Embed Size (px)
Citation preview

SEPTEMBER 2013 January 2014 Inside this issue:
Focus on Members 4
Education Updates 3
Healthy Michigan Plan to Provide Coverage Soon 3
Cashing In On Revenue Cycle Improvements 5
Careers 6
Michigan Affordable Healthcare 7
Presumptive Eligibility and Healthcare Reform 10
Do The Math ‐ Investing in Fundraising Can Really Pay Off 9
Chapter Happenings 12
President’s Message Dear Western Michigan HFMA Members,
I hope the holiday season was filled with much warmth, love and enjoyment. I’m looking forward to the New Year and the life moments ahead of me. My labs, Chloe and Autumn,
keep me busy. They have been trained as registered therapy dogs so we are always on the go. They are so wonderful with patients and filled with pure love that keeps my life very entertaining. Our November education session was another huge success. Vickie Kunz, as always, gave us the most up-to date MHA news. MHA is such a value to our association and our hospitals.
The program committee, led by Mary Oomen and Luke Check, is working hard to bring you quality sessions. The January meeting on the 22nd is based on Revenue Cycle. Please share your thoughts and ideas with these intervals on anything that might be of interest to you. We also are going to have a special “sweet treats” meeting on February 14th on cost reports. We’ll also hear from Laura Appel at MHA, with an update on healthcare expansion. Warm Regards, Barbara A. Shelley 2013-2014 Western Michigan Chapter President 517-203-7500 [email protected]

Page 2
Member Profile
Page 2
Nick Gates Nick graduated from Albion College with a B.A. in Economics and Management and furthered his education by obtaining an MBA from Michigan State University. Upon graduation from Albion, he started his career at Ernst & Young, LLP in Detroit focused primarily on auditing manufactur-ing clients. He left Ernst & Young in 2002 and joined Meadowbrook Insurance Group in South-
field, MI gaining experience with SEC reporting and financial analysis. Appreciating all that West Michigan has to offer, Nick and his wife de-cided to relocate to the Grand Rapids area where he accepted a role in finance at Priority Health, a subsidiary of Spectrum Health. He has had various roles within the Priority Health finance team and is currently Senior Director, Controller with Priority Health. He has had the privi-lege of collaborating with many talented professionals working closely together to prepare for unprecedented change as a result of the Afford-able Care Act. Nick states he couldn’t be prouder to work for an or-ganization that is so focused on caring for its community. When Nick took the position as a Senior Accountant at Priority Health, he knew very little about the healthcare industry. He was impressed with the reputation and growth of both Spectrum Health and Priority Health and was eager to learn more about the industry. He realized quickly that this was a very complex industry…and it has continued to become more complex. Healthcare is such a vital industry to our com-munities and Nick is proud to play a role in improving the quality of coverage and care that they offer them. Nick looks at his HFMA membership as access to a network of healthcare and health insurance professionals. In an industry that is constantly evolving through both innovation and regulatory changes, being able to have a forum to share ideas is invaluable. Outside of work, Nick spends much of his time with his wife and four young children. If there is any spare time left over, he loves reading or watching one of Michigan’s great professional and collegiate sports teams. Nick, welcome to healthcare, and HFMA!
N
EW
ME
MB
ER
S
Lindsey Roeters Senior Tax Accountant Spectrum Health Mark Demarest Spectrum Health

Page 3
Upcoming Events Webinars HFMA national or chapter webinar’s offer you an easy way to get the information you need on pressing healthcare finance topics. From the comfort of your office, you can participate in a Webinar and find the strategies and tools you need to help your organization achieve success. Take advantage of these and don’t forget to report your time and everyone in attendance to the Education Chairperson, Luke Check [email protected].
Meetings We are adding a special meeting in February for 2014! As always we try to bring you topics that are most cur-rent to help you with our daily struggles. We are al-ways looking for new and exciting topic’s as well as speakers. Let us know if you have any ideas. You can notate them on your survey. Always remember to sign in at the registration desk. This helps us keep track of education hours for our members. See you on the 22nd for our Revenue Cycle meeting! January 22, 2014 Revenue Cycle February 14, 2014 “Sweet Treats” - Cost Reports & Healthcare Expansion
Healthy Michigan Plan to Provide Coverage Soon
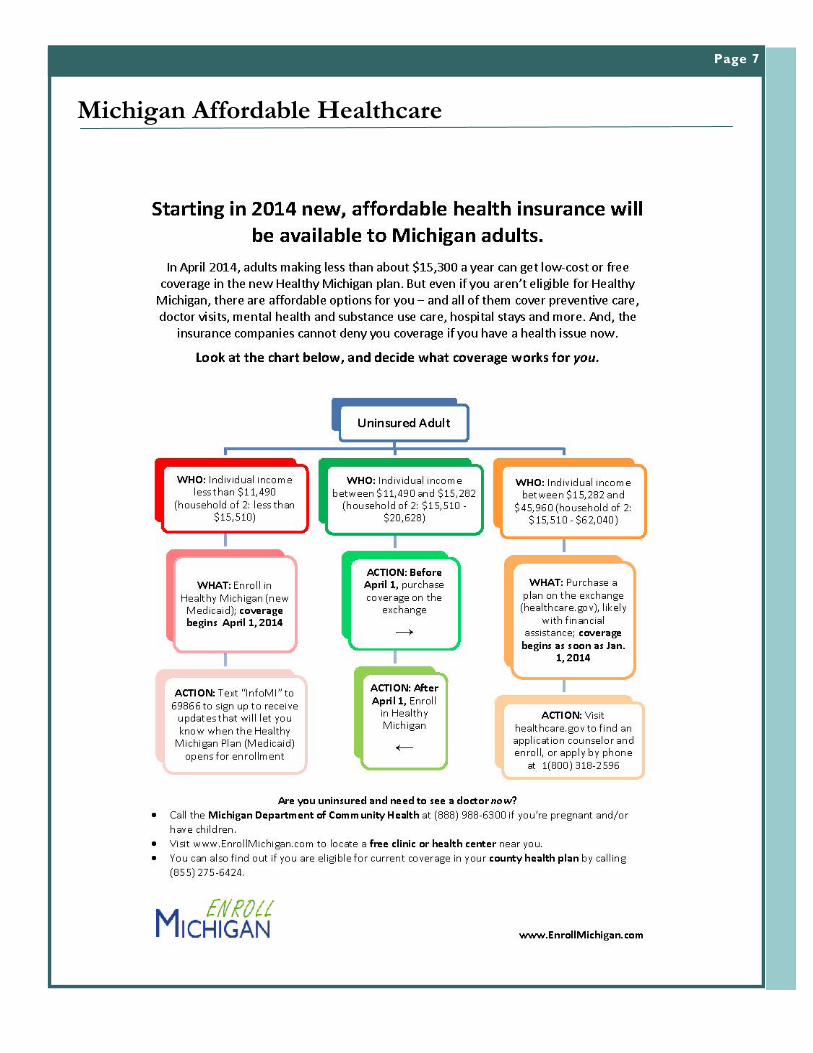
Members encountering uninsured patients who may be eligible for the Healthy Michigan plan (expanded Medicaid) in 2014 should instruct those patients to text “InfoMI” to the number 69866. Doing so will register them for text updates, sponsored by the Enroll Michigan coalition, on en-rollment in the Healthy Michigan plan and other helpful coverage information. Members are also encouraged to distribute informational flyers to un-insured patients who have not yet determined their eligibility for new coverage. The Healthy Michigan plan is expected to take ef-fect April 1, 2014 and will provide health insurance to more than 400,000 uninsured adults who make up to $11,490 (for an individual) annually. Members with questions about the flyer or text message ser-vice may contact Ruthanne Sudderth ([email protected]) at the Michigan Health & Hospital Association. See page 7 for more information!
Answers on page 9
Page 4
Member Profile
Page 4
Melissa Alcumbrack Melissa currently works as a Financial Analyst for Spectrum Health in Grand Rapids. She received her BBA and MSA from Western Michigan University; while in college, she worked in accounting for a couple manufacturing businesses. Following graduation, Melissa went on to work in public accounting at Crowe Horwath, LLP in tax for about a year and a half, and received her CPA license.
Melissa chose to move out of public accounting and into healthcare because she knew there would be new challenges in this changing industry; also, she really appreciates working for a nonprofit organization and the care that Spectrum brings to the community as well as its employees. Since Melissa is new to the healthcare industry she is hoping her HFMA membership will help her gain useful healthcare knowledge that she can apply to her job. She looks forward to meeting new people and learning what organizations can do to meet the upcoming challenges facing the healthcare community. Outside of work, Melissa’s greatest passion is training, and riding horses; she also enjoys taking her new puppy for walks, going camping, and any activity that is near water. Perhaps most important, Melissa is looking forward to getting married in May, 2014! Looking ahead, Melissa hopes to continue learning more about the healthcare industry and facilitate any necessary chang-es personally as well as within her organization to meet upcoming challenges.

Page 5
Cashing in on Revenue Cycle Improvements
Page 5
There is nothing more important to potential creditors than a borrower’s liquidity position. With all of the uncertainty in the health care industry—and the economy today for that matter—there is no substitute for the margin of safety and flexibility that cash provides. Most health care providers recognize the importance of liquidity and treat the cash on their balance sheet as sacred. But defending the balance sheet is only part of the battle. Surprisingly, many managers fail to take the necessary steps to increase their liquidity position. Of course, there are myriad factors that can undermine a hospital’s efforts to generate cash flow from operations: payor reimbursement, economic conditions, competitive landscape, cost and supply of labor, demographics of the market, etc. While it is true that hospital management has little to no control over these factors, there are other areas where it could have an equal—if not greater—impact to the credit profile. In particular, managing the payment cycle can help cash flow, but it also serves as a signal to potential creditors. Having a consistent focus on improving these measures demonstrates to creditors that manage-ment is competent and attentive to issues that it can affect. Conversely, large fluctuations in bad debt ex-pense and/or days in accounts receivable or a large percentage of “old” receivables causes a financial analyst to question the competency of management and the integrity of the historical income statements. Challenges to Increasing Liquidity The Affordable Care Act introduces additional uncertainty into an already murky revenue picture for health care providers throughout the country. Who is covered by insurance and how much will the in-sured be required to self-fund will likely remain uncertain for some time. Although state budgets have improved somewhat, uncertainty remains in state Medicaid reimbursement programs. The integration of technology, such as electronic health records, holds great long-term promise, but short-run costs, shifting requirements and implementation challenges make planning difficult. Most creditors will expect a com-petent management team to have a plan, which is robust enough to provide flexibility with each of the above factors; however, banks and other creditors also recognize that these issues are challenges and any plan to address them will be fraught with uncertainty. Given the uncertainty of supply/demand, pricing and expenses, it is imperative that providers improve cash flow through factors that are within their control. Indeed, it is more important than ever that man-agement develop a “fortress balance sheet,” to borrow a term often used in the banking industry. One clear indication of the importance of liquidity is the view of the rating agencies. The measures: cash to debt and days cash on hand have the clearest correlation to hospital ratings of all the metrics shown in the Standard and Poor’s industry medians. Obviously, increasing revenue and cutting expenses are two ways of increasing cash, but options for affecting the profit and loss statement are usually limited. One can do nothing about the supply/demand balance and there is little to be done about reimbursement rates. Cutting expenses is always good, but by far the largest expense—personnel costs—is the hardest and most painful to cut. Other sources of revenue—investment income, contributions, government alloca-tions, etc.—are usually dependent on external factors, which defy management intervention.
by: Ritchie Dickey, Lancaster Pollard
Continued on page 10

Page 6
Career Opportunities
If you have a healthcare position that you would like posted for your facility, please contact Dennis Page at dennisp@abscollect or (616) 741-0441. There is no charge as we see this as a benefit to our members. Please go to our website at www.wmihfma.org to see more detailed information on the postings below. MICHIGAN BASED POSITIONS:
Collections & Customer Service Coordinator: Holland Hospital
Manager of Patient Financial Services: Holland Hospital
Manager of Reimbursement: McLaren Greater Lansing
Revenue Cycle Manager: Baraga County Memorial Hospital
NATIONAL POSITIONS: Revenue Cycle Director: Genesis Healthcare System (OH)
Director of Accounting: Illinois Hospital System
CBO Directors: Pennsylvania & Mississippi
Page 7
Michigan Affordable Healthcare

Page 8
Imagine being sick and uninsured. ... Now imagine the worries that might plague you. Are you sick "enough" to require care? Where do you go? Will a provider see you? How will you pay the bill?
As a provider, a different set of worries plagues you when uninsured patients decide they do require care –and walk through your doors. Imagine if your staff could ask these patients a few questions to determine if they are eligible for immediate Medicaid coverage. A new option under the Affordable Care Act
(ACA) is making this possible for many.
Presumptive Eligibility Presumptive eligibility (PE) enables qualified hospitals to make immediate (but temporary!) decisions about patients' eligibility for Medicaid and the Children's Health Insurance Program (CHIP) based on preliminary information, like gross family income. This up-front decision connects the patient to Medicaid coverage without going through the full eligibility and verification process.
In turn, hospitals are reimbursed for services provided during this temporary eligibility period. Reimbursement begins for services provided the day the PE decision is made and is awarded at regular Medicaid rates, even if the patient eventually is determined ineligible for Medicaid.
Following a hospital's PE decision, patients are required to submit a full application through the regular process. In the meantime, patients' temporary coverage will continue until the day a full Medicaid or CHIP decision is rendered or on the last day of the month following the PE determination if an application has not been filed, whichever is earlier.
PE is a practice today used by some hospitals, but under the ACA it will be an option extended to all qualified hospitals. Although PE is a state policy option, qualified hospitals that provide Medicaid services will be
allowed to use PE even if a state does not choose to implement it.
Provider Considerations Providers will be required to maintain a certain level of accuracy when executing PE determinations and may be required to help patients complete the full Medicaid application process. These types of regulations will be established by on a state-by-state basis.
Providers should keep in mind the follow-up work required to ensure patients granted coverage through PE successfully complete a full application. This could mean additional work for hospital staff in the area of outreach, screening and application assistance.
Although PE creates the opportunity for a Win-Win situation for both the patient and provider, hospitals should exercise caution to ensure they are aware of and prepared to manage follow-up requirements, including tracking for compliance purposes.
For more information on presumptive eligibility, visit the L&S Associates website and check out our Industry Resources section, located under News & Events.
Presumptive Eligibility and Health Care Reform

Page 9
Do The Math - Investing in Fundraising Can Really Pay Off
M any hospital fundraising programs are
underperforming and underfunded.
And although performance improve-
ment initiatives are increasingly common in hospi-
tals, they are still rare in hospital fundraising opera-
tions.
As a source of internally generated capital, your
hospital’s or health system’s fundraising operation is
becoming increasingly important. And with the
bond rating agencies now factoring in your perfor-
mance in philanthropy, your interest in the mysteries
of fundraising should be increasing.
If you do the math, it’s clear that investing in fund-
raising operations can really pay off. To demonstrate
how in the health care world, let’s compare invest-
ing in facilitating philanthropy with investing to build
service line volume. Although net margins vary from
hospital to hospital — with many struggling to make
2 percent or 3 percent — for the sake of comparison
let’s assume that your hospital is netting 5 percent
from service line operations.
Fundraising costs vary, as well. Taking into account
development staff time and associated expenses,
the true cost can be as low as 20 cents per dollar
raised, or less in highly effective fundraising opera-
tions. It also can be significantly higher in fundraising
operations that do not yield a good return on invest-
ment.
Let’s assume your hospital’s fundraising operation is
running a 25 percent cost ratio.
Based on these assumptions, what’s the result if we
invest $1 million to increase service line revenue and
another $1 million to increase philanthropic revenue,
and both efforts are successful? Through philanthro-
py, you need to bring in $4 million in gifts to put $3
million on the bottom line. Through service line oper-
ations, you need to earn $60 million in revenue to
get the same bottom line results.
So if you put a fundraising performance improve-
ment initiative in place, and it yields an additional $4
million in philanthropy, you achieve the same bot-
tom line impact as increasing other revenue by $60
million — or even more, depending on the service
line’s operating margin and the hospital’s fundrais-
ing costs.
How do you achieve such results? The solution starts
with a multiyear fundraising business plan presenting
a strong performance improvement program, a
credible financial pro forma, and a discussion that
builds confidence in the strategy and shows a dili-
gent assessment of risk vs. reward.
Reed is president of the Performance Advantage unit of Mar-keting Partners, Inc., with offices in Michigan and Florida. He is long-time member of HFMA. His primary focus is the ap-plication of lean six sigma thinking in performance improve-ment for healthcare fundraising. He may be reached at [email protected].
by: Steven A. Reed, Member, Western Michigan Chapter HFMA

Page 10
Cashing in on Revenue Cycle Improvements continued
Uncovering Cash Trapped in Working Capital Given the lack of options for intervention on the revenue side and the challenges for affecting change on the expense side, one might feel as though balance sheet improvement is not possible. This view fails to recognize that there might be significant cash tied up in working capital and this is an area where management can exert influence. In fact, decreasing just five days in the payment cycle can have huge impact on company’s balance sheet.
The example may appear trivial, but five days of accounts receivable (AR) represents more than $4 million in this case. Many health care providers can achieve changes of this magnitude in 6 months to one year, with proper attention and a focus on gradual improvements. Representatives of Com-munity Hospital Corporation, a company that pro-vides consulting and management services to rural and community hospitals, noted that even more extreme examples exist. In one case, a hospital was showing more than 30 days of “unbilled” ac-counts, resulting in serious cash flow shortfalls. The example in the table also points out the in-creased margin of safety from turning over ac-counts receivable. If an emergency occurred, this
organization would not have excess cash to cover its obligations; likely, it would have to sell assets, factor receivables or execute some other compro-mise. This demonstrates the danger of looking at working capital as a measure of short-term liquidi-ty strength. Reducing its days in accounts receiva-ble by 10% effectively creates an emergency fund of more than $4 million. Furthermore, an increase in accounts receivable balances often signals to an analyst a number of problems: revenue may have been overstated, bad debt may have been under-stated, management is unable or unwilling to ef-fectively deal with its payers, processes and proce-dures are not adequate to process claims and a host of other deficiencies that relate to management effectiveness.
The process of filing and collecting claims is lengthy even in the best of circumstances, but of-tentimes hospitals focus solely on the tail end of the process (i.e., collections). Clearly, collecting for services rendered is vital, but there are a num-ber of steps prior to collections, which provide an opportunity to eliminate waste. This is an area where hospitals can learn from process improve-ment techniques used in other industries. Process Improvement Using Toyota Production System’s or other lean manufacturing methodology, providers can focus on eliminating waste and making the process more efficient. As with any process, there is an oppor-tunity to eliminate waste at every stage and there are many different kinds of waste: transportation, inventory, motion, waiting, overprocessing, over-production, defects, resources and talent. All of which can contribute to time in the process. One key point that the most effective providers emphasize is precertification on the front end. Ob-taining authorization before a patient even arrives is a key to eliminating waste later in the process.
Continued on page 11

Page 11
Cashing in on Revenue Cycle Improvements continued
The idea is that taking extra time and devoting re-sources before the patient arrives eliminates the need to hassle patients or negotiate with insurers later in the process and more importantly, upfront authoriza-tion greatly reduces bad debt due to misunderstand-ing over coverage or inability to pay. Precertification also provides an opportunity to improve patient satisfaction. By clearly articulating the patient’s financial responsibility before a proce-dure, indeed before the patient arrives, the hospital avoids promoting sticker shock and limits difficult conversations when a patient does not have the ca-pacity to pay. Failure to precertify procedures tends to create waste of overproduction and overpro-cessing. Another key aspect of efficiency within the revenue cycle is the education and training of persons respon-sible for tasks throughout the billing cycle. With the rapid changes in the health care industry, it is diffi-cult to stay up to date on requirements. In addition, constantly evolving technology and system infra-structure can create a stressful environment for those responsible for managing the system. Keeping the workforce confident that they are performing the job accurately is important and training is vital in this regard. Perhaps equally important is ensuring that the staff is accountable for and empowered in perform-ing the tasks from scheduling through billing and collections. Generally, billing errors are the result of poor training or a failure of institutional focus on the importance of quality. Errors of this type are known as “defects” in lean manufacturing terminology and this is perhaps the most expensive form of waste as defects often lead to performing the same task two or more times. Ideally, work teams can be cross-trained to ensure a full understanding of the process and the organiza-tional structure is arranged to minimize hand-offs between departments. Movement of activities be-tween departments tends to create waste by “inventory” build-up, “waiting” times, and increases the risk of “defects.”
Many providers despair of the inability to make sig-nificant reductions in bad debt or days in accounts receivable, but as with any task, advancement is a gradual evolution of marginal improvements. Con-sidering the demands on time of management and staff, it may seem difficult to justify devoting re-sources to process improvement, but the benefit of increased liquidity and demonstration of manage-ment effectiveness can greatly enhance a provider’s credit profile.
Ritchie Dickey is a vice president with Lancaster Pollard and is based out of the firm’s office in Atlan-ta. He may be reached at: [email protected].
Hyperlinks: Liquidity: http://www.investopedia.com/terms/ l/liquidity.asp Measures; http://www.lancasterpollard.com/news/TCI-june-july-2012-fe-financial-fitness Toyota Production System’s or other lean manufac-turing methodology: http://en.wikipedia.org/wiki/Lean_manufacturing

Page 12
Chapter Happenings
Chapter Happenings
(L) Barb Shelley presents (R) Mary Oomen the Follmer Award for outstanding service
Joel Bersche and Lisa St. Aubin
Left to Right: Kathie Townsend, Vickie Kunz and Kathy Fletcher
Catherine Sinning (L) and Lisa Platte (R)
Tom Salisbury and Julie Zukowski

Page 13
Chapter Happenings
L to R: Kathy Fletcher, Mark Johnson, and Kathie Townsend
Rhonda VanDrunen, David Raymond, Terry Steele
Tom Moyer and Barb Shelley
Barb Shelley presents Gerhard Schuett with the Frederick T. Muncie Gold Award

Page 14
We’re on the web! www.wmihfma.org
Western Michigan Chapter Newsletter strongly encourages submission of material for
publication. Articles should be typewritten and submitted to the editor three weeks prior to the deadlines listed below. The editor reserves the right to edit materials and accept or reject
contributions whether solicited or not. HFMA Founders
points are granted for any arti-cles published in Western
Michigan Chapter Newsletter.
Design and Layout Coordinator
Pam Allen The Rybar Group, Inc.
Address communications to:
Western Michigan Chapter Newsletter
Editor Thomas Salisbury
Pennock Health System 1009 W Green Street
Hastings, MI 49058 E-Mail:
Newsletter Schedule:
September 2013
November 2013
January 2014
March 2014
May 2014
Executive Committee
President: Barb Shelley
L & S Associates, Inc.
Past President: Barb Shelley
L & S Associates, Inc.
President Elect: Lisa St. Aubin
City of Eaton Rapids
Secretary: Lisa Fox
Hayes Green Beach Memorial Hospital
Treasurer: Rebecca Havlicek
Trinity Health
Director: Mary Oomen
North Ottawa Community Hospital
Director: Luke Check
Americollect
Director: Dave Roberts
Chesme Capital Financial
Director: Mark DeVirgilio
Reimbursement Consultant
Director: Joel Bersche
United Healthcare
HFMA Chairpersons
Chapter Matters: Dave Roberts Finance Committee
Oliver Jurkovic Nominating Committee
Barb Shelley Founders Committee
Cynthia Masselink Yerger Committee Rebecca Havlicek
Leadership Committee Barb Shelley
Education: Mary Oomen – Luke Check
Program Committee Mary Oomen
Spring Conference Program Committee Lisa Fox
Co-Chair: Barb Shelley Registration/Reception Committee
Elizabeth Hendren Rhonda VanDrunen
Sponsorship Committee Erv Kortering
Robin Beeman
Webinars Lisa Fox
Communication: Mark DeVirgilio
Public/Professional Relations Committee Dennis Page
Website Committee Dennis Page
Newsletter Committee Tom Salisbury
Rhiannon Bierenga
Membership: Joel Bersche Membership Committee
Joel Bersche Certification Committee
Gary Polkowski Directory Committee
Janice Myers





























