Upload
hacong
View
217
Download
0
Embed Size (px)
Citation preview
JFA Purple Orange - ACT Office of the Senior Practitioner - Interim Report March 2017
Minimising and Eliminating Restrictive Practices.
A Consultation for the ACT Government
Acknowledgment
We gratefully acknowledge the assistance of the following persons who contributed ideas and perspectives as part of a co-design process for the development of this report.
Christina Ryan, CEO, Advocacy For Inclusion Fiona May, Chief Executive Officer, ADACAS Jan Kruger, Director, Imagine More
Robert Altomare, Executive Officer, PWD ACT Steve Fox, Manager, NDS in ACT
Simon Viereck, Executive Officer, Mental Health Community Coalition ACT Purity Goj, Program Manager, Mental Health Consumer Network ACT Charlie Richardson, Mental Health Community Coalition ACT
Richard Bruggemann, Senior Practitioner, Disability SA Sue Salthouse, WWDACT
Susan Helyar, Director, ACTCOSS
Agency details
JFA Purple Orange 104 Greenhill Road
Unley SA 5061 AUSTRALIA
Telephone: + 61 (8) 8373 8333
Fax: + 61 (8) 8373 8373
Email: [email protected] Website: www.purpleorange.org.au
Facebook: www.facebook.com/jfapurpleorange
JFA Purple Orange is a non-government, social profit organisation. Anchored on dialogue with people living with disability, their families, service providers, government and other stakeholders, we seek to identify policy and practice that has the prospect of advancing peoples chances of a good life. Our work is anchored on the principles of Personhood and Citizenhood. Our work includes research, evaluation, capacity building, consultancy, and hosted initiatives.
ISBN: 978-0-9804509-4-1March 2017.
Contents
Background and Summary4The structure of this report9Evaluation of data: findings from Phase 2 consultations9Main themes: What are the biggest issues and concerns relating to restrictive practices in the ACT and the establishment of an Office of the Senior Practitioner?9A lack of awareness and consistency of what constitutes restrictive practices10The use of restrictive practices in Mental Health settings across the ACT11A lack of capacity within the sector for managing behaviour and its etiology12The need for leadership that drives a strategy and culture change regarding restrictive practices across the sector13A lack of current reporting of the use of restrictive practices and any associated long- term data15Differing opinions regarding the use of restrictive practices16Possible solutions to minimising and eliminating restrictive practices in the ACT17A strategy around training and awareness-raising around restrictive practices17A focus on training and awareness-raising strategies within educational institutes ... 18A capacity-building model to increase knowledge and skills across the sector regarding the use of restrictive practices19Considerations for training and capacity-building21Design Features and Recommendations for an ACT Office of the Senior Practitioner22Considerations in establishing an Office of the Senior Practitioner for the ACT25Conclusion26Appendix 1: Copy of online survey questions28
1. Background and Summary
The purpose of this paper is to report on a community consultation that is being led by JFA Purple Orange on how an Office of the Senior Practitioner might operate in the ACT. A discussion paper released in January 2017 gives an overview of what is meant by restrictive practices, the extent to which such practices are an issue in the ACT, and how these issues might be addressed through an Office of the Senior Practitioner.
From late January to early March 2017, a range of opportunities were offered for people to give their views about this topic. This report provides an overview of the findings, opinions and recommendations that have emerged through Phase 2 consultations. This report also provides a set of possible features and components that could be considered should adoption and design of an Office of the Senior Practitioner be undertaken by the ACT government.
For the purpose of this project the definition of restrictive practices offered by the Government of South Australia has been utilised:
Restrictive practices refer to any practice, device or action that removes or restricts another persons freedom, movement or ability to make a decision. This includes detention, seclusion, exclusion, aversive restraint, chemical restraint, physical restraint, mechanical restraint, environmental restraint and psycho-social restraint. Restrictive practices do not include therapeutic or safety devices/practices, where the device or practice is being used for its intended purpose and the person is not resisting or objecting to its use.[footnoteRef:1] [1: SA Government DCSI Safeguarding People with Disability Overarching Policy DIS/366 POL-SER-002-2013]
Restrictions can include (but are not necessarily limited to):
mechanical, such as devices that limit a persons movements (and this includes the removal and/ or disengagement of mechanical supports that assist the persons movements)
seclusion, such as the sole confinement of a person at any time in any room where the doors and windows cannot be opened by that person
environmental, such as preventing free access to all parts of a persons environment or house (for example locking the refrigerators)
social, such as the imposition of sanctions that restrict the persons access to relationships/opportunities they value
chemical, such as medications that blunt the persons emotions, cognition, and motor activity
physical, such as holding or pinning down by another person
psycho-social restraints, such as power control strategies[footnoteRef:2] which might include threats, intimidation, fear, coercion, discipline, or retaliation [2: Power-control strategies are defined in South Australias Safeguarding People with Disability Restrictive Practices Policy as the use of power-control strategies to influence a persons behaviour. This includes but is not limited to directing the persons behaviour through voice tone, commands or threats and the use of punishment, including ignoring the person and withholding basic human rights, such as positive social interaction, personal belongings or a favoured activity.]
organisational, such as excluding the person from activities, and restrictions to the person's choice
communication restraint, such as switching off someones communication device
decision making restraint, such as failing to provide options for supported decision making
While taking action to avert a clear and present risk of harm is understandable, there are a number of problems with the imposition of restrictive practices. These include (but are not necessarily limited to):
the negative consequences the restrictive practice by its nature can have on the persons progress towards good life chances, their general well-being, physically and psychologically including the impact on self-esteem
restrictive practices that are focused on behaviour suppression as opposed to supporting genuine positive behaviour change
restrictive practices that are focused on a negative reinforcement paradigm (the use of punishment to extinguish an unwanted behaviour, as opposed to positive reinforcement paradigms that focus on rewarding the emergence of behaviour choices that can advance the persons life chances)
restrictive practices that are inadequate in terms of their conceptualisation and implementation
restrictive practices that are inadequate in terms of a clearly defined timeframe and process for review
restrictive practices that constitute an assault on the persons human rights
restrictive practices that are crafted and/or executed by staff with inadequate skills and perspective.
It is recognised that the use of restrictive practices may not always be intentional but that actions taken, or not taken, inadvertently have the effect of restricting a persons preferences and actions, and/or contravening their rights. The person using the restrictive practice may argue that there is no malicious intent and that it is just the way that things are done. However, this is not an adequate defence for the continuation of such practices.
A targeted set of questions was formed for use in Phase 2 of this consultation project, alongside a similar set of questions that formed an online survey. Some consultations used all of these questions whereas others were of a workshop format and asked participants to identify issues related to the use of restrictive practices across the ACT sector and to brainstorm possible solutions to these issues. Appendix 1 provides a copy of the survey questions whilst Box 1 outlines examples of the questions used in telephone and face-to-face consultations which occurred between January and March 2017.
Consultation questions: face-to-face and telephone consultations
1. Do you think the ACT Government should set up an Office of the Senior Practitioner to help ensure that restrictive practices are kept to a minimum, and ideally eliminated, in the ACT?
Who could run this?
2. Do you think it would be a good idea for there to be a register of every person who is being subjected to restrictive practices?
How could that register work, including reporting?
Who could run the register?
3. What should be the priorities in a strategy to raise awareness of the problems of restrictive practices?
Do you think an ACT OSP could do this or do you think there is some other ACT or national agency that could do this?
4. How might an ACT OSP build capacity for best practice within the health, education and community services sectors, so that more staff know how to provide alternatives to restrictive practices?
5. Which other ACT and national laws, regulations and frameworks do you think an ACT OSP needs to link to (to avoid duplication, gaps, etc.), and how do you think this should happen?
How might an ACT OSP link in for example with care and protection legislation and services, official visitor schemes, human rights legislation and complaints, ACAT treatment orders etc.?
Box 1: Questions used in face-to-face and telephone consultations
More than 70 participants took part in these consultations. Face-to-face consultations were held across multiple venues in Canberra. In addition, other forms of participation included 1:1 phone consultations, individual or organizational submissions and completion of an online survey.
See Figure 1 for a visual representation of the different styles of participation recorded in this consultation.
7%
Face-to-face consultations
20%
56%
17%
Individual 1:1
consultations
Online survey participation
Individual or organisational submission
Figure 1: Forms of participation
A series of public and agency-supported consultations were held across February and March 2017 in Canberra. Concurrently, individual consultations, online survey and individual or organisational submissions were offered as additional forms of participation. Table 1 shows the venues and locations of in-person consultations held for this project in Canberra throughout February and March 2017.
Locations and venues of consultations
National Disability Services, ACT
Belconnen, ACT: public consultation
ACT Mental Health Consumer Network
Civic, ACT: public consultation
Mental Health Community Coalition ACT
ACT Council of Social Services
Women With Disability ACT
People With Disabilities ACT
Imagine More, ACT
ACT Disability, Aged and Carer Advocacy Service (ADACAS)
Examples of stakeholder groups represented within consultations
Staff involved in prison and justice systems
Mental health consumers
Disability service providers including frontline workers and senior managers
Staff involved in disability advocacy and support roles
ACT government health workers
Staff involved in human rights issues
Allied health workers
Staff related to interstate Office of the Senior Practitioner units
Consumers including family members, parents, both men and women living with disability
Staff involved in aged care provision
Staff involved in education sector
Staff involved in mental health sector
Table 2: Overview of stakeholder groups represented via consultations
1.1.The structure of this report
This report serves as an interim report following the Phase 2 consultation process and a thorough data analysis. We have focussed in this report on using content gained from consultations to inform the possible role of an Office of the Senior Practitioner within the ACT. Therefore, the themes and recommendations presented here address the main conceptual elements relating to this focus. We plan to add detailed operational considerations of establishing an oversight body for minimising and eliminating restrictive practices in the ACT in our final Phase 3 report in June 2017.
However, it is acknowledged that there is of course interaction between content-related reporting (the main conceptual elements focussed upon in this report) and process- based discussion (the detailed operational considerations to be focussed upon in the Phase 3 report). Where necessary, we have provided signals within our reporting of the describing the issues and opinions gained from Phase 2 consultations of any operational considerations that are necessary for reflection.
2. Evaluation of data: findings from Phase 2 consultations
Following the consultations, data was analysed using thematic analysis to achieve a coded list of emerging themes. These findings are outlined below and comprise the major issues and concerns related to the use of restrictive practices across the ACT, possible solutions to these issues and the possible role and function of an ACT-based Office of the Senior Practitioner or similar oversight body.
For the majority of participants, there was solid support for an Office of the Senior Practitioner or similar oversight body to be established within the ACT. However, a minority of participants were reluctant to support an Office of the Senior Practitioner in the ACT without knowing what this is or how it would work. Some participants were also unhappy that they didnt know whether Office of the Senior Practitioner models in other states have been successful in minimising and eliminating the use of restrictive practices.
The majority of participants were able to understand that the issue of restrictive practices involves complex factors including at-risk physical and social environments and long-established habitual practices. Whilst there was evident caution from some participants in supporting the establishment of a formal body, especially if it sits within a government directorate, the majority were happy to voice their views on how such an Office or body could be established and the roles, functions and responsibilities that should be attached. For the purposes of this report, the findings are presented and discussed in regards to a future Office of the Senior Practitioner for the ACT, with the knowledge that some hesitance for this type of body has been duly noted in this section of the report.
2.1. Main themes: What are the biggest issues and concerns relating to restrictive practices in the ACT and the establishment of an Office of the Senior Practitioner?
The main themes that emerged from data analysis are detailed in the below section of this report. Table 3 provides a summary of the themes.
Main themes relating to restrictive practices in the Act and the establishment of an Office of the Senior Practitioner
Theme 1
A lack of awareness and consistency of what constitutes restrictive practices
Theme 2
Use of restrictive practices within mental health settings
Theme 3
A lack of capacity within the sector for managing behaviour and its etiology
Theme 4
The need for leadership that drives a strategy and culture change regarding restrictive practices across the sector
Theme 5
An issue with current reporting of the use of restrictive practices and a lack of long-term data
Theme 6
Differing opinions regarding the use of restrictive practices
Table 3: Main themes from data analysis of Phase 2 Consultations
2.1.1. A lack of awareness and consistency of what constitutes restrictive practices
Participants reported a lack of awareness around restrictive practices and a lack of understanding within the sector on what the term means. This has led to a gap in the definition around restrictive practices and what is occurring on the frontline. Multiple examples have been provided whereby restrictive practices are occurring across various settings, including educational, residential, domestic, clinical, community and public settings. Our consultations have highlighted that there is too strong an emphasis currently in the ACT on physical protective practices and a lack of specific training to guide service providers and/or staff to consider the etiologic cause of behaviours (e.g. to ask themselves why is this behaviour occurring?).
The viewpoint established in the earlier discussion paper in January 2017 endorses the notion that restrictive practices should only be used where they are proportionate and justified in order to protect the rights or safety of the person or others.[footnoteRef:3] It is important to recognize that, within Phase 2 consultations, participants highlighted examples of restrictive practices that are practices intended to avoid harm. It is acknowledged that at times an individual is the recipient of restrictive practices for reasons of safety. However, it has been reported during consultations that practices are often used in the name of safety with many examples falling into this category (e.g. locked doors, no access to kitchen at certain times of day and seatbelt guards), where such practices are being carried out without the person undertaking that practice being aware of the practice being restrictive. [3: Overview of restrictive practices, and the key issues for consideration in relation to the establishment of an Office of the Senior Practitioner. Public discussion paper, JFA Purple Orange, January 2017]
Likewise, disability, community and social services providers have reported that they often see restrictive practices being used by family members; often this is because the family members involved do not know a better way to manage peoples behaviour. The classic statement of people dont know what they dont know has been raised several times during these consultations.
As many restrictive practices are occurring but not being recognised as restrictive practices, this suggests there are not adequate training packages or guidelines to assist people to practice any differently. For example, a service provider who attended a consultation readily acknowledged that many staff are engaging in restrictive practices without having any awareness of this.
Similarly, some providers raised concerns in consultations about the role of guardians in relation to restrictive practices; that guardians might be operating beyond the boundaries of the formal guardianship role. It was acknowledged that when someone is appointed guardian, their practice might be influenced by what they perceive the persons best interests are as opposed to what they know about what the person actually wants. It was suggested that often people make decisions based on their own anxieties rather than honouring the best interests of the individual involved.
This signals that there may be a need to provide guardians with support for their role so their involvement in methodologies such as Supported Decision Making and their capacity to understand possible alternatives to restrictive pract
The concerns highlighted here suggest that there is a significant need across the ACT for a targeted training and awareness-raising strategy to be implemented, which can help to guide people to consider the reasons for behaviour, inclusive of environmental and contextual factors. Any work around this issue needs to include a focus on alternative practices and be oriented to person- centred principles, the personal safety of all involved and the use of less restrictive alternatives.
2.1.2. The use of restrictive practices in Mental Health settings across the ACT Two consultations were hosted by mental health specific agencies, with several mental health consumers attending one of these sessions. The most significant issue for this group of individuals is
the need for a cultural shift in the ACT and a move to a different viewpoint of restrictive practices. While it is recognized that the new Mental Health Act has allowed for more decisions to be made by a consumer, it was felt that there is still a lot of development and reform to be done in this area. A key question asked by a participant during this consultation was Consumer voices are being heard more but it is still not enough. We question if the new Mental Health Act will lead to a change in practice or will it just be a legislative change without any real on the ground changes?
These consultations, with involvement from staff working in mental health policy and mental health consumers, offered many examples of restrictive practices within clinical and in-patient hospital settings. It was heard that restrictive practices become the normal practice for many mental health consumers, particularly those who may have had several stays in hospital following a mental health crisis or an acute episode. Unfortunately, it has been the experience of those in attendance that hospital and clinical staff often do not allow for cathartic behaviour that is considered therapeutic by many mental health consumers. The examples put forward in relation to this include:
1. crying/shrieking/screaming
2. emotional outbursts
3. banging on to the wall in frustration
4. burying head in pillow
5. hiding under clothes/sheets/cupboards/bed to hide/have personal space
6. putting hands over eyes to try and make oneself feel calmer)
7. art therapy techniques such as drawing frantically/filling a page with coloured ink
8. Singing/chanting/rocking/swaying
All of these practices are often seen as challenging behaviours by medical or clinical staff. At times, punitive measures are used by staff in hospitals to fix the problem as this is how these behaviours are construed. For the mental health consumers contributing to this consultation, the advantages and therapeutic benefits of the above behaviours are not well understood, nor recognized as anything but challenging behaviours by clinical and other hospital staff.
This speaks to a significant need for greater input from peer support workers in service settings. Peer support workers can offer valuable insights to both patients/clients/individuals as well as staff.
It is easily recognized that hospitals are time-poor environments with reliance upon continually changing shift workers. Unfortunately, the viewpoint of many mental health consumers present at consultations is that the use of restrictive practices in hospital settings is a by-product of a tension between effective support and limited time. The belief of many was that it is time efficient for hospitals and institutions to practice restrictive interventions rather than to develop a model which sees additional time and focus given to evaluation of each case situation with an emphasis on positive support. One consumer stated As it stands at the moment, the majority of inpatient care for mental health patients is not therapeutic care, it is simply risk management. For this person, restrictive practices are embedded in current hospital systems because these practices adequately and efficiently remove the risk in many cases.
2.1.3. A lack of capacity within the sector for managing behaviour and its etiology It is important to note that behaviours of concern often stem from issues surrounding an individuals choices and therefore are not necessarily requiring coordinated plans such as a behaviour support
plan. For instance, we recognize that if a persons choices are not being honoured then this situation would not be best responded to by an Office of the Senior Practitioner but rather by a service that matches the needs and desires of the individual. However, the issue of an under-developed capacity across the ACT sector to identify, manage and respond to restrictive practices and interventions has been readily acknowledged in consultations with stakeholder groups. This suggests a clear need for significant capacity building to take place, with the possibility of an ACT Office of the Senior Practitioner taking the lead in strategising support for this across the sector.
For some contributors, there are challenges around key information not reaching appropriate service providers. Examples were given where information was not arriving to the people it needed to reach, such as relevant issues not being handed over to school staff. This raised a further concern around how people and their support needs are documented, with opinion raised that there was a
need to grow capacity for stronger documentation and communication within this sector. Examples given included staff not having access to specific behavioural and background information.
The consultation revealed a view that there needs to be resource capacity in schools for coping with behaviours in the moment, to deal with and respond to incidents. At this stage it is believed that not all organisations within the ACT sector are equipped with specific information on restrictive practices. This suggests a need for a readymade policy and practice toolkit or a similar resource that staff could be furnished with to guide their response. It was recognised that it is important to find the balance between dignity (e.g. respect and honour of a persons individual desires and freedoms) with risk and duty of care. A toolkit or similar resource could go some way with assisting with this. Such a resource by nature could also assist with raising awareness about the reality of restrictive practices.
Similarly, the issue of a need to build capacity in mainstream space also emerged through consultations. In one consultation, there was a key recommendation for there to be a graduated introduction between a school and students. In this way, families, children and the school could all be encouraged to get to know one another underneath a model that fosters recognition of positive behaviour support and behaviour etiology.
Furthermore, capacity-building was identified as being required within prison settings and service provision for people intersecting with justice systems. A concern around a lack of information about the pathway of people who end up in prison systems was raised. Potentially, there might be a role for an ACT Office of the Senior Practitioner to intervene upstream and make significant changes in this space.
Similarly, there was concern about practices carried out within prison systems to safeguard against restrictive interventions. For example, on release from prison, there is concern that people are often released with a reputation and few supports solidly in place for them. There is a need for capacity building within prison systems to make sure that people do not fall through the gaps. In particular, there is a need for building capacity within prisons to support positive networks for incarcerated persons. This speaks to a possible role for an ACT Office of the Senior Practitioner around the quality of release planning for individuals from prison systems.
2.1.4. The need for leadership that drives a strategy and culture change regarding restrictive practices across the sector
It was clear following consultations that there is a perceived need for a strategy leader within the ACT to drive change around restrictive practices. Within consultations, it could be seen that people are aware of the need for a cultural change across the sector regarding the ways in which restrictive practices are viewed. For instance, examples provided made it clear that often in places or settings where restrictive practices are seen to be occurring there are a variety of factors that can influence staff behaviour or responses to situations. These factors include:
1. Poor working conditions and low morale among staff in some settings
2. Culture within workplaces -currently there is evidence of restrictive practice use that comes through risk aversion.
3. Conflict-driven environment
4. Staff turnover rate
On account of this list, it is critical to consider the surrounding culture of an organisation, service or setting in which restrictive practices may be carried out. Some participants acknowledged that the implementation of the new Mental Health Act offers some improvements to the issue of restrictive practices as the Act opens up the ability for greater dialogue between clinicians to speak to family members. However, across the sector there was a view that an Office of the Senior Practitioner (or similar oversight body) could act as a leader to drive strategy and change. Participants spoke of a current culture of risk management and risk aversion in relation to the use of restrictive practices and the need for a focus on behavioural management and understanding across the sector.
Examples were given in line with this of challenging behaviours being met by staff across settings who are operating within a culture of risk management. Such a culture therefore does not focus on identifying the cause of behaviour nor is it oriented towards ways to change future behaviours.
Discussion of the impact of culture continued as issues of capacity building around restrictive practices were considered. There was concern that simply providing training in the way of a toolkit or package is not enough. Some participants argued that the focus needs to be on a long-term investment on training from an oversight body such as an Office of the Senior Practitioner. It was considered that various support mechanisms needed to be embedded within any training packages offered; such as equipping the workforce with ways of feeling supported to carry out the training.
The following suggestions were offered regarding training support mechanisms:
Access to a fellow worker via a buddy system
Access to an expert in a similar field of work/setting of work
Access to additional everyday support as needed- supervision, debriefing, peer support, refresher training, case examples, and online forums.
Following discussion of this the suggestion of implementing a Communities of Practice model was made. It was felt that a sustainable continuous model to support the type of training needed to minimise and eliminate restrictive practices in the ACT could be offered via a Communities of Practice approach, where collective learning takes place amongst practitioners seeking to develop a shared repertoire of resources: experiences, stories, tools, and ways of addressing recurring problems.[footnoteRef:4] [4: Eckert, P. 2006. Communities of Practice. Encyclopedia of Language and Linguistics, 683-685.]
Furthermore, concerns were raised around larger systemic cultural issues related to the use of restrictive practices within mainstream community and public settings. There was a view that a strategic awareness-raising strategy was required. For example, how can we inform people in the public domain about eliminating restrictive practices? How can we successfully build peoples awareness around this topic? One suggestion offered is to systematically work through public settings (such as shopping centres and community spaces) and speak to staff with some simple information about how they might respond to and potentially diffuse a situation they may witness. This could be achieved with straightforward training materials that provide explanations of many
behaviours as not being intentional and offer some alternative responses to involving authorities or responding with knee-jerk reactions.
Further suggestions included a strategic plan that includes relationship-building with local people (such as frequent members of the community who come in to do their shopping or hang out at the mall). This suggestion is focused on developing context around members of the community so that if certain behaviors occur there is more known background and context to supplement any incident.
This suggestion assists with building a culture across the whole of the ACT whereby people are equipped with awareness, techniques and strategies to respond to behaviours in a different manner to practices that may unfold from a culture of risk management. Similarly, the question was raised of availability of a quiet space at local places such as shopping malls. This is one way to set up a program whereby negotiations are made with management of malls to make a space (e.g. an office or enclosed area) available for those requiring a private space. It is possible that an ACT Office of the Senior Practitioner could become a strategy leader for training in this space and coordinate strategies around this accordingly.
2.1.5. A lack of current reporting of the use of restrictive practices and any associated long-term data
Currently, participants felt that there is a system of underreporting the use of restrictive practices. Many participants saw a need for an Office of the Senior Practitioner with a role that is mandated to require people to report on restrictive practices.
Some suggestions around reporting included a standardised form that could be easily submitted to a central repository. Other suggestions included devising a mechanism whereby people can contact the Office of the Senior Practitioner without providing their details (e.g. anonymous and confidential). It was felt that this added measure would see a better uptake of any reporting process that is implemented. In addition, people felt that an Office of the Senior Practitioner or similar oversight body around the use of restrictive practices should carry out regular spot checks and audits at a variety of settings (e.g. educational institutions, residential care facilities, hospitals, within service provider organisations.)
There was overwhelming support for the implementation of a register to record and report against the use of restrictive practices within the ACT. Provided that personal and sensitive information would be appropriately stored, participants felt that regular reporting based on information captured within a register would be extremely useful for further understanding the scope of the issue and informing capacity building within the sector. It is important to acknowledge that some participants were cautious towards the notion of a register as they felt this could lead to persons being introduced to services by way of reputation (that is, a record within an accessible register may allow a person to be considered by other services as presenting with challenging behaviour or complex problems). Participants felt that it would be necessary for any information within a register to be appropriately protected and that the primary use for a register would be for identifying the use of restrictive practices across the sector and using this data to better understand the scope and circumstances relating to these interventions.
Some comments on this issue of a register were captured from consultations:
Yes, there should be a register of every person where restrictive practices are being used -I like the idea as it makes people (e.g. Service providers, staff) accountable and it formalises the processes relating to the use of restrictive practices- currently it is not formal.
A register provides data to show the story of restrictive practices use in ACT and would let people know what is going on and the different circumstances.
It will make people aware that they are carrying out restrictive practices, which they might not be aware of. This will help lead to more understanding and possible behaviour change from staff around complex behaviour management and type of thing
Currently, as far as we can tell, the State of Victoria is the only jurisdiction in which a register of the use of restrictive practices is maintained. It can be seen from the most current Victorian Senior Practitioner Report that the information held within this register offers very insightful and useful data around restrictive interventions, compulsory treatment and behaviour support plan quality. For example, specific reports have been developed that overview the use of chemical, mechanical, physical restraint and seclusion and more specific reports to inform services of specific sets of data, such as time of day that people have been reported to be restrained or secluded.[footnoteRef:5] Participants could see that regular reports informed by restrictive interventions data would be very useful to organisations across the sector and could assist services to minimise their use of restrictive practices and increase their focus on positive behaviour support strategies. However, we note that the ACT Mental Health Act 2015 requires registers to be kept of seclusion, restraint and forcible giving of medication.[footnoteRef:6] These registers are kept in inpatient facilities, but potentially they could technically apply to other settings as well. If a role of an ACT Office of the Senior Practitioner is to keep a register of restrictive practice it is worth noting this overlap. There could be a potential for a partnership between an Office of the Senior Practitioner register and existing registers such as those mandated by the ACT Mental Health Act. [5: Senior Practitioner Report 2015-2016, Department of Health and Human Services, Victorian State Government] [6: Mental Health Act 2015, Australian Capital Territory Parliamentary Counsel, available at www.legislation.act.gov.au]
In addition, some other ideas were put forward regarding the implementation of a register. For example, in one consultation, participants favoured the idea that a register could be used to house examples of positive interventions as a way of highlighting the benefit and impact of alternative avenues to the use of restrictive practices. A system like this was considered to have the potential to assist in both training and awareness-raising across the sector.
2.1.6. Differing opinions regarding the use of restrictive practices
During the consultations, several contributors provided examples of ways in which they believed the use of restrictive practices could have a positive benefit for an individual. These benefits were described as being over and above any safety-related factors and were considered by contributors as being a therapeutic benefit, such as restrictions that provide comfort and relaxation. These individuals expressed sincere concern that this viewpoint of the use of restrictive practices might not be understood in a rush to regulate the use of restrictive interventions.
For the Phase 3 component of this work we will pay careful regard to the possibility of any therapeutic benefits following the use of restrictive practices. It is possible that people might see therapeutic benefits from interventions in the absence of other avenues being explored. We suggest that the only way to judge the extent of any claimed therapeutic benefit would be to draw comparisons with alternative practices.
2.2. Possible solutions to minimising and eliminating restrictive practices in the ACT
It was recognised by the majority of participants that the sector has low skill in regards to alternatives to restrictive practices with few training or capacity-building opportunities. Several solutions were put forward by participants to minimise and eliminate the use of restrictive practices across the sector. These potential solutions are outlined below:
1. There is a need for a strategy around training and capacity building regarding the use of alternatives to restrictive practices
2. There is a need to skill up the sector about how to get to know individuals within services
3. There is a need for better choice driven planning
4. There is a need to aim for better continuity of staff across services and organisations- a strategy is needed to support service providers be encouraged to support profiles where there is better continuity (that is, less staff per person but more skills in fewer people).
5. There is a need to employ positive behavioural support specialists
2.2.1. A strategy around training and awareness-raising around restrictive practices
The majority of participants spoke of a need for specific training regarding restrictive practices and behaviour support to be developed and made accessible throughout the ACT.
Different needs could be identified across the sector in relation to this training. For example, a representative from a disability service provider stated: there is not a great deal of knowledge in the disability sector in ACT around restrictive practices. no uniform guidelines for organisations to teach staff and no mandatory training is available.
For others, discussion of a need for training followed examples given of the use of restrictive practices for signing off on medication by doctors to chemically restrain individuals following behaviours of concern. Some participants from the disability sector felt that specific training for this situation was much needed, particular alongside a robust awareness-raising strategy that would help to define restrictive practices. In particular, it was felt that there was a need for a solid definition around restrictive practices that would resonate across the sector and be reinforced through training.
The format that such training could take yielded rich discussions within consultations. Many suggestions were received, with consideration given to style and delivery methods. For some participants, they suggested that this type of training be built into existing workforce training or professional development programs. Other people felt that there needed to be a way that
organisations were held accountable for supplying necessary training around alternatives to restrictive practices, with one suggestion being to appoint a staff member with oversight responsibility for this, in a similar vein to Chief Fire Warden training responsibilities. Under this design, participant felt that the onus would then lie with each organisation to complete regulated training and to make the decision of who is appointed. This takes the concept of restrictive practices training further from simply guidelines for best practice and instead to a mandatory and regulated procedure that must be adhered to and accounted for.
Other discussions in relation to this topic focused on training methods and content. Some participants proposed that training be implemented under a human rights framework and designed to allow for access from all staffing levels of an organisation or service. Logistical issues were also discussed with one suggestion of a mobile training team to be established under direction from an Office of the Senior Practitioner. Mobile teams could visit different services and organisations in their own settings and use a train the trainer model in order for capacity to be quickly built up across the sector.
2.2.2. A focus on training and awareness-raising strategies within educational institutes
A large number of examples of restrictive practices used within educational settings were provided throughout this consultation project. It was recognised by some participants that the education sector in ACT has put out a safe and supportive practices guide which states that restrictive practices should only be used within the context of a positive behaviour support approach, and only after all other less restrictive options have been applied, or are not practicable in the circumstances. They must not be used to gain compliance in students.[footnoteRef:7] However, some participants felt that the use of restrictive practices in mainstream schools was in some cases being regularly applied to gain compliance in students and that the focus or context of positive behavioural approaches had been lost. This suggests a need for capacity building at mainstream schools around supporting students with disabilities. [7: Safe and Supportive Schools Policy, ACT Government, Education Directorate]
In addition to the overall suggestions around training and awareness-raising to assist in minimising and eliminating restrictive practices, some participants suggested the wide-spread adoption of techniques like the buddy system; pairing an older child with a younger child with a disability. This notion focusses on the idea of natural ambassadors that in every school there are students who will take on leadership roles and advocate for buddying and inclusion.
Techniques such as this lead us to consideration of Best Practice in relationship building for school settings. Are there strategies that schools can adopt to get to know a student with complex behavior? Discussions from consultations suggested that simple strategies that necessitate relationship building could see a marked difference in the experience of schooling for students who have complex needs and exhibit challenging behaviours. For instance, simply having a culture of staff and workers who seek to identify straightforward likes or dislikes, interests and hobbies could build a significant rapport and understanding between staff and students. Asking questions such as What does Alex like? Whats his favourite food? Whats his favourite part of the day? could provide significant insight into a students experience of a school day. It is useful to consider how such strategies could be best established and promoted across the education sector.
2.2.3. A capacity-building model to increase knowledge and skills across the sector regarding the use of restrictive practices
Discussions around capacity building within this consultation have yielded fruitful suggestions of ways in which a model to address capacity building could be developed for implementation across the ACT. Several components to capacity-building were considered; these include existing systems already in use across organisations in the area of minimising and eliminating restrictive practices, ways of upskilling the workforce and methods for increasing knowledge and awareness of restrictive practices and interventions.
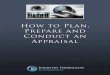
Top (smallest) component: specific skills set required to address the situation
Applicable to situations where there are complex problems and challenging behaviours seen. A detailed Behavioural Analysis
Middle component: Generic Sector Capacity Building required
Applicable to situations where it is necessary to think about some issues- are a persons basic needs being met?
Bottom (largest) component: Awareness- raising strategies required to address the situation
Goals of awareness-raising strategies: a focus on rights, self-regulation, consequences of practices used
Figure 2: Proposed capacity-building model for use across the ACT sector
The focus around training and capacity building within the data received for this consultation led to consideration of a proposed model for capacity building and increasing knowledge and skills across the sector in regards to the use of restrictive practices. Figure 2 outlines a three-stage model to reflect the components and differing situational or context requirements of capacity-building and training. A pyramid-shaped model, the largest component can be seen as the bottom section of the pyramid, suggesting that for a large percentage of time the only requirement within the capacity- building space is around awareness-raising of the sue of restrictive practices across the ACT sector.
The goals of such awareness-raising activities would be:
1. Promoting staff and workers to consider the rights of individuals they are working with;
2. Promotion of strategies to teach behaviours to staff around self-regulation
3. Sufficient training around definitions of restrictive practices, examples and explanations of the consequences for individuals upon whom restrictive practices or interventions are used.
The middle of the pyramid model reflects that across the sector there are a percentage of situations or cases whereby some generic capacity-building and training is required. For this stage of the model it is necessary for staff to be considering issues or behaviours from some individuals and questioning if the basic needs for that individual are being met; for example does the issue stem from a communication issue, a lack of explanation around a process, or a change in routine that has not been outlined to an individual. In this way, users of this model or framework are being prompted to consider whether or not a persons choices are being honoured before establishing plans of behavioural support.
The final, smallest section of this conceptual framework for capacity-building illustrates that for a small percentage of situations there is a need for specific skills and specialist training to be applied. For these situations, a detailed behavioural analysis may be required to assess and better understand complex problems and challenging behaviours.
The proposed model suggests that for the majority of the time, awareness-raising strategies and generic capacity building across the sector would be sufficient to provide staff and workers with adequate skills and knowledge. For the smaller proportion of complex cases and situations, specialized training and methods of analysis could be provided to assist in these situations.
Some useful feedback was provided within consultations regarding the issue of capacity building. Many participants could see a need for a system that allowed for specialist skill training as it was required- that it at the top end of the proposed model above. One participant stated: It comes back down to understanding and managing behaviour- I think people [frontline workers, staff and service providers] need to know when to call in an expert and they need to have a mechanism for gaining that kind of support and special training. This seems to be a key consideration emerging from these consultations. The provision of guidance about when to call in an expert for complex
behaviours would depend on both the availability of an expert as well as resources being available to pay for the expert. Alongside this, it would be necessary for requirements related to this to be implemented sector-wide. In particular, the relationship with an Office of the Senior Practitioner or other oversight body providing or commissioning this kind of expert support would need to be clearly stipulated and appropriately resourced for any subsequent reporting and compliance regime.
Other participants could see a need for training to be provided to staff around non- restrictions for some incidents. For example a person running may stop running if chasing ceases. A person exhibiting challenging or resistant behaviour following being pressured to do something may stop that behavior if pressure is ceased or diverted into a different approach.
Overall, participants were keen to see a stronger training and capacity-building model rolled out that is situated within a positive behaviour support framework. It was considered that the skills and competencies offered by Positive Behaviour Support (PBS) training were highly appropriate and
accessible to many situations within which restrictive interventions may currently be used. Positive Behaviour Support is a behaviour management system used by staff, educators and service providers to understand and resolve what is causing and contributing to an individual's challenging behaviour. Often, an individual's inappropriate behaviours are difficult to change because they are functional; that is, they serve a purpose for that individual. These behaviours are supported by reinforcement in the environment; for example, adults may reinforce a childs undesired behaviours because the child will receive objects and/or attention because of his/her behaviour. Positive Behaviour Support frameworks are embraced by many organisations with many promoting them as a preferred approach to working with behaviours of concern. The ACT Government promotes the use of PBS models in their school policy.[footnoteRef:8] Furthermore, in their evidence-based guidelines for minimising and eliminating the need for restrictive practices in the disability sector, the Australian Psychological Society also advocate that clinicians working with individuals presenting challenging behaviour should work within a positive behaviour support framework.[footnoteRef:9] It seems apt to suggest that if a thorough training program is initiated throughout the ACT around minimising and eliminating the need for restrictive interventions then the PBS approach comes with an existing evidence-informed base and current guidelines for use across the sector. [8: Safe and Supportive Schools Policy, ACT Government, Education Directorate] [9: Evidence-based guidelines to reduce the need for restrictive practices in the disability sector. Australian Psychological Society, 2011.]
2.2.4. Considerations for training and capacity-building
There were some considerations raised regarding the implementation and roll-out of any training and capacity-building strategies for the ACT. Some participants belonged to professions that are self- regulated, meaning that it can be hard for these staff to access accredited on-the-job training. For instance, staff working in allied health can have a variety of training pathways to become qualified in their professional field which then leads to staff having base knowledge that is of differing standards.
Other participants stated that any training would have to cover topics such as supported and substitutive decision making, person-centred care models or positive behaviour support. Their view was that there are many workers, involved in providing care and services across the ACT, who do not have basic skills in this, just as they dont have knowledge of these principles. Similarly, many participants felt that restrictive practices could be related to a lack of ability within the sector to achieve high quality planning for individuals and their needs. Thus, there is a need for training and capacity-building to be offered around developing support plans that are of high quality with consideration of avenues of practice.
It was also recommended that consideration be given to methods by which information around training and capacity-building opportunities or requirements are disseminated. For example, it would be necessary for whichever body is ultimately overseeing restrictive practices in the ACT to make sure they have adequate communication pathways through peak bodies for health, social services and allied health workers. Examples of bodies include via the Australian Health Practitioners Regulation Authority (AHPRA), Allied Health Professionals Australia (AHPA) and the ACT Teacher Quality Institute. Participants identified that however governance of restrictive practices for the ACT is formed any information, training, support or policy advice must be disseminated by regulatory bodies or membership bodies. This would ensure that people who work in formal paid services and informal services are in contact with and readily connected to bodies distributing this information.
In considering any recommendations given in this report related to training or capacity-building activities, it is necessary to note that this is an area that will require comprehensive investigation of overall education and training capacity across the sector. Certainly there is merit in suggesting that a wider environmental scan of resources and capability currently in existence and how these could be utilised in educational and conscious-raising activities related to restrictive practices. For example, if current sector development or training programs exist within the sector then it may not be necessary for the whole of education and funding to be the responsibility of an ACT Office of the Senior Practitioner. Rather, any oversight body may provide complementary measures alongside any such existing measures. We anticipate that the Phase 3 report will address these considerations in more detail.
3. Design Features and Recommendations for an ACT Office of the Senior Practitioner
Following analysis of the data captured within survey responses, consultations and submissions several design features have been identified as key recommendations for an ACT-based Office of the Senior Practitioner.
Awareness-raising activities, access to specialist advice and maintenance of a register from which regular reporting is undertaken were design elements that emerged through the process of consultations. Two different views were raised regarding the roles of an ACT Office of the Senior Practitioner in relation to providing sign-off on the use of restrictive practices and providing a monitoring and investigation role. Some participants identified that an OSP could be given authority to provide sign-off to the use of restrictive practices, possibly in consultation with a review panel comprised of multidisciplinary members to inform decision-making. However, other participants suggested that any sign-off authority should come from an external body (that is, not within an Office of the Senior Practitioner) and instead the ACT OSP should undertake the role of monitoring the use of restrictive practices and carrying out investigations.
There could be benefits with either approach taken. Certainly, if an Act Office of the Senior Practitioner were given authority to provide sign-off on the use of restrictive practices in individual cases then this is a specific function to be carried out accordingly by a dedicated office. However participants who saw that these two functions should be separated held the view that establishment of an external body to grant necessary sign-off and permission regarding restrictive practices would allow an OSP the position to manage roles of monitoring and investigation of the use of restrictive practices across the sector.
Box 2 provides an overview of all features.
Key design features for a future ACT Office of the Senior Practitioner
Design element
Detailed description
Awareness-raising and capacity building
A role within an Office of the Senior Practitioner to take the lead on awareness-raising around restrictive practices for the ACT and be a strategy leader around this
Specialist input
A system established whereby people working in the sector have access to a specialist for input into designing a plan around restrictive practices. This is to safeguard against a system whereby no assistance is provided to staff for developing a plan and then it is submitted to an Office of the Senior Practitioner and is requiring further information or refinement.
External sign-off and/or a role of monitoring and investigation
Two possibilities were raised: an Office of the Senior Practitioner in ACT could be given the ability to provide sign-off on cases involving restrictive practices- this decision process could be informed by a multi-disciplinary review panel. Alternatively, this role could be provided to an external body whilst an ACT OSP takes on the role of monitoring and investigating the use of restrictive practices across the sector.
Register and reporting function
An expectation that an ACT Office of the Senior Practitioner could undertake establishment and maintenance of a confidential register of restrictive practices, and that regular reporting on this data is released from the Office of the Senior Practitioner.
Box 2: Key design features for a future ACT Office of the Senior Practitioner
Consultation participants saw many roles and functions that could be performed by an ACT Office of the Senior Practitioner. These include:
Performing spot audits
Oversee capacity-building and training programs around the use of restrictive practices in the ACT
Building collaboration with key stakeholders within the pharmacist industry, which was a key recommendation from contributors representing the mental health sector
Best practice alerts- the Office of the Senior Practitioner could put out regular alerts to industry (e.g. a weekly bulletin) to maintain regular conversation. This could provide regular communication with service providers around best practice in this space.
Regular reporting- maintaining a register and reporting against this data would be useful to inform services of the scope of restrictive practices across the sector
The Office of the Senior Practitioner could be a well-informed independent voice to bring helpful attention to issues and opportunities across the Act sector. This could include opportunities to increase attention to: community values, capacity building activities and issues related to resources.
Many participants felt that the anchor point for an ACT Office of the Senior Practitioner should be around a Positive Behaviour Support framework and applied behavioural analysis. This is proposed on the premise that if the response to a behaviour honours a persons choice then behavior is likely to stop. Individuals are usually angry because they want something different (e.g. often there is an environmental cause or trigger). Also, a number of contributors were clear that there will be many
situations where the person is at risk of subjection to restrictive practices because they are angry or frustrated at being in current arrangements that do not reflect their choices. As such, the solution does not require a Positive Behaviour Support framework but instead a focus on honouring the persons choices. An ACT Office of the Senior Practitioner could take the lead in awareness related to this issue.
The characteristics of a person or persons who carry out the role of a senior practitioner were discussed at length within this consultation. One person stated: You need someone whos prepared to make a very rigid decisions as to if something should or should not be allowed. Other participants named various qualifications, backgrounds or experience that they felt were necessary for a person to fully execute this role. Examples included human rights specialist, psychologist, lawyer, trained healthcare provider or social services background.
The overall characteristics and factors required for consideration were:
to be skilled at understanding the circumstances of people subjected to restrictive practices
to be established in collaboration with other services and policy makers
to require mandatory reporting
to offer outreach services such as spot audits, training and capacity building, counselling of staff, case by case assessment or advice.
to have an office or panel of staff with different skill sets. For instance, there could be an Expert Committee established. This could be a multidisciplinary mix of people, including a teacher. This committee could act a sign off committee for the key work that is undertaken by the Office of the Senior Practitioner.
There was support amongst participants for a Restrictive Practices governing panel to be established, to oversee the use of restrictive practices across the ACT. Such panels operate in the Senior Practitioner offices within NSW and SA. Participants felt that any review panel would need to be made up of representatives from various backgrounds, settings and sectors. The possible list included:
1. Educational representative
2. Mental health consumers
3. Members of disability community
4. Carer/family member support representatives
5. Allied health workers
6. Frontline workers
7. Clinical and hospital representatives
8. Housing and social services representatives
9. Residential care facilities representatives
10. Legal experts
11. Local government representatives
12. Human rights expert
We anticipate delving into a deeper discussion in relation to this issue as part of the final report discussions and recommendations for this consultation.
3.1.Considerations in establishing an Office of the Senior Practitioner for the ACT
It is recognised that there are existing organisations across the ACT sector already performing reviews of restrictive practices. For example, the Seclusion and Restraint Review Panel has been established at Canberra Hospital and several mental health consumers sit on this panel as consumer representatives. Consultation participants expressed support for this panel and further suggested that it could carry a larger mandate. Similarly, an ACT based not-for-profit care provider runs a Restrictive Practices panel where senior practitioners come together to regularly review existing plans for restrictive interventions with their clients.
There is good sense in establishing partnerships with existing models or systems that carry out similar investigation and assessment practices. Some examples of this include the Official Visitors Scheme and the ACT Civil and Administrative Tribunal (ACAT).[footnoteRef:10][footnoteRef:11] There are also other organisations performing large-scale training in key areas that might overlap with the training and capacity- building areas mentioned in this report. The national Dementia Behaviour Management Advisory Service (DBMAS) for example is funded by the Australian government to offer capacity and knowledge building, mentoring and clinical supervision to people living with dementia, care workers, health professionals and family carers who are supporting a person with dementia and behavioural and psychological changes.[footnoteRef:12] [10: https://www.ptg.act.gov.au/resources/visitor-scheme accessed 20th March 2017] [11: http://www.acat.act.gov.au/ accessed 20th March 2017] [12: http://dbmas.org.au/what-we-do/who-is-eligible/ accessed 20th March 2017]
Furthermore, we are aware of the importance of considering existing legislation (both legislative law and case law) that could be built upon rather than writing new legislation with the establishment of an oversight body for Restrictive Practices across the ACT sector. It is significant to look at existing legislations or policies in other jurisdictions in which an Office of the Senior Practitioner has been established. For example, Victoria and Tasmania operate under a legislative regime, with Victoria using the Disability Act 2006 and Tasmania following the Disability Services Act 2011. In South Australia the Disability Services Act 1993 contains provisions for safeguarding policies and procedures, which includes alternatives to restrictive practices. New South Wales does not have a legislation that specifically covers restrictive practices; instead the use of restrictive practices in NSW is governed by the Department of Family and Community Services Behaviour Support Policy and Practice manual with main principles drawn from the Disability Inclusion Act 2014.
It is anticipated that our Phase 3 report due in June 2017 will provide detailed recommendations and considerations relating to the establishment of an ACT Office of the Senior Practitioner, including detailed provision of insights of processes occurring within other Office of the Senior Practitioner models across Australia.
4. Conclusion
Key elements from Phase 2 consultations are summarised in Box 3. These elements have been discussed within this report and we aim to centre Phase 3 consultations around these elements in order to build on these discussions.
Key elements for an ACT Office of the Senior Practitioner informed by Phase 2 consultation
Element
Detailed description
Awareness-raising and capacity building
A role within an Office of the Senior Practitioner to take the lead on awareness-raising around restrictive practices for the ACT and be a strategy leader around this
Specialist input
A system established whereby people working in the sector have access to a specialist for input into designing a plan around restrictive practices. This is to safeguard against a system whereby no assistance is provided to staff for developing a plan and then it is submitted to an Office of the Senior Practitioner and is requiring further information or refinement.
External sign-off and/or a role of monitoring and investigation
Two possibilities were raised: an Office of the Senior Practitioner in ACT could be given the ability to provide sign-off on cases involving restrictive practices- this decision process could be informed by a multi-disciplinary review panel. Alternatively, this role could be provided to an external body whilst an ACT OSP takes on the role of monitoring and investigating the use of restrictive practices across the sector.
Register and reporting function
An expectation that an ACT Office of the Senior Practitioner could undertake establishment and maintenance of a confidential register of restrictive practices, and that regular reporting on this data is released from the Office of the Senior Practitioner.
Suggested roles of ACT Office of the Senior Practitioner
1. Performing spot audits
2. Oversee capacity-building and training programs around the use of restrictive practices in the ACT
3. Building collaboration with key stakeholders within the pharmacist industry, which was a key recommendation from contributors representing the mental health sector
4. Best practice alerts- the Office of the Senior Practitioner could put out regular alerts to industry (e.g. a weekly bulletin) to maintain regular conversation. This could provide regular communication with service providers around best practice in this space.
5. Regular reporting- maintaining a register and reporting against this data would be useful to inform services of the scope of restrictive practices across the sector
Suggested necessary skills, characteristics and experience of a Senior Practitioner
1. Needs to be skilled at understanding the circumstances of people subjected to restrictive practices
2. Needs to be established in collaboration with other services and policy makers
Box 3: Key elements from Phase 2 consultations
5. Appendix 1: Copy of online survey questions
The ACT Government has commissioned JFA Purple Orange to undertake a consultation process to inform the establishment of an Office of the Senior Practitioner (OSP)
This survey is to inform the design of a regulatory approach for minimising and eliminating restrictive practice for vulnerable people in the ACT Community. Prior to taking this survey, we suggest that you read the discussion paper 'An overview of restrictive practices, and the key issues for consideration in relation to the establishment of an Office of the Senior Practitioner - January 2017' which sets out the main considerations when thinking about an Office of the Senior Practitioner in the ACT.
You can find the paper on our website (http://www.actosp.org.au)
Welcome to the ACT OSP survey
About you
1. Could you please indicate if you are:
(you can select as many options as apply to your situation)
A person living with a disability or mental illness
A family member or friend of a person living with disability or mental illness
Work for a disability 'service provider' (e.g. disability accommodation, disability employment, at home support, respite and day programs etc.)
Work for a mental health service provider Work for an education provider
A clinician providing behavioural support
An advocacy organisation or consumer governed organisation A government representative
A peak organisation
Work for an aged care provider Work for a health service provider A clinician or allied health therapist Other (please specify below)
About what restrictive practices mean
2. Do you think the term restrictive practice is widely understood in the ACT? Yes
No
3. Which of the following do you think are restrictive practices? (Tick all that apply)
Mechanical, such as devices that limit a persons movements (and this includes the removal and/ or disengagement of mechanical supports that assist the persons movements)
Seclusion, such as the sole confinement of a person at any time in any room where the doors and windows cannot be opened by that person to get out
Environmental, such as preventing the person's access to all parts of their house/environment (for example locking the refrigerators, or locking the door to the kitchen)
Social, such as stopping the person accessing people they mutually know or social opportunities that are important to them
Chemical, such as medications that blunt the persons emotions, cognition, physical activity and movement
Physical, such as holding or pinning down by another person
Psycho-social restraints, such as where another person uses threats, intimidation, fear, coercion, discipline, or retaliation
Organisational, such as excluding the person from activities, and restrictions to the person's choice
Communication restraint, such as switching off someones communication device
Decision making restraint, such as failing to provide options that help the person make their own choices and decisions
Other
Please use the box below to provide more information about your answers
4. Should the ACT adopt a clear definition of restrictive practice? Yes
No
About your experiences of restrictive practice
5. Have you had personal experience of restrictive practice?
(this question relates to the person themselves as the recipients, please go to question 9 if you are answering on behalf of someone else)
Yes (go to Question 6) No (go to Question 9)
6. What types of restrictive practice did you personally experience?
(again this question relates to the person themselves as the recipient, so please go to question 9 if you are answering on behalf of someone else)
Mechanical Seclusion Environmental Social Chemical Physical Psycho-social Organisational
Communication restraint Decision making restraint Other (please specify below)
7. How long ago did you personally experience restrictive practice?
please specify in the comment box
8. Do you feel that the restrictive practice was a reasonable response to your situation, or would you have preferred something different?
please specify in the comment box
9. Has someone you know had personal experience of restrictive practice? Yes (go to Question 10)
No (go to Question 14)
10. What types of restrictive practice did that person experience?
please tick below as many as apply
Mechanical Seclusion Environmental Social Chemical Physical Psycho-social Organisational
Communication restraint Decision making restraint Other (please specify below)
11. How long ago did that person experience restrictive practice?
please specify in the comment box
12. Did that person feel that the restrictive practice was a reasonable response to their situation, or would they have preferred something different?
please specify in the comment box
13. Do you think it was reasonable?
please specify in the comment box
14. Are you aware of restrictive practices being used in any particular settings?
If yes, please tick below as many as apply
School
Congregate home / group home
Institution. eg. large scale accommodation service
Day option program Disability service Aged care facility
In-patient mental health unit Private home
Hospital Custodial setting No, not aware
Other (please specify below)
About whether there should be laws or regulations about restrictive practices
15. Are there any situations where restrictive practices are unavoidable? Yes (go to Question 16)
No (go to Question 17)
16. If yes, please provide details of situations where you think restrictive practices might need to be used
17. Should there be a law or regulation that allows restrictive practices to only happen in certain circumstances?
Yes (go to Question 18) No (go to Question 19)
18. If so, what types of things do you think that law or regulation should say about when restrictive practices can or can't be used?
19. What else could help?
About whether there should be external permission for restrictive practices
20. Should service providers (disability service providers, mental health service providers, schools, and other services for children, aged care providers, etc) have to get external permission before they can use restrictive practices on someone?
Yes (go to Question 21) No (go to Question 26)
It depends (please specify below, then go to Question 21)
21. Should a new ACT Office of the Senior Practitioner have the responsibility for giving permission to an organisation to use restrictive practices?
Yes (go to Question 22) No (go to Question 23)
22. What qualifications, skills and experience should the Senior Practitioner have?
(use the box below and then go to question 26)
23. If you think there should be external permission, but not an ACT Office of the Senior Practitioner, is there some other ACT or national agency that could do this and why do you think they would be the right agency?
(use the box below and then go to question 24)
24. If you think there does not need to be external permission, who should be in charge of such decisions inside the service provider?
25. What qualifications, skills and experience should that person have (or panel, if you think there should be more than one person involved in making the decision)?
About whether there should be a register showing where restrictive practices are happening
26. Do you think it would be a good idea for there to be a register of every person who is being subjected to restrictive practices, so that the arrangements can be tracked and reported on?
Yes (go to Question 27) No (go to Question 30)
27. If yes, how do you think that register should work, including how it is reported?
28. Do you think an ACT Office of the Senior Practitioner should run the register? Yes (go to Question 30)
No (go to Question 29)
29. Who else could have the responsibility for running the register, and why would they be a good choice for this?
About whether there should be a strategy to raise awareness about restrictive practices
30. Do you think it is important there is a strategy to raise awareness of the problems of restrictive practices?
Yes (go to Question 31) No (go to Question 32)
31. Do you think an ACT Office of the Senior Practitioner could do this? Yes (go to Question 33)
No (go to Question 32)
32. Who else could have the responsibility for running a strategy to raise awareness of the problems of restrictive practice, and why would they be a good choice for this?
33. What would be the priorities in that strategy for raising awareness?
About whether there should be a strategy to build sector capacity to use alternatives to Restrictive Practices
34. Do you think it is important there is a strategy to build skills within service providers, so that more staff know how to provide alternatives to restrictive practices?
Yes (go to Question 35) No (go to Question 36)
35. Do you think an ACT Office of the Senior Practitioner could do this? Yes (go to Question 37)
No (go to Question 36)
36. Who else could have the responsibility for running a strategy to build sector capacity, so that more staff know how to provide alternatives to restrictive practices?
Also tell us why you think they would be a good choice for this
37. Are there any particular skill areas that you think should be prioritised in this strategy?
About duplication and gaps
38. The ACT and Commonwealth Governments already have some laws, regulations and policies which may be relevant to the issue of restrictive practices.
Which ones do you think an ACT Office of the Senior Practitioner would definitely need to connect with, to avoid duplication or gaps?
Please use the box below to explain your preference
39. If there is an ACT Office of the Senior Practitioner, which of the following do you think would be the best way to govern it (select one only):
A separate, statutory authority, with the Senior Practitioner reporting directly to the ACT Legislative Assembly
A separate, statutory authority, with the Senior Practitioner reporting to a Government Minister
A separate, statutory authority, with the Senior Practitioner reporting directly to a board that includes a range of perspectives, clinicians, people living with disability, families, mental health, etc
Place it within an existing ACT government department Place it within an existing ACT commission
Other
About governance
40. The ACT and Commonwealth Governments already have some services that come into contact with people who may be subject to restrictive practices. This may include care and protection services, official visitor schemes, rights complaints services, ACT treatment order arrangements, and other duties undertaken by offices within the ACT Human Rights Commission, including the Discrimination, Health
Services, Disability & Community Services Commissioner, the Public Advocate, and the Children and Young People Commissioner.
Which ones do you think an ACT Office of the Senior Practitioner would definitely need to connect with, to avoid duplication or gaps?
41. Is there anything else you would like to share with us about the issue of restrictive practices?
Thank you for sharing your views in this survey.
If you would like to provide additional comments about the establishment of an Office of the Senior Practitioner we welcome written submissions to:
ACT OSP
JFA Purple Orange PO Box 701
Unley Business Centre SA 5061
Or via email - [email protected], using the subject header 'ACT OSP consultation' Or call us on 1300 857 327 and ask for the ACT OSP project.
To keep in touch with this consultation, including the results of this survey, go to www.actosp.org.au