Embed Size (px)
Citation preview

Judicious Use of Anticoagulation: A Case-Based Approach
Michael B. Streiff, MD, FACPAssociate Professor of Medicine and Pathology
Division of HematologyMedical Director, Johns Hopkins Anticoagulation
Management Service and Outpatient Clinics

Disclosures
• Research Funding– Bristol-Myers Squibb– NIH/NHLBI
• Consulting– Sanofi-aventis– Eisai, Inc. – Daiichi-Sankyo– Janssen Healthcare– BiO2
• Speaking Honoraria– Sanofi-aventis– Ortho-McNeil
• Educational Grants– Sanofi-Aventis– Covidien

Anticoagulation for pregnancy loss
• 32 year old woman with 2 previous first trimester pregnancy losses asks about LMWH to prevent miscarriages. You advise her to – Start therapeutic dose LMWH– Start prophylactic dose LMWH– Start prophylactic dose LMWH + Aspirin 100 mg– Start no antenatal prophylaxis

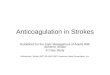
LMWH does not improve pregnancy outcomes: The ALIFE Study
Placebo (N=121)
Aspirin 80 mg (N=120)
Aspirin 80 mg + Nadroparin 2850 IU(N=123)
Completed Study (N=103)
Completed Study (N=97)
Completed Study (N=99)
364 women with at least 2pregnancylosses
Kaandorp S et al. NEJM 2010

Baseline characteristics
Characteristic Aspirin + LMWH (N=123)
Aspirin (N=120)
Placebo (N=121)
Age (yrs.) 34±5 33±5 34±5
Previous miscarriages
3 (2-15) 3 (2-9) 3 (2-12)
≥ 3 miscarriages 73 (59%) 71 (59%) 74 (61%)
≥ 1 late losses 40 (33%) 38 (32%) 35 (29%)
Previous live birth 53 (43%) 45 (38%) 46 (38%)
Thrombophilia 13 (12%) 17 (17%) 17 (17%)
Kaandorp S et al. NEJM 2010

LMWH did not increase the live birth rate
Kaandorp S et al. NEJM 2010

Thrombophilia did not affect live birth rate
Nadroparin + ASA
ASA Placebo0
10
20
30
40
50
60
70
8069.2
64.7
52.948.9
58.5 58
ThrombophiliaNo Thrombophilia
Live
Bir
th R
ate
(%)
Kaandorp SP et al. NEJM 2010

Anticoagulation does not prevent early pregnancy loss
• Open-label RCT of enox 40 mg/d + ASA 75 mg vs. surveillance alone
• PMHx ≥ 2 losses 24 weeks or less
• Begin 7 weeks gestation or less
• Conclusion- Prophylactic AC does not improve pregnancy outcomes
Pregnancy loss Bleeding0
5
10
15
20
25
20
15.6
22
16
Surveillance aloneEnox 40 + ASA
Adv
erse
Eve
nts
(%)
N=294
Clark P et al. Blood 2010

Heparin + Aspirin reduces pregnancy loss in Antiphospholipid Syndrome
• Metanalysis of 5 RCTs of UFH/LMWH + aspirin versus aspirin
• Regimens- UFH 5000-20000 units + aspirin 75-81 mg and LMWH 5000 + aspirin 75-81 mg
• Conclusion- UFH/LMWH + ASA improves live birth rates Live Birth
0
10
20
30
40
50
60
70
80
55.8
74.3
Aspirin (N=163)UFH/LMWH + ASA (N=171)
Live
Bir
ths
(%)
Mak A et al. Rheumatol 2010
RR 1.3

Anticoagulation- Less or More?
• A 65 year old man with a St Jude aortic valve is scheduled to undergo a prostatectomy for cancer. When should he resume full-dose anticoagulation?– 12 hours post-op– 24 hours post-op– 36 hours post-op– 72 hours post-op

Perioperative AC- Is less more?
• Metanalysis of 34 studies of 12,278 patients
• Outcomes- Thromboembolism and Bleeding
• Limitation- Lack of RCT• Conclusion- Value of
perioperative bridging unclear Bleeding Thrombosis
0
2
4
6
8
10
12
14
1613.6
0.4
8.5
0.2
3.4
0.6
Full Dose Prophy DoseNo Bridge
Patie
nts
(%)
Siegal D et al. Circulation 2012

Less is more for perioperative AC
• Prospective Cohort of 1262 patients
• Low risk- AVR w/o Afib-prophylactic LMWH
• High risk- MVR, AVR w/Afib or stroke- Enox 0.7 mg/kg q12h
• Post-op- resume AC day 1-3 based upon hemostasis Thrombosis Major Bleed
0
0.5
1
1.5
2
2.5
3
1.7
2.7
0
0.700000000000001
High TE risk Low TE risk
Pengo V et al. Circulation 2009

Thromboembolism Risk Stratification Thromboembolic Risk
Atrial Fibrillation Mechanical Valve Venous Thromboembolism
High CHADS2 score 5 or 6 Any Mitral valveOlder valve (Caged-ball, Tilting disk)Recent stroke/TIA
Recent (within 3 mos.) VTESevere thrombophilia
Intermediate CHADS2 score 3 or 4 Bileaflet Aortic valve + TE risk factors
VTE within 3-12 mos.Recurrent VTE, Active CancerNon-severe thrombophilia
Low CHADS2 score 0-2 Bileaflet Aortic valve w/o TE risk factors
VTE > 12 mos.
TE risk factors= A fib, Cardiac failure, HTN, DM, Age > 75, Stroke/TIADouketis JD Blood 2011

Bleeding Risk Assessment Low Bleeding Risk Procedures High Bleeding Risk Procedures
CholecystectomyAbdominal hysterectomyGI Endoscopy ± biopsy or stentPacemaker insertion, EP testingDental extractionsCarpal tunnel repairDilatation/currettageSkin Cancer excisionAbdominal herniaHydrocele repairCataract surgeryBronchoscopy ± biopsy Central Venous Catheter removalSkin, Thyroid, Breast, Lymph node biopsy
Cardiac surgeryAbdominal aneurysm repairNeurosurgeryUrologic surgeryHead and Neck surgeryHip/knee replacementBack surgeryKidney biopsyPolypectomy/sphincterotomyTransurethral prostate resection General surgeryVascular surgeryAny major surgery (> 45 minutes)
Spyropoulos AC and Douketis JD Blood 2012

AC Management
Surgical Bleeding risk Pre-operation Post-operation
Low Last dose LMWH 24 hours before
Resume LMWH 24 hours post-op if hemostasis adequateStart warfarin with LMWH
High Last dose LMWH 24 hours before
Resume LMWH 48-72 hours post-op if hemostasis adequate or start prophylactic dose 24 hours post-op or avoid LMWHStart warfarin with LMWH

Anticoagulation for VTE• 65 year old man develops a right femoral-
popliteal vein DVT 1 week after right knee replacement. A thrombophilia evaluation reveals he is heterozygous for the factor V Leiden mutation. How long should he be treated?– 6 weeks– 3 months– 12 months– Indefinite

Anticoagulation for VTE
• 48 year old man presents with progressive dyspnea over 1 week and left leg discomfort. CT angiogram identifies bilateral PE. Duplex study finds a left leg DVT. No VTE risk factors are identified. How long should he be treated?– 3 months– 6 months– 12 months– Indefinite

Do the Results of Thrombophilia Tests Help to Determine Duration of Therapy?
Baglin, 2003 Christiansen, 2005 Santamaria 2005 Prandoni 20070
5
10
15
20
25
30
35
40
45
Thrombophilia No thrombophilia
HR 1.5 (0.8-2.8)
(N= 570)24 mos.
(N=474)84 mos.
(N=267)46 mos.
(N=1626)50 mos.
HR 1.4 (0.9-2.2)
HR 1.8 (1-3.1)
HR 2.0 (1.5-2.7)
Rec
urre
nt V
TE
(%
)

Thrombophilia-Assessing the risk
• High risk thrombophilia– Antithrombin deficiency - 1.8 % per year (95% CI 1.1-2.6%)– Protein C deficiency - 1.5% per year (1.1-2.1%)– Protein S deficiency - 1.9% per year (1.3-2.6%)
• Moderate risk thrombophilia– Factor V Leiden - 0.5% per year (0.4-0.6%)– Prothrombin gene mutation - 0.3% per year (0.2-0.5%)– Factor VIII - 0.5% per year (0.4-0.5%)
• Low risk thrombophilia– Factor IX - 0.1% per year (0.02-0.2%)– Factor XI - 0.2% per year (0.06-0.6%)– Hyperhomocysteinemia – 0.1% per year (0.05-0.3%)
Lijfering WM et al. Blood 2009

Antiphospholipid syndrome is associated with recurrent thromboembolism
0 6 12 18 24 30 36 42 480
5
10
15
20
25
30
35
ACL - ACL +
Rec
urre
nt V
TE
(%
)
Months
Schulman S , et al. Am J Med 1998; 104: 332-338
P=0.0013

VTE recurrence rate varies depending upon initial trigger for the event
0 4 8 12 16 20 240
5
10
15
20
25
Recent surgery Non-surgical risk factor Idiopathic
Time after cessation of therapy (months)
Cum
ulat
ive
recu
rren
t VT
E (
%)
Baglin T et al., Lancet 2003
N = 570

VTE Setting influences recurrence risk
• Systematic review of prospective cohort studies and RCTs
• 15 Studies• 5159 Subjects• Follow up- 3-96 months• Conclusion- Setting of
thrombosis strongly influences recurrence rate
Surgi
cal tr
igger
Non-surgi
cal tr
igger
Idiopathic
012345678
0.700000000000001
4.2
7.4
Recu
rren
t VTE
(% p
er p
at.-y
r)
Iorio A et al. Arch Intern Med 2010

D dimer and recurrent VTE
• D dimer- an indirect marker of activated coagulation
• PROLONG study (Palareti G et al. NEJM 2006)
– F/U 1.4 years• Systematic Review (Verhovsek M
et al. Ann Intern Med 2008)
– 7 studies, 1888 patients– Recurrent VTE- Abnl vs.
nl DD (8.9% vs. 3.5% per year)
N=608

How do we identify the low risk patient with idiopathic VTE?
• Prospective cohort study of 665 patients with idiopathic VTE– Enrolled at 12 centers, 4 countries prior to DC of warfarin after 5-7
months of therapy– Information of 76 laboratory and clinical variables associated with VTE
were collected– Multivariate analysis used to develop clinical prediction rule for
recurrent VTE• Results
– F/U population 600/665 (90%)– Mean F/U -18 months (1-47 mos.)– Annual risk of recurrent VTE 9.3% per year (7.7%-11.3%)
• Men 13.7% (10.8%-17%)• Women 5.5% (3.7%-7.8%)
Rodger MA, et al. CMAJ 2008;179(5):417-26

Clinical prediction rule for recurrent VTE in women
Rodger MA, et al. CMAJ 2008;179(5):417-26

Risk stratification for idiopathic VTE: The Vienna Risk Model
Eichinger S et al. Circulation 2010
0 12 24 36 48 60 72 84 96108
12005
10152025303540
Months after discontinuation of anticoagula-tion
VTE
(%)
http://www.meduniwien.ac.at/user/georg.heinze/zipfile/ViennaPredictionModel.html

Indefinite Anticoagulation: Weighing the risks
Thrombosis Bleeding

Assessing Bleeding Risk: The HAS-BLED Score
• HASBLED– Hypertension (uncontrolled
SBP>160) = 1 point– Abnormal renal/liver function
= 1 or 2 points– Stroke = 1 point– Bleeding (or anemia) = 1
point– Labile INRs (TTR<60%)= 1
point– Elderly (Age > 65 years)= 1
point– Drugs or alcohol= 1 or 2
points
Low (0
-1 pt.)
Intermediat
e (2-3 pts.
)
High (4
+)0123456789
2.66
5.54
8.11
Maj
or B
leed
(per
100
pt.-
yrs.
)
N=44,771
Pisters R et al. Chest 2010; Olesen JB, et al. JTH 2011

Central Venous Catheter Prophylaxis
• 67 year old man has just had a right subclavian Hickman CVC placed for chemotherapy for recently diagnosed NHL. What should be used for CVC thrombosis prophylaxis?– Warfarin 1 mg daily– Enoxaparin 40 mg daily– Dalteparin 5000 units daily– No prophylaxis necessary

CVC Prophylaxis
• Open RCT of low dose warfarin 1 mg vs. no warfarin
• Start 3 days before CVC insertion
• Outcome-Venogram with symptoms or at 90 days
• Conclusion- Low dose warfarin prevents CVC thrombosis
0 10 20 30 40 50 60 70 80 900
5
10
15
20
25
30
35
40
Warfarin No Warfarin
Days
Veno
us T
hrom
bosi
s (%
)
Bern MM et al. Ann Intern Med 1990
P<0.001

Catheter ProphylaxisStudy Regimen Outcome
assessmentDVT (%) P Value
Bern et al. 1990
Warfarin 1 mgNo treatment
Venogram 9.537.5
<0.001
Monreal et al. 1996
Dalteparin 2500 No treatment
Venogram 662
0.002
Reichardt et al. 2002
Dalteparin 5000No treatment
Clinical 3.73.4
0.9
Couban et al. 2003
Warfarin 1 mgPlacebo
Clinical 4.64
0.81
Verso et al. 2004
Enoxaparin 40 mgPlacebo
Venogram 14.118
0.35

0 1 2 3 4 5 6 7 8 9 1011120
2
4
6
8
10
12
14
16
Fixed-dose Dose-adjusted
Time from randomization (mos.)
Thro
mbo
sis
(%)
P=0.002
Young AM, et al. Lancet 2009
• A multicenter (N=68) open label study of warfarin CVC prophylaxis (N=1590)
• Study Arms-– No warfarin (404) vs. warfarin
1 mg (408)– Warfarin 1 mg (471) vs.
warfarin (INR1.5-2.0) ( 473)
• Conclusion- Dose-adjusted warfarin is required to prevent CVC DVT
Adjusted dose warfarin prevents CVC thrombosis: WARP study

Elevated INR- Less vitamin K is more
• 70 year old man taking warfarin for atrial fibrillation has an INR of 7. He does not have any signs of bleeding. What should you do?– Hold warfarin and administer vitamin K 2.5 mg po– Hold warfarin and administer vitamin K 2.5 mg IV– Hold warfarin and recheck INR in 1-2 days– Hold warfarin and administer Vitamin K 2.5 mg
and 3 units of FFP

Less vitamin K is more safe
• RCT of vitamin K 1.25 mg or placebo for pts. with INR 4.5-10
• Setting- 14 AC clinics in US, Canada, Italy
• Outcomes- Symptomatic bleeding or thromboembolism within 90 days
• Conclusion- Oral Vit K does not improve outcomes with INR 4.5-10
Bleeding Major Bleed
TE Death02468
1012141618 16.3
1.1
4
1.9
15.8
2.5 32
Placebo (N=369)Vitamin K 1.25mg (N=355)
Crowther MA et al. Ann Intern Med 2009

Is less is more?
• 72 year old man with atrial fibrillation who has been on warfarin 5 mg daily for 3 months. Today his INR is 1.8. No reason identified. What should you do with his warfarin dose?– Increase his dose to 7.5 mg MWF, 5 mg ROW (21% dose
increase), recheck 1 week– Increase his dose to 7.5 mg daily (50% dose increase),
recheck 1 week– Increase his dose to 7.5 mg W, 5 mg ROW (7% dose
increase, recheck 1 week– Continue same dose, recheck 1 week

Less dose adjustment=more time in range
• Observational study of warfarin management
• Setting- 94 AC clinics, 3961 patients
• Outcome- Time in therapeutic range
• Conclusion- Excessive warfarin dose changes lead to poorer INR control
INR 2-3 INR 1.9-3.1
INR 1.8-3.2
INR 1.7-3.3
62
64
66
68
70
72
74
76
67
69
74
71
INR Target Range
Tim
e in
ther
apeu
tic ra
nge
(%)
Rose AJ et al. J Thromb Haemost 2009

Is less LMWH more?
• A 65 year old man with an atrial fibrillation (CHADS2 score 3) who has been on warfarin for 4 months has an INR of 1.5. Your nurse asks you for advice. You suggest…– LMWH + warfarin dose increase– Warfarin dose increase only

Less LMWH is safe
• Retrospective study of patients in Kaiser CO AC clinics
• Low INR and therapeutic INR groups
• Only 13 patients received LMWH
• Outcomes- Bleeding and TE at 90 days
• Conclusion- LMWH not necessary for most patients with low INR
Thrombosis
Bleeding Death0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
0.4
1.5
0.20.1
0.8
0.2
Low INR (N=1080)Therapeutic INR (N=1517)
Patie
nts
(%)
Clark NP et al. Pharmacother 2008

Conclusions
• Anticoagulation is not indicated for recurrent early pregnancy loss except perhaps APS
• Therapeutic AC should be used sparingly in the post-operative period
• Setting rather than presence of thrombophilia dictates duration of therapy
• Risk stratification models can help determine the risk of recurrent VTE and bleeding in patients with idiopathic VTE
• Central venous catheter prophylaxis remains of unproven benefit
• Studies continue to optimize warfarin management

Questions ?