Embed Size (px)
Citation preview

Journal of the International Society of Head and Neck Trauma (ISHANT)
Updated review
Clearing Cervical Spine Injury in the Unconscious or Obtunded Adult
Lothaire Gérard
Imperial Medical school, London, UK
Received July 2017. Accepted following peer review November 2017. Published December 2017
JISHANT 2017:5
Introduction
Approximately 500–600 people sustain traumatic spine injuries each year in the UK 1. 55% of all spinal fractures occur in the cervical region 2.
“Clearing” the cervical spine involves the exclusion of injuries to both the bones and soft tissues of the neck (C1 to T1). In many patients, this is possible following careful clinical examination. However, in unconscious or obtunded patients, clearing the C-spine by clinical examination alone is not possible and imaging is required.
As prolonged use of collars is known to cause complications, C-spine clearance should therefore be an
immediate priority in all trauma patients3.
When assessing the C-spine, it should be noted that around 10% of patients with a C-spine fracture have other, noncontiguous vertebral fractures2. Therefore, the entire spine should always be investigated. If one fracture is identified a careful look for a second fracture is mandatory.
WHAT GUIDANCE CURRENTLY EXISTS?
The Canadian C-spine rule 4 and the NEXUS criteria 5 are the most commonly used methods of clearing C-spine injuries, but neither of these detail how to clear the C-spine in obtunded or

Journal of the International Society of Head and Neck Trauma (ISHANT)
unconscious patients. However, there are many other good resources providing guidance on C-spine clearance in patients with GCS scores <13. Some of the most comprehensive ones include:
i) Vienna C-spine protocol for critically injured patients (VCS) 6
ii) Alfred Spinal Clearance Management Protocol 7
iii) National Institute for Health and Clinical Excellence (NICE) Clinical Guideline 176 8
iv) Diagnostic Imaging Pathways Group (DIP) - Cervical Spine Injury Guidance9
v) Eastern Association for the Surgery of Trauma (EAST) Management Guidelines for Identification of Cervical Spine Injuries Following Trauma 10
Others exist (Click to see table)
HOW DO THESE GUIDELINES DIFFER?
The majority of guidelines agree that CT is the best choice in assessment for C-spine injury in obtunded or comatose patients and that MRI can be used as a supplementary assessment if available. Some older guidelines suggest that 3-view cervical “trauma series” should be used first 6, 11, but more recent guidelines do not include this assessment, as it has
been shown that they provide no additional information than that derived from CT 10, 12. Concerns have been raised over radiation exposure in CT scans compared to plain films. However, levels of exposure in CT of the head or C-spine are far less than with CT scans of the abdomen 13.
Research suggests that there is no evidence that MRI should be used as a stand-alone assessment 14. This is well known to visualise bone poorly. There are still questions as to the risk/benefit ratio of MRI if CT is normal 10 and it has been suggested that MRI is unnecessary if cervical CT and motor function assessment are both normal 15-17. Nevertheless, MRI can identify ‘soft tissue’ injuries otherwise missed on CT and may enable any subsequent imaging to be targeted at areas of soft tissue injury which accompany fractures14.
SCOPE OF THIS GUIDANCE
This summary guidance applies to patients who:
1. Have a GCS of ≤13
2. Are 16 years of age or older
It does not apply to patients who:
1. Have sustained penetrating neck injuries

Journal of the International Society of Head and Neck Trauma (ISHANT)
SUMMARY OF GUIDANCE
1. C-spine injury should be suspected in all patients presenting with an altered level of consciousness following blunt trauma (especially above the clavicle). These patients need to have their C-spine cleared and should have their neck immobilised with a collar until this can be done 2.
2. Patients with a suspected C-spine injury and a GCS of ≤13 should have an urgent multidetector computed tomography (MDCT) or Helical CT scan of the C-spine (slices less than 2mm), with sagittal and coronal reconstructions, to assess for vertebral fractures 13,18,19. If a fracture is detected at this stage, proceed to step 5.
3. If no vertebral fractures are detected on CT imaging, clinical assessment of the patient’s motor function should be performed15-17. This should include assessment of the following20:
i) motor response
ii) muscle tone
iii) deep tendon reflexes
iv) plantar reflexes
If no abnormalities in motor function are detected, proceed to step 6.
4. If motor function is abnormal on clinical examination, the patient should undergo an MRI scan of the C-spine, to rule out potential injury to soft tissues (ligaments, disc interspaces, and facet capsules)15-17. If no injuries are detected at this stage, proceed to step 6.
5. If an injury to the C-spine is detected on either CT or MRI imaging, spinal immobilisation should be continued, the on-call spinal surgeons should be contacted and definitive management should be initiated 7,21,22.
6. If CT imaging reveal no injuries and either assessment of motor function or MRI reveal no abnormalities, the risk of missing a C-spine injury is deemed to be less than the risk of complications due to prolonged spinal immobilisation. The C-spine can therefore be cleared and C-spine immobilisation discontinued. This decision should be made with the support of a consultant and following clearance of the entire spine 7, 23.
7. The absence of a C-spine injury does not rule out injuries to the thoracic, lumbar or sacral spine. Therefore, caution should still be exercised and steps should be taken to rule out other spinal injuries 2, 24.
A NOTE ON DIFFERENT IMAGING MODALITIES
CT: Current literature points to CT being the best imaging modality to

Journal of the International Society of Head and Neck Trauma (ISHANT)
assess for the presence of C-spine injury in obtunded or unconscious patients. MDCT or Helical CT scans with sagittal and coronal reconstructions slices up to 2mm from C1 to T1, should be used 13,18,19. CT should be performed within one hour of identification of risk factors and reported within one hour of the scan8. This is now a key performance indicator in many trauma centres.
Radiographs: Single lateral plain radiographs are now widely recognised as being inadequate21. Whilst three-view cervical ‘trauma series’ show increased sensitivity compared to the single lateral view, these are no longer regarded as adequate in facilities where CT is available13. If used, three-view plain radiographs should be supplemented by CT to define suspicious or poorly visualised areas11.
MRI: There is consensus that MRI of the C-spine is not a good stand- alone investigation, but should be used to complement CT. This can identify ‘soft tissue’ injuries to supportive ligaments, disc interspaces, and facet capsules14. However MRI can be difficult to undertake in intensive care patients25.
Dynamic Fluoroscopy: Fluoroscopy is a safe test but has not been shown to have any diagnostic advantage over CT19. This test is often difficult in obtunded or comatose patients and may miss instability of the lower C-spine and
therefore should not be used in these patients10, 26.
All imaging should be assessed and reported on by an experienced radiologist so as not to miss any subtle signs21.
Learning points
1 Clearing the cervical spine in obtunded or comatose patients following blunt trauma is not possible with clinical examination alone and requires imaging.
2 Current guidelines still differ in their recommendations of the best imaging techniques. If unsure, always follow your agreed local protocol.
3 C-spine injury should be assumed until the C-spine is adequately cleared.
4 Injuries to other parts of the spine may be present even in the absence of C-spine injuries and should therefore always be investigated.
Abbreviations
C-spine: cervical spine
GCS: Glasgow coma scale score
MDCT: multi-detector computed tomography
CT: computed tomography

Journal of the International Society of Head and Neck Trauma (ISHANT)
MRI: magnetic resonance imaging
NICE: National Institute for Health and Care Excellence
EAST: Eastern Association for the Surgery of Trauma
References
1. National Institute for Health and Care Excellence. Assessment for spinal injury in major trauma - final scope. [Online] 2012 [Accessed: 10th June 2017]. Available from: https://www.nice.org.uk/ [Accessed: 10th June 2017]
2. American College of Surgeons. Advanced Trauma Life Support ATLS. (9). Available from: http://www.44c.in.ua/files/book11.pdf
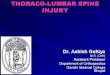
Clearing the cervical spine in an obtunded or comatose patient
- Continue C-Spine immobilisation
- Contact spine surgeon
- Initiate definitive management
Abnormal
Abnormal
- Clear C-Spine - Collar may be removed
(decision should be made with support of a consultant)
Normal
MRI (if available)
Abnormal
Asses gross motor function
C-Spine MDCT or Helical CT with sagittal + coronal reconstructions
Immobilisation with collar
Normal
Normal
Clearing Cervical Spine Injury in the Unconscious or Obtunded Adult

Journal of the International Society of Head and Neck Trauma (ISHANT)
3. Morris CG, McCoy EP, Lavery GG. Spinal immobilisation for unconscious patients with multiple injuries. Annals of Internal Medicine. [Online] 2001;322(7464): 780–782. Available from: doi:10.1136/bmj.a2718
4. Stiell IG, Wells GA, Vandemheen KL, Vandemheen KL, Reardon M. The Canadian C-Spine Rule for Radiography in Alert and Stable Trauma Patients. Journal of the American Medical Association. [Online] 2001;286(15): 1841–1848. Available from: doi:10.1001/jama.286.15.1841
5. Hoffman JR, Mower WR, Wolfson AB, Todd KH, Zucker MI, National X-Radiography Utilization Study Group. Validity of a Set of Clinical Criteria to Rule Out Injury to the Cervical Spine in Patients with Blunt Trauma. The New England Journal of Medicine. [Online] 2000;343: 94–99. Available from: doi:10.1056/NEJM200007133430203
6. Platzer P, Jaindl M, Thalhammer G, Dittrich S, Wieland T, Vecsei V, et al. Clearing the cervical spine in critically injured patients: A comprehensive C-spine protocol to avoid unnecessary delays in diagnosis. European Spine Journal. [Online] 2006;15(12): 1801–1810. Available from: doi:10.1007/s00586-006-0084-1
7. http://www.alfredicu.org.au/assets/Documents/Services-Docs/Trauma-Docs/Spinal-Clearance-Management-Protocol-Jun06-A.pdf
8. National Institute for Health and Clinical Excellence. NICE Guidelines CT head and Spine Imaging. 2014; 1–4. Available from: https://www.nice.org.uk/guidance/cg176/resources/imaging-algorithm-498950893
9. Department of Health Western Australia - Diagnostic Imaging Pathways. Cervical Spine Injury. [Online] Available from: http://www.imagingpathways.health.wa.gov.au/index.php/imaging-pathways/musculoskeletal-trauma/bone-and-joint-trauma/cervical-spine-injury
10. Como JJ, Diaz JJ, Dunham CM, Chiu WC, Duane TM, Capella JM, et al. Practice management guidelines for identification of cervical spine injuries following trauma: update from the eastern association for the surgery of trauma practice management guidelines committee. The Journal of trauma. [Online] 2009;67(3): 651–659. Available from: doi:10.1097/TA.0b013e3181ae583b
11. Hadley MN, Walters BC, Grabb PA, Oyesiku NM, Przybylski GJ, Resnick DK, et al. Guidelines for the management of acute cervical spine and spinal cord injuries.

Journal of the International Society of Head and Neck Trauma (ISHANT)
Clinical neurosurgery. [Online] 2002;49: 407–498. Available from: http://www.aans.org/Education and Meetings/~/media/Files/Education and Meetingf/Clinical Guidelines/TraumaGuidelines.ashx
12. Padayachee L, Cooper DJ, Irons S, Ackland HM, Thomson K, Rosenfeld J, et al. Cervical spine clearance in unconscious traumatic brain injury patients: dynamic flexion-extension fluoroscopy versus computed tomography with three-dimensional reconstruction. Journal of Trauma Injury Infection And Critical Care. [Online] 2006;60(2): 341–345. Available from: doi:10.1097/01.ta.0000195716.73126.12
13. Morris CGT, McCoy É. Clearing the cervical spine in unconscious polytrauma victims, balancing risks and effective screening. Anaesthesia. [Online] 2004;59(5): 464–482. Available from: doi:10.1111/j.1365-2044.2004.03666.x
14. D’Alise MD, Benzel EC, Hart BL. Magnetic resonance imaging evaluation of the cervical spine in the comatose or obtunded trauma patient. Journal of Neurosurgery: Spine. [Online] 1999;91(1): 54–59. Available from: doi:10.3171/spi.1999.91.1.0054
15. James IAO, Moukalled A, Yu E, Tulman DB, Bergese SD, Jones CD, et al. A systematic review of the need for MRI for the clearance of cervical spine injury in obtunded blunt trauma patients after normal cervical spine CT. Journal of Emergencies, Trauma, and Shock. [Online] 2014;7(4): 251–255. Available from: doi:10.4103/0974-2700.142611
16. Steigelman M, Lopez P, Dent D, Myers J, Corneille M, Stewart R, et al. Screening cervical spine MRI after normal cervical spine CT scans in patients in whom cervical spine injury cannot be excluded by physical examination. American Journal of Surgery. [Online] Elsevier Inc.; 2008;196(6): 857–863. Available from: doi:10.1016/j.amjsurg.2008.07.040
17. Schuster R, Waxman K, Sanchez B, Becerra S, Chung R, Conner S, et al. Magnetic resonance imaging is not needed to clear cervical spines in blunt trauma patients with normal computed tomographic results and no motor deficits. The Journal of the American Medical Association. [Online] 2005;140(8): 762–766. Available from: doi:140/8/762 [pii]\r10.1001/archsurg.140.8.762
18. Khanna P, Chau C, Dublin A, Kim K, Wisner D. The Value of Cervical Magnetic Resonance Imaging in the Evaluation of the Obtunded or Comatose Patient With Cervical Trauma, No Other Abnormal Neurological Findings, and a Normal

Journal of the International Society of Head and Neck Trauma (ISHANT)
Cervical Computed Tomography. The Journal of Trauma: Injury, Infection, and Critical Care. [Online] 2011;72(3): 1. Available from: doi:10.1097/TA.0b013e31822b77f9
19. Spiteri V, Kotnis R, Singh P, Elzein R, Madhu R, Brooks A, et al. Cervical dynamic screening in spinal clearance: now redundant. The Journal of Trauma: Injury, Infection, and Critical Care. [Online] 2006;61(5): 1171–7; discussion 1177. Available from: doi:10.1097/01.ta.0000236000.95954.9a
20. Bateman DE. Neurological Assessement of Coma. Journal of Neurology, Neurosurgery and Psychiatry. [Online] 2001;71(suppl 1): i13–i17. Available from: doi:http://dx.doi.org/10.1136/jnnp.71.suppl_1.i13
21. Harrison PMB, Cairns CMB. Clearing the cervical spine in the unconscious patient. Continuing Education in Anaesthesia, Critical Care and Pain. [Online] 2008;8(4): 117–120. Available from: doi:10.1093/bjaceaccp/mkn022
22. Anderson P a, Lindsey RW, Schoenfeld AJ, Harris MB, Guagala Z. Clearing the Cervical Spine in the Blunt Trauma Patient. The Journal of the American Academy of Orthopaedic Surgeons. [Online] 2010;18(3): 149–159. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20190105
23. Raza M, Elkhodair S, Zaheer A, Yousaf S. Safe cervical spine clearance in adult obtunded blunt trauma patients on the basis of a normal multidetector CT scan - A meta-analysis and cohort study. Injury. [Online] Elsevier Ltd; 2013;44(11): 1589–1595. Available from: doi:10.1016/j.injury.2013.06.005
24. Berne JD, Velmahos GC, El-Tawil Q, Demetriades D, Asensio JA, Murray JA, et al. Value of Complete Cervical Helical Computed Tomographic Scanning in Identifying Cervical Spine Injury in the Unevaluable Blunt Trauma Patient with Multiple Injuries: A Prospective Study. The Journal of Trauma: Injury, Infection, and Critical Care. [Online] 1999;47(5): 896. Available from: http://ovidsp.tx.ovid.com/sp-3.25.0a/ovidweb.cgi?QS2=434f4e1a73d37e8c6a240dd2f6a7d9edc8d488370a9e9608fd77dc9f49e0900f86dbeb78fd08806c8d4b177b2d8358ab61834095e760b8972884b6a6d6a62a0a197f76034129a90e07c7a246b1b2b75a22c4d4e3ba000c25ac6656faf6342dbcea3210866f
25. British Association of Spinal Surgeons, Society of British Neurologial Surgeons. British Orthopaedic Associtation Inclusions : BOAST 2 : Spinal Clearance

Journal of the International Society of Head and Neck Trauma (ISHANT)
In The Trauma Patient Standards for Practice Audit : 2015;(March): 43. Available from: https://www.boa.ac.uk/wp-content/uploads/2015/03/BOAST-2-March-2015.pdf
26. Bolinger B, Shartz M, Marion D. Bedside fluoroscopic flexion and extension cervical spine radiographs for clearance of the cervical spine in comatose trauma patients. The Journal of trauma. [Online] 2004;56(1): 132–136. Available from: doi:10.1097/01.TA.0000044629.69247.0A
Accepted November 2017
Comments? - go to Forums to discuss this and any other topics of interest