Embed Size (px)
Citation preview

Molecular Pathogenesis of Hodgkin’s Lymphoma:Increasing Evidence of the Importance ofthe MicroenvironmentChristian Steidl, Joseph M. Connors, and Randy D. Gascoyne
From the British Columbia CancerAgency, University of British Columbia,Vancouver, British Columbia, Canada.
Submitted September 19, 2010;accepted January 4, 2011; publishedonline ahead of print at www.jco.org onApril 11, 2011.
Supported in part by the Michael SmithFoundation for Health Research, theLymphoma Research Foundation, and apostdoctoral fellowship from theCancer Research Society (Steven E.Drabin fund; C.S.); Project Grant No.019001 from the Terry Fox FoundationNew Frontiers Program (J.M.C.,R.D.G.); and Grant No. 178536 from theCanadian Institutes for Health Research(R.D.G.).
Authors’ disclosures of potential con-flicts of interest and author contribu-tions are found at the end of thisarticle.
Corresponding author: RandyGascoyne, MD, Department of Pathol-ogy and Experimental Therapeutics,British Columbia Cancer Agency, 675West 10th Ave, Room 5-113, Vancou-ver, BC V5Z 1L3, Canada; e-mail:[email protected].
© 2011 by American Society of ClinicalOncology
0732-183X/11/2999-1/$20.00
DOI: 10.1200/JCO.2010.32.8401
A B S T R A C T
Hodgkin’s lymphoma (HL) represents the most common subtype of malignant lymphoma in youngpeople in the Western world. Most patients can be cured with modern treatment strategies,although approximately 20% will die after relapse or progressive disease. The histologic hallmarkof the disease is the presence of the characteristic Hodgkin Reed-Sternberg (HRS) cells in classicalHL and so-called lymphocyte-predominant (LP) cells in nodular lymphocyte-predominant HL. HL isunique among all cancers because malignant cells are greatly outnumbered by reactive cells in thetumor microenvironment and make up only approximately 1% of the tumor. Expression of avariety of cytokines and chemokines by the HRS and LP cells is believed to be the driving force foran abnormal immune response, perpetuated by additional factors secreted by reactive cells in themicroenvironment that help maintain the inflammatory milieu. The malignant HRS and LP cellsmanipulate the microenvironment, permitting them to develop their malignant phenotype fully andevade host immune attack. Gene expression signatures derived from non-neoplastic cells correlatewell with response to initial and subsequent therapies, reflecting their functional relevance. Recentbiomarker studies have added texture to clinical outcome predictors, and their incorporation intoprognostic models may improve our understanding of the biologic correlates of treatment failure.Moreover, recent preclinical and clinical studies have demonstrated that the tumor microenvironmentrepresents a promising therapeutic target, raising hope that novel treatment strategies focused on theinterface between malignant and reactive cells will soon emerge.
J Clin Oncol 29. © 2011 by American Society of Clinical Oncology
INTRODUCTION
Hodgkin’s lymphoma (HL) accounts for approxi-mately 11% of all malignant lymphomas.1 The mor-phologic hallmarks of this unique lymphoma wereinitially described more than 100 years ago; it ischaracterized by the presence of Hodgkin Reed-Sternberg (HRS) cells in classical HL (cHL) and so-called lymphocyte-predominant (LP) cells innodular lymphocyte-predominant HL (NLPHL).2
Typically, malignant cells are greatly outnumberedby reactive cells in a microenvironment that in-cludes lymphocytes, macrophages, eosinophils,mast cells, plasma cells, stromal cells, fibroblasts, andother cells.3 Specifically in cHL, the frequencies of allthese cellular components, including the HRS cells,vary considerably between cHL subtypes; lympho-cyte rich, lymphocyte depleted, mixed cellularity(MC), and nodular sclerosis (NS).
Independent of advances in understanding theetiology and molecular biology of HL, the introduc-tion of polychemotherapy has reduced the numberof patients who succumb to the disease by more than
60% since the early 1970s.4 Consequently, most pa-tients are cured by modern treatment strategies. Im-portant milestones in our understanding of HLinclude first, separation of HL into cHL versusNLPHL; second, development of distinct treatmentstrategies for limited versus advanced disease; andthird, validation of the International PrognosticScore for advanced disease.5,6 Since its introductionin 1998, the International Prognostic Score has be-come the gold standard for risk assessment andstratification and been used to guide treatment de-cisions in advanced cHL. However, it can be antici-pated that progress, especially among those 20% ofpatients who are still destined to die after relapse orprogressive disease, will be tightly linked to novelbiomarker discovery and targeted therapies for re-lapsed disease.7
In this review, we will first focus on the cross-talk between malignant and reactive cells in the mi-croenvironment mediated by cytokines andchemokines expressed in HL tissue. These solublefactors mediate the specific cellular composition of
JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I C L E
© 2011 by American Society of Clinical Oncology 1
http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2010.32.8401The latest version is at Published Ahead of Print on April 11, 2011 as 10.1200/JCO.2010.32.8401
Copyright 2011 by American Society of Clinical Oncology
Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

the reactive infiltrate, promote receptor-mediated signaling, and cul-tivate immune privilege for malignant cells. We will then review theprognostic implications of the tumor microenvironment and finallydiscuss novel therapeutic approaches targeting the microenvironmentor microenvironment-dependent receptor signaling.
CROSSTALK BETWEEN CELLS: THE IMPORTANCE OFCYTOKINES AND CHEMOKINES IN HL
Cytokines and chemokines are low–molecular weight proteins with awide variety of functions that work either in a paracrine manner to
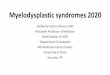
modulate the activity of surrounding cells or in an autocrine fashion todirectly affect the cells that produce them. Specifically, these autocrineand paracrine interactions lead to the particular cellular compositionfound in HL and contribute to the proliferation and antiapoptoticphenotype of HRS cells (Fig 1). Although the cytokine and chemokinemilieu in HL tissues is complex and interactive, a clear understandingof this biology will be clinically relevant in the future as therapies aredeveloped that disrupt the crosstalk between malignant cells and themicroenvironment. Hence, improved insight into the biology will becritical to introducing these novel biologic treatments into clinicalpractice. This section focuses on the involvement of cytokines in the
Eosinophil FGF1/2IL-13
IL-13R
CCL11/Eotaxin
HRS cell
Mast cell
Macrophage
T cell(Treg /TH2)
NK cell
B cell
FibroblastFibroblast
Plasma cell
Cytotoxic T cell
CCL5
CD30
CD30L
CD30L
CD30IL-5MEC
CSF1
CSF1R
TARCMDCCCL20
TNF-αLT-αTGF-βBAFF
CCR4
CD40
CD40L
TNFRfamily
CXCL16
CCR3/CCR10
CCR10
BLCIL-4
CCR3
CCR3
CX3CL1
CX3CR1
MIF
IL-10TGFβ
PDL1
T cell(TH1)
PD-1
IFNγ
IFNγ
Gal-1
CD7
IL-2
IL-2R
CD74
FASLCD95
APRIL
Neutrophil
IL8
IL8
CXCR1/2
HLA-G
Fig 1. Schematic of the crosstalk between malignant Hodgkin Reed-Sternberg (HRS) cells and the tumor microenvironment in classical Hodgkin’s lymphoma. In thecenter, a bi-nucleated HRS cell is shown expressing characteristic surface molecules as well as secreted cytokines and chemokines. Surrounding the HRS cells arecell types representative of the non-neoplastic cells attracted and activated by these molecules. The cells in the microenvironment themselves express a variety ofchemokines and cytokines that further shape the reactive infiltrate and provide signaling for HRS cells. Only the main activating and inhibitory functions (arrows) ofpredominantly membrane-bound (purple triangles) and secreted molecules mediated by surface receptors (pink) are illustrated; other interactions exist. IL, interleukin;FGF, fibroblast growth factor; TNF-�, tumor necrosis factor �; LT-�, lymphotoxin �; TGF-�, transforming growth factor �; BAFF, B-cell activating factor; APRIL, aproliferation-inducing ligand; BLC, B lymphocyte chemoattractant; TNFR, tumor necrosis factor receptor; FASL, Fas ligand; MEC, mucosae-associated epithelialchemokine; Treg, T regulatory cell; TH, T helper cell; TARC, thymus and activation-related chemokine; MDC, macrophage-derived chemokine; Gal-1, galectin-1; PDL,programmed cell death 1 ligand; IFN-�, interferon gamma; NK, natural killer.
Steidl, Connors, and Gascoyne
2 © 2011 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

formation of the microenvironment and highlights how, in return,HRS cells receive signals from the microenvironment through sur-face receptors.
The clinical and pathologic features of HL reflect an abnormalimmune response that is thought to be the result of expression of avariety of cytokines and chemokines by the HRS cells, altering thecomposition and function of the cells in the surrounding microenvi-ronment and shaping the specific histopathologic appearance of thelymph node.8,9 Moreover, the reactive cells in the microenvironmentproduce specific cytokines and chemokines that help maintain andeven amplify the intense inflammatory reaction.10 Table 1 summa-rizes the most commonly described cytokines and chemokines in HLand their main functions. Of note, most of the studies in HL havefocused on NSHL and MCHL, because NLPHL, lymphocyte-rich andlymphocyte-depleted cHL account for only a minority of cases.2 Inaddition to the variability of cytokine expression in the different HLsubtypes, Epstein-Barr virus (EBV) positivity also influences the rela-tive expression of certain cytokines (eg, CXCL10, CXCL9, CCL5,and CCL3).9
COMPOSITION OF THE MICROENVIRONMENT
The most abundant cells found in HL are infiltrating CD4� T cells.58
Several studies have revealed that the main subset of these cells displaysa phenotype of T helper 2 (TH2) and T regulatory (Treg) cells, partic-ularly those in the direct vicinity of HRS cells.13,59 HRS cells secreteregulated upon activation, normal T cell expressed and secreted(CCL5), thymus and activation-related chemokine (CCL17), andmacrophage-derived chemokine (CCL22), potent chemokines thathave all been shown to attract CCR4-expressing TH2 and Treg cells inHL.32,46,47,49-52 CCL5 has also been shown to attract mast cells com-monly found in HL.46 Together with T helper 1 (TH1) cells, HRS cellsthemselves produce interferon gamma,11,15,16 an important enhancerof macrophage function. HRS cells also produce granulocyte colony-stimulating factor (CSF1) and fractalkine (CX3CL1), chemokines anddifferentiation factors of monocytes and their progenitors explainingvariable infiltration by macrophages.40,43,60,61 In general, macro-phages have been shown to be critical enhancers of tumor progression,to promote cell migration, and to suppress antitumor immunity inmany cancers, including lymphoma.62 Particularly in HL, secretion ofmacrophage migration inhibitory factor (MIF) may contribute to theproliferation of HRS cells, which frequently express the CD74 receptoron their surface20,63; CD74 has been previously implicated in signalingand accessory functions for immune cell activation.64 Interleukin (IL)-8 expression by macrophages might also contribute to neutrophilinfiltration, which has been frequently described, most commonlyin NSHL.53,54
Expression of IL-13, tumor necrosis factor (TNF) �, and fibro-blast growth factors by HRS cells has been well described,18,27,41 andthis leads to the activation and proliferation of fibroblasts, most prom-inently seen in NSHL.48,65 Fibroblasts themselves can attract eosino-phils and TH2 cells through secretion of eotaxin (CCL11).48
Furthermore, IL-5 and mucosae-associated epithelial chemokine(CCL28) expression of HRS might contribute to tissue eosino-philia.19,39 CCL28 and CXCL16 have been described as correlated withplasma cell infiltration, a variable feature in cHL.39
B cells of various maturational stages are part of the normalcellular composition of lymph nodes, but in HL, this architecture isdisturbed to varying degrees. Therefore, it remains an open question ifand how reactive B cells are specifically attracted into the microenvi-ronment of HL, or whether they represent remnants not displaced byHL. However, as part of the general inflammatory reaction, variouscytokines, including TNF-� and lymphotoxin �, with effects on B-celldifferentiation, proliferation, and chemotaxis have been shown to beexpressed, which play critical roles in the initiation of germinal centerreactions.21,33,66 In NLPHL, expression of B cell–attracting chemokine1 (CXCL13) has been demonstrated in a subset of cases.67
AUTOCRINE AND PARACRINE RECEPTOR SIGNALING BYHRS CELLS
Although the malignant HRS cells gain a survival advantage by dereg-ulated transcription factor networks and genetic lesions altering in-trinsic signaling, the fully developed proliferation and antiapoptoticphenotype of HRS cells are critically dependent on their interactionwith the microenvironment.68 In HL, the cooperation of direct genetichits in signaling pathways with microenvironment-dependent signal-ing is most evident in the activation of nuclear factor kappa B (NF�B)and Janus kinase–signal transducer and activator of transcription sig-naling (JAK-STAT; Fig 2). Many mutations and structural alterationsin the genes involved in these pathways leading to constitutive activity,including chromosomal gains, overexpression of pathway genes,69-74
and inactivating mutations of tumor suppressor genes have beendescribed.75-82 Moreover, the microenvironment provides signalingvia surface receptors, namely IL receptors,83 members of the TNFreceptor (TNFR) family,84 and receptor tyrosine kinases.85
Prominent receptor family members involved in activation of thecanonical NF�B pathway, including CD30 (TNFR superfamily [SF],member 8), CD40 (TNFRSF5), receptor activator of NF�B(TNFRSF11A), and TNFR1 (TNFRSF1A), have been shown to beexpressed on the surface of HRS cells.29,45,86,87 These receptors can beactivated by membrane-bound or secreted ligands such as receptoractivator of NF�B ligand (TNFSF11, autocrine29), CD30L (TNFSF8,mast cells,30 eosinophils31), CD40L (TNFSF5, TH2/Treg86), TNF-�(autocrine, macrophages and lymphocytes33,34), and lymphotoxin �(autocrine21). Furthermore, in EBV-positive HL, the expression ofviral oncogene LMP1 leads to protein aggregates in the cellular mem-brane mimicking an active CD40 receptor that similarly activatesNF�B signaling.88 Alternative activation (so-called noncanonical acti-vation) of the NF�B pathway can be achieved via the receptors trans-membrane activator and calcium modulator and cyclophilin ligandinteractor (TNFRSF13B) and B-cell maturation antigen (TNFRSF17)after engagement by their ligands a proliferation-inducing ligand(TNFSF13) and B-cell activating factor (TNFSF13B).28,89 Notably, theseligands are expressed not only by HRS cells but also by a variety of cellsin the microenvironment, including macrophages, neutrophils, mastcells, and plasma cells, suggesting a prominent paracrine network.28
The constitutive activity of the Janus kinase–STAT pathway isexemplified by autocrine and paracrine signaling of IL-13, whichengages the IL-13 receptor and leads to HRS cell proliferation andsurvival by phosphorylated STAT6.18,90 Additionally, STAT3 activa-tion through IL-21 and STAT5 activation have been described inHL.91,92 Overall, expression of a large number of ILs that display
Microenvironment in Hodgkin’s Lymphoma
www.jco.org © 2011 by American Society of Clinical Oncology 3Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.
Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

Table 1. Cytokines and Chemokines Involved in the Pathogenesis of Hodgkin’s Lymphoma
NameAlternative
Name Biological Function/Function in Hodgkin’s LymphomaReference
No.
TH1 cytokinesIL-2 Lymphokine T-cell growth factor 11, 12IL-12 — Growth factor for activated T and NK cells 13, 14IFN-� — Macrophage activation, CXCL10 induction 11, 15-17
TH2 cytokinesIL-4 BCGF1 B-cell activation 12, 16IL-5 EDF Eosinophil differentiation 12, 18, 19IL-6 IFNB2 B- and plasma cell activation and maturation 12, 20-22IL-9 P40 Mast cell activation 23, 24IL-10 CSIF Negative regulation of TH1 cytokines 16, 25, 26IL-13 — B-cell maturation and activation, fibroblast stimulation, CCL17 and
CCL22 induction18, 27
TNF receptor ligandsTNFSF13B BAFF B- and HRS cell proliferation and differentiation 28TNFSF11 RANKL Augmentation of T-cell activation by dendritic cells, HRS cell stimulation 29TNFSF13 APRIL B- and HRS cell proliferation and differentiation 19TNFSF8 CD30L T-cell stimulation 30, 31CD40LG TNFSF5 B- and HRS cell proliferation 32LTA TNFSF1 B-cell growth factor, collagen synthesis 21TNF-� TNFSF2 CCL11 production enhancement through fibroblasts, collagen synthesis 33, 34
Other cytokinesIL-1A IL-1� Proinflammatory cytokine, fibrosis and sclerosis induction 33, 35IL-1B IL-1� Fibrosis and sclerosis induction 33, 35TGF-� — B- and T-cell suppression, fibroblast proliferation, associated with
nodular sclerosis subtype26, 36
IL-3 Multi-CSF Growth factor for HRS cells 37, 38IL-7 — Growth factor for B and T cells 39MIF — Blocks cytotoxic T lymphocyte response 40VEGF — Endothelial cell growth, angiogenesis 41, 42CSF1 M-CSF Monocyte growth and differentiation 20, 43, 44CSF2 GM-CSF Granulocyte, macrophage, and eosinophil differentiation 12, 22, 45
ChemokinesCC chemokines (�-chemokines)
CCL1 I-309 Monocyte chemotaxis 32, 39CCL2 MCP-1 Monocyte and basophil chemotaxis 33CCL5 RANTES T-cell, eosinophil, and mast cell recruitment 16, 46, 47CCL11 Eotaxin Eosinophil accumulation, produced by fibroblasts (TNF-� induced) 16, 39, 48CCL13 MCP-4 Monocyte chemotactic protein 14
32CCL17 TARC Induction of TH2 response and regulatory T cells 49-51CCL19 MIP-3� Promotes B- and T-cell migration 32CCL20 MIP-3� Lymphocyte recruitment 32CCL22 MDC TH2 response and regulatory T cell induction 16, 32, 39, 52CCL28 MEC Plasma cell and eosinophil recruitment 39
CXC chemokines (�-chemokines)CXCL8 IL-8 Neutrophil recruitment 53-56CXCL9 MIG Reactive infiltrate in EBV-positive disease 9, 16CXCL10 IP-10 Reactive infiltrate in EBV-positive disease 16, 32, 40, 50CXCL12 SDF1 Monocyte migration stimulation 57CXCL13 BLC B lymphocyte migration 32, 57CXCL16 SRPSOX Recruitment of plasma cells 39
CX3C chemokinesCX3CL1 Fractalkine Chemotactic for T cells, NK cells and monocytes 40
Abbreviations: TH, T helper cell; IL, interleukin; NK, natural killer; IFN-�, interferon gamma; TNF, tumor necrosis factor; TNFSF, TNF superfamily; BAFF, B-cellactivating factor; HRS, Hodgkin Reed-Sternberg; RANKL, receptor activator of nuclear factor kappa B ligand; APRIL, a proliferation-inducing ligand; LTA, lymphotoxinalpha; GM-CSF, granulocyte macrophage colony-stimulating factor; MIF, macrophage migration inhibitory factor; VEGF, vascular endothelial growth factor; MCP,monocyte chemotactic protein; TARC, thymus and activation-related chemokine; MDC, macrophage-derived chemokine; MEC, mucosae-associated epithelialchemokine; MIG, monokine induced by gamma interferon; EBV, Epstein-Barr virus; IP-10, 10KDa interferon gamma-induced protein; SDF, stromal cell–derivedfactor; BLC, B lymphocyte chemoattractant; SRPSOX, scavenger receptor for phospatidylserine and oxidised low-density lipoprotein.
Steidl, Connors, and Gascoyne
4 © 2011 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

receptor-specific binding similar to that seen with IL-13 has beenreported in HL8,93 (Table 1), including ligands binding to IL-2 recep-tor complexes94,95 and the IL-3,37,38 IL-6,12,96 and IL-7 receptors.97
Recently, receptor tyrosine kinase signaling has been reported toplay an important role in the pathogenesis of HL. In particular, the
surface receptors mesenchymal-epithelial transition factor (c-MET),tyrosine receptor kinase A (TRKA), and discoidin domain receptortyrosine kinase 2 (DDR2) are expressed and mediate survival signalingin HRS cells through paracrine signaling.98-102 The respective ligandsof these receptors are thought to be produced by cells of the
RANK
CD40 TNFR1/2
CD30 BCMA TACI
DDR2
collagen type I
TRKA
NGFBAFFAPRIL
CD40LCD30LRANKL
c-MET
HGF
Canonical NFκB Alternative NFκB Tyrosine receptor kinases
IL-2RIL-3RIL-6RIL-7RIL-13R
STAT-3
STAT-6
IL-4, IL13
JAK-STAT signaling
IL-6, IL-10IL-2, IL-7, IL-9, IL-15IL-3, IL-5, GM-CSF
STAT-5
TNF-αLT-α
NFκB complex
I
c M
RIP
IKKβ
NEMOIKKα
TRAF
IκB complex
MAP3K14
IKKαIKKβ
Transcriptional regulation:
Proteasomal
- Inflammation- Cell proliferation
- Survival- Differentiation
degradation
TRAF
STAT
STAT
STAT dimers/oligomers
STAT STAT
JAK1JAK2JAK3TYK2
STATSTAT
Apoptosis, cell cycle control,protein synthesis, DNA damage repair
IKK complex
IκBαIκBε
p50 RELAp52 RELB
p100 RELB
P
P
PP
Januskinase
P
P
RAS
RAF
MEK
ERK
SHP2
SOS
GAB1
PDK
AKT
p21MDM2 mTOR
PI3KGRB2
BAD
Fig 2. Pathway activation in Hodgkin Reed-Sternberg cells through signaling from the microenvironment. Soluble and membrane-bound signaling molecules producedby reactive cells (paracrine activation) activate the Janus kinase–signal transducer and activator of transcription signaling (JAK-STAT) and canonical and alternativenuclear factor kappa B (NF�B) pathways and receptor tyrosine kinases. For the JAK-STAT signaling pathway, the most commonly expressed interleukins (ILs), ILreceptors, and activated STATs are shown. For the NF�B pathway, only the principal activation cascades are shown, and inhibitor of � kinase (I�K) complex activationby other kinases are described. Downstream signaling of receptor tyrosine kinases is shown using the example of tyrosine kinase receptor A (TRKA) and illustratingthe Ras and Akt pathways; other signal transduction pathways exist. GM-CSF, granulocyte macrophage colony-stimulating factor; RANKL, receptor activator of NF�Bligand; TNF-�, tumor necrosis factor �; LT-�, lymphotoxin �; APRIL, a proliferation-inducing ligand; BAFF, B-cell activating factor; HGF, hepatocyte growth factor; NGF,nerve growth factor; TACI, transmembrane activator and CAML interactor; BCMA, B-cell maturation antigen; c-MET, mesenchymal-epithelial transition factor; DDR,discoidin domain receptor tyrosine kinase; TYK2, tyrosine kinase 2; RIP, receptor-interacting protein; TRAF, TNF receptor–associated factor 1; MAP3K, mitogen-activated protein 3 kinase; SHP2, Src homology 2 domain–containing tyrosine phosphatase; SOS, son of sevenless homolog 1 (Drosophila); GRB2, growth factorreceptor–bound protein 2; PI3K, phosphoinositide 3-kinase; ERK, extracellular signal-regulated kinase; MEK, MAP-ERK kinase; PDK, 3-phosphoinositide–dependantprotein kinase; BAD, BCL2-associated agonist of cell death; MDM, mouse double minute; mTOR, mechanistic target of rapamycin.
Microenvironment in Hodgkin’s Lymphoma
www.jco.org © 2011 by American Society of Clinical Oncology 5Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.
Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

microenvironment. Hepatocyte growth factor (HGF), a specific li-gand of c-MET, is expressed by CD21� follicular dendritic cells.99
Collagen type I, the high-affinity ligand of TRKA, is expressed byfibroblasts, and nerve growth factor (NGF) –producing granulocyteswere found abundantly in the direct vicinity of HRS cells.100 Further-more, autocrine activation loops have been suggested for the platelet-derived growth factor receptor (PDGFRA) and EPH receptor B1(EPHB1). In summary, cytokine and chemokine expression have beenextensively studied in HL, and specific ligand-receptor interactionshelp explain the composition of the tumor environment and down-stream receptor signaling critically influencing the phenotype of ma-lignant cells.
IMMUNE ESCAPE BY HRS CELLS
As discussed, HRS cells are dependent on the extensive inflammatorymicroenvironment and use receptor signaling pathways to maintaintheir high proliferative capacity and antiapoptotic phenotype. How-ever, HRS cells also appear to orchestrate their microenvironment inmany ways to evade host immune attack. As evidenced in HIV-associated HL, malignant cells can thrive in an environment in whichhost immunity is globally impaired.103 Moreover, in recent years,specific mechanisms have been uncovered detailing how HRS cellsinduce a favorable microenvironment with suppressed antitumor im-mune activity.
Major advances have been made that characterize the pheno-types and functions of specific T-cell subsets,104 including immuno-suppressive Treg cells, which are abundant in tissue biopsies ofHL.105,106 Specifically, it has been shown that HRS cells producechemokines such as CCL5, CCL17, and CCL22, which attract TH2and Treg cells49,52,107 and secrete IL-7, an IL capable of inducingdifferentiation of CD4�naive T cells toward FOXP3�Treg cells.97,108
Treg and HRS cells themselves produce IL-10 and transforminggrowth factor � (TGF-�), which exert inhibitory effects on T-celleffector functions, especially on cytotoxic T lymphocytes(CTLs).8,25,105,109 In addition, prostaglandin E2 (PGE2) has been im-plicated as a contributor to immunosuppression and pathogenesis ofHL110,111 similar to cancer progression of solid tumors.112 PGE2 leadsto decreased CD4� T-cell activation through inhibition of leukocyte-specific protein tyrosine kinase (LCK),113 suggesting that PGE2 con-tributes to the CD4� T-cell impairment observed in HL. The cellsproducing PGE2 have yet to be determined.
Another important mechanism by which HRS cells evade hostimmune response is by overexpression of surface molecules maintain-ing peripheral tolerance. For example, the overexpression of Fas ligand(CD95L) that has been described in virtually all HRS cells of NS andMC subtypes114-116 induces apoptosis in tumor-specific CTLs.117
Similarly, galectin-1 (LGLAS1) was found to be overexpressed on thesurface of HRS cells in HL, correlating with a reduced CD8� infiltra-tion at the tumor site.118 In cocultures of activated T cells with HL celllines, galectin-1 induced secretion of TH2 cytokines and expansion ofTreg cells, whereas knockdown of galectin-1 increased overall T-cellviability and restored the TH1/TH2 balance.119 Furthermore, overex-pression of ligands of the receptor molecule programmed cell death 1(PD1), PD1 ligand 1 (PDL1; CD274) itself, and PDL2 (CD273) hasbeen described in HL.120,121 PD1 belongs to the CD28 costimulatoryreceptor superfamily expressed on CTLs and can modify T-cell activ-
ity by providing a second signal to T cells via the PD1 receptor, inconjunction with signaling through the T-cell receptor.122 In the set-ting of HL, PD1 ligand overexpression has been shown to contributeto the T-cell exhaustion observed in infiltrating T cells. A recent studyestablished a link between copy number gains of chromosome 9pwhere PDL1 and PDL2 reside and overexpression of these moleculesin NSHL.121
Loss of HLA class I and II molecules on the surface of HRS cellsoccurs in a substantial proportion of cases and is correlated with latentEBV infection. HRS cell escape from immune surveillance has beensuggested as a functional consequence of this finding,123-125 becausethe reduced immunogenicity of HRS cells could impair activation ofCTLs (major histocompatibility complex [MHC] class I recognition)and CD4� T cells (MHC class II recognition). However, the under-lying causes for this downregulation of HLA molecules and the exactfunctional consequences are largely unexplored in HL. In particular,no correlation between chromosomal loss and underexpression ofHLA molecules has been found in two HL cell lines.126 Interestingly,certain HLA types are correlated with genetic susceptibility to HL—EBV-positive HL cases in particular—suggesting that certain poly-morphisms might effect antigen presentation to CTLs.127-129
Furthermore, expression of the nonclassical MHC class I gene HLA-G,the ligand for inhibitory receptors found on natural killer (NK) cells,subsets of T cells, and other immune cells may lead to evasion ofNK-cell and CTL-mediated immune responses and has been impli-cated in the pathogenesis of HL.130 Such surface expression has beenidentified by immunohistochemistry (IHC) in more than half of cHLcases, and a strong correlation with absence of classical MHC class Imolecule expression and EBV-negative status has been seen.
In summary, it is now well established that the phenotypicchanges that characterize HRS cells allow for efficient escape from thehost immune attack through various mechanisms, including release ofchemokines shaping an immunosuppressive microenvironment aswell as the expression of surface molecules gaining immune privilegethrough the reduction of HRS cell immunogenicity. However, most ofthe underlying genetic mechanisms remain to be discovered.
BIOMARKERS IN HL: CORRELATIONS TO TREATMENT OUTCOME
As the impact of the microenvironment on the specific pathobiologyof HL becomes increasingly clear, more and more work is focused oncorrelation of biomarkers with treatment outcome. Although treat-ment regimens have been remarkably stable in the last two decades,specific aspects of patient selection, varying histologies, and treat-ments might influence cross-comparability and in part explain differ-ing conclusions from these studies. In general, although a plethora ofbiomarkers associated with clinical outcome have been described,none of these factors has influenced clinical practice to date. The mainreason for this unsuccessful clinical translation lies in the lack ofreproducibility between independent patient cohorts and prognosticimplications that are not of significant magnitude to justify a change inclinical management. For individual biomarkers, reproducibility ofIHC scoring has been suggested as a reason for inconclusive results,and thus more robust multigene predictors have been reported basedon expression profiling.131,132 Table 2 summarizes some of thebiomarkers for which outcome correlations have been described, sep-arated into studies using IHC and gene expression profiling. The focus
Steidl, Connors, and Gascoyne
6 © 2011 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

of these studies has been cHL, because there are no biologic markersyet identified that can predict treatment outcome or transformation toan aggressive lymphoma in patients with NLPHL.
HISTOPATHOLOGY
The first biomarker studies in cHL used classical histopathologic ap-proaches to describe the specific cellular composition of subtypes andinvestigate correlations with treatment outcome. Although in initialreports, the rare lymphocyte-depleted subtype and grade 2 nodularsclerosis were reported to be associated with poor response to initialtherapy and decreased survival,149 there is now overwhelming evi-dence that none of the cHL subtypes are correlated with survival usingmodern treatment modalities.133,150-152 Similarly, the number of HRScells is not prognostically relevant. Tissue eosinophilia is still a subjectof debate; a large study investigating diagnostic biopsies found a strong
correlation between the presence of eosinophils and freedom fromtreatment failure and overall survival (OS),31 in agreement with areport showing prolonged disease-free survival in patients with heavyeosinophilic infiltration in NSHL.153 However, several other studiescould not confirm this finding.150,154,155 Mast cell infiltration has alsobeen linked to poor prognosis in cHL,156 and a recent study usingc-kit/CD117 IHC was able to link the number of mast cells to unfa-vorable outcome after primary therapy157; however, these data haveyet to be validated. These factors affecting HRS cells and the microen-vironment as assessed by routine histopathology are of interest. How-ever, none has yet had an impact on clinical practice.
MACROPHAGES
Some of the first biomarker studies in the modern treatment era wereconducted in the 1980s and suggested that increased numbers of
Table 2. Biomarkers With Outcome Correlations Described in the Literature
Immunohistochemistry
Marker/Signature Expressed on/Staining Pattern Function Outcome CorrelationReference
No.
Granzyme B Cytotoxic T cells Target cell lysis Adverse (PFS, OS) 133-137TIA-1 Cytotoxic T cells Target cell lysis Adverse (EFS, OS) 136,138FOXP3 Regulatory T cells Transcriptional regulation Favorable (EFS) 137-139CD20 Background B cells B-cell differentiation Favorable (OS, EFS) 132,140BCL11A Background B cells, plasmacytoid dendritic
cellsTranscriptional regulation Favorable (OS, EFS) 140
HLA-DR HRS cells Antigen presentationCD68, PNA Macrophages Scavenger receptor Favorable (FFS) 123ALDH1A1 Macrophages Oxidative
pathway/metabolismAdverse (PFS, DSS) 132,141
STAT1 Macrophages Transcriptional activation Adverse (DSS) 142EBV-encoded small RNAs HRS cells Activation of NF�B Adverse in elderly patients,
favorable in youngpatients (FFS, OS)
143-147
MMP11 HRS cells, macrophages, endothelial cells,extracellular
Tissue remodeling Adverse (PFS) 132
Gene Expression Profiling
Main Gene Components Outcome Correlation Reference No.
Angiogenic signature ADH1B, CD93, SRPX, PLA2G2A, GPR126 Adverse (primary treatment failure) 132Adipocyte signature GLUL, MGST1, COL1A2, FABP4 Adverse (primary treatment failure) 132Fibroblast function/extracellular
matrix remodelingAdverse: MMP2, MMP3, TIMP1, COL1A1,
COL4A1, COL4A2, COL5A1, COL18A1,COL16A1, MFAP2, THBS1/2, FN1,EDNRA, ITGB5, LAMA4; favorable:TIMP4, SPON1, LAMB1, TACR1, CCL26
Discordant: adverse/favorable(primary treatment outcome)
142,148
B-cell signature BCL11A, BANK1, STAP1, BLNK, FCER2,CD24, CCL21
Favorable (primary treatmentoutcome)
132,140
Cytotoxic T-cell signature CD3D, CD8B1, CTSL, CD26, SH2D1A,IFI16, RGS13, CR2, ELL3, CCDC23,PPM1L, TRA@, PIK3CA
Adverse (primary treatmentoutcome)
131,132,142
Plasmacytoid dendritic cells ITM2A, SRPX, CTSB, APP Adverse (primary treatmentoutcome)
132
Macrophage signature ALDH1A1, LYZ, STAT1, ITGA4, CCL13,MS4A4A, CCL23, VCAN, HSP90AB3P,HSP90AB1, CTSB, CFL1, JMJD6,MAPK7, IKBKG, RAB7A, RXRA,MAPK13
Adverse (primary treatmentoutcome)
131,132,142
Abbreviations: PFS, progression-free survival; OS, overall survival; TIA-1, T-cell–restricted intracellular antigen 1; EFS, event-free survival; FOXP3, forkhead boxprotein 3; BCL11A, B-cell lymphoma/leukemia 11A; HRS, Hodgkin Reed-Sternberg; FFS, failure-free survival; PNA, peanut agglutinin; DSS, disease-specific survival;ALDH1A1, aldehyde dehydrogenase 1A1; STAT, signal transducer and activator of transcription signaling; EBV, Epstein-Barr virus; NF�B, nuclear factor kappa B;MMP11, matrix metalloproteinase 11.
Microenvironment in Hodgkin’s Lymphoma
www.jco.org © 2011 by American Society of Clinical Oncology 7Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.
Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

macrophages, as measured using peanut agglutinin–binding cells,were associated with more frequent constitutional symptoms andrelapse.141,158 The association of macrophages with adverse treatmentoutcome has now been confirmed in an increasing number of patientcohorts. In a gene expression profiling study investigating the mi-croenvironment, the authors found several genes expressed by mac-rophages, including STAT1 and ALDH1A1, to be significantlycorrelated with disease-specific survival when investigated by IHC.142
The importance of these markers was also confirmed in an indepen-dent patient cohort using quantitative reverse-transcriptase polymer-ase chain reaction from archival paraffin material.131 However, it wasnot confirmed in a second study by the same group, in which theauthors found a correlation of the macrophage activation genes LYZand STAT1 with favorable outcome.159 Most recently, tumor tissuesignatures of monocytes and tumor-associated macrophages werefound by gene expression profiling in patients with therapy-refractorydisease or relapse when compared with patients who sustained long-term remissions.132 Most importantly, in independent validation ex-periments, the authors demonstrated that the enumeration of CD68�macrophages in lymph node biopsies was a strong and independentpredictor of disease-specific survival. These data are encouraging; inthis study, it could be demonstrated that the number of CD68�macrophages was also significantly associated with the outcome ofsecondary treatments such as autologous stem-cell transplanta-tion. Overall, the adverse prognostic impact of tumor-associatedmacrophages in cHL biopsies can now be considered as firmlyestablished in patients treated with doxorubicin, bleomycin, vin-blastine, and dacarbazine (ABVD) or ABVD-like chemotherapyregimens. The correlation of tumor-associated macrophages withadverse clinical course and tumor progression has also been re-ported in follicular lymphoma160 and many other solid tumors inwhich macrophages stimulate tumor growth, angiogenesis, tumorcell migration, and invasion.62
T-CELL SUBSETS
Another biomarker in the microenvironment of HL was described byOudejans et al,134 who found that an increased number of activatedCTLs in tissue biopsies of patients was associated with unfavorableclinical outcome. The authors used granzyme B (GrB) as an IHCmarker and found GrB-expressing cells in the vast majority of patients,but they showed that patients with more than 15% GrB� cells hadsignificantly shorter progression-free survival and OS. In a subsequentstudy of 83 patients with cHL using GrB IHC, this same factor wasfound to correlate with OS and to be independent of both age andstage in multivariate analysis.135 Several subsequent studies by inde-pendent groups validated these initial studies of CTLs as useful predic-tors of prognosis in cHL but also identified other T-cell subsetsassociated with treatment outcome.133,135-138,157,161 Despite this ear-lier work, the most useful T-cell marker combination for determiningprognosis using IHC is still a subject of debate. In a large series of 257patients with cHL represented on a tissue microarray, the number ofFOXP3� Treg cells correlated with prolonged event- and disease-freesurvival, and the authors were able to validate the negative prognosticimpact of CTLs.138 However, in this study, TIA-1—another cytotoxicgranule marker—was used to enumerate CTLs, and the number ofGrB-activated CTLs was not significantly associated with poor prog-
nosis. Accordingly, high ratios of FOXP3�/TIA-1� T cells138 wereassociated with favorable event- and disease-free survival and OS,whereas high ratios of FOXP3�/GrB� cells137 were shown to beassociated with favorable failure-free survival and OS. The correlationof high numbers of intratumoral FOXP3� regulatory cells with OSand failure-free survival was validated in a subsequent study.139 Incontrast, high numbers of regulatory T cells have mostly been reportedto be associated with unfavorable outcome in various solid tumors.162
The reason for these unexpected findings remains unclear. In anattempt to link T-cell infiltration to the specific biology of HRS cells,the prognostically favorable low number of cytotoxic cells (CD8� Tlymphocytes, CD57� NK cells, and GrB� cells) was linked to over-expression of antiapoptotic proteins in HRS cells.163 Interestingly,recent work has shown that lack of HLA class II cell-surface expressionon HRS cells was frequently observed, and this finding was associatedwith EBV-negative disease status, HLA class I loss, and adverse out-come in multivariate analysis.123 However, because loss of HLA class IIlikely leads to diminished activation of TH1 cells and thereby a re-duced cytotoxic antitumor response, the exact functional mechanismsremain to be clarified linking increased numbers of intratumoralCTLs with unfavorable outcome.
Furthermore, signatures of cytotoxic T cells have been identifiedusing gene expression profiling, suggesting that overexpression ofcertain T-cell activation genes such as CD8B1, CD3D, CTSL, CD26,and SH2D1A might be correlated with inferior outcome.131,132,142
Additional biomarker studies investigating the prognostic impact ofT-cell subsets together with tumor-associated macrophages are antic-ipated to address the question of whether combinations of IHC mark-ers with well-established clinical risk factors might further improve thepredictive value of a single biomarker alone.
BACKGROUND B CELLS
Recently, the number of CD20� background B cells was reported tobe significantly associated with treatment outcome in two indepen-dent studies.132,140 Both studies found an overrepresentation of signa-tures of benign B cells in diagnostic biopsies of patients whose primarytreatments were successful and were able to demonstrate using CD20IHC significant correlations with OS and disease-specific survival,respectively. Although in one study the prognostic impact of thenumber of CD20� background B cells on OS was independent ofclinical parameters,140 the second study found a strong correlation ofCD20� cells with clinical stage.72 Interestingly, another marker ex-pressed on B cells—BCL11A—was an even better predictor for OS,possibly because of an association of BCL11A� plasmacytoid den-dritic cells with favorable outcome.
FOLLICULAR DENDRITIC CELLS
The presence and distribution of follicular dendritic cells (FDCs)have been studied in both cHL and NLPHL using IHC.164,165 Thesestudies reveal the close spatial relationship of HRS and LP cells with theFDC network. In one study of cHL, the authors reported a correlationbetween the absence of FDCs and unfavorable outcome.166 In afollow-up study, the association with outcome was validated, but onlyin the context of certain patterns of CD21� FDC staining.167 The
Steidl, Connors, and Gascoyne
8 © 2011 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

longest OS was observed in patients with well-defined follicle-likestructures compared with visible but largely destroyed FDC mesh-works (intermediate survival) and absence of FDCs (poor survival).These data suggest that not only the number of FDCs but also the levelof destruction of normal lymph node architecture might be an impor-tant variable for outcome prediction.
EBV ASSOCIATION
EBV infection of HRS cells occurs in up to 60% of patients in somestudies but varies with geographic location, age, sex, clinical stage,and histologic type.168 Recent gene expression profiling data haveshed more light on immune-related cells in EBV-positive versusEBV-negative disease, specifically identifying a TH1/antiviral re-sponse in EBV-positive patients.140 Furthermore, an increasednumber of cytotoxic T cells has been linked to EBV positivity.134
The impact of EBV infection on outcome is controversial, withsome studies showing no impact150,169 and others favorable143,170 orunfavorable outcomes.144,145 These discrepancies might result in partfrom patient selection and confounding differences in demographicfactors, because there is an increasing body of work supporting anassociation between EBV positivity and adverse outcome in olderadult patients144-146 and a favorable effect in younger, specificallypediatric, patients.143,144,147 Additional studies might clarify the clini-cal value of these findings; the apparent age dependence has hamperedthe translation of EBV status into a widely used biomarker.
SERUM MARKERS
It has been shown that certain cytokines, chemokines, and othersoluble factors are detectable in the sera of patients with HL, andmultiple studies have focused on the negative prognostic impact ofthese molecules.17,171,172 In general, increased levels of these serummarkers can be interpreted as surrogates for active crosstalk betweenHRS cells and their microenvironment. Characteristically, many ofthose markers, including sCD30, serum IL-2 receptor, solubleintercellular adhesion molecule (sCD54), and vascular cell adhe-sion molecule 1 (sCD106), have shown correlations to one an-other, and elevated levels have been reported to be associated withadvanced tumor stage and unfavorable prognosis.173-176 Althoughall these markers have shown prognostic significance, their inde-pendent value in comparison with the established clinical surro-gate markers for tumor burden and disease activity has not beenconvincingly demonstrated.
GENOME-WIDE STUDIES
Gene expression profiling studies have contributed substantially toimproved understanding of the disease with respect to the inherentphenotypic features of malignant HRS cells177,178 and the specificcomposition of the microenvironment.132,140,142,148 Using the un-biased approach of transcriptome-wide gene expression profiling,gene signatures have been identified that correlate with failure orsuccess after primary treatments. Many of these signatures can berelated to cellular compartments represented in whole-tissue biop-sies. Some of these signatures have been subsequently validated by
IHC, including tissue-associated macrophages, background reac-tive B cells, and CTLs132,140,142; however, confirmation is stillneeded for others (Table 2). Of note, the prognostic implications ofangiogenesis, adipoctyes, and dendritic cells have been studied inother lymphomas.179-181
Proteomic studies have recently been performed in HL. Twoapproaches have been chosen thus far, one using total cell lysates,the other studying the secretome of HRS cells.40,182,183 These stud-ies have demonstrated the potential value for developing noveldiagnostic tools by identifying specific profiles linked to certainlymphoma entities and have helped to characterize secreted pro-teins that are critically involved in the crosstalk of HRS cells withtheir microenvironment.40 However, no outcome correlationshave been described to date.
Only one study has investigated correlations of a micro-RNAprofile, which was previously found in HL,184 with outcome. Theauthors found that miR-135a expression was associated with a higherprobability of relapse and shorter disease-free survival.185
THERAPEUTIC APPROACHES TARGETING THETUMOR MICROENVIRONMENT
Although HL is overall a successfully treated disease, treatment failurein a substantial proportion of patients and treatment-related early andlate sequelae of chemotherapy and radiotherapy underscore the needfor novel therapeutic approaches, especially for relapsed HL. No newdrugs have been approved for HL in the past two decades186; however,many agents are being tested in preclinical studies and currently en-rolling active trials. Table 3 lists a selection of novel therapeutic agentsin HL that are thought to target reactive cells in the microenvironmentor surface receptors on the malignant cells or to interfere with down-stream receptor signaling.
The concept that the tumor microenvironment might be apromising therapeutic target has been reinforced by reports in re-lapsed HL about the efficacy of the pyrimidine analog gemcitabine,210
a cytotoxic agent that has been reported to specifically target Tregcells.211 Furthermore, the results of a study combining the anti-CD20monoclonal antibody rituximab with gemcitabine in relapsed HL areencouraging and suggest that a combined treatment targeting reactiveB and T cells in the microenvironment might be an effective ap-proach.188 Trials targeting CD20� B cells using radioimmunoconju-gates have been initiated.191 However, it remains controversial if theefficacy of anti-CD20 immunotherapy results from the direct killing ofHRS cells that do occasionally express CD20212 or from the depletionof HRS cell–supporting reactive B cells in the microenvironment.187
Of note, two gene expression profiling studies have observed a corre-lation between increased numbers of background B cells and favorableprognosis, a finding that needs further clarification in the context ofrituximab treatment.132,140 Support for a direct effect on HRS cells alsocomes from a recent study suggesting that HRS progenitor cells mightexpress CD20 on their surface and could be eradicated by ritux-imab.213 Unequivocally, treatment effects in NLPHL have been attrib-uted to a direct effect on the CD20-expressing LP cells.189,190 Otherantibodies with a predominant effect on the microenvironment thatare currently being tested in clinical trials including patients with HLare represented by alemtuzumab (anti CD52)193 and galiximab (anti-CD80).192 Furthermore, immunotherapy with EBV-specific cytotoxic
Microenvironment in Hodgkin’s Lymphoma
www.jco.org © 2011 by American Society of Clinical Oncology 9Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.
Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

effector cells has shown promising results, providing proof of princi-ple for adoptive immunotherapy with ex vivo expanded viral antigen-specific T cells.208 Remarkably, in a subsequent study, five of sixpatients with relapsed HL had a tumor response; of these five, fourachieved complete remissions that were sustained for more than9 months.209
Because of the increased expression of members of the TNFreceptor family and the dependence of malignant cells on TNFreceptor downstream signaling, these molecules are consideredideal targets for specific agents in HL. TNFRSF8 (CD30) in partic-ular has been the target of a number of preclinical and clinicalstudies, of which the anti-CD30 compounds SGN-30 andMDX060 can be considered representative but disappointing inphase I/II clinical trials194,214 because of limited efficacy in relapseddisease. However, using an alternative strategy of conjugating ananti-CD30 antibody with the cytotoxic antimicrotubule agentmonomethyl auristatin E (ie, SGN-35 or brentuximab vedotin),195
much higher partial and complete remission rates were achieved.196 Itis noteworthy that in a heavily pretreated patient cohort, tumorreductions were documented in more than 80% of patients. As aresult, additional clinical trials with brentuximab vedotin as a
single agent and in combination with ABVD are currently recruit-ing. An anti-CD40 (TNFRSF5) antibody (HCD122198) trial and astudy of the combination bortezomib with agonistic anti–TNF-related apoptosis-inducing ligand receptor 2 (TNFRSF10B) com-pound AMG655197 are enrolling patients with HL; however, resultsare still pending. A number of novel drugs have downstream re-ceptor signaling as their primary targets, of which everolimus(mammalian target of rapamycin, phosphoinositide 3-kinasepathway),199 bortezomib (TNFR signaling, NF�B pathway),200
and vorinostat (STAT6, IL signaling)204 have shown promisingpreclinical results. Of these, however, bortezomib as a single agentin relapsed HL had low clinical efficacy.202 Combination therapiesare now being tested.
In summary, therapies targeting cells in the microenvironmentor disrupting microenvironment-dependent signaling in the malig-nant cells seem to be effective and show promise in patients withrelapsed HL. Current clinical trials are also focusing on combinationtherapies with classical chemotherapy agents. Randomized trials com-paring these novel agents with the current standard of care for first-and second-line therapies will ultimately determine their significancein the overall landscape of HL treatment.
Table 3. Selected Therapeutic Agents in Hodgkin’s Lymphoma and Their Presumed Targets
Drug Main Target Reference No./Clinical Trial No.
Cellular targets in microenvironmentRituximab CD20� B cells 187-190
CD20� HRS cells (LP cells)131�I�tositumomab CD20� B cells NCT00484874
CD20� HRS cells (LP cells)90�Y�ibritumomab tiuxetan CD20� B cells 191
CD20� HRS cells (LP cells)Galiximab CD80� B cells, follicular dendritic cells, HRS cells 192
NCT00516217Alemtuzumab CD52� cells in microenvironment 193
NCT01030900Receptor signaling on HRS cells
MDX-060 CD30� HRS cells 194NCT00284804
SGN-35 CD30� HRS cells 195,196NCT00947856, NCT01100502, NCT01060904
AMG655 TNFRSF10B (TRAIL-R2) on HRS cells 197NCT00791011
HCD122 CD40� HRS cells, TH2/Treg signaling 198NCT00670592
Downstream signalingEverolimus TNFR signaling: PI3K, mTOR 199
NCT00967044Bortezomib NF�B signaling: inhibition of degradation of I�B 200-202
NCT00439361Vorinostat Histone modification, JAK-STAT signaling (pSTAT6) 203,204Panobinostat Histone modification 205
NCT00742027Other
Lenalidomide Immunomodulation, anti-angiogenic 206,207NCT00540007
Cytotoxic T lymphocytes EBV-positive disease: viral LMP2 208,209
NOTE. US Food and Drug Administration clinical trail numbers according to http://clinicaltrials.gov.Abbreviations: HRS, Hodgkin Reed-Sternberg; LP, lymphocyte predominant; TNFRSF, tumor necrosis factor receptor superfamily; TH, T helper cell; Treg, T
regulatory cell; PI3K, phosphoinositide 3-kinase; mTOR, mechanistic target of rapamycin; NF�B, nuclear factor kappa B; I�B, inhibitory kappa B; JAK-STAT, Januskinase–signal transducer and activator of transcription signaling; EBV, Epstein-Barr virus; LMP2, latent membrane protein 2.
Steidl, Connors, and Gascoyne
10 © 2011 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTSOF INTEREST
The author(s) indicated no potential conflicts of interest.
AUTHOR CONTRIBUTIONS
Manuscript writing: All authorsFinal approval of manuscript: All authors
REFERENCES
1. Horner MJ, Ries LAG, Krapcho M, et al (eds):SEER Cancer Statistics Review, 1975-2006, Na-tional Cancer Institute. http://seer.cancer.gov/csr/1975_2006/
2. Swerdlow SH, Campo E, Harris NL, et al(eds): WHO Classification of Tumours of Haemato-poietic and Lymphoid Tissues. Lyon, France, Inter-national Agency for Research on Cancer, 2008
3. Pileri SA, Ascani S, Leoncini L, et al: Hodg-kin’s lymphoma: The pathologist’s viewpoint. J ClinPathol 55:162-176, 2002
4. Diehl V, Stein H, Hummel M, et al: Hodgkin’slymphoma: Biology and treatment strategies forprimary, refractory, and relapsed disease. Hematol-ogy Am Soc Hematol Educ Program 225-247, 2003
5. Hasenclever D, Diehl V: A prognostic scorefor advanced Hodgkin’s disease: International Prog-nostic Factors Project on Advanced Hodgkin’s Dis-ease. N Engl J Med 339:1506-1514, 1998
6. Engert A, Plutschow A, Eich HT, et al:Reduced treatment intensity in patients with early-stage Hodgkin’s lymphoma. N Engl J Med 363:640-652, 2010
7. DeVita VT Jr, Costa J: Toward a personalizedtreatment of Hodgkin’s disease. N Engl J Med362:942-943, 2010
8. Skinnider BF, Mak TW: The role of cytokinesin classical Hodgkin lymphoma. Blood 99:4283-4297, 2002
9. Teruya-Feldstein J, Tosato G, Jaffe ES: Therole of chemokines in Hodgkin’s disease. Leuk Lym-phoma 38:363-371, 2000
10. Khan G: Epstein-Barr virus, cytokines, andinflammation: A cocktail for the pathogenesis ofHodgkin’s lymphoma? Exp Hematol 34:399-406,2006
11. Dukers DF, Jaspars LH, Vos W, et al: Quan-titative immunohistochemical analysis of cytokineprofiles in Epstein-Barr virus-positive and -negativecases of Hodgkin’s disease. J Pathol 190:143-149,2000
12. Klein S, Jucker M, Diehl V, et al: Productionof multiple cytokines by Hodgkin’s disease derivedcell lines. Hematol Oncol 10:319-329, 1992
13. Ma Y, Visser L, Blokzijl T, et al: TheCD4�CD26� T-cell population in classical Hodgkin’slymphoma displays a distinctive regulatory T-cell pro-file. Lab Invest 88:482-490, 2008
14. Schwaller J, Tobler A, Niklaus G, et al:Interleukin-12 expression in human lymphomas andnonneoplastic lymphoid disorders. Blood 85:2182-2188, 1995
15. Gerdes J, Kretschmer C, Zahn G, et al:Immunoenzymatic assessment of interferon-gamma inHodgkin and Sternberg-Reed cells. Cytokine 2:307-310, 1990
16. Teruya-Feldstein J, Jaffe ES, Burd PR, et al:Differential chemokine expression in tissues in-volved by Hodgkin’s disease: Direct correlation ofeotaxin expression and tissue eosinophilia. Blood93:2463-2470, 1999
17. Kurzrock R, Redman J, Cabanillas F, et al:Serum interleukin 6 levels are elevated in lymphomapatients and correlate with survival in advanced
Hodgkin’s disease and with B symptoms. CancerRes 53:2118-2122, 1993
18. Kapp U, Yeh WC, Patterson B, et al: Interleu-kin 13 is secreted by and stimulates the growth ofHodgkin and Reed-Sternberg cells. J Exp Med 189:1939-1946, 1999
19. Samoszuk M, Nansen L: Detection ofinterleukin-5 messenger RNA in Reed-Sternbergcells of Hodgkin’s disease with eosinophilia. Blood75:13-16, 1990
20. Hsu SM, Hsu PL: The nature of Reed-Sternberg cells: Phenotype, genotype, and otherproperties. Crit Rev Oncog 5:213-245, 1994
21. Foss HD, Herbst H, Oelmann E, et al: Lym-photoxin, tumour necrosis factor and interleukin-6gene transcripts are present in Hodgkin and Reed-Sternberg cells of most Hodgkin’s disease cases.Br J Haematol 84:627-635, 1993
22. Merz H, Fliedner A, Orscheschek K, et al:Cytokine expression in T-cell lymphomas and Hodg-kin’s disease: Its possible implication in autocrine orparacrine production as a potential basis for neoplas-tic growth. Am J Pathol 139:1173-1180, 1991
23. Merz H, Houssiau FA, Orscheschek K, et al:Interleukin-9 expression in human malignant lym-phomas: Unique association with Hodgkin’s diseaseand large cell anaplastic lymphoma. Blood 78:1311-1317, 1991
24. Glimelius I, Edstrom A, Amini RM, et al: IL-9expression contributes to the cellular composition inHodgkin lymphoma. Eur J Haematol 76:278-283,2006
25. Herbst H, Foss HD, Samol J, et al: Frequentexpression of interleukin-10 by Epstein-Barr virus-harboring tumor cells of Hodgkin’s disease. Blood87:2918-2929, 1996
26. Atayar C, Poppema S, Blokzijl T, et al: Ex-pression of the T-cell transcription factors, GATA-3and T-bet, in the neoplastic cells of Hodgkin lympho-mas. Am J Pathol 166:127-134, 2005
27. Skinnider BF, Elia AJ, Gascoyne RD, et al:Interleukin 13 and interleukin 13 receptor are fre-quently expressed by Hodgkin and Reed-Sternbergcells of Hodgkin lymphoma. Blood 97:250-255, 2001
28. Chiu A, Xu W, He B, et al: Hodgkin lym-phoma cells express TACI and BCMA receptors andgenerate survival and proliferation signals in re-sponse to BAFF and APRIL. Blood 109:729-739,2007
29. Fiumara P, Snell V, Li Y, et al: Functionalexpression of receptor activator of nuclear factorkappaB in Hodgkin disease cell lines. Blood 98:2784-2790, 2001
30. Molin D, Fischer M, Xiang Z, et al: Mast cellsexpress functional CD30 ligand and are the predom-inant CD30L-positive cells in Hodgkin’s disease. Br JHaematol 114:616-623, 2001
31. von Wasielewski R, Seth S, Franklin J, et al:Tissue eosinophilia correlates strongly with poorprognosis in nodular sclerosing Hodgkin’s disease,allowing for known prognostic factors. Blood 95:1207-1213, 2000
32. Maggio EM, Van Den Berg A, Visser L, et al:Common and differential chemokine expression pat-terns in rs cells of NLP, EBV positive and negativeclassical Hodgkin lymphomas. Int J Cancer 99:665-672, 2002
33. Xerri L, Birg F, Guigou V, et al: In situexpression of the IL-1-alpha and TNF-alpha genes byReed-Sternberg cells in Hodgkin’s disease. Int JCancer 50:689-693, 1992
34. Kretschmer C, Jones DB, Morrison K, et al:Tumor necrosis factor alpha and lymphotoxin pro-duction in Hodgkin’s disease. Am J Pathol 137:341-351, 1990
35. Ree HJ, Crowley JP, Dinarello CA: Anti-interleukin-1 reactive cells in Hodgkin’s disease.Cancer 59:1717-1720, 1987
36. Hsu SM, Lin J, Xie SS, et al: Abundantexpression of transforming growth factor-beta 1 and-beta 2 by Hodgkin’s Reed-Sternberg cells and byreactive T lymphocytes in Hodgkin’s disease. HumPathol 24:249-255, 1993
37. Aldinucci D, Olivo K, Lorenzon D, et al: Therole of interleukin-3 in classical Hodgkin’s disease.Leuk Lymphoma 46:303-311, 2005
38. Aldinucci D, Poletto D, Gloghini A, et al:Expression of functional interleukin-3 receptors onHodgkin and Reed-Sternberg cells. Am J Pathol160:585-596, 2002
39. Hanamoto H, Nakayama T, Miyazato H, et al:Expression of CCL28 by Reed-Sternberg cells de-fines a major subtype of classical Hodgkin’s diseasewith frequent infiltration of eosinophils and/or plasmacells. Am J Pathol 164:997-1006, 2004
40. Ma Y, Visser L, Roelofsen H, et al: Proteom-ics analysis of Hodgkin lymphoma: Identification ofnew players involved in the cross-talk between HRScells and infiltrating lymphocytes. Blood 111:2339-2346, 2008
41. Khnykin D, Troen G, Berner JM, et al: Theexpression of fibroblast growth factors and theirreceptors in Hodgkin’s lymphoma. J Pathol 208:431-438, 2006
42. Giles FJ, Vose JM, Do KA, et al: Clinicalrelevance of circulating angiogenic factors in pa-tients with non-Hodgkin’s lymphoma or Hodgkin’slymphoma. Leuk Res 28:595-604, 2004
43. Hsu PL, Lin YC, Hsu SM: Expression ofmacrophage colony-stimulating factor (M-CSF) intwo Hodgkin’s Reed-Sternberg (H-RS) cell lines,HDLM-1 and KM-H2, and in H-RS cells in tissues. IntJ Hematol 54:315-326, 1991
44. Lamprecht B, Walter K, Kreher S, et al:Derepression of an endogenous long terminal re-peat activates the CSF1R proto-oncogene in humanlymphoma. Nat Med 16:571-579, 2010
45. Pinto A, Aldinucci D, Gloghini A, et al: Humaneosinophils express functional CD30 ligand andstimulate proliferation of a Hodgkin’s disease cellline. Blood 88:3299-3305, 1996
46. Fischer M, Juremalm M, Olsson N, et al:Expression of CCL5/RANTES by Hodgkin and Reed-Sternberg cells and its possible role in the recruit-ment of mast cells into lymphomatous tissue. Int JCancer 107:197-201, 2003
47. Buri C, Korner M, Scharli P, et al: CC chemo-kines and the receptors CCR3 and CCR5 are differ-entially expressed in the nonneoplastic leukocyticinfiltrates of Hodgkin disease. Blood 97:1543-1548,2001
48. Jundt F, Anagnostopoulos I, Bommert K, etal: Hodgkin/Reed-Sternberg cells induce fibroblasts
Microenvironment in Hodgkin’s Lymphoma
www.jco.org © 2011 by American Society of Clinical Oncology 11Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.
Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

to secrete eotaxin, a potent chemoattractant for Tcells and eosinophils. Blood 94:2065-2071, 1999
49. van den Berg A, Visser L, Poppema S: Highexpression of the CC chemokine TARC in Reed-Sternberg cells: A possible explanation for the char-acteristic T-cell infiltratein Hodgkin’s lymphoma.Am J Pathol 154:1685-1691, 1999
50. Ohshima K, Tutiya T, Yamaguchi T, et al:Infiltration of Th1 and Th2 lymphocytes around Hodg-kin and Reed-Sternberg (H&RS) cells in Hodgkin dis-ease: Relation with expression of CXC and CCchemokines on H&RS cells. Int J Cancer 98:567-572,2002
51. Peh SC, Kim LH, Poppema S: TARC, a CCchemokine, is frequently expressed in classic Hodg-kin’s lymphoma but not in NLP Hodgkin’s lym-phoma, T-cell-rich B-cell lymphoma, and most casesof anaplastic large cell lymphoma. Am J Surg Pathol25:925-929, 2001
52. Hedvat CV, Jaffe ES, Qin J, et al:Macrophage-derived chemokine expression in clas-sical Hodgkin’s lymphoma: Application of tissuemicroarrays. Mod Pathol 14:1270-1276, 2001
53. Foss HD, Herbst H, Gottstein S, et al:Interleukin-8 in Hodgkin’s disease: Preferential ex-pression by reactive cells and association with neu-trophil density. Am J Pathol 148:1229-1236, 1996
54. Luciani MG, Stoppacciaro A, Peri G, et al:The monocyte chemotactic protein a (MCP-1) andinterleukin 8 (IL-8) in Hodgkin’s disease and in solidtumours. Mol Pathol 51:273-276, 1998
55. Trumper L, Jung W, Dahl G, et al: Interleukin-7,interleukin-8, soluble TNF receptor, and p53 proteinlevels are elevated in the serum of patients withHodgkin’s disease. Ann Oncol 5:93-96, 1994 (suppl 1)
56. Gorschluter M, Bohlen H, Hasenclever D, etal: Serum cytokine levels correlate with clinical pa-rameters in Hodgkin’s disease. Ann Oncol 6:477-482, 1995
57. Hopken UE, Foss HD, Meyer D, et al: Up-regulation of the chemokine receptor CCR7 in clas-sical but not in lymphocyte-predominant Hodgkindisease correlates with distinct dissemination ofneoplastic cells in lymphoid organs. Blood 99:1109-1116, 2002
58. Poppema S, Bhan AK, Reinherz EL, et al: Insitu immunologic characterization of cellular constit-uents in lymph nodes and spleens involved byHodgkin’s disease. Blood 59:226-232, 1982
59. Poppema S, Lai R, Visser L, et al: CD45(leucocyte common antigen) expression in T and Blymphocyte subsets. Leuk Lymphoma 20:217-222,1996
60. Alexander WS: Cytokines in hematopoiesis.Int Rev Immunol 16:651-682, 1998
61. Truman LA, Ford CA, Pasikowska M, et al:CX3CL1/fractalkine is released from apoptotic lym-phocytes to stimulate macrophage chemotaxis.Blood 112:5026-5036, 2008
62. Qian BZ, Pollard JW: Macrophage diversityenhances tumor progression and metastasis. Cell141:39-51, 2010
63. Stein R, Qu Z, Cardillo TM, et al: Antiprolif-erative activity of a humanized anti-CD74 monoclo-nal antibody, hLL1, on B-cell malignancies. Blood104:3705-3711, 2004
64. Leng L, Metz CN, Fang Y, et al: MIF signaltransduction initiated by binding to CD74. J Exp Med197:1467-1476, 2003
65. Ohshima K, Akaiwa M, Umeshita R, etal: Interleukin-13 and interleukin-13 receptor inHodgkin’s disease: Possible autocrine mechanismand involvement in fibrosis. Histopathology 38:368-375, 2001
66. Vu F, Dianzani U, Ware CF, et al: ICOS,CD40, and lymphotoxin beta receptors signal se-quentially and interdependently to initiate a germinalcenter reaction. J Immunol 180:2284-2293, 2008
67. Nam-Cha SH, Roncador G, Sanchez-Verde L,et al: PD-1, a follicular T-cell marker useful for recog-nizing nodular lymphocyte-predominant Hodgkin lym-phoma. Am J Surg Pathol 32:1252-1257, 2008
68. Kuppers R: The biology of Hodgkin’s lym-phoma. Nat Rev Cancer 9:15-27, 2009
69. Joos S, Menz CK, Wrobel G, et al: ClassicalHodgkin lymphoma is characterized by recurrentcopy number gains of the short arm of chromosome2. Blood 99:1381-1387, 2002
70. Martın-Subero JI, Gesk S, Harder L, et al:Recurrent involvement of the REL and BCL11A lociin classical Hodgkin lymphoma. Blood 99:1474-1477, 2002
71. Chui DT, Hammond D, Baird M, et al: Clas-sical Hodgkin lymphoma is associated with frequentgains of 17q. Genes Chromosomes Cancer 38:126-136, 2003
72. Steidl C, Telenius A, Shah SP, et al: Genome-wide copy number analysis of Hodgkin Reed-Sternberg cells identifies recurrent imbalances withcorrelations to treatment outcome. Blood 116:418-427, 2010
73. Mathas S, Johrens K, Joos S, et al: ElevatedNF-kappaB p50 complex formation and Bcl-3 ex-pression in classical Hodgkin, anaplastic large-cell,and other peripheral T-cell lymphomas. Blood 106:4287-4293, 2005
74. Martin-Subero JI, Wlodarska I, Bastard C, etal: Chromosomal rearrangements involving theBCL3 locus are recurrent in classical Hodgkin andperipheral T-cell lymphoma. Blood 108:401-402,2006; author reply 402-403
75. Cabannes E, Khan G, Aillet F, et al: Mutationsin the IkBa gene in Hodgkin’s disease suggest atumour suppressor role for IkappaBalpha. Oncogene18:3063-3070, 1999
76. Emmerich F, Meiser M, Hummel M, et al:Overexpression of I kappa B alpha without inhibitionof NF-kappaB activity and mutations in the I kappa Balpha gene in Reed-Sternberg cells. Blood 94:3129-3134, 1999
77. Jungnickel B, Staratschek-Jox A, BrauningerA, et al: Clonal deleterious mutations in the Ikap-paBalpha gene in the malignant cells in Hodgkin’slymphoma. J Exp Med 191:395-402, 2000
78. Emmerich F, Theurich S, Hummel M, et al:Inactivating I kappa B epsilon mutations in Hodgkin/Reed-Sternberg cells. J Pathol 201:413-420, 2003
79. Schmitz R, Hansmann ML, Bohle V, et al:TNFAIP3 (A20) is a tumor suppressor gene in Hodg-kin lymphoma and primary mediastinal B cell lym-phoma. J Exp Med 206:981-989, 2009
80. Weniger MA, Melzner I, Menz CK, et al:Mutations of the tumor suppressor gene SOCS-1 inclassical Hodgkin lymphoma are frequent and asso-ciated with nuclear phospho-STAT5 accumulation.Oncogene 25:2679-2684, 2006
81. Mottok A, Renne C, Willenbrock K, et al:Somatic hypermutation of SOCS1 in lymphocyte-predominant Hodgkin lymphoma is accompanied byhigh JAK2 expression and activation of STAT6.Blood 110:3387-3390, 2007
82. Maggio EM, Stekelenburg E, Van den BergA, et al: TP53 gene mutations in Hodgkin lymphomaare infrequent and not associated with absence ofEpstein-Barr virus. Int J Cancer 94:60-66, 2001
83. Leonard WJ: Role of Jak kinases and STATsin cytokine signal transduction. Int J Hematol 73:271-277, 2001
84. Karin M, Gallagher E: TNFR signaling:Ubiquitin-conjugated TRAFfic signals control stop-and-go for MAPK signaling complexes. ImmunolRev 228:225-240, 2009
85. Manning G, Whyte DB, Martinez R, et al: Theprotein kinase complement of the human genome.Science 298:1912-1934, 2002
86. Carbone A, Gloghini A, Gruss HJ, et al: CD40ligand is constitutively expressed in a subset of T celllymphomas and on the microenvironmental reactive Tcells of follicular lymphomas and Hodgkin’s disease.Am J Pathol 147:912-922, 1995
87. Messineo C, Jamerson MH, Hunter E, et al:Gene expression by single Reed-Sternberg cells:Pathways of apoptosis and activation. Blood 91:2443-2451, 1998
88. Kilger E, Kieser A, Baumann M, et al:Epstein-Barr virus-mediated B-cell proliferation isdependent upon latent membrane protein 1, whichsimulates an activated CD40 receptor. Embo J 17:1700-1709, 1998
89. Schwaller J, Went P, Matthes T, et al: Para-crine promotion of tumor development by the TNFligand APRIL in Hodgkin’s disease. Leukemia 21:1324-1327, 2007
90. Skinnider BF, Elia AJ, Gascoyne RD, et al:Signal transducer and activator of transcription 6 isfrequently activated in Hodgkin and Reed-Sternbergcells of Hodgkin lymphoma. Blood 99:618-626, 2002
91. Scheeren FA, Diehl SA, Smit LA, et al: IL-21is expressed in Hodgkin lymphoma and activatesSTAT5: evidence that activated STAT5 is requiredfor Hodgkin lymphomagenesis. Blood 111:4706-4715, 2008
92. Kube D, Holtick U, Vockerodt M, et al: STAT3is constitutively activated in Hodgkin cell lines.Blood 98:762-770, 2001
93. Aldinucci D, Gloghini A, Pinto A, et al: Theclassical Hodgkin’s lymphoma microenvironmentand its role in promoting tumour growth and im-mune escape. J Pathol 221:248-263, 2010
94. Tesch H, Gunther A, Abts H, et al: Expres-sion of interleukin-2R alpha and interleukin-2R betain Hodgkin’s disease. Am J Pathol 142:1714-1720,1993
95. Trumper LH, Brady G, Bagg A, et al: Single-cell analysis of Hodgkin and Reed-Sternberg cells:Molecular heterogeneity of gene expression andp53 mutations. Blood 81:3097-3115, 1993
96. Jucker M, Abts H, Li W, et al: Expression ofinterleukin-6 and interleukin-6 receptor in Hodgkin’sdisease. Blood 77:2413-2418, 1991
97. Cattaruzza L, Gloghini A, Olivo K, et al: Func-tional coexpression of Interleukin (IL)-7 and its re-ceptor (IL-7R) on Hodgkin and Reed-Sternberg cells:Involvement of IL-7 in tumor cell growth and mi-croenvironmental interactions of Hodgkin’s lym-phoma. Int J Cancer 125:1092-1101, 2009
98. Pons E, Uphoff CC, Drexler HG: Expressionof hepatocyte growth factor and its receptor c-metin human leukemia-lymphoma cell lines. Leuk Res22:797-804, 1998
99. Teofili L, Di Febo AL, Pierconti F, et al:Expression of the c-met proto-oncogene and itsligand, hepatocyte growth factor, in Hodgkin dis-ease. Blood 97:1063-1069, 2001
100. Renne C, Willenbrock K, Kuppers R, et al:Autocrine- and paracrine-activated receptor tyrosinekinases in classic Hodgkin lymphoma. Blood 105:4051-4059, 2005
101. Willenbrock K, Kuppers R, Renne C, et al:Common features and differences in the transcrip-tome of large cell anaplastic lymphoma and classical
Steidl, Connors, and Gascoyne
12 © 2011 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

Hodgkin’s lymphoma. Haematologica 91:596-604,2006
102. Renne C, Minner S, Kuppers R, et al: Auto-crine NGFbeta/TRKA signalling is an important sur-vival factor for Hodgkin lymphoma derived cell lines.Leuk Res 32:163-167, 2008
103. Carbone A, Gloghini A, Serraino D, et al:HIV-associated Hodgkin lymphoma. Curr Opin HIVAIDS 4:3-10, 2009
104. Sakaguchi S, Miyara M, Costantino CM, et al:FOXP3� regulatory T cells in the human immunesystem. Nat Rev Immunol 10:490-500
105. Marshall NA, Christie LE, Munro LR, et al:Immunosuppressive regulatory T cells are abundantin the reactive lymphocytes of Hodgkin lymphoma.Blood 103:1755-1762, 2004
106. Gandhi MK, Lambley E, Duraiswamy J, et al:Expression of LAG-3 by tumor-infiltrating lympho-cytes is coincident with the suppression of latentmembrane antigen-specific CD8� T-cell function inHodgkin lymphoma patients. Blood 108:2280-2289,2006
107. Aldinucci D, Lorenzon D, Cattaruzza L, et al:Expression of CCR5 receptors on Reed-Sternbergcells and Hodgkin lymphoma cell lines: Involvementof CCL5/Rantes in tumor cell growth and microen-vironmental interactions. Int J Cancer 122:769-776,2008
108. Tanijiri T, Shimizu T, Uehira K, et al: Hodgkin’sReed-Sternberg cell line (KM-H2) promotes a bidirec-tional differentiation of CD4�CD25�Foxp3� T cellsand CD4� cytotoxic T lymphocytes from CD4� naiveT cells. J Leukoc Biol 82:576-584, 2007
109. Kadin ME, Agnarsson BA, Ellingsworth LR,et al: Immunohistochemical evidence of a role fortransforming growth factor beta in the pathogenesisof nodular sclerosing Hodgkin’s disease. Am JPathol 136:1209-1214, 1990
110. Passwell J, Levanon M, Davidsohn J, et al:Monocyte PGE2 secretion in Hodgkin’s disease andits relation to decreased cellular immunity. Clin ExpImmunol 51:61-68, 1983
111. Cayeux SJ, Beverley PC, Schulz R, et al:Elevated plasma prostaglandin E2 levels found in 14patients undergoing autologous bone marrow orstem cell transplantation. Bone Marrow Transplant12:603-608, 1993
112. Harris SG, Padilla J, Koumas L, et al: Prosta-glandins as modulators of immunity. Trends Immu-nol 23:144-150, 2002
113. Chemnitz JM, Driesen J, Classen S, et al:Prostaglandin E2 impairs CD4� T cell activation byinhibition of lck: Implications in Hodgkin’s lym-phoma. Cancer Res 66:1114-1122, 2006
114. Kim LH, Eow GI, Peh SC, et al: The role ofCD30, CD40 and CD95 in the regulation of prolifer-ation and apoptosis in classical Hodgkin’s lym-phoma. Pathology 35:428-435, 2003
115. Walker PR, Saas P, Dietrich PY: Role of Fasligand (CD95L) in immune escape: The tumor cellstrikes back. J Immunol 158:4521-4524, 1997
116. Verbeke CS, Wenthe U, Grobholz R, et al:Fas ligand expression in Hodgkin lymphoma. Am JSurg Pathol 25:388-394, 2001
117. Dotti G, Savoldo B, Pule M, et al: Humancytotoxic T lymphocytes with reduced sensitivity toFas-induced apoptosis. Blood 105:4677-4684, 2005
118. Gandhi MK, Moll G, Smith C, et al: Galectin-1mediated suppression of Epstein-Barr virus specificT-cell immunity in classic Hodgkin lymphoma. Blood110:1326-1329, 2007
119. Juszczynski P, Ouyang J, Monti S, et al: TheAP1-dependent secretion of galectin-1 by ReedSternberg cells fosters immune privilege in classical
Hodgkin lymphoma. Proc Natl Acad Sci U S A104:13134-13139, 2007
120. Yamamoto R, Nishikori M, Kitawaki T, et al:PD-1-PD-1 ligand interaction contributes to immuno-suppressive microenvironment of Hodgkin lym-phoma. Blood 111:3220-3224, 2008
121. Green MR, Monti S, Rodig SJ, et al: Integrativeanalysis reveals selective 9p24.1 amplification, in-creased PD-1 ligand expression, and further inductionvia JAK2 in nodular sclerosing Hodgkin lymphoma andprimary mediastinal large B-cell lymphoma. Blood 116:3268-3277, 2010
122. Keir ME, Butte MJ, Freeman GJ, et al: PD-1and its ligands in tolerance and immunity. Annu RevImmunol 26:677-704, 2008
123. Diepstra A, van Imhoff GW, Karim-Kos HE,et al: HLA class II expression by Hodgkin Reed-Sternberg cells is an independent prognostic factorin classical Hodgkin’s lymphoma. J Clin Oncol 25:3101-3108, 2007
124. Huang X, van den Berg A, Gao Z, et al:Expression of HLA class I and HLA class II by tumorcells in Chinese classical Hodgkin lymphoma pa-tients. PLoS One 5:e10865, 2010
125. Poppema S: Immunobiology and pathophys-iology of Hodgkin lymphomas. Hematology Am SocHematol Educ Program 231-238, 2005
126. Kluiver J, Kok K, Pfeil I, et al: Global correla-tion of genome and transcriptome changes in clas-sical Hodgkin lymphoma. Hematol Oncol 25:21-29,2007
127. Diepstra A, Niens M, Vellenga E, et al: Asso-ciation with HLA class I in Epstein-Barr-virus-positiveand with HLA class III in Epstein-Barr-virus-negativeHodgkin’s lymphoma. Lancet 365:2216-2224, 2005
128. Hjalgrim H, Rostgaard K, Johnson PC, et al:HLA-A alleles and infectious mononucleosis sug-gest a critical role for cytotoxic T-cell response inEBV-related Hodgkin lymphoma. Proc Natl Acad SciU S A 107:6400-6405, 2010
129. Niens M, Jarrett RF, Hepkema B, et al:HLA-A*02 is associated with a reduced risk andHLA-A*01 with an increased risk of developingEBV� Hodgkin lymphoma. Blood 110:3310-3315,2007
130. Diepstra A, Poppema S, Boot M, et al: HLA-Gprotein expression as a potential immune escapemechanism in classical Hodgkin’s lymphoma. Tis-sue Antigens 71:219-226, 2008
131. Sanchez-Espiridion B, Sanchez-Aguilera A,Montalban C, et al: A TaqMan low-density array topredict outcome in advanced Hodgkin’s lymphomausing paraffin-embedded samples. Clin Cancer Res15:1367-1375, 2009
132. Steidl C, Lee T, Shah SP, et al: Tumor-associated macrophages and survival in classicHodgkin’s lymphoma. N Engl J Med 362:875-885,2010
133. Asano N, Oshiro A, Matsuo K, et al: Prognosticsignificance of T-cell or cytotoxic molecules phenotypein classical Hodgkin’s lymphoma: A clinicopathologicstudy. J Clin Oncol 24:4626-4633, 2006
134. Oudejans JJ, Jiwa NM, Kummer JA, et al:Activated cytotoxic T cells as prognostic marker inHodgkin’s disease. Blood 89:1376-1382, 1997
135. ten Berge RL, Oudejans JJ, Dukers DF, et al:Percentage of activated cytotoxic T-lymphocytes inanaplastic large cell lymphoma and Hodgkin’s dis-ease: An independent biological prognostic marker.Leukemia 15:458-464, 2001
136. Alvaro-Naranjo T, Lejeune M, Salvado-UsachMT, et al: Tumor-infiltrating cells as a prognosticfactor in Hodgkin’s lymphoma: A quantitative tissue
microarray study in a large retrospective cohort of267 patients. Leuk Lymphoma 46:1581-1591, 2005
137. Kelley TW, Pohlman B, Elson P, et al: Theratio of FOXP3� regulatory T cells to granzyme B�cytotoxic T/NK cells predicts prognosis in classicalHodgkin lymphoma and is independent of bcl-2 andMAL expression. Am J Clin Pathol 128:958-965,2007
138. Alvaro T, Lejeune M, Salvado MT, et al:Outcome in Hodgkin’s lymphoma can be predictedfrom the presence of accompanying cytotoxic andregulatory T cells. Clin Cancer Res 11:1467-1473,2005
139. Tzankov A, Meier C, Hirschmann P, et al:Correlation of high numbers of intratumoral FOXP3�regulatory T cells with improved survival in germinalcenter-like diffuse large B-cell lymphoma, follicularlymphoma and classical Hodgkin’s lymphoma. Haemato-logica 93:193-200, 2008
140. Chetaille B, Bertucci F, Finetti P, et al: Molec-ular profiling of classical Hodgkin lymphoma tissuesuncovers variations in the tumor microenvironmentand correlations with EBV infection and outcome.Blood 113:2765-3775, 2009
141. Ree HJ, Kadin ME: Macrophage-histiocytesin Hodgkin’s disease: The relation of peanut-agglutinin-binding macrophage-histiocytes to clinico-pathologic presentation and course of disease.Cancer 56:333-338, 1985
142. Sanchez-Aguilera A, Montalban C, de laCueva P, et al: Tumor microenvironment and mitoticcheckpoint are key factors in the outcome of classicHodgkin lymphoma. Blood 108:662-668, 2006
143. Engel M, Essop MF, Close P, et al: Improvedprognosis of Epstein-Barr virus associated childhoodHodgkin’s lymphoma: Study of 47 South Africancases. J Clin Pathol 53:182-186, 2000
144. Keegan TH, Glaser SL, Clarke CA, et al:Epstein-Barr virus as a marker of survival afterHodgkin’s lymphoma: A population-based study.J Clin Oncol 23:7604-7613, 2005
145. Diepstra A, van Imhoff GW, Schaapveld M,et al: Latent Epstein-Barr virus infection of tumorcells in classical Hodgkin’s lymphoma predicts ad-verse outcome in older adult patients. J Clin Oncol27:3815-3821, 2009
146. Jarrett RF, Stark GL, White J, et al: Impact oftumor Epstein-Barr virus status on presenting fea-tures and outcome in age-defined subgroups ofpatients with classic Hodgkin lymphoma: A population-based study. Blood 106:2444-2451, 2005
147. Kwon JM, Park YH, Kang JH, et al: The effectof Epstein-Barr virus status on clinical outcome inHodgkin’s lymphoma. Ann Hematol 85:463-468,2006
148. Devilard E, Bertucci F, Trempat P, et al: Geneexpression profiling defines molecular subtypes ofclassical Hodgkin’s disease. Oncogene 21:3095-3102, 2002
149. MacLennan KA, Bennett MH, Tu A, et al:Relationship of histopathologic features to survivaland relapse in nodular sclerosing Hodgkin’s disease:A study of 1659 patients. Cancer 64:1686-1693,1989
150. Hess JL, Bodis S, Pinkus G, et al: Histopatho-logic grading of nodular sclerosis Hodgkin’s disease:Lack of prognostic significance in 254 surgicallystaged patients. Cancer 74:708-714, 1994
151. van Spronsen DJ, Vrints LW, Hofstra G, etal: Disappearance of prognostic significance of histo-pathological grading of nodular sclerosing Hodgkin’sdisease for unselected patients, 1972-92. Br J Haema-tol 96:322-327, 1997
Microenvironment in Hodgkin’s Lymphoma
www.jco.org © 2011 by American Society of Clinical Oncology 13Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.
Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

152. Gobbi PG, Cavalli C, Federico M, et al: Increasinginterdependency of prognosis- and therapy-related fac-tors in Hodgkin’s disease. Acta Haematol 81:34-40, 1989
153. Enblad G, Sundstrom C, Glimelius B: Infiltra-tion of eosinophils in Hodgkin’s disease involvedlymph nodes predicts prognosis. Hematol Oncol11:187-193, 1993
154. Mir R, Anderson J, Strauchen J, et al: Hodg-kin disease in patients 60 years of age or older:Histologic and clinical features of advanced-stagedisease—The Cancer and Leukemia Group B. Can-cer 71:1857-1866, 1993
155. Axdorph U, Porwit-MacDonald A, GrimforsG, et al: Tissue eosinophilia in relation to immuno-pathological and clinical characteristics in Hodgkin’sdisease. Leuk Lymphoma 42:1055-1065, 2001
156. Molin D, Edstrom A, Glimelius I, et al: Mastcell infiltration correlates with poor prognosis inHodgkin’s lymphoma. Br J Haematol 119:122-124,2002
157. Canioni D, Deau-Fischer B, Taupin P, et al:Prognostic significance of new immunohistochemi-cal markers in refractory classical Hodgkin lym-phoma: A study of 59 cases. PLoS One 4:e6341,2009
158. Colby TV, Hoppe RT, Warnke RA: Hodgkin’sdisease: A clinicopathologic study of 659 cases.Cancer 49:1848-1858, 1982
159. Sanchez-Espiridion B, Montalban C, Lopez A,et al: A molecular risk score based on four functionalpathways for advanced classical Hodgkin lymphoma.Blood 116:e12-e17, 2010
160. Farinha P, Masoudi H, Skinnider BF, et al:Analysis of multiple biomarkers shows that lymphoma-associated macrophage (LAM) content is an indepen-dent predictor of survival in follicular lymphoma (FL).Blood 106:2169-2174, 2005
161. Schreck S, Friebel D, Buettner M, et al:Prognostic impact of tumour-infiltrating Th2 andregulatory T cells in classical Hodgkin lymphoma.Hematol Oncol 27:31-39, 2009
162. Menetrier-Caux C, Gobert M, Caux C: Differ-ences in tumor regulatory T-cell localization andactivation status impact patient outcome. CancerRes 69:7895-7898, 2009
163. Alvaro T, Lejeune M, Garcıa JF, et al: Tumor-infiltrated immune response correlates with altera-tions in the apoptotic and cell cycle pathways inHodgkin and Reed-Sternberg cells. Clin Cancer Res14:685-691, 2008
164. Alavaikko MJ, Hansmann ML, Nebendahl C,et al: Follicular dendritic cells in Hodgkin’s disease.Am J Clin Pathol 95:194-200, 1991
165. Delsol G, Meggetto F, Brousset P, et al:Relation of follicular dendritic reticulum cells toReed-Sternberg cells of Hodgkin’s disease withemphasis on the expression of CD21 antigen. Am JPathol 142:1729-1738, 1993
166. Alavaikko MJ, Blanco G, Aine R, et al: Follic-ular dendritic cells have prognostic relevance inHodgkin’s disease. Am J Clin Pathol 101:761-767,1994
167. Baur AS, Meuge-Moraw C, Michel G, et al:Prognostic value of follicular dendritic cells in nodu-lar sclerosing Hodgkin’s disease. Histopathology32:512-520, 1998
168. Glaser SL, Lin RJ, Stewart SL, et al: Epstein-Barr virus-associated Hodgkin’s disease: Epidemio-logic characteristics in international data. Int JCancer 70:375-382, 1997
169. Enblad G, Sandvej K, Lennette E, et al: Lackof correlation between EBV serology and presenceof EBV in the Hodgkin and Reed-Sternberg cells of
patients with Hodgkin’s disease. Int J Cancer 72:394-397, 1997
170. Morente MM, Piris MA, Abraira V, et al:Adverse clinical outcome in Hodgkin’s disease isassociated with loss of retinoblastoma protein ex-pression, high Ki67 proliferation index, and absenceof Epstein-Barr virus-latent membrane protein 1expression. Blood 90:2429-2436, 1997
171. Warzocha K, Bienvenu J, Ribeiro P, et al:Plasma levels of tumour necrosis factor and itssoluble receptors correlate with clinical features andoutcome of Hodgkin’s disease patients. Br J Cancer77:2357-2362, 1998
172. Weihrauch MR, Manzke O, Beyer M, et al:Elevated serum levels of CC thymus and activation-related chemokine (TARC) in primary Hodgkin’s dis-ease: Potential for a prognostic factor. Cancer Res65:5516-5519, 2005
173. Gause A, Pohl C, Tschiersch A, et al: Clinicalsignificance of soluble CD30 antigen in the sera ofpatients with untreated Hodgkin’s disease. Blood77:1983-1988, 1991
174. Ambrosetti A, Nadali G, Vinante F, et al:Serum levels of soluble interleukin-2 receptor inHodgkin disease: Relationship with clinical stage,tumor burden, and treatment outcome. Cancer 72:201-206, 1993
175. Christiansen I, Enblad G, Kalkner KM, et al:Soluble ICAM-1 in Hodgkin’s disease: A promisingindependent predictive marker for survival. LeukLymphoma 19:243-251, 1995
176. Christiansen I, Sundstrom C, Enblad G, et al:Soluble vascular cell adhesion molecule-1 (sVCAM-1)is an independent prognostic marker in Hodgkin’sdisease. Br J Haematol 102:701-709, 1998
177. Kuppers R, Klein U, Schwering I, et al: Iden-tification of Hodgkin and Reed-Sternberg cell-specific genes by gene expression profiling. J ClinInvest 111:529-537, 2003
178. Brune V, Tiacci E, Pfeil I, et al: Origin andpathogenesis of nodular lymphocyte-predominantHodgkin lymphoma as revealed by global gene ex-pression analysis. J Exp Med 205:2251-2268, 2008
179. Lenz G, Wright G, Dave SS, et al: Stromalgene signatures in large B-cell lymphomas. N EnglJ Med 359:2313-2323, 2008
180. Farinha P, Kyle A, Minchinton A, et al: Vas-cularization predicts overall survival and risk of trans-formation in follicular lymphoma. Haematologica 95:2157-2160, 2010
181. Iqbal J, Weisenburger DD, Greiner TC, etal: Molecular signatures to improve diagnosis inperipheral T-cell lymphoma and prognostication inangioimmunoblastic T-cell lymphoma. Blood 115:1026-1036
182. Fujii K, Kondo T, Yokoo H, et al: Proteinexpression pattern distinguishes different lymphoidneoplasms. Proteomics 5:4274-4286, 2005
183. Carvalho PC, Carvalho Mda G, Degrave W, etal: Differential protein expression patterns obtainedby mass spectrometry can aid in the diagnosis ofHodgkin’s disease. J Exp Ther Oncol 6:137-145,2007
184. Navarro A, Gaya A, Martinez A, et al: Mi-croRNA expression profiling in classic Hodgkin lym-phoma. Blood 111:2825-2832, 2008
185. Navarro A, Diaz T, Martinez A, et al: Regula-tion of JAK2 by miR-135a: Prognostic impact inclassic Hodgkin lymphoma. Blood 114:2945-2951,2009
186. Younes A: Novel treatment strategies forpatients with relapsed classical Hodgkin lymphoma.Hematology Am Soc Hematol Educ Program 507-519, 2009
187. Younes A, Romaguera J, Hagemeister F, etal: A pilot study of rituximab in patients with recur-rent, classic Hodgkin disease. Cancer 98:310-314,2003
188. Oki Y, Pro B, Fayad LE, et al: Phase 2 studyof gemcitabine in combination with rituximab inpatients with recurrent or refractory Hodgkin lym-phoma. Cancer 112:831-836, 2008
189. Schulz H, Rehwald U, Morschhauser F, et al:Rituximab in relapsed lymphocyte-predominantHodgkin lymphoma: Long-term results of a phase 2trial by the German Hodgkin Lymphoma StudyGroup (GHSG). Blood 111:109-111, 2008
190. Rehwald U, Schulz H, Reiser M, et al: Treat-ment of relapsed CD20� Hodgkin lymphoma withthe monoclonal antibody rituximab is effective andwell tolerated: Results of a phase 2 trial of theGerman Hodgkin Lymphoma Study Group. Blood101:420-424, 2003
191. Younes A, Wong F: Experience with 90Y-ibritumomab tiuxetan for relapsed classical Hodgkinlymphoma. Ann Oncol 20:1147-1148, 2009
192. Leonard JP, Friedberg JW, Younes A, et al: Aphase I/II study of galiximab (an anti-CD80 monoclo-nal antibody) in combination with rituximab for re-lapsed or refractory, follicular lymphoma. Ann Oncol18:1216-1223, 2007
193. Rodig SJ, Abramson JS, Pinkus GS, et al:Heterogeneous CD52 expression among hemato-logic neoplasms: Implications for the use of alem-tuzumab (CAMPATH-1H). Clin Cancer Res 12:7174-7179, 2006
194. Ansell SM, Horwitz SM, Engert A, et al: Phase I/IIstudy of an anti-CD30 monoclonal antibody (MDX-060) inHodgkin’s lymphoma and anaplastic large-cell lym-phoma. J Clin Oncol 25:2764-2769, 2007
195. Okeley NM, Miyamoto JB, Zhang X, et al:Intracellular activation of SGN-35, a potent anti-CD30 antibody-drug conjugate. Clin Cancer Res16:888-897, 2010
196. Younes A, Forero-Torres A, Bartlett NL, et al:Multiple complete responses in a phase 1 dose-escalation study of the antibody-drug conjugateSGN-35 in patients with relapsed or refractoryCD30-positive lymphomas. Presented at the AnnualMeeting of the American Society of Hematology,San Francisco, CA, December 6-9, 2008 (abstr 1006)
197. Georgakis GV, Li Y, Humphreys R, et al:Activity of selective fully human agonistic antibodiesto the TRAIL death receptors TRAIL-R1 and TRAIL-R2in primary and cultured lymphoma cells: Induction ofapoptosis and enhancement of doxorubicin- andbortezomib-induced cell death. Br J Haematol 130:501-510, 2005
198. Luqman M, Klabunde S, Lin K, et al: Theantileukemia activity of a human anti-CD40 antago-nist antibody, HCD122, on human chronic lympho-cytic leukemia cells. Blood 112:711-720, 2008
199. Johnston PB, Ansell SM, Colgan JP, et al:MTOR inhibition for relapsed or refractory Hodgkinlymphoma: Promising single agent activity witheverolimus (RAD001). Presented at the AnnualMeeting of the American Society of Hematology,Atlanta, GA, December 8-11, 2007 (abstr 2555)
200. Zheng B, Georgakis GV, Li Y, et al: Inductionof cell cycle arrest and apoptosis by the proteasomeinhibitor PS-341 in Hodgkin disease cell lines isindependent of inhibitor of nuclear factor-kappaBmutations or activation of the CD30, CD40, andRANK receptors. Clin Cancer Res 10:3207-3215,2004
Steidl, Connors, and Gascoyne
14 © 2011 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.Copyright © 2011 American Society of Clinical Oncology. All rights reserved.

201. Younes A, Pro B, Fayad L: Experience withbortezomib for the treatment of patients with re-lapsed classical Hodgkin lymphoma. Blood 107:1731-1732, 2006
202. Blum KA, Johnson JL, Niedzwiecki D, et al:Single agent bortezomib in the treatment of re-lapsed and refractory Hodgkin lymphoma: Cancerand leukemia Group B protocol 50206. Leuk Lym-phoma 48:1313-1319, 2007
203. Kirschbaum MH, Goldman BH, Zain JM, etal: Vorinostat (suberoylanilide hydroxamic acid) inrelapsed or refractory Hodgkin lymphoma: SWOG0517. Presented at the Annual Meeting of theAmerican Society of Hematology, Atlanta, GA, De-cember 8-11, 2007 (abstr 2574)
204. Buglio D, Georgakis GV, Hanabuchi S, et al:Vorinostat inhibits STAT6-mediated TH2 cytokineand TARC production and induces cell death inHodgkin lymphoma cell lines. Blood 112:1424-1433,2008
205. Younes A, Sureda A, Ben-Yehuda D, et al:Phase II study of oral panobinostat in patients withrelapsed/refractory Hodgkin lymphoma (HL) after
high-dose chemotherapy with autologous stem celltransplant. Haematologica 94, 2009 (suppl 2; abstr34)
206. Fehniger TA, Larson S, Trinkaus K, et al: APhase II Multicenter Study of Lenalidomide in Pa-tients with Relapsed or Refractory Classical HodgkinLymphoma (cHL): Preliminary Results. Presented atthe Annual Meeting of the American Society ofHematology, San Francisco, CA, December 6-9,2008 (abstr 2595)
207. Kuruvilla J, Taylor D, Wang L, et al: Phase IItrial of lenalidomide in patients with relapsed orrefractory Hodgkin lymphoma. Presented at theAnnual Meeting of the American Society of Hema-tology, San Francisco, CA, December 6-9, 2008(abstr 3052)
208. Bollard CM, Aguilar L, Straathof KC, et al:Cytotoxic T lymphocyte therapy for Epstein-Barrvirus� Hodgkin’s disease. J Exp Med 200:1623-1633, 2004
209. Bollard CM, Gottschalk S, Leen AM, et al:Complete responses of relapsed lymphoma follow-ing genetic modification of tumor-antigen present-
ing cells and T-lymphocyte transfer. Blood 110:2838-2845, 2007
210. Oki Y, Younes A: Current role of gemcitabinein the treatment of Hodgkin lymphoma. Leuk Lym-phoma 49:883-889, 2008
211. Correale P, Del Vecchio MT, La Placa M, etal: Chemotherapeutic drugs may be used to en-hance the killing efficacy of human tumor antigenpeptide-specific CTLs. J Immunother 31:132-147,2008
212. Rassidakis GZ, Medeiros LJ, Viviani S, et al:CD20 expression in Hodgkin and Reed-Sternbergcells of classical Hodgkin’s disease: Associationswith presenting features and clinical outcome. J ClinOncol 20:1278-1287, 2002
213. Jones RJ, Gocke CD, Kasamon YL, et al:Circulating clonotypic B cells in classic Hodgkinlymphoma. Blood 113:5920-5926, 2009
214. Bartlett NL, Younes A, Carabasi MH, et al:A phase 1 multidose study of SGN-30 immuno-therapy in patients with refractory or recurrentCD30� hematologic malignancies. Blood 111:1848-1854, 2008
■ ■ ■
Acknowledgment
We thank Sibrand Poppema, MD, PhD, for his many contributions to the field and for reviewing this manuscript prior to submission.
Microenvironment in Hodgkin’s Lymphoma
www.jco.org © 2011 by American Society of Clinical Oncology 15Downloaded from jco.ascopubs.org on November 19, 2013. For personal use only. No other uses without permission.
Copyright © 2011 American Society of Clinical Oncology. All rights reserved.