Embed Size (px)
Citation preview

Use your NHS well
Joint Dementia Strategy2010- 2015
Kensington and Chelsea
234572 Dementia Strategy Doc.indd 1 10/8/10 12:47:00

2
Foreword:
The Dementia Strategy for Kensington and Chelsea is published at a time of growing recognition of the impact of dementia on our society over the coming years. At one level this is a resource challenge, but on another and more profound one, it is about the quality of life we expect for our residents. The experience of people with dementia, and their families, will be a key measure of our success or failure as commissioners and providers of services. In our vision for Kensington and Chelsea we set out how we will operate as the health advocate for people with dementia, and their families, in the Royal Borough.
The prevention and management of dementia will be a significant challenge over the coming years in the absence of a strategic approach to commissioning care, largely because of the complex way in which the condition is expressed. Dementia has several forms. It may mean that people are less able to remember things, make sense of the world around them or to deal with the normal changes that come with advancing age. Dementia is stressful for all concerned, and while the person with dementia will increasingly rely on their family and friends, those carers also need support so that they can go on coping for as long as they want. It is now, thankfully, recognised that dementia is not, and must not be seen as, the end of life. People can live with dementia and have much happiness and fulfilment for a number of years. Our role is to ensure they have the support and care they need to make this a reality. We will challenge the old scenarios for these people, and support our colleagues in social care, the NHS, private sector and voluntary organisations in providing excellent services for each one.
We will base our approach on the principles set out in the national strategy – Living Well with Dementia, published in February 2009. We will improve understanding of dementia among the public so that people are better informed of the potential to delay some forms of dementia by looking after their diet, taking exercise and maintaining social contact. We want people to feel confident that their GP will be able to diagnose dementia and be able to signpost them to support and to appropriate services. We will ensure that a diagnosis of dementia is followed up by a package of support and care to meet changing needs, right through to the end of life. We will provide access to early diagnosis, which is made quickly and sensitively communicated by well trained staff. We will provide support to carers and those close to someone with dementia, so that they can go on caring for as long as they want. We will ensure that people have choice and control over their care pathway, including access to personalised budgets and a range of best-practice services as appropriate.
We are committed to deliver this vision within five years, with changes starting in 2010. We will preserve and promote that which is excellent in our Borough, while energetically addressing the gaps. Through realising this vision, we will focus our resources on where they will have most impact on the experience and happiness of all those living with dementia.P Molyneux P Wright J Daintith
Chair,
NHS Kensington and Chelsea
Chief Executive,
NHS Kensington and Chelsea
Executive Director of Health, Housing and
Adult Social Care.
Royal Borough of Kensington and Chelsea
Dementia is not a natural consequence of ageing and it is not true that nothing can be done
for people with the condition. In reality, a great deal can be done to help people overcome the
problems of dementia, to prevent crises and to improve the quality of life of all involved.
We must remove the stigma attached to dementia, which is similar in many ways to the stigma
that cancer used to carry in the past.
Living Well with Dementia: A National Dementia Strategy. 2009
234572 Dementia Strategy Doc.indd 2 10/8/10 12:47:00

Use your NHS well3
Executive Summary
Background:
• The Joint Dementia Strategy for Kensington and Chelsea 2010 – 2015 is a response to the growing demand for dementia services that we will see over the next five years. This is linked to a growing population of older people, and our commitment to improving early identification of dementia. This includes those with young onset dementia.
• The Joint Dementia Strategy is also a local response to the National Dementia Strategy, Living Well with Dementia, launched in February 2009.
• Finally, and most importantly, the Joint Dementia Strategy is informed by feedback from local people that current services have many good aspects, but are unevenly distributed, inequitable and hard to navigate. The strategy sets out the principles which will support a new pathway for services for people with dementia.
What is covered in the strategy?
As in the National Strategy, our local plan will be based around three themes, forming a new pathway:• Raising awareness and understanding,• Early diagnosis and support,• Living well with dementia.
• As part of achieving this, dementia is approached in the strategy as a long-term condition, and will benefit from being built into plans for integrated health systems.
• Polysystems for dementia will include new developments in intermediate care and community based care for the elderly teams run by primary care. These are designed to reduce use of hospital and residential care, and improve the quality of life for people with dementia and their carers.
The Local Context:
The strategy uses local and pan-London analysis to show that:• We believe there will be a 5% increase in the number of people with dementia by 2021, of which 14%
will be from Black and Minority ethnic groups. • 61% of our older people in Kensington and Chelsea live alone.• We have currently identified less than 40% of those with dementia in Kensington and Chelsea. • New services need to reach those not currently receiving services and be flexible and accessible to people
from a range of cultural backgrounds and socio-economic environments.
Measuring success:
There are three outcomes which we will monitor using National and pan-London objectives and standards:• A single pathway to support living at home for as long as possible.• Improved understanding by people with dementia and their carers of where to find advice and support.
This will include individual guidance where needed.• We will improve understanding of dementia amongst professionals and the public.
Next steps:
The strategy will underpin a commissioning plan and implementation, starting in 2010. It is anticipated that services will be fully redesigned by 2015.
234572 Dementia Strategy Doc.indd 3 10/8/10 12:47:00

4
1. What is Dementia?
Dementia stems from a range of disorders affecting the brain. It comes in different forms, the commonest being Alzheimer’s disease and vascular disease.
Dementia manifests itself in a wide variety of ways, including loss of memory, and changes to personality. It is more common in people over 65 years of age, but can occur in younger people and is then known as young onset dementia. In all cases, the capacity for a person with dementia to deal with the normal changes that come with advancing age, and to go on looking after themselves is affected increasingly over time.
A risk with any diagnosis or explanation of a disease, is that it may cause us to focus on their disease and disability, seeing their treatment as a medical challenge. Modern approaches to the management of dementia include a social model of disability. This is the view that the person with dementia is as disabled as their environment makes them. For this reason, effective partnerships are at the core of this strategy, to provide services for the whole person and their family which will retain independence and quality of life for as long a possible.
2. Why do we need a strategy?
I got the diagnosis on the phone by somebody I had never met telling me, “Your husband has
Alzheimer’s and vascular dementia.” That was probably the worst possible way.
That was absolutely infuriating. (Carer)
They didn’t give me enough information. I came away thinking, “What do we do now, where to
go from here?” I have a prescription in one hand and a note for blood tests in the other and
nobody had said what the CAT scan showed… nobody had given me the information.
I am the person who is going to deal with my husband. (Carer)
Living Well with Dementia. P31-32
2.1. The priority for NHS Kensington and Chelsea is to be the health advocate for every person in our Borough. Yet we know that many people are still not receiving the services they need or in the way they want them. We need a strategy to deliver the vision set out in the foreword, so that everyone has access to excellent dementia services.
2.2. As people are living longer, we will see a growth in the number of people with dementia. We need to plan ahead to ensure that this group of people have the best experience of life for as long as possible.
2.3. There is also a group of people who experience young onset dementia – before the age of 65. This can manifest itself in behaviour changes which are hard to identify given that people may not consider dementia as a cause. This then contributes to added stress for the person developing the illness, their family and those working with them.
2.4. We know from talking with people with dementia, their carers and professionals, that while there are some excellent services in the Royal Borough, they are not joined up. This is further examined in Section 5 of this document. As a result, people have to negotiate different care pathways and may not receive the services they need and to which they are entitled. If we are to challenge the view that a diagnosis of dementia is the end of active life, we need services which provide the right support to each individual so that they can plan and live their life to the full.
234572 Dementia Strategy Doc.indd 4 10/8/10 12:47:00

Use your NHS well5
2.5. This is a joint strategy because the PCT and Royal Borough understand that it is not possible to provide joined up, seamless services at the right level for each person, unless we plan, commission and implement a new approach together. This will also involve joint management of budgets, where this supports our vision.
2.6. The Government’s strategy on dementia was published in February 2009. Living Well with Dementia: A National Dementia Strategy i, sets out public expectation and government requirements for quality of care. The strategy describes three key themes along the pathway: • Raising awareness and understanding, • Early diagnosis and support, • Living well with dementia.
2.7. These themes underpin the Kensington and Chelsea pathway as set out at Section 7 of this document. They provide a framework for our strategy to provide excellent local services. The thinking in the national strategy has been further developed by Healthcare for London in the Dementia Services Guideii published in October 2009. These documents need to be read alongside the National Carers’ Strategy iii and the End of Life Strategy iv, as part of the national framework to support people with dementia.
3. What does our strategy cover?
3.1. First and foremost our strategy is about prevention and early diagnosis, so that the experience of individuals is improved in relation to all aspects of the disease. As well as this work, we will examine the role and effectiveness of existing and new services at every stage of the dementia pathway.
3.2. In designing our strategy, we have reflected the national guidance in our local planning. We have also linked our approach to the development plans for other services, which affect the same population.
The strategy broadly covers the following areas with more detail provided in Appendix 1 to this document:
3.2.1. Prevention and early intervention: This includes information and advice on how to avoid dementia and where to go for advice if you feel
that you, or someone you know, may be showing signs of the disease. Central to this is clarity about where to seek help and what to do.
Prevention and early intervention are key to tackling stigma in relation to dementia, which comes from fear and not knowing what can be done.
3.2.2. Carers: We understand in Kensington and Chelsea that we have an irreplaceable resource in our carers, across
the spectrum of need. For people with dementia, research indicates that people with a carer are 20 times less likely to need residential carev. Looking after our carers is integral to this strategy.
3.2.3. Community based care: Where possible, we will provide services through primary and community services.
As set out above, dementia is a term covering a range of disorders affecting the brain. Some of its manifestations may be challenging and best treated by mental health experts. However, the association with mental illness can be difficult and frightening. In order to achieve our vision, we know that destigmatising dementia is important. We would therefore not envisage our services being based within mental health, except where needed.
3.2.4. Intermediate Care: Intermediate care is a time-limited recovery programme over 6 – 8 weeks, to support people to regain
their confidence and skills after a period of illness or relapse. It aims to end the process by which admission to hospital all too often leads to transfer to residential care, rather than a return home.
234572 Dementia Strategy Doc.indd 5 10/8/10 12:47:00

6
There is a strong link between modernising current dementia services and the development of intermediate and care for older people teams run by primary care. These are designed to reduce use of hospital and residential care, and improve the quality of life for people with dementia and their carers.
3.2.5. People with Learning Disabilities: People with learning disabilities are more vulnerable to developing dementia than the general
population. As this group lives longer, we will see an increase in the incidence of dementia. Our services need to encompass their needs.
All too often a diagnosis of dementia is missed in a person with a learning disability due to a double risk of ‘diagnostic overshadowing’ i.e. when a person’s main condition (learning disability) leads to clinicians not considering further underlying issues and diagnoses – such as dementia in a case of changed behaviourvi.
We will produce a joint strategy on learning disabilities in 2010, which will include the specific needs of those in this group affected by dementia.
3.2.6. Medication issues: There is research to show that people with dementia, including those in residential care, may be
inappropriately maintained on anti-psychotic drugs for long periods. The Government has pledged to challenge thisvii. At the same time, there is research showing that use of pain relief medication may be lower than for those without dementiaviii. The over-use of antipsychotic drugs in people with dementia and the under-prescribing of pain control will be addressed in our services and monitoring processes.
3.2.7. End of Life: Our strategy includes a commitment that people who choose to die at home, are supported in so
doing, including those with dementia.
4. Who has been involved in putting together this strategy?
4.1. The Department of Health produced Living Well with Dementia: A National Dementia Strategy in February 2009. This underpins our approach.
4.2. There have been three main groups involved in developing our local approach to the national guidance. These groups are carers and people with dementia, clinicians and independent experts in providing services for people with dementia:
4.2.1. Carers and people with dementia: In August 2008, an event was organised in the Borough on prevention and early diagnosis of
dementiaix. Those attending included carers and people with dementia, members of the public wishing to know more about prevention, and members of the Health and Social Care Reference Group for Older People.
234572 Dementia Strategy Doc.indd 6 10/8/10 12:47:01

Use your NHS well7
As we progress to implement the strategy, we will set up further stakeholder events and other ways to support good communication between commissioners and those affected by dementia.
4.2.2. Providers in statutory, voluntary, private and social care fields: A steering group of clinical and voluntary sector providers has provided important information on what
is available in the Borough and how this might be improved. With the launch of the national strategy, this information was contextualised.
As we move forward, we will develop new and existing roles to meet the needs of developing services. This means that we will work on our workforce and how best to use the skills and resources we have in our staff, current or future. We will work with key stakeholders to identify and support innovation, including joint appointments, training and budgets.
4.2.3. Independent experts: The Dementia Services Development Centre in Stirling (NDSC), a recognised international expert
resource on the management of dementia, has provided an independent review of our services and building design. They have identified improvements to the pathway from an external perspective. DSDC will deliver a programme of training for people working with people with dementia in care homes, hospital and the community during 2010-11. They will also audit a number of our premises so that we make them as accessible to people with dementia as possible, and will advise on what changes at home will help people live there longer. Their expertise will be sought as we develop our local pathway.
5. Local Context
5.1. Information source: Information used in this section is from the Dementia Services Guide, Appendix 1x and the Kensington and Chelsea Joint Strategic Needs Assessment (JSNA)xi.
5.2. Number and identification: • There are approximately 700,000 people in the UK with dementia, of which 570,000 are in England. • This translates to 64,600 people with dementia in London. • Kensington and Chelsea has an estimated 1,451 residents with dementia. Of these, 140 (10%) are
estimated to be from Black and minority ethnic (BME) groups. • Identification of people with dementia averages 37% across London – and is currently at 34% in
Kensington and Chelsea. Increasing the level of detection so that effective services can be planned for and provided, is a priority for our vision to be delivered.
5.3. Growth:
5.3.1. The number of people with dementia will grow: • Nationally, it is estimated that it will double over 30 years, to 1.2m. • In London there is estimated to be an increase of around 14% (or 8,200 additional people) between
2005 and 2021. • For Kensington and Chelsea, PCT-based estimates differ from estimates published in the Dementia
Services Guide. • The Dementia Services Guide (which uses figures from Dementia UK) estimates that Kensington and
Chelsea will experience the greatest rise in London, with a 54% rise between 2005 and 2021, or around 700 additional people.
• However, NHS Kensington and Chelsea estimate a far more modest rise in the borough, of about 9% between 2005 and 2021, or around 120 people.
234572 Dementia Strategy Doc.indd 7 10/8/10 12:47:01

8
5.3.2. The PCT considers the Dementia UK estimate for Kensington and Chelsea to be unrealistically high, as it uses the Office for National statistics (ONS) population projections to predict population growth. These projections are not used locally due to methodological weaknesses. The PCT’s own estimates are generated from the GLA (low) population projections and are felt to be more realistic, particularly given past trends in population growth.
5.3.3. Using the PCT estimates, which take into account the changing age and ethnic structure of the population, the estimated number of people from Black and minority ethnic groups with dementia is summarised below. There will be a rising proportion of patients from these groups:
Estimated increase of people with dementia, and proportion of those people from BME groups, over time
Total number of people with dementia
Number from BME groups
Proportion of total from BME groups
2005 1,380 120 9%
2010 1,410 150 11%
2015 1,450 180 12%
2021 1,500 210 14%
Source: NHS Kensington and Chelsea Public Health. Date rounded to nearest 10. Using Ethnic GLA (low) 2008
5.4. Accommodation: • Living alone is a risk factor for identifying dementia, and may lead to under-stimulus which is also a
risk. With 61% of our older people living on their own, the highest proportion in London, our services need to be particularly sensitive in reaching people who are isolated.
• At the same time, and as a function of pressure on accommodation in the Royal Borough, there are very few specialised dementia beds in residential care within Kensington and Chelsea. People may be placed outside the locality, but it is also the case that a lot of care is provided at home. Ensuring excellent quality of care for all our residents, wherever they are, must be achieved.
• We have started a project with colleagues in the Supporting People Team to examine alternatives to residential care. This includes independent tenancies with support, and the role of ‘floating support’ teams which come to where the person with dementia is living.
• Another aspect of this strategy is to improve access to, and design of, housing in the Borough for people with dementia, so that they can live independently, with their carer or professional support, for longer.
• We will ensure that new developments for older people in the Royal Borough benefit from these lessons, and we will look at how the concept of lifetime communities which is being developed in the United States to support elders there, might be applied in Kensington and Chelseaxii.
5.5. Hospital admissions and stays • We are working with colleagues in acute hospitals to provide support to people with dementia
during hospital stays. A key part of this is having well-defined pathways out of hospital. In this way, clinicians in hospitals are clear and confident about where a patient will go for ongoing care. We will also use the opportunities provided by the voluntary sector to support people and their carers in hospital settings.
• Care for people with dementia may be sub-optimal for hospital admissions where the primary diagnosis is not dementia. There is a need to ensure that dementia is recorded and managed regardless of the acute medical or surgical condition being treated. This will be addressed in the service level agreements with acute providers. Acute hospitals should also ensure that people admitted with
234572 Dementia Strategy Doc.indd 8 10/8/10 12:47:01

Use your NHS well9
dementia, who may not be known to services in primary care or mental health have a care pathway developed and that this is communicated to the appropriate clinical service for ongoing care.
• The intermediate care team, rapid response team and training programmes are essential to providing a support system when people leave hospital.
5.6. Carer and User experience: Insight gained from the consultation event with carers and people with dementia in August 2008 was that: • Services are not joined up, and are hard to navigate or know about. • Too few professionals outside of specialist services are able to identify or manage dementia effectively. • Rapid specialist assessment was wanted, with 50% wanting their GP to tell them the news, and 50%
a specialist. • Continuity of care is important, but there was divided view on whether this should be via familiar
services or a new provision such as a dementia nurse or someone to guide the person with dementia through services.
• Our strong voluntary sector needs to be part of the partnership provision in Kensington and Chelsea.
6. So, how are services currently provided?
6.1. In this section we look at services and gaps. An overriding theme is that there are good services in the Borough, but they are not well connected, or integrated with other services.
6.2. The project board for the dementia strategy gave us an understanding of local services. These were then independently reviewed by the Dementia Services Development Centre. The findings from this work are summarised below:
6.3. Primary Care:
6.3.1. During the visit by Professor June Andrews of the Dementia Services Development Centre, it was apparent that the absence of a referral pathway to specialist assessment and non-clinical support is an obstacle to GP management of patients with dementia.
6.3.2. There is also a need for appropriate training for all primary care staff – and other health groups – to identify dementia and be aware of non-pharmacological treatments that can be delivered in primary care.
• Gap: clearly defined pathway of care; training.
6.4. Specialist services:
6.4.1. While there is some excellent practice and expertise in the Borough, there are different services in the north and south providing widely different experiences for patients and carers. Neither the north nor south of the Borough has access to all the basic provision recommended in the Dementia Services Guide (endnote 2).
• Gap: consistent and integrated pathway of care.
234572 Dementia Strategy Doc.indd 9 10/8/10 12:47:05

10
6.5. Hospital care:
6.5.1. There is work to be done to improve the speed of discharge from hospital for people with dementia and to provide alternatives to transferring people to residential care from hospital.
6.5.2. Hospital staff feel they cannot discharge, unless they are clear that the person will cope at home. • Gap: dementia leadership in hospital, pathway, training, rapid response and intermediate service,
integrated response, design audit and advice for the home.
6.6. Accommodation:
6.6.1. There is limited space in the Borough for new accommodation. We need to make the most of what we have in private and publicly-owned provision, with the aim of encouraging and supporting independent living for as long as possible.
6.6.2. In order to achieve this, we will provide design advice to private and publicly owned provision as part of the care package. We will also improve access to information about equipment and adaptations.
• Gap: design audit and advice.
6.7. Day and residential care:
6.7.1. As above, residential care in the Borough is limited. All day care for older people in the borough is subject to a review at this time. One of the issues the review will address is what dementia-specific day care is required, and how people with dementia who wish to use standard day care can be supported in doing so.
6.7.2. Training and design of buildings is variable in these settings, with staff expressing an interest in further development.
• Gap: training, design audit and advice for centres.
6.8. Partnership between the PCT and Borough:
6.8.1. There has been a history of developing services without reference to each other’s development. This is inefficient and has contributed to the complexity and fragmentation of pathways.
• Gap: integrated planning, effective commissioning linked to need, non-clinical guidance through the pathway.
6.9. The Voluntary Sector:
6.9.1. The Borough is well endowed with voluntary organisations with an interest in dementia care, as well as carer support. In a shrinking financial climate, Dr Andrews identified the potential benefits of more focus in carer support and provision for people with dementia.
• Gap: training; effective commissioning linked to need.
234572 Dementia Strategy Doc.indd 10 10/8/10 12:47:05

Use your NHS well11
7. Turning the vision into reality – where we want to be in five years time
By bringing together the information gathered in this report, we can see where we have good services, and where there are gaps or room for improvement. We have considered different ways to deliver the necessary change, and have chosen to identify a set of outcomes and to deliver these through a selected number of the objectives from Living Well with Dementia: A National Dementia Strategy.
We believe that by focussing our plan around these outcomes and objectives, we will have the basis to deliver swift and effective change.
7.1. How will we know our new services are working?We will focus achievement around three key outcomes:
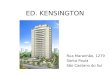
7.1.1. First, we will construct a single pathway so that people are maintained at home for as long as they, and their carer want. According to the Dementia Development Centre at Stirling University people with dementia can often avoid hospital admissions and long term care if the right services are in place. People with dementia rarely come out of hospital at their previous level of functioning. Early diagnosis and support will help people with dementia to stay at home for longer in future. To illustrate the change the strategy hopes to achieve, the graph below compares a typical pathway with the anticipated pathway resulting from early diagnosis and improved support. It should be noted that these are generalisations and each case leads to a slightly different trajectory.
7.1.2. Second, we will check that people with dementia and their carers know what to do and
where to find advice and support right from the start. For this to happen, there needs to be a clear point of access to services and advice along the way. This support may be supplied by someone from the statutory or voluntary sector who can act as a guide and companion throughout the course of the illness.
7.1.3. Third, we will see a better understanding of dementia – amongst professionals and the public. This involves information and training, supporting GPs to feel able to make effective diagnosis and treatment plans for people with dementia, and an associated rise in identification of people with the disease from its current level of 30% up to at least 60% in three years.
7.2. How will we achieve those outcomes?We will measure progress using the 17+ objectives set out in the National Dementia Strategy.
We will measure our achievement of these objectives against the 15 standards set out in the Department of Health and London Councils audit of dementia services in the Capital, launched in December 2009. The description of these standards can be seen at Appendix 2.
Intensity of care
Care in hospital
Care at home
Usual pathway
Pathway in future
Time elapsed since diagnosis
234572 Dementia Strategy Doc.indd 11 10/8/10 12:47:05

12
These two quality measures are brought together in the following table:
Measuring success in Kensington and Chelsea – using the national objectives and pan-London standards:
NDS priority Action in K&C DH and London Council Standards
Objective 1: Improving public and professional awareness of dementia
• We will focus current social marketing and public health campaigns on tackling those areas that support people in avoiding vascular dementia – such as stopping smoking, managing their alcohol intake and avoiding weight gain.
• We will work with people with dementia and their carers to find ways to address stigma, as a key barrier to people accessing services early on.
• 2• 4• 5• 14
Objective 2: Good quality early diagnosis and intervention for all
• Health care professionals including those in generic services will receive the training they need to identify dementia through using standard screening tools, assessments and investigations.
• Initial assessment and investigations will take place in primary care including those outlined in the NICE-SCIE guidelines e.g. for identifying causes of confusionxiii. If a diagnosis of dementia requiring specialist investigation or support is suspected, the clinician will then refer the patient on.
• The specialist service will be part of a single care pathway.
• 14• 3• 10
Objective 3: Good quality information for people with dementia and their carers
• We will provide written and web-based products providing information about dementia and its treatment.
• We will include dementia in our literature on mental wellbeing and prevention.
• We will work with existing groups of service users and carers to integrate this information into other packs so that awareness of dementia is raised.
• We will support the voluntary sector provision of courses about dementia.
• 4• 2
Objective 4: Enabling easy access to care, support and advice following diagnosis
• We will make sure that all patients with dementia are added to the GP register of dementia patients.
• Also, that where there is a diagnosis of dementia, people and their carers receive post diagnostic counselling, support and information.
• We will put in place senior clinical advice for those working in the community and hospital.
• We will also put in place a system by which there is referral to a non-clinical dementia guide to be the key point of contact to advocate for the patient and carer. They will ensure that
• 2•8
234572 Dementia Strategy Doc.indd 12 10/8/10 12:47:05

Use your NHS well13
NDS priority Action in K&C DH and London Council Standards
people have access to Living Well planning including information for patients and carers, links into social networks, learning activities, cognitive stimulation and physical exercise and a regular review of well being.
• The contact will also provide links to personalisation advice and financial planning including income maximisation support.
• Each person with dementia will have a care planning programme: this will include review of physical health needs, and review of psychological needs with special care for vulnerable groups including women living alone, people with learning disabilities, people over 85, and those with co-morbidities.
• Information must be shared with other professionals.
Objective 5: Develop structured peer support and learning networks
• We will continue to support the networks for service users and carers which are available through leisure, nutrition and exercise provision in the Royal Borough.
• We will work with providers to develop a cohort of people who will lead on dementia in their place of work.
• 2 • 8
Objective 6: Improve community personal services for people living at home
• Through partnership we will provide integrated services to support people in remaining at home.
• 10• 14
Objective 7: Implement the New Deal for Carers
• We will seek out carers of people with dementia so we can offer a carers’ assessment and services, including respite care, time to look after themselves, and the support of other carers.
• Older people in particular are hard to find as those in receipt of a pension do not receive a carers’ grant. We will make specific issues to find older carers of people with dementia.
• 10
Objective 8: Improve the quality of care for people with dementia in general hospitals
• We will ensure that our rapid response, intermediate and other services support the speedy discharge of people with dementia from hospital.
• We will provide hospital staff with training and information about the pathway available so that they feel able to move people back home, knowing they will be supported.
• We will ensure that information is shared between professionals, including end of life planning.
• 9• 15
234572 Dementia Strategy Doc.indd 13 10/8/10 12:47:05

14
NDS priority Action in K&C DH and London Council Standards
Objective 9: Improved intermediate care
•We will integrate our planning of dementia services with colleagues in intermediate care.
• 10
Objective 10: Considering the potential for housing support and related services
• We will develop a strategy around accommodation with colleagues in Supporting People and social care.
• We will work towards commissioning services for people with dementia only from those organisations which have received and acted upon a dementia design audit and where staff have undertaken an appropriate level of training in dementia care.
• 11• 15• 7
Objective 11: Living well with dementia in care homes
• As with other forms of accommodation, we will work towards commissioning services for people with dementia only from those organisations which have received and acted upon a dementia design audit and where staff have undertaken an appropriate level of training in dementia care.
• 12• 15
Objectives 12: Improved end of life care
• We will establish communication between clinical groups so that end of life planning is understood and respected. This includes out of hours systems.
• 13
Objective 13: An informed and effective workforce for people with dementia
• Training to be integrated as a requirement in contracts.
• We will source and promote good training opportunities.
• 14
Objective 14: A joint commissioning strategy for dementia
•This strategy will be supported by implementation and monitoring processes.
•1
Objective 15: Improve assessment and regulation of health and care services and of how systems are working
• Quality outcomes to be integrated into contracts.
• 15
Objective 16: Provide a clear picture of research about the causes and possible future treatments of dementia
• We will work with experts in the field to ensure that our services are based on excellent research.
• We will support and promote research and teaching to improve care.
• 2• 4
Objective 17: Effective national and regional support for local
• We will use the guidance available nationally, through London and through independent experts to implement our strategy to achieve excellent services.
• 1
234572 Dementia Strategy Doc.indd 14 10/8/10 12:47:05

Use your NHS well15
8. Next steps – what we will do next?
• We will develop a service specification for the service based on the feedback we have received from clinicians, providers, people with dementia and their carers.
• We will set out an action plan for change, and how we will commission that change through redesign or recommissioning.
• We will share our progress with the public and professionals and make further change based on their feedback.
• We will make the best use we can of our resources locally and nationally.
9. Conclusion
The Kensington and Chelsea Dementia Strategy is a five-year commitment to redesigning and, where necessary, recommissioning services to address gaps identified by needs assessment, including feedback from clinicians, providers, those using services and the public.
The strategy is based around a vision grounded in improving patient outcomes.
We would like to thank all those who have taken part in the journey so far.
234572 Dementia Strategy Doc.indd 15 10/8/10 12:47:06

16
Appendix 1: Summary of key policy documents in Kensington and Chelsea
Intermediate Care programme:
This development is a service to provide short-term treatment, which consists of an assessment followed by a short-term, intensive rehabilitation programme for a maximum of 8 weeks. The aim of this package is to enable people to return home after a spell in hospital. At the moment, a number of people go from hospital to residential care, because they appear to be unable to manage at home. While this may be the case in the short-term after discharge, when a person may be disorientated and feel nervous about a return home, the situation can change with intermediate care providing an intensive recovery-focussed programme over 8 weeks. At the end of this, the person may have regained their health and confidence, and not need residential care.
While many older people may become disorientated and lose confidence on entering hospital, this is much more the case for those with dementia. Once in unfamiliar surroundings, people with dementia are vulnerable to losing what capacity they have for independence. In addition, they may have problems communicating their basic needs such as for pain relief. All this will add up to give an appearance of much greater vulnerability and need for residential care, than if they were assessed at home. The longer a person with dementia is in hospital, the more disorientated they may become and less able to pick up the threads of their previous life.
Therefore, intermediate care has a particularly valuable role for people with dementia in supporting timely discharge from hospital, and a focussed rehabilitation programme in the familiar surroundings of their own home.
Intermediate care is evidence based, including in the treatment of people with mild to moderate dementia. For this reason, development of intermediate care and the dementia pathway are linked in Kensington and Chelsea.
Rapid Response:
This is a Borough-led programme to retain people at home when they are imminently about to be hospitalised. It dovetails with the intermediate care development by keeping people out of hospital in crisis
Carer’s Joint Strategy 2009 – 2013:
The strategy reflects the priorities of the national carers’ strategy: Carers at the Heart of 21st Century and Families and Communities (2008). These will be achieved through a step change in services.
This will include the development of a carer-led support and information ‘hub’; increased personalisation; carer breaks to attend their own medical appointments; increase provision for respite.
Mental health for older people:
The development of two community mental health teams for older people was undertaken in 2007-8, which has expanded community provision considerably, and led to a reduction in bed use.
Memory services have grown up in the north and south – with a clinic based at Chelsea and Westminster in the south, and an assessment service in a day hospital in the north of the Borough. Neither of these services provides access to the full range of provision suggested in the Dementia Services Guide, and our plan will address these gaps, while providing equality of provision across the Borough.
234572 Dementia Strategy Doc.indd 16 10/8/10 12:47:06

Use your NHS well17
Primary care:
An older people’s team is planned by practice based commissioning. Work is underway to integrate this with plans around dementia, intermediate care and rapid response planning.
End of Life:
End of Life Strategy 2008 -2011
This strategy sets out the PCT’s action plan in relation to end of life. It draws on national guidance and feedback from work with local people about where they would wish to die, and what support they would need for this to happen.
Delivering on this strategy will include a focus on those with dementia. A combination of forward planning, ensuring that all involved in the person’s care are aware of their plan and wishes, primary care involvement, support to the carer and effective use of rapid response and intermediate care, we will facilitate this essential element of a caring dementia pathway.
People with Learning Disabilities:
All too often a diagnosis of dementia is missed in a person with a learning disability due to a double risk of ‘diagnostic overshadowing’ i.e. when a person’s main condition (learning disability) leads to clinicians not considering further underlying issues and diagnoses – such as dementia in a case of changed behaviourvi.
A joint strategy for this group is being written. It will include the specific issues raised in this document around identifying and managing dementia for those with a learning disability who develop the disease. It will include planning around research indicating that pain control may be insufficient in those with a learning disabilityxiv.
Medicines management:
This encompasses two key areas at the moment: • A review of the use of antipsychotics at an individual level in any resident of this Borough. • Addressing the issue of effective management of pain for those with dementia.
There is research to show that people with dementia, including those in residential care, may be inappropriately maintained on anti-psychotic drugs for long periods. The Government has pledged to challenge this problemvii. At the same time, there is research showing that use of pain relief medication may be lower than for those without dementiaviii.
We will address this in our service plans, through training programmes, leadership and expert input to ensure that best practice is adopted everywhere.
234572 Dementia Strategy Doc.indd 17 10/8/10 12:47:06

18
Appendix 2: Standards for the audit of dementia services in London
Department of Health and London Councils, December 2009:
Standard Description
1 A Local Joint Commissioning Strategy for People with Dementia and their Carers
2 Dementia Awareness and Healthy Living
3 Access to an Integrated Care Pathway
4 Information and Support
5 Dementia Advisory Role
6 Peer Support Networks
7 Support at Home
8 Support to Carers
9 General Hospital Care
10 Intermediate Care
11 Environmental Interventions
12 Care Homes
13 End of Life Care
14 Skilled Workforce
15 Provision of Quality Services
234572 Dementia Strategy Doc.indd 18 10/8/10 12:47:06

Use your NHS well19
Endnotesi Department of Health. (2009). Living Well with Dementia: A National Dementia Strategy. Gateway
ref 11198. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_094058
ii Healthcare for London. (2009). Dementia Services Guide. http://www.healthcareforlondon.nhs.uk/assets/Mental-health/HealthcareforLondon_Dementia-services-
guide.pdf
iii Department of Health. (2008). Carers at the Heart of 21st Century Families and Communities: a caring system on your side, a life of your own. http://www.dh.gov.uk/en/publicationsandstatistics/publications/publicationspolicyandguidance/DH_085345
iv Department of Health. (2008). End of Life Care Strategy – promoting high quality care for adults at the end of life. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_086277
v Banerjee S et al. Predictors of institutionalisation in people with dementia. Journal of Neurology Neurosurgery and Psychiatry. 74:1315-1316, 2003
vi Dementia and people with learning disabilities: guidance on assessment, diagnosis, treatment and support of people with a learning disability who develop dementia. Royal College of Psychiatrist. 2009. http://www.rcpsych.ac.uk/files/pdfversion/cr155.pdf
vii http://www.dh.gov.uk/en/News/Recentstories/DH_108330
viii Pain in Older People and People with Dementia: A practice guide. DSDC 2007. http://www.dementia.stir.ac.uk
xi Transforming the quality of dementia care: consultation on a national dementia strategy. 11.9.08. Available from [email protected]
x Dementia Services Guide, Appendix 1. http://www.healthcareforlondon.nhs.uk/assets/Mental-health/01-Dementia-Needsassessment-v2.0.pdf
xi Kensington and Chelsea Joint Needs Assessment. Fact Sheets 2009. http://www.rbkc.gov.uk/voluntaryandpartnerships/healthandwell-being/datafactsheets/healthill-healthdisability.aspx
xii Creating Communities for a Lifetime http://www.community4alifetime.org/
xiii NICE-SCIE. Joint publication: Dementia – Supporting people with dementia and their carers in health and social care. http://www.scie.org.uk/publications/misc/dementia/index.asp
xiv Responding to the pain experience of older people with a learning difficulty and dementia. Joseph Rowntree Foundation. Kerr, D; Cunningham C; Wilkinson H. www.jrf.org.uk
234572 Dementia Strategy Doc.indd 19 10/8/10 12:47:06

234572 Dementia Strategy Doc.indd 20 10/8/10 12:47:06