Embed Size (px)
Citation preview

Robert L. Talbert, Pharm. D.College of Pharmacy
The University of Texas at AustinSchool of Medicine
University of Texas Health Science Center at San Antonio
JNC 8 (VIII): What new is going to be in the
guidelines?

Objectives2
Review JNC VII Current BP definitions Recommended therapy stage 1 and stage 2 Compelling indications
Discussion current trials and relevant older studiesSpeculate how JNC VIII might look

Hypertension3
Persistent elevation of arterial blood pressure (BP)National Guideline
7th Report of the Joint National Committee on the Detection, Evaluation, and Treatment of High Blood Pressure (JNC7)
~72 million Americans (31%) have BP > 140/90 mmHgMost patients asymptomatic Cardiovascular morbidity & mortality risk directly
correlated with BP; antihypertensive drug therapy reduces cardiovascular & mortality risk
Chobanian AV, et al. Hypertension 2003;42(6):1206–1252.

Target-Organ Damage4
Brain: stroke, transient ischemic attack, dementiaEyes: retinopathy Heart: left ventricular hypertrophy, anginaKidney: chronic kidney disease Peripheral Vasculature: peripheral arterial disease

Adult Classification 5
Classification Systolic Blood Pressure (mmHg)
Diastolic Blood Pressure (mmHg)
Normal Less than 120 and Less than 80
Prehypertension 120-139 or 80-89
Stage 1 hypertension 140-159 or 90-99
Stage 2 hypertension > 160 or > 100
Chobanian AV, et al. Hypertension 2003;42(6):1206–1252.

Classification for Adults6
Classification based on average of > 2 properly measured seated BP measurements from > 2 clinical encounters
If systolic & diastolic blood pressure values give different classifications, classify by highest category
> 130/80 mmHg: above goal for patients with diabetes mellitus or chronic kidney disease
Prehypertension: patients likely to develop hypertension

Treatment Goals7
Reduce morbidity & mortality Select drug therapy based on evidence demonstrating
risk reduction
Patient Population Target Blood PressureMost patients < 140/90 mmHgDiabetes mellitus < 130/80 mmHgChronic kidney disease <130/80 mmHg
Chobanian AV, et al. Hypertension 2003;42(6):1206–1252.

2007 AHA Recommendations8
More aggressive BP lowering for high risk patients
Rosendorff C, et al. Circulation 2007;115(21):2761–2788.
Most patients for general prevention <140/90 mmHgPatients with diabetes (CAD risk equivalent), significant CKD, known CAD (MI, stable angina, unstable angina), noncoronary atherosclerotic vascular disease (ischemic stroke, TIA, PAD, abdominal aortic aneurism [CAD risk equivalents]), Framingham risk score > 10%
<130/80 mmHg
Patients with left ventricular dysfunction (HF) <120/80 mmHg

ALLHAT9
Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)
Primary endpoints fatal CHD nonfatal MI
Secondary endpoints other hypertension-related complications
HF stroke
ALLHAT Officers and Coordinators. JAMA 2002;288(23):2981–2997.

ALLHAT10
Prospective, double-blind trial randomized patients to:
chlorthalidone amlodipine doxazosin lisinopril-based therapy
42,418 patients: age > 55 yr with HTN + 1 additional CV risk factor (mean subject participation 4.9 years)
Thiazide-type diuretics remain unsurpassed for reducing CV morbidity & mortality in most patients
ALLHAT Officers and Coordinators. JAMA 2002;288(23):2981–2997.

JNC7 Recommendations11
Thiazide-like diuretics preferred 1st line therapy based on clinical trials showing morbidity & mortality reductions ALLHAT confirms 1st line role of thiazide diuretics
Compelling indications: comorbid conditions where specific drug therapies provide unique long-term benefits based on clinical trials drug therapy recommendations are in combination with or in place
of a thiazide diuretic
Chobanian AV et al. Hypertension 2003;42(6):1206–1252.

Clinical Controversy12
Avoiding Cardiovascular Events through COMbination Therapy in Patients LIving with Systolic Hypertension (ACCOMPLISH)
Endpoint: composite of death from CV causes, hospitalization for angina, nonfatal MI or stroke, coronary revascularization, & resuscitation after cardiac arrest
Prospective, double-blind, industry sponsored trial randomized patients to benazepril + amodipdine or benazepril + HCTZ 11,506 patients with HTN & high CV risk
Combination benazepril + amlodipine superior to benazepril + HCTZ for reducing CV events in high risk patients
Jamerson KA, et al. N Engl J Med. 2009;359(23):2417-2428.

13ACE: angiotensin-converting enzyme; ARB: angiotensin receptor blocker; CCB: calcium channel blocker; DBP: diastolic blood pressure; SBP: systolic blood pressure

1414

Lifestyle Modifications15
Modification Recommendation
Approximate Systolic Blood Pressure Reduction (mm Hg)a
Weight loss Maintain normal body weight (body mass index 18.5–24.9 kg/m2)
5–20 per 10-kg weight loss
DASH-type dietary patterns
Consume a diet rich in fruits, vegetables, and low-fat dairy products with a reduced content of saturated and total fat
8–14
Reduced salt intake
Reduce daily dietary sodium intake as much as possible, ideally to 65 mmol/day (1.5 g/day sodium, or 3.8 g/day sodium chloride)
2–8
Physical activity
Regular aerobic physical activity (at least 30 min/day, most days of the week)
4–9
Moderation of alcohol intake
Limit consumption to 2 drinks/day in men and 1 drink/day in women and lighter-weight persons
2–4DASH, Dietary Approaches to Stop Hypertension.a Effects of implementing these modifications are time and dose dependent and could be greater for some patients.
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy:A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com/

MRFIT Design10.5 Year Follow Up
• Randomized 1° prevention in 12,866 high risk men aged 35-57 yr with DBP >90 mmHg
• Interventions included dietary counseling for cholesterol reduction, smoking cessation and control of high blood pressure– Usual care– Special intervention using stepped care
• Diet• HCTZ or chlorthalidone: 50 or 100 mg daily• Antiadrenergic • Arteriolar vasodilator
• Primary end point – CHD mortality
MRFIT Research Group. Circulation 1990;82:1616-1628

MRFIT Design
• In 1st half of 1980, DSMB recommended that chlorthalidone, not HCTZ be the step 1 diuretic for SI hypertensive men– Maximum dose to be 50 mg QD
• “The data leading to the protocol change indicated that in the 9 clinics whose staff prescribed HCTZ predominantly, the trend of mortality was unfavorable for SI men compared to UC men, whereas it was favorable in the 6 clinics whose staff primarily used chlorthalidone.”
MRFIT Research Group. Circulation 1990;82:1616-1628Bartsch G, et al. Circulation 1984:70 (suppl II):1438

Predominately Prescribing HCTZ Before April 1980
CHD All cause
SI rate UC rate Diff (%) SI rate UC rate Diff (%)
Up to 3/80 3.17 2.18 +44% 5.76 4.96 +16.5
4/80-12/85 3.73 5.17 -28% 9.68 12.97 -25.5
Thru 12/85 3.46 3.74 -7.9 7.82 9.15 -14.8
MRFIT Research Group. Circulation 1990;82:1616-1628

Predominately Prescribing Chlorthalidone Before April 1980
CHD All cause
SI rate UC rate Diff (%) SI rate UC rate Diff (%)
Up to 3/80 1.56 3.68 -58.2 4.29 7.17 -30.9
4/80-12/85 3.84 4.31 -8.4 9.24 9.13 +2.5
Thru 12/85 2.76 4.01 -30.3 6.9 8.21 -15.7
MRFIT Research Group. Circulation 1990;82:1616-1628

ANBP-2: Study Overview
20
6083 patients with mean age of 72 years (aged 65-84 years) An older population than ALLHAT 97% white
Randomization to either ACEI or mostly HCTZ Additional drugs could be used to reach goals
(beta-blockers, CCBs, alpha-blockers)Subjects followed for a median of 4.1 yearsPrimary end point: number of total CV events or death
from any cause
ANBP2: Second Australian National Blood Pressure Study.
Wing LMH et al. N Engl J Med. 2003;348:583-592.

ANBP-2: Inclusion and Exclusion
21
Inclusion: Average SBP of 160 mm Hg or Average DBP of 90 mm Hg, with SBP of 140 mm Hg Absence of CV events in past 6 months
Exclusion Life-threatening illness Contraindication to ACEI or diuretic Plasma creatinine of more than 2.5 mg/dL Malignant HTN Dementia
Wing LMH. N Engl J Med. 2003;348:583-592.

ANBP-2 Blood Pressures
Wing LMH. N Engl J Med. 2003;348:583-592.
NSD

ANBP-2: Results
• No difference between the groups in the change of DBP at any time point• Pattern of BP reduction with 2 treatments was similar among men and women
23
Wing LMH. N Engl J Med. 2003;348:583-592.

Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)
• R, DB, active control trial in 33,357 participants ≥55 yo with HTN and 1 other RF
• Interventions– Chlorthalidone 12.5-25 mg/d– Amlodipine 2.5-10 mg/d– Lisinopril 10-40 mg/d
• Primary outcome: Combined fatal CHD or nonfatal MI• Analysis ITT
ALLHAT Officers. JAMA 2002;288:2981-97

Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)
ALLHAT Officers. JAMA 2002;288:2981-97
“No difference between treatments”

ALLHAT Pre-specified SubgroupsHeart Failure-Amlodipine
ALLHAT Officers. JAMA 2002;288:2981-97

ALLHAT Pre-specified SubgroupsHeart Failure-Lisinopril
ALLHAT Officers. JAMA 2002;288:2981-97

PK/PD of HCTZ and Chlorthalidone
Carter BL, et al. Hypertension 2004;43:4-9

HCTZ vs. Chlorthalidone
R, single-blinded 8 week, XO study in 30 patientsChlorthalidone 12.5 mg/d force titrated to 25 mg/dHCTZ 25 mg/d force titrated to 50 mg/d24 hr ambulatory BP (main outcome) at baseline and 8
week + office BP measurements
Ernst ME, et al. Hypertension 2006;47:352-358

Ambulatory SBPMean SBP over 24 Hr, Daytime, Nightime
Ernst ME, et al. Hypertension 2006;47:352-358

Mean Change in Ambulatory SBP
Ernst ME, et al. Hypertension 2006;47:352-358

Adverse Effects
• Mean change in potassium– Week 2
• HCTZ -0.3±0.4 meq/L• Chlorthalidone -0.4±0.4 meq/L
– Week 8• HCTZ -0.4±0.4 meq/L• Chlorthalidone -0.5±0.4 meq/L
• Similar % had hypokalemia• No patients experienced symptoms with hypokalemia
Ernst ME, et al. Hypertension 2006;47:352-358

Clinical ControversyCombined RAAS Therapy
33
CV events risk further reduced when ARB combined with an ACE inhibitor for patients with left ventricular dysfunction
Data supports ACE/ARB combination therapy for patients with severe forms of nephrotic syndrome
Combination ACE/ARB therapy not well studied as standard treatment for HTN
Significantly higher risk of adverse effects such as hyperkalemia and renal dysfunction

ONTARGETARB + ACEI
34
ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial (ONTARGET)
Endpoint: composite of death, dialysis, SCr doubling Prospective, randomized, multicenter, double-blind trial;
patients randomized patients to ramipril, telmisartan, combination of both 25,620 patients > age 55 yr with diabetes & end-organ damage or
established atherosclerotic vascular diseaseCombination therapy reduces proteinuria more than
monotherapy but worsens major renal outcomesMann JF, et al. Lancet 2008;372:547-543.

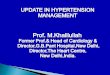
ONTARGET: Primary outcome results
Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial
N = 25,620 with vascular disease or high-risk diabetes
ONTARGET Investigators. N Engl J Med. 2008;358:1547-59.
Cumulativehazard ratio
0.20
0.15
0.10
0.05
0.000 1 2 3 4 5
Follow-up (years)
Telmisartan Ramipril Telmisartan plus ramipril

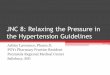
ONTARGET: Incidence of primary outcome and components
ONTARGET Investigators. N Engl J Med. 2008;358:1547-59.
*Patients could have multiple events in this category CV = cardiovascular, HF = heart failure, MI = myocardial infarction, RR = risk ratio.
Outcome
Ramipril (n = 8576)
Telmisartan (n = 8542)
Combination (n =
8502)Telmisartan vs ramipril
Combination vs ramipril
Primary outcome* 16.5% 16.7% 16.3% 1.01 RR
(0.94–1.09)0.99 RR
(0.92–1.07)
Death from CV causes 7.0% 7.0% 7.3% 1.00 RR
(0.89–1.12)1.04 RR
(0.93–1.17)
MI* 4.8% 5.2% 5.2% 1.07 RR (0.94–1.22)
1.08 RR (0.94–1.23)
Stroke* 4.7% 4.3% 4.4% 0.91 RR (0.79–1.05)
0.93 RR (0.81–1.07)
HF hospital-ization* 4.1% 4.6% 3.9% 1.12 RR
(0.97–1.29)0.95 RR (0.82–1.10)

ONTARGET: Secondary outcomes
OutcomeRamipril
(n = 8576)Telmisartan(n = 8542)
Combination(n = 8502)
Telmisartan vs ramipril
Combination vs ramipril
Death fromCV causes, MI, stroke
14.1% 13.9% 14.1% 0.99 RR(0.91–1.07)
1.00 RR(0.93–1.09)
Revasculari-zation 14.8% 15.1% 15.3% 1.03 RR
(0.95–1.11)1.04 RR
(0.97–1.13)
Angina hos-pitalization 10.8% 11.2% 11.2% 1.04 RR
(0.95–1.14)1.04 RR
(0.95–1.14)
Worsening/New angina 6.6% 6.3% 6.3% 0.95 RR
(0.84–1.07)0.96 RR
(0.85–1.08)
Any HF 6.0% 6.3% 5.6% 1.05 RR(0.93–1.19)
0.94 RR(0.83–1.07)
Renalimpairment 10.2% 10.6% 13.5% 1.04 RR
(0.96–1.14)1.33 RR*
(1.22–1.44)
ONTARGET Investigators. N Engl J Med. 2008;358:1547-59.*P < 0.001

3838

Renin Inhibitor39
1st agent FDA approved in 2007: aliskirenInhibits angiotensinogen to angiotensin I conversionFDA approved as monotherapy & combination therapy
with other antihypertensives Efficacy demonstrated with other antihypertensives
including amlodipine, HCTZ, ACEIs/ARBsDoes not block bradykinin breakdown
less cough than ACE InhibitorsAdverse effects: orthostatic hypotension, hyperkalemia

ALTITUDE Trial40
Aliskiren 300 mg/d or placebo + ACEI or ARBT2DM with albuminuria, AMI and reduced renal fucntion,
stroke and reduced renal function, CAD with reduced renal function
8,606 patients in 36 countriesTerminated due to increased risk and futility for efficacy

ALTITUDE Outcomes41
Variable Aliskiren (N=4283)
Placebo (N=4296)
HR 95% CI P-value
2° composite outcome-CV
444 (10.4%) 396 (9.2%) 1.14 0.99, 1.30 0.0664
Non-fatal stroke 112 (2.6%) 85 (2.0%) 1.34 1.01, 1.77 0.0439
ALTITUDE Warning Letter January 2012
Other endpoints including the composite primary outcome were notsignificantly different

Are We Using the Wrong Beta Blocker?Should Beta Blockers be First Line?
42
Atenolol is a commonly studied and used beta blocker T1/2 6-7 hours
Metoprolol succinate is an extended release, controlled onset formulation Approved for systolic heart failure Other indications: hypertension, angina, arrhythmias

43
Atenolol vs. Metoprolol Succinate
Sarafidis P, et al. J Clin Hypertens 2008:10:112-118

All Beta Blockers vs. Other Antihypertensivwes44
Ram CV. Am J Cardiol 2010;106:1819-25

Beta Blockers Other Than Atenolol vs Other Antihypertensives
45
Ram CV. Am J Cardiol 2010;106:1819-25

Atenolol vs Other Antihypertensives46
Ram CV. Am J Cardiol 2010;106:1819-25

Speculations on JNC VIII47
Diuretics will remain first line therapy Chlorthalidone vs. HCTZ
Beta blockers will be dropped to 2nd or 3rd line therapy Action may be based on incorrect assumptions about dosing of beta
blockers (atenolol)Combination RAAS inhibition may carry more risk than
benefit and will probably not be recommended (some exceptions)
Aldosterone antagonism will continue to be overlookedStrong emphasis on combination therapy