Embed Size (px)
Citation preview

Journal of Applied Biomedicine 15 (2017) 313–320
Contents lists available at ScienceDirect
Journal of Applied Biomedicine
journal homepage: www.elsev ier .com/ locate / jab
Original research article
Film wound dressing with local anesthetic based on insolublecarboxymethycellulose matrix
Lenka Vinklárkováa, [114_TD$DIFF]Ruta Masteikováa,*, Gabriela Foltýnováa, [115_TD$DIFF]Jan Muselíka,Sylvie Pavlokováa, [116_TD$DIFF]Jurga Bernatonien _eb, [117_TD$DIFF]David Vetchýa
[118_TD$DIFF]aUniversity of Veterinary and Pharmaceutical Sciences Brno, [119_TD$DIFF]Faculty of Pharmacy, Department of Pharmaceutics, [120_TD$DIFF]Brno, Czech Republicb[123_TD$DIFF]Lithuanian University of Health Sciences, [124_TD$DIFF]Faculty of Pharmacy, Department of Drug Technology and Social Pharmacy, [125_TD$DIFF]Kaunas, Lithuania
A R T I C L E I N F O
Article history:
Received 31 August 2016Received in revised form 19 May 2017Accepted 7 August 2017Available online 23 August 2017Keywords:Carboxymethylcellulose partiallysubstitutedCarboxymethylcellulose acidic formFilm wound dressingTopical anesthesiaLidocaine
* Corresponding author at: DepartmentUniversity of Veterinary and PharmaceuticBrno 612 42, Czech Republic.
E-mail address: [email protected] (R.
http://dx.doi.org/10.1016/j.jab.2017.08.0021214-021X/© 2017 Faculty of Health and S
of Pharmacal Science
Masteikov
ocial Scien
A B S T R A C T
The aim of the presented research was to formulate, prepare and evaluate novel film wound dressingscontaining lidocaine hydrochloride. The conversion of partially substituted fibrous sodium carboxy-methylcellulose (CMC) to an acidic form of CMC enabled the formation of an insoluble matrix whichconsequently provided the prepared films with excellent handling properties in their wet state. The drugconcentration which was incorporated into an external layer of the film was 5mg/cm2. The filmsdemonstrated satisfactory mass and drug content uniformity as well as an acidic surface pHadvantageous for wound application. An in vitro drug release test proved that the insoluble CMCmatrix served as a reliable carrier without slowing down the release of lidocaine hydrochloride � morethan 90% of the drug was released during the first 15min, indicating a quick rate of anesthetic action. Theprepared films could be potential wound dressings for comfortable and efficient topical anesthesiabefore/after procedures on the wound.© 2017 Faculty of Health and Social Sciences, University of South Bohemia in Ceske Budejovice. Published
by Elsevier Sp. z o.o. All rights reserved.
Introduction
Wound-related pain can be temporary (acute) or persistent(chronic) (Woo et al., 2008). Acute wound pain can be exacerbatedwhenever the wound is handled or manipulated: during dressingremoval, wound cleansing or debridement (removing of necrotictissues). In contrast, persistent (chronic) wound pain is abackground symptom that exists at rest and between wound-related procedures. The level of pain depends on the causes of thepain � procedural pain (e.g. during dressing removal) andoperative pain (e.g. wound debridement) are worse than pain atrest (Arroyo-Novoa et al., 2009). Unresolved pain predisposesindividuals to stress and associated physiological responses thatcan impair wound healing (Boateng and Catanzano, 2015; Woo,2011), often leading to the need for pharmacological interventionsfor pain prevention.
eutics, Faculty of Pharmacy,s Brno, Palackeho tr. 1946/1,
á).
ces, University of South Bohemia
Separate analgesic strategies may be required for backgroundpain and the pain arising from wound procedures (Orsted, 2010).Guidelines for pharmacological wound painmanagement based onthe recommendations by the World Health Organization recom-mend the use of non-steroidal anti-inflammatory drugs (NSAIDs)or acetaminophen for patients with mild to moderate pain (Briggsand Bou, 2002; Woo et al., 2008). NSAIDs provide good pain relief.Moreover, they can positively influence inflammatory processes inthe wound, since there is a tendency in chronic wounds for theinflammatory response (an important element in the initialwounding response) to become exaggerated (Boateng andCatanzano, 2015). The treatment of wound infection, by reducingbacterial load and thereby reducing the inflammatory stimulus tothe nervous system, should also result in a reduction in pain(Boateng and Catanzano, 2015; Sarheed et al., 2016). Unfortunately,oral use of NSAIDs as well as systemic administration of highantibiotic doses can lead to serious side effects such asgastrointestinal problems, risk of renal failure, prolonged bleedingtime due to impaired coagulation, allergic reactions etc. (Meeket al., 2010; Sarheed et al., 2016; Wallace and Vong, 2008). For thisreason, non-pharmacological strategies and topical agents toachieve optimal wound-related painmanagement are an attractivesolution. Topical agents and correctly selected dressings play a
in Ceske Budejovice. Published by Elsevier Sp. z o.o. All rights reserved.

314 L. Vinklárková et al. / J. Appl. Biomed. 15 (2017) 313–320
critical role in alleviatingwound-related pain (Boateng et al., 2008;Woo et al., 2008). Recently, an evaluation of the effect of ibuprofenin the form of a foam dressing (Biatain Ibu) on persistent andtemporarywound pain underwent clinical trials (Fogh et al., 2012).The ibuprofen foam dressing was shown to consistently relievewound pain in exuding wounds of various etiologies (Romanelliet al., 2009), thus, local pain relief by this dressing is possible in themost common, painful, exuding, chronic and acute/traumaticwounds and therefore is a safer alternative for systemic paintreatment (Arapoglou et al., 2011).
For the management of procedural or operative pain, localanesthesia, which includes infiltration or topical application ofanesthetics, is usually used. Infiltration anesthesia (injection intothe tissue in and around the wound) per se induces discomfort,may worsen “needle anxiety” in pediatric subjects, and distort thewound site (Eidelman et al., 2005). Moreover, Eidelman et al.(2005) found that the majority of clinical trials demonstratedequivalent or superior analgesic efficacy for topical formulationscompared with conventional lidocaine infiltration.
Lidocaine is an essential drug on the World Health Organiza-tion’s essential drug list, and is considered efficacious, safe andcost-effective for any health-care system (Weinberg et al., 2015).The efficacy of topical lidocaine alone or in combinationwith otheranesthetic agents in the management of acute wound pain hasbeen confirmed in clinical practice (Cuomo et al., 2015; Desai et al.,2014; Gaufberg et al., 2007; Little et al., 2009; Pasero, 2013).According to Sussman and Bates-Jensen (2012), lidocaine in theform of a soakmay be recommended as a quick and efficientway toreduce local wound pain during debridement procedures. Anotheroption is EMLA cream (containing a eutectic mixture of lidocaineand prilocaine), which is only intended for contact with intactadjacent skin. Nevertheless, Blanke and Hallern (2003) found that,on the basis of clinical experience, the topical application of EMLAcream directly to the wound before sharp debridement is efficient,economical, safe, and tolerable for the patient. One commondisadvantage of topical analgesics is the amount of time neededbefore effect (usually 20–30 and up to 60min prior to procedures(Sussman and Bates-Jensen, 2012)). For this reason they are moresuitable for non-emergent procedures. Another deficiency oftopical liquid or semisolid anesthetics is the messiness ofapplication and removal (Little et al., 2009). Currently, if theanesthetic must be applied directly to thewound topically, there isno other choice than a liquid or semisolid preparation. Thus thedevelopment of new, more sophisticated forms is required. Filmwound dressing is a pharmaceutical form without the drawbackmessy application and removal. Moreover, film application allowsmore precise dosing of active substances.
Films, as pharmaceutical dosage forms, are currently used fororal, buccal or ophthalmic application with a variety of medicatedor non-medicated preparations on the market. The film wounddressings on themarket are non-medicated ones intended only forprotection of the wound against the effects of the surroundingenvironment or mechanical injury (Sussman, 2010). For thisreason, there have been many studies into how to prepare filmwound dressings with an active substance (Boateng et al., 2013;Jridi et al., 2017; Liakos et al., 2013; Pereira et al., 2013; Thu et al.,2012;Wang et al., 2012). None of these, however, were dedicated tothe development of a wound dressing with the rapid release of alocal anesthetic.
Different polymers may be used to prepare the film. Naturalmaterials are more friendly on bodily tissues than synthetic ones,and are therefore often studied for wound care applications (Juncuetal., 2016;Maveretal., 2015;Ramli andWong,2011;Xuetal., 2007).An ideal film dressingmust be supple and possess homogenous andsmooth surfaces (Ramli and Wong, 2011). Transparency is anotherimportant property allowing for the wound’s assessment without
removingthedressing(Sussman,2010).Filmspreparedfromsodiumcarboxymethylcellulose (NaCMC) possess all these characteristics.Moreover, carboxymethylcellulose (CMC) is generally regarded as anontoxic,nonirritant,andbiocompatiblematerialwhichpredestinesit for use in food, cosmetic, pharmaceutical, and biomedicalapplications, including materials for wound care (Rowe et al.,2015). All of these factors make it a suitable candidate in thepreparation of medicated film. A whole range of scientific worksdeals with the preparation and evaluation of medicated CMC films.However, these films are mainly intended for buccal/oral drugdelivery (Gajdziok et al., 2015; Landová et al., 2013; Raju et al., 2011;Ramineni et al., 2013; Saha et al., 2013; Semalty et al., 2010; Vetchýet al., 2014), andmuch less forwound therapy (Donnadioet al., 2016;Vinklárková et al., 2015). The application properties of film wounddressings differ quite significantly from those intended for buccal/oral applications. Wound dressings are applied on a much largersurface area than buccal preparations. For this reason, goodmechanical properties of medicated CMC films are required.Especially once wetted, they must maintain the cohesiveness thatenables them to be easily manipulated and removed withoutresidues. One option is to reinforce the film with a supportingmaterial aswasdone inourprevious study (Vinklárkováet al., 2015).The other option is to prepare film containing an acidic form of CMC(HCMC), which is insoluble in water, thus more wet resistant. Theidea that film containing HCMCwould be of increased strength wasdescribed for the first time by Butler (1962) in his US patent.However, the patent contains only the general preparationconditions, and lacked precise description of the technology andevaluations methods necessary for the preparation of films withsuitable properties for wound application. Moreover, the techniquedescribed inpatentwas fornon-medicatedfilmsonly. Filmsbasedoninsoluble CMCwith an active substance have not yet to be preparedand evaluated.
The aim of the presented research was to prepare a novel filmwound dressings based on an insoluble carboxymethylcellulosematrix with lidocaine hydrochloride as an active compound, andevaluate their physicochemical properties as well as in vitro drugrelease.
[131_TD$DIFF]Material and methods
The partially substituted (degree of substitution 0.34) sodiumcarboxymethylcellulose (NaCMC) in the form of non-woven textile(Hcel1 NaT) was supplied by Holzbecher, spol. s r.o., Bleaching &Dyeing Plant in Zlí9c (Czech Republic), lidocaine hydrochloride,macrogol 300, glycerin and hydrochloric acid (all Ph. Eur. grade)were purchased from Fagron (Czech Republic). All other chemicalsand reagents used in the study were of analytical grade.
Preparation of films
Films based on an insoluble carboxymethylcellulose (CMC)matrix were prepared using an sequential solvent casting method.Amodified technique according to the US patent (Butler,1962) wasused. In order to create the insoluble CMC (HCMC) matrix, theacidification of both polymer dispersion and casted film wasnecessary. Both the acidification of the polymer dispersionwithoutany further treatment of the film and the acidification of castedNaCMC film itself without previously acidifying the dispersionproved insufficient. The acidification of NaCMC film itself did notachieve required mechanical properties. It is likely that the HCMCmatrixwas not completely formed. Similarly,films prepared fromadispersion acidified to a pH value of 3 or higher without additionaltreatment of casted films were low in quality. Acidification to pHvalues lower than 3 resulted in precipitation and loss of film-forming properties. The double acidification led to the creation of

L. Vinklárková et al. / J. Appl. Biomed. 15 (2017) 313–320 315
films with suitable properties. Thus the films were prepared asfollows: The polymer dispersion was composed of 1% (w/w)NaCMC and 2% (w/w) macrogol 300 or glycerin in purified water.Non-woven sodium carboxymethylcellulose textile (Hcel NaT) wascut into small pieces and poured over with a solution of macrogolor glycerin in hot water (80 �C). This mixturewas heated in awaterbath tomaintain a temperature of 80 �C for 3h, then stirred using aCito-UNGUATOR 2000 dispersing device (SMS Heiztechnik GmbH,Deutschland) set on program “Gel”, and heated again for 1h at thesame temperature. Then the mixture was left to cool and swell atan ambient temperature for 24h. The next day the NaCMCdispersion was acidified under continuous stirring using a 5%solution of hydrochloric acid (HCl) until a pH value of 3 wasachieved. Then 25g of the resulting dispersion was casted on aglass Petri dish 10 cm in diameter and pre-dried in the oven(Heratherm, Germany) at 70 �C for 1h followed by 24h of drying atambient conditions. The dry films were left in the Petri dishes, andacidification/washing was administered as follows: 20ml of 5%solution of HCl for 20min! straining! rinsing with purifiedwater!20ml of purified water for 20min! straining!20ml ofpurified water for 20min! straining!20ml of 5% solution ofmacrogol or glycerin for 20min! straining. Macrogol or glycerinwas added into the final washing liquid to compensate for theseplasticizers washed away from the film during the acidification/washing process. The final layer of filmwas created from a solutionof lidocaine hydrochloride � to obtain the required concentrationof the drug (5mg/cm2) 5 g of 6.3% solution for one Petri dish wereadded. Once the final layer was applied, the films were left to dryunder ambient conditions. The dried films were peeled from thePetri dishes, examined visually for morphological defects (e.g.cracks, shrinking, etc.) which can affect handling, testing andapplication as well as aesthetic appearance, and stored in a closedbox to await testing. Films without active substance were made inthe same manner for comparison of physical properties.
Microscopic properties and thickness
The microscopic properties of the prepared films wereevaluated using an optical microscope (STM-902 ZOOM, Opting,Czech Republic) and a color digital camera (DFW �700, Sony,Japan). The appearance of the films was observed at a magnifica-tion factor of 20 and 50. Illustrative digital imageswere taken at thesame time.
At the measurement of film thickness, a rectangular sample ofthe film was vertically fixed in a holder, the microscope wasfocused on the edge of the film, and the sample thickness wasmeasured at 10 different places along the film. This was repeated5 times with each film sample.
Swelling property
The swelling properties of the prepared films weremeasured ina physiological buffer solution of pH 7.2 (PBS). For these purposes,an artificial wound model developed by us was used. This woundmodel consisted of a Petri dish and absorptive sponge soaked in atest liquid. The surface of the sponge was rough resembling thesurface ofwound. The amount of PBSwas 20ml, whichwas enoughto soak the sponge and create a thin layer of a liquid on the surfaceimitating the wound exudate. 6.25 cm2 (2.5�2.5 cm) samples ofthe filmwere cut and weighed (Wd). The sample was placed on thesurface of thewoundmodel, the Petri dishwas coveredwith a lid toprevent water evaporation, and swollen films were then weighedat determined time intervals (Ws). The degree of swelling Sw in thefilm was calculated as
Sw= (Ws � Wd)/Wd (1)
Surface pH
The surface pH of the prepared films was evaluated using aWTW pH 3210 SET 2 pH-meter (WTW, Germany) with a flat glasselectrode. Alterations of the surface pH in the conditionssimulating the wound environment were assessed using anartificial wound model (as described above). 6.25 cm2
(2.5�2.5 cm) samples of the film were cut and put on the surfaceof the wound model. The Petri dish was covered with a lid toprevent water evaporation, and surface pH was measured atdetermined time intervals in triplicate.
Mechanical properties
A modified method according to Shidhaye et al. (2008) wasused to evaluate themechanical properties of the prepared films indry state and after swelling for 3h on an artificial wound model.A CT3 Texture Analyzer (Brookfield, USA) equipped with a 4.5 kgload cell and TexturePro CT software was used to determine thetensile strength of the prepared films. Film samples (10� 40mm)were held between two clamps of a TA-DGA probe positioned at adistance of 2 cm. The lower clamp was held stationary and thestrips of the film were stretched by the upper clamp moving at arate of 0.5mm/s until the strip broke. The work done during thisprocess and the deformation (elongation) of the film at themoment of tearingwere bothmeasured. This processwas repeatedfive times for each film sample.
Uniformity of mass
For this evaluation, the adapted test as described in EuropeanPharmacopoeia (chapter 2.9.5. Uniformity of mass of single-dosepreparations) was applied. 20 units of precisely cut samples fromrandom sites of the prepared films (2.5�2.5 cm) were weighedindividually, and the average mass� SD was determined. Theindividual masses were then compared with the average mass andthe percentage of deviation was calculated.
Uniformity of drug content
For this evaluation, the adapted test as described in EuropeanPharmacopoeia (chapter 2.9.6. Uniformity of content of single-dose preparations) was applied. 10 units (5�5 cm) were preciselycut from random sites of the prepared films and dissolvedseparately in beakers containing 200ml of PBS. Standard solutionsof 0.15, 0.3, 0.45, 0.6 and 0.75% lidocaine hydrochloride (w/w)wereprepared using a PBS, and calibration curves using HPLC wereconstructed. The HPLC system employed was a YL 9100 chromato-graph (Young Lin Instrument, South Korea), using a variablewavelength UV detector set at 210nm. Analysis was performed ona Polaris C18 column (250� 4.6mm; 5mm) at temperature 30 �C.A mixture containing 0.2% (w/w) phosphoric acid in water andacetonitrile (75:25) was used as a mobile phase, at a flow rate of1ml/min and injection volume of 3ml. The average concentrationof lidocaine hydrochloride in each sample, percentage deviationand SD were then calculated.
[132_TD$DIFF]In vitro drug release
A standard paddle dissolution apparatus Sotax AT7 Smart(Donau Lab, Zurich, Switzerland), as described in the EuropeanPharmacopoeia, was employed to evaluate drug release. A portionof 25 cm2 (5�5 cm) of filmwas used. A side of the filmwithout thedrug was attached using double adhesive tape to an inert glassplate as described by Okamoto et al. (2001), then the vessel wasfilled with 500ml of PBS, and maintained at 32 �C (temperature of

[(Fig._1)TD$FIG]
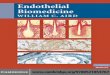
Fig. 1. Appearance of wetted film after application to small lesion.
[(Fig._2)TD$FIG]
Fig. 2. Microscopic appearance of the film without drug: [110_TD$DIFF](A) surface of film, (B)edge of film with easily recognizable fibers (magnification 20�, bar 500mm).
[(Fig._3)TD$FIG]
Fig. 3. Microscopic appearance of the film with lidocaine hydrochloride: [111_TD$DIFF](A)magnification 20�, bar 500mm, [112_TD$DIFF](B) magnification 50�, bar 100mm.
316 L. Vinklárková et al. / J. Appl. Biomed. 15 (2017) 313–320
skin surface) while stirring at 50 rpm. Two-milliliter samples werecollected automatically at predetermined time intervals andreplaced with an equal amount of PBS to maintain a constantvolume. Lidocaine hydrochloride releasewas quantified byHPLC asdescribed above and was expressed as a cumulative percentreleased versus time for the 3-h duration of the study.
Statistical analysis
All experiments were carried out at least in triplicate, and datawas expressed as amean� standard deviation (SD). Comparison ofthe means was performed by analysis of variance (ANOVA) at asignificance level of a =0.05. [103_TD$DIFF]p-values were used as a decisivecriterion for indication of significance. The statistical significanceof parameters was confirmed if the [104_TD$DIFF]p-value was equal to or smallerthan a. Statistical evaluation of data was performed by means ofQC.Expert software, version 3.2.
Results and discussion
Partially substituted microfibrous NaCMC (non-woven textileHcel1NaT) was used in order to increase themechanical resilienceof the films after wetting. It was assumed that non-substitutedfibers would act as fillers. According to Paunonen (2013), if thefiller is well dispersed in the polymer matrix, an improvement inthe mechanical properties is usually observed. Despite theexcellent cohesiveness of the wetted films, thanks to the micro-fibrous NaCMC and proved in our previous study (Vinklárkováet al., 2015), it was still necessary to reinforce them even more toenhance handling properties. For this reason, a technologicalprocedure that enables the creation of an insoluble matrix of theacidic form of CMC (HCMC)was chosen. Macrogol 300 and glycerinwere used as plasticizers. The solvent casting method was chosenfor film preparation. It is a widely used manufacturing process formaking films distinguished by its relative simplicity and the lowcost that system setup incurs at a research laboratory scale(Morales and McConville, 2011).
In the case of medicated film, an active substance may beincorporated in different ways. Considering the fact that theassumed indication of the film was anesthesia before painfulintervention on the wound, the onset of action must be rapid. Forthis reason, lidocaine hydrochloride was incorporated as theexternal layer on only one side of film in the form of finecrystallized, evenly distributed and firmly adhered particles on thesurface (see microscopic appearance). The concentration of thedrug in the film was expressed as mg/cm2 of film. This expressionfacilitates dosage since wound dressings are applied to a certainsurface area. Perumal et al. (2008) even postulate thatdetermination by weight is erroneous because the final dosageform is determined by area instead of weight in the particularcase of films.Moreover, expression related to area is independentof the weight of the film which may vary considerably, as filmsmade from hydrophilic polymers tend to fluctuate in terms ofmoisture content (Paunonen, 2013). A concentration of 5mg/cm2
was chosen on the basis of doses for topical application oflidocaine proven in clinical practice (Cuomo et al., 2015, Pasero,2013; Sussman and Bates-Jensen, 2012).
Visual examination demonstrated that prepared films werehomogenous with a smooth surface. Although the presence ofinsoluble HCMC did not allow the excellent transparency typicalof films from NaCMC, the prepared films were translucentenough to facilitate observation of wound conditions, especiallywhenwetted (Fig. 1). Dry films were firm and resilient, and filmswith glycerin were more flexible than macrogol ones. Afterwetting they both became soft and pliable, with good adherenceto the skin. However, conversion of NaCMC to HCMC led to a loss
of bioadhesive/mucoadhesive properties which are distinctive tofilms from NaCMC (Vetchý et al., 2014). Nevertheless, this changeof properties would be positive when applied to wounds as a localanesthetic, as it enables very easy and quick removal withoutresidues.

Table 1Thickness, mass, mechanical properties and uniformity of drug content of prepared films.
Films with macrogol 300 Films with glycerin
withoutdrug
withlidocaine
withoutdrug
with lidocaine
Thickness (mm)a 71.73�12.12 101.86�8.14 68.36�4.87 101.8�8.53Mass of sample 2.5�2.5 cm (mg)b 44.4�2.9 76.2�5.8 37.9�2.6 72.3�4.0Mechanical propertiesc
– dry film� tensile strength (N) 5.39�0.26 2.83�0.51 5.84�0.53 3.39�0.23
� deformation/elongation (mm) 3.12�0.32 3.26�0.47 2.52�0.21 3.09�0.18
� � work done (mJ) 9.19�0.91 5.87�1.39 8.01�1.24 5.57�0.23
– swelled film after 3h on the artificial wound model� tensile strength (N) 3.53�0.21 1.66�0.17 3.74�0.64 1.81�0.27
� deformation/elongation (mm) 4.22�0.15 4.29�0.13 3.52�0.39 5.35�0.29
� � work done (mJ) 6.82�0.19 3.27�0.27 6.0�1.56 4.83�0.96
Uniformity of drug content (sample 5�5 cm)d – –
– average content (mg) 126.8�7.02 131.06�8.65– deviation from the stated content (125mg/25 cm2) (%) 101.44 104.84– marginal deviation below average content (%) 95.69 93.16– marginal deviation above average content (%) 108.6 113.5
Mean� SD (a[109_TD$DIFF]n =50, bn =20, cn =5, dn =10).
L. Vinklárková et al. / J. Appl. Biomed. 15 (2017) 313–320 317
Observation of microscopic appearance of prepared filmsconfirmed that partially substituted CMC maintained a fibrousnature (Fig. 2). Medicated films contained evenly distributedparticles of crystallized lidocaine hydrochloride (Fig. 3).
Film thickness is an important parameter from a technologicalstandpoint. Uniform thickness indicates a correct preparationmethod and a strong likelihood of drug content uniformity as wellas a regular process of drug release. The thickness of prepared filmswas dependent on drug content � films with lidocaine hydrochlo-ride were thicker ([105_TD$DIFF]p<0.05) than lidocaine-free ones (Table 1). Theinfluence of type of plasticizer (macrogol or glycerin) wasnegligible ( [106_TD$DIFF]p>0.05).
The swelling behavior of the films is an important property fortheir practical application. Liquid-uptake of the film prevents dry-out and creates conditions for moist wound healing (Pišlová et al.,2015). It may be affected by several factors such as pH or thepresence and character of ions. A physiological buffer solution ofpH 7.2 is similar to wound fluid with regard to ion content as well
[(Fig._4)TD$FIG]Fig. 4. Swelling behavio
as pH value, thus determined swelling values of prepared filmscould adequately reflect those in a real wound.
The films exhibited a low degree of swelling (Fig. 4), indicatingweak holding capacity for the exudatewhile still maintaining theirexcellent structural integrity for a reasonable time period.The degree of swelling (Sw) increased only slightly with time.The higher swelling values were obtained from medicated films([105_TD$DIFF]p < 0.05). Most likely, a lidocaine salt of CMC with a higherswelling responsiveness was formed during preparation. Theinfluence of type of plasticizer on swelling properties was notconfirmed.
Alterations to the surface pH of the films during 3h inconditions simulating a wound environment are shown in Fig. 5.The figure demonstrates that surface pH increased with time([105_TD$DIFF]p<0.05) probably due to an ion-exchange reaction resulting inthe gradual formation of sodium or potassium salts of the CMC.Nevertheless, all prepared films retained acidic pH values(pH<4.5). This evaluation is very important because it reflects
r of prepared films.

[(Fig._5)TD$FIG]
Fig. 5. Alterations of surface pH in the conditions simulating wound environment.
[(Fig._6)TD$FIG]
Fig. 6. Mechanical properties of prepared films: tensile strength and deformation/elongation of film at the moment of tearing (*[99_TD$DIFF]p<0.05 film without drug vs. filmwith lidocaine, [113_TD$DIFF]�p<0.05 dry film vs. wetted film).
[(Fig._7)TD$FIG]
Fig. 7. Release of lidocaine hydrochloride from prepared films.
318 L. Vinklárková et al. / J. Appl. Biomed. 15 (2017) 313–320
the impact of the wound dressing on the wound environment. It isknown that pH plays a significant role inwoundhealing. In general,lowering pH has shown to result in an improvement of woundhealing (inhibition of microbial growth, alteration of activity ofmatrix metalloproteinases etc.) (Percival et al., 2014). Because thesupposed duration of the application of the prepared lidocainefilms should be relatively short, immediate influence on woundhealing need not be significant. However, inhibition of microbialgrowth is also important for short application. Likewise, synergy ofantimicrobial activity should be hypothesized since both lidocainehydrochloride (Johnson et al., 2008) and acidic form of CMC (Touatiet al., 2013) itself are active against microorganisms, thus preparedfilms should be especially beneficial when treating infectedwounds.
The mechanical properties of the prepared films are shown inTable 1. Characterization of mechanical properties is importantbecause film dressings are required to be durable, stress resistant,
soft, flexible, pliable and elastic in order to cope with the stressesexerted by different parts of the body (Boateng et al., 2008). Thesedesirable characteristics can be achieved by investigating theirtensile properties to ensure a balance between flexibility andrigidity. Fig. 6 demonstrates comparable mechanical properties ofprepared films. Films with glycerin had slightly better mechanicalproperties than macrogol plasticized ones, but this difference wasnot statistically significant ([107_TD$DIFF]p>0.05), thus the influence ofplasticizer was not proved. The greatest statistically significantdifferences ([105_TD$DIFF]p<0.05) were noticeable between films with andwithout lidocaine or dry and swelled ones. Not surprisingly, lowervalues of tensile strength, higher elongation and less worknecessary to tear the film were all observed in swelled films.The lower tensile strength of medicated films was probably causedby the interaction of anionic HCMC and cationic lidocainehydrochloride leading to the formation of a compound with worsemechanical properties. The fact that added active compounds, ingeneral, affectmechanical properties of CMC films, is also stated byPaunonen (2013). Nevertheless, both medicated films and lido-caine-free ones manifested excellent handling properties afterswelling (3h onwoundmodel), making them extremely beneficialin clinical applications. It would be interesting to compare themechanical properties of prepared films with these described inthe patent (Butler, 1962) which gave us this idea. Unfortunately,direct comparison was impossible due to differing units ofmeasurement of tensile strength used in the patent which couldnot be converted. Nevertheless, a relative comparison of strengthloss after wetting seemed to favor our films � wet films in thepatent were ca. five times weaker than dry ones, whereas theweakening of films prepared by us was less than half of dry valueafter swelling on the woundmodel (Table 1). This finding confirmsthe correctness of the developed technology.
According to European Pharmacopoeia, not more than 2 of theindividual masses may deviate from the average mass by morethan 10% if a pharmaceutical form has an average mass 80mg orless, and none deviates by more than twice that percentage. Allprepared films met these requirements. Films prepared withglycerin were slightly lighter than those with macrogol ([108_TD$DIFF]p<0.05),regardless of lidocaine content (Table 1).
European Pharmacopoeia does not state the requirements formedicated films regarding drug content. Thus, requirements fortransdermal patches or ophthalmic inserts, as the most similar

L. Vinklárková et al. / J. Appl. Biomed. 15 (2017) 313–320 319
pharmaceutical forms to film wound dressings, should be applied.In the case of transdermal patches, the preparation complies withthe test of if the average content of 10 dosage units is between 90%and 110% of stated content and if the individual content of eachdosage unit is between 75% and 125% of the average content. In thecase of ophthalmic inserts, the preparation complies with the testof if each individual content is between 85% and 115% of theaverage content. The values shown in Table 1 confirm that theprepared filmsmet the requirements for both transdermal patchesand ophthalmic inserts.
Not surprisingly, drug release from prepared films was veryrapid, because lidocaine hydrochloride is highly water-soluble andwas incorporated as the external layer of the film.More than 90% ofthe drug released during the first 15min, and the remainingcontent of lidocaine was released within an hour (Fig. 7). The datashows almost identical release profiles both for films containingmacrogol and those containing glycerin. Drug release from theprepared films was similar to the observations made by Murataet al. (2010), who investigated fast dissolving films expected to beapplied in the oral cavity or Vakili et al. (2012), who studiedlidocaine hydrochloride release from porous cellulose filmmatrices. Sustained/extended release may be achieved if lidocaineis dispersed in a polymer matrix, as done by Repka et al. (2005) orOkamoto et al. (2001). However, extended release was not the aimof our study. We assumed that the drug-containing layer woulddissolvewithin a short time period and release the drug toward thewound surface where the local anesthetic action of lidocainehydrochloride could take effect. The dissolution test proved thatthe insoluble carboxymethylcellulose matrix served as a reliablecarrier, without slowing down the release of lidocaine hydrochlo-ride. The resultwas a dosage form that can be expected to provide aquick and satisfactory rate of anesthetic action as a prepared filmwound dressing.
[133_TD$DIFF]Conclusion
Film wound dressings based on an insoluble carboxymethyl-cellulose matrix were successfully prepared using a sequentialsolvent casting method. Films containing lidocaine hydrochloridepossess properties making them suitable for use as comfortableand efficient topical anesthetics. This is due to their firmness andresiliency in dry state and excellent handling properties, softness,pliability, good transparency, and adherence to the skin afterswelling. The high flexibility of wetted films provides goodadaptability to the wound or other treated surfaces with disruptedskin integrity. The prepared films showed an acidic surface pHadvantageous for wound application, as well as satisfactory massand drug content uniformity. The films exhibited a low degree ofswelling, indicating weak holding capacity for the exudate, whichis typical of themost polymeric films. An in vitro drug release studyconfirmed rapid lidocaine hydrochloride release. The principalimplication of the developed technology is that it is suitable for thepreparation of both drug-containing film wound dressings andnon-medicated ones. Films without an active substance could beused to protect slightly exuding or non-exuding wounds (such asepithelizing wounds) against injury and the growth of micro-organisms, thanks to its good mechanical properties and lowsurface pH values. The described technology for drug incorpo-ration, when a highly soluble active substance or combination ofsuch substances form a layer on only one side of the film, isparticularly beneficial for preparationswith rapid drug release� inthe case of local anesthesia the combination of several activesshould result in major improvement of effect. These attributes, aswell as evaluation of long-term stability or in vivo effects, willhowever, require further investigations.
Conflict of [134_TD$DIFF]interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
Acknowledgement
This work was supported by finances from the TechnologyAgency of the Czech Republic ALFA program (research project No.TA04010065).
References
Arapoglou, V., Katsenis, K., Syrigos, K.N., Dimakakos, E.P., Zakopoulou, N., Tsoutsos,D., Gjedsbel, K., Glynn, C., Schäfer, E., Petersen, B., 2011. Analgesic efficacy of anibuprofen-releasing foamdressing comparedwith local best practice for painfulexuding wounds. J. Wound Care 20, 319–325.
Arroyo-Novoa, C.M., Figueroa-Ramos, M.I., Miaskowski, C., Padilla, G., Stotts, N.,Puntillo, K.A., 2009. Acute wound pain: gaining a better understanding. Adv.Skin Wound Care 22, 373–380.
Blanke,W., Hallern, B.V., 2003. Sharpwound debridement in local anaesthesia usingEMLA cream: 6 years' experience in 1084 patients. Eur. J. Emerg. Med. 10, 229–231.
Boateng, J., Catanzano, O., 2015. Advanced therapeutic dressings for effectivewoundhealing � a review. J. Pharm. Sci. 104, 3653–3680.
Boateng, J.S., Matthews, K.H., Stevens, H.N.E., Eccleston, G.M., 2008. Wound healingdressings and drug delivery systems: a review. J. Pharm. Sci. 97, 2892–2923.
Boateng, J.S., Pawar, H.V., Tetteh, J., 2013. Polyox and carrageenan based compositefilm dressings containing anti-microbial and anti-inflammatory drugs foreffective wound healing. Int. J. Pharm. 441, 181–191.
Briggs, M., Torra, I., Bou, J.E., 2002. Pain at wound dressing changes: a guide tomanagement. EWMAPositionDocument Pain atWoundDressing Changes.MEPLtd., London, pp. 12–17.
Butler, R.W., 1962. Preparation of free acid cellulose ether films. US 3 (064), 313.Cuomo, R., D'Aniello, C., Grimaldi, L., Nisi, G., Botteri, G., Zerini, I., Brandi, C., 2015.
EMLA and lidocaine spray: a comparison for surgical debridement in venous legulcers. Adv. Wound Care 4, 358–361.
Desai, C., Wood, F.M., Schug, S.A., Parsons, R.W., Fridlender, C., Sunderland, V.B.,2014. Effectiveness of a topical anaesthetic spray as analgesia for dressingchanges: a double-blinded randomized pilot trial comparing an emulsion withan aqueous lidocaine formulation. Burns 40, 106–112.
Donnadio, A., Ambrogi, V., Pietrella, D., Pica, M., Sorrentino, G., Casciola, M., 2016.Carboxymethylcellulose films containing chlorhexidine-zirconium phosphatenanoparticles: antibiofilm activity and cytotoxicity. RSC Adv. 6, 46249–46257.
Eidelman, A.E., Weiss, J.M., Enu, I.K., Lau, J., Carr, D.B., 2005. Comparative efficacyand costs of various topical anesthetics for repair of dermal lacerations: asystematic review of randomized, controlled trials. J. Clin. Anaesth. 17, 106–116.
Fogh, K., Andersen, M.B., Bischoff-Mikkelsen, M., Bause, R., Zutt, M., Schilling, S.,Schmutz, J.-L., Borbujo, J., Jimenez, J.A., Cartier, H., Jørgensen, B., 2012. Clinicallyrelevant pain relief with an ibuprofen-releasing foam dressing Results from arandomized, controlled, double-blind clinical trial in exuding, painful venousleg ulcers. Wound Repair Regen. 20, 815–821.
Gajdziok, J., Holešová, S., Štembírek, J., Pazdziora, E., Landová, H., Doležel, P., Vetchý,D., 2015. 2015. Carmellose mucoadhesive oral films containing vermiculite/chlorhexidine nanocomposites as innovative biomaterials for treatment of oralinfections. BioMed. Res. Int. 15 Article ID 580146.
Gaufberg, S.V., Walta, M.J., Workman, T.P., 2007. Expanding the use of topicalanesthesia in wound management: sequential layered application of topicallidocaine with epinephrine. Am. J. Emerg. Med. 25, 379–384.
Johnson, S.M., John, B.E.S., Dine, A.P., 2008. Local anaesthetics as antimicrobialagents: a review. Surg. Infect. (Larchmt) 9, 205–213.
Jridi,M., Sellimi, S., Ben Lassoued, K., Beltaief, S., Souissi, N., Mora, L., Toldra, F., Elfeki,A., Nasri, M., Nasri, R., 2017.Wound healing activity of cuttlefish gelatin gels andfilms enriched by henna ([135_TD$DIFF]Lawsonia inermis) extract. Colloids Surf. A:Physicochem. Eng. Aspects 512, 71–79.
Juncu, G., Stoica-Guzun, A., Stroescu, M., Isopencu, G., Jinga, S.I., 2016. Drug releasekinetics from carboxymethylcellulose-bacterial cellulose composite films. Int. J.Pharm. 510, 485–492.
Landová, H., Dan�ek, Z., Gajdziok, J., Vetchý, D., Štembírek, J., 2013. Mucoadhesivefilms as perspective oral dosage form. �Ces. Slov. Farm. 62, 4–11.
Liakos, I., Rizzello, L., Bayer, I.S., Pompa, P.P., Cingolani, R., Athanassiou, A., 2013.Controlled antiseptic release byalginate polymerfilms and beads. CarbohydratePolym. 92, 176–183.
Little, C., Kelly, O.J., Jenkins, M.G., Murphy, D., McCarron, P., 2009. The use of topicalanaesthesia during repair of minor lacerations in Departments of EmergencyMedicine: a literature review. Int. Emerg. Nursing 17, 99–107.
Maver, T., Maver, U., Mostegel, F., Griesser, T., Spirk, S., Smrke, D.M., Stana-Kleinschek, K., 2015. Cellulose 22, 749–761.
Meek, I.L., van de Laar, M.A.F.J., Vonkeman, H.E., 2010. Non-steroidal anti-inflammatory drugs: an overview of cardiovascular risk. Pharmaceuticals 3,2146–2162.

Mo
Mu
Oka
OrsPas
Pau
Per
Per
Per
Pišl
Raj
Ram
Ram
Rep
Rom
Row
Sah
Sar
Sem
Shi
Sus
Sus
Thu
Tou
Vak
Vet
Vin
Wa
Wa
We
Wo
Wo
Xu,
320 L. Vinklárková et al. / J. Appl. Biomed. 15 (2017) 313–320
rales, J.O., McConville, J.T., 2011. Manufacture and characterization ofmucoadhesive buccal films. Eur. J. Pharm. Biopharm. 77, 187–199.rata, Y., Takashi, I., Kofuji, K., Nishida, N., Kamaguchi, R., 2010. Preparation of fastdissolving films for oral dosage from natural polysaccharides. Materials 3,4291–4299.moto, H., Taguchi, H., Iida, K., Danjo, K., 2001. Development of polymer filmdosage forms of lidocaine for buccal administration: I. Penetration rate andrelease rate. J. Control. Release 77, 253–260.ted, M.E., 2010. Wound infection & pain management. Wounds Int. 1, 1–6.ero, C., 2013. Lidocaine patch 5% for acute pain management. J. PeriAnaesthesiaNursing 28, 169–173.nonen, S., 2013. Strength and barrier enhancements of cellophane and cellulosederivative films: a review. BioResourses 8, 3098–3121.cival, S.L., McCarty, S., Hunt, J.A., Woods, E.J., 2014. The effects of pH on woundhealing, biofilms, and antimicrobial efficacy. Wound Repair Regen. 22, 174–186.eira, R.F., Mendes, A., Bártolo, P.J., 2013. Novel alginate/aloe vera hydrogel blendsas wound dressings for the treatment of several types of wounds. Chem. Eng.Trans. 32, 1009–1014.umal, V., Govender, T., Lutchman, D., Mackraj, I., 2008. Investigating a newapproach to film casting for enhanced drug content uniformity in polymericfilms. Drug Dev. Ind. Pharm. 34, 1036–1047.ová, M., Kolá�rová, K., Vosmanská, V., Kvítek, O., Švor9cík, V., 2015. Preparation ofpolysaccharide films based on chitosan and cellulose. Chem. Listy 109, 942–945.u, S., Reddy, S.P., Kumar, A., Deepthi, A., Sreeramulu, R.K., Reddy, M.P.V., 2011.Flash release oral films of metoclopramide for pediatric use: formulation and [136_TD$DIFF]invitro evaluation. J. Chem. Pharm. Res. 3, 636–646.ineni, S.K., Cunningham, L.L., Dziubla, T.D., Puleo, D.A., 2013. Development ofimiquimod-loaded mucoadhesive films for oral dysplasia. J. Pharm. Sci. 102,593–603.li, N.A., Wong, T.W., 2011. Sodium carboxymethylcellulose scaffolds and theirphysicochemical effects on partial thickness wound healing. Int. J. Pharm. 403,73–82.ka, M.A., Gutta, K., Prodduturi, S., Munjal M. m Stodghill, S.P., 2005.Characterization of cellulosic hot-melt extruded films containing lidocaine. Eur.J. Pharm. Biopharm. 59, 189–196.anelli, M., Dini, V., Polignano, R., Bonadeo, P., Maggio, G., 2009. Ibuprofen slow-release foam dressing reduces wound pain in painful exuding wounds:preliminary findings from an international real-life study. J. Dermatol.Treatment 20, 19–26.e, R.C., Sheskey, P.J., Quinn, M.E. (Eds.), 2015. Handbook of PharmaceuticalExcipients. Pharmaceutical Press, London 888 p.a, S., Tomaro-Duchesneau, C., Daoud, J.T., Tabrizian, M., Prakash, S., 2013. Novelprobiotic dissolvable carboxymethyl cellulose films as oral healthbiotherapeutics: [138_TD$DIFF]in vitro preparation and characterization. Expert Opin. DrugDeliv. 10, 1471–1482.
heed, O., Ahmed, A., Shouqair, D., Boateng, J., 2016. Antimicrobial dressings forimproving wound healing. In: Alexandrescu, V.A. (Ed.), Wound Healing - NewInsights into Ancient Challenges. InTech, pp. 373–398 (10–5772/61906, https://www.intechopen.com/books/wound-healing-new-insights-into-ancient-challenges/antimicrobial-dressings-for-improving-wound-healing).alty, A., Semalty, M., Nautiyal, U., 2010. Formulation and evaluation ofmucoadhesive buccal films of enalapril maleate. Ind. J. Pharm. Sci. 72, 571–575.dhaye, S.S., Saindane, N.S., Sutar, S., Kadam, V., 2008. Mucoadhesive bilayeredpatches for administration of sumatriptan succinate. AAPS PharmSciTech 9,909–916.sman, C., Bates-Jensen, B., 2012. Management of wound pain. In: Sussman, C.,Bates-Jensen, B.M. (Eds.), Wound Care: A Collaborative Practice Manual forHealth Professionals.. Wolters Kluwer Lippincott Williams & WilkinsPhiladelphia, pp. 535–572.sman, G., 2010. Technology update: understanding film dressings.Wounds Int.1,23–25., H.-E., Zulfakar, M.H., Ng, S.-F., 2012. Alginate based bilayer hydrocolloidfilms aspotential slow-release modern wound dressing. Int. J. Pharm. 434, 375–383.ati, G., Barry, M., Cauet, H., Biendo, M., Strohl, P., 2013. Antibacterial effect ofmodified cellulose: [139_TD$DIFF]in vitro and clinical study potential applications in theprevention of surgical site infection. Hojení Ran [Wound Healing] 7, 25–26.ili, H., Genina, N., Ehlers, H., Bobacka, J., Sandler, N., 2012. Using ion-selectiveelectrodes to study the drug release from porous cellulose matrices.Pharmaceutics 4, 366–376.chý, D., Landová, H., Gajdziok, J., Doležel, P., Dan�ek, Z., Štembírek, J., 2014.Determination of dependencies among [140_TD$DIFF]in vitro and in vivo properties ofprepared mucoadhesive buccal films using multivariate data analysis. Eur. J.Pharm. Biopharm. 86, 498–506.klárková, L., Masteiková, R., Vetchý, D., Doležel, P., Bernatonien _e, J., 2015. 2015.Formulation of novel layered sodium carboxymethylcellulose film wounddressings with ibuprofen for alleviating wound pain. BioMed Res. Int. 11 ArticleID 892671.llace, J.L., Vong, L., 2008. NSAID-induced gastrointestinal damage and the designof GI-sparing NSAIDs. Curr. Opin. Invest. Drugs 9, 1151–1156.ng, T., Zhu, X.-K., Xue, X.-T., Wu, D.-Y., 2012. Hydrogel sheets of chitosan, honeyand gelatin as burn wound dressings. Carbohydr. Polym. 88, 75–83.inberg, L., Peake, B., Tan, C., Nikfarjam, M., 2015. Pharmacokinetics andpharmacodynamics of lignocaine. A review. World J. Anaesthesiol. 4, 17–29.o, K., Sibbald, G., Fogh, K., Glynn, C., Krasner, D., Leaper, D., Österbrink, J., Price, P.,2008. Assessment and management of persistent (chronic) and total woundpain. Int. Wound J. 5, 205–215.o, K.Y., 2011. Exploring the effects of pain and stress onwound healing. Adv. SkinWound Care 25, 38–44.H., Ma, L., Shi, H., Gao, C., Han, C., 2007. Chitosan-hyaluronic acid hybrid film as anovel wound dressing: [141_TD$DIFF][97_TD$DIFF]in vitro and in vivo studies. Polym. Adv. Technol.18, 869–875.