Embed Size (px)
Citation preview

FEDERAL HEALTH REPORTING JOINT SERVICE BY RKI AND DESTATIS
Journal of Health Monitoring
Establishment of a migration-sensitive health monitoring at the Robert Koch Institute – Results of the IMIRA project
SEPTEMBER 2019ISSUE 3
1

Journal of Health Monitoring Index
Journal of Health Monitoring 2019 4(3)
Establishment of a migration-sensitive health monitoring at the Robert Koch Institute – Results of the IMIRA project
3 Editorial Health monitoring should reflect population diversity
7 Focus The health of children and adolescents with a migration background in Germany – Results of the cross-sectional KiGGS Wave 2 study
29 Concepts & Methods Health reporting on people with a migration background – Selection and definition of (core) indicators
49 Concepts & Methods Concepts for migration-sensitive health monitoring
2

Journal of Health Monitoring EDITORIAL
3
Editorial: Health monitoring should reflect population diversity
Journal of Health Monitoring 2019 4(3)
Journal of Health Monitoring · 2019 4(3) DOI 10.25646/6072Robert Koch Institute, Berlin
Bärbel-Maria Kurth 1, Oliver Razum 2
1 Robert Koch Institute, Berlin 2 Bielefeld University
Submitted: 15.08.2019 Accepted: 20.08.2019 Published: 18.09.2019
yet been able to provide reliable data on people with a migration background, a problem largely due to the small number of cases. In the German Health Interview and Examination Survey for Adults (DEGS1), people with a migration background were not sufficiently included [4]. As a result, the Improving Health Monitoring in Migrant Populations (IMIRA) project was initiated in 2016 with the aim of both expanding health monitoring at the Robert Koch Institute to include people with a migration background and further developing health reporting on migration and health. The IMIRA project will be concluded at the end of 2019 [5].
In this issue of the Journal of Health Monitoring, we provide results from the IMIRA project with a focus on the expansion of health reporting. The first article presents The health of children and adolescents with a migration back-ground in Germany. The second article, Health reporting on people with a migration background – Selection and definition of (core) indicators, describes the process of developing a set of (core) indicators and its results. This article is the conceptional basis for the selected indicators in the focus article.
The third article in this issue, Concepts for migra-tion-sensitive health monitoring, focuses on the further development and review of relevant migration-related con-cepts (e.g. acculturation and discrimination). The primary aim here is to better assess and depict the diversity of the German resident population in the long-term, thereby also advancing health research in the context of migration.
Editorial: Health monitoring should reflect population diversity
Germany is a migration country. In 2018, 23.6% of the pop-ulation had a migration background [1], which means that they, or at least one of their parents, were born without German citizenship. People with a migration background are heterogeneous in regard to their opportunities, their socioeconomic situation, their language skills, the reasons they migrated to Germany and their healthcare needs. Any analysis of migration and health must be sure to take these factors into account.
The Robert Koch Institute (RKI) is currently expanding its health monitoring activities, which have been developed over the last few years, and its health reporting system, which has been established for many years. People with a migration background should be included in national health surveys according to their proportion of the popu-lation in order to enable representative statements on their health status. Here, accounting for the diversity of people with a migration background and simultaneously ensuring comparability of different data sources presents a signifi-cant challenge.
The inclusion of people with a migration background in the health surveys conducted by the RKI has been suc-cessful in the context of both the baseline study of the Ger-man Health Interview and Examination Survey for Children and Adolescents (KiGGS) and its follow-up KiGGS Wave 2 due to the application of specific measures [2, 3]. To date, this has been implemented only partial in regards to the adult population. The German Health Update (GEDA), for example, which is conducted at regular intervals, has not

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
Editorial: Health monitoring should reflect population diversityJournal of Health Monitoring EDITORIAL
4
within the research and reporting process helps to increase both the understanding of potential barriers and reserva-tions and the ability to face them.
The upcoming nationwide interview and examination survey for adults, the Health and Nutrition Survey in Ger-many (gern survey), which will be conducted by the Robert Koch Institute in cooperation with the Max Rubner Insti-tute in 2020, aims to apply the insights gained from the IMIRA project on how to better reach people with a migra-tion background. It is also essential for the future develop-ment of health monitoring that these factors will be taken into account and be continuously developed, in order to do justice to the diversity of the German pop ulation and adequately reflect the health of all people living in Germany. We hope that the findings presented in this issue will be of use to other studies in the future, and we appreciate your interest.
Corresponding authorDr Bärbel-Maria KurthRobert Koch Institute
Department of Epidemiology and Health MonitoringGeneral-Pape-Str. 62–66 D-12101 Berlin, Germany
E-mail: [email protected]
Please cite this publication asKurth BM, Razum O (2019)
Editorial: Health monitoring should reflect population diversity. Journal of Health Monitoring 4(3): 3-6.
DOI 10.25646/6072
The German version of the article is available at: www.rki.de/journalhealthmonitoring
As well as further developing health reporting and the content-related concepts used in surveys, the IMIRA pro-ject has developed strategies to works towards the long-term inclusion of people with a migration background into health monitoring. For this, two feasibility studies were conducted to test innovative approaches to recruiting par-ticipants for interview surveys and overcoming language barriers in examination surveys [5, 6]. The results confirm [7, 8] that multilingual materials and face-to-face interviews are very helpful when trying to improve the inclusion of hard-to-reach populations. The response rates among peo-ple with limited German-language skills in examination surveys can be increased with the utilisation of a video interpreting service and multilingual information videos.
The insights presented in the articles of this issue, and the findings from the feasibility studies, allow us to iden-tify the following factors as fundamental to a diversity- oriented health monitoring: Firstly, the use of multilingual and diversity-sensitive materials is important as is the pro-vision of different data collection formats, e.g. online, in writing, or face-to-face interviews. Personal contact is very effective in increasing the response rates of people with a migration background in order to motivating them to participate in a study or also to conduct an interview. Language mediation via a video interpreting service is a practical way to overcome language barriers during exam-ination surveys. Increasing diversity-sensitivity in staff train-ing sessions, in the development of materials and in the identification of relevant concepts is essential to establish-ing responsible and discrimination-free health reporting on migration and health. Actively engaging people with a migration background either as staff or as external advisers

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
Editorial: Health monitoring should reflect population diversityJournal of Health Monitoring EDITORIAL
5
Conflicts of interestBärbel-Maria Kurth leads the KiGGS study. Oliver Razum is chairman of the Advisory Board of the IMIRA project.
References 1. Statistisches Bundesamt (2018) Bevölkerung und Erwerbstätig-
keit. Bevölkerung mit Migrationshintergrund – Ergebnisse des Mikrozensus 2017. Fachserie 1 Reihe 2.2. Destatis, Wiesbaden
2. Schenk L, Neuhauser H, Ellert U (2008) Kinder- und Jugend-gesundheitssurvey (KiGGS) 2003 – 2006: Kinder und Jugend-liche mit Migrationshintergrund in Deutschland. Beiträge zur Gesundheitsberichterstattung des Bundes. RKI, Berlin. https://edoc.rki.de/handle/176904/3215 (As at 15.07.2019)
3. Frank L, Yesil-Jürgens R, Born S et al. (2018) Improving the inclu-sion and participation of children and adolescents with a migra-tion background in KiGGS Wave 2. Journal of Health Monitoring 3(1):126-142. https://edoc.rki.de/handle/176904/5640 (As at 15.07.2019)
4. Saß AC, Grüne B, Brettschneider AK (2015) Beteiligung von Men-schen mit Migrationshintergrund an Gesundheitssurveys des Robert Koch-Instituts. Bundesgesundheitsbl 58(6):533-542. https://edoc.rki.de/handle/176904/2385 (As at 15.07.2019)
5. Santos-Hövener C, Schumann M, Schmich P et al. (2019) Improving the information base regarding the health of people with a migration background. Project description and initial find-ings from IMIRA. Journal of Health Monitoring 4(1):46-57. https://edoc.rki.de/handle/176904/5915 (As at 15.07.2019)
6. Zeisler L, Lemcke J, Bilgic L et al. (2019) Integration of Migrant Populations into Health Monitoring in Germany: Results from a Feasibility Study. Survey Methods: Insights from the Field. https://surveyinsights.org/?p=10780 (As at 15.07.2019)
7. Brand T, Samkange-Zeeb F, Dragano N et al. (2019) Participation of Turkish Migrants in an Epidemiological Study: Does the Recruitment Strategy Affect the Sample Characteristics? J Immigr Minor Health 21:811-819
8. Reiss K, Dragano N, Ellert U et al. (2014) Comparing sampling strategies to recruit migrants for an epidemiological study. Results from a German feasibility study. Eur J Public Health 24:721-726

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
Editorial: Health monitoring should reflect population diversityJournal of Health Monitoring EDITORIAL
6
Imprint
This work is licensed under a Creative Commons Attribution 4.0
International License.
The Robert Koch Institute is a Federal Institute within the portfolio of the German Federal Ministry of Health
Journal of Health Monitoring
PublisherRobert Koch InstituteNordufer 20 D-13353 Berlin, Germany
EditorsSusanne Bartig, Johanna Gutsche, Dr Birte Hintzpeter, Dr Franziska Prütz, Dr Martina Rabenberg, Dr Alexander Rommel, Dr Livia Ryl, Dr Anke-Christine Saß, Stefanie Seeling, Martin Thißen, Dr Thomas ZieseRobert Koch InstituteDepartment of Epidemiology and Health MonitoringUnit: Health ReportingGeneral-Pape-Str. 62–66D-12101 BerlinPhone: +49 (0)30-18 754-3400E-mail: [email protected]/journalhealthmonitoring-en
TypesettingGisela Dugnus, Kerstin Möllerke, Alexander Krönke
Translation Simon Phillips/Tim Jack
ISSN 2511-2708
Note External contributions do not necessarily reflect the opinions of the Robert Koch Institute.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
Journal of Health Monitoring
7
FOCUS
Journal of Health Monitoring · 2019 4(3) DOI 10.25646/6074 Robert Koch Institute, Berlin
Carmen Koschollek *, Susanne Bartig *, Alexander Rommel, Claudia Santos-Hövener, Thomas Lampert
* contributed equally
Robert Koch Institute, Berlin Department of Epidemiology and Health Monitoring
Submitted: 27.03.2019 Accepted: 24.06.2019 Published: 18.09.2019
The health of children and adolescents with a migration background in Germany
The health of children and adolescents with a migration background in Germany – Results of the cross-sectional KiGGS Wave 2 study
AbstractOver a third (36.5%) of young people living in Germany have a migration background. Based on the data of the second follow-up to the German Health Interview and Examination Survey for Children and Adolescents (KiGGS Wave 2, 2014-2017), the health situation of 11- to 17-year-olds with and without a migration background is described using selected indicators. In order to account for the diversity among children and adolescents with a migration background, the health indicators used in this study are stratified by migration background but also by additional migration-related characteristics. In addition, the results from the various subgroups are also stratified by sociodemographic characteristics. No differences in self-assessed general health or the outpatient utilisation of paediatric and general medical services were identified between 11- to 17-year-olds with and without a migration background. However, migration-related differences were identified in health behaviour: whereas children and adolescents with a one- or two-sided migration background are more frequently overweight (including obesity), they consume risky amounts of alcohol less often than those of the same age without a migration background. Finally, the outcomes of the indicators also vary according to migration-related and sociodemographic characteristics.
MIGRATION · MIGRATION BACKGROUND · KIGGS · HEALTH MONITORING · HEALTH REPORTING
1. Introduction
Data from the 2017 microcensus demonstrate that around 19.3 million people in Germany have a migration back-ground. As such, almost a quarter of the population in Ger-many (23.6%) was born either themselves or at least one parent without German citizenship. More than one third of the young people in Germany (36.5%) have a migration background and 20.3% of the migrant population under the age of 18 have experienced migration themselves; in other words, they were born abroad and moved to Germa-ny at a later date [1]. International migration can be defined
as the cross-border relocation of a person’s permanent place of residence [2, 3]. This biographical event can influ-ence the health situation of migrants and their children born in Germany (second-generation migrant) through various factors before, during and after migration [4, 5]. Although children and adolescents born in Germany are neither directly affected by the living conditions found in their parents’ country of origin nor by the process of migra-tion itself, the situation can still influence their health (for example, due to discrimination). At the same time, the socialisation of children and adolescents with a migration background may be marked by cultural conflicts: in

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
8
FOCUS
without a German citizenship, an onomastic procedure was used to send out invitations to prospective participants in the language of their probable country of origin. Addi-tionally, the survey materials were translated and the field teams received intercultural training [13].The results from the KiGGS baseline study (2003-2006), which was the first to implement a migration-sensitive study design as part of the Robert Koch Institute’s health monitoring framework, indicate differences in the health situation between chil-dren and adolescents with and without a migration back-ground. The study found that a significantly lower propor-tion of 11- to 17-year-olds with a two-sided migration background rate their health as good or very good com-pared to those without or with a one-sided migration back-ground. In addition, children and adolescents with a two-sided migration background are disproportionately affected by overweight and obesity. However, they also consume alcohol less frequently than the comparison groups (chil-dren and adolescents with a one-sided or without a migra-tion background). Overall, the results from the KiGGS base-line study indicate a high level of heterogeneity among children and adolescents with a migration background. As such, individual health indicators may vary considerably by sex, country of origin and the length of stay [14]. In this regard, it is essential that studies go beyond merely distin-guishing between the presence or lack of a migration back-ground.
Based on the set of core indicators of the Federal Health Reporting on people with a migration background, the health situation of 11- to 17-year-old children and adoles-cents with and without a migration background is described using selected health indicators collected in KiGGS Wave 2
addition to their own family’s values and ways of life, chil-dren with a migration background are also influenced by the ways of thinking and the norms characterising the host society. On the other hand, children and adolescents can also influence the health of their parents by mediating dur-ing their parents’ interactions with health care institutions [5-7].
Migration status alone is an inadequate means of analysing health-related inequalities [8, 9]. As such, further explanatory factors, such as a person’s social situation, also need to be taken into account when studying health inequalities [10]. However, the data available to describe the health of the population with a migration background is inadequate. For example, the proportion of migrants in health surveys often does not correspond to their propor-tion of the population. In addition to peculiarities in par-ticipant behaviour, linguistic barriers, mistrust and con-cerns about sensitive questions or consequences concerning the residence status of (non-)participation lead to lower rates of survey participation among people with a migration background [11, 12]. Therefore, a migration-sen-sitive approach is essential in order to better involve peo-ple with a migration background in health surveys.
The German Health Interview and Examination Survey for Children and Adolescent (KiGGS) regularly collects nationwide representative data on the health of children and adolescents. The second follow-up survey (KiGGS Wave 2, 2014-2017), which was designed as an interview and examination survey, implemented a multi-level migra-tion-sensitive approach with the aim of increasing the par-ticipation of families with a migration background. In addi-tion to an oversampling of children and adolescents
KiGGS Wave 2
Second follow-up to the German Health Interview and Examination Survey for Children and Adolescents
Data owner: Robert Koch Institute
Aim: Providing reliable information on health status, health-related behaviour, living condi-tions, protective and risk factors, and health care among children, adolescents and young adults living in Germany, with the possibility of trend and longitudinal analyses
Study design: Combined cross-sectional and cohort study
Cross-sectional study in KiGGS Wave 2Age range: 0 -17 yearsPopulation: Children and adolescents with permanent residence in GermanySampling: Samples from official residency registries - randomly selected children and adolescents from the 167 cities and municipal-ities covered by the KiGGS baseline studySample size: 15,023 participants
KiGGS cohort study in KiGGS Wave 2Age range: 10 -31 yearsSampling: Re-invitation of everyone who took part in the KiGGS baseline study and who was willing to participate in a follow-up Sample size: 10,853 participants
KiGGS survey waves▶ KiGGS baseline study (2003-2006),
examination and interview survey▶ KiGGS Wave 1 (2009-2012),
interview survey▶ KiGGS Wave 2 (2014-2017),
examination and interview survey
More information is available at www.kiggs-studie.de/english

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
9
FOCUS
dance with the American Association for Public Opinion Research’s (AAPOR) Response Rate 2 [19].
2.2 Indicators
This article describes four health indicators from different fields of action from the core indicator set on the health of people with a migration background of the Federal Health Reporting. In addition to self-assessed general health (field of action: promoting and strengthening health), prevalence of overweight (including obesity) and risky alcohol consump-tion (field of action: promoting and strengthening health-con-scious behaviour), this article also describes the utilisation of outpatient medical care provided by general practitioners and paediatricians (field of action: promotion of equal access to health care services). The results are stratified by migra-tion background (without migration background versus one-sided or two-sided migration background), by migra-tion-related characteristics (parental length of stay in Ger-many and language spoken at home) and sociodemograph-ic characteristics (sex, age and socioeconomic status).
The analyses are based on self-reported information provided by children and adolescents aged between 11 and 17 and – for some indicators – on information provided by their parents. Participants aged 11 to 17 were only consid-ered if they and their parents had provided a valid ques-tionnaire (n=6,103; 3,195 girls and 2,908 boys). Missing values resulted in differing numbers of participants for individual indicators
(see also the article on Health reporting on people with migration background – Selection and definition of (core) indicators in this issue of the Journal of Health Monitor-ing). In line with the recommendations within the referred paper, the results are stratified by migration-related and sociodemographic characteristics.
2. Methodology2.1 Study design
KiGGS is part of the health monitoring system at the Robert Koch Institute and includes repeated cross-section-al surveys of children and adolescents aged 0 to 17 (KiGGS cross-sectional study) that are representative for Germany. The KiGGS baseline study (2003-2006) was conducted as an examination and interview survey, the first follow-up study (KiGGS Wave 1, 2009-2012) as a telephone-based interview survey and KiGGS Wave 2 (2014-2017) as an examination and interview survey. The concept and design of KiGGS have been described in detail elsewhere [15-18].
Prospective participants were randomly selected for KiGGS Wave 2 from the official residency registries of the 167 representative cities and municipalities that were cho-sen for the baseline study. A number of measures have been conducted to increase the study participation and to ensure that the sample was representative of the popula-tion in Germany [13, 18].
Overall, 15,023 children and adolescents (7,538 girls, 7,485 boys) took part in KiGGS Wave 2 (response rate 40.1%). A total of 3,567 children and adolescents (1,801 girls, 1,766 boys) participated in the examinations (response rate 41.5%). The response rate was calculated in accor-
The data from KiGGS Wave 2 provides the opportunity for a differentiated description of the health of children and adolescents based on migra-tion-related and sociodemo-graphic characteristics.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
10
FOCUS
overweight, including obesity. The data on body weight and height used in the analyses were collected directly from the children aged 11 or above by self-assessment. The analyses include valid data from 4,739 children and adolescents with-out a migration background (2,447 girls, 2,292 boys) and from 1,022 peers with a migration background (563 girls, 459 boys).
Alcohol consumptionThe KiGGS study collected data on the lifetime prevalence of alcohol consumption among children and adolescents aged 11 or above. The participants were asked ‘Have you ever drunk alcohol?’ and could answer either ‘Yes’ or ‘No’. The prevalence of risky alcohol consumption was assessed using the Alcohol Use Disorders Identification Test (-Con-sumption, AUDIT-C), a short test used to measure the lev-el and frequency of alcohol consumption [24]. First of all, the frequency of alcohol consumption is assessed by ask-ing the participants the following question: ‘How often do you have a drink containing alcohol, such as a glass of wine, beer, mixers, spirits or liqueurs?’ The following response categories were provided: ‘Never’, ‘Monthly or less’, ‘2 to 4 times a month’, ‘2 to 3 times a week’ and ‘4 or more times a week’. Data was then collected on the number of alco-holic drinks that were typically consumed in one day (the following answer categories were available: ‘1 to 2’, ‘3 to 4’, ‘5 to 6’, ‘7 to 9’, ‘10 or more alcoholic drinks’). A short addi-tional note served to ensure that responses remained objec-tive: ‘A drink refers to a small bottle of beer = 0.33 l, a small glass of wine or champagne = 0.125 l, a double spirit or liqueur = 4 cl, or a mixer drink = 1 Alcopop’). AUDIT-C’s third question is about heavy episodic drinking, which is defined
Health indicators
General healthThis study uses self-assessed general health to describe the health of children and adolescents with and without a migration background. The results on subjective health are based on self-assessments provided by the 11- to 17-year-olds. In accordance with the recommendations of the World Health Organization (WHO) [20], young people were asked ‘How is your health in general?’ Response categories were ‘very good’, ‘good’, ‘average’, ‘poor’ and ‘very poor’. In the following the proportion of children and adolescents who assessed their overall health as ‘good’ or ‘very good’ is reported. As such, the analyses are based on data from 4,937 children and adolescents aged between 11 and 17 with-out a migration background (2,552 girls, 2,385 boys) and 1,093 peers with a migration background (604 girls, 489 boys).
Body Mass IndexThe body mass index (BMI), a measurement of a person’s body weight divided by the square of body height (kg/m²), is used to classify underweight, normal weight, overweight and obesity. Due to growth-related changes in childhood and adolescence, the BMI values are divided into percen-tiles that account for differences in age and sex [21]. In Ger-many, the reference system of Kromeyer-Hauschild is used to define the BMI classifications. Children and adolescents with a BMI above the 90th percentile are classified as over-weight, and those with a BMI above the 97th percentile are classified as obese [22, 23]. This core indicator describes the proportion of children and adolescents affected by

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
11
FOCUS
Characteristics of stratification
Sociodemographic characteristicsPrevalences are presented separately for girls and boys. In line with the categories of the German Youth Protection Act, the participants are classified into children (aged between 11 and 13) and adolescents (aged between 14 and 17). A family’s socioeconomic status (SES) was measured through an index based on the information parents pro-vided on educational background, occupational status and income situation (equivalised disposable income) [25]. This enabled the participants to be categorised as either belong-ing to a family with a low, medium or high SES.
Migration-related characteristicsIn addition to sex, age and SES, results are stratified by migration background. The definition of the migration back-ground in KiGGS is based both on the country of birth of the child and the parents as well as on the citizenship of the parents. Thus, there is a two-sided migration back-ground if both parents were not born in Germany or do not have the German citizenship. If the child and at least one of its parents was born abroad this is also defined as a two-sided migration background. A one-sided migration background is given if one parent was born abroad or does not have German citizenship [6, 14].
The results are also stratified by a second migration- related characteristic – the length of stay of the child’s par-ents in Germany. Parents were asked the question ‘Since when has Germany been your main country of residence?’ by either stating ‘Since I was born’ or by providing the year that they came to Germany. The length of stay of parents
as the consumption of six or more alcoholic drinks on one occasion at least once a month (response categories: ‘Never’, ‘Less than monthly’, ‘Monthly’, ‘Weekly’, ‘Daily or almost daily’). A total score was calculated from the answers provided to these three questions in order to depict the distribution of risky alcohol consumption. Valid data for risky alcohol consumption are available for 4,815 children and adolescents without a migration background (2,504 girls, 2,311 boys) and 1,080 peers with a migration back-ground (594 girls, 486 boys).
Utilisation of outpatient medical careData on the utilisation of paediatric and general medical services was collected using the following question: ‘Please tell us which doctors in private practice of the following disciplines you have consulted for your child in the last 12 months and how often’ (data provided by the parents of children and adolescents aged between 11 and 13, and by young people themselves aged 14 or above). Explicitly included are ‘home visits, but not doctor contacts in the hospital or in a medical spa’. The response categories ‘Pae-diatrician’ and ‘General practitioner’ were merged to form a single category. The analyses describe the proportion of children and adolescents who have visited paediatricians and/or general practitioners in the last twelve months. The results are based on valid data from 4,882 children and adolescents without a migration background (2,547 girls, 2,335 boys) and from 1,067 peers with a migration back-ground (592 girls, 475 boys).

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
12
FOCUS
reported unweighted case numbers (n). All analyses were performed with Stata 15.1 (Stata Corp., College Station, TX, USA, 2017) using a data set of KiGGS Wave 2 specially compiled for migration-related analyses. Stata survey com-mands were used during all of the analyses to account for any clustering that might have occurred due to the selec-tion of the sample points and the weighting applied to cal-culate confidence intervals and p-values [28].The results are presented as prevalences with 95% confidence intervals (95% CI). Prevalences are estimates, the precision of which can be assessed through the use of confidence intervals; wide confidence intervals thereby indicate a greater statis-tical uncertainty in the results. Univariate logistic regres-sion was used to calculate odds ratios (OR) and p-values in order to measure the strength of a statistical relation-ship. A statistically significant difference between groups is assumed when the corresponding p-value is smaller than 0.05. Odds ratios indicate the factor by which the statisti-cal chance of a health outcome occurring in a particular group is higher or lower than in the reference group.
3. Results
The participants’ sociodemographic and migration-related characteristicsOf the 6,103 participants (3,195 girls and 2,908 boys), more than half are aged between 14 and 17 years old (59.4%); slightly less than half are aged between 11 and 13 years (40.6%). Based on data from 6,082 children and adolescents, the majority belongs to the medium SES group (62.0%); around one in five belongs to the low SES group (20.2%) and slightly fewer belong to the high SES group (17.8%).
in Germany was calculated as the difference between the survey year and the year that the parents moved to Ger-many. Answers provided by the mother were taken into account if she or both parents had moved to Germany; answers from the father were used if he was the only one having moved to Germany. Following categories were built according to the answers: ‘Always or for more than 20 years’, ‘11 to 20 years’ and ‘0 to 10 years’. Thus, the first category also includes children and adolescents that do not have a migration background. Prevalences were also stratified by a third migration-related characteristic – the language spoken at home. Parents were asked ‘Which lan-guages do you speak at home?’ They could choose between ‘German’ or ‘Further languages’. If the parents selected the latter, they could indicate two ‘Further languages’. Accord-ing to parents’ answers, the categories ‘Only German’, ‘Ger-man and further language(s)’ or ‘Only further language(s)’ were built to describe the language spoken at children and adolescents’ homes.
2.3 Statistical analysis
The calculations were carried out using a weighting factor that corrects deviations within the sample from the popu-lation structure with regard to regional structure (rural area/urban area), age (in years), sex, federal state (as of 31 December 2015), German citizenship (as of 31 December 2014) and the parents’ level of education according to the CASMIN classification (Comparative Analysis of Social Mobility in Industrial Nations [26], Microcensus 2013 [27]). The proportions described in this article represent weight-ed proportions and may differ accordingly from the

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
13
FOCUS
are few significant differences in self-assessed general health. The subgroup analysis demonstrates that girls whose parents have lived in Germany between 11 and 20 years rate their health as very good or good less frequent-ly than girls whose parents have been living in Germany for more than 20 years or who have always lived in the country. The same applies to the 14- to 17-year-old sub-group. Additionally in the group with a low SES, children and adolescents whose parents have lived between 11 and 20 years in Germany rate their own health as very good or good slightly less frequently than those whose parents have lived in Germany for more than 20 years or who have always lived in the country (Annex Table 1).
In general, no significant differences were identified between the participants according to the language spoken at home. However, a significant difference was identified among the boys: boys who speak only German at home rate their health as very good or good less frequently than boys who do not speak German at home. Among 14- to 17-year-olds, those who speak German in addition to one or more further languages at home rate their overall health as very good or good somewhat less frequently than those whose only home language is German (Annex Table 1).
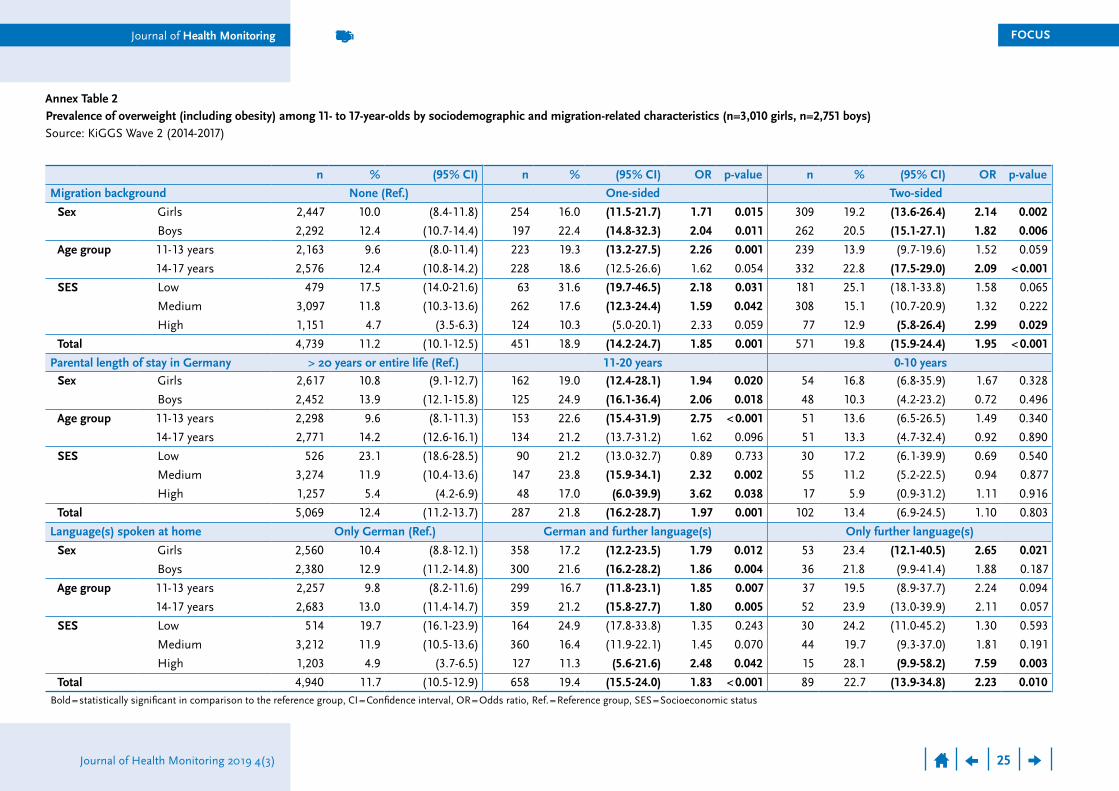
Body Mass IndexChildren and adolescents with a one-sided or two-sided migration background are affected by overweight (includ-ing obesity) significantly more frequently than children and adolescents without a migration background (Figure 1 and Annex Table 2). This applies to girls as well as boys. Differ-ences in the frequency of overweight were also identified according to age: whereas 11- to 13-year-old children with
Three out of four participants do not have a migration background (74.5%); nearly one tenth has a one-sided migration background (9.1%) and approximately one sixth has a two-sided migration background (16.5%). Of the lat-ter, 24.1% have their own experience of migration, and, therefore, moved to Germany from abroad. The most com-mon countries of birth among 11- to 17-year-olds with expe-riences of migration are Poland (n=17), Syria (n=13) and Russia (n=11). The analyses of parental length of stay are based on data from 5,767 participants. The vast majority of parents have either been living in Germany for more than 20 years or have always lived in the country (88.8%). From 8.1% of participants parents have lived between 11 and 20 years in Germany; only a small minority of par-ents have lived in Germany for ten years or less (3.1%). Data are available from 6,021 participants on the language spoken in their home. Four out of five children and adoles-cents speak only German at home (80.2%); about one in six speak German and one or more further languages at home (16.7%). Only a very small minority does not speak German at all at home (3.1%).
General healthThe vast majority of participants assessed their general health as very good or good. No significant differences were identified between the groups according to migration back-ground (without migration background 89.4%, one-sided migration background 89.1%, two-sided migration back-ground 87.1%). Even further stratification by sex, age and SES, revealed no significant differences in self-assessed general health based on migration background (Annex Table 1).For the other migration-related characteristics there
No differences in self-assessed general health were identified between 11- to 17-year-olds with and without a migration background.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
14
FOCUS
Figure 1 Prevalence of overweight (including obesity)
among 11- to 17-year-olds by sociodemographic and migration-related characteristics
(n=3,010 girls, n=2,751 boys)Source: KiGGS Wave 2 (2014-2017)
Proportion (%)
10
20
30
40
50
Girls Boys 11-13 years 14-17 years TotalLow SES Medium SES High SES Two-sided migration background One-sided migration background No migration background
Migration background
Proportion (%)
10
20
30
40
50
Girls Boys 11-13 years 14-17 years Low SES Medium SES High SES Total0-10 years11-20 years>20 years or always
Parental length of stay in Germany
Proportion (%)
10
20
30
40
50
Only further language(s)German and further language(s)Only German
60
Girls Boys 11-13 years 14-17 years TotalLow SES Medium SES High SES
Language(s) spoken at home
SES = Socioeconomic status

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
15
FOCUS
(Figure 1 and Annex Table 2). Both girls and boys who speak one or more further languages in addition to German at home are more frequently affected by overweight than girls and boys whose only home language is German. This also applies to girls who do not speak German at home. The finding that children and adolescents who speak one or more languages in addition to German at home are more frequently affected by overweight is evident in both age groups (Figure 1 and Annex Table 2). In terms of SES, children and adolescents from the high SES group who do not speak German at home are more frequently affected by overweight than children and adolescents who speak only German at home. The same applies to those who speak German at home in addition to one or more further languages (Figure 1 and Annex Table 2).
Alcohol consumptionAs much as 14.5%, children and adolescents without a migration background state that they consume risky amounts of alcohol significantly more often than those with a one-sided or two-sided migration background (Figure 2 and Annex Table 3). This finding holds true for both sexes. Among 14- to 17-year-olds, young people with a one- or two-sided migration background consume risky amounts of alcohol significantly less frequently than those without a migration background. Differences were also identified between the SES groups with regard to migration background. Whereas in the low and high SES groups children and adolescents with a one-sided migration background consume risky amounts of alcohol less frequently, in the low and medium SES group this applies to those with a two-sided migration background
a one-sided migration background are more frequently affected by overweight than children without a migration background of the same age, in the group of the 14- to 17-year-olds, overweight is more common among those with a two-sided migration background. Significant differ-ences are also evident in all three SES groups. In the groups with a low or medium SES, 11- to 17-year-olds with a one-sid-ed migration background are more frequently affected by overweight than those without a migration background. In the group with a high SES, young people with a two-sid-ed migration background are more frequently affected by overweight than their peers without a migration back-ground (Figure 1 and Annex Table 2).
Differences were also identified with regard to paren-tal length of stay in Germany. Children and adolescents whose parents have lived in Germany between 11 and 20 years are more frequently affected by overweight than those whose parents have lived in Germany for more than 20 years or for their entire life. This difference is evident among girls and boys. Among 11- to 13-year-olds whose parents have lived in Germany between 11 and 20 years are also more frequently affected by overweight than those whose parents have lived in Germany for more than 20 years or for their entire life. This difference is also found in the groups with a medium or high SES (Figure 1 and Annex Table 2).
A number of differences were also identified in terms of the language spoken at home. Overall, children and ado-lescents who either speak German at home in addition to one or more further languages or who do not speak Ger-man at home are more frequently affected by overweight compared with those who speak only German at home
Children and adolescents with a migration background are more frequently overweight than their peers without a migration background but consume risky amounts of alcohol less frequently.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
16
FOCUS
Figure 2 Prevalence of risky alcohol consumption
among 11- to 17-year-olds by sociodemographic and migration-related characteristics
(n=3,098 girls, n=2,797 boys) Source: KiGGS Wave 2 (2014-2017)
SES = Socioeconomic status * The prevalence of risky alcohol consumption in these groups was (almost) zero percent.
Proportion (%)
5
10
15
20
25
30
Girls Boys 11-13 years 14-17 years TotalTwo-sided migration background One-sided migration background No migration background
Low SES Medium SES High SES
Migration background
* *
Proportion (%)
5
10
15
20
25
0-10 years11-20 years>20 years or alwaysGirls Boys 11-13 years 14-17 years TotalLow SES Medium SES High SES
Parental length of stay in Germany
* **
Proportion (%)
5
10
15
20
25
30
Girls Boys 11-13 years 14-17 years TotalOnly German
Low SES Medium SES High SES Only further language(s)German and further language(s)
Language(s) spoken at home
* * ** *

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
17
FOCUS
subgroups by sex, age, SES or parental length of stay (Annex Table 4).
However, one difference was found according to the language spoken at home in general and in one subgroup: children and adolescents in the high SES group who speak one or more further languages in addition to German at home make use of paediatric treatment and/or general medical services more frequently than those who speak only German at home (Annex Table 4).
4. Discussion
This article aims to describe the health situation of 11- to 17-year-olds based on the core indicators of the Federal Health Reporting on people with a migration background from the fields of health status, health behaviour and health care. In order to account for the diversity found among children and adolescents, the data were also stratified by additional migration-related and sociodemographic char-acteristics that go beyond the concept of migration back-ground.
Self-assessments of general health (subjective health) were used to provide information about health status. Var-ious longitudinal studies have demonstrated that self-as-sessments are useful predictors for the utilisation of med-ical services, chronic diseases, and mortality [29]. Most children and adolescents rated their general health as very good or good. Only few differences according to migra-tion-related characteristics in individual subgroups were identified.
With regard to the prevalence of overweight (including obesity) the analyses of KiGGS Wave 2 indicate migra-
(Figure 2 and Annex Table 3). Children and adolescents whose parents have lived in Germany for more than 20 years or for their entire life have a higher frequency of risky alcohol consumption than those whose parents have lived in Germany for less than 20 years (Annex Table 3). The subgroup analysis demonstrates that the same applies to girls and to 14- to 17-year-olds. In the group with a medi-um SES, those whose parents have been living in Germany for more than 20 years or for their entire life consume risky amounts of alcohol significantly more frequently than chil-dren and adolescents whose parents have lived in Germa-ny between 11 and 20 years (Figure 2 and Annex Table 3).
Differences in the frequency of risky alcohol consump-tion were also associated with the language spoken at home. Children and adolescents whose only home lan-guage is German state that they consume risky amounts of alcohol about three times more frequently (14.0%) than those who speak one or more further languages or who do not speak German at home (Figure 2 and Annex Table 3). Among the boys in all three SES groups, those who speak German at home alongside one or more further languages have a lower frequency of alcohol consumption than those whose only home language is German. In addition, among the girls and 14- to 17-year-olds, those who do not speak German at home consume risky amounts of alcohol less frequently than their peers (Figure 2 and Annex Table 3).
Utilisation of outpatient medical careIn total, more than three quarters of children and adoles-cents have made use of outpatient paediatric treatment or general medical services over the last twelve months. No migration-related differences were identified in the
Journal of Health Monitoring 2019 4(3)
Journal of Health Monitoring
The utilisation of paediatric or general medical services did not differ between children and adolescents with and without a migration background.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
18
FOCUS
this was not offered to all participating children and ado-lescents. Compared to self-reported data, examination data are regarded as more reliable indicators. However, the number of cases is too low for differentiated analyses within the group of children and adolescents with a migra-tion background in the age group under consideration. In contrast, the analyses show that children and adolescents with a one- or two-sided migration background consume risky amounts of alcohol significantly less frequently than their peers without a migration background. Previous research suggests associations between alcohol con-sumption and the presence of a migration background for e.g. cultural or religious reasons depending on the country of birth [14, 34, 35]. Due to the small number of cases and the lack of relevant determinants in the KiGGS survey (such as religious affiliation), this association can-not be further investigated in this article. No migration- related differences were identified among children and adolescents in terms of the utilisation of health care ser-vices: the majority of children and adolescents had used paediatric and/or general medical services during the last twelve months independent of an own or familial history of migration. Children and adolescents with a migration background only showed slight differences in the utilisa-tion of outpatient medical care with regard to parental length of stay. Thus, a shorter length of parental stay in Germany was associated with a slightly lower utilisation of paediatric and general medical services. This may be due to the lack of knowledge about the German health system that migrants may have resulting from the shorter length of stay. In addition, experiences with discrimina-tion and structural barriers related, i.a., to residence sta-
tion-related differences between children and adolescents. Hence, 11- to 17-year-olds with a migration background are more frequently affected by overweight than their peers without a migration background. According to some expla-native approaches, the higher prevalence of overweight can be attributed, among other things, to the partially unhealth-ier diets among children and adolescents with a migration background [30]. The results of the KiGGS baseline study show that both a longer length of stay in Germany and belonging to the group of second-generation migrants are associated with higher levels of consumption of soft drinks and fast foods etc. In addition, children and adolescents with a two-sided migration background, especially girls, tend to have a higher prevalence of physical inactivity than their peers without a migration background [14].
However, both risk factors for overweight – an unhealthy diet and lower levels of physical activity – can-not be attributed to a migration background alone; there-fore, a more in-depth analysis is required of the causes of overweight. It is possible that the financial restrictions that migrant families may face lead to a lower consump-tion of healthy foods and less use of leisure activities involving physical activity [21]. Living environments pro-vide a further possible explanation and, thus, the avail-ability of fast food restaurants and (the lack of) local lei-sure activities [31, 32]. This association could be analysed in the future by linking survey data with geodata [33]. How-ever, as a limiting factor it should be noted that self-re-ported data on overweight were used from the KiGGS study, as these are available for all participants. Body weight and height were measured in a standardised man-ner in the examination part of the KiGGS survey, however,
For selected health indica-tors, there are significant differences in sociodemo-graphic and migration- related characteristics between 11- to 17-year-olds.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
19
FOCUS
migration background, however, it is generally difficult to win people from this status group for surveys [15, 38].
Another problem concerning case numbers arises when comparing among children and adolescents with migration background: Differences in terms of utilisation of health care services may exist between those with migration back-ground and those without German citizenship depending on their residency status (temporary versus permanent residence permits) and associated legal access to health-care. However, these differences cannot be investigated using current data due to the small number of cases that are available.
In addition to the number of cases, the insufficient con-sideration of migration-sensitive concepts in KiGGS Wave 2 represents a further limitation. For example, data on reli-gious affiliation could help explain the lower level of alco-hol consumption among children and adolescents with a migration background – this indicator cannot be substi-tuted by ‘origin from a country with a predominantly Mus-lim population’ just as the indicator ‘language spoken at home’ cannot adequately replace the self-assessed German language proficiency.
As part of the framework provided by the Robert Koch Institute’s Improving Health Monitoring in Migrant Pop-ulations (IMIRA) project, various concepts that have been used within the health monitoring in the past have been revised and expanded for migration-sensitive components (see also Concepts for migration-sensitive health monitor-ing in this issue of the Journal of Health Monitoring). In the future, these concepts are to be used to account for the diversity of the population in Germany and to assess approaches that go beyond the mere concept of migration
tus can provide further explanations [36, 37]. It is surpris-ing, however, that language, which the current literature identifies as a barrier to accessing health care, appears to have no association with the utilisation of paediatric or general health care services. However, it is important to note as another limiting factor of the KiGGS study, that the language spoken at home only provides an approxi-mation of a person’s German language skills. Moreover, KiGGS Wave 2 did not collect data on ‘self-assessed Ger-man language proficiency’ as recommended in the migra-tion-related indicator set of the Federal Health Reporting.
Overall, the results show that children and adolescents with and without a migration background have a similar level of good health. However, there are differences in out-comes associated with health behaviour (diet and physical activity, substance use). Although the KiGGS Wave 2 sam-ple almost reflects the actual population with regard to the proportion of families with a migration background, an in-depth analysis of the differences in health behaviour would require larger case numbers in order to account for the diversity found among children and adolescents with a migration background. At the same time, the current analyses merely represent initial results. As a next step, multivariate models are required to examine the impact of migration-related variables after controlling for sociode-mographic and socioeconomic characteristics. For exam-ple, in order to assess the validity of the assumption that an unhealthy diet and a lack of physical activity are primar-ily associated with financial constraints rather than a migra-tion background, families with a low SES – with and with-out a migration background – should be more strongly integrated in future health surveys. Irrespective of their

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
20
FOCUS
Corresponding authorCarmen Koschollek
Robert Koch Institute Department of Epidemiology and Health Monitoring
General-Pape-Str. 62–66 D-12101 Berlin, Germany
E-mail: [email protected]
Please cite this publication asKoschollek C, Bartig S, Rommel A, Santos-Hövener C, Lampert T (2019)
The health of children and adolescents with a migration background in Germany – Results of the cross-sectional KiGGS Wave 2 study.
Journal of Health Monitoring 4(3): 7-28. DOI 10.25646/6074
The German version of the article is available at: www.rki.de/journalhealthmonitoring
Data protection and ethicsKiGGS Wave 2 is subject to strict compliance with the data protection provisions set out in the EU General Data Pro-tection Regulation (GDPR) and the Federal Data Protection Act (BDSG). Hannover Medical School’s ethics committee assessed the ethics of the study and provided its approval (No. 2275-2014). Participation in the study was voluntary. The participants and/or their parents/legal guardians were also informed about the aims and contents of the study, and about data protection. Informed consent was obtained in writing.
FundingKiGGS is funded by the Federal Ministry of Health and the Robert Koch Institute.
background when studying health differences. It is essen-tial to ensure the long-term, representative involvement of all population groups in health monitoring at the Robert Koch Institute. In order to ensure that people with a migra-tion background are properly integrated into health surveys, the IMIRA project has further developed the migration- sensitive methods of participant recruitment and survey methods used in the KiGGS baseline study and in KiGGS Wave 2 [39]. In the future, the results will be incorporated into an integrated overall concept of health monitoring at the Robert Koch Institute.
Despite the migration-related limitations outlined above, the KiGGS study constitutes a unique data source to describe the health of children and adolescents in Germany. In particular, the KiGGS baseline study and KiGGS Wave 2, which were conceived as interview and examination sur-veys, are unique as they made use of migration-sensitive study designs. Another peculiarity is the KiGGS cohort, which allows life course analyses. With this approach, long-term effects of exposures in different phases of life and environments can be analysed and correlated [5, 40]. Life course epidemiology has not yet been widely applied to people with migration background due to the lack of data. However, with the KiGGS study, data are now available to analyse the complex conditional factors that affect the health of children and adolescents with a migration back-ground.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
21
FOCUS
8. Razum O, Karrasch L, Spallek J (2016) Migration. Eine vernach-lässigte Dimension gesundheitlicher Ungleichheit. Bundesge-sundheitsbl 59(2):259-265
9. Schenk L, Bau AM, Borde T et al. (2006) Mindestindikatorensatz zur Erfassung des Migrationsstatus. Empfehlungen für die epide-miologische Praxis. Bundesgesundheitsbl 49(9):853-860. https://edoc.rki.de/handle/176904/1061 (As at 04.04.2019)
10. Lampert T, Richter M, Schneider S et al. (2016) Soziale Ungleich-heit und Gesundheit. Stand und Perspektiven der sozialepide-miologischen Forschung in Deutschland. Bundesgesundheitsbl 59(2):153-165. https://edoc.rki.de/handle/176904/2478 (As at 04.04.2019)
11. Borde T (2006) Migrationssensible Studiendesigns – Wozu brau-chen wir welches Konzept? In: Robert Koch-Institut (Ed) Migrati-onssensible Studiendesigns zur Repräsentation des Migrations-status in der Gesundheitsforschung – Tagung in Kooperation mit dem Robert Koch-Institut und dem Interdisziplinären For-schungsverbund Epidemiologie in Berlin (EpiBerlin) am 25. November 2005. RKI, Berlin
12. Schenk L (2002) Migrantenspezifische Teilnahmebarrieren und Zugangsmöglichkeiten im Kinder- und Jugendgesundheitssurvey. Gesundheitswesen 64(1):59-68
13. Frank L, Yesil-Jürgens R, Born S et al. (2018) Improving the inclu-sion and participation of children and adolescents with a migra-tion background in KiGGS Wave 2. Journal of Health Monitoring 3(1):126-142. https://edoc.rki.de/handle/176904/5640 (As at 04.04.2019)
14. Schenk L, Neuhauser H, Ellert U et al. (2008) Kinder- und Jugendgesundheitssurvey (KiGGS) 2003-2006: Kinder und Jugendliche mit Migrationshintergrund in Deutschland. Beiträge zur Gesundheitsberichterstattung des Bundes. RKI, Berlin. https://edoc.rki.de/handle/176904/3215 (As at 04.04.2019)
15. Kamtsiuris P, Lange M, Schaffrath Rosario A (2007) Der Kinder- und Jugendgesundheitssurvey (KiGGS): Stichprobendesign, Response und Nonresponse-Analyse. Bundesgesundheitsbl 50(5-6):547-556. https://edoc.rki.de/handle/176904/401 (As at 04.04.2019)
16. Lange M, Butschalowsky H, Jentsch F et al. (2014) Die erste KiGGS- Folgebefragung (KiGGS Welle 1): Studiendurchführung, Stichpro-bendesign und Response. Bundesgesundheitsbl 57(7):747-761. https://edoc.rki.de/handle/176904/1888 (As at 04.04.2019)
Conflicts of interest The authors declared no conflicts of interest.
Acknowledgement Foremost we would like to express our gratitude to both the participants and their parents. We would also like to thank everyone at the 167 study sites who provided us with space and active support on site.
KiGGS Wave 2 could not have been conducted without the dedication of numerous colleagues at the Robert Koch Institute. We would especially like to thank the study teams for their excellent work and their exceptional commitment during the three-year data collection phase.
References1. Statistisches Bundesamt (2018) Bevölkerung und Erwerbstätig-
keit. Bevölkerung mit Migrationshintergrund – Ergebnisse des Mikrozensus 2017. Fachserie 1 Reihe 2.2. Destatis, Wiesbaden
2. Lederer HW (2004) Indikatoren der Migration. Europäisches Forum für Migrationsstudien, Bamberg
3. Bundesministerium des Innern (2016) Migrationsbericht des Bundesamtes für Migration und Flüchtlinge im Auftrag der Bun-desregierung. Migrationsbericht 2015. BMI, Berlin
4. Schenk L (2007) Migration und Gesundheit – Entwicklung eines Erklärungs- und Analysemodells für epidemiologische Studien. Int J Public Health 52(2):87-96
5. Spallek J, Zeeb H, Razum O (2011) What do we have to know from migrants‘ past exposures to understand their health status? A life course approach. Emerg Themes Epidemiol 8(1):6
6. Schenk L, Ellert U, Neuhauser H (2007) Kinder und Jugendliche mit Migrationshintergrund in Deutschland. Methodische Aspek-te im Kinder- und Jugendgesundheitssurvey (KiGGS). Bundesgesundheitsbl 50(5/6):590-599. https://edoc.rki.de/handle/176904/408 (As at 04.04.2019)
7. Maier S, Giersiefen A, Klocke A (2016) Die gesundheitliche Lage von Kindern und Jugendlichen mit Migrationshintergrund in Deutschland. Pädiatrische Praxis 86(1):21-32

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
22
FOCUS
27. Research Data Centres of the Federal Statistical Office and Statis-tical Offices of the Länder (2017) Microcensus, 2013, own calcu-lations. https://www.forschungsdatenzentrum.de/en/household/micro-census (As at 20.11.2017 )
28. Stata Corp (2017) Stata Survey Data Reference Manual, Release 15. https://www.stata.com/manuals/svy.pdf (As at 03.04.2019)
29. Robert Koch-Institut (Ed) (2015) Gesundheit in Deutschland. Gesundheitsberichterstattung des Bundes. Gemeinsam getragen von RKI und Destatis. RKI, Berlin. https://edoc.rki.de/handle/176904/3248 (As at 04.04.2019)
30. Schenk L, Anton V, Baer NR et al. (2016) Ernährungsmuster von Kindern und Jugendlichen mit Migrationshintergrund: Ergeb-nisse der KiGGS-Studie. Public Health Forum 24(3):205-208
31. Lakes T, Burkart K (2016) Childhood overweight in Berlin: intra-urban differences and underlying influencing factors. Int J Health Geogr 15(12)
32. Reimers A, Wagner M, Alvanides S et al. (2014) Proximity to Sports Facilities and Sports Participation for Adolescents in Germany. PLoS ONE 9(3) e93059
33. Thißen M, Niemann H, Varnaccia G et al. (2017) Welches Poten-zial haben Geoinformationssysteme für das bevölkerungsweite Gesundheitsmonitoring in Deutschland? Perspektiven und Her-ausforderungen für das Gesundheitsmonitoring am Robert Koch-Institut. Bundesgesundheitsbl 60(12):1440-1452
34. Strupf M, Gomes de Matos E, Soellner R et al. (2017) Trinkver-halten von Personen verschiedener Herkunftsregionen in Deutschland: Ein Vergleich mit Personen ohne Migrationshinter-grund. Suchttherapie 18(2):90-97
35. Orth B (2017) Der Alkoholkonsum Jugendlicher und junger Erwachsener in Deutschland. Ergebnisse des Alkoholsurveys 2016 und Trends. BZgA-Forschungsbericht. Bundeszentrale für gesundheitliche Aufklärung, Köln
36. Razum O, Geiger I, Zeeb H et al. (2004) Gesundheitsversorgung von Migranten. Dtsch Arztebl 101(43):A2882-2887
37. Robert Koch-Institut (Ed) (2008) Schwerpunktbericht: Migration und Gesundheit. RKI, Berlin. https://edoc.rki.de/handle/176904/3194 (As at 04.04.2019)
38. Neller K (2005) Kooperation und Verweigerung: eine Non- Response-Studie. ZUMA Nachrichten 29(57)
17. Mauz E, Gößwald A, Kamtsiuris P et al. (2017) New data for action. Data collection for KiGGS Wave 2 has been completed. Journal of Health Monitoring 2(S3):2-27. https://edoc.rki.de/handle/176904/2812 (As at 04.04.2019)
18. Hoffmann R, Lange M, Butschalowsky H et al. (2018) KiGGS Wave 2 cross-sectional study – participant acquisition, response rates and representativeness. Journal of Health Monitoring 3(1):78-91. https://edoc.rki.de/handle/176904/5637 (As at 04.04.2019)
19. The American Association for Public Opinion Research (2016) Standard Definitions: Final Dispositions of Case Codes and Out-come Rates for Surveys. 9th edition. AAPOR, Deerfield
20. de Bruin A, Pivacet H, Nossikov A (1996) Health interview sur-veys: towards harmonization of methods and instruments. WHO Regional Publications European Series, Copenhagen
21. Schienkiewitz A, Brettschneider AK, Damerow S et al. (2018) Overweight and obesity among children and adolescents in Ger-many. Results of the cross-sectional KiGGS Wave 2 study and trends. Journal of Health Monitoring 3(1):15-22. https://edoc.rki.de/handle/176904/5627.2 (As at 04.04.2019)
22. Kromeyer-Hauschild K, Moss A, Wabitsch M (2015) Referenz-werte für den Body-Mass-Index für Kinder, Jugendliche und Erwachsene in Deutschland: Anpassung der AGA-BMI-Referenz im Altersbereich von 15 bis 18 Jahren. Adipositas 9(3):123-127
23. Kromeyer-Hauschild K, Wabitsch M, Kunze D et al. (2001) Per-zentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben. Monatsschr Kinderheilkd 148:807-818
24. Bush K, Kivlahan DR, McDonell MB et al. (1998) The AUDIT alco-hol consumption questions (AUDIT-C): An effective brief screen-ing test for problem drinking. Arch Intern Med 158(16):1789-1795
25. Lampert T, Hoebel J, Kuntz B et al. (2018) Socioeconomic status and subjective social status measurement in KiGGS Wave 2. Journal of Health Monitoring 3(1):108-125. https://edoc.rki.de/handle/176904/5639 (As at 04.04.2019)
26. Brauns H, Scherer S, Steinmann S (2003) The CASMIN Educa-tional Classification in International Comparative Research. In: Hoffmeyer-Zlotnik JHP, Wolf C (Eds) Advances in Cross-National Comparison: A European Working Book for Demographic and Socio-Economic Variables. Springer US, Boston, P. 221-244

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
23
FOCUS
39. Santos-Hövener C, Schumann M, Schmich P et al. (2019) Improving the information base regarding the health of people with a migration background. Project description and initial find-ings from IMIRA. Journal of Health Monitoring 4(1):46-57. https://edoc.rki.de/handle/176904/5915 (As at 04.04.2019)
40. Spallek J, Razum O (2016) Migration und Gesundheit. In: Richter H, Hurrelmann K (Eds) Soziologie von Gesundheit und Krankheit. Springer Fachmedien, Wiesbaden, P. 153-166

24
FOCUSThe health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
n % (95% CI) n % (95% CI) OR p-value n % (95% CI) OR p-valueMigration background None (Ref.) One-sided Two-sided
Sex Girls 2,552 87.7 (86.0-89.2) 274 86.6 (80.4-91.1) 0.91 0.690 330 83.8 (77.8-88.5) 0.73 0.150
Boys 2,385 90.9 (89.3-92.3) 211 91.9 (84.4-96.0) 1.14 0.739 278 90.4 (85.5-93.8) 0.94 0.811
Age group 11-13 years 2,262 92.1 (90.4-93.5) 241 90.7 (83.3-95.1) 0.84 0.637 261 91.9 (87.6-94.7) 0.97 0.907
14-17 years 2,675 87.5 (85.7-89.1) 244 87.7 (81.8-91.9) 1.02 0.919 347 84.6 (79.5-88.6) 0.79 0.254
SES Low 505 86.1 (81.4-89.7) 64 83.1 (67.2-92.2) 0.79 0.627 197 85.1 (78.7-89.8) 0.92 0.783
Medium 3,227 89.4 (87.9-90.8) 283 89.7 (84.9-93.1) 1.03 0.901 327 89.5 (84.3-93.1) 1.01 0.972
High 1,193 91.9 (90.0-93.4) 135 93.0 (86.8-96.4) 1.18 0.661 78 88.6 (77.5-94.6) 0.69 0.391
Total 4,937 89.4 (88.1-90.5) 485 89.1 (84.8-92.3) 0.97 0.892 608 87.1 (83.6-90.0) 0.80 0.206
Parental length of stay in Germany > 20 years or entire life (Ref.) 11-20 years 0-10 yearsSex Girls 2,734 88.4 (86.8-89.9) 172 77.5 (68.6-84.5) 0.45 0.002 58 88.1 (66.3-96.5) 0.97 0.963
Boys 2,549 91.5 (90.0-92.7) 134 87.7 (76.6-93.9) 0.66 0.322 52 93.1 (83.0-97.4) 1.25 0.668
Age group 11-13 years 2,402 92.8 (91.2-94.1) 168 87.2 (78.9-92.6) 0.53 0.054 57 92.4 (80.8-97.2) 0.95 0.926
14-17 years 2,881 88.2 (86.6-89.6) 138 78.3 (68.9-85.5) 0.48 0.007 53 89.1 (68.2-96.9) 1.10 0.893
SES Low 554 87.4 (83.1-90.8) 95 76.9 (65.1-85.6) 0.48 0.044 33 92.9 (80.2-97.7) 1.89 0.311
Medium 3,414 90.2 (88.9-91.4) 156 87.5 (80.6-92.1) 0.76 0.308 59 86.8 (65.2-95.8) 0.71 0.597
High 1,303 91.7 (89.9-93.2) 53 89.6 (78.8-95.2) 0.78 0.571 17 100.0 – – –
Total 5,283 90.0 (88.9-91.0) 306 82.4 (75.6-87.6) 0.52 0.004 110 90.7 (79.7-96.0) 1.08 0.869
Language(s) spoken at home Only German (Ref.) German and further language(s) Only further language(s)
Sex Girls 2,672 87.5 (85.8-89.0) 383 84.8 (79.5-89.0) 0.80 0.270 58 85.5 (67.4-94.4) 0.84 0.748
Boys 2,476 91.4 (89.8-92.7) 320 88.2 (82.1-92.4) 0.70 0.199 40 98.9 (92.8-99.6) 8.75 0.032
Age group 11-13 years 2,362 91.8 (90.1-93.2) 325 91.5 (86.4-94.8) 0.97 0.908 42 97.1 (89.1-99.3) 2.97 0.132
14-17 years 2,786 87.9 (86.2-89.4) 378 83.1 (78.1-87.2) 0.68 0.043 56 88.8 (72.4-96.0) 1.09 0.881
SES Low 540 86.7 (82.1-90.2) 177 80.2 (72.1-86.4) 0.62 0.117 33 96.0 (77.9-99.4) 3.71 0.184
Medium 3,345 89.5 (88.1-90.8) 387 90.6 (86.4-93.6) 1.12 0.612 48 86.4 (61.1-96.2) 0.74 0.678
High 1,251 91.7 (89.9-93.2) 132 93.0 (86.2-96.6) 1.21 0.638 16 82.9 (47.2-96.3) 0.44 0.342
Total 5,148 89.6 (88.3-90.6) 703 86.5 (82.6-89.7) 0.75 0.105 98 91.3 (79.7-96.6) 1.24 0.678Bold = statistically significant in comparison to the reference group, CI = Confidence interval, OR = Odds ratio, Ref. = Reference group, SES = Socioeconomic status
Annex Table 1 Prevalence of self-assessed very good or good general health among 11- to 17-year-olds by sociodemographic and migration-related characteristics (n=3,156 girls, n=2,874 boys)Source: KiGGS Wave 2 (2014-2017)
25
FOCUSThe health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
n % (95% CI) n % (95% CI) OR p-value n % (95% CI) OR p-valueMigration background None (Ref.) One-sided Two-sided
Sex Girls 2,447 10.0 (8.4-11.8) 254 16.0 (11.5-21.7) 1.71 0.015 309 19.2 (13.6-26.4) 2.14 0.002
Boys 2,292 12.4 (10.7-14.4) 197 22.4 (14.8-32.3) 2.04 0.011 262 20.5 (15.1-27.1) 1.82 0.006
Age group 11-13 years 2,163 9.6 (8.0-11.4) 223 19.3 (13.2-27.5) 2.26 0.001 239 13.9 (9.7-19.6) 1.52 0.059
14-17 years 2,576 12.4 (10.8-14.2) 228 18.6 (12.5-26.6) 1.62 0.054 332 22.8 (17.5-29.0) 2.09 < 0.001
SES Low 479 17.5 (14.0-21.6) 63 31.6 (19.7-46.5) 2.18 0.031 181 25.1 (18.1-33.8) 1.58 0.065
Medium 3,097 11.8 (10.3-13.6) 262 17.6 (12.3-24.4) 1.59 0.042 308 15.1 (10.7-20.9) 1.32 0.222
High 1,151 4.7 (3.5-6.3) 124 10.3 (5.0-20.1) 2.33 0.059 77 12.9 (5.8-26.4) 2.99 0.029
Total 4,739 11.2 (10.1-12.5) 451 18.9 (14.2-24.7) 1.85 0.001 571 19.8 (15.9-24.4) 1.95 < 0.001
Parental length of stay in Germany > 20 years or entire life (Ref.) 11-20 years 0-10 yearsSex Girls 2,617 10.8 (9.1-12.7) 162 19.0 (12.4-28.1) 1.94 0.020 54 16.8 (6.8-35.9) 1.67 0.328
Boys 2,452 13.9 (12.1-15.8) 125 24.9 (16.1-36.4) 2.06 0.018 48 10.3 (4.2-23.2) 0.72 0.496
Age group 11-13 years 2,298 9.6 (8.1-11.3) 153 22.6 (15.4-31.9) 2.75 < 0.001 51 13.6 (6.5-26.5) 1.49 0.340
14-17 years 2,771 14.2 (12.6-16.1) 134 21.2 (13.7-31.2) 1.62 0.096 51 13.3 (4.7-32.4) 0.92 0.890
SES Low 526 23.1 (18.6-28.5) 90 21.2 (13.0-32.7) 0.89 0.733 30 17.2 (6.1-39.9) 0.69 0.540
Medium 3,274 11.9 (10.4-13.6) 147 23.8 (15.9-34.1) 2.32 0.002 55 11.2 (5.2-22.5) 0.94 0.877
High 1,257 5.4 (4.2-6.9) 48 17.0 (6.0-39.9) 3.62 0.038 17 5.9 (0.9-31.2) 1.11 0.916
Total 5,069 12.4 (11.2-13.7) 287 21.8 (16.2-28.7) 1.97 0.001 102 13.4 (6.9-24.5) 1.10 0.803
Language(s) spoken at home Only German (Ref.) German and further language(s) Only further language(s)
Sex Girls 2,560 10.4 (8.8-12.1) 358 17.2 (12.2-23.5) 1.79 0.012 53 23.4 (12.1-40.5) 2.65 0.021
Boys 2,380 12.9 (11.2-14.8) 300 21.6 (16.2-28.2) 1.86 0.004 36 21.8 (9.9-41.4) 1.88 0.187
Age group 11-13 years 2,257 9.8 (8.2-11.6) 299 16.7 (11.8-23.1) 1.85 0.007 37 19.5 (8.9-37.7) 2.24 0.094
14-17 years 2,683 13.0 (11.4-14.7) 359 21.2 (15.8-27.7) 1.80 0.005 52 23.9 (13.0-39.9) 2.11 0.057
SES Low 514 19.7 (16.1-23.9) 164 24.9 (17.8-33.8) 1.35 0.243 30 24.2 (11.0-45.2) 1.30 0.593
Medium 3,212 11.9 (10.5-13.6) 360 16.4 (11.9-22.1) 1.45 0.070 44 19.7 (9.3-37.0) 1.81 0.191
High 1,203 4.9 (3.7-6.5) 127 11.3 (5.6-21.6) 2.48 0.042 15 28.1 (9.9-58.2) 7.59 0.003
Total 4,940 11.7 (10.5-12.9) 658 19.4 (15.5-24.0) 1.83 < 0.001 89 22.7 (13.9-34.8) 2.23 0.010Bold = statistically significant in comparison to the reference group, CI = Confidence interval, OR = Odds ratio, Ref. = Reference group, SES = Socioeconomic status
Annex Table 2 Prevalence of overweight (including obesity) among 11- to 17-year-olds by sociodemographic and migration-related characteristics (n=3,010 girls, n=2,751 boys)Source: KiGGS Wave 2 (2014-2017)

26
FOCUSThe health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
n % (95% CI) n % (95% CI) OR p-value n % (95% CI) OR p-valueMigration background None (Ref.) One-sided Two-sided
Sex Girls 2,504 16.6 (14.8-18.6) 267 8.6 (5.4-13.2) 0.47 0.004 327 3.3 (1.7-6.4) 0.17 < 0.001
Boys 2,311 12.5 (10.6-14.6) 207 7.0 (4.0-11.9) 0.52 0.037 279 5.4 (2.7-10.5) 0.40 0.016
Age group 11-13 years 2,219 0.1 (0.0-0.3) 236 0.0 – – – 266 0.0 – – –
14-17 years 2,596 24.7 (22.6-27.0) 238 14.3 (10.0-20.2) 0.51 0.002 340 6.8 (4.2-10.8) 0.22 < 0.001
SES Low 487 16.4 (12.6-21.2) 63 4.2 (1.0-15.3) 0.22 0.038 197 2.6 (0.9-7.2) 0.14 0.001
Medium 3,158 15.0 (13.4-16.7) 277 9.9 (6.4-15.1) 0.63 0.058 325 6.2 (3.3-11.3) 0.38 0.006
High 1,159 11.6 (9.5-14.0) 131 5.4 (2.5-11.2) 0.44 0.045 78 5.2 (2.1-12.2) 0.42 0.071
Total 4,815 14.5 (13.2-15.9) 474 7.8 (5.4-11.2) 0.50 0.001 606 4.4 (2.7-7.1) 0.27 < 0.001
Parental length of stay in Germany > 20 years or entire life (Ref.) 11-20 years 0-10 yearsSex Girls 2,685 14.7 (13.0-16.6) 171 4.6 (2.3-8.9) 0.28 < 0.001 56 0.6 (0.1-4.4) 0.04 0.001
Boys 2,472 11.4 (9.6-13.4) 137 5.6 (1.9-15.4) 0.46 0.179 52 2.5 (0.3-16.3) 0.20 0.122
Age group 11-13 years 2,359 0.1 (0.02-0.3) 170 0.0 – – – 57 0.0 – – –
14-17 years 2,798 21.8 (19.7-24.0) 138 9.4 (5.0-17.1) 0.37 0.005 51 3.2 (0.6-15.5) 0.12 0.016
SES Low 535 11.8 (8.6-16.0) 97 4.5 (1.3-14.6) 0.35 0.128 32 0.0 – – –
Medium 3,342 14.0 (12.4-15.6) 158 5.5 (2.3-12.2) 0.36 0.024 59 2.8 (0.4-17.6) 0.18 0.092
High 1,268 10.8 (8.9-13.1) 51 6.4 (2.2-16.9) 0.56 0.307 16 3.9 (0.6-22.2) 0.34 0.272
Total 5,157 13.0 (11.7-14.4) 308 5.1 (2.7-9.5) 0.36 0.003 108 1.6 (0.3-8.2) 0.11 0.011
Language(s) spoken at home Only German (Ref.) German and further language(s) Only further language(s)
Sex Girls 2,622 15.8 (14.0-17.6) 380 5.4 (3.2-8.9) 0.31 < 0.001 55 1.6 (0.2-10.8) 0.09 0.017
Boys 2,403 12.3 (10.5-14.4) 317 3.6 (1.6-8.0) 0.26 0.002 40 8.1 (2.0-27.4) 0.63 0.539
Age group 11-13 years 2,317 0.1 (0.0-0.3) 0 0.0 – – – 42 0.0 – – –
14-17 years 2,708 23.8 (21.6-26.1) 328 7.6 (4.9-11.6) 0.26 < 0.001 53 6.7 (2.0-19.7) 0.23 0.021
SES Low 521 14.7 (11.2-19.0) 179 3.5 (1.5-7.7) 0.21 < 0.001 31 0.0 – – –
Medium 3,276 14.6 (13.0-16.3) 382 5.6 (3.1-10.0) 0.35 0.002 48 11.2 (3.7-29.5) 0.74 0.625
High 1,217 11.5 (9.6-13.9) 129 3.8 (1.7-8.5) 0.30 0.006 15 0.0 – – –
Total 5,025 14.0 (12.7-15.4) 697 4.5 (2.9-6.9) 0.29 < 0.001 95 4.5 (1.4-13.4) 0.29 0.044Bold = statistically significant in comparison to the reference group, CI = Confidence interval, OR = Odds ratio, Ref. = Reference group, SES = Socioeconomic status, AUDIT-C = Alcohol Use Disorder Identification Test (-Consumption)
Annex Table 3 Prevalence of risky alcohol consumption (AUDIT-C) among 11- to 17-year-olds by sociodemographic and migration-related characteristics (n=3,098 girls, n=2,797 boys)Source: KiGGS Wave 2 (2014-2017)

27
FOCUSThe health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
n % (95% CI) n % (95% CI) OR p-value n % (95% CI) OR p-valueMigration background None (Ref.) One-sided Two-sided
Sex Girls 2,547 78.9 (76.7-81.0) 268 84.1 (77.5-89.1) 1.41 0.127 324 80.3 (73.4-85.8) 1.09 0.699
Boys 2,335 77.6 (75.2-80.0) 207 74.1 (66.0-80.8) 0.82 0.336 268 74.0 (66.7-80.2) 0.82 0.324
Age group 11-13 years 2,267 81.3 (78.7-83.7) 239 85.0 (79.0-89.5) 1.30 0.229 256 81.3 (73.3-87.3) 1.00 0.997
14-17 years 2,615 76.1 (73.7-78.3) 236 74.5 (67.5-80.4) 0.92 0.630 336 75.1 (68.5-80.7) 0.95 0.776
SES Low 496 80.4 (74.9-85.0) 66 88.7 (78.2-94.5) 1.92 0.123 191 79.8 (72.0-85.8) 0.96 0.877
Medium 2,566 78.9 (76.9-80.9) 273 75.7 (69.8-80.8) 0.83 0.238 321 74.2 (66.7-80.5) 0.77 0.186
High 904 74.4 (70.8-77.7) 133 80.2 (70.0-87.5) 1.39 0.258 76 81.8 (71.9-88.7) 1.54 0.157
Total 4,882 78.3 (76.5-79.9) 475 79.4 (75.0-83.2) 1.07 0.623 592 77.2 (72.4-81.4) 0.94 0.687
Parental length of stay in Germany > 20 years or entire life (Ref.) 11-20 years 0-10 yearsSex Girls 2,724 79.6 (77.5-81.5) 167 84.5 (76.7-90.1) 1.40 0.209 57 63.7 (44.8-79.1) 0.45 0.049
Boys 2,494 76.8 (74.5-78.9) 131 75.7 (65.6-83.6) 0.94 0.824 49 79.3 (61.5-90.2) 1.16 0.752
Age group 11-13 years 2,407 81.5 (79.0-83.7) 164 82.8 (74.5-88.8) 1.09 0.744 54 78.6 (60.3-89.9) 0.84 0.705
14-17 years 2,811 75.9 (73.7-77.9) 134 78.2 (68.7-85.4) 1.14 0.607 52 65.5 (47.4-80.0) 0.61 0.199
SES Low 546 81.2 (75.6-85.8) 92 81.7 (70.3-89.4) 1.03 0.927 31 76.5 (51.7-90.8) 0.75 0.627
Medium 3,376 78.2 (76.2-80.2) 154 78.8 (70.2-85.4) 1.03 0.891 57 66.2 (49.0-79.9) 0.54 0.102
High 1,285 75.3 (71.9-78.4) 52 79.7 (66.5-88.6) 1.29 0.480 17 81.9 (57.0-93.9) 1.49 0.526
Total 5,218 78.1 (76.5-79.7) 298 80.3 (74.2-85.2) 1.14 0.495 106 71.6 (58.3-81.9) 0.70 0.259
Language(s) spoken at home Only German (Ref.) German and other language(s) Only other language(s)
Sex Girls 2,664 79.2 (77.0-81.2) 375 82.7 (77.6-86.9) 1.26 0.204 57 74.6 (56.5-86.9) 0.77 0.545
Boys 2,420 77.0 (74.6-79.3) 312 75.5 (68.8-81.2) 0.92 0.651 40 77.2 (59.7-88.5) 1.01 0.989
Age group 11-13 years 2,366 81.4 (78.9-83.6) 320 83.2 (76.5-88.2) 1.13 0.600 41 80.7 (62.6-91.3) 0.96 0.923
14-17 years 2,718 75.8 (73.4-78.0) 367 76.4 (70.5-81.4) 1.04 0.833 56 73.5 (58.5-84.5) 0.89 0.743
SES Low 532 80.1 (74.5-84.7) 171 83.3 (75.8-88.9) 1.24 0.445 33 76.8 (56.6-89.4) 0.82 0.698
Medium 3,307 78.5 (76.5-80.4) 381 74.6 (68.4-79.9) 0.80 0.194 47 79.6 (66.3-88.6) 1.07 0.854
High 1,234 75.1 (71.6-78.3) 130 84.3 (77.4-93.3) 1.77 0.016 16 55.8 (34.5-75.1) 0.42 0.058
Total 5,084 78.1 (76.4-79.7) 687 79.1 (75.0-82.7) 1.06 0.654 97 75.7 (63.9-84.6) 0.87 0.650Bold = statistically significant in comparison to the reference group, CI = Confidence interval, OR = Odds ratio, Ref. = Reference group, SES = Socioeconomic status
Annex Table 4 12-month prevalence of the utilisation of outpatient paediatric and/or general medical services among 11- to 17-year-olds by sociodemographic and migration-related characteristics (n=3,139 girls, n=2,810 boys)Source: KiGGS Wave 2 (2014-2017)

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
The health of children and adolescents with a migration background in GermanyJournal of Health Monitoring
28
FOCUS
The Robert Koch Institute is a Federal Institute within the portfolio of the German Federal Ministry of Health
This work is licensed under a Creative Commons Attribution 4.0
International License.
Imprint
Journal of Health Monitoring
PublisherRobert Koch InstituteNordufer 20 D-13353 Berlin, Germany
EditorsSusanne Bartig, Johanna Gutsche, Dr Birte Hintzpeter, Dr Franziska Prütz, Dr Martina Rabenberg, Dr Alexander Rommel, Dr Livia Ryl, Dr Anke-Christine Saß, Stefanie Seeling, Martin Thißen, Dr Thomas ZieseRobert Koch InstituteDepartment of Epidemiology and Health MonitoringUnit: Health ReportingGeneral-Pape-Str. 62–66D-12101 BerlinPhone: +49 (0)30-18 754-3400E-mail: [email protected]/journalhealthmonitoring-en
TypesettingGisela Dugnus, Kerstin Möllerke, Alexander Krönke
Translation Simon Phillips/Tim Jack
ISSN 2511-2708
Note External contributions do not necessarily reflect the opinions of the Robert Koch Institute.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
29
Health reporting on people with a migration background – Selection and definition of (core) indicators
AbstractAs part of the project Improving Health Monitoring in Migrant Populations (IMIRA), a (core) set of indicators was developed to describe the health of people with a migration background. This work was underpinned by research into and assessment of relevant data sources in the field of migration and health.Initially, four fields of action were identified together with a number of associated topics and potential indicators for each of the area’s individual topics. The choice of core indicators was based on (1) a systematic comparison of widely accepted indicator systems, (2) an assessment of public health relevance, (3) comprehensibility and (4) informative value, as well as (5) the availability of (largely) representative data that could properly account for the diversity of the migrant population. The (core) indicator set was finalised using an internal and external indicator development process that involved an interdisciplinary expert panel. This resulted in the selection of 25 core indicators; 41 additional indicators were documented as part of an ‘extended’ indicator set. The (core) set of indicators is to be continually developed in line with the work being undertaken to improve the integration of people with a migration background in the health monitoring conducted at the Robert Koch Institute. In the future, the indicator set is to be incorporated into an overall concept to regular, migration-related health reporting.
MIGRATION · PEOPLE WITH MIGRATION BACKGROUND · INDICATORS · HEALTH · HEALTH REPORTING
1. Introduction
Federal Health Reporting regularly provides information about the health of the population in Germany. It uses cur-rent representative data to describe temporal developments and to identify health policy areas where action needs to be taken. Evidence-based findings can be used to draw up measures aimed at improving and strengthening the health of the population and assessing the potential impact of these measures [1-3].
People with a migration background account for a sig-nificant proportion of the population in Germany: accord-ing to the microcensus, almost a quarter of the population in Germany (23.6%) was born either themselves or at least one parent without German citizenship. Almost half of the population with a migration background (48.9%) holds a foreign passport, and more than two-thirds moved to Germany themselves (68.4%) [4]. Through various factors, the cross-border relocation of a person’s permanent cen-tre of life (international migration) [5, 6] influences the life
Journal of Health Monitoring · 2019 4(3) DOI 10.25646/6073 Robert Koch Institute, Berlin
Susanne Bartig, Alexander Rommel, Annelene Wengler, Claudia Santos-Hövener, Thomas Lampert, Thomas Ziese
Robert Koch Institute, Berlin Department of Epidemiology and Health Monitoring
Submitted: 18.04.2019 Accepted: 19.06.2019 Published: 18.09.2019

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
30
situation of immigrants and the generation born in Ger-many before, during and after the biographical event of migration [7, 8].
Generalisations about the health of people with a migra-tion background cannot reflect the heterogeneity of this population group. The health chances and disease risks vary within the migrant population according to sociode-mographic and migration-related factors. As such, reliable data are crucial in order to identify health policy areas where action needs to be taken. However, very few sources of data (currently) exist that include both a repre-sentative sample of the migrant population and informa-tion about their health [9, 10]. At the 2015 Integration Sum-mit, representatives from politics, migrants’ organisations and the health sector emphasised the importance of ensur-ing that epidemiology and health reporting regularly con-sider the health of people with a migration background [11].
The Improving Health Monitoring in Migrant Popula-tions project (IMIRA, project duration 2016-2019), which was conducted at the Robert Koch Institute, aimed to improve the information available on the health of people with a migration background. One of the project's subgoals was the development of a concept for the regular health reporting on people with a migration background [12]. As part of the expansion of health reporting, a (core) set of indicators was developed to describe the health of people with a migration background, which is presented in this article. In the future, the (core) indicator set is to be inte-grated into Federal Health Reporting’s overall approach and will act as a framework that provides orientation for migration-related health reporting. The following questions were posed during the development of the set of indica-
tors: Which topics and indicators should be taken into account when describing the health of people with a migra-tion background? Which indicators are particularly relevant to migration-related health reporting (see Info box)? Which data sources are suitable for describing these indicators?
Following the principle of monitoring, a limited num-ber of meaningful and measurable core indicators have been selected [13, 14] to provide the most comprehensive overall picture possible of the health situation of people with a migration background. In addition to the core indi-cators, an ‘extended indicator set’ was also drawn up. In contrast to the core set of indicators, the extended set also includes conceptually relevant indicators for which no reli-able data sources could be identified (‘ideal type’ indica-tors). Therefore, in the context of this article, the umbrella term ‘(core) indicator set’ refers to both the ‘core indica-tors’ and the ‘extended indicator set’ for describing the health of people with a migration background.
2. The conceptual development of the (core) indicator set
The following provides more details about the individual steps that were undertaken to develop a (core) indicator set for migration-related Federal Health Reporting. In par-allel to the conceptual development of the (core) indicator set, a list of existing data sources (survey and routine data) was compiled before specific criteria were used to review their potential applicability to health reporting on people with a migration background (Figure 1).
The results from the review of the availability of relia-ble data in the field of migration and health were essen-tial to the selection of the core indicators. Due to their
Info box: Defining indicators and core indicators
Indicators are empirically measurable values that provide indications about issues that can-not be directly quantified or that are difficult to quantify [15, 16]. In this article, core indicators have high (1) public health relevance, (2) com-prehensibility, plausibility and (3) informative value, (4) are used at the national and inter-national level and (5) can be described using a representative data source. Furthermore, they have been identified as particularly relevant by an expert-supported procedure.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSJournal of Health Monitoring
31
Health reporting on people with a migration background – Selection and definition of (core) indicators
order to identify relevant topics for migration-related health reporting. A provisional selection of topics was made once these topics had been assigned to relevant fields of action. This selection depended on an assessment of a topic’s public health relevance but also took current research into the population with a migration background and the avail-ability of relevant indicators for each topic into account.
2.2 The development of the indicators and the derivation of the core indicators (steps 3 and 4)
In line with the ZWERG guidelines for indicator evaluation (central importance, efficiency, simplicity, timeliness, accu-racy) [20], ‘ideal type’ indicators were drawn up for each of the topics. These indicators have to be informative, easy to understand, comprehensible and relevant to the con-ception of public health policies (Figure 2). Due to the issues related to data availability (see Section 3), the extend-ed set of indicators also includes indicators that cannot currently be described by representative data. In contrast,
considerable importance for the development of the (core) indicator set, the data-specific challenges faced by migra-tion-related health reporting and the criteria-based selec-tion of data sources are explained in more detail below (see Section 3).
2.1 The identification of relevant fields of action and topics (steps 1 and 2)
Based on the World Health Organization’s (WHO's) [17-19] European guidelines on the health of people with a migra-tion background and the existing structure of Federal Health Reporting, four fields of action were identified that constituted the conceptual framework. These were: (1) pro-moting and strengthening health, (2) promoting and strengthening health-conscious behaviour, (3) promoting health-related resources and reducing risks, and (4) pro-moting equal access to health care services. Subsequently, nationwide reviews and explanatory approaches in the field of migration and health were systematically assessed in
In order to describe the health of the population as comprehensively as possible, a limited number of core indicators are to be used that account for the diversity found within the migrant population.
Figure 1Work steps for the development of a
(core) indicator set for migration-related health reporting
Source: Own diagram
1. Identification of relevant fields of action
2. Exploration of topics
Researchand
evaluation of
data sources
3. Development of indicators
4. Derivation of core indicators
5. Harmonisation of topics and indicators
6. Finalisation of the (core) indicator set

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
32
Economic Co-operation and Development (OECD) and the EU [24]. Additionally, the indicators published in the 2018 ‘Report on the health of refugees and migrants in the WHO European Region: no public health without refugee and migrant health’ were taken into account [25].
A research report was produced that includes the pub-lic health relevance for each topic, the state of scientific research with regard to the population with a migration background, an overview of the extended indicators and details of the conceptual approach used to derive the core indicators. Furthermore, profiles were compiled for each of the core indicators. In addition to the definition of the core indicator, these include recommendations on possible data
the existence of reliable data was an essential criterion for the selection of the core indicators (Figure 2). Furthermore, each core indicator was also derived conceptually on the basis of a comparison of established indicator systems that provided for an assessment of how widespread an indica-tor was at the national and international level. In addition to the Federal Health Reporting and the indicator set used by the Permanent Working Group of the Highest State Health Authorities (AOLG) [21], the review also considered the European Core Health Indicators (ECHI) of the Euro-pean Commission [22], the Core Health Indicators of the World Health Organization [23], and the core indicators (Health at a Glance) selected by the Organisation for
The availability of representative data is a crucial criterion in the selection of core indicators.
1. Identification of relevant fields of action
2. Exploration of topics
Researchand
evaluation of
data sources
3. Development of indicators
3. Development of indicators ▶ Public health relevance
▶ Comprehensibility and plausibility
▶ Informative value
4. Derivation of core indicators ▶ Availability of representative data
▶ National and international dissemination
4. Derivation of core indicators
5. Harmonisation of topics and indicators
6. Finalisation of the (core) indicator set
+
Figure 2Criteria for the development of indicators
and derivation of core indicatorsSource: Own diagram

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
33
Board were in the top categories (7-9). Topics that the Advi-sory Board deemed relevant for the description of the health of people with a migration background were taken into account in the final selection. However, topics were excluded if they could not be described with data from an adequate source. As such, the final selection of core indi-cators was based on the results from the internal and exter-nal indicator development process as well as on data avail-ability.
3. The selection of data sources for the (core) indicator set
Reliable data are essential for identifying health policy areas of action to strengthen the health of people with a migration background. However, the data situation is still inadequate [10, 26]. Only a few data sources are available that provide a comprehensive picture of both the health sit-uation and the migration background and permit differ-entiated analyses of subgroups within the migrant popu-lation, such as by country of origin or the length of stay in Germany.
3.1 Data-specific challenges in health reporting on peo-ple with a migration background
Official statistics and routine health care data (such as billing data) commonly only include information about citi-zenship, which means that it is impossible to identify spe-cific migrant subpopulations (such as naturalised citizens or ethnic German resettlers) within the data. In addition, due to a lack of information on the social situation, which
sources and a brief outline of the scientific background. These details provided the foundation for the internal and external indicator development process that was used to finalise the (core) indicator set.
The profile drawn up for the prevalence of obesity has been included in the Annex as an example (Annex Table 1). In addition, the research report, which among others includes a description of the criteria-based selection of (core) indicators, is available on the IMIRA website.
2.3 Harmonisation and finalisation of the (core) indicator set (steps 5 and 6)
The topics were analysed using a multi-step process: after they had been selected using a project-internal process, the various units at the Robert Koch Institute’s Department of Epidemiology and Health Monitoring also conducted a review of the selected topics. IMIRA’s Advisory Board was then asked to assess the topics for relevance and to select those that should be considered as part of migration-relat-ed health reporting. In a written, semi-standardised proce-dure, the Advisory Board used a 9-point scale ranging from 1 (not relevant) to 9 (highly relevant) to evaluate the rele-vance of the topics and their determinants for describing the health of people with a migration background. In addi-tion, once a particular field of action had been completed, an opportunity was provided to comment on or add to the topics. The Advisory Board was also informed that the aim of the process was to draw up a limited number of core topics from which a ‘lean’ set of indicators could be derived.
In the evaluation, topics were considered (highly) rele-vant if at least 60% of the ratings provided by the Advisory

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
34
data and data from official statistics was examined. In the review, data sources were included which (1) contained health-related information and (2) collected data on migra-tion background or migration-related characteristics (such as country of birth, length of stay in Germany or residency status). In addition, these data sources had to be nation-wide surveys of the entire population in order to enable a comparison between the population with and without a migration background and to apply the findings to Germa-ny as a whole (3). The results were harmonised with anoth-er review of data sources in the field of migration and health and published [35].
3.3 Evaluation of data sources
The data sources identified by the review were evaluated and prioritised using selected criteria. The aim was to describe the health of people with a migration background using data sources that were (1) up-to-date, (2) (largely) representative and (3) enable statements to be made according to subpopulations in order to take account of the diversity of this population group. In order to ensure representativeness, data sources that applied migra-tion-sensitive study designs were prioritised. To ensure representativeness studies that implemented specific measures to reach people with a migration background either during sampling (such as by oversampling people without German citizenship when using population regis-tries), or during the survey itself (such as by using multi-lingual survey tools) were prioritised. To adequately reflect the heterogeneity of the population with a migration back-ground, it should also be possible to make differentiated
has already been empirically proven as a relevant influenc-ing factor of health inequalities [27], the analysis of health- related routine data is clearly limited [28, 29]. Since the sole characteristic “migration background (yes vs. no)” is inad-equate for analysing health inequalities [30, 31], other migra-tion-related characteristics (e.g. country of birth, length of stay) must also be taken into account in addition to aspects of the social situation. People with a migration background are often underrepresented in (health) surveys; this means that the proportion of migrants in health surveys often does not correspond to their proportion of the population. This can be due to factors such as linguistic barriers in the pro-cess of data collection, which can lead to the systematic exclusion of people with a migration background [32-34]. A migration-sensitive study design, therefore, is essential if the population with a migration background is to be better integrated into surveys.
In line with the challenges identified above, data sources were assessed for their possible uses to migration-related health reporting. The following briefly outlines the proce-dure that was used to select relevant survey data for use in the health reporting on people with a migration back-ground.
3.2 A review of existing (health) surveys
A review was first undertaken of all potential data sources. In addition to the surveys conducted as part of the RKI’s health monitoring framework, surveys by other research institutions (such as the Socio-Economic Panel and the microcensus) were also taken into account. As part of another IMIRA subproject, the possibility of using routine
The diversity of the population with a migration background should be taken into account when describing health indicators.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
35
tor. The profiles produced for the core indicators contain the corresponding data sources with information on type of data, data holder and periodicity. In addition to the rec-ommended data sources, the profiles also include data sources that could still be used to describe the indicator but that do not apply a migration-sensitive study design.
4. Results
66 indicators were selected to describe the health of peo-ple with a migration background; 25 of these were defined as core indicators. An overview of the (core) indicators can be found in the Annex (Annex Table 3). Certain indicators are only relevant to children and adolescents (such as ear-ly detection examinations), others are only applicable to adults (such as cancer screening in general and cervical cancer screening).
4.1 Characteristics used for stratification
Alongside sociodemographic determinants, people with a migration background differ according to diverse migra-tion-related characteristics such as country of birth, migrant generation, length of stay, residency status, their motives for migration, and their German language skills [31, 42]. As such, different health opportunities and disease risks exist within the migrant population, which means that general-ising about the health of people with a migration back-ground produces inadequate results. In order to properly account for the diversity of the population with a migration background, analyses undertaken using the (core) indicator framework should be stratified by selected characteristics.
statements according to other relevant determinants of the health situation (migration-related and sociodemographic characteristics). A detailed description of the criteria-based assessment of each data source can be found in the research report published on IMIRA’s website.
3.4 The selection of data sources and their assignment to specific indicators
A total of 28 nationwide surveys (Annex Table 2) collect data on at least one health-related aspect in addition to characteristics that enable the identification of participants with a migration background [36]. However, there are clear differences between these data sources with regard to tar-get-group representativeness and the opportunities that they offer in terms of differentiated analyses by sociode-mographic and migration-related characteristics.
For the adult population, the criteria used for the anal-ysis led to the prioritisation of the microcensus [37], the Socio-Economic Panel (SOEP) [38, 39] and the German Health Interview and Examination Survey for Adults (DEGS1) [40]. If it is possible to describe an indicator with data from more than one source, the studies are listed in order of recommended use. The second wave of the Ger-man Health Interview and Examination Survey for Children and Adolescents (KiGGS Wave 2, 2014-2017), employed a migration-sensitive study design that led to an almost rep-resentative integration of families with a migration back-ground [41]. As such, it was selected as the preferred data source for describing the health of children and adolescents.
The prioritised data sources were compared for each topic, and recommendations were derived for each indica-
A total of 66 indicators were selected, 25 of which are core indicators.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
36
The mental health of people with a migration back-ground may be affected by specific psychosocial factors such as uncertainties about residency status, discrimina-tion and traumatic experiences. This particularly applies to refugees. Combined with social disadvantages, migra-tion-specific factors can place multiple burdens on people with a migration background [46-49]. However, in addition to migration-specific burdens, people with a migration background also have particular psychosocial resources that can have a significant impact on their mental wellbe-ing as well as their ability to cope with stress [50, 51]. In order to describe mental health, ‘lifetime prevalence of a depressive disorder (self-reported medical diagnosis)’ is recommended as the core indicator for adults with a migra-tion background. For children and adolescents, the ‘preva-lence of mental health problems in the last six months’ should be used. Furthermore, the use of the ‘lifetime preva-lence of anxiety disorders (self-reported medical/psycho-therapeutic diagnosis)’ is recommended.
Infectious diseases are a major cause of morbidity and mortality, particularly in countries with a low standard of living. In addition to the higher prevalence of certain infec-tious diseases in some countries of origin, both the migra-tion process itself and the conditions in the country of des-tination (such as shared accommodation) can increase the risk of infectious diseases [52, 53]. However, information about migration background is only available for a limited number of diseases that are subject to mandatory report-ing in accordance with the Protection against Infection Act [44, 53]. Data availability, established indicator systems, and the results of the interdisciplinary indicator develop-ment process, led to the selection of ‘tuberculosis cases
In addition to sex, age and socioeconomic status (low, medi-um, high), analyses should also provide for a differentiated description of migration background (population without a migration background, population with direct experi ences of migration, and second-generation migrants). Depend-ing on the health indicator in question and the opportuni-ties that the data offer for analysis, the following extended framework characteristics should be included in addition to country of birth: length of stay, residency status, the motive behind migration and self-assessed German lan-guage skills. This is important because aspects such as lin-guistic and structural barriers, which result from a person’s residency status, can have an impact on their utilisation of health care services [43, 44].
4.2 Promoting and strengthening health
‘Self-assessed general health as good to very good’ and the ‘12-month prevalence of chronic diseases in general’ were selected as core indicators to describe the general health of people with a migration background.
In the field of physical health (noncommunicable dis-eases), the following core indicators (each as self-reported medical diagnosis) have been derived on the basis of the
“world’s biggest killers” [45] named by the WHO and taking into account the still inadequate data quality for the pop-ulation with a migration background: the ‘lifetime preva-lence of heart disease, including cardiac insufficiency/heart failure’ and the ‘lifetime prevalence of stroke’ to map car-diovascular diseases, the ‘lifetime prevalence of bronchial asthma’ to map respiratory diseases and the ‘lifetime preva-lence of diabetes mellitus’.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
37
themselves) less frequently engage in sporting activities and tend to be more frequently affected by overweight and obesity (children and adolescents with a one-sided as well as two-sided migration background). They, however, con-sume less frequently alcohol in risky amounts (this applies to first- and second-generation migrants) [42, 56-58]. The ‘prevalence of risky alcohol consumption’ and the ‘preva-lence of current tobacco smoking (occasional to daily/reg-ular)’ are recommended as core indicators of substance use/addiction.
4.4 Promoting health-related resources and reducing risks
On the one hand, people with a migration background face specific health risks compared to the population without a migration background. On the other hand, people with a migration background have their own specific health- related resources [7, 59]. Alongside a rejection of substance use due to religious beliefs, which depends on the country of birth, and particular dietary habits, the resources that migrant populations may have include a pronounced level of social cohesion within the population itself. ‘A middle to high level of social support’ is a health-related resource [60] and was selected as the core indicator in the field of social and personal resources. Whereas no indicators asso-ciated with living and working conditions were classed as (highly) relevant, ‘experiences of discrimination (occasion-al to frequent)’ was selected as a core indicator of the migra-tion-specific burden faced by members of ethnic minorities.
among people born outside of Germany as a proportion of all tuberculosis cases’ as the core indicator of infectious diseases.
As citizenship is the only migration-related characteris-tic recorded in official statistics of life expectancy and causes of death, no core indicator was defined for mortal-ity. However, against the background of the limited infor-mative value of the available data sources, mean life expec-tancy at birth, standardised mortality rate, infant mortality, causes of death and deaths due to suicide were selected as extended indicators.
4.3 Promoting health-conscious behaviour
Previous research has identified marked differences in the migrant population in terms of dietary behaviour and phys-ical activity [42, 54, 55]. Therefore, the following core indi-cators were selected to ensure that migration-related health reporting regularly includes descriptions of dietary be -haviour and physical activity: the ‘prevalence of sporting inactivity’, ‘daily vegetable consumption’ as a predictor of healthy eating, and the ‘proportion of children who have been exclusively breastfed for at least six months in line with the World Health Organization’s recommendations’. Body mass index (BMI), a ratio of body weight to height (squared), is a measure used to classify underweight, normal weight, overweight and obesity. In addition to the ‘prevalence of overweight’, the ‘prevalence of obesity’ should also be taken into account when describing the BMI of people with a migration background. The current state of research indicates that people with a migration back-ground (especially people who experienced migration

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
38
Improving Health Monitoring in Migrant Populations (IMIRA) project conducted at the Robert Koch Institute. 25 core indicators were selected through a process based on the conceptual derivation of core indicators and an indi-cator development process undertaken together with an interdisciplinary panel of experts. In addition, an extended set of indicators was established that documents 41 addi-tional indicators that can be used to conduct a more in-depth analysis of a specific topic. The extended indicator set also contains a number of ‘ideal type’ indicators for which no reli able data source could be found.
A major challenge in the development of the set of (core) indicators was the availability of reliable data that provided for a representative description of people with a migration background and enable differentiated statements accord-ing to individual subpopulations. Deficits in the data par-ticularly exist in terms of indicator-based descriptions of health status and the utilisation of health services. Within the framework of the IMIRA project, feasibility studies were carried out into improving the integration of people with a migration background in the health monitoring under-taken at the Robert Koch Institute. The resulting findings will be integrated into the next nationwide interview and examination survey of the adult population (the Health and Nutrition Survey in Germany, gern survey). In addition, a survey sample will also be drawn of people without Ger-man citizenship. The aim is to collect representative data for the population with a migration background, with which statements can be made for specific groups within the migrant population [12]. Against this background, it can be assumed that the data available for describing the health of people with a migration background will improve in the
4.5 Promoting equal access to health care services
When utilising the services provided by the health care sys-tem, people with a migration background (especially peo-ple who experienced migration themselves) may face spe-cific barriers that make equal participation difficult. In addition to obstacles on the individual level, such as a lack of German language skills, experiences of discrimination and structural barriers (such as those associated with res-idency status) can have an impact on equal access to health care [44, 61-63].
In order to describe the migrant population’s utilisation of preventive services, the ‘full utilisation of the U3 to U9 early detection examinations’ and ‘vaccination rates for the first and second measles vaccinations’ were defined as core indicators for children. The ‘12-month prevalence of cervi-cal cancer screening’ was classed as particularly relevant during the international comparison of established indica-tor systems and the internal indicator development pro-cess. In addition, 'adherence with the recommended utili-sation of dental check-ups’ was also included as a core indicator. The ‘12-month prevalence of the utilisation of outpatient paediatric and general medical services’ was selected to describe the utilisation of health care services by children and adolescents; the ‘12-month prevalence of the utilisation of outpatient services from general practi-tioners’ was selected in this case for adults.
5. Conclusion and outlook
A (core) indicator set was drawn up to describe the health of people with a migration background as part of the
The (core) indicator set is to be integrated into an overall concept to regular, migration-related health reporting.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
39
Data protection and ethicsAll of the Robert Koch Institute’s studies are subject to strict compliance with the data protection provisions set out in the EU General Data Protection Regulation (GDPR) and the Federal Data Protection Act (BDSG). Charité – Universitätsmedizin Berlin’s ethics committee assessed and approved the ethics of the IMIRA feasibility study ‘inter-view survey’ (EA1/210/17). The Ethics Committee of the Berlin Chamber of Physicians assessed and approved the ethics of the IMIRA feasibility study ‘examination survey’ (Eth 21/17). Both study protocols were also assessed by the Federal Commissioner for Data Protection and Freedom of Information (13-401/008#0085). Participation in the studies was voluntary. The participants were also informed about the aims and contents of the study, and about data protection. Informed consent was obtained in writing.
FundingThe IMIRA project receives funding from the Federal Min-istry of Health (funding code: ZMVI1-2516FSB408).
Conflicts of interestThe authors declared no conflicts of interest.
AcknowledgementWe would like to thank the Advisory Board of IMIRA for participating in the semi-standardised procedure used to finalise the (core) indicator set.
future, which also goes hand in hand with the continuous development of the data-driven core indicator set.
In general, the quality of migration-related health report-ing depends on the existence of meaningful indicators that are based on representative data. Moreover, these indica-tors must enable differentiated statements according to relevant sociodemographic and migration-related charac-teristics in order to take into account the diversity of the population. Finally, health reporting should be undertaken in a sensitive and anti-discriminatory manner; this is par-ticularly important in the current climate of right-wing pop-ulist discourse. This entails critical reflection on the termi-nologies and categories employed by reporting as well as the avoidance of stigmatisation and marginalisation.
Corresponding authorSusanne Bartig
Robert Koch Institute Department of Epidemiology and Health Monitoring
General-Pape-Str. 62–66 D-12101 Berlin, Germany
E-mail: [email protected]
Please cite this publication asBartig S, Rommel A,Wengler A, Santos-Hövener C,Lampert T et al. (2019)
Health reporting on people with a migration background – Selection and definition of (core) indicators.
Journal of Health Monitoring 4(3): 29-48. DOI 10.25646/6073
The German version of the article is available at: www.rki.de/journalhealthmonitoring

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
40
12. Santos-Hövener C, Schumann M, Schmich P et al. (2019) Improving the information base regarding the health of people with a migration background. Project description and initial find-ings from IMIRA. Journal of Health Monitoring 4(1):46-57. https://edoc.rki.de/handle/176904/5915 (As at 04.04.2019)
13. Filsinger D (2014) Monitoring und Evaluation. Perspektiven für die Integrationspolitik von Bund und Ländern. WISO-Diskurs. Friedrich-Ebert-Stiftung, Bonn
14. Konferenz der für Integration zuständigen Ministerinnen und Minister/Senatorinnen und Senatoren der Länder (IntMK) (2019) Fünfter Bericht zum Integrationsmonitoring der Länder. Bericht 2019. Berichtsjahre 2015-2017. IntMK, Berlin. http://www.integrationsmonitoring-laender.de/berichte (As at 04.04.2019)
15. Kromrey H (2009) Empirische Sozialforschung. Modelle und Methoden der standardisierten Datenerhebung und Datenaus-wertung. Lucius und Lucius, Stuttgart
16. Meyer W (2004) Indikatorenentwicklung: Eine praxisorientierte Ein-führung. Arbeitspapiere 10. Centrum für Evaluation, Saarbrücken. https://www.ssoar.info/ssoar/handle/document/11124 (As at 04.04.2019)
17. World Health Organization, Regional Office for Europe (2016) Strategy and action plan for refugee and migrant health in the WHO European Region. WHO, Copenhagen
18. World Health Organization (2008) Resolution WHA61.17. Health of migrants. Sixty-first World Health Assemply. WHO, Geneva
19. World Health Organization (2008) Health of migrants. Report by the Secretariat. Sixty-first World Health Assembly. WHO, Geneva
20. Gesundheitsförderung Schweiz (2017) Projektziele formulieren. https://www.quint-essenz.ch/de/topics/1133 (As at 04.04.2019)
21. Arbeitsgemeinschaft der Obersten Landesgesundheitsbehörden (AOLG) (2003) Indikatorensatz für die Gesundheitsberichterstat-tung der Länder. Dritte, neu bearbeitete Fassung. Ministerium für Gesundheit, Soziales, Frauen und Familie des Landes Nord-rhein-Westfalen, Bielefeld
22. European Commission, Directorate-General for Health and Food Safety (2017) Health indicators. ECHI – European Core Health Indicators. https://ec.europa.eu/health/indicators/echi/list_en (As at 04.04.2019)
23. World Health Organization (2018) Global Reference List of 100 Core Health Indicators (plus health-related SDGs). WHO, Geneva. https://www.who.int/healthinfo/indicators/2018/en/ (As at 04.04.2019)
References1. Brand H, Michelsen K, Achterberg P et al. (2009) Policy Impact
Assessment of Public Health Reporting (PIA PHR). Final report. Institute of Health and Work NRW, Center for Public Health, Bielefeld
2. Lampert T, Horch K, List S et al. (2010) Federal Health Reporting: Objectives, Tasks and Uses. GBE Kompakt 1/2010. Robert Koch Institute, Berlin. https://edoc.rki.de/handle/176904/3092 (As at 04.04.2019)
3. World Health Organization (2008) Health Information Systems. Toolkit on monitoring health systems strengthening. WHO, Geneva
4. Statistisches Bundesamt (2018) Bevölkerung und Erwerbstätig-keit. Bevölkerung mit Migrationshintergrund – Ergebnisse des Mikrozensus 2017. Fachserie 1 Reihe 2.2. Destatis, Wiesbaden
5. Bundesministerium des Innern (2016) Migrationsbericht des Bundesamtes für Migration und Flüchtlinge im Auftrag der Bun-desregierung. Migrationsbericht 2015. BMI, Berlin. https://www.bamf.de/SharedDocs/Anlagen/DE/Publikationen/Migrationsberichte/migrationsbericht-2015.pdf?__blob=publica-tionFile (As at 04.04.2019)
6. Lederer HW (2004) Indikatoren der Migration. Europäisches Forum für Migrationsstudien, Bamberg
7. Schenk L (2007) Migration und Gesundheit – Entwicklung eines Erklärungs- und Analysemodells für epidemiologische Studien. International Journal of Public Health 52(2):87-96
8. Spallek J, Zeeb H, Razum O (2011) What do we have to know from migrants‘ past exposures to understand their health status? A life course approach. Emerg Themes Epidemiol 8(1):6
9. Brzoska P, Ellert U, Kimil A et al. (2015) Reviewing the topic of migration and health as a new national health traget for Germany. International Journal of Public Health 60(1):13-20
10. Die Beauftragte der Bundesregierung für Migration, Flüchtlinge und Integration (2016) 11. Bericht der Beauftragten der Bundes-regierung für Migration, Flüchtlinge und Integration – Teilhabe, Chancengleichheit und Rechtsentwicklung in der Einwanderungs-gesellschaft Deutschland. https://www.bundesregierung.de/resource/ (As at 04.04.2019)
11. Die Beauftragte der Bundesregierung für Migration, Flüchtlinge und Integration (2019) Gesundheit und Integration. Teilhabe an Präven-tion, medizinischer und pflegerischer Versorgung, Rehabilitation. https://www.integrationsbeauftragte.de/Webs/IB/DE/Themen/GesellschaftUndTeilhabe/Gesundheit/gesundheit_node.html (As at 04.04.2019)

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
41
34. Schenk L, Neuhauser H (2005) Methodische Standards für eine migrantensensible Forschung in der Epidemiologie. Bundes gesundheitsbl 48(3):279-286. https://edoc.rki.de/handle/176904/1091 (As at 04.04.2019)
35. Dyck M, Wenner J, Wengler A et al. (2019) Migration und Gesundheit in Deutschland – eine Bestandsaufnahme der Daten-quellen. Bundesgesundheitsbl (efirst)
36. Dyck M, Wenner J, Wengler A et al. (2019) Migration und Gesundheit in Deutschland – eine Bestandsaufnahme der Daten-quellen. Zusatzmaterial: Migration und Gesundheit in Deutsch-land – eine Bestandsaufnahme der Datenquellen. Bundes gesundheitsbl (efirst)
37. Forschungsdatenzentren der Statistischen Ämter des Bundes und der Länder (2017) Microcensus, 2013. https://www.forschungsdatenzentrum.de/en/household/microcensus (As at 20.11.2017)
38. Kroh M, Schupp J (2017) The SOEP Migration Survey and Refu-gee Sample. Report from the SOEP. In: Britzke J, Schupp J (Eds) SOEP Wave Report. DIW/SOEP, Berlin, P. 41-43
39. Liebau E, Tucci I (2015) Migrations- und Integrationsforschung mit dem SOEP von 1984 bis 2012: Erhebung, Indikatoren und Potenziale. SOEP Survey Papers, Series C – Data Documentation, DIW/SOEP, Berlin
40. Kamtsiuris P, Lange M, Hoffmann R et al. (2013) The first wave of the German Health Interview and Examination Survey for Adults (DEGS1) Sampling design, response, weighting, and representativeness. Bundesgesundheitsbl 56(5/6):620-630. https://edoc.rki.de/handle/176904/1519 (As at 04.04.2019)
41. Frank L, Yesil-Jürgens R, Born S et al. (2018) Improving the inclu-sion and participation of children and adolescents with a migra-tion background in KiGGS Wave 2. Journal of Health Monitoring 3(1):126-142. https://edoc.rki.de/handle/176904/5640 (As at 04.04.2019)
42. Rommel A, Saß AC, Born S et al. (2015) Die gesundheitliche Lage von Menschen mit Migrationshintergrund und die Bedeutung des sozioökonomischen Status. Erste Ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS 1). Bundes gesundheitsbl 58(6):543-552. https://edoc.rki.de/handle/176904/2383 (As at 04.04.2019)
43. Razum O, Wenner J, Bozorgmehr K (2016) Wenn Zufall über den Zugang zur Gesundheitsversorgung bestimmt: Geflüchtete in Deutschland. Gesundheitswesen 78(11):711-714
24. OECD/EU (2018) Health at a Glance: Europe 2018 – State of Health in the EU Cycle. OECD Publishing, Paris. https://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-europe-2018_health_glance_eur-2018-en (As at 04.04.2019)
25. World Health Organization, Regional Office for Europe (2018) Report on the health of refugees and migrants in the WHO Euro-pean Region: No public health without refugee and migrant health. WHO, Copenhagen. http://www.euro.who.int/__data/assets/pdf_file/0004/392773/ermh-eng.pdf?ua=1 (As at 04.04.2019)
26. Zeeb H, Razum O (2006) Epidemiologische Studien in der Migrationsforschung. Ein einleitender Überblick. Bundesgesundheitsbl 49 (9): 845-852.
27. Lampert T, Richter M, Schneider S et al. (2016) Soziale Ungleich-heit und Gesundheit. Stand und Perspektiven der sozialepide-miologischen Forschung in Deutschland. Bundesgesundheitsbl 59(2):153-165. https://edoc.rki.de/handle/176904/2478 (As at 04.04.2019)
28. Butler J, Albrecht NJ, Ellsäßer G et al. (2007) Migrationssensible Datenerhebung für die Gesundheitsberichterstattung. Arbeits-gruppe Gesundheitsberichterstattung des Arbeitskreises „Migra-tion und öffentliche Gesundheit“. Bundesgesundheitsbl 50(10):1232-1239
29. Reiss K, Makarova B, Spallek J et al. (2013) Identifizierung und Rekrutierung von Menschen mit Migrationshintergrund für epi-demiologische Studien in Deutschland. Gesundheitswesen 75(6):49-58
30. Razum O, Karrasch L, Spallek J (2016) Migration. Eine vernach-lässigte Dimension gesundheitlicher Ungleichheit. Bundes gesundheitsbl 59(2):259-265
31. Schenk L, Bau AM, Borde T et al. (2006) Mindestindikatorensatz zur Erfassung des Migrationsstatus. Empfehlungen für die epide-miologische Praxis. Bundesgesundheitsbl 49(9):853-860. https://edoc.rki.de/handle/176904/1061 (As at 04.04.2019)
32. Borde T (2006) Migrationssensible Studiendesigns – Wozu brau-chen wir welches Konzept? Migrationssensible Studiendesigns zur Repräsentation des Migrationsstatus in der Gesundheitsfor-schung – Tagung in Kooperation mit dem Robert Koch-Institut und dem Interdisziplinären Forschungsverbund Epidemiologie in Berlin (EpiBerlin) am 25 November 2005. RKI, Berlin, P. 15-23
33. Saß AC, Grüne B, Brettschneider AK (2015) Beteiligung von Men-schen mit Migrationshintergrund an Gesundheitssurveys des Robert Koch-Instituts. Bundesgesundheitsbl 58(6):533-542. https://edoc.rki.de/handle/176904/2385 (As at 04.04.2019)

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
42
56. Robert Koch-Institut (2015) Gesundheit in Deutschland. Gesund-heitsberichterstattung des Bundes. Gemeinsam getragen von RKI und Destatis. RKI, Berlin. https://edoc.rki.de/handle/176904/3248 (As at 04.04.2019)
57. Koschollek C, Bartig S, Rommel A et al. (2019) The health of chil-dren and adolescents with a migration background in Germany – Results of the cross-sectional KiGGS Wave 2 study. Journal of Health Monitoring 4(3):7-28. www.rki.de/journalhealthmonitoring-en (As at 18.09.2019)
58. Strupf M, Gomes de Matos E, Soellner R et al. (2017) Trinkverhal-ten von Personen verschiedener Herkunftsregionen in Deutsch-land: Ein Vergleich mit Personen ohne Migrationshintergrund. Suchttherapie 18(2):90-97
59. Spallek J, Razum O (2008) Erklärungsmodelle für die gesundheit-liche Situation von Migrantinnen und Migranten. In: Bauer U, Bittlingmayer UH, Richter M (Eds) Health Inequalities. Determi-nanten und Mechanismen gesundheitlicher Ungleichheit. VS Verlag für Sozialwissenschaften, Wiesbaden, P. 271-288
60. Borgmann L, Rattay P, Lampert T (2017) Social support as a health resource in Germany. Journal of Health Monitoring 2(4):110-115. https://edoc.rki.de/handle/176904/2920 (As at 04.04.2019)
61. Bermejo I, Hölzel LP, Kriston L (2012) Subjektiv erlebte Barrieren von Personen mit Migrationshintergrund bei der Inanspruchnah-me von Gesundheitsmaßnahmen. Bundesgesundheitsbl 55(8):944-953
62. Razum O, Geiger I, Zeeb H et al. (2004) Gesundheitsversorgung von Migranten. Deutsches Ärzteblatt 101(43):A2882–2887
63. Schouten BC, Meeuwesen L (2006) Cultural differences in medi-cal communication: A review of the literature. Patient Education and Counseling 64:21-34
44. Razum O, Zeeb H, Meesmann U et al. (2008) Migration und Gesundheit. Schwerpunktbericht der Gesundheitsberichterstat-tung. Robert Koch Institute, Berlin. https://edoc.rki.de/handle/176904/3194 (As at 04.04.2019)
45. World Health Organization (2013) Global action plan for the prevention and control of noncommunicable diseases 2013-2020. WHO, Geneva
46. Brzoska P, Reiss K, Razum O (2010) Arbeit, Migration und Gesundheit. In: Badura B, Schröder H, Klose J et al. (Eds) Fehl-zeiten-Report 2010. Vielfalt managen: Gesundheit fördern – Potenziale nutzen. Springer Verlag, Berlin Heidelberg, P. 129-139
47. Igel U, Brähler E, Grande G (2010) Der Einfluss von Diskriminie-rungserfahrungen auf die Gesundheit von MigrantInnen. Psychi-atrische Praxis 37(4):183-190
48. Schouler-Ocak M, Aichberger MC, Penka S et al. (2015) Psychi-sche Störungen bei Menschen mit Migrationshintergrund in Deutschland. Bundesgesundheitsbl 58(6):527-532
49. Spallek J, Razum O (2016) Migration und Gesundheit. In: Richter H, Hurrelmann K (Eds) Soziologie von Gesundheit und Krank-heit. Springer Fachmedien, Wiesbaden 2016, P. 153-166
50. Kirkcaldy B, Wittig U, Furnham A et al. (2006) Migration und Gesundheit. Psychosoziale Determinanten. Bundesgesund heitsbl 49(9):873-883
51. Singh S, McBride K, Kak V (2015) Role of Social Support in Exam-ining Acculturative Stress and Psychological Distress Among Asian American Immigrants and Three Sub-groups: Results from NLAAS. J Immigr Minor Health 17(6):1597-1606
52. European Centre for Disease Prevention and Control (2014) Assessing the burden of key infectious diseases affecting migrant populations in the EU/EEA. Technical Report. ECDC, Stockholm
53. Kuehne A, Fiebig L, Jansen K et al. (2015) Migrationshintergrund in der infektionsepidemiologischen Surveillance in Deutschland. Bundesgesundheitsbl 58(6):560-568. https://edoc.rki.de/handle/176904/2379 (As at 04.04.2019)
54. Winkler G (2003) Ernährungssituation von Migranten in Deutschland – was ist bekannt? Teil 1: Gesundheits- und Ernäh-rungssituation. Ernährungs-Umschau 50(5):170-175
55. Winkler G (2003) Ernährungssituation von Migranten in Deutschland – was ist bekannt? Teil 2: Ernährungsverhalten. Ernährungs-Umschau 50(6): 119-121

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
43
Annex Table 1 Example of a profile using the core indicator
obesity prevalenceSource: Own table
Indicator: Obesity prevalence
Type Core indicatorDimension Dietary behaviour and physical activityDefinition Proportion of adults with a BMI of 30kg/m² or higher; proportion of children and adoles-
cents with a BMI above the 97th percentile of the reference population
Data sources Adult population Children and adolescentsRecommended data sources Microcensus KiGGS
Data type Primary data (self-reported) Primary data (self-reported)Periodicity 4 years 5-6 yearsData owner German Federal Statistical Office Robert Koch Institute
Additional data sources SOEP, DEGS1 /
Data sources without a migration-sensitive field program
GEDA HBSC Studie
Scientific background
� The prevalence of obesity not only varies by migrant generation but also by country of birth.
� In addition, sex and age-specific effects on the prevalence of obesity can be observed within the migrant population.
References
– Kromeyer-Hauschild K, Moss A, Wabitsch M (2015) Referenzwerte für den Body-Mass-Index für Kinder, Jugendliche und Erwachsene in Deutschland: Anpassung der AGA-BMI-Referenz im Altersbereich von 15 bis 18 Jahren. Adipositas 9(3):123-127
– Schenk L, Neuhauser H, Ellert U (2008) Kinder- und Jugendgesundheitssurvey (KiGGS) 2003-2006: Kinder und Jugendliche mit Migrationshintergrund in Deutschland. Beiträge zur Gesundheitsberichterstattung des Bundes. RKI, Berlin
– Robert Koch-Institut (Ed) (2015) Gesundheit in Deutschland. Gesundheitsberichterstattung des Bundes. Gemeinsam getragen von RKI und Destatis. RKI, Berlin
BMI = Body Mass Index, SOEP = Socio-Economic Panel, DEGS1 = German Health Interview and Examination Survey for Adults, GEDA = German Health Update, KiGGS = German Health Interview and Examination Survey for Children and Adolescents, HBSC = Health Behaviour in School-aged Children

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
44
Annex Table 2 Overview of the sources identified during
the review of survey data in the field of migration and health
(in alphabetical order)Source: Own table
1) Alcohol survey – Federal Centre for Health Education (BZgA)2) Children of Immigrants Longitudinal Survey in Four European Countries (CILS4EU)3) Drug affinity among young people in the Federal Republic of Germany – Federal Centre for Health Education (BZgA)4) Epidemiological Survey of Substance Abuse in Germany (ESA)5) Eurobarometer6) European Social Survey (ESS)7) European Union Statistics on Income and Living Conditions (EU-SILC)8) European Values Survey (EVS)9) Gambling survey – Federal Centre for Health Education (BZgA)
10) Generations and Gender Survey (GGS)11) German Ageing Survey (DEAS)12) German General Social Survey (ALLBUS)13) German Health Interview and Examination Survey for Adults (DEGS1)/German National Health Interview and Examination
Survey 1998 (GNHIES98)14) German Health Interview and Examination Survey for Children and Adolescents (KiGGS)15) German Health Update (GEDA)16) German Oral Health study (DMS)17) German Survey on Volunteering (FWS)18) Health Behaviour in School-aged Children (HBSC)19) IAB-BAMF-SOEP Survey of Refugees in Germany – Institute for Employment Research (IAB), Socio-Economic Panel (SOEP) of
the German Institute for Economic Research (DIW Berlin) and the Research Centre on Migration, Integration, and Asylum of the Federal Office for Migration and Refugees (BAMF)
20) IAB-SOEP migration sample – Institute for Employment Research (IAB) and the Socio-Economic Panel (SOEP) of the German Institute for Economic Research (DIW Berlin)
21) leben in der Arbeit. German cohort study on work, age and health (lidA)22) Microcensus23) National Educational Panel Study (NEPS)24) Panel Analysis of Intimate Relationships and Family Dynamics (pairfam)25) Programme for the International Assessment of Adult Competencies (PIAAC)26) Socio-Economic Panel (SOEP)27) Study on Refugees 2014 by the Federal Office for Migration and Refugees (BAMF)28) Survey of Health, Ageing and Retirement in Europe (SHARE)

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
45
Annex Table 3 Overview of the (core) indicators for
the description of the health situation of people with a migration background by topic
and field of actionSource: Own table
Topic Indicator Data source adults/children
1. Promoting and strengthening health
1.1 General health
Subjective health Self-assessed general health (good to very good) SOEP/KiGGSHealth-related restrictions in everyday life (A)
Prevalence of health restrictions in everyday life (somewhat to severely limited) SOEP
Health-related quality of life Children/adolescents: total score from the Kidscreen 10 questionnaire (good to very good health-related quality of life)
KiGGS
Adults: total score from the Short Form 36 questionnaire (good to very good health-related quality of life)
DEGS1
Chronic diseases (general) 12-month prevalence of chronic diseases in general SOEP/KiGGS1.2 Physical health
Cardiovascular diseasesHeart disease (A)
Lifetime prevalence of heart disease, including cardiac insufficiency and heart failure (self-reported medical diagnosis)
SOEP
Stroke (A) Lifetime prevalence of stroke (self-reported medical diagnosis) SOEPHypertension (A) Lifetime prevalence of hypertension (self-reported medical diagnosis) SOEP
Cancer (A) Lifetime prevalence of cancer (self-reported medical diagnosis) SOEP
Respiratory diseasesBronchial asthma Lifetime prevalence of bronchial asthma (self-reported medical diagnosis) SOEP/KiGGSChronic obstructive pulmonary disease (COPD)
Lifetime prevalence of chronic obstructive pulmonary disease (self-reported medical diagnosis)
/
Diabetes mellitus Lifetime prevalence of diabetes mellitus (self-reported medical diagnosis) SOEP/KiGGSAllergic diseases Lifetime prevalence of at least one allergic disease (self-reported medical diagnosis) DEGS1/KiGGSMusculoskeletal conditions: joint disease (A) Lifetime prevalence of musculoskeletal disorders (self-reported medical diagnosis) SOEP
Injuries Accident rate Microcensus/ KiGGS
1.3 Mental health
Depressive disorder (A) Lifetime prevalence of a depressive disorder (self-reported medical diagnosis) SOEPAnxiety disorders Lifetime prevalence of anxiety disorders (self-reported medical/psychotherapeutic diagnosis) DEGS1/KiGGSPost-traumatic stress disorders Lifetime prevalence of a post-traumatic stress disorder /Dementias Prevalence of dementia /Mental health problems (C) Prevalence of mental health problems in the last six months
(total score from the Strengths and Difficulties Questionnaire)KiGGS
Attention Deficit Hyperactivity Disorder (ADHD) (C)
Lifetime prevalence of self-reported medical diagnosis of ADHD KiGGS
DEGS1 = German Health Interview and Examination Survey for Adults, KiGGS = German Health Interview and Examination Survey for Children and Adolescents, SOEP = Socio-Economic Panel Bold = core indicators, C = only relevant to children and adolescents, A = only relevant to adults

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
46
Topic Indicator Data source adults/children
1.4 Infectious diseases
Tuberculosis Tuberculosis cases among people born outside of Germany as a proportion of all tuberculosis cases Registration data held in accordance with the Protection against Infection Act
HIV/AIDS New diagnoses of HIV among people of non-German origin as a proportion of total new HIV diagnoses Registration data held in accordance with the Protection against Infection Act
Hepatitis A Hepatitis A cases among people with a migration background as a proportion of all hepatitis A cases
Syphilis (A) Syphilis cases among people of non-German origin as a proportion of all syphilis casesVaccine-preventable childhood diseases (C)
Lifetime prevalence of vaccine-preventable childhood diseases (measles, mumps, rubella, whooping cough)
KiGGS
1.5 MortalityLife expectancy Mean life expectancy at birth in years (German vs non-German citizenship) Official birth and
death statisticsMortality rate Standardised mortality rate (German vs non-German citizenship)Infant mortality (C) Infant mortality per 1,000 live births (German vs non-German citizenship)Causes of death Five most common causes of death (German vs non-German citizenship) Causes of death
statisticsSuicide Deaths due to suicide (German vs non-German citizenship)
2. Promoting health-conscious behaviour
2.1 Dietary behaviour and physical activity
Physical (in)activity Prevalence of adherence to the World Health Organization’s recommendations on physical activity DEGS1/KiGGSSporting (in)activity Prevalence of sporting inactivity (no sports to very rarely) SOEP/KiGGSFruit consumption Daily fruit consumption DEGS1/KiGGSVegetable consumption Daily vegetable consumption DEGS1/KiGGSBreastfeeding (C) Proportion of children who have been exclusively breastfed for at least six months in line with the
World Health Organization’s recommendationsKiGGS
Consumption of sugary soft drinks
Daily consumption of sugary soft drinks DEGS1/KiGGS
Body Mass Index (BMI)Prevalence of overweight Microcensus/KiGGSPrevalence of obesity Microcensus/KiGGS
2.2 Substance use/addiction
Tobacco use Prevalence of current tobacco smoking (occasional to daily/regular) Microcensus/KiGGSAlcohol consumption Prevalence of risky alcohol consumption (risk-related consumption) SOEP/KiGGSAlcohol consumption Prevalence of heavy episodic drinking SOEP/KiGGSConsumption of illicit drugs
Lifetime prevalence of illicit drug use (excluding cannabis use) Epidemiological Survey of Sustance Abuse/Drug Affinity Study
Problematic, pathological gambling (A)
Proportion of people with at least problematic gambling behaviour Gambling Survey
HIV = Human Immunodeficiency Virus, AIDS = Acquired Immune Deficiency Syndrome, DEGS1 = German Health Interview and Examination Survey for Adults, KiGGS = German Health Interview and Examination Survey for Children and Adolescents, SOEP = Socio-Economic PanelBold = core indicators, grey lettering = data sources with a low data quality rating for migration and health issues, C = only relevant to children and adolescents, A = only relevant to adults
Annex Table 3 Continued Overview of the (core) indicators for
the description of the health situation of people with a migration background by topic
and field of actionSource: Own table

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
47
Topic Indicator Data source adults/children
3. Promoting health-related resources and reducing risks
3.1 Social and personal resources
Health literacy A score of sufficient or above on the overall index in the short version of the survey used in the European Health Literacy Study (HLS-EU-Q16)
/
Social support A middle to high level of social support DEGS1/KiGGSReligiousness Subjectively rated religiousness (religious to very religious) SOEP/-
3.2 Living and working conditions
Workload (A) Prevalence of subjectively perceived health risk of employment GEDALiving environment Subjective impact of noise pollution from road traffic (moderate to very strong) DEGS1/KiGGS
3.3 Migration-specific, psychosocial burdensExperiences of discrimination Experiences of discrimination (occasional to frequent) SOEP/KiGGSSense of belonging/ feeling of not belonging
A feeling of affiliation to the country of origin vs a feeling of affiliation to Germany SOEP/-
4. Promoting equal access to health care services
4.1 Utilisation of preventive services
Vaccinations (A) Vaccination rates for seasonal influenza /Vaccinations (C) Vaccination rates for the first and second measles vaccinations KiGGS
Vaccinations (C)Prevalence of self-reported full vaccination against human papillomavirus (HPV) KiGGSVaccination rates – complete primary immunisation against tetanus KiGGS
Early detection examinations (C) Full utilisation of the U3 to U9 early detection examinations KiGGSCancer screening (general) (A) Regular utilisation of cancer screening DEGS1Cervical cancer screening (A) 12-month prevalence of cervical cancer screening DEGS1Prenatal care (A) Number of prenatal medical examinations (at least five) /Dental check-ups (C) Adherence with the recommended utilisation of dental check-ups KiGGS
4.2 Utilisation of health care services
Outpatient care (paediatrics, general) (C)
12-month prevalence of the utilisation of outpatient paediatric and general medical services KiGGS
Outpatient care (general) (A) 12-month prevalence of the utilisation of outpatient services from general practitioners DEGS1Inpatient care 12-month prevalence of the utilisation of hospital treatment DEGS1/KiGGSPsychosocial/ psychotherapeutic care
12-month prevalence of the utilisation of services from medical or psychological psychotherapists DEGS1/KiGGS
Unmet needs 12-month prevalence of unmet care needs GEDARehabilitative care (A) Utilisation of a rehabilitation measure in the last three years (inpatient or outpatient) DEGS1Geriatric nursing care (A) Proportion of the total population in need of nursing care (nursing quota) /
DEGS1 = German Health Interview and Examination Survey for Adults, GEDA = German Health Update, KiGGS = German Health Interview and Examination Survey for Children and Adole-scents, SOEP = Socio-Economic PanelBold = core indicators, grey lettering = data sources with a low data quality rating for migration and health issues, C = only relevant to children and adolescents, A = only relevant to adults
Annex Table 3 Continued Overview of the (core) indicators for
the description of the health situation of people with a migration background by topic
and field of actionSource: Own table

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSHealth reporting on people with a migration background – Selection and definition of (core) indicatorsJournal of Health Monitoring
48
The Robert Koch Institute is a Federal Institute within the portfolio of the German Federal Ministry of Health
This work is licensed under a Creative Commons Attribution 4.0
International License.
Imprint
Journal of Health Monitoring
PublisherRobert Koch InstituteNordufer 20 D-13353 Berlin, Germany
EditorsSusanne Bartig, Johanna Gutsche, Dr Birte Hintzpeter, Dr Franziska Prütz, Dr Martina Rabenberg, Dr Alexander Rommel, Dr Livia Ryl, Dr Anke-Christine Saß, Stefanie Seeling, Martin Thißen, Dr Thomas ZieseRobert Koch InstituteDepartment of Epidemiology and Health MonitoringUnit: Health ReportingGeneral-Pape-Str. 62–66D-12101 BerlinPhone: +49 (0)30-18 754-3400E-mail: [email protected]/journalhealthmonitoring-en
TypesettingGisela Dugnus, Kerstin Möllerke, Alexander Krönke
Translation Simon Phillips/Tim Jack
ISSN 2511-2708
Note External contributions do not necessarily reflect the opinions of the Robert Koch Institute.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
49
Concepts for migration-sensitive health monitoring
AbstractAccording to microcensus data, nearly one quarter of the German population has a migration background. This means that either themselves or at least one parent was born without German citizenship. Based on the currently available data and due to the underrepresentation of specific population groups, representative findings on the health of the total population residing in Germany are only possible to a limited degree. Against this backdrop, the Robert Koch Institute initiated the Improving Health Monitoring in Migrant Populations (IMIRA) project. The project aims to establish a migration-sensitive health monitoring system and to better represent people with a migration background in health surveys conducted by the Robert Koch Institute. In this context it is crucial to review and further develop relevant migration-sensitive concepts and appropriate surveying instruments. To achieve this, the concepts of acculturation, discrimination, religion and subjective social status were selected. This article theoretically embeds these concepts. Furthermore, we describe their application in epidemiology as well as provide a proposal on how to measure and operationalise these concepts. Moreover, recommendations for action are provided regarding the potential application of these concepts in health monitoring at the Robert Koch Institute.
MIGRATION · HEALTH MONITORING · ACCULTURATION · DISCRIMINATION · SUBJECTIVE SOCIAL STATUS
1. Introduction
Since its founding, the Federal Republic of Germany has been an immigration country [1]. Based on microcensus data, in 2017, around 19.3 million people living in Germa-ny have a migration background [2]. This means that either themselves or at least one parent was born without Ger-man citizenship. Due to the heterogeneity of this popula-tion group, general statements on the health of people with a migration background should be avoided. However, numerous studies that applied a more nuanced analysis of living situations show that disease risks and health resources can vary depending on a set of factors such as
region of origin, reasons for migration as well as people’s experiences before, during and after migration.
In studies on health status, health behaviour, the utili-sation of medical services, health pro motion and preven-tion services in the general population, people who are included in the category “migration background” are so far mostly underrepresented. In spite of this population group comprising around one quarter of the total population, val-idated data is nonetheless lacking [3, 4]. Surveys on migra-tion and health tend to merely consider whether a person has a migration background (yes/no), an approach that does not adequately reflect the heterogeneity of people liv-ing in Germany [5].
Journal of Health Monitoring · 2019 4(3) DOI 10.25646/6075 Robert Koch Institute, Berlin
Maria Schumann *, Katja Kajikhina *, Antonino Polizzi, Navina Sarma, Jens Hoebel, Marleen Bug, Susanne Bartig, Thomas Lampert, Claudia Santos-Hövener
* contributed equally
Robert Koch Institute, Berlin Department of Epidemiology and Health Monitoring
Submitted: 07.03.2019 Accepted: 16.05.2019 Published: 18.09.2019

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
50
Against this backdrop, the Robert Koch Institute (RKI) initiated the Improving Health Monitoring in Migrant Pop-ulations (IMIRA) project. The objective is to establish migration-sensitive health monitoring, better reach people with a migration background and include them in Robert Koch Institute health surveys on a longitudinal basis [5-7]. One of the IMIRA sub-projects aims to adapt and further develop concepts (sub-project 2) of migration-sensitive health monitoring. The objective is to identify migra-tion-sensitive concepts that would reach beyond the min-imum indicator set currently applied to operationalise migration background as developed by Schenk et al. [8]. Beyond citizenship and country of birth, the indicator set contains parent’s country of birth, year of immigration to Germany, German as mother tongue (yes/no), self- assessed German language proficiency (very good, good, average, poor, very poor) and residency status (temporary, permanent, German citizenship) [8]. Additionally, research into the current scientific literature led to the identification of further relevant concepts in the field of migration and health. Among these were the concepts of acculturation, discrimination, religion as well as subjective social status. The aim is to better illustrate important aspects of the dif-ferent living situations of the population living in Germany and to better explain health inequalities.
The concepts identified, their operationalisation and measurement as well as the recommendations to establish migration-sensitive health monitoring at the RKI are based on an ideal approach that, potentially, will be applied in the future. This would provide opportunities to use the chosen items on migration history (including country of birth, citizenship, duration of stay) and discrimination experi-
ences as well as sense of belonging, religion and subjective social status within future health surveys by the RKI. Already, the relevant dimensions of the concepts identified have largely become part of the core indicator set used to anal-yse the health of people with a migration background in health reporting (see the article Health reporting on peo-ple with a migration background – Selection and definition of (core)indicators in this issue). Besides migration back-ground, these include the country of birth, German lan-guage proficiency, social networks as well as discrimination experiences. Duration of stay, residency status, reasons for migrating, feeling of belonging and religion are all part of the extended indicator set.
This article presents the selected concepts in more detail. It provides a theoretical basis, an overview of the concept’s application in epidemiology thus far as well as a proposal for measurement and operationalisation. Surveying instru-ments were selected based on both previous research find-ings and ethical principles developed by civic organisations. Moreover, they were cognitively tested and subsequently optimised in the six languages (Arabic, German, Italian, Croatian, Polish and Turkish) which correspond to the over-all population for the upcoming Health and Nutrition Sur-vey in Germany (gern survey), a joint study by the Robert Koch Institute and the Max Rubner Institute. Cognitive testing included interviews of participants of different age, sex and educational levels who were native speakers of the six languages mentioned. After completing the written questionnaire, which contained all the items to be tested, respondents were asked about their feelings, understand-ing of the questions and how to answer them using a stan-dardised interview guide. The partial transcripts were then

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
51
Multidimensional approaches take this one step further and consider additional dimensions that are surveyed inde-pendently [26]. All approaches have in common that they attempt to calculate an acculturation score and provide a statement on a person’s degree of acculturation.
As part of IMIRA sub-project 2, a systematic review of the literature was conducted to (1) provide an overview of the degree to which the concept of acculturation has already been used in epidemiologic research on the health of peo-ple with a migration background; (2) identify the different options of operationalising and measuring the concept of acculturation; and (3) develop recommendations to survey the concept of acculturation in the context of health sur-veys in Germany (original papers with quantitative approaches in German and English; search strategy apply-ing a combination of terms such as acculturation, migra-tion, method, health; specialised data bases MEDLINE, SCOPUS and Science Direct; further information and cri-teria can be found at [27]).
2.1 Operationalising and measuring acculturation
The majority of the studies identified were conducted in the US, yet a few also in Europe. These mainly analyse the links between the acculturation of diverse groups of peo-ple with a migration background and/or who have different ethnic backgrounds with regard to different health out-comes. Due to significant inconsistencies related to the definition, operationalisation and measurement of the con-cept in the studies considered, no general statements on the impact of processes of acculturation on the health of people with a migration background are possible [16, 26, 28].
qualitatively analysed using the Constant Comparative Method [9]. Based on these findings the questionnaire was then adapted where necessary. The article closes with rec-ommendations on those aspects that should be considered when using the presented concepts in epidemiological research.
2. Acculturation
Originally, the concept of acculturation was developed in British and North American anthropology as an attempt to describe the process of cultural changes in people as a result of the contact between people from different cultures dur-ing the colonial era at the end of the 19th century [10, 11]. Today, the concept has been applied in numerous further disciplines, such as medicine, psychology, public health and epidemiology [12, 13]. Numerous studies on the connection between acculturation and health have been conducted [14-20]. The results show great inconsistencies regarding the direction and strength of effects shown [21]. General conclusions regarding the interdependencies between acculturation and health are therefore not possible [22].
In principle, there are three distinguishable theoretical approaches. One-dimensional approaches describe accul-turation as a linear continuum stretching from not accultur-ated to acculturated. These approaches view acculturation as a process of transition from a person’s original culture to the new one [23]. Two-dimensional approaches of accul-turation in turn understand acculturation as a process tak-ing place on two different planes. People with a migration background thereby integrate elements of the new culture as well as discard elements of their original culture [24, 25].

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
52
2.2 Operationalisation and measurement of relevant dimensions
Migration historyFor migration history, the variables within the minimum indicator set by Schenk et al. [8] were revised and supple-mented. Beyond country of birth and citizenship, parents’ country of birth as well as data on the year of immigration to Germany would be collected. Collecting data on parent citizenship is also recommended. Furthermore, this data would allow researchers to calculate how long a person has been in the country of residence, the number of years that have passed since migration and their age at immigration. Regarding residency status, we would basically apply the categories developed by the Federal Office for Migration and Refugees (BAMF), yet adapt them where necessary [31]. Cognitive testing indicated that translated questionnaires should also provide the answer categories in German. Fre-quently, respondents learn the German terminology of resi-dency regulations (for example Erlaubnis zum Daueraufent-halt in der Europäischen Union, Aufenthaltsgestattung or Duldung) after arriving in Germany and therefore appear to use them mostly in German. Often, they either do not know or there is no equivalent term in their native language. A new aspect would also be to collect data on the reasons for migration (motivation). The motivating reasons for migration we propose are also based on the categories of surveys by BAMF (for employment, training, according to international law, humanitarian or political refugees, family, late repatriates or other reasons) [32]. Following cognitive testing, these were supplemented by further frequently men-tioned reasons such as the answer ‘to have a better future’.
For example, these studies have used a diverse set of proxy variables and acculturation scales. These are used to col-lect data on migration history, language, (ethnic) back-ground and a person’s social environment. Based on these dimensions, an acculturation score is then usually calcu-lated that aims to provide statements on a person’s degree of acculturation. In this context, however, it remains unclear how the multiple dimensions relate to each other and whether changes in one dimension (such as greater lan-guage proficiency) also lead to changes in other dimen-sions (such as stronger social networks) [29, 30].
Due to the numerous gaps regarding the theoretical establishment of the concept of acculturation, the incon-sistencies related to its operationalisation and measure-ment as well as a critical discussion of an approach that generalises and categorises people as members of a ‘cul-ture’ (based on ascribed and often ethicising traits), we have decided not to introduce the concept of acculturation as such or to calculate an acculturation score in the health studies of the Robert Koch Institute. Nonetheless, our review identified four thematic dimensions within the scales measuring acculturation in the literature. Based on those, proxies and items were identified that we intend to survey within future migration-sensitive health monitoring. These would be a person’s migration history, their language skills (German and native language), subjective feeling of belonging and social support. These relevant factors need to be taken into consideration when explaining differences in health/health outcomes of people with a migration back-ground.
Relevant migration-related characteristics such as language, sense of belonging and migration history should be surveyed without making generalising statements on degrees of ‘acculturation’.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
53
as well as the representative survey Ausgewählte Migranten-gruppen in Deutschland (RAM 2015) by the Federal Office for Migration and Refugees (BAMF). The item ‘How strong-ly do you feel you are a part of German society?’ would be followed by a five item Likert scale (very strongly, strongly, partly, barely, not at all). The feeling of belonging to the country of origin would also be implemented by using a corresponding answer scale based on the IAB-SOEP migra-tion sample template and the RAM of the BAMF: ‘And how strongly do you feel you are a part of the society of your country of origin (i.e. the country in which you or your par-ents were born)?’ It is thereby important to recognise that surveying a subjective feeling of belonging in the context of health is relevant not only for people with a migration background. The subjective feeling of belonging also influ-ences the health of other population groups, which is why surveying this feeling should not be limited to the migra-tion sample.
Social support A person’s social environment emerged as the fourth glob-al dimension from the review of the literature on the con-cept of acculturation. This included proxies as well as items within acculturation scales that survey for example the ori-gin of friends or people in the neighbourhood, or contact with family members in the country of origin, but also knowledge of political and social questions, dietary habits and other items that aim to operationalise belonging to a culture. These questions on the social environment oper-ationalised in this manner are only posed to people with a migration background. The reason behind these questions is an idea of fixed and generalisable traits and social
LanguageLanguage surveying was also further developed. The min-imum indicator set [8] only collected data on German as a native language (yes/no) as well as a person’s self-assessed German language skills (very good, good, average, poor, very poor). We now recommend a four-step approach. In a first step, data on a person’s native language would be collected by asking ‘Which language is your native lan-guage?’ followed by a list of ten languages plus a box to enter any other language. The ten languages selected would cover the most frequently spoken languages in the overall population including German. These would include Arabic, Italian, Croatian, Polish and Turkish. In a second step, like in the minimum indicator set, respondents would be asked to self-assess their language proficiency. This would initial-ly aim to collect data on German proficiency based on Brand et al. [15] by using the item ‘How good do you think your German is?’ on a five item answer scale (very good, good, average, poor, very poor). The third step would con-sist of surveying a person’s native language (except Ger-man) with the item ‘How well do you speak your native language (except German)?’ followed by the same five pos-sible answers. Moreover, the language used during the interview (or in the questionnaire) would be established as a proxy variable.
Feeling of belongingFrom our perspective, surveying the subjective feeling of belonging in German society should be conducted analo-gous to the migration sample of the Institute for Employ-ment Research (IAB), the Socio-Economic Panel (SOEP) of the German Institute for Economic Research (DIW Berlin)

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
54
concerning the methodological and ethical recommenda-tions to collect data on discrimination, the instruments applied would have to be optimised in terms of the dimen-sions surveyed and the terminology used [35, 36].
An analysis of current research regarding the link between discrimination and health was carried out (reviews and orig-inal studies, search strategy using combined MeSH terms such as discrimination, racism, health, mental health, healthcare, gender, socioeconomic status, MEDLINE data-base). In addition, different survey instruments were com-pared and discussed that have already been used in repeated representative surveys in Germany, including the RKI’s KiGGS study and the surveys by the Socio-Economic Panel, by the Berlin Institute for Integration and Migration Research, as well as the Federal Government’s anti-discrimination agency. Furthermore, a summary of the recommendations on methodological and ethical principles to survey ethnic-ity and anti-discrimination data that have been developed for German-speaking countries by civil society institutions, the federal anti-discrimination agency and research institu-tions was developed [35-37].
3.1 Operationalising and measuring subjectively per-ceived discrimination
The majority of studies were published in North America, with a smaller number coming from European countries. They show a clear correlation between discrimination and health when outcomes such as mental health, overall/phys-ical health, health behaviour and use of healthcare and pre-vention services are considered. A variety of scales, indi-vidual items and instruments are used to operationalise
interactions that are thought to define or nullify a supposed belonging to a category ‘culture’ which itself is based on unclear assumptions and attributions.
Against this backdrop, we recommend mapping the social environment as part of an approach for migra-tion-sensitive health monitoring at the Robert Koch Insti-tute based on social support and using none of the above-mentioned ‘acculturation’ items. These would – as done in previous health surveys of the RKI – be surveyed according to the Oslo 3 Social Support Scale. The scale is an instrument frequently applied in Europe to measure perceived social support [33, 34]. Participants thereby answer three questions with a four item response format on the number of people they would consider themselves close to or people that they can rely on, how many other people are in their lives and the availability of neighbour-hood assistance.
3. Discrimination
Interpersonal and structural discrimination play a crucial role in physical and mental health. People can suffer from racist discrimination independently of whether they have a migration background according to the the current micro-census definition or not (for example on grounds of origin, appearance, accent, name). Surveying data on discrimina-tion in the context of health monitoring at the RKI poten-tially provides a basis to analyse perceived discrimination and the health of those affected. At the RKI, subjectively felt discrimination has been surveyed once in the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). However, it became clear that,
Surveying (anti-)discrimina-tion data provides the basis for a more differentiated analysis of the health of a heterogeneous population.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
55
and applied to some concrete settings, for example, to inves-tigate discrimination in a medical setting [42]. The frequency of experiences of discrimination is surveyed with a 5-item Likert scale (very often, often, sometimes, rarely, never).
The following question asks about the possible reasons for the reported experiences also with regard to possible ascriptions and allows multiple answers: ‘What do you think was the main reason for these experiences? (Multi-ple answers possible. Please also consider how others pos-sibly see you)’. We also formulate answers according to the established item set of the everyday discrimination scale [40, 41] as well as based on the six categories of the general equal treatment act: ‘sex’, ‘origin, accent, language, appearance, name’, ‘religion’, ‘chronic disease, impair-ment', ‘sexual orientation’, ‘age’ and supplement these with ‘weight’, socioeconomic status (‘education, income’) and ‘unemployment’.
We would also expand the instrument to include ques-tions on the frequency of discrimination experiences in the health and care sector and in contact with authorities: ‘How often have you been treated unfairly or worse than other people in the following situations? In the health or care sector (for example during a doctor’s appointment, at hos-pital, assisted living, care facility), during contacts with public offices or authorities (e.g. registration offices, immi-gration offices, job centres, police)’. The frequency of expe-rienced discrimination will again be surveyed by using the Likert scale. These questions aim to collect data in the fields particularly relevant to health monitoring. Potentially, it will enable the identification of subjectively perceived barriers to access healthcare and health services due to discrimi-nation. Yet discrimination also has public health relevance
perceived discrimination as subjectively worse or less favourable treatment in everyday life, in relevant areas of life (offices, shops) or disadvantage in structural areas such as the housing market or in professional life. Studies sur-vey the possible grounds for discrimination as well as the frequency of experienced discrimination. A large number of publications explicitly examines the connection between racial discrimination and health [38, 39].
There are important methodological and ethical aspects to consider when collecting anti-discrimination data. Infor-mation needs to be provided voluntarily, external ascrip-tions have to be avoided and the relevant groups should participate in developing the content and instruments, data collection and analysis. Ensuring an intersectional perspec-tive, i.e. collecting data on all dimensions of discrimination without limiting the perspective to single factors such as migration background or country of origin is also essential [35].
On this basis, we have developed a proposal for a three stage approach. Initially, we would survey the subjectively perceived frequency of interpersonal discrimination expe-riences in people’s everyday lives by applying the 5-item everyday discrimination scale [40, 41]. The scale asks ‘In your day-to-day life how often have any of the following things happened to you?’ and offers the following situations as answers: ‘You receive poorer service than other people at restaurants or stores.’, ‘You are treated with less respect’, ‘People act as if they think you are not smart.’, ‘People act as if they are afraid of you. ’, ‘You are threatened/harassed’. This 5-item variant of the scale has been widely used in Eng-lish-speaking countries and validated for numerous popu-lation groups. Moreover, the scale has already been adapted

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
56
and life satisfaction is, however, of particular health rele-vance. We are therefore considering including the question: ‘How important is religion for your everyday well-being and life satisfaction?’ followed by a four item answer scale (very important, slightly important, not so important, not impor-tant at all). The survey conducted by the Socio-Economic Panel on religion as a resource of social cohesion already applied this question in this manner [47].
5. Subjective social status
Numerous empirical studies consistently show that peo-ple with a low socioeconomic status (SES) face an increased risk of developing disease and dying at a younger age [48-51]. Conceptually, SES is understood as a multidimen-sional construct and classically measured based on the three ‘objective’ indicators of education, occupation and income [52, 53]. SES measurement is therefore based on factors that significantly influence the position of people at the ‘top and bottom’ of society [54]. Using objective SES indicators attributes a status position to people. However, this attribution is not always congruent with how people assess their own status. To account for this subjective perspective, health research is increasingly supplement-ing objective SES indicators with subjective status indica-tors [55-57]. Subjective social status (SSS) indicates where people see themselves on the social ladder and the status group they feel they belong to.
Research in recent years indicates that a lower SSS, inde-pendently of objective SES, is associated with poorer phys-ical and mental health [55, 56, 58-60]. Such an association between SSS and health has also been observed among
in people’s dealings with administrative offices, institutions and public facilities, for example when applying for health services. These two structural areas were selected follow-ing the evaluation of the cognitive pre-tests conducted with relevant groups of persons.
4. Religion
The term religion is defined as the belief in a higher power resulting from belonging to a religious creed such as Chris-tianity, Islam, Judaism, Buddhism or Hinduism [43]. Dur-ing recent years, a series of empirical studies has investi-gated the influence of religion on physical and mental health as well as mortality [44-46].
According to the proposal for health monitoring at the RKI, the initial question will address the belonging to one of the religious creeds. Similar to the study Deutschland postmigrantisch by the Forschungsgruppe Junge Islambe-zogene Themen in Deutschland (JUNITED) at the Berlin Institute for Integration and Migration Research (BIM) at the Humboldt University of Berlin, one question would have to be: ‘What is your religion?’ The possible answers would be the five major world religions (Christianity, Islam, Judaism, Hinduism, Buddhism), plus the options ‘any other religion’, ‘no religion’, as well as ‘I prefer not to answer this question’. Originally, our concept foresaw surveying par-ticipation in community life as a further social resource. However, the results of the cognitive pre-tests showed that the translations of the concept of community life give rise to very different associations. As a result, this question was not included in the set of recommended questions. The question of the connection between religion, well-being
Religion can influence health and serves as an important explanatory factor for health differences.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
57
would position themselves on this social ladder. The texts contained in the MacArthur Scale thereby explicitly refer-ence the classical socioeconomic factors of education, occupation and income. Relative self-assessment general-ly takes place with regard to the society of the country in which respondents live. The MacArthur Scale can thus be applied to people with and without a migration background. Figure 1 shows the German version of the MacArthur Scale which has been used in RKI surveys to collect data on SSS in Germany and which has already been tested for con-struct validity in the general population [57].
5.2 Measuring hypothetical SSS in the country of origin
One US study [69] applied a MacArthur Scale-based ques-tionnaire to collect data on subjective social status. At the point of interview, people who have migrated were asked to assess what their current social position in their country of origin would be if they had continued to live there [70]. Figure 2 shows the adapted version of the instrument in German, which has already been applied in an RKI feasi-bility study. While country of residence SSS data is collect-ed independently by health studies and can be used as an (in)dependent variable, collecting data on the hypothetical, country of origin SSS of migrants is generally not done separately, but in combination with measuring country of residence SSS.
One question that can be addressed by combining both items is, for example, whether a discrepancy between the hypothetical SSS in the country of origin and the SSS in the country of residence has a health impact. For some immi-grant population groups in the US, it has been observed
people with a migration background [61]. The association is not only evident in cross-sectional studies. Observations from longitudinal studies and experimental studies also indicate that SSS has an independent effect on health and disease risks [62-65]. It is assumed that a low SSS reflects perceived social disadvantages and relative deprivation, which in turn cause feelings of injustice, anger, inferiority or shame [66-68]. Permanent or recurring feelings of this kind could lead to a chronic state of stress and thus to an increased risk of disease for people with low SSS [68]. Partly, however, SSS could also express aspects of socioeconomic conditions that are not covered by the three classic SES indi-cators such as wealth, over-indebtedness or social security.
Often it is difficult to assess people’s SES prior to migra-tion, i.e. in their country of origin. Generally, it is difficult to translate their socioeconomic conditions in their coun-tries of origin to the context of their country of residence, such as educational attainment or the status their occupa-tion grants them. In these cases, SSS could provide an adequate and, for research, pragmatic solution. It should be noted, however, that SSS cannot fully substitute objec-tive SES indicators, especially as the effects of objective and subjectively perceived living conditions on health would then become indistinguishable.
5.1 Measuring SSS in the country of residence (Germany)
In health research and epidemiology, the MacArthur Scale of Subjective Social Status has internationally established as the standard instrument to measure SSS [55, 56]. The instrument includes a ladder with ten rungs representing social structure. Interviewees are asked to mark where they
Data on subjective social status can help analyse the effects of perceived social conditions and social mobility on the health of people with a migration history.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
58
that on average the health of people who consider their status in the country of residence to be lower than their hypothetical status in their country of origin is poorer [70, 71]. The control group was comprised of migrants not perceiv-ing such a status discrepancy. However, this association played out differently depending on the country of origin [70]. So far, the mechanisms underlying these results have not been sufficiently clarified. Possibly, however, perceived downward social mobility due to migration or counterfac-tual thinking (‘Had I never migrated...’) could be psycho- social stressors that impact the health of migrants.
6. Methodological outlook
A sustained discussion on the diversity of our society in the context of epidemiologic and public health research hinges on a continuous reflection of the concepts and categories applied, and on avoiding ascriptions-based generalisations. The concepts presented in this article are an important development of the conceptual basis of health monitoring at the RKI which allow an inclusion of several migration-sen-sitive components. The discussion of various migration-sen-sitive concepts and surveying instruments should provide a basis to better account for the heterogeneity and diversi-ty of people in Germany in future data collection and anal-ysis. Even though the large number of migration-related questions might increase the probability of non-response, and thus the generation of unusable data, it does provide more detailed insights into one’s history of migration (for example duration of stay, residency status or motives for migration). This should enable a better understanding of the concomitant health effects far beyond the indicator of
Figure 2 Adapted version of the MacArthur Scale to
assess the subjective assessment of the hypothetical social status in the country of
origin for people with a migration background*
Source: Own figure
*The text is a translation based on the German-language version of the questionnaire item. It has not yet been validated for use in questionnaire surveys and is only included in this manuscript for reasons of readability.
Figure 1German version of a MacArthur Scale to assess
the subjective social status of adultsSource: Hoebel et al. 2015 [57]
Think of a ladder with 10 rungs representing where people stand in Germany.
At the top of the ladder are the people who are the best off – those who have the most money, the most education and the most respected jobs. At the bottom are the people who are the worst off – who have the least money, least education, and the least respected jobs or no job.
The higher up you are on this ladder, the closer you are to the people at the very top; the lower you are, the closer you are to the people at the very bottom.
Where would you place yourself on this ladder?
Please indicate the rung where you think you stand at this time in your life, relative to other people in Germany.
Now think of the country you moved from, that is, your country of origin. Think of a ladder with 10 rungs represent-ing where people stand in your country of origin today.
At the top of the ladder are the people who are the best off – those who have the most money, the most education and the most respected jobs. At the bottom are the people who are the worst off – who have the least money, least education, and the least respected jobs or no job.
The higher up you are on this ladder, the closer you are to the people at the very top; the lower you are, the closer you are to the people at the very bottom.
Where would you place yourself on this ladder? Please indicate the rung where you think you stand if you were still in your country of origin today.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
59
need to include new forms of reachability, discrimina-tion-free settings and accessibility of surveys in different languages [35]. Using questionnaires in various languages requires a methodological discussion of the specific demands of questionnaire translation. Instead of a word-for-word translation, the aim will generally be for an idiomatic translation, i.e. one that clearly renders the mean-ing and concepts of a text in the foreign language. Within the IMIRA project, a standard operation procedure was developed that considers the team approach (also called committee approach) as an important element in the idiomatic translation of questionnaires. It intends to involve several native translators with different qualifications in the translation process to prevent translations from being both too vague and having too much of a personal style [72]. Finally, the quality of the instruments - with regard for exam-ple to validity - should also be proven for the translated versions. Cognitive pre-testing with participants from all relevant language groups including German should allow the identification of where improvements can be made.
Beyond translations, this applies to the entire research process. The participation of people with a migration back-ground as well as of those who are affected by racist dis-crimination, yet who are not included in the migration back-ground category according to the definition, would be essential to optimise research settings. This applies as much to the development and establishment of migra-tion-sensitive concepts as to the application, evaluation and communication of the results. Furthermore, attention should be paid to discrimination-free framework settings for interviews, for example by training the intercultural and communicative capacities of interviewers [35].
migration background (yes/no) or of a generation within a family that has migrated. Factors such as the subjective belonging to a group and discrimination, religious creed as well as subjective social status may also be important fac-tors to explain differences in health outcomes between peo-ple with and without a history of migration. This will allow for a more detailed description of these factors for example in the context of health survey data collection also with regard to possible interdependencies and correlations, such as the connection between subjective social status and discrimination or a person’s feeling of belonging to the society. The concepts developed should potentially provide a basis to portray the health resources and burdens as well as the needs and requirements of diverse population groups in a more differentiated way. RKI health survey data could contribute to future discussions on equity in health and social participation as well as discrimination. Using the described concepts, the basis for further differentiated data analyses of the health of people with migration background can be improved, also enabling a responsible communica-tion of the results to researchers, politics and the broader public. From our perspective, several concepts should not be used exclusively for people with a migration background but applied in perspective to all population groups, since some of them - such as discrimination or religion - impact the health of all people living in Germany.
When applying these concepts to improve the migra-tion-sensitivity of health monitoring at the RKI and public health research in general, some methodological questions need to considered, which we discuss in the following. It will be important to create adequate framework condi-tions and adapt questionnaire instruments, measures that
In a longer term perspective, the concepts presented are to be applied not merely in surveys related to migration, but to all population groups.

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
60
Data protection and ethicsAll of the Robert Koch Institute’s studies are subject to strict compliance with the data protection provisions set out in the EU General Data Protection Regulation (GDPR) and the Federal Data Protection Act (BDSG). Cognitive pre-tests were conducted by the market and social research institute USUMA in Berlin. USUMA conducts surveys strict-ly in accordance with the provisions of DIN ISO 20252 ‘Market and social research services’, the agreed guidelines of the working group Deutscher Markt- und Sozial-forschungsinstitute e.V. (ADM) as well as the internation-al code of the International Chamber of Commerce (ICC) and the European Society for Opinion and Market Research (ESOMAR) for market and social research.
In particular, all stages of the project fulfil the following guidelines:
� International code of the ICC/ESOMAR for market and social research and the declaration for the territory of the Federal Republic of Germany regarding the ICC/ESOMAR as well as data analytics (‘German Declara-tion’)
� ISO 20252 quality standards (standards regarding qual-ity assurance in market and social research)
� Guideline on the Treatment of Addresses in Market and Social Research
� Regulation of the European Parliament and of the Coun-cil on the protection of individuals with regard to the processing of personal data and the free movement of such data (GDPR).
Approval by an ethics committee was not required as the pre-tests did not require the collection of personal data.
In the future, beyond the four concepts presented here, it will be necessary to consider further aspects. These could include, for example, social resources and coping strategies, vigilance, resilience and self-efficacy. These approaches are part of a necessary shift of focus in the discourse on health and migration, which is too often focused on deficits, towards a capacities and resources oriented perspective.
Addressing the diversity of the population in the context of epidemiological analyses will require new approaches. Intersectional perspectives for example should, where pos-sible, also be applied in epidemiology - social categories need to be analysed not separately but with regard to how they intersect each other. This emphasises the need for a discussion of how to apply and bring together a diverse set of analytical approaches in quantitative health research [73]. The analyses of different health settings may better reflect the situation of the population as a whole.
Corresponding authorMaria Schumann
Robert Koch Institute Department of Epidemiology and Health Monitoring
General-Pape-Str. 62–66 D-12101 Berlin, Germany
E-mail: [email protected]
Please cite this publication asSchumann S, Kajikhina K, Polizzi A, Sarma N, Hoebel J et al. (2019)
Concepts for migration-sensitive health monitoring. Journal of Health Monitoring 4(3): 49-65.
DOI 10.25646/6075
The German version of the article is available at: www.rki.de/journalhealthmonitoring

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
61
8. Schenk L, Bau AM, Borde T et al. (2006) Mindestindikatorensatz zur Erfassung des Migrationsstatus - Empfehlungen für die epidemiologische Praxis. Bundesgesundheitsbl 49(9):853-860
9. Ridolfo H, Schoua-Glusberg A (2011) Analyzing Cognitive Interview Data Using the Constant Comparative Method of Analysis to Understand Cross-Cultural Patterns in Survey Data. Field Methods 23(4):420-438
10. Redfield R, Linton R, Herskovits MJ (1936) Memorandum for the study of acculturation. Am Anthropol 38(1):149-152
11. Häußling R, Oberwittler D, Antweiler C et al. (2016) In: Kopp J, Steinbach A (Eds) Grundbegriffe der Soziologie. VS Verlag für Sozialwissenschaften, Wiesbaden, P. 1-24
12. Henry JP, Cassel JC (1969) Psychosocial factors in essential hypertension recent epidemiologic and animal experimental evidence. Am J Epidemiol 90(3):171-200
13. Abraido-Lanza AF, Armbrister AN, Florez KR et al. (2006) Toward a theory-driven model of acculturation in public health research. Am J Public Health 96(8):1342-1346
14. Ahluwalia IB, Ford ES, Link M et al. (2007) Acculturation, weight, and weight-related behaviors among Mexican Americans in the United States. Ethn Dis 17(4):643-649
15. Brand T, Samkange-Zeeb F, Ellert U et al. (2017) Acculturation and health-related quality of life: results from the German National Cohort migrant feasibility study. Int J Public Health 62(5):521-529
16. Carter-Pokras O, Zambrana RE, Yankelvich G et al. (2008) Health status of Mexican-origin persons: do proxy measures of accultur-ation advance our understanding of health disparities? J Immigr Minor Health 10(6):475-488
17. Kim MJ, Lee SJ, Ahn YH et al. (2007) Dietary acculturation and diet quality of hypertensive Korean Americans. J Adv Nurs 58(5):436-445
18. Lesser IA, Gasevic D, Lear SA (2014) The association between acculturation and dietary patterns of South Asian immigrants. PLoS One 9(2):e88495
19. Morawa E, Erim Y (2014) Acculturation and depressive symp-toms among Turkish immigrants in Germany. Int J Environ Res Public Health 11(9):9503-9521
20. Sussman NM, Truong N (2011) “Please extinguish all cigarettes”: The effects of acculturation and gender on smoking attitudes and smoking prevalence of Chinese and Russian immigrants. Int J Intercult Relat 35(2):163-178
Participation in the studies was voluntary. The participants were also informed about the aims and contents of the study, and about data protection. Informed consent was obtained in writing.
FundingThe IMIRA project receives funding from the Federal Min-istry of Health (funding code: ZMVI1-2516FSB408).
Conflicts of interestThe authors declared no conflicts of interest.
References1. Spallek J, Razum O (2016) Migration und Gesundheit. In:
Richter M, Hurrelmann K (Eds) Soziologie von Gesundheit und Krankheit. Springer Fachmedien Wiesbaden, Wiesbaden, P. 153-166
2. Statistisches Bundesamt (2018) Bevölkerung mit Migrations-hintergrund. Ergebnisse des Mirkozensus 2017. Fachserie 1, Reihe 22. Destatis, Wiesbaden
3. Razum O, Bunte A, Gilsdorf A et al. (2016) Gesundheitsversor-gung von Geflüchteten: Zu gesicherten Daten kommen. Dtsch Arztebl International 113(4):130-133
4. Saß AC, Grüne B, Brettschneider AK et al. (2015) Beteiligung von Menschen mit Migrationshintergrund an Gesundheitssurveys des Robert Koch-Instituts. Bundesgesundheitsbl 58(6):533-542. https://edoc.rki.de/handle/176904/2385 (As at 12.06.2019)
5. Santos-Hövener C, Schumann M, Schmich P et al. (2019) Improving the information base regarding the health of people with a migration background. Project description and initial findings from IMIRA. Journal of Health Monitoring 4(1):46-57. https://edoc.rki.de/handle/176904/5915 (As at 12.06.2019)
6. Butler J, Albrecht NJ, Ellsäßer G et al. (2007) Migrationssensible Datenerhebung für die Gesundheitsberichterstattung. Bundesgesundheitsbl 50(10):1232-1239
7. Schenk L, Neuhauser H (2005) Methodische Standards für eine migrantensensible Forschung in der Epidemiologie. Bundesgesundheitsbl 48:279-286

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
62
33. Dalgard OS, Dowrick C, Lehtinen V et al. (2006) Negative life events, social support and gender difference in depression: a multinational community survey with data from the ODIN study. Soc Psychiatry Psychiatr Epidemiol 41(6):444-451
34. Kilpeläinen K, Aromaa A and and the ECHIM Core Group (2008) European health indicators: development and initial implementa-tion: final report of the ECHIM project. National Public Health Institute, Helsinki. https://www.uzis.cz/cz/echim/final-report.pdf (As at 12.06.2019)
35. Baumann AL, Egenberger V, Supik L (2018) Erhebung von Antidiskriminierungsdaten in repräsentativen Wiederholungs-befragungen. Bestandsaufnahme und Entwicklungsmöglich-keiten. Antidiskriminierungsstelle des Bundes, Berlin. http://www.antidiskriminierungsstelle.de/SharedDocs/Down-loads/DE/publikationen/Expertisen/Datenerhebung.pdf?__blob=publicationFile&v=3 (As at 12.06.2019)
36. Ahyoud NA, Kwesi J, Bartsch S et al. (2018) Wer nicht gezählt wird, zählt nicht. Antidiskriminierungs- und Gleichstellungsdaten in der Einwanderungsgesellschaft – eine anwendungsorientierte Einführung. Vielfalt entscheidet – Diversity in Leadership, Citizens For Europe, Berlin. https://www.kultur-oeffnet-welten.de/media/material-down-loads/antidiskriminierungs_-_gleichstellungsdaten_-_einfueh-rung.pdf (As at 12.06.2019)
37. Supik L (2017) Statistik und Diskriminierung. In: Scherr A, El-Mafaalani A, Yüksel G (Eds) Handbuch Diskriminierung. Springer Fachmedien Wiesbaden, Wiesbaden, P. 191-207
38. Paradies Y, Ben J, Denson N et al. (2015) Racism as a Determi-nant of Health: A Systematic Review and Meta-Analysis. PLOS ONE 10(9):1-48
39. Pascoe E, Smart-Richman L (2009) Perceived discrimination and health: a meta-analytic review. Psychol Bull 135:531-554
40. Sternthal MJ, Slopen N, Williams DR (2011) Racial Disparities in Health: How Much Does Stress Really Matter? Du Bois Rev 8(1):95-113
41. Williams DR, Yu Y, Jackson JS et al. (1997) Racial Differences in Physical and Mental Health: Socioeconomic Status, Stress, and Discrimination. J Health Psychol 2(3):335-351
42. Peek ME, Nunez-Smith M, Drum M et al. (2011) Adapting the everyday discrimination scale to medical settings: reliability and validity testing in a sample of African American patients. Ethn Dis 21(4):502-509
21. Fox M, Thayer Z, Wadhwa PD (2017) Assessment of accultura-tion in minority health research. Soc Sci Med 176:123-132
22. Hunt LM, Schneider S, Comer B (2004) Should “acculturation” be a variable in health research? A critical review of research on US Hispanics. Soc Sci Med 59(5):973-986
23. Gordon MM (1964) Assimilation in American Life: The Role of Race, Religion, and National Origins. Oxford University Press, New York
24. Berry JW (1997) Immigration, Acculturation, and Adaptation. Appl Psychol 46(1):5-34
25. Sam DL (2006) Acculturation: Conceptual background and core components. In: Berry JW (Ed) The Cambridge handbook of acculturation psychology. Cambridge University Press, New York, P. 11-26
26. Thomson MD, Hoffman-Goetz L (2009) Defining and measuring acculturation: a systematic review of public health studies with Hispanic populations in the United States. Soc Sci Med 69(7):983-991
27. Schumann M, Bartig S, Bug M et al. (2018) Acculturation in epidemiological research among migrant populations: a systematic review. https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=88234 (As at 12.09.2018)
28. Phinney JS (1996) When we talk about American ethnic groups, what do we mean? Am Psychol 51(9):918-927
29. Fox M, Thayer Z, Wadhwa PD (2017) Acculturation and health: the moderating role of socio-cultural context. Am Anthropol 119(3):405-421
30. Schwartz SJ, Unger JB, Zamboanga BL et al. (2010) Rethinking the concept of acculturation: implications for theory and research. Am Psychol 65(4):237-251
31. Bundesamt für Migration und Flüchtlinge (BAMF) (2019) Aufenthalt in Deutschland. http://www.bamf.de/DE/Willkommen/Aufenthalt/WichtigeInfor-mationen/wichtigeinformationen-node.html;jsessionid=D0D8B-53CD2E825523D063B31D419E2BE.2_cid294 (As at 25.02.2019)
32. Bundesministerium des Innern (Ed) (2015) Migrationsbericht des Bundesamtes für Migration und Flüchtlinge im Auftrag der Bundesregierung. Migrationsbericht 2013. BMI, Berlin. http://www.bamf.de/SharedDocs/Anlagen/DE/Publikationen/Migrationsberichte/migrationsbericht-2013.pdf?__blob=publica-tionFile (As at 12.06.2019)

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
63
55. Adler NE, Epel ES, Castellazzo G et al. (2000) Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy, white women. Health Psychol 19(6):586-592
56. Hegar R, Mielck A (2010) „Subjektiver sozialer Status“. Stellen-wert für die Untersuchung und Verringerung von gesundheit-licher Ungleichheit. Präv Gesundheitsf 5(4):389-400
57. Hoebel J, Müters S, Kuntz B et al. (2015) Messung des subjekti-ven sozialen Status in der Gesundheitsforschung mit einer deutschen Version der MacArthur Scale. Bundesgesundheitsbl 58(7):749-757
58. Zell E, Strickhouser JE, Krizan Z (2018) Subjective social status and health: a meta-analysis of community and society ladders. Health Psychol 37(10):979-987
59. Tang KL, Rashid R, Godley J et al. (2016) Association between subjective social status and cardiovascular disease and cardio-vascular risk factors: a systematic review and meta-analysis. BMJ Open 6(3):1-14
60. Cundiff JM, Matthews KA (2017) Is subjective social status a unique correlate of physical health? A meta-analysis. Health Psychol 36(12):1109-1125
61. Leu J, Yen IH, Gansky SA et al. (2008) The association between subjective social status and mental health among Asian immigrants: investigating the influence of age at immigration. Soc Sci Med 66(5):1152-1164
62. Singh-Manoux A, Marmot MG, Adler NE (2005) Does subjective social status predict health and change in health status better than objective status? Psychosom Med 67(6):855-861
63. Nobles J, Weintraub MR, Adler NE (2013) Subjective socioeco-nomic status and health: relationships reconsidered. Soc Sci Med 82:58-66
64. Schubert T, Süssenbach P, Schäfer SJ et al. (2016) The effect of subjective social status on depressive thinking: an experimental examination. Psychiatry Res 241:22-25
65. Demakakos P, Biddulph JP, de Oliveira C et al. (2018) Subjective social status and mortality: the English Longitudinal Study of Ageing. Eur J Epidemiol 33(8):729-739
66. Smith HJ, Pettigrew TF, Pippin GM et al. (2012) Relative deprivation: a theoretical and meta-analytic review. Pers Soc Psychol Rev 16(3):203-232
43. Mehnert A, Höcker A (2011) Religion und körperliche Gesund-heit-empirische Befunde und Erklärungsansätze. In: Gesund-heit-Religion-Spiritualität. Konzepte, Befunde und Erklärungs-ansätze. Juventa, Weinheim, P. 247-257
44. Chatters LM (2000) Religion and Health: Public Health Research and Practice. Annu Rev Public Health 21:335-367
45. Koenig HG (2015) Religion, spirituality, and health: a review and update. Adv Mind Body Med 29(3):19-26
46. Koenig HG (2009) Research on Religion, Spirituality, and Mental Health: A Review. Can J Psychiatry 54:283-291
47. Traunmüller R (2008) Religion als Ressource sozialen Zusam-menhalts? Eine empirische Analyse der religiösen Grundlagen, SOEP papers on Multidisciplinary Panel Data Research. Deutsches Institut für Wirtschaftsforschung, Berlin. https://www.diw.de/documents/publikationen/73/diw_01.c. 90639.de/diw_sp0144.pdf (As at 12.06.2019)
48. Mielck A (2000) Soziale Ungleichheit und Gesundheit: Empiri-sche Ergebnisse, Erklärungsansätze, Interventionsmöglichkeiten. Verlag Hans Huber, Bern
49. Richter M, Hurrelmann K (2009) Gesundheitliche Ungleichheit: Grundlagen, Probleme, Perspektiven. VS Verlag für Sozialwissen-schaften, Wiesbaden
50. Marmot M, Wilkinson RG (2005) Social determinants of health. Oxford University Press, Oxford
51. Robert Koch- Institut (Ed) (2017) Gesundheitliche Ungleichheit in verschiedenen Lebensphasen. Gesundheitsberichterstattung des Bundes. Gemeinsam getragen von RKI und Destatis. Robert Koch-Institut, Berlin. https://edoc.rki.de/handle/176904/3266 (As at 12.06.2019)
52. Galobardes B, Shaw M, Lawlor DA et al. (2006) Indicators of socioeconomic position. In: Oakes JM, Kaufman JS (Eds) Methods in social epidemiology. Jossey-Bass, San Francisco, P. 47-85
53. Lampert T, Kroll LE (2009) Die Messung des sozioökonomi-schen Status in sozialepidemiologischen Studien. In: Richter M, Hurrelmann K (Eds) Gesundheitliche Ungleichheit: Grundlagen, Probleme, Perspektiven. VS Verlag für Sozialwissenschaften, Wiesbaden, P. 309-334
54. Lynch J, Kaplan G (2000) Socioeconomic position. In: Berkman LF, Kawachi I (Eds) Social epidemiology. Oxford University Press, New York, P. 13-35

Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
64
67. McLeod JD (2013) Social stratification and inequality. In: Aneshensel CS, Phelan JC, Bierman A (Eds) Handbook of the sociology of mental health. Springer, Dordrecht, P. 229-
68. Hoebel J, Lampert T (2018) Subjective social status and health: multidisciplinary explanations and methodological challenges. J Health Psychol (efirst)
69. Alegria M, Takeuchi D, Canino G et al. (2004) Considering context, place and culture: the National Latino and Asian American Study. Int J Methods Psychiatr Res 13(4):208-220
70. Alcántara C, Chen CN, Alegría M (2014) Do post-migration perceptions of social mobility matter for Latino immigrant health? Soc Sci Med 101:94-106
71. Nicklett EJ, Burgard SA (2009) Downward social mobility and major depressive episodes among Latino and Asian-American immigrants to the United States. Am J Epidemiol 170(6):793-801
72. Behr D, Braun M, Dorer B (2015) Messinstrumente in internatio-nalen Studien GESIS - Lebniz-Institut für Sozialwissenschaften (GESIS Survey Guidelines), Mannheim
73. Rommel A, Strasser S, Pöge K (2018) Perspectives of LGBTIQ* migrants, refugees and ethnic minorities for the development of a gender-sensitive and intersectional health reporting in Germany. European Journal of Public Health 28(Suppl 4):270
Journal of Health Monitoring
Journal of Health Monitoring 2019 4(3)
CONCEPTS & METHODSConcepts for migration-sensitive health monitoringJournal of Health Monitoring
65
The Robert Koch Institute is a Federal Institute within the portfolio of the German Federal Ministry of Health
This work is licensed under a Creative Commons Attribution 4.0
International License.
Imprint
Journal of Health Monitoring
PublisherRobert Koch InstituteNordufer 20 D-13353 Berlin, Germany
EditorsSusanne Bartig, Johanna Gutsche, Dr Birte Hintzpeter, Dr Franziska Prütz, Dr Martina Rabenberg, Dr Alexander Rommel, Dr Livia Ryl, Dr Anke-Christine Saß, Stefanie Seeling, Martin Thißen, Dr Thomas ZieseRobert Koch InstituteDepartment of Epidemiology and Health MonitoringUnit: Health ReportingGeneral-Pape-Str. 62–66D-12101 BerlinPhone: +49 (0)30-18 754-3400E-mail: [email protected]/journalhealthmonitoring-en
TypesettingGisela Dugnus, Kerstin Möllerke, Alexander Krönke
Translation Simon Phillips/Tim Jack
ISSN 2511-2708
Note External contributions do not necessarily reflect the opinions of the Robert Koch Institute.





























