .01).
One single institution fully published trial53 stopped atan interim evaluation of 60% accrual (14 patientsrandomized to WBRT alone and 13 patients randomizedto WBRT plus radiosurgery). There was no survivalbenefit with the use of radiosurgery boost as comparedwith WBRT alone in patients with multiple brainmetastases. Patients treated with WBRT and radiosurgeryboost were reported to have better brain control versusthose patients treated with WBRT alone.

218 M.N. Tsao et al Practical Radiation Oncology: July-September 2012
Caveats
None of the trials have examined validated quality oflife outcomes with patients managed with WBRT aloneversus WBRT and radiosurgery boost. Given noexpected survival benefit, either option of WBRTalone with possible salvage treatment or upfrontWBRT and radiosurgery boost may be offered forselected patients with multiple brain metastases. It isunclear from these published trials whether there isbenefit with radiosurgery boost to more than 4 lesions.
However, there are level 3 data on patients undergoingradiosurgery for 4 or more intracranial metastasessuggesting a survival benefit, and that total intracranialvolume rather than number of brain metastases may be themore important predictor of survival.52 At present, thereare insufficient high-quality data on whether certainhistologies benefit from the use of radiosurgery to treatmore than 4 intracranial metastases.
When new brain metastases are seen on the planningscan the day of radiosurgery, it may be reasonable toproceed and complete the radiosurgical procedure to all thelesions visualized even if they exceed a total of 4 brainmetastases. Alternatively, not performing radiosurgery andproceeding with WBRT would also be considered areasonable option in these patients.
Newly diagnosed brain metastases: Single ormultiple brain metastasis(es), radiosurgeryalone versus WBRT and radiosurgery
5. Is there survival, brain control difference, orneurocognitive difference in patients treatedwith radiosurgery alone versus WBRTand radiosurgery?
Interpretative summarySelected patients with brain metastasis(es) may be
treated with radiosurgery alone. A further alternative isWBRT and radiosurgery boost. A third option for selectedpatients with multiple brain metastases is WBRT alone.There have been no convincing survival differencesamong the 3 options listed above, although none of thetrials have been adequately powered to detect anythingother than very large survival differences.
More trials are needed to assess whether there aredifferences in neurocognitive and quality of life outcomeswhen WBRT is omitted in selected patients who aretreated with radiosurgery alone. There is level 3 evidencethat the increased risk of brain recurrence with a strategyof radiosurgery alone (if patients are not monitored andfollowed adequately) may be associated with symptom-atic recurrence, which may not recover fully despitesalvage treatment.88
Evidence summary
Radiosurgery alone versus WBRT and radiosurgery
One fully published trial56 reported on the use ofradiosurgery alone versus WBRT and radiosurgery inselected patients with 1 to 4 brain metastases. The numberof patients with single brain metastases (n = 68) was toosmall to perform meaningful subset analyses.
As such, results were reported for both single andmultiple brain metastases patients. No overall survivaldifference between the 2 groups was found, with a mediansurvival of 7.5 months (WBRT and radiosurgery) versus8 months (radiosurgery alone) (P = .42).
However, the 12-month brain tumor recurrence rate was48.6% in the WBRT and the radiosurgery group comparedwith 76.4% for the radiosurgery alone group (P b .001).
Deterioration in mini-mental score examination(MMSE) occurred in 14 of 36 WBRT and radiosurgerypatients (39%) versus 12 of 46 radiosurgery alone patients(26%; P = .21), and there was no difference in actuarialcurves of freedom-from-3-point drop in MMSE (P = .73).Among patients with MMSE decline, the average durationuntil deterioration of the MMSE was 16.5 months in theWBRT and radiosurgery group as compared with 7.6months in the radiosurgery alone group (P = .05). Theshorter duration to neurocognitive decline (as measuredby the MMSE) was felt by the authors to be attributable tothe increased risk of brain relapse in the radiosurgeryalone group.57 It should be noted, however, that theMMSE is a poor measure of neurocognition as it lacksadequate sensitivity.58
Chang et al54 reported a randomized trial that examinedpatients with 1 to 3 brain metastases treated with WBRTand radiosurgery versus radiosurgery alone. The study wasstopped according to early stopping rules on the basis thatthere was a high probability (96%) that patients randomlyassigned to receive WBRT and radiosurgery were morelikely to show a decline in learning andmemory at 4monthscompared with patients assigned to receive radiosurgeryalone. At 4 months, patients treated with WBRT andradiosurgery had measurable decline in learning andmemory as compared with patients treated with radiosur-gery alone (52% vs 24%, respectively) despite higher ratesof local and distant brain control in patients treated withWBRT and radiosurgery. It remains to be reported whetherneurocognitive outcomes are different between the strategyof radiosurgery alone versus WBRT and radiosurgery atdifferent time points (other than 4 months).
Additionally, there was a survival difference betweenthe 2 arms not readily explained by treatment selection,raising the possibility of inadvertent randomization orselection differences between the 2 groups. An imbalancein the arms of the trial with respect to medications (such asanti-seizure medications and benzodiazepines) may alsoaffect neurocognitive outcomes.

Brain metastases: An ASTRO guideline 219Practical Radiation Oncology: July-September 2012
The subset of patients with single brain metastasis wasnot analyzed separately.
Radiosurgery or surgery alone versus WBRT andradiosurgery or surgery
The EORTC 22952-26001 trial23 included patientswith 1 to 3 brain metastases. Three hundred fifty-ninepatients were recruited. One hundred ninety-nine patientsunderwent radiosurgery and 160 underwent surgery. Forthe radiosurgery group, 100 patients were allocated topost-radiosurgery observation and 99 patients wereallocated to post-radiosurgery WBRT. In the surgerygroup, 79 patients were allocated to postsurgeryobservation and 81 patients were allocated to adjuvantWBRT. Patients eligible for radiosurgery had 1 to 3metastases of solid tumors (small cell lung cancer,lymphoma, leukemia, myeloma, and germ cell tumorswere excluded) and brain metastasis size ≤3.5 cm indiameter for a single lesion (≤2.5 cm for 2 to 3 lesions).A complete resection was required for patients whounderwent surgery.
Overall survival (10.9 months vs 10.7 months) wassimilar in both arms (P = .89). WBRT reduced the 2-yearrelapse rate both at initial sites (surgery: 59% to 27%, P b.001; radiosurgery: 31% to 19%, P = .040) and at new sites(surgery: 42% to 23%, P = .008; radiosurgery: 48% to33%, P = .023). In well-performing patients with stablesystemic disease and 1 to 3 brain metastases, treated withinitial radiosurgery or surgery, WBRT can be withheld ifserial imaging for follow-up is performed. For patientsundergoing surgery for a single brain metastasis, postop-erative local irradiation is an option that should beinvestigated as adjuvant irradiation substantially reducesthe risk of tumor bed recurrence.
Caveats
There is a suggestion based on 1 randomized trial54 thatomission of WBRT after radiosurgery for single brainmetastasis is associated with better neurocognitive out-comes based on formal neurocognitive testing. More trialsaddressing the question of neurocognitive outcomes in thesetting of radiosurgery alone and omission of upfrontWBRT are needed.
These radiosurgery trials assessed selected patients withsmall oligometastases to the brain (up to 4 metastases). It isunknown if there is a cutoff for the maximum number oftargets appropriate for radiosurgery. Total target volume aswell as number of targets may be important for safety andefficacy. A prospective nonrandomized series of patients55
with 1 to 10 brain metastases treated with initialradiosurgery (without WBRT) required less than 10 ccvolume for the largest tumor and less than 15 cc totaltumor volume. Median survival was 0.83 years, 0.69years, 0.69 years, 0.59 years, and 0.62 years for 1, 2, 3-4,5-6, and 7-10 metastases, respectively.
A phase II trial of radiosurgery for 1 to 3 newlydiagnosed brain metastases from histologies (renal cellcarcinoma, melanoma, and sarcoma), which historicallyhave been deemed radioresistant to fractioned externalbeam radiotherapy, was reported by the Eastern Cooper-ative Oncology Group50 (ECOG) as discussed previously.Because the intracranial relapse rate was moderately highin this study using radiosurgery alone (25.8% at 3 monthsand 48.3% at 6 months), the authors concluded thatdelaying WBRT may be appropriate for some subgroupsof patients with “radioresistant” histologies, but routineavoidance of WBRT should be approached judiciously.Whether WBRT should be routinely omitted in radiosur-gery eligible patients with “radioresistant” histologiesremains controversial. There is level 3 evidence that theincreased risk of brain relapse with radiosurgery alone maybe associated with symptomatic recurrences that may notbe reversible with salvage brain treatment.88 In this ECOGtrial, the actuarial incidence of failure within theradiosurgery field at 3 months was 19.3% and at 6 monthswas 32.2%. The brain relapse rate and radiosurgery failurerate in the ECOG trial were similar to the radiosurgeryalone arm in the Aoyama et al,56 Kocher et al,23 andChang et al54 trials.
The trials reported have examined the use ofradiosurgery alone versus WBRT and radiosurgeryboost. There have been no trials that have examinedpatients treated with radiosurgery alone versusWBRT alone.
Newly diagnosed brain metastases: Multiplebrain metastases
6. What is the role of comfort measures orpalliative supportive care alone versus WBRT inpatients with multiple brain metastases?
Interpretative summaryFor selected patients with poor life expectancy (less
than 3 months), the use of whole brain radiotherapy may ormay not significantly improve symptoms from brainmetastases. Comfort measures only, or short course (20Gy in 5 daily fractions) whole brain radiotherapy, arereasonable options.
Evidence summary
WBRT plus supportive care versus supportivecare alone
Only 1 older randomized trial,59 performed in the pre-computed tomographic era, compared WBRT plussupportive care versus supportive care alone (oralprednisone). Median survival in the prednisone alonearm was 10 weeks as compared with 14 weeks in thecombined arm (P value not stated).

220 M.N. Tsao et al Practical Radiation Oncology: July-September 2012
There is 1 on-going Medical Research Council trial(Quartz)87 that randomizes patients to optimal supportivecare using dexamethasone versus optimal supportive careusing dexamethasone and whole brain radiotherapy forpatients with inoperable brain metastases from non-smallcell lung cancer. Outcomes of interest include quality oflife, overall survival, and side effects.
Caveats
There are consistent predictors for poor survival of brainmetastases patients that include poor performance statusand active uncontrolled disease.13-21 Until better therapy isavailable for these poor prognostic patients, supportivecomfort measures without WBRT can be considered.
7. What is the optimal WBRT dosefractionation schedule?
Interpretative summaryNo differences in overall survival or symptom control
have been demonstrated among the commonly usedfractionation schemes, including 30 Gy in 10 dailyfractions or 20 Gy in 5 daily fractions. Other commondose fractionation schedules of WBRT are 37.5 Gy in 15daily fractions and 40 Gy in 20 daily (or twice daily)fractions. This interpretation is consistent with the AANSguideline on whole brain radiotherapy.4
Evidence summary
Altered WBRT dose fractionation schedulesNumerous trials have examined various dose fraction-
ation schedules of WBRT.60-69 No altered dose fraction-ation scheme has shown improvement in either survival orsymptom control (neurologic functional status, neurologicsymptom relief, palliative index, or performance status) ascompared with 20 Gy in 5 fractions or 30 Gy in 10 fractionsof daily WBRT. One trial randomized patients of goodperformance status with brain metastases not suitable forsurgical excision to either 40 Gy in 20 fractions of 2 Gytwice daily versus 20 Gy in 5 daily fractions.68 There wasno difference in median survival (19 weeks in both arms).Another randomized trial examined the use of 40 Gy in 20twice daily fractions versus 20 Gy in 4 daily fractions.69
The primary endpoint of brain progression favored patientstreated with 40 Gy in 20 twice daily fractions (44% vs 64%,P = .03). The secondary endpoint of death from brainprogression was no different between the 2 groups, P = .17.The authors concluded that intracranial disease control wasimproved in patients treated with 40 Gy in 20 twice dailyfractions as compared with 20 Gy in 4 daily fractions.
Caveats
Differences in neurocognitive outcomes have not beenwell studied among the different fractionation schemes.
These trials also did not examine different dosefractionation schedules in the setting of single brainmetastasis treated with surgery. In addition, optimaldose fractionation schedules of WBRT were notexamined in the setting of upfront WBRT withradiosurgery or in the setting of WBRT at the timeof salvage after radiosurgery alone.
8. What is the role of WBRT and radiosensitizersversus WBRT alone in the management ofpatients with brain metastases?
Interpretative summaryThere is no evidence of survival benefit with the use of
radiosensitizers and whole brain radiotherapy.
Evidence summary
WBRT plus radiosensitizers versus WBRT aloneThere have been a few randomized trials70-76 that have
examined the use of radiosensitizers (lonidamine, metro-nidazole, misonidazole, bromodeoxyuridine, motexafingadolinium, and efaproxyn or RSR-13). Overall, noradiosensitizer has improved survival.
Although, the use of motexafin gadolinium wasreported to reduce neurologic progression in patientswith non-small cell lung cancer metastatic to the brain,76
the U.S. Food and Drug Administration did not approvethe use of motexafin gadolinium for non-small cell lungcancer patients with brain metastases in 2007.
A subset analysis of breast cancer patients treated withRSR-13 andWBRT was reported to show an improvementin survival and quality of life as compared with WBRTalone.70 However, the subsequent larger trial designedspecifically with breast cancer patients failed to showbenefit with the use of RSR-13 and WBRT.71 In 2004, theU.S. Food and Drug Administration Oncologic DrugsAdvisory committee did not recommend approval of RSR-13 as an adjunct to WBRT in patients with brainmetastases from breast cancer.
Caveats
More trials are needed to assess the role (if any) ofnovel radiosensitizers in patients with brain metastases.
9. What is the role of chemotherapy and WBRT?
Interpretative summaryAlthough chemotherapy trials reported improved
brain response rates with the use of combined chemo-therapy and WBRT, this was at the cost of toxicity andno overall survival advantage was found with theaddition of chemotherapy.77-82 There currently is nohigh quality evidence to support the routine use ofchemotherapy in the management of brain metastases.

Brain metastases: An ASTRO guideline 221Practical Radiation Oncology: July-September 2012
Evidence summary
Chemotherapy and WBRTThere have been 8 trials examining the use of
chemotherapy for brain metastases.77-84 The chemother-apy agents used were chloroethylnitrosoureas, teniposide,fotemustine, temozolomide, thalidomide, and topotecan.One trial examined the use of early versus delayed WBRTwith chemotherapy in patients with metastatic non-smallcell lung cancer.83 No survival difference was seenbetween early versus delayed WBRT with chemotherapy.Another trial84 examined the use of primary chemotherapyfor newly diagnosed non-small cell lung cancer withsynchronous brain metastases (with delayed WBRT atbrain relapse) versus WBRT administered first. Nosurvival difference was reported between the 2 arms.
Caveats
Further trials are needed to assess the role ofchemotherapy (including novel systemic agents) in themanagement of patients with brain metastases.
Conclusions
Treatment options for brain metastases more than 30years ago were limited to steroids and whole brainradiotherapy and rarely surgery. Management optionstoday have expanded to include comfort measures(including the use of steroids), WBRT and, in selectedpatients, surgery or radiosurgery. Optimal managementdepends on patient factors (such as age, performancestatus), tumor factors (such as extracranial cancer activity,as well as number, size, location, and histopathology ofbrain metastases) and available treatment options (such asexperienced radiosurgery services and neurosurgeons).
The most important endpoint should be the decidingfactor for which treatment is most appropriate. For selectedpatients with single brain metastasis, the use of surgery orradiosurgery has been shown to improve survival and thisshould be the primary consideration.
Treatment options which have been shown to improvewhole brain control (such as the use of WBRT) or localbrain control (such as the use of radiosurgery) withoutsurvival benefit for selected multiple brain metastasespatients are more difficult in terms of best treatmentchoice. The most important outcome likely is quality oflife (taking into account the morbidity of symptomaticbrain recurrence and the morbidity of treatment such asneurocognitive decline, which may be associated with theuse of WBRT or the side effects associated with theprolonged use of dexamethasone). Quality of life hasinconsistently been measured in these trials and drop-outsare a problem with assessing this endpoint.
Numerous research opportunities exist to improveoutcomes (survival, quality of life, brain control, andneurocognitive function) not only in the initial manage-ment of patients with brain metastases but also in the areaof salvage treatment.
Acknowledgments
The authors would like to thank the following in-dividuals who served as expert reviewers of the manu-script: Steven N. Kalkanis, MD, Penny K. Sneed, MD, andMinesh Mehta, MB, ChB. This paper is dedicated and inmemoriam of Jian Z. Wang, PhD. We also acknowledgeShari Siuta for her administrative assistance.
This document was prepared by the GuidelinesSubcommittee of the Clinical Affairs and QualityCommittee (CAQC) of ASTRO in coordination withthe Third International Consensus Conference onPalliative Radiotherapy.
ASTRO Guidelines present scientific, health, andsafety information and may to some extent reflectscientific or medical opinion. They are made available toASTRO members and to the public for educational andinformational purposes only. Any commercial use of anycontent in this Guideline without the prior written consentof ASTRO is strictly prohibited.
Adherence to this Guideline will not ensure successfultreatment in every situation.
Furthermore, this Guideline should not be deemedinclusive of all proper methods of care or exclusive ofother methods of care reasonably directed to obtainingthe same results. The ultimate judgment regarding thepropriety of any specific therapy must be made by thephysician and the patient in light of all circumstancespresented by the individual patient. ASTRO assumes noliability for the information, conclusions, and findingscontained in its Guidelines. In addition, this Guidelinecannot be assumed to apply to the use of theseinterventions performed in the context of clinical trials,given that clinical studies are designed to evaluate orvalidate innovative approaches in a disease for whichimproved staging and treatment are needed or arebeing explored.
This Guideline was prepared on the basis of informa-tion available at the time the Task Group was conductingits research and discussions on this topic. There may benew developments that are not reflected in this Guideline,and that may, over time, be a basis for ASTRO to considerrevisiting and updating the Guideline.
Appendix 1
MEDLINE search strategy:Medline Ovid 1966 to Nov. 3, 2010
222 M.N. Tsao et al Practical Radiation Oncology: July-September 2012
1. exp Brain Neoplasms/2. ((brain or brainstem or intracranial or posterior
fossa) adj3 (cancer⁎ or carcinom⁎ or tumor⁎ ortumour⁎ or neoplasm⁎)).mp.
3. 3 1 or 24. exp Neoplasm Metastasis/ or metastas⁎.mp.5. Radiotherapy/6. Radiotherapy, Adjuvant/7. (radiotherapy or radiat⁎ or radiosurg⁎).mp.8. Combined Modality Therapy/9. Radiosurgery/
10. gamma knife.mp.11. or/5-1012. 3 and 4 and 1113. randomized controlled trial.pt.14. controlled clinical trial.pt.15. randomized.ab.16. placebo.ab.17. radiotherapy.fs.18. randomly.ab.19. trial.ab.20. groups.ab.21. or/13-2022. 12 and 2123. limit 22 to yr = ”1966 - 2010”24. (animals not (humans and animals)).sh.25. 23 not 24
key:mp = title, original title, abstract, name of substance
word, subject heading word, unique identifierpt = publication typeab = abstractfs = floating subheadingsh = subject heading
EMBASE search strategy:Embase Ovid 1980 to 2010 week 46
1. exp Central Nervous System Tumor/2. exp brain cortex/3. ((brain or brainstem or intracranial or posterior
fossa) adj3 (neoplasm⁎ or cancer⁎ or carcinoma⁎ ortumor⁎ or tumour⁎)).mp.
4. or/1-35. Brain Metastasis/ or metastas⁎.mp.6. 4 and 57. exp radiosurgery/8. multimodality cancer therapy/9. Radiotherapy/
10. Cancer radiotherapy/11. (radiotherap⁎ or radiosurg⁎).mp.12. gamma knife.mp.13. radiat⁎.mp.14. or/7-1315. 6 and 1416. random⁎.ti,ab.
17. factorial⁎.ti,ab.18. (crossover⁎ or cross over⁎ or cross-over⁎).ti,ab.19. placebo⁎.ti,ab.20. (doubl⁎ adj blind⁎).ti,ab.21. (singl⁎ adj blind⁎).ti,ab.22. assign⁎.ti,ab.23. allocat⁎.ti,ab.24. volunteer⁎.ti,ab.25. crossover procedure/26. double blind procedure/27. randomized controlled trial/28. single blind procedure/29. or/16-2830. 15 and 2931. animal/ or nonhuman/ or animal experiment/32. human/33. 31 and 3234. 31 not 3335. 30 not 3436. limit 35 to yr = ”1980 - 2010”
key:mp = title, abstract, subject headings, heading word,
drug trade name, original title, device manufacturer, drugmanufacturer name
ti = titleab = abstract
CENTRAL search strategy:CENTRAL Issue 4, 2010
#1. MeSH descriptor Brain Neoplasms explode all trees#2. brain⁎ near/3 (cancer⁎ or carcinoma⁎ or tumor⁎ or
tumour⁎ or neoplasm⁎)#3. brainstem near/3 (cancer⁎ or carcinoma⁎ or tumor⁎
or tumour⁎ or neoplasm⁎)#4. intracranial near/3 (cancer⁎ or carcinoma⁎ or tumor⁎
or tumour⁎ or neoplasm⁎)#5. posterior fossa near/3 (cancer⁎ or carcinoma⁎
tumor⁎ or tumour⁎ or neoplasm⁎)#6. (#1 OR #2 OR #3 OR #4 OR #5)#7. MeSH descriptor NeoplasmMetastasis explode all trees#8. metastas⁎#9. (#7 OR #8)
#10. MeSH descriptor Radiotherapy explode all trees#11. MeSH descriptor Radiotherapy, Adjuvant explode
all trees#12. radiotherapy or radiat⁎ or radiosurg⁎#13. MeSH descriptor Combined Modality Therapy
explode all trees#14. MeSH descriptor Radiosurgery explode all trees#15. gamma knife#16. (#7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13
OR #14 OR #15)#17. (#6 AND #9 AND #16)#18. (#17), from 1980 to 2010
(Literature search courtesy of the Cochrane Library.)

Brain metastases: An ASTRO guideline 223Practical Radiation Oncology: July-September 2012
References
1. Mehta MP, Tsao MN, Whelan TJ, et al. The American Society forTherapeutic Radiology and Oncology (ASTRO) evidence-basedreview of the role of radiosurgery for brain metastases. Int J RadiatOncol Biol Phys. 2005;63:37-46.
2. Tsao MN, Lloyd N, Wong RKS, Chow E, Rakovitch E, LaperriereN. Whole brain radiotherapy for the treatment of multiple brainmetastases–Full review. Cochrane Database Syst Rev. 2006;3:CD003869.
3. Tsao MN, Lloyd NS, Wong RK, et al. Clinical practice guideline onthe optimal radiotherapeutic management of brain metastases. BMCCancer. 2005;5:34.
4. Gaspar LE, Mehta MP, Patchell RA, et al. The role of whole brainradiation therapy in the management of newly diagnosed brainmetastases: a systematic review and evidence based clinical practiceguideline. J Neurooncol. 2010;96:17-32.
5. Kalkanis SN, Kondziolka D, Gaspar LE, et al. The role of surgicalresection in the management of newly diagnosed brain metastases:a systematic review and evidence-based clinical practice guideline.J Neurooncol. 2010;96:33-43.
6. Mehta MP, Paleologos NA, Mikkelsen T, et al. The role ofchemotherapy in the management of newly diagnosed brainmetastases: a systematic review and evidence-based clinical practiceguideline. J Neurooncol. 2010;96:71-83.
7. Linskey ME, Andrews DW, Asher AL, et al. The role of stereotacticradiosurgery in the management of patients with newly diagnosedbrain metastases: a systematic review and evidence-based clinicalpractice guideline. J Neurooncol. 2010;96:45-68.
8. Ryken TC, McDermott M, Robinson PD, et al. The role of steroids inthe management of brain metastases: a systematic review andevidence-based clinical practice guideline. J Neurooncol. 2010;96:103-114.
9. Chougule PB, Burton-Williams M, Saris M, et al. Randomizedtreatment of brain metastases with gamma knife radiosurgery, wholebrain radiotherapy or both. [Abstract] Int J Radiat Oncol Biol Phys.2000;48:114.
10. Noordijk EM, Vecht CJ, Haaxma-Reiche H, et al. The choice oftreatment of single brain metastasis should be based on extra-cranial tumor activity and age. Int J Radiat Oncol Biol Phys. 1994;29:711-717.
11. Vecht CJ, Haaxma-Reiche H, Noordijk EM, et al. Treatment ofsingle brain metastasis: Radiotherapy alone or combined withneurosurgery? Ann Neurol. 1993;33:583-590.
12. US Preventative Services Task Force Evidence Syntheses, formerlySystematic Evidence Reviews. Rockville (MD): Agency forHealthcare Research and Quality (US). 1998.
13. Gaspar LE, Scott C, Rotman M, et al. Recursive partitioning analysis(RPA) of prognostic factors in three Radiation Therapy OncologyGroup (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys.1997;37:745-751.
14. Gaspar LE, Scott C, Murray K, Curran W. Validation ofthe RTOG recursive partitioning analysis (RPA) classificationfor brain metastases. Int J Radiat Oncol Biol Phys. 2000;47:1001-1006.
15. Sperduto PW, Berkey B, Gaspar LE, Mehta M, Curran W. A newprognostic index and comparison to three other indices for patientswith brain metastases: an analysis of 1960 patients in the RTOGdatabase. Int J Radiat Oncol Biol Phys. 2008;70:510-514.
16. Weltman E, Salvajoli JV, Brandt RA, et al. Radiosurgery for brainmetastases: a score index for predicting prognosis. Int J RadiatOncol Biol Phys. 2000;46:1155-1161.
17. Lorenzoni J, Devriendt D, Massager N, et al. Radiosurgerytreatment of brain metastases: estimation of patient eligibilityusing three stratification systems. Int J Radiat Oncol Biol Phys.2004;60:218-224.
18. Golden DW, Lamborn KR, McDermott MW, et al. Prognosticfactors and grading systems for overall survival in patients treatedwith radiosurgery for brain metastases: variation by primary site.J Neurosurg. 2008;109(Suppl):77-86.
19. Rades D, Dunst J, Schild SE. A new scoring system to predicting thesurvival of patients treated with whole brain radiotherapy for brainmetastases. Strahlenther Onkol. 2008;184:251-255.
20. Sperduto PW, Chao ST, Sneed PK, et al. Diagnosis-specificprognostic factors, indexes, and treatment outcomes for patientswith newly diagnosed brain metastases: a multi-institutionalanalysis of 4259 patients. Int J Radiat Oncol Biol Phys. 2010;77:655-661.
21. Sperduto PW, Xu Z, Sneed P, et al. The graded prognosticassessment for women with brain metastases from breast cancer(GPA-Breast): a Diagnosis-Specific Prognostic Index. Int J RadiatOncol Biol Phys. 2010;78(suppl):S6-S7.
22. Patchell RA, Tibbs PA, Regine WF, et al. Postoperative radiotherapyin the treatment of single metastasis to the brain. JAMA. 1998;280:1485-1489.
23. Kocher M, Soffietti R, Abacioglu U, et al. Adjuvant whole-brainradiotherapy versus observation after radiosurgery or surgicalresection of one to three cerebral metastases: results of the EORTC22952-26001 study. J Clin Oncol. 2011;29:134-141.
24. Roos DE, Wirth A, Burmeister BH, et al. Whole brain irradiationfollowing surgery or radiosurgery for solitary brain metastases:mature results of a prematurely closed randomized Trans-TasmanRadiation Oncology Group trial (TROG 98.05). Radiother Oncol.2006;80:318-322.
25. Bindal RK, Sawaya R, Leavens ME, Lee JJ. Surgical treatment ofmultiple brain metastases. J Neurosurg. 1993;79:210-216.
26. Roberge D, Petrecca K, El Refae M, Souhami L. Whole brainradiotherapy and tumor bed radiosurgery following resection ofsolitary brain metastasis. J Neuro Oncol. 2009;95:95-99.
27. Soltys SG, Adler JR, Lipani JD, et al. Stereotactic radiosurgery of thepostoperative resection cavity for brain metastases. Int J RadiatOncol Biol Phys. 2008;70:187-193.
28. Jagannathan J, Yen CP, Ray DK, et al. Gamma knife radiosurgeryto the surgical cavity following resection of brain metastases.J Neurosurg. 2009;111:431-438.
29. Do L, Pezner R, Radany E, Liu A, Staud C, Badie B. Resectionfollowed by stereotactic radiosurgery to resection cavity forintracranial metastases. Int J Radiat Oncol Biol Phys. 2009;73:486-491.
30. Quigley MR, Fuhrer R, Karlovits S, Karlovits B, Johnson M. Singlesession stereotactic radiosurgery boost to the post-operative site inlieu of whole brain radiation in metastatic brain disease.J Neurooncol. 2008;87:327-332.
31. Mathieu D, Knodziolka D, Flickinger JC, et al. Tumor bedradiosurgery after resection of cerebral metastases. Neurosurg.2008;62:817-823.
32. Bahl G, White G, Alksne J, Vemuri L, Spear MA. Focal radiationtherapy of brain metastases after complete surgical resection. MedOncol. 2006;23:317-324.
33. Hwang SW, Abozed MM, Hale A, et al. Adjuvant Gamma Kniferadiosurgery following surgical resection of brain metastases: a9-year retrospective cohort study. J Neurooncol. 2010;98:77-82.
34. Tolentino PJ. Brain metastases secondary to breast cancer: treatmentwith surgical resection and stereotactic radiosurgery. Mo Med.2009;106:428-431.
35. Karlovits BJ, Quigley MR, Karlovits SM, et al. Stereotacticradiosurgery boost to the resection bed for oligometastatic braindisease: challenging the tradition of adjuvant whole-brain radiother-apy. Neurosurg Focus. 2009;27:E7.
36. Lindvall P, Bergström P, Löfroth PO, Tommy Bergenheim A. Acomparison between surgical resection in combination with WBRTor hypofractionated stereotactic irradiation in the treatment ofsolitary brain metastases. Acta Neurochir. 2009;151:1053-1059.

224 M.N. Tsao et al Practical Radiation Oncology: July-September 2012
37. Limbrick Jr DD, Lusis EA, Chicoine MR, et al. Combined surgicalresection and stereotactic radiosurgery for treatment of cerebralmetastases. Surg Neurol. 2009;71:280-288.
38. Iwai Y, Yamanaka K, Yasui T. Boost radiosurgery for treatment ofbrain metastases after surgical resections. Surg Neurol. 2008;69:181-186.
39. Iwadate Y, Namba H, Yamaura A. Whole brain radiation therapy isnot beneficial as adjuvant therapy for brain metastases comparedwith localized irradiation. Anticancer Res. 2002;22:325-330.
40. Coucke PA, Zouhair A, Ozsahin M, De Tribolet N, Mirimanoff RO.Focalized external radiotherapy for resected solitary brain metastasis:does the dogma stand? Radiother Oncol. 1998;47:99-101.
41. Roberge D, Souhami L. Tumor bed radiosurgery following resectionof brain metastases: a review. Technol Cancer Res Treat. 2010;9:597-602.
42. Mintz AH, Kestle J, Rathbone MP, et al. A randomized trial to assessthe efficacy of surgery in addition to radiotherapy in patients withsingle brain metastasis. Cancer. 1996;78:1470-1476.
43. Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial ofsurgery in the treatment of single metastasis to the brain. N Engl JMed. 1990;322:494-500.
44. Muacevic A, Wowra B, Siefert A, Tonn JC, Steiger HJ, Kreth FW.Microsurgery plus whole brain irradiation versus Gamma Knifesurgery alone for treatment of single metastasis to brain: arandomized controlled multicentre phase III trial. J Neurooncol.2008;87:299-307.
45. Roos DE, Smith JG, Stephens SW, et al. Radiosurgery versussurgery, both with adjuvant whole brain radiotherapy, for solitarybrain metastases: a randomized controlled trial. Clin Oncol (R CollRadiol). 2011;23:646-651.
46. Schöggl A, Kitz K, Reddy M, et al. Defining the role of stereotacticradiosurgery versus microsurgery in the treatment of single brainmetastases. Acta Neurochir (Wien). 2000;142:621-626.
47. O'Neill BP, Iturria NJ, Link MJ, Pollock BE, Ballman KV, O'FallonJR. A comparison of surgical resection and stereotactic radiosurgeryin the treatment of solitary brain metastases. Int J Radiat Oncol BiolPhys. 2003;55:1169-1176.
48. Rades D, Kueter JD, Veninga T, Gliemroth J, Schild SE. Wholebrain radiotherapy plus stereotactic radiosurgery (WBRT +SRS)versus surgery plus whole brain radiotherapy (OP+WBRT) for 1-3brain metastases: results of a matched pair analysis. Eur J Cancer.2009;45:400-404.
49. Rades D, Kueter JD, Pluemer A, Veninga T, Schild SE. A matched-pair analysis comparing whole-brain radiotherapy plus stereotacticradiosurgery versus surgery plus whole-brain radiotherapy and aboost to the metastatic site for one to two brain metastases. Int JRadiat Oncol Biol Phys. 2009;73:1077-1081.
50. Manon R, O'Neill A, Knisely J, et al. Phase II trial ofradiosurgery for one to three newly diagnosed brain metastasesfrom renal cell carcinoma, melanoma and sarcoma: an EasternCooperative Oncology Group Study (E 6397). J Clin Oncol.2005;23:8870-8876.
51. Andrews DW, Scott CB, Sperduto PW, et al. Whole brain radiationtherapy with and without stereotactic radiosurgery boost for patientswith one to three brain metastases: Phase III results of the RTOG9508 randomised trial. Lancet. 2004;363:1665-1672.
52. Bhatnagar AK, Flickinger JC, Kondziolka D, Lunsford LD.Stereotactic radiosurgery for four or more intracranial metastases.Int J Radiat Oncol Biol Phys. 2006;64:898-903.
53. Kondziolka D, Patel A, Lunsford LD, Kassam A, Flickinger JC.Stereotactic radiosurgery plus whole brain radiotherapy versusradiotherapy alone for patients with multiple brain metastases. IntJ Radiat Oncol Biol Phys. 1999;45:427-434.
54. Chang EL, Wefel JS, Hess KR, et al. Neurocognition in patients withbrain metastases treated with radiosurgery or radiosurgery pluswhole-brain irradiation: a randomised controlled trial. Lancet Oncol.2009;10:1037-1044.
55. Serizawa T, Hirai T, Nagano O, et al. Gamma knife radiosurgery for1-10 brain metastases without prophylactic whole-brain radiationtherapy: analysis of cases meeting the Japanese prospective multi-institute study (JLG0901) inclusion criteria. J Neurooncol. 2010;98:163-167.
56. Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery pluswhole-brain radiation therapy vs stereotactic radiosurgery alone fortreatment of brain metastases: a randomized controlled trial. JAMA.2006;295:2483-2491.
57. Aoyama H, Tago M, Kato N, et al. Neurocognitive function ofpatients with brain metastasis who received either whole brainradiotherapy plus stereotactic radiosurgery or radiosurgery alone. IntJ Radiat Oncol Biol Phys. 2007;68:1388-1395.
58. Meyers CA, Wefel JS. The use of the mini-mental state examinationto assess cognitive functioning in cancer trials: no ifs, ands, buts orsensitivity. [Editorial] J Clin Oncol. 2003;21:3557-3558.
59. Horton J, Baxter DH, Olson KB. The management of metastases tothe brain by irradiation and corticosteroids. Am J Roentgenol RadiumTher Nucl Med. 1971;111:334-336.
60. Haie-Meder C, Pellae-Cosset B, Laplanche A, et al. Results of arandomized clinical trial comparing two radiation schedules in thepalliative treatment of brain metastases. Radiother Oncol. 1993;26:111-116.
61. Borgelt B, Gelber R, Kramer S, et al. The palliation of brainmetastases: final results of the Radiation Therapy Oncology Group.Int J Radiat Oncol Biol Phys. 1980;6:1-9.
62. Borgelt B, Gelber R, Larson M, Hendrickson F, Griffin T, Roth R.Ultra-rapid high dose irradiation schedules for the palliation of brainmetastases: final results of the first two studies by the RadiationTherapy Oncology Group. Int J Radiat Oncol Biol Phys. 1981;7:1633-1638.
63. Chatani M, Teshima T, Hata K, Inoue T, Suzuki T. Whole brainirradiation for metastases from lung carcinoma. A clinical investi-gation. Acta Radiol Oncol. 1985;24:311-314.
64. Harwood AR, Simson WJ. Radiation therapy of cerebral metastases:a randomized prospective clinical trial. Int J Radiat Oncol Biol Phys.1977;2:1091-1094.
65. Kurtz JM, Gelber R, Brady LW, Carella RJ, Cooper JS. Thepalliation of brain metastases in a favourable patient population: Arandomized clinical trial by the Radiation Therapy Oncology Group.Int J Radiat Oncol Biol Phys. 1981;7:891-895.
66. Murray KJ, Scott C, Greenberg H, et al. A randomized phase IIIstudy of accelerated hyperfracionation versus standard in patientswith unresectable brain metastases: a report of the Radiation TherapyOncology Group (RTOG) 9104. Int J Radiat Oncol Biol Phys.1997;39:571-574.
67. Priestman TJ, Dunn J, Brada M, et al. Final results of the RoyalCollege of Radiologists' trial comparing two different radiotherapyschedules in the treatment of cerebral metastases. Clin Oncol (R CollRadiol). 1996;8:308-315.
68. Davey P, Hoegler D, Ennis M, Smith J. A phase III study ofaccelerated versus conventional hypofractionated whole brainirradiation in patients of good performance status with brainmetastases not suitable for surgical excision. Radiother Oncol.2008;88:173-176.
69. Graham PH, Bucci J, Browne L. Randomized comparison of wholebrain radiotherapy, 20 Gy in 4 daily fractions versus 40 Gy in 20twice-daily fractions for brain metastases. Int J Radiat Oncol BiolPhys. 2010;77:648-654.
70. Scott C, Suh J, Stea B, Nabid A, Hackman J. Improvedsurvival, quality of life, and quality adjusted survival in breastcancer patients treated with efaproxiral (Efaproxyn) plus wholebrain radiation therapy for brain metastases. Am J Clin Oncol.2007;30:580-587.
71. Suh JH, Stea B, Tankel K, et al. Results of the phase III ENRICH(RT-016) study of efaproxiral administered concurrent with wholebrain radiation therapy (WBRT) in women with brain metastases
Brain metastases: An ASTRO guideline 225Practical Radiation Oncology: July-September 2012
from breast cancer. Int J Radiat Oncol Biol Phys. 2008;72(Suppl):S50-S51.
72. DeAngelis LM, Currie VE, Kim JH, et al. The combined use ofradiation therapy and lonidamide in the treatment of brainmetastases. J Neurooncol. 1989;7:241-247.
73. Eyre HJ, Ohlsen JD, Frank J, et al. Randomized trial of radiotherapyversus radiotherapy plus metronidazole for the treatment ofmetastatic cancer to brain. J Neurooncol. 1984;2:325-330.
74. Komarnicky LT, Phillips TL, Martz K, Asbell S, Isaacson S, UrtasunR. A randomized phase III protocol for the evaluation ofmisonidazole combined with radiation in the treatment of patientswith brain metastases (RTOG -7916). Int J Radiat Oncol Biol Phys.1991;20:53-58.
75. Phillips TL, Scott CB, Leibel SA, Rotman M, Weigensberg IJ.Results of the randomized comparison of radiotherapy andbromodeoxyuridine with radiotherapy alone for brain metastases:report of RTOG trial 89-05. Int J Radiat Oncol Biol Phys. 1995;33:339-348.
76. Mehta MP, Shapiro WR, Phan SC, et al. Motexafin gadoliniumcombined with prompt whole brain radiotherapy prolongs time toneurologic progression in nonsmall-cell lung cancer patients withbrain metastases: results of a phase III trial. Int J Radiat Oncol BiolPhys. 2009;73:1069-1076.
77. Postmus PE, Haaxma-Reiche H, Smit EF, et al. Treatment of brainmetastases of small-cell lung cancer: comparing teniposide andteniposide with whole brain radiotherapy- a phase III study of theEuropean Organization for the Research and Treatment of LungCancer Cooperative Group. J Clin Oncol. 2000;18:3400-3408.
78. Ushio Y, Arita N, Hayakawa T, et al. Chemotherapy of brainmetastases from lung carcinoma: a controlled randomized study.Neurosurg. 1991;28:201-205.
79. Antonadou D, Paraskevaidis M, Saris G, et al. Phase II randomizedtrial of temozolomide and concurrent radiotherapy in patients withbrain metastases. J Clin Oncol. 2002;20:3644-3650.
80. Mornex F, Thomas L, Mohr P, et al. Randomized phase III trial offotemustine versus fotemustine plus whole brain irradiation in
cerebral metastases of melanoma. [Article in French] CancerRadiother. 2003;7:1-8.
81. Knisely JPS, Berkey B, Chakravarti A, et al. A phase III study ofconventional radiation therapy plus thalidomide versus conventionalradiation therapy for multiple brain metastases (RTOG 0118). Int JRadiat Oncol Biol Phys. 2008;71:79-86.
82. Neuhaus T, Ko Y, Muller RP, et al. A phase III trial of topotecan andwhole brain radiation therapy for patients with CNS-metastases dueto lung cancer. Br J Cancer. 2009;100:291-297.
83. Robinet G, Thomas P, Breton JL, et al. Results of a phase IIIstudy of early versus delayed whole brain radiotherapy withconcurrent cisplatin and vinorelbine combination in inoperablebrain metastasis of non-small cell lung cancer: Groupe Françaisde Pneumo-Cancérologie (GFPC) Protocol 95-1. Ann Oncol.2001;12:59-67.
84. Lee DH, Han J-Y, Kim HT, et al. Primary chemotherapy for newlydiagnosed NSCLC with synchronous brain metastases comparedwith WBRT administered first. Result of a randomized pilot study.Cancer. 2008;113:143-149.
85. Komosinska K, Kepka L, Niwinska A, et al. Prospective evaluationof the palliative effect of whole brain radiotherapy in patients withbrain metastases and poor performance status. Acta Oncol. 2010;49:382-388.
86. Campos S, Davey P, Hird A, et al. Brain metastasis from anunknown primary or primary brain tumour? A diagnostic dilemma.Curr Oncol. 2009;16:62-66.
87. Cancer Research UK. A trial looking at the treatment of lungcancer which has spread to the brain (Quartz). Available at:http://cancerhelp.cancerresearchuk.org/trials/a-trial-looking-at-the-treatment-oflung-cancer-which-has-spread-to-the-brain. AccessedSeptember 19, 2011.
88. Regine WF, Huhn JL, Patchell RA, et al. Risk of symptomaticbrain tumor recurrence and neurologic deficit after radiosurgeryalone in patients with newly diagnosed brain metastases:results and implications. Int J Radiat Oncol Biol Phys. 2002;52:333-338.

A S T R O / A C R G U I D E T O
RADIATION ONCOLOGY CODING 2010
2014 GUIDE
COMPREHENSIVE GUIDE INCLUDES UPDATES FROM 2011 – 2014

Copyright© 2014 by the American Society for Radiation Oncology and the American College of Radiology.
All rights reserved. No part of this publication covered by the copyright herein may be reproduced or cop-ied in any form or by any means – graphic, electronic or mechanical, including photocopying, taping or information storage and retrieval systems – without written permission of the publishers.
CPT© copyright 2013 American Medical Association. All rights reserved.
Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT© and the AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The AMA assumes no liability for data contained or not contained herein.
CPT© is a registered trademark of the American Medical Association.
The responsibility for the content of any “National Correct Coding Policy” included in this product is with the Centers for Medicare and Medicaid Services, and no endorsement by the AMA is intended or should be implied. The AMA disclaims responsibility for any consequences or liability attributable to or related to any use, nonuse or interpretation of information contained in this product.
T A R G E T I N G C A N C E R C A R E
76 | C P T C O P Y R I G H T © 2 0 1 3 A M E R I C A N M E D I C A L A S S O C I AT I O N . A L L R I G H T S R E S E R V E D.
13Stereotactic radiosurgery (SRS) is a technique for delivering a high dose of radiation to a specifi c target.
STEREOTACTICRADIOSURGERY

CHAPTER 13
STEREOTACTIC RADIOSURGERY (SRS) CPT® CODES 77371, 77372, 77432
STEREOTACTIC RADIOSURGERY (SRS) IS A TECHNIQUE FOR DELIVERING A HIGH DOES OF RADIATION TO A SPECIFIC TARGET while delivering a minimal dose to surrounding tissues. This technique is used to treat defined target(s) in the head and spine. It is typically performed in a single session, but can be performed in a limited number of sessions, up to a maximum of five. Stereotactic treatment depends on the accurate and reproducible spatial correlation of the target and the radiation source using three-dimensional CT and/or MR simulation. Extreme precision of patient positioning is essential for accurate treatment delivery. This additional precision is achieved through rigid immobilization, such as with a rigid frame, or with image-based techniques.
Stereotactic treatments can be given with either photon or particle therapy. In both approaches, multiple beams converge on the target. Thus, the target gets a much higher dose than surrounding tissues, and a steep dose gradient can be obtained close to the periphery of the target. This technique is capable of great accuracy and precision and can deliver radiation dosages within 1 mm of the planned position.
The radiation oncologist is responsible for target volume delineation, treatment planning, supervising the patient positioning, proper alignment of treatment beams and management of the patient during treatment. From a billing and coding perspective, there is a difference in the codes used for single fraction cranial SRS and fractionated cranial SRS (2- 5 fractions) and all spinal SRS (1-5 fractions) as further explained in the section Radiation Treatment Management in this chapter.
COMMON CLINICAL INDICATIONS SRS is appropriate for the treatment of certain malignant and benign neoplasms of the brain and spine, cranial nerves and meninges, arteriovenous malformations of cerebral vessels and other non-neoplastic conditions for which it has been established to be effective. This includes both primary and metastatic diseases. Movement disorders such as Parkinson's disease, essential tremor and other disabling tremors may be treated with stereotactic radiosurgery when stereotactic thalamotomy cannot be performed. SRS is often effective therapy for trigeminal neuralgia refractory to medical management.
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 146
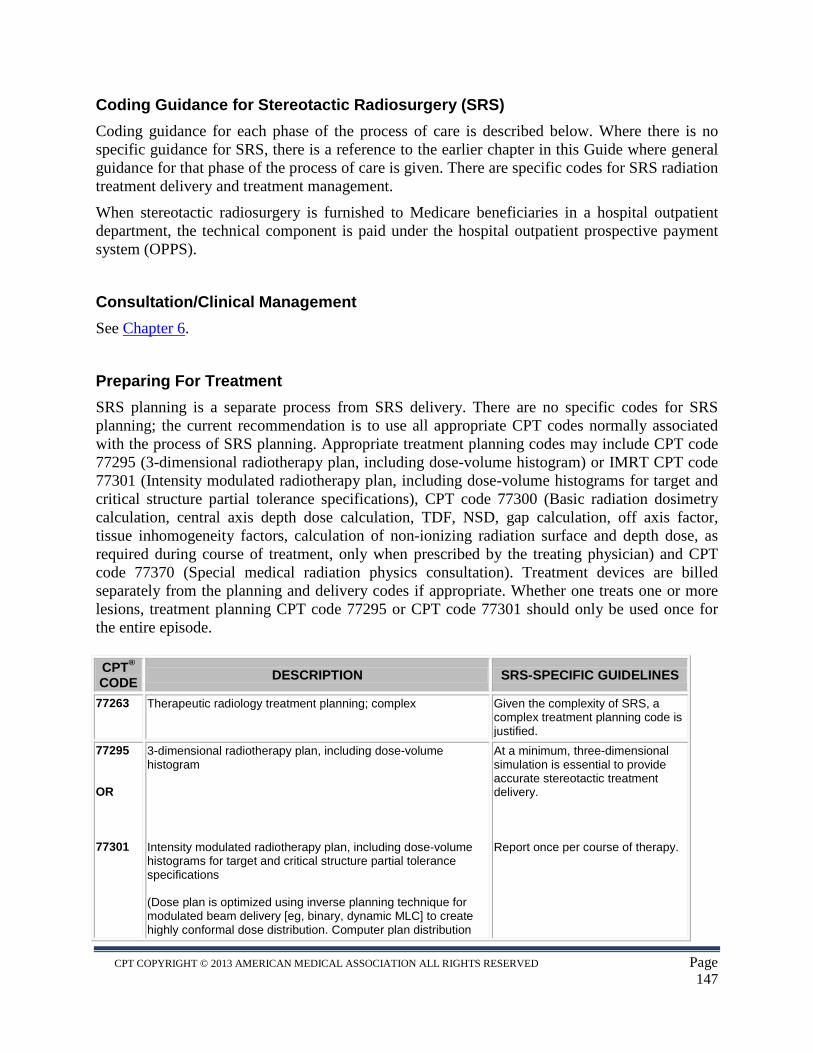
Coding Guidance for Stereotactic Radiosurgery (SRS) Coding guidance for each phase of the process of care is described below. Where there is no specific guidance for SRS, there is a reference to the earlier chapter in this Guide where general guidance for that phase of the process of care is given. There are specific codes for SRS radiation treatment delivery and treatment management.
When stereotactic radiosurgery is furnished to Medicare beneficiaries in a hospital outpatient department, the technical component is paid under the hospital outpatient prospective payment system (OPPS).
Consultation/Clinical Management See Chapter 6.
Preparing For Treatment SRS planning is a separate process from SRS delivery. There are no specific codes for SRS planning; the current recommendation is to use all appropriate CPT codes normally associated with the process of SRS planning. Appropriate treatment planning codes may include CPT code 77295 (3-dimensional radiotherapy plan, including dose-volume histogram) or IMRT CPT code 77301 (Intensity modulated radiotherapy plan, including dose-volume histograms for target and critical structure partial tolerance specifications), CPT code 77300 (Basic radiation dosimetry calculation, central axis depth dose calculation, TDF, NSD, gap calculation, off axis factor, tissue inhomogeneity factors, calculation of non-ionizing radiation surface and depth dose, as required during course of treatment, only when prescribed by the treating physician) and CPT code 77370 (Special medical radiation physics consultation). Treatment devices are billed separately from the planning and delivery codes if appropriate. Whether one treats one or more lesions, treatment planning CPT code 77295 or CPT code 77301 should only be used once for the entire episode. CPT® CODE DESCRIPTION SRS-SPECIFIC GUIDELINES
77263 Therapeutic radiology treatment planning; complex Given the complexity of SRS, a complex treatment planning code is justified.
77295 OR 77301
3-dimensional radiotherapy plan, including dose-volume histogram Intensity modulated radiotherapy plan, including dose-volume histograms for target and critical structure partial tolerance specifications (Dose plan is optimized using inverse planning technique for modulated beam delivery [eg, binary, dynamic MLC] to create highly conformal dose distribution. Computer plan distribution
At a minimum, three-dimensional simulation is essential to provide accurate stereotactic treatment delivery. Report once per course of therapy.
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 147

must be verified for positional accuracy based on dosimetric verification of the intensity map with verification of treatment set-up and interpretation of verification methodology)
Medical Radiation Physics, Dosimetry, Treatment Devices and Special Services There are no SRS-specific codes for medical radiation physics, dosimetry, treatment devices and special services. However, the codes for basic dosimetry CPT® code 77300, CPT code 77370 and complex devices CPT code 77334 can be used as described below. See Chapter 8 for further guidance. CPT® CODE DESCRIPTION SRS-SPECIFIC GUIDELINES
77300 Basic radiation dosimetry calculation, central axis depth dose calculation, TDF, NSD, gap calculation, off axis factor, tissue inhomogeneity factors, calculation of non-ionizing radiation surface and depth dose, as required during course of treatment, only when prescribed by the treating physician
One unit for each arc in linear accelerator system. One unit for each shot in Cobalt-60. Maximum of 10 units.
77370 Special medical radiation physics consultation May be reasonable and necessary if ordered by the Radiation Oncologist.
77334 Treatment devices, design and construction; complex (irregular blocks, special shields, compensators, wedges, molds or casts)
One unit for each unique combination of beam angle and collimator pattern or each unique arc; certain carrier limitations may apply. One unit for each helmet in Cobalt-60.
77338 Multi-leaf collimator (MLC) device(s) for intensity modulated radiation therapy (IMRT), design and construction, per IMRT plan
If IMRT planning code 77301 is used for coding treatment planning then one CPT 77338 should be used to code for the devices.
Radiation Treatment Delivery CMS has historically used HCPCS G-codes to distinguish between robotic and non-robotic SRS delivery methods. In the CY 2014 Hospital Outpatient Prospective Payment System (HOPPS) final regulations, CMS announced that as of January 1, 2014, the agency will no longer differentiate between robotic and non-robotic linac-based SRS through HCPCS G-codes. For CY 2014, CMS will replace the existing four HCPCS codes: G0173, G0251, G0339 and G0340 with the SRS CPT® codes 77372 and 77373. The chart below provides a summary of these changes.
2013 CPT® OR HCPCS
Code DESCRIPTOR 2014 CPT®
Code DESCRIPTOR
77371 Radiation treatment delivery, stereotactic radiosurgery (SRS), complete course of
77371 Radiation treatment delivery, stereotactic radiosurgery (SRS), complete course of treatment of cranial lesion(s) consisting of 1 session; multi-source Cobalt-60 based
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 148
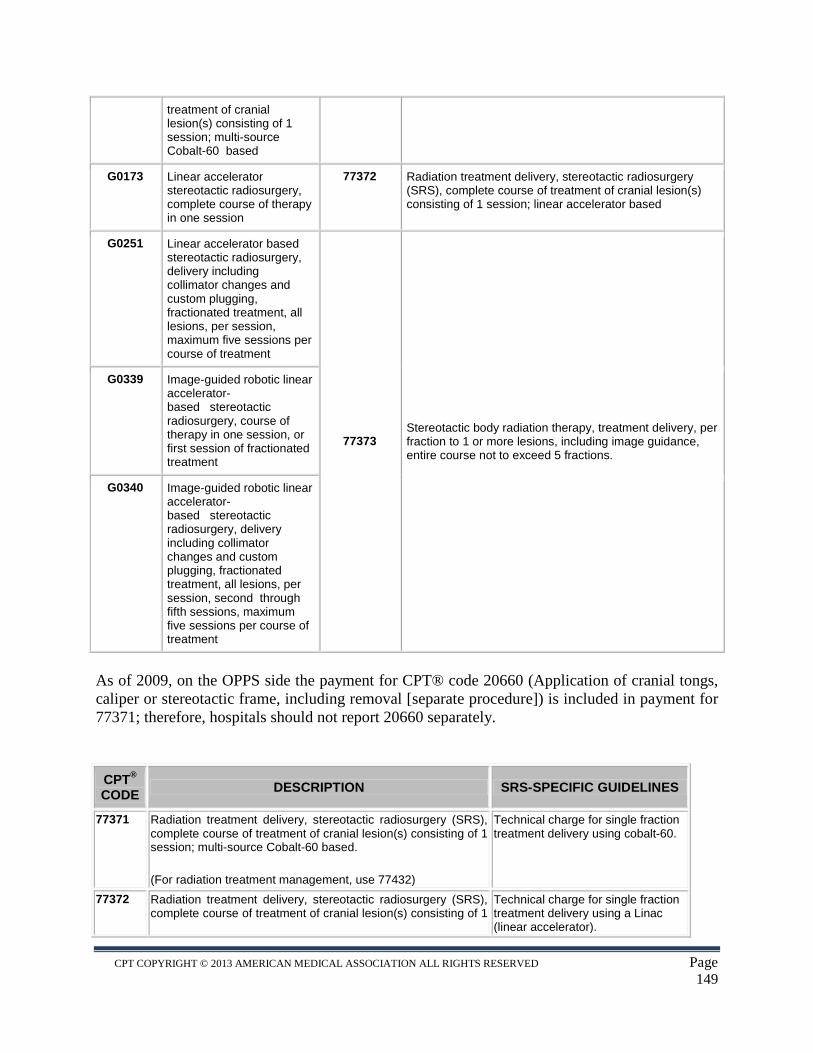
treatment of cranial lesion(s) consisting of 1 session; multi-source Cobalt-60 based
G0173 Linear accelerator stereotactic radiosurgery, complete course of therapy in one session
77372 Radiation treatment delivery, stereotactic radiosurgery (SRS), complete course of treatment of cranial lesion(s) consisting of 1 session; linear accelerator based
G0251 Linear accelerator based stereotactic radiosurgery, delivery including collimator changes and custom plugging, fractionated treatment, all lesions, per session, maximum five sessions per course of treatment
77373 Stereotactic body radiation therapy, treatment delivery, per fraction to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions.
G0339 Image-guided robotic linear accelerator-based stereotactic radiosurgery, course of therapy in one session, or first session of fractionated treatment
G0340 Image-guided robotic linear accelerator-based stereotactic radiosurgery, delivery including collimator changes and custom plugging, fractionated treatment, all lesions, per session, second through fifth sessions, maximum five sessions per course of treatment
As of 2009, on the OPPS side the payment for CPT® code 20660 (Application of cranial tongs, caliper or stereotactic frame, including removal [separate procedure]) is included in payment for 77371; therefore, hospitals should not report 20660 separately.
CPT® CODE DESCRIPTION SRS-SPECIFIC GUIDELINES
77371 Radiation treatment delivery, stereotactic radiosurgery (SRS), complete course of treatment of cranial lesion(s) consisting of 1 session; multi-source Cobalt-60 based.
(For radiation treatment management, use 77432)
Technical charge for single fraction treatment delivery using cobalt-60.
77372 Radiation treatment delivery, stereotactic radiosurgery (SRS), complete course of treatment of cranial lesion(s) consisting of 1
Technical charge for single fraction treatment delivery using a Linac (linear accelerator).
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 149
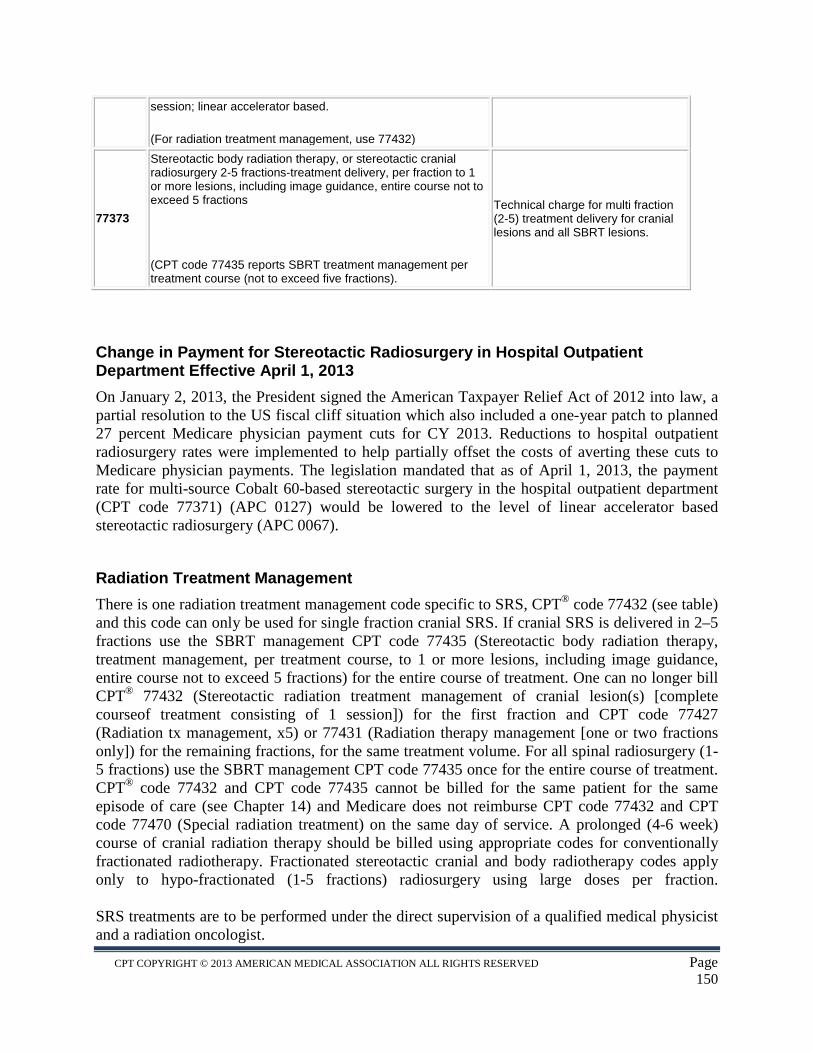
session; linear accelerator based.
(For radiation treatment management, use 77432)
77373
Stereotactic body radiation therapy, or stereotactic cranial radiosurgery 2-5 fractions-treatment delivery, per fraction to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions
(CPT code 77435 reports SBRT treatment management per treatment course (not to exceed five fractions).
Technical charge for multi fraction (2-5) treatment delivery for cranial lesions and all SBRT lesions.
Change in Payment for Stereotactic Radiosurgery in Hospital Outpatient Department Effective April 1, 2013 On January 2, 2013, the President signed the American Taxpayer Relief Act of 2012 into law, a partial resolution to the US fiscal cliff situation which also included a one-year patch to planned 27 percent Medicare physician payment cuts for CY 2013. Reductions to hospital outpatient radiosurgery rates were implemented to help partially offset the costs of averting these cuts to Medicare physician payments. The legislation mandated that as of April 1, 2013, the payment rate for multi-source Cobalt 60-based stereotactic surgery in the hospital outpatient department (CPT code 77371) (APC 0127) would be lowered to the level of linear accelerator based stereotactic radiosurgery (APC 0067).
Radiation Treatment Management There is one radiation treatment management code specific to SRS, CPT® code 77432 (see table) and this code can only be used for single fraction cranial SRS. If cranial SRS is delivered in 2–5 fractions use the SBRT management CPT code 77435 (Stereotactic body radiation therapy, treatment management, per treatment course, to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions) for the entire course of treatment. One can no longer bill CPT® 77432 (Stereotactic radiation treatment management of cranial lesion(s) [complete courseof treatment consisting of 1 session]) for the first fraction and CPT code 77427 (Radiation tx management, x5) or 77431 (Radiation therapy management [one or two fractions only]) for the remaining fractions, for the same treatment volume. For all spinal radiosurgery (1-5 fractions) use the SBRT management CPT code 77435 once for the entire course of treatment. CPT® code 77432 and CPT code 77435 cannot be billed for the same patient for the same episode of care (see Chapter 14) and Medicare does not reimburse CPT code 77432 and CPT code 77470 (Special radiation treatment) on the same day of service. A prolonged (4-6 week) course of cranial radiation therapy should be billed using appropriate codes for conventionally fractionated radiotherapy. Fractionated stereotactic cranial and body radiotherapy codes apply only to hypo-fractionated (1-5 fractions) radiosurgery using large doses per fraction. SRS treatments are to be performed under the direct supervision of a qualified medical physicist and a radiation oncologist.
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 150
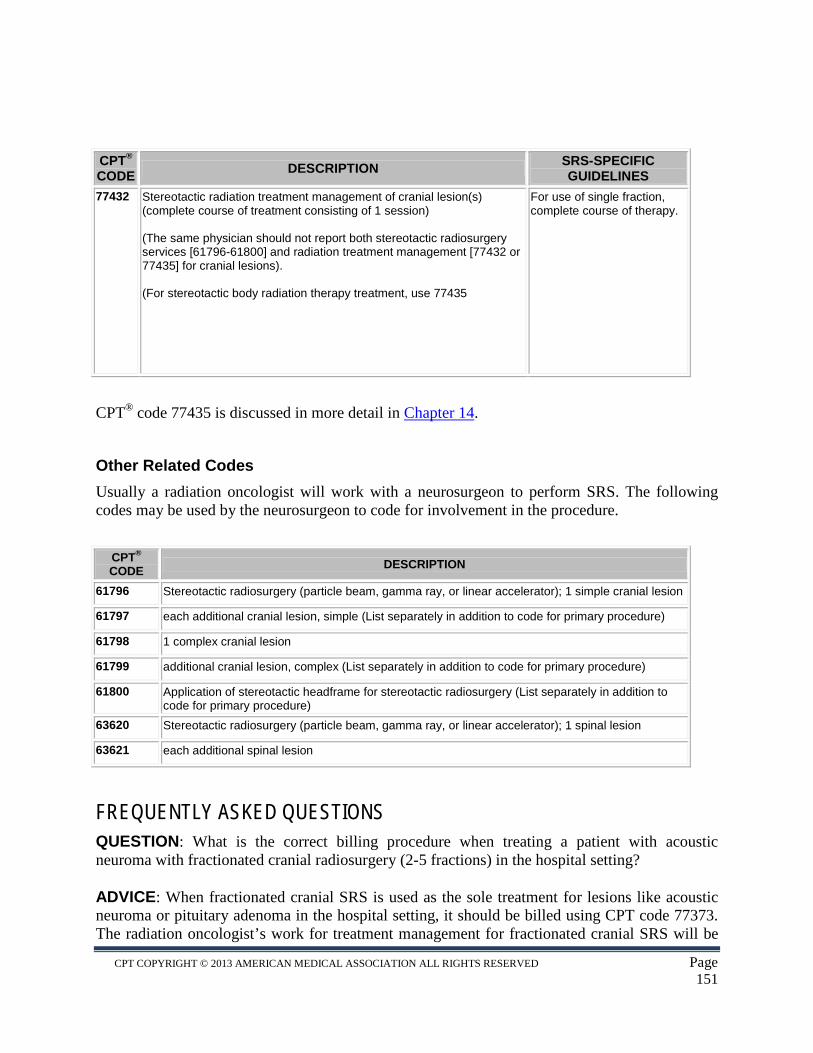
CPT® CODE DESCRIPTION SRS-SPECIFIC
GUIDELINES 77432 Stereotactic radiation treatment management of cranial lesion(s)
(complete course of treatment consisting of 1 session) (The same physician should not report both stereotactic radiosurgery services [61796-61800] and radiation treatment management [77432 or 77435] for cranial lesions). (For stereotactic body radiation therapy treatment, use 77435
For use of single fraction, complete course of therapy.
CPT® code 77435 is discussed in more detail in Chapter 14.
Other Related Codes Usually a radiation oncologist will work with a neurosurgeon to perform SRS. The following codes may be used by the neurosurgeon to code for involvement in the procedure.
CPT® CODE DESCRIPTION
61796 Stereotactic radiosurgery (particle beam, gamma ray, or linear accelerator); 1 simple cranial lesion
61797 each additional cranial lesion, simple (List separately in addition to code for primary procedure)
61798 1 complex cranial lesion
61799 additional cranial lesion, complex (List separately in addition to code for primary procedure)
61800 Application of stereotactic headframe for stereotactic radiosurgery (List separately in addition to code for primary procedure)
63620 Stereotactic radiosurgery (particle beam, gamma ray, or linear accelerator); 1 spinal lesion
63621 each additional spinal lesion
FREQUENTLY ASKED QUESTIONS QUESTION: What is the correct billing procedure when treating a patient with acoustic neuroma with fractionated cranial radiosurgery (2-5 fractions) in the hospital setting?
ADVICE: When fractionated cranial SRS is used as the sole treatment for lesions like acoustic neuroma or pituitary adenoma in the hospital setting, it should be billed using CPT code 77373. The radiation oncologist’s work for treatment management for fractionated cranial SRS will be
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 151

reported with CPT code 77435 for the whole course of treatment, and not with CPT code 77432 or 77427. This only applies to a complete course of radiosurgery treatment for up to five fractions.
QUESTION: How should a provider treat a patient with 4 metastatic brain lesions? Is it appropriate to treat the patient using sequential single-fraction SRS?
ADVICE: For synchronous brain metastases that will be treated with single fraction SRS on Linac-based, the correct code for treatment delivery would be 77372. The code for treatment management is 77432. Each of the 4 lesions is treated fully in a single fraction. Depending on the size and location of some synchronous brain metastases, they may need to be treated with fractionated stereotactic radiosurgery, for which the SBRT codes apply for treatment delivery and radiation oncologist professional codes. The correct code for treatment delivery would be 77373. The code for treatment management is 77435. All of the 4 lesions will be treated fully in up to 5 fractions over a 10 day period.
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 152
84 | C P T C O P Y R I G H T © 2 0 1 3 A M E R I C A N M E D I C A L A S S O C I AT I O N . A L L R I G H T S R E S E R V E D.
14Stereotactic body radiationtherapy (SBRT) describes the delivery of potent doses of radiation using numerous carefully directed fi elds to extracranial sites.
STEREOTACTICS O C CBODYRADIATIONTHERAPY
CHAPTER 14
STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT® CODES 77373, 77435
STEREOTACTIC BODY RADIATION THERAPY (SBRT) describes the delivery of potent doses of radiation using numerous carefully directed fields to extracranial sites.23 It has been considerably difficult translating stereotactic treatments in the brain to treating tumors in the body. The major obstacles to such an approach are related to motion and fixation. Unlike the brain, organ motion in the body is the rule due to breathing and filling or emptying of hollow viscous structures such as bladder and intestines. Using conventionally fractionated (low daily dose) radiation, radiation oncologists identify a "margin" of normal tissue around tumor targets to account for daily variations in the position of the target to avoid missing target portions on any given day. These margins range from 2 to 3 centimeters (cm) depending on the location of the target. SBRT utilizes significantly higher daily doses per fraction, a treatment biologically very different from conventionally fractionated radiation. Wide margins of 2 to 3 cm would result in unacceptable damage to surrounding normal tissue. To successfully accomplish stereotactic treatments outside of the brain with significantly smaller margins, one must utilize a combination of reliable immobilization or repositioning systems, devices capable of decreasing internal organ motion or accounting for organ motion, along with image guidance. SBRT is defined and billed on the basis of the number of fractions employed (total course of therapy consisting of five fractions or less), assuming all other required parameters are met for guidance, precision and medical necessity, and is unrelated to the equipment utilized. The term "robotic" is not limited to any one vendor but rather represents the delivery of SBRT under computer control. The SBRT codes discussed in this chapter are also used to code all spinal stereotactic radiosurgery (SRS) treatments and all cranial SRS treatments given in 2-5 fractions.
The process of care for SBRT has now been established, as SBRT has been performed since the early 1990s and is distinct from conventional radiation therapy. SBRT may be used as an alternative to conventional open surgery for treating various lesions and may be an effective and safer alternative than conventional radiation therapy for certain presentations of cancers and other non-cancer targets. Direct physician involvement, image guidance and immobilization are integral to stereotactic treatment for these diverse body sites.
The medical physicist should perform a second check calculation before initiating the first treatment to ensure the monitor units used to deliver the planned treatment are correct. With a radiation oncologist, the medical physicist should ensure all of the treatment parameters are
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 154
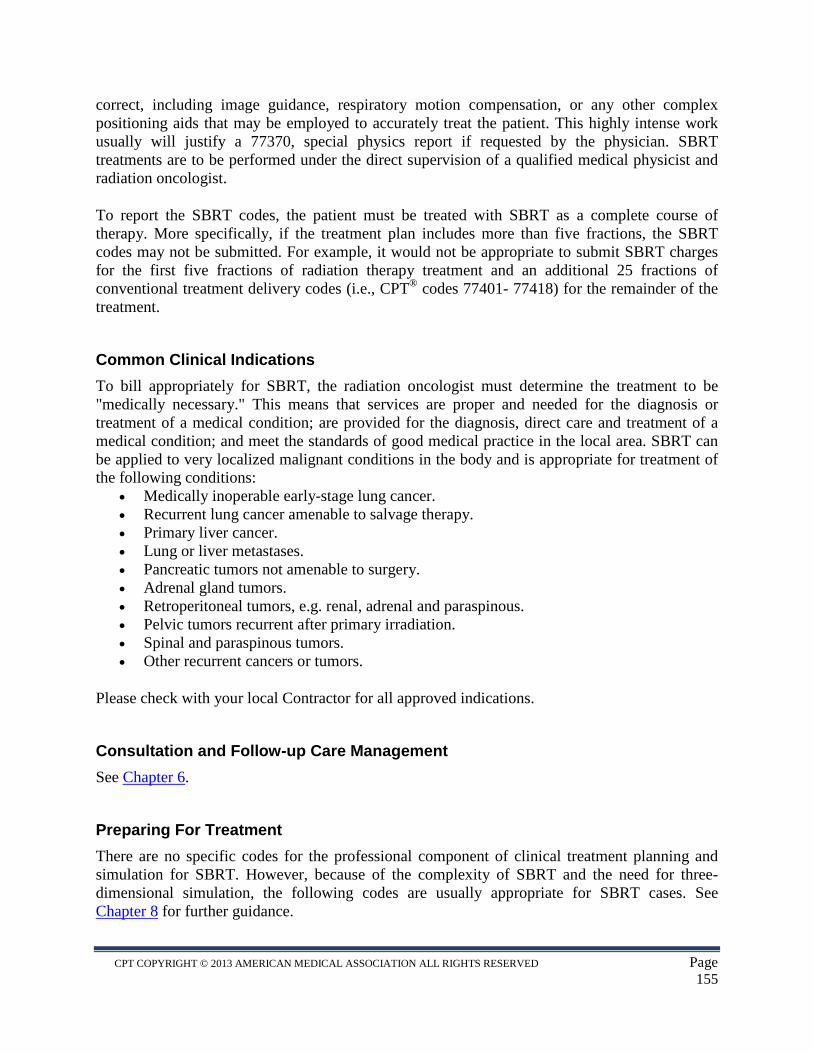
correct, including image guidance, respiratory motion compensation, or any other complex positioning aids that may be employed to accurately treat the patient. This highly intense work usually will justify a 77370, special physics report if requested by the physician. SBRT treatments are to be performed under the direct supervision of a qualified medical physicist and radiation oncologist.
To report the SBRT codes, the patient must be treated with SBRT as a complete course of therapy. More specifically, if the treatment plan includes more than five fractions, the SBRT codes may not be submitted. For example, it would not be appropriate to submit SBRT charges for the first five fractions of radiation therapy treatment and an additional 25 fractions of conventional treatment delivery codes (i.e., CPT® codes 77401- 77418) for the remainder of the treatment.
Common Clinical Indications To bill appropriately for SBRT, the radiation oncologist must determine the treatment to be "medically necessary." This means that services are proper and needed for the diagnosis or treatment of a medical condition; are provided for the diagnosis, direct care and treatment of a medical condition; and meet the standards of good medical practice in the local area. SBRT can be applied to very localized malignant conditions in the body and is appropriate for treatment of the following conditions:
• Medically inoperable early-stage lung cancer. • Recurrent lung cancer amenable to salvage therapy. • Primary liver cancer. • Lung or liver metastases. • Pancreatic tumors not amenable to surgery. • Adrenal gland tumors. • Retroperitoneal tumors, e.g. renal, adrenal and paraspinous. • Pelvic tumors recurrent after primary irradiation. • Spinal and paraspinous tumors. • Other recurrent cancers or tumors.
Please check with your local Contractor for all approved indications.
Consultation and Follow-up Care Management See Chapter 6.
Preparing For Treatment There are no specific codes for the professional component of clinical treatment planning and simulation for SBRT. However, because of the complexity of SBRT and the need for three- dimensional simulation, the following codes are usually appropriate for SBRT cases. See Chapter 8 for further guidance.
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 155
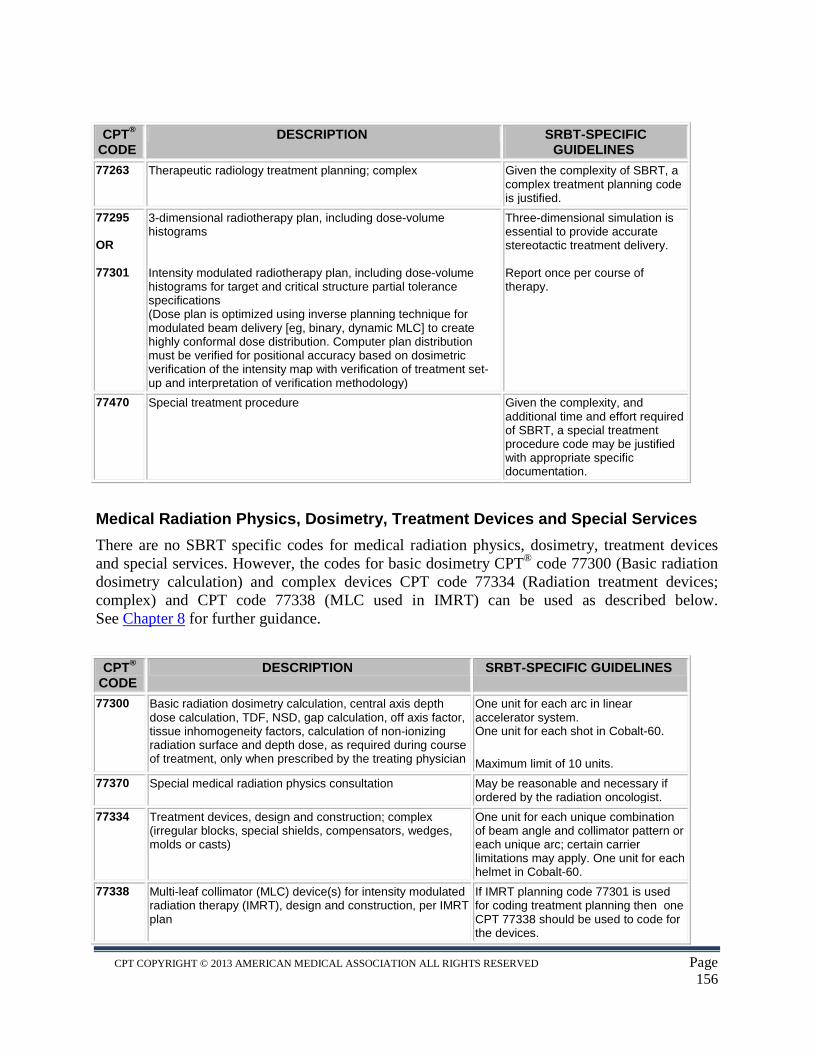
CPT® CODE
DESCRIPTION SRBT-SPECIFIC GUIDELINES
77263 Therapeutic radiology treatment planning; complex Given the complexity of SBRT, a complex treatment planning code is justified.
77295 OR 77301
3-dimensional radiotherapy plan, including dose-volume histograms Intensity modulated radiotherapy plan, including dose-volume histograms for target and critical structure partial tolerance specifications (Dose plan is optimized using inverse planning technique for modulated beam delivery [eg, binary, dynamic MLC] to create highly conformal dose distribution. Computer plan distribution must be verified for positional accuracy based on dosimetric verification of the intensity map with verification of treatment set-up and interpretation of verification methodology)
Three-dimensional simulation is essential to provide accurate stereotactic treatment delivery. Report once per course of therapy.
77470 Special treatment procedure Given the complexity, and additional time and effort required of SBRT, a special treatment procedure code may be justified with appropriate specific documentation.
Medical Radiation Physics, Dosimetry, Treatment Devices and Special Services There are no SBRT specific codes for medical radiation physics, dosimetry, treatment devices and special services. However, the codes for basic dosimetry CPT® code 77300 (Basic radiation dosimetry calculation) and complex devices CPT code 77334 (Radiation treatment devices; complex) and CPT code 77338 (MLC used in IMRT) can be used as described below. See Chapter 8 for further guidance.
CPT®
CODE DESCRIPTION SRBT-SPECIFIC GUIDELINES
77300 Basic radiation dosimetry calculation, central axis depth dose calculation, TDF, NSD, gap calculation, off axis factor, tissue inhomogeneity factors, calculation of non-ionizing radiation surface and depth dose, as required during course of treatment, only when prescribed by the treating physician
One unit for each arc in linear accelerator system. One unit for each shot in Cobalt-60.
Maximum limit of 10 units. 77370 Special medical radiation physics consultation May be reasonable and necessary if
ordered by the radiation oncologist. 77334 Treatment devices, design and construction; complex
(irregular blocks, special shields, compensators, wedges, molds or casts)
One unit for each unique combination of beam angle and collimator pattern or each unique arc; certain carrier limitations may apply. One unit for each helmet in Cobalt-60.
77338 Multi-leaf collimator (MLC) device(s) for intensity modulated radiation therapy (IMRT), design and construction, per IMRT plan
If IMRT planning code 77301 is used for coding treatment planning then one CPT 77338 should be used to code for the devices.
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 156
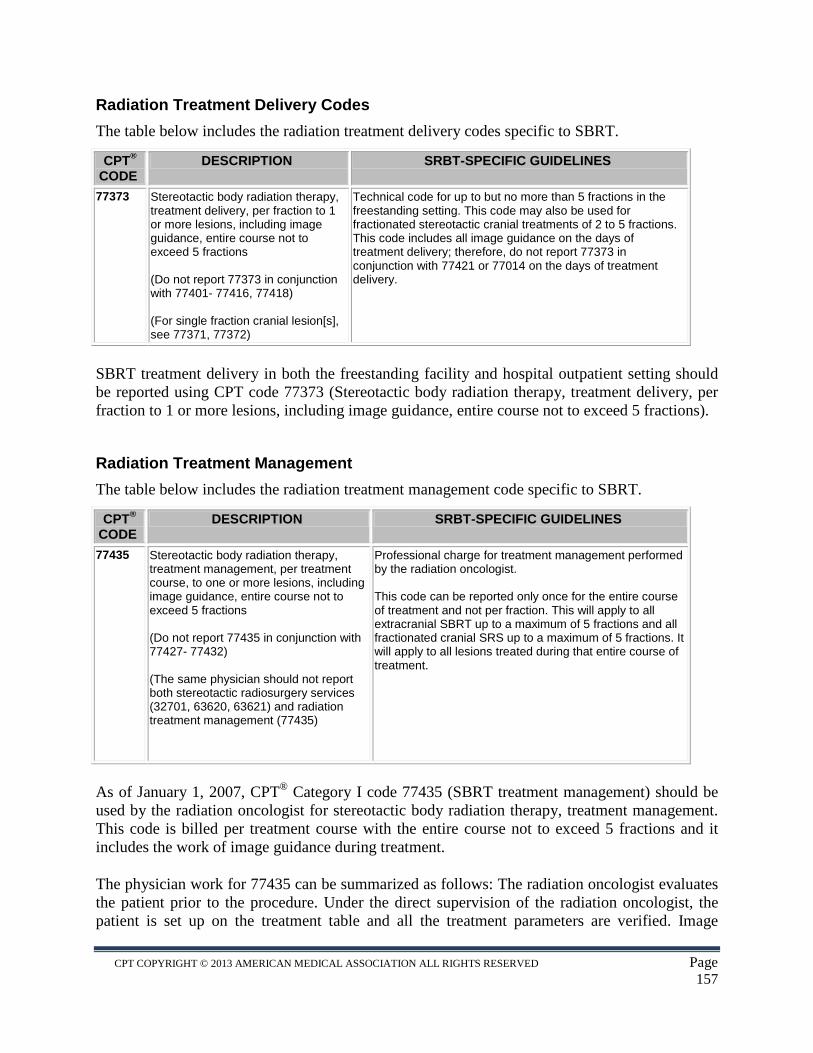
Radiation Treatment Delivery Codes The table below includes the radiation treatment delivery codes specific to SBRT.
CPT® CODE
DESCRIPTION SRBT-SPECIFIC GUIDELINES
77373 Stereotactic body radiation therapy, treatment delivery, per fraction to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions (Do not report 77373 in conjunction with 77401- 77416, 77418) (For single fraction cranial lesion[s], see 77371, 77372)
Technical code for up to but no more than 5 fractions in the freestanding setting. This code may also be used for fractionated stereotactic cranial treatments of 2 to 5 fractions. This code includes all image guidance on the days of treatment delivery; therefore, do not report 77373 in conjunction with 77421 or 77014 on the days of treatment delivery.
SBRT treatment delivery in both the freestanding facility and hospital outpatient setting should be reported using CPT code 77373 (Stereotactic body radiation therapy, treatment delivery, per fraction to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions).
Radiation Treatment Management The table below includes the radiation treatment management code specific to SBRT.
CPT® CODE
DESCRIPTION SRBT-SPECIFIC GUIDELINES
77435 Stereotactic body radiation therapy, treatment management, per treatment course, to one or more lesions, including image guidance, entire course not to exceed 5 fractions (Do not report 77435 in conjunction with 77427- 77432) (The same physician should not report both stereotactic radiosurgery services (32701, 63620, 63621) and radiation treatment management (77435)
Professional charge for treatment management performed by the radiation oncologist. This code can be reported only once for the entire course of treatment and not per fraction. This will apply to all extracranial SBRT up to a maximum of 5 fractions and all fractionated cranial SRS up to a maximum of 5 fractions. It will apply to all lesions treated during that entire course of treatment.
As of January 1, 2007, CPT® Category I code 77435 (SBRT treatment management) should be used by the radiation oncologist for stereotactic body radiation therapy, treatment management. This code is billed per treatment course with the entire course not to exceed 5 fractions and it includes the work of image guidance during treatment.
The physician work for 77435 can be summarized as follows: The radiation oncologist evaluates the patient prior to the procedure. Under the direct supervision of the radiation oncologist, the patient is set up on the treatment table and all the treatment parameters are verified. Image
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 157
guidance, and respiratory correlation if required, may be achieved through a variety of methods, all of which are supervised, corrected and approved in real time by the physician. The physician assesses and approves all of the ongoing images used for localization, tumor tracking, any gating application, as well as any complementary single (beam's eye) view localization images for any of the fields or arcs that are arranged to deliver a dose. The radiation oncologist remains available throughout SBRT treatment to manage the execution of the treatment and make real-time adjustments in response to patient motion, target movement, or equipment issues to ensure accuracy and safety. The physician also evaluates the patient post-procedure. All other work generally associated with CPT code 77427 (Radiation treatment management, five treatments) is included and should not be separately coded.
Much of the radiation oncologist's work in establishing the above treatment parameters is performed in conjunction with the qualified medical physicist, who should be present and participate in delivering SBRT treatment.
FREQUENTLY ASKED QUESTIONS QUESTION: What are the appropriate and/or reasonable units of service for CPT 77300 for an SBRT case? ADVICE: The radiation dose per field is routinely independently calculated and verified before the course of radiation treatment, and reported using CPT code 77300. Some systems may use a dataset of 100 - 200 beams to treat a lesion and many of them may undergo independent calculations to ensure accuracy for the patient treatment. A proportion of the beams may have a variance of over 10 percent on independent calculations and these may be evaluated by the physician for assessing the dose contribution from these beams. ASTRO does not recommend that all 100 – 200 beams be billed individually as a separate CPT 77300 charge. While more may be medically indicated under certain circumstances, the American Society for Radiation Oncology does not recommend routinely coding CPT code 77300 more than ten times per course when using SBRT.
CPT COPYRIGHT © 2013 AMERICAN MEDICAL ASSOCIATION ALL RIGHTS RESERVED Page 158