Embed Size (px)
Citation preview

Janyne AfsethResearch Network
ManagerScottish Cancer Research
Network

Describe the drug development process
Review the ethical framework that underpins clinical research
Discuss current trends in cancer research – and where we are going
Discuss the role of the nurse in clinical trials

Patient
Behind the scenes Trial management
team
Statistician
Lab scientists
Regulation,
Management and approval
Clinic
Ethics Committees
Sponsors, Funding Sources
Regulatory Groups
Doctors, Nurses
NHS Laboratory Staff

Research study
Conducted in human volunteers
Designed to answer specific questions
Uses scientifically controlled methods

Evaluate the efficacy of new drug therapies and drug side effects (combinations of drugs, new ways of giving treatment, new types of treatment)
Evaluate the use and effectiveness of interventions, i.e.. surgical or diagnostic procedures (Scans, screening tests,surgical procedures)
Evaluate programs of cancer prevention and control (vitamins,foods, drugs)
Evaluate the psychological impact of treatment on patients (quality of life studies)
Quest to advance knowledge often benefits research subjects.
Patients may directly benefit from advanced therapies or indirectly from the satisfaction of contributing to society
Research benefits society as a whole Safe ways of new drug/novel agent
development

Lind (1747) comparative study using citrus in the treatment of scurvy (6 arms)
19th century utilized basic trial concepts in the development of of drugs and vaccines
Early 20th century studies focused on the prophylaxis and treatment of infectious diseases
1948 first placebo, controlled randomised trial
1960’s – present over 50 new drugs have been developed for treatment of cancer

Gold standard for evaluating new practices and therapeutic agents in medicine
The reason is that investigators could introduce bias and invalidate conclusions by the manner that they assigned patients to treatment groups

Question to be answered needs to be defined
Study endpoints Study then designed to test this
hypothesis using statistical methods Investigators must evaluation also
evaluate what is clinically significant (i.e likely to change practice)
Ensure consistency Define a specific plan of action Contain the following elements:
Introduction Eligibility Criteria Schedule of events Toxicity evaluation/dose reduction Kinetic sampling information Drug storage and admixture information Evaluation of response/follow up

Phase I maximum tolerated dose Phase II determines drug
activity/response Phase III compared to standard
therapy Phase IV post marketing studies

Medicines and Health Care Products Regulatory Agency (UK) (MHRA)/FDA (USA)• Must give authorisation for trials• Can inspect sites for compliance with
research legislation• Ultimately decide if the evidence for usage
in an indication can be licensed

1948 NHS committee set up to look at limiting prescriptions
1960s Thalidomide sparked the formation of the Committee on the Safety of Drugs
1968 Medicines Act provided for a comprehensive system of licensing affecting manufacture, sale, supply and importation of medicinal products.
MHRA also controls clinical trials, advertising, quality control, manufacture of unlicensed products and control of imports

Nuremberg Code (1947) basic moral, ethical, and legal concepts for experimentation. Developed as a result of experiments done in the Nazi concentration camps.
Helsinki Declaration (1964) Recommendations to guide the physician in biomedical research involving human subjects. Includes basic principles, medical research combined with professional care, and non-therapeutic biomedical research guidelines

10-12 years and £550 million to develop a new medicine
20% of world’s top medicines were discovered and developed in UK
£9 million invested in UK R&D daily
-www.abpi.org.uk

Drug Companies• £500 million annually
International/national Trial Organizations• EORTC• NCRI
Government Funding• Medical research council (MRC)• Department of Health (England)/CSO (Scotland)
Cancer Charities• Cancer Research UK (largest cancer research
organisation outside US)• The Leukaemia Research Fund •

All will have ‘patient selection criteria’
Doctors and nurses identify patients through multidisciplinary meetings and by screening clinic lists
Some patients will self refer Must pass all eligibility criteria to go
on (i.e. bloods, scans etc.
New treatment may work, drug not available outside of trial
Improving cancer treatment for other patients Close monitoring Patients treated in a centre where clinical trials
are done do better than people with a similar stage and type of cancer

Altruism Family pressure Unwillingness to “give up” Hope of benefit Input into care They think the treatments may be better
Fear of being allocated to control group
Too far to travel Desire to have Dr. choose treatment Guinea Pigs Complex Consent process Disliked focusing on disease

Participation is voluntary No coercion or inducement Information verbally and in writing Time to consider Support and communication
1940-50s the effect of mustard gas as therapeutic agent investigated.
50-60s combination chemotherapy Bone marrow transplant, hormonal
agents (Tamoxifen – 1970s) Biological agents

Allows selectivity with less toxicity As the understanding of how cancer cells
survive, thrive and spread can allow researchers to target these mechanisms.

Vascular Epithelial Growth Factor (VEGF) inhibitors• Avastin, Thalidomide
PARP inhibitors Epidermal Growth Factor Receptor
(EGFR) inhibitors• Herceptin, cetuximab, Iressa
Proteasome Inhibitors• velcade
• Angiogenesis is the formation of new blood vessels from pre-existing vasculature
• Angiogenesis is highly dependent on the VEGF signalling pathway
• VEGFR-2 is the most important VEGF signalling pathway for angiogenesis
• VEGF is frequently overexpressed in cancer and is associated with poor prognosis
• Without a blood supply, tumours do not grow larger than 1–2mm
• As tumours grow they become hypoxic, which leads to the up-regulation of angiogenic factors such as VEGF
• Stimulates the production of new vasculature
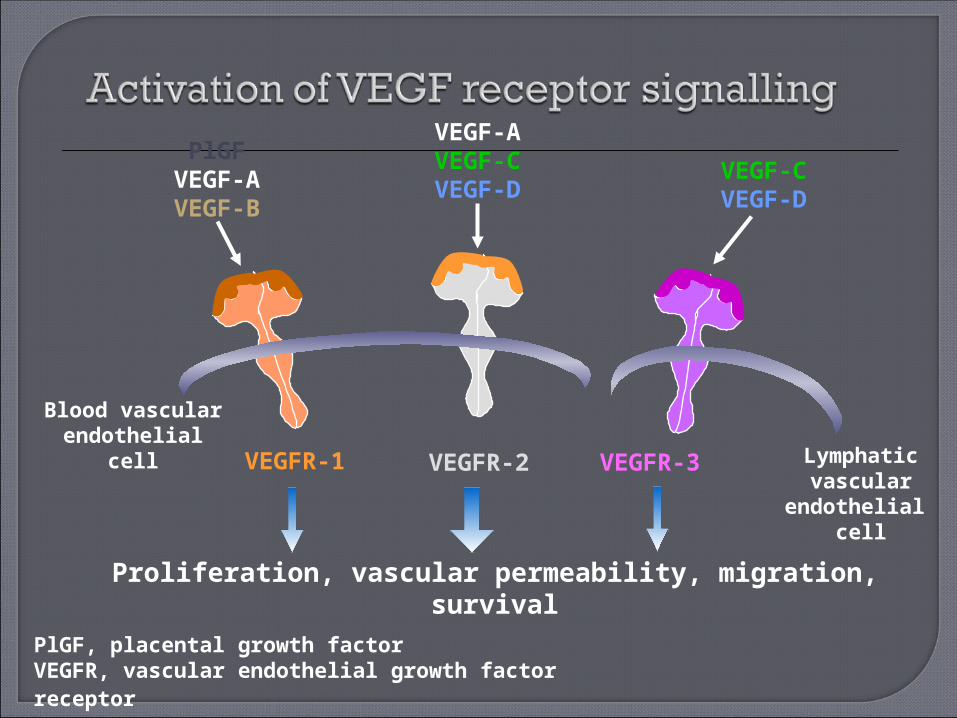
Blood vascularendothelial cell
Proliferation, vascular permeability, migration, survival
PlGFVEGF-AVEGF-B
VEGF-AVEGF-CVEGF-D
VEGF-CVEGF-D
PlGF, placental growth factor VEGFR, vascular endothelial growth factor receptor
Lymphatic vascular
endothelial cell
VEGFR-2VEGFR-1 VEGFR-3

Anti-VEGF antibodies
Lymphatic vascular
endothelial cell
Blood vascularendothelial cell
VEGFR-1VEGFR-2
VEGFR-3
Monoclonal antibody
VEGF-B
VEGF-D
VEGF-A
VEGF-C
Ligands

Blood vascularendothelial cell
Angiogenesis
Lymphatic vascular
endothelial cell
VEGFR-2VEGFR-1 VEGFR-3
Lymphangiogenesis
VEGFR-TKIs VEGF-B
VEGF-D
VEGF-A
VEGF-C
Ligands
X X X
VEGFR-TKI
Inhibition X
VEGFR-TKI, vascular endothelial growth factor receptor-tyrosine kinase inhibitor
• Inhibiting VEGF signalling• inhibits growth of new tumour vessels• decreases vascular density, diameter and
permeability• may induce regression of recently developed tumour
microvessels• Therapeutic inhibition of tumour angiogenesis should be
effective in a broad range of solid malignancies• Target tissue is in direct contact with blood, facilitating
drug delivery
Patient advocate Patient educator Direct care provider Coordinator Administrator Data manager
The potential for unexpected side effects is high with the pattern not yet established
Supportive care – what works with chemotherapy may not be the same for newer agent
Synergy of drugs is often unknown Information of to larger multidisciplinary
team is essential Patient involvement and time commitment
often may be much greater with the associated education needs
Scientific discovery New drug development Improved procedures Benefits to patients Economic development

???