Embed Size (px)
Citation preview

SURGICAL SKILLS EDUCATION IN
UROLOGY – DOES IT MATTER?
Jeff McKay
Scott Bagnell

Conflict of Interest Statement
No conflict of interests to state

Outline
1. Definitions
2. Do we need surgical simulation? Why?
3. Types of surgical simulation in urology
4. Strengths/weaknesses of simulation
5. Implementing simulation curriculum into
residency program

Outline
1. Definitions
2. Do we need surgical simulation? Why?
3. Types of surgical simulation in urology
4. Strengths/weaknesses of simulation
5. Implementing simulation curriculum into
residency program

Definitions
Simulator
Device that enables operator to reproduce or represent test
conditions or phenomena likely to occur in actual
performance
Fidelity
How “realistic” is the simulator
Low or High-fidelity
Merrium-Webster Online Dictionary. Avail at www.merrium-
webster.com

Fidelity
Low fidelity ureteroscopy trainer
High fidelity ureteroscopy
trainer
Matsumoto et al. The effect of bench model fidelity on endourological skills: a randomized
controlled study. J Urol 2002. 1243-1247

Definitions
Virtual Reality
Artificial environment which is experienced through sensory
stimuli provided by a computer and in which one’s actions
partially demonstrate what happens in the environment
Merrium-Webster Online Dictionary. Avail at www.merrium-
webster.com

Virtual Reality simulators

VALIDATION
Validity
Instrument appropriately measures what it was intended to
measure
Subjective and objective benchmarks
Wignall et al. Surgical simulation: a urological perspective. J Urol 2008. 179; 1690-1699

Subjective Validity Assessment
Face validity
Test seems reasonable and appropriate
Content validity
Assures contents of test cover relevant areas
Wignall et al. Surgical simulation: a urological perspective. J Urol 2008. 179; 1690-1699

Objective Validity Assessment
Criterion validity
Correlation of results of tool with established tool
Predictive validity
- Extent which scores on new test predict future clinical performance
Construct validity
Used if no clear standard exists for comparison
Wignall et al. Surgical simulation: a urological perspective. J Urol 2008. 179; 1690-1699

Objective Structured Assessment of Technical
Skills Examination
Best measure of operative performance
Checklists & global rating scales for evaluation of
tasks
Few simulators have undergone rigorous tests that
would fully validate use for training or proficiency
assessment
Wignall et al. Surgical simulation: a urological perspective. J Urol 2008. 179; 1690-1699

Outline
1. Definitions
2. Do we need surgical simulation? Why?
3. Types of surgical simulation in urology
4. Strengths/weaknesses of simulation
5. Implementing simulation curriculum into
residency program

Need for Surgical Simulation in Urology
Decreasing opportunities for residents to learn in OR
Limited work hours
Financial constraints – surgical efficiency
Fear of litigation
Increasingly complex cases
Practising surgeons often learning new skills
*Anastakis et al. Evaluating the effectiveness of a 2-year curriculum in surgical skills center.
Am J Surg 2003; 185: 378

Barriers to Surgical Simulation
Small market
Few simulators validated for teaching
High cost of software design
High cost of simulators at centres
Selecting and retaining suitable faculty
1. Wignall et al. Surgical Simulation: A Urological Perspective. J Urol 2007
2. Forster et al. Surgical simulators in urological training – views of UK
training programme directors BJU Int 2011.

Outline
1. Definitions
2. Do we need surgical simulation? Why?
3. Types of surgical simulation in urology
4. Strengths/weaknesses of simulation
5. Implementing simulation curriculum into
residency program

Types of Surgical Simulation in Urology
Cystoscopy
Ureteroscopy
TURP/TURBT
PCNL with Renal Access
Laparoscopy
Robotics

Types of Surgical Simulation in Urology
Cystoscopy
Ureteroscopy
TURP/TURBT
PCNL with Renal Access
Laparoscopy
Robotics

Cystoscopy – Surgical simulation
Schout et al. Transfer of cysto-urethroscopy skills from virtual-reality simulator to
the operating room. A randomized control trial. BJU Int 2009

Cystoscopy – surgical simulation
100 interns randomized
Schout et al. Transfer of cysto-urethroscopy skills from virtual-reality simulator to
the operating room. A randomized control trial. BJU Int 2009

Cystoscopy – surgical simulation
Schout et al. Transfer of cysto-urethroscopy skills from virtual-reality simulator to
the operating room. A randomized control trial. BJU Int 2009

Cystoscopy – surgical simulation
Schout et al. Transfer of cysto-urethroscopy skills from virtual-reality simulator to
the operating room. A randomized control trial. BJU Int 2009

Cystoscopy – Surgical simulation Conclusion
Interns who trained on UroMentor outperformed controls
Schout et al. Transfer of cysto-urethroscopy skills from virtual-reality simulator to
the operating room. A randomized control trial. BJU Int 2009

Types of Surgical Simulation in Urology
Cystoscopy
Ureteroscopy
TURP/TURBT
PCNL with Renal Access
Laparoscopy
Robotics

Ureteroscopy – surgical simulation
Ureteroscopy – surgical simulation
Research QUESTION:
Does bench model fidelity affect surgical skills?
40 4th year med students randomized to:
1. Didactic session (7)
2. Low fidelity bench model practice (16)
3. High fidelity bench model practice (17)
Matsumoto et al. The effect of bench model fidelity on endourological skills: a randomized
controlled study. J Urol 2002. 1243-1247

Ureteroscopy – Surgical Simulation
Matsumoto et al. The effect of bench model fidelity on endourological skills: a randomized controlled study. J Urol 2002. 1243-1247

Ureteroscopy – surgical simulation
Conclusion:
1. Low-fidelity and high-fidelity significantly improved GRS
and pass rate
2. Low fidelity had similar results to high fidelity at a much
cheaper cost
Matsumoto et al. The effect of bench model fidelity on endourological skills: a randomized
controlled study. J Urol 2002. 1243-1247

Ureteroscopy – surgical simulation
20 2nd year medical students randomized to:
1. Control (untrained) group
2. Test (trained) group
Watterson et al. A randomized, prospective blinded study validating the acquisition of ureteroscopy
skills using a computer based virtual reality endourological simulator. J Urol 2002

URO Mentor – VR Simulation
Watterson et al. A randomized, prospective blinded study validating the acquisition of ureteroscopy
skills using a computer based virtual reality endourological simulator. J Urol 2002

Results
Watterson et al. A randomized, prospective
blinded study validating the acquisition of
ureteroscopy skills using a computer based
virtual reality endourological simulator. J Urol
2002

Ureteroscopy – surgical simulation
Established:
Face validity
Content validity
Not established
Criterion validity
Watterson et al. A randomized, prospective blinded study validating the acquisition of ureteroscopy
skills using a computer based virtual reality endourological simulator. J Urol 2002

Ureteroscopy – surgical simulation
16 Urology residents assessed on basket extraction of
distal ureteric stone using UroMentor VR simulator
Performance on VR simulator compared to high fidelity
bench model (UroScopic Trainer)
Matsumodo et al. Virtual reality ureteroscopy simulator as a valid tool
for assessing endourological skills. Int J Urol. 2006.

VR simulator vs high fidelity bench model
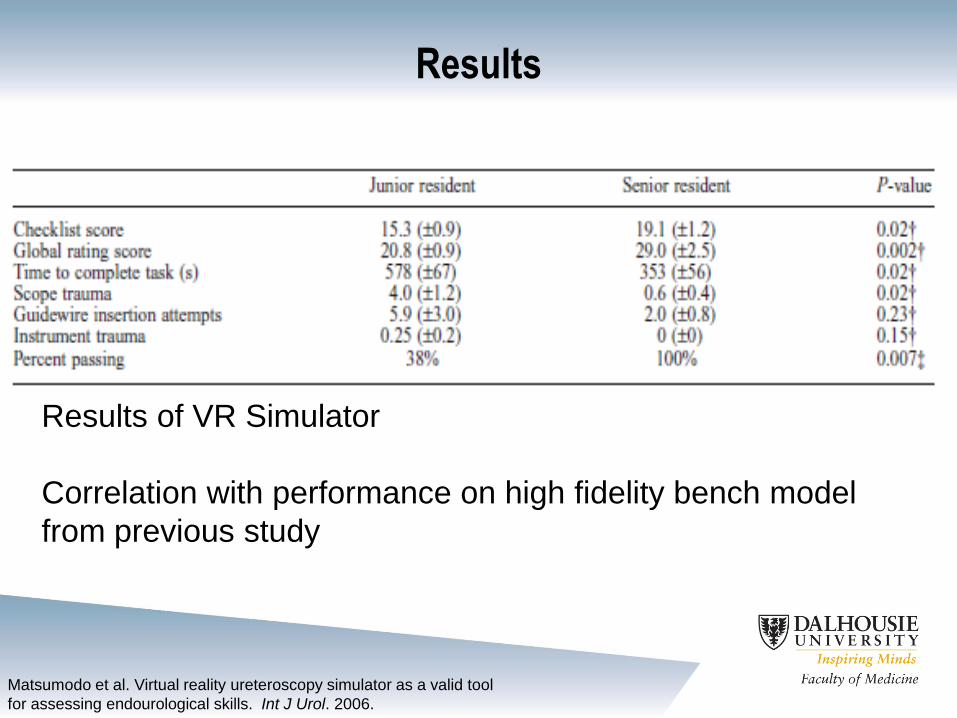
Results
Results of VR Simulator
Correlation with performance on high fidelity bench model
from previous study
Matsumodo et al. Virtual reality ureteroscopy simulator as a valid tool
for assessing endourological skills. Int J Urol. 2006.

Conclusions
UroMentor is a useful tool for the assessment of
resident performance
Predictive validity and content validity as performance
correlated with UroScopic trainer
Future studies needed to correlate performance in the
OR
Matsumodo et al. Virtual reality ureteroscopy simulator as a valid tool
for assessing endourological skills. Int J Urol. 2006.

Types of Surgical Simulation in Urology
Cystoscopy
Ureteroscopy
TURP/TURBT
PCNL with Renal Access
Laparoscopy
Robotics

TURP – Surgical Simulation
URO-Trainer
VR simulator SurgicalSIM
TURP simulator

Simbionix TURP trainer

TURP – Surgical Simulation
• Version 1.0 of VR based TURP simulator
• 72 board certified urologists
• 19 novices
Participants:
• Completed pre-task questionnaire
• Viewed training video
• Performed pre-compiled 5-minute resection task

Results
Sweet et al. Face, content and construct validity of the University of Washington virtual reality
transurethral prostate resection trainer. J Urol 2004; 172: 1953-1957

Conclusions
Face, content, construct validity for v1.0 of Univ of
Washington TURP Simulator
Need predictive validity study to complete validation
Integration of simulator into training is appropriate
Not validated for assessment until more rigorous
validation complete
Sweet et al. Face, content and construct validity of the University of Washington virtual reality
transurethral prostate resection trainer. J Urol 2004; 172: 1953-1957

TURBT Simulation
24 medical students
12 residents in urology
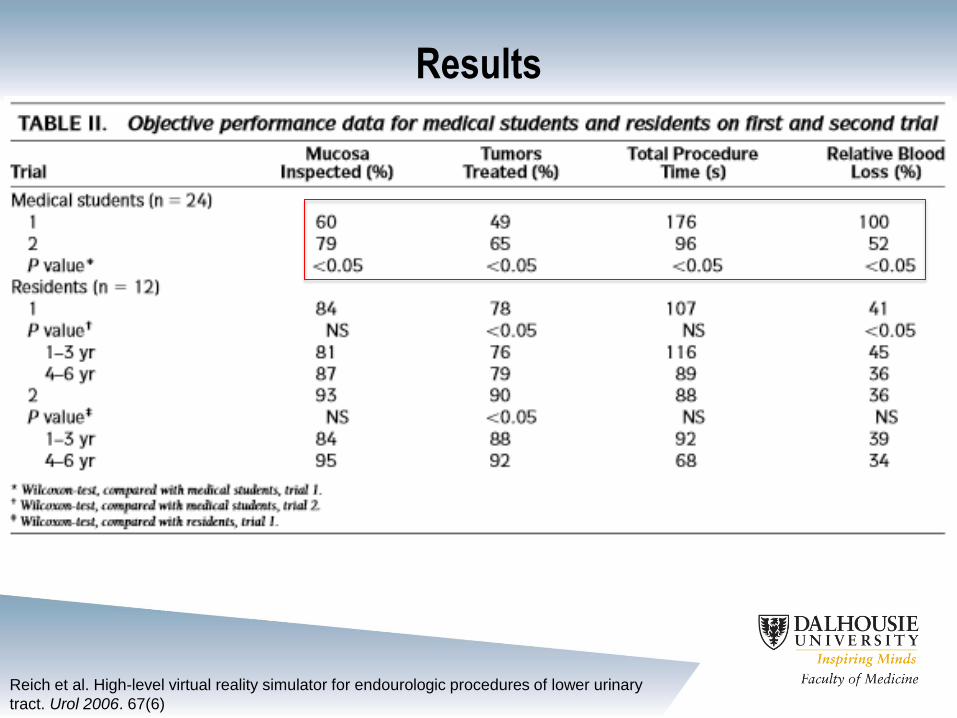
Results
Reich et al. High-level virtual reality simulator for endourologic procedures of lower urinary
tract. Urol 2006. 67(6)

Conclusions
Face, content and construct validity achieved
Results of this study support need for prospective RCT
for predictive validity
TURP model to be added in the future
Reich et al. High-level virtual reality simulator for endourologic procedures of lower urinary
tract. Urol 2006. 67(6)

Types of Surgical Simulation in Urology
Cystoscopy
Ureteroscopy
TURP/TURBT
PCNL with Renal Access
Laparoscopy
Robotics

PERC RENAL ACCESS & PCNL TRAINERS

PERC Mentor
63 subjects
• 31 medical students
• 31 residents
• 1 fellow

Global Rating Scale
Knudsen et al. A randomized, controlled, prospective study validating the acquisition of
percutaneous renal collecting systm access skills using a computer based hybrid virtual
reality srugical simulator: phase I. J Urol 2006

Results - PercMentor
Knudsen et al. A randomized, controlled, prospective study validating the acquisition of
percutaneous renal collecting systm access skills using a computer based hybrid virtual
reality srugical simulator: phase I. J Urol 2006

Results - PercMentor
Knudsen et al. A randomized, controlled, prospective study validating the acquisition of
percutaneous renal collecting systm access skills using a computer based hybrid virtual
reality srugical simulator: phase I. J Urol 2006

Conclusions
Training on Perc mentor was beneficial in learning and
performing steps of renal collecting system access
using VR model
Face, content and convergent validity established
Predictive ability to be tested in Phase II using live
porcine model
Knudsen et al. A randomized, controlled, prospective study validating the acquisition of
percutaneous renal collecting systm access skills using a computer based hybrid virtual
reality srugical simulator: phase I. J Urol 2006

Types of Surgical Simulation in Urology
Cystoscopy
Ureteroscopy
TURP/TURBT
PCNL with Renal Access
Laparoscopy
Robotics

Laparoscopy – Surgical Skills
CORRECT USE OF
BOX TRAINERS
INCORRECT USE
OF BOX TRAINERS

Laparoscopy – Surgical Skills

Laparoscopy – low fidelity
12 Urology residents
• 6 into training group
• 6 into non-training group
Traxer et al. The impact of intense laparoscopic skills training on the operative performance of
urology residents. J Urol 2001 166;1658-1661

No significant difference
between groups
Traxer et al. The impact of intense laparoscopic skills training on the operative performance of urology
residents. J Urol 2001 166;1658-1661

Laparoscopy – VR simulation
Brewin et al. Face, content and construct validation of the first virtual reality
laparoscopic nephrectomy simulator. BJU Int 2009.
• 8 expert urological laparoscopic surgeons
• 10 trainee urologists (performing or observing)
• 10 novice urologists (observation)

Results
Brewin et al. Face, content and construct validation of the first virtual reality
laparoscopic nephrectomy simulator. BJU Int 2009.

Conclusions
Face, content and construct validity established
Good training tool for Lap Radical Nephrectomy
Need predictive studies
Brewin et al. Face, content and construct validation of the first virtual reality
laparoscopic nephrectomy simulator. BJU Int 2009.

Types of Surgical Simulation in Urology
Cystoscopy
Ureteroscopy
TURP/TURBT
PCNL with Renal Access
Laparoscopy
Robotics

Robotics – surgical simulation
Da Vinci Robot surgical simulator
Hung et al. Face, content and construct validity of a novel robotic surgery simulator. J Urol 2011

Robotics – Surgical simulation
Hung et al. Face, content and construct validity of a novel robotic surgery simulator. J Urol 2011
16 novices (no surgical training)
32 intermediates (median 0 robotic cases)
15 experts (median 315 robotic cases)

Results
Hung et al. Face, content and construct validity of a novel robotic surgery simulator. J Urol 2011

Results
Hung et al. Face, content and construct validity of a novel robotic surgery simulator. J Urol 2011

Conclusion
Face, content and construct validity of da Vinci Skills
simulator established
Predictive studies need to be completed
Further software development with procedure based
modules to augment usefulness for advanced training
Hung et al. Face, content and construct validity of a novel robotic surgery simulator. J Urol 2011

Outline
1. Definitions
2. Do we need surgical simulation? Why?
3. Types of surgical simulation in urology
4. Strengths/weaknesses of simulation
5. Implementing simulation curriculum into
residency program

Strengths & Weaknesses
Strengths
Safe way to practice without compromising patient care
Gain familiarity with procedure before assisting
Muscle memory to aid in OR
Cost – some low fidelity models cheap and portable
Possible use for assessment in the future

Weaknesses
Cost
Predictive validity still needs to be determined for many
simulators
Some simulators may not be realistic
Adequate training and supervision for simulation
Strengths & Weaknesses

Outline
1. Definitions
2. Do we need surgical simulation? Why?
3. Types of surgical simulation in urology
4. Strengths/weaknesses of simulation
5. Implementing simulation curriculum into
residency program

Simulation in Urology
Positive transfer of skills from simulation to OR1
USA urology training programs2:
68% have simulation education centres
88% of urological depts have access to these
- 76% laparoscopy
- 16% cystoscopy
- 21% ureterorenoscopy
- 12% percutaneous renal access
- 8% TURP
1Laguna et al. How far will simulators be involved into training? J Endourol 2011 2Le et al. The current role of medical simulation in american urological residency programs:
an assessment by program directors. J Urol 2007

Implementing Simulation in Residency Training
Surgical simulation should be complementary to
standard surgical training
Future holds updated software, new simulators, new
technologies
No ideal curricula or model currently exists

Future of Surgical Simulation at DALHOUSIE
Simbionix TURP Simulator

Outline
1. Definitions
2. Do we need surgical simulation? Why?
3. Types of surgical simulation in urology
4. Strengths/weaknesses of simulation
5. Implementing simulation curriculum into
residency program
References 1. Merrium-Webster Online Dictionary. Avail at www.merrium-webster.com
2. Matsumoto et al. The effect of bench model fidelity on endourological skills: a randomized
controlled study. J Urol 2002. 1243-1247
3. *Anastakis et al. Evaluating the effectiveness of a 2-year curriculum in surgical skills center.
Am J Surg 2003; 185: 378
4. Forster et al. Surgical simulators in urological training – views of UK training programme
directors BJU Int 2011.
5. Schout et al. Transfer of cysto-urethroscopy skills from virtual-reality simulator to the
operating room. A randomized control trial. BJU Int 2009
6. Watterson et al. A randomized, prospective blinded study validating the acquisition of
ureteroscopy skills using a computer based virtual reality endourological simulator. J Urol
2002
7. Matsumodo et al. Virtual reality ureteroscopy simulator as a valid tool for assessing
endourological skills. Int J Urol. 2006.
8. Sweet et al. Face, content and construct validity of the University of Washington virtual reality
transurethral prostate resection trainer. J Urol 2004; 172: 1953-1957

References cont’d
9. Reich et al. High-level virtual reality simulator for endourologic procedures of lower urinary
tract. Urol 2006. 67(6)
10. Knudsen et al. A randomized, controlled, prospective study validating the acquisition of
percutaneous renal collecting systm access skills using a computer based hybrid virtual
reality srugical simulator: phase I. J Urol 2006
11. Traxer et al. The impact of intense laparoscopic skills training on the operative performance
of urology residents. J Urol 2001 166;1658-1661
12. Brewin et al. Face, content and construct validation of the first virtual reality laparoscopic
nephrectomy simulator. BJU Int 2009
13. Hung et al. Face, content and construct validity of a novel robotic surgery simulator. J Urol
2011
14. Laguna et al. How far will simulators be involved into training? J Endourol 2011
15. Le et al. The current role of medical simulation in american urological residency programs:
an assessment by program directors. J Urol 2007

Questions?





























